
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Drug Saf. Regul. , 04 August 2023
Sec. Advanced Methods in Pharmacovigilance and Pharmacoepidemiology
Volume 3 - 2023 | https://doi.org/10.3389/fdsfr.2023.1213771
 Takahiro Niimura1,2
Takahiro Niimura1,2 Mitsuhiro Goda1,3*
Mitsuhiro Goda1,3* Koji Miyata1
Koji Miyata1 Jun Matsumoto4Toshihiko Yoshioka1,3Hirofumi Hamano2,5
Jun Matsumoto4Toshihiko Yoshioka1,3Hirofumi Hamano2,5 Fuka Aizawa1,3
Fuka Aizawa1,3 Kenta Yagi1,2Yuki Izawa-Ishizawa1,6Yoshito Zamami1,5
Kenta Yagi1,2Yuki Izawa-Ishizawa1,6Yoshito Zamami1,5 Keisuke Ishizawa1,2,3
Keisuke Ishizawa1,2,3Introduction: The combination of atezolizumab, an immune checkpoint inhibitor (ICI), and bevacizumab, a vascular endothelial growth factor (VEGF) inhibitor, is the first choice for systemic therapy in hepatocellular carcinoma. Immune-related cardiovascular toxicity—myocarditis and pericarditis—are known to occur during ICI treatment. By contrast, VEGF inhibitors (VEGFIs) cause cardiovascular complications such as hypertension and heart failure. Thus, different cardiovascular toxicities have been recognized for ICIs and VEGFIs, but the impact of their combination remains unclear. Here, we aimed to investigate the cardiovascular toxicity profile of atezolizumab in combination with bevacizumab using the World Health Organization adverse event reporting database—VigiBase.
Methods: We analyzed data included in VigiBase till December 2022. To evaluate the frequency of reports related to atezolizumab, bevacizumab, and their combinations for 21 adverse events, we calculated the reporting odds ratio and information component. Analyses of the fatality of various cardiovascular toxicities associated with the use of each drug were performed.
Results: The database included 84,951, 10,595, and 2,092 reports of treatment with bevacizumab, atezolizumab, and their combination, respectively. The disproportionality signal of hypertension, arterial embolism and thrombosis, supraventricular tachyarrhythmias, heart failure, myocarditis, hemorrhage-related clinical events, venous embolism and thrombosis, cardiomyopathy, respiratory failure with combination regimen of atezolizumab and bevacizumab was detected. Signals of these adverse events were also detected treatment with either atezolizumab or bevacizumab alone. Venous embolism and thrombosis exhibited the highest fatality rate in the two drug combination (12.82%) relative to those of atezolizumab (6.19%) and bevacizumab (4.54%).
Discussion: Cardiovascular toxicity, owing to the combination of atezolizumab and bevacizumab, was similar to that of each single agent, and no new safety concerns were observed. Caution should be exercised when combining the two drugs since the fatality rate of thromboembolism increases with combination treatment.
Immune checkpoint inhibitors (ICIs) exert anti-tumor effects by inducing an immune response against tumors and have become the standard treatment for several types of cancer (Motzer et al., 2022; Reck et al., 2022; Shiravand et al., 2022). Recently, combination therapy with various molecular-targeted drugs has also been investigated. For example, vascular endothelial growth factor inhibitors (VEGFIs) improve tumor microenvironment and enhance the efficacy of immunotherapy by normalizing blood vessels and promoting the infiltration and activation of immune cells, including effector T cells (Ren et al., 2021). Since the excessive production of VEGF suppresses immunity, combination therapy with ICIs and VEGFIs has been used in hepatocellular carcinoma and other types of cancer to enhance the individual anti-tumor effect of ICIs and VEGFIs (Fukumura et al., 2018).
Although the combination of VEGFIs and ICIs may enhance anti-tumor effects, both VEGFIs and ICIs are associated with cardiovascular toxicities, including hypertension, heart failure, and pericardial disease (Salem et al., 2018). Bevacizumab, a VEGFI, is associated with cardiovascular toxicities such as hypertension and thrombosis due to vascular endothelial damage caused by VEGF inhibition (Ferrara, 2004), while ICIs cause myocarditis and other conditions through activation of various immune responses, including T cells (Moslehi et al., 2021).
Therefore, VEGFIs and ICIs manifest their cardiovascular toxicity via their effects on vascular endothelial cells and immune cells, respectively. VEGF signaling affects immune cells, including T and dendritic cells, and a combination of VEGFIs and ICIs may enhance cardiovascular toxicity and increase risk (Yi et al., 2019; Ren et al., 2021). The cardiovascular toxicity profile of VEGFIs and ICIs combination has not yet been determined.
Therefore, in this study, we investigate the cardiovascular toxicity profile of atezolizumab in combination with bevacizumab using the World Health Organization (WHO) adverse event reporting database and determine the differences in the cardiovascular toxicity profiles of each drug alone.
VigiBase, the global WHO database of adverse events, provides data on reported potential side effects of medicinal products and is maintained by the Uppsala Monitoring Centre and is the world’s largest database of adverse event reports, with more than 28 million reports collected globally since 1968 (Uppsala Monitoring Centre, UMC, 2023, VigiBase). In this study, we used data provided by VigiBase as of December 2022. VigiBase contains duplicate reports; hence, the reports determined by the Uppsala Monitoring Centre to have the potential for duplicate reporting were excluded from the analysis. Of the 33,188,305 reports, 32,520,983 were included in the analysis, excluding 667,322 reports suspected of duplication. Downloaded data were processed using SQLite databases 3.33.0 (SQLite Consortium, Charlotte, NC, United States). The requirement of informed consent from patients was waived for this study because this is an observational study using anonymized data from a global database (VigiBase), which did not involve any treatment intervention or collection of human samples.
In this study, we used the definition of adverse events as per the description provided in the Medical Dictionary for Regulatory Activities (MedDRA) developed by the International Conference on Harmonization of Technical Requirements for the Registration of Pharmaceuticals for Human Use (ICH, 2019, MedDRA). Twenty-one cardiovascular toxicities, including hypertension, hemorrhage, embolism and thrombosis, arrhythmias, and myocarditis, of atezolizumab, bevacizumab, and their combination were investigated as previously described (Salem et al., 2018; Goldman et al., 2021). Each cardiovascular toxicity is defined in Supplementary Table S1.
Categorical variables are summarized as frequencies and percentages. A disproportionality analysis was performed to identify the relationship between drugs and adverse events. Reporting odds ratios (RORs) and information components (IC) were used as indicators in the disproportionality analysis (Bate et al., 1998; Rothman et al., 2004; Norén et al., 2013). Adverse event reports were divided into four groups: 1) the number of reports on specific adverse events for a drug of interest, 2) the number of reports on other adverse events for a drug of interest, 3) the number of reports on specific adverse events without a drug of interest, and 4) the number of reports on other adverse events without a drug of interest. RORs were calculated as follows:
ICs were calculated using the number of expected reports no specific adverse event for the drug of interest (Nexpected) and the number of reports on a specific adverse event for the drug of interest (Nobserved), as follows:
A signal was detected when the lower limit of the 95% confidence interval (CI) for RORs and ICs exceeded 1 and 0, respectively (Bate et al., 1998; van Puijenbroek et al., 2002). For ROR, the signal was evaluated when the number of (a) was >3. For adverse events for which a signal was detected in both ROR and IC, drug-drug interaction signals were evaluated using the Ω shrinkage measure. The signal was considered detected when the lower limit of the 95% confidence interval of the Ω exceeded 0 (Norén et al., 2008; Xia et al., 2022). Analyses of the fatality of various cardiovascular toxicities associated with the use of each drug were performed. These analyses were performed using R version 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria).
Overall, VigiBase included data from 32,520,983 reports, of which 84,951 involved bevacizumab use, 10,595 involved atezolizumab use, and 2,092 involved the use of both drugs. Approximately 60% of the reports in which age was stated reported an age of ≥45 years (23,867,872 reports stated the age vs. 14,538,974 reports stated an age of ≥45 years) (Supplementary Table S2).
The number of females in the bevacizumab group was higher than that of males (43,506 reports for females vs. 30,717 reports for males), whereas the number of males in the atezolizumab (5,478 reports for males vs. 4,194 reports for females) and two-drug combination groups (1,135 reports for males vs. 759 reports for females) was higher than that of females.
Bevacizumab treatment was associated with more reports of hypertension (95% CI min of ROR: 5.28, 95% CI min of IC: 2.31), arterial embolism and thrombosis (95% CI min of ROR: 2.26, 95% CI min of IC: 1.14), myocardial infarction (95% CI min of ROR: 1.42, 95% CI min of IC: 0.48), central nervous system ischemia (95% CI min of ROR: 2.32, 95% CI min of IC: 1.18), supraventricular tachyarrhythmias (95% CI min of ROR: 2.03, 95% CI min of IC: 0.99), ventricular tachyarrhythmias (95% CI min of ROR: 1.89, 95% CI min of IC: 0.87), heart failure (95% CI min of ROR: 1.94, 95% CI min of IC: 0.93), shock (95% CI min of ROR: 1.35, 95% CI min of IC: 0.41), pericarditis (95% CI min of ROR: 1.19, 95% CI min of IC: 0.21), hemorrhage-related clinical events (95% CI min of ROR: 2.08, 95% CI min of IC: 1), bleeding-related laboratory abnormalities (95% CI min of ROR: 1.4, 95% CI min of IC: 0.42), cerebral hemorrhage (95% CI min of ROR: 2.01, 95% CI min of IC: 0.98), pulmonary hypertension (95% CI min of ROR: 1.57, 95% CI min of IC: 0.61), venous embolism and thrombosis (95% CI min of ROR: 6.25, 95% CI min of IC: 2.57), cardiomyopathy (95% CI min of ROR: 3.68, 95% CI min of IC: 1.84), respiratory failure (95% CI min of ROR: 1.36, 95% CI min of IC: 0.42) (Table 1).
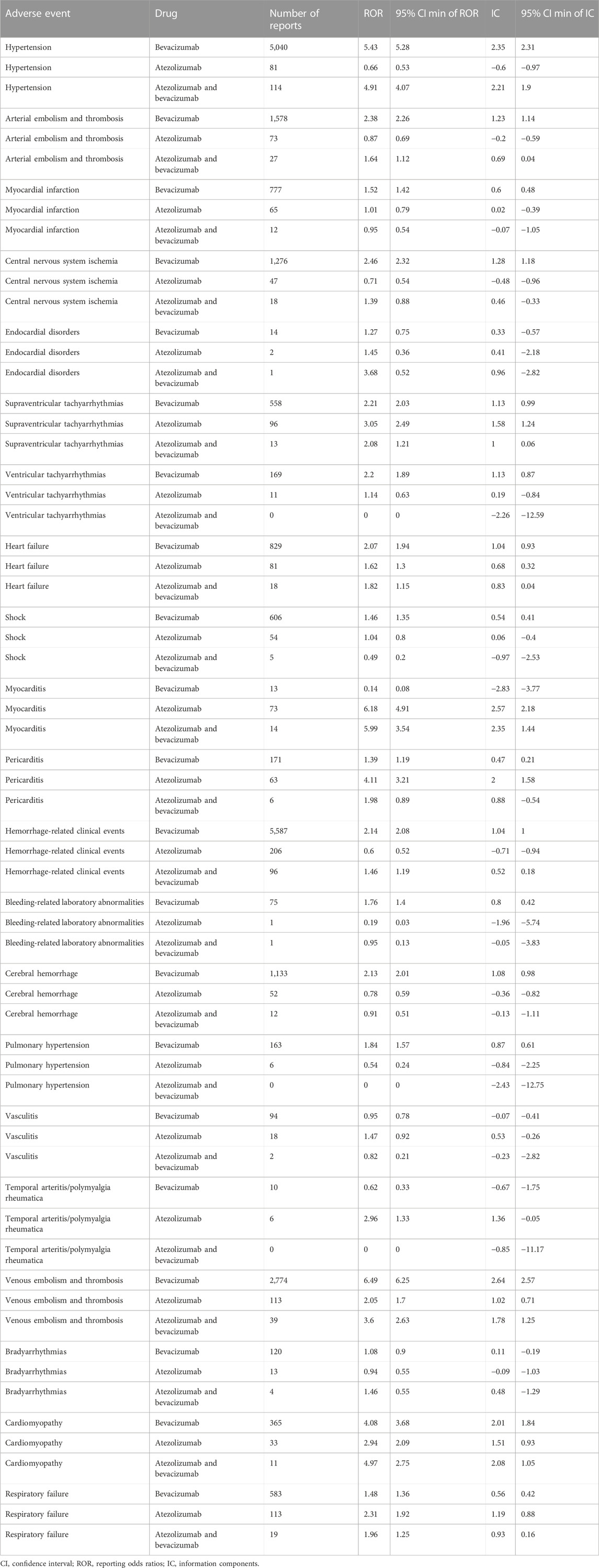
Table 1. Reporting odds ratio for cardiovascular toxicity in all reports.
In atezolizumab users, a significant increase in the reports of supraventricular tachyarrhythmias (95% CI min of ROR: 2.49, 95% CI min of IC: 1.24), heart failure (95% CI min of ROR: 1.3, 95% CI min of IC: 0.32), myocarditis (95% CI min of ROR: 4.91, 95% CI min of IC: 2.18), pericarditis (95% CI min of ROR: 3.21, 95% CI min of IC: 1.58), venous embolism and thrombosis (95% CI min of ROR: 1.7, 95% CI min of IC: 0.71), cardiomyopathy (95% CI min of ROR: 2.09, 95% CI min of IC: 0.93), respiratory failure (95% CI min of ROR: 1.92, 95% CI min of IC: 0.88) was observed.
The disproportionality signal of hypertension (95% CI min of ROR: 4.07, 95% CI min of IC: 1.9), arterial embolism and thrombosis (95% CI min of ROR: 1.12, 95% CI min of IC: 0.04), supraventricular tachyarrhythmias (95% CI min of ROR: 1.21, 95% CI min of IC: 0.06), heart failure (95% CI min of ROR: 1.15, 95% CI min of IC: 0.04), myocarditis (95% CI min of ROR: 3.54, 95% CI min of IC: 1.44), hemorrhage-related clinical events (95% CI min of ROR: 1.19, 95% CI min of IC: 0.18), venous embolism and thrombosis (95% CI min of ROR: 2.63, 95% CI min of IC: 1.25), cardiomyopathy (95% CI min of ROR: 2.75, 95% CI min of IC: 1.05), respiratory failure (95% CI min of ROR: 1.25, 95% CI min of IC: 0.16) with the two-drug combination regimen of bevacizumab and atezolizumab was detected.
A disproportionality analysis by sex and age was also performed (Supplementary Tables S3–S6). Arterial embolism and thrombosis (male[95% CI min of ROR: 0.49, 95% CI min of IC: −1.19], female[95% CI min of ROR: 1.87, 95% CI min of IC: 0.65]), heart Failure (male[95% CI min of ROR: 0.73, 95% CI min of IC: −0.68], female[95% CI min of ROR: 1.56, 95% CI min of IC: 0.29]), respiratory failure (male[95% CI min of ROR: 0.72, 95% CI min of IC: −0.7], female[95% CI min of ROR: 1.79, 95% CI min of IC: 0.5]), myocarditis (male[95% CI min of ROR: 2.35, 95% CI min of IC: 0.83], female[95% CI min of ROR: 1.06, 95% CI min of IC: −1.23]), hemorrhage-related clinical events (male[95% CI min of ROR: 1.17, 95% CI min of IC: 0.13], female[95% CI min of ROR: 0.86, 95% CI min of IC: −0.32]), cardiomyopathy (male[95% CI min of ROR: 1.77, 95% CI min of IC: 0.27], female[95% CI min of ROR: 1.5, 95% CI min of IC: −0.46])showed differences in the frequency of reports in the stratified analysis by sex for atezolizumab and bevacizumab users.
In the age-stratified analysis, differences were observed in the frequency of event reports for heart failure (young[95% CI min of ROR: 1.82, 95% CI min of IC: 0.63], old[95% CI min of ROR: 0.17, 95% CI min of IC: −3.02]), hemorrhage-related clinical events (young[95% CI min of ROR: 1.14, 95% CI min of IC: 0.11], old[95% CI min of ROR: 0.58, 95% CI min of IC: −0.89]), cardiomyopathy (young[95% CI min of ROR: 2.97, 95% CI min of IC: 0.99], old[95% CI min of ROR: 0.46, 95% CI min of IC: −2.88]), respiratory failure (young[95% CI min of ROR: 1.18, 95% CI min of IC: 0.03], old[95% CI min of ROR: 1.05, 95% CI min of IC: −0.42]) for atezolizumab and bevacizumab users.
For adverse events in which both ROR and IC signals were detected, drug-drug interactions were evaluated using the Ω shrinkage measure (Table 2). Five adverse events were evaluated, namely, supraventricular tachyarrhythmias (Ω: −0.99, 95% CI lower limit: −1.78), heart failure (Ω: −0.54, 95% CI lower limit: −1.21), venous embolism and thrombosis (Ω: −1.01, 95% CI lower limit: −1.47), cardiomyopathy (Ω: −0.26, 95% CI lower limit: −1.11), and respiratory failure (Ω: −0.49, 95% CI lower limit: −1.14). No signal was detected in any of the adverse events.
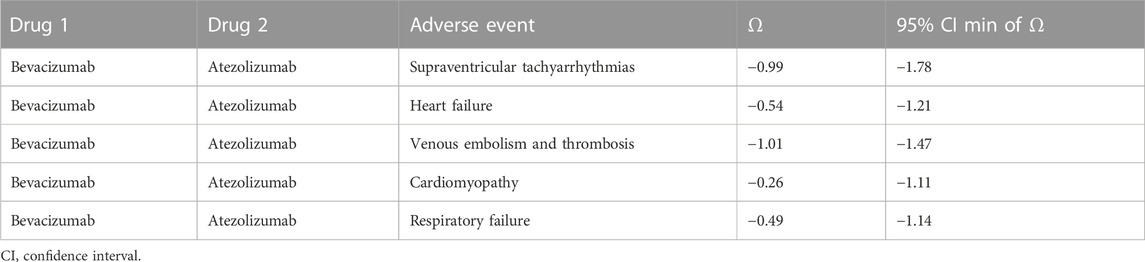
Table 2. Drug-drug interaction signals for cardiovascular toxicity in all reports.
Fatality rates were evaluated for five adverse events in which signals were detected for the combination of atezolizumab and bevacizumab (Figure 1). Venous embolism and thrombosis exhibited the highest fatality rate in the two-drug combination (12.82%) compared with that of atezolizumab (6.19%) or bevacizumab (4.54%) alone. In the case of respiratory failure, the fatality rate of two-drug combination (36.84%) was lower than that of atezolizumab (40.71%) but higher than that of bevacizumab (28.30%). No deaths were reported due to cardiomyopathy (atezolizumab: 6.06%, bevacizumab: 3.56%), hypertension (atezolizumab: 1.23%, bevacizumab: 0.32%), or supraventricular tachyarrhythmias (atezolizumab: 2.08%, bevacizumab: 1.43%) for the two-drug combination group.
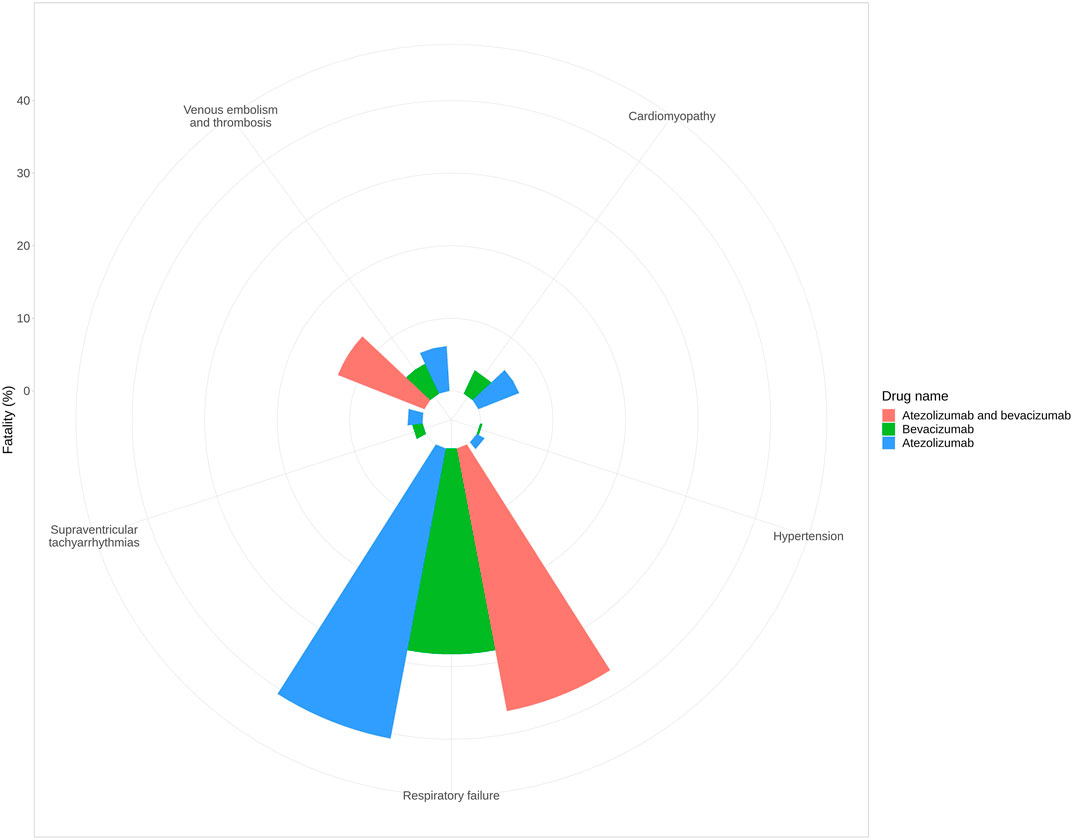
Figure 1. Fatality rate of each adverse event.
This study systematically analyzed the world’s largest adverse events database—VigiBase—to determine the cardiovascular toxicity profile of atezolizumab, bevacizumab, and their combination. The cardiovascular toxicity of the combination of atezolizumab and bevacizumab can be predicted from the cardiovascular toxicities of each drug, and no synergistic increase in adverse events was observed when the two drugs were co-administered. With regard to thromboembolism, a trend toward a higher fatality rate was demonstrated for the combination of atezolizumab and bevacizumab relative to their individual use.
In addition to the combination of atezolizumab and bevacizumab for hepatocellular carcinoma treatment, ICI- and VEGFI-based anticancer therapies are being developed for various cancers, such as gastric and gastroesophageal adenocarcinomas (Saeed et al., 2021). Particularly, a VEGF inhibitor in combination with a PD-1/PD-L1 inhibitor has shown favorable results in PD-1/PD-L1 inhibitor-resistant patients, and the combination therapy of ramucirumab and pembrolizumab is under investigation (Reckamp et al., 2022). However, there is limited data on the cardiovascular toxicity profile of the two types of inhibitors when used together.
To our knowledge, this is the largest study to investigate the cardiovascular toxicity profile of atezolizumab in combination with bevacizumab. We utilized the global WHO database of spontaneous adverse event reports to investigate a wide range of cardiovascular toxicities that are difficult to assess in individual clinical trials. The results of this study suggest that management should consider the respective cardiovascular toxicity profiles when both drugs are used in combination.
In the current study, we observed a trend toward a higher lethality rate of venous embolism and thrombosis when ICIs and VEGFIs were used together compared with their individual use. The mechanisms involved in the increased frequency of thromboembolism with ICIs remain unclear but include increased tissue factor production in monocytes associated with T-cell activation (Zou et al., 2021). In addition, a higher risk of venous thromboembolism has been reported in patients with c-reactive protein flares early after ICI administration (Moik et al., 2022), and increased secretion of various cytokines associated with inflammatory responses may contribute to coagulation abnormalities. The possible mechanisms of thromboembolism caused by VEGFIs include exposure to procoagulant phospholipids under the endothelium by inhibiting endothelial cell regeneration and decreased production of nitric oxide and prostacyclin (Kamba and McDonald, 2007; Nalluri et al., 2008). Therefore, it is possible that a potent reaction occurs when the two drugs were used together since each has a different mechanism contributing to thromboembolism formation. More detailed studies will be needed in the future regarding the risk of thromboembolism when both drugs are used together.
Thromboembolism is a multifactorial condition with various risk factors (Eichinger, 2016; Hamza and Mousa, 2020). Studies evaluating the risk of thromboembolism associated with cancer chemotherapy suggest that the risk of thromboembolism is significantly higher in patients older than 70 years than that in those younger (Vergati et al., 2013). Regarding sex, females are reportedly at risk for cancer-related thromboembolism, including patients not receiving chemotherapy (Khorana et al., 2007). Similar to the results of studies on these risk factors, the present study showed that thromboembolism was reported more frequently in elderly patients and females among those who received atezolizumab plus bevacizumab. By contrast, thromboembolism was reported less frequently in males who received atezolizumab plus bevacizumab than in patients who did not. Since the incidence of thromboembolism is influenced by the type of cancer and the presence or absence of radiation therapy, more detailed studies on the effect of sex differences on the incidence of thromboembolism associated with atezolizumab plus bevacizumab are needed (Abdol Razak et al., 2018).
This study has some limitations. First, this study was conducted using a database of spontaneous adverse event reports, and it was not possible to determine the causal relationship between each drug and the reported adverse events. The study only reports an association between the drugs and the adverse events, and more prospective observational studies should be conducted in the future. However, the results of previous studies were similar with regard to the risk of cardiovascular toxicity when atezolizumab and bevacizumab were used individually (Economopoulou et al., 2015; Totzeck et al., 2017; Ball et al., 2019; Gan et al., 2022). Second, the past treatment and medical history of the patients included in this study are unclear. Various anticancer drugs and underlying diseases act as risk factors for cardiovascular diseases. There may be differences in the presence or absence of risk factors between the use and non-use groups for each drug. Third, there is a possibility of adverse event reporting bias since VigiBase accumulates data from various sources, including medical professionals and pharmaceutical companies. In addition, management practices for adverse events may have changed depending on the reporting year.
To the best of our knowledge, no other studies have investigated the cardiovascular toxicity profile of ICIs in combination with anti-VEGF antibodies. Antibodies have different targets of action and, therefore, different adverse events. In the current study, we found that the adverse event profiles of both drugs, when used in combination, reflect the adverse event profiles of each drug when used alone, but with some differences. Cardiovascular toxicity induced by these drugs can sometimes be lethal and requires close monitoring. The results of this study contribute to the management strategies necessary to ensure the safety of cancer immunotherapy.
The data analyzed in this study is subject to the following licenses/restrictions: Data will be made available upon requests directed to the corresponding author and after approval of a proposal. Requests to access these datasets should be directed to TN, bmlpbXVyYUB0b2t1c2hpbWEtdS5hYy5qcA==.
Study design, data collection, analysis, interpretation, and statistical analysis: TN, KM, JM, and TY. Drafting manuscript: TN, JM, and HH. Revision manuscript: TN, MG, JM, HH, FA, KY, YI-I, YZ, and KI. All authors contributed to the article and approved the submitted version.
This research was supported by grants from the Japan Society for the Promotion of Science Grants-in-Aid for Scientific Research (grant numbers: 21K20720 and 22K15319) and Grant-in-Aid for Transformative Research Areas (B) (grant number: 20H05798).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fdsfr.2023.1213771/full#supplementary-material
Abdol Razak, N. B., Jones, G., Bhandari, M., Berndt, M. C., and Metharom, P. (2018). Cancer-associated thrombosis: An overview of mechanisms, risk factors, and treatment. Cancers 10, 380. doi:10.3390/cancers10100380
Ball, S., Ghosh, R. K., Wongsaengsak, S., Bandyopadhyay, D., Ghosh, G. C., Aronow, W. S., et al. (2019). Cardiovascular toxicities of immune checkpoint inhibitors: JACC review topic of the week. J. Am. Coll. Cardiol. 74, 1714–1727. doi:10.1016/j.jacc.2019.07.079
Bate, A., Lindquist, M., Edwards, I. R., Olsson, S., Orre, R., Lansner, A., et al. (1998). A Bayesian neural network method for adverse drug reaction signal generation. Eur. J. Clin. Pharmacol. 54, 315–321. doi:10.1007/s002280050466
Economopoulou, P., Kotsakis, A., Kapiris, I., and Kentepozidis, N. (2015). Cancer therapy and cardiovascular risk: Focus on bevacizumab. Cancer Manag. Res. 7, 133–143. doi:10.2147/CMAR.S77400
Eichinger, S. S. (2016). Cancer associated thrombosis: Risk factors and outcomes. Thromb. Res. 140 (1), S12–S17. doi:10.1016/S0049-3848(16)30092-5
Ferrara, N. (2004). Vascular endothelial growth factor: Basic science and clinical progress. Endocr. Rev. 25, 581–611. doi:10.1210/er.2003-0027
Fukumura, D., Kloepper, J., Amoozgar, Z., Duda, D. G., and Jain, R. K. (2018). Enhancing cancer immunotherapy using antiangiogenics: Opportunities and challenges. Nat. Rev. Clin. Oncol. 15, 325–340. doi:10.1038/nrclinonc.2018.29
Gan, L., Liu, D., Ma, Y., Chen, X., Dai, A., Zhao, S., et al. (2022). Cardiotoxicity associated with immune checkpoint inhibitors: Current status and future challenges. Front. Pharmacol. 13, 962596. doi:10.3389/fphar.2022.962596
Goldman, A., Maor, E., Bomze, D., Liu, J. E., Herrmann, J., Fein, J., et al. (2021). Adverse cardiovascular and pulmonary events associated with chimeric antigen receptor T-cell therapy. J. Am. Coll. Cardiol. 78, 1800–1813. doi:10.1016/j.jacc.2021.08.044
Hamza, M. S., and Mousa, S. A. (2020). Cancer-associated thrombosis: Risk factors, molecular mechanisms, future management. Clin. Appl. Thromb. Hemost. 26, 1076029620954282. doi:10.1177/1076029620954282
ICH (2019). MedDRA. Available at: https://www.meddra.org/how-to-use/support-documentation/english (Accessed February 14, 2019).
Kamba, T., and McDonald, D. M. (2007). Mechanisms of adverse effects of anti-VEGF therapy for cancer. Br. J. Cancer. 96, 1788–1795. doi:10.1038/sj.bjc.6603813
Khorana, A. A., Francis, C. W., Culakova, E., Kuderer, N. M., and Lyman, G. H. (2007). Frequency, risk factors, and trends for venous thromboembolism among hospitalized cancer patients. Cancer 110, 2339–2346. doi:10.1002/cncr.23062
Moik, F., Riedl, J., Barth, D., Chan, W. E., Wiedemann, S., Höller, C., et al. (2022). Early dynamics of C-reactive protein predict risk of venous thromboembolism in patients with cancer treated with immune checkpoint inhibitors. Blood 140 (1), 1250–1251. doi:10.1182/blood-2022-160087
Moslehi, J., Lichtman, A. H., Sharpe, A. H., Galluzzi, L., and Kitsis, R. N. (2021). Immune checkpoint inhibitor–associated myocarditis: Manifestations and mechanisms. J. Clin. Invest. 131, e145186. doi:10.1172/JCI145186
Motzer, R. J., Jonasch, E., Agarwal, N., Alva, A., Baine, M., Beckermann, K., et al. (2022). Kidney Cancer, version 3.2022, NCCN clinical practice guidelines in oncology. J. Natl. Compr. Canc. Netw. 20, 71–90. doi:10.6004/jnccn.2022.0001
Nalluri, S. R., Chu, D., Keresztes, R., Zhu, X., and Wu, S. (2008). Risk of venous thromboembolism with the angiogenesis inhibitor bevacizumab in cancer patients: A meta-analysis. JAMA 300, 2277–2285. doi:10.1001/jama.2008.656
Norén, G. N., Hopstadius, J., and Bate, A. (2013). Shrinkage observed-to-expected ratios for robust and transparent large-scale pattern discovery. Stat. Methods Med. Res. 22, 57–69. doi:10.1177/0962280211403604
Norén, G. N., Sundberg, R., Bate, A., and Edwards, I. R. (2008). A statistical methodology for drug-drug interaction surveillance. Stat. Med. 27, 3057–3070. doi:10.1002/sim.3247
Reck, M., Remon, J., and Hellmann, M. D. (2022). First-line immunotherapy for non–small-cell lung cancer. J. Clin. Oncol. 40, 586–597. doi:10.1200/JCO.21.01497
Reckamp, K. L., Redman, M. W., Dragnev, K. H., Minichiello, K., Villaruz, L. C., Faller, B., et al. (2022). Phase II randomized study of ramucirumab and pembrolizumab versus standard of care in advanced non–small-cell lung cancer previously treated with immunotherapy-lung-MAP S1800A. J. Clin. Oncol. 40, 2295–2306. doi:10.1200/JCO.22.00912
Ren, S., Xiong, X., You, H., Shen, J., and Zhou, P. (2021). The combination of immune checkpoint blockade and angiogenesis inhibitors in the treatment of advanced non-small cell lung cancer. Front. Immunol. 12, 689132. doi:10.3389/fimmu.2021.689132
Rothman, K. J., Lanes, S., and Sacks, S. T. (2004). The reporting odds ratio and its advantages over the proportional reporting ratio. Pharmacoepidemiol. Drug Saf. 13, 519–523. doi:10.1002/pds.1001
Saeed, A., Park, R., and Sun, W. (2021). The integration of immune checkpoint inhibitors with VEGF targeted agents in advanced gastric and gastroesophageal adenocarcinoma: A review on the rationale and results of early phase trials. J. Hematol. Oncol. 14, 13. doi:10.1186/s13045-021-01034-0
Salem, J. E., Manouchehri, A., Moey, M., Lebrun-Vignes, B., Bastarache, L., Pariente, A., et al. (2018). Cardiovascular toxicities associated with immune checkpoint inhibitors: An observational, retrospective, pharmacovigilance study. Lancet Oncol. 19, 1579–1589. doi:10.1016/S1470-2045(18)30608-9
Shiravand, Y., Khodadadi, F., Kashani, S. M. A., Hosseini-Fard, S. R., Hosseini, S., Sadeghirad, H., et al. (2022). Immune checkpoint inhibitors in cancer therapy. Curr. Oncol. 29, 3044–3060. doi:10.3390/curroncol29050247
Totzeck, M., Mincu, R. I., and Rassaf, T. (2017). Cardiovascular adverse events in patients with cancer treated with bevacizumab: A meta-analysis of more than 20 000 patients. J. Am. Heart Assoc. 6, e006278. doi:10.1161/JAHA.117.006278
UMC (2023). Uppsala monitoring Centre. Available at: https://who-umc.org/vigibase/(Accessed January 7, 2023).
van Puijenbroek, E. P., Bate, A., Leufkens, H. G., Lindquist, M., Orre, R., and Egberts, A. C. (2002). A comparison of measures of disproportionality for signal detection in spontaneous reporting systems for adverse drug reactions. Pharmacoepidemiol. Drug Saf. 11, 3–10. doi:10.1002/pds.668
Vergati, M., Della-Morte, D., Ferroni, P., Cereda, V., Tosetto, L., La Farina, F., et al. (2013). Increased risk of chemotherapy-associated venous thromboembolism in elderly patients with cancer. Rejuvenation Res. 16, 224–231. doi:10.1089/rej.2013.1409
Xia, S., Gong, H., Zhao, Y., Guo, L., Wang, Y., Zhang, B., et al. (2022). Association of pulmonary sepsis and immune checkpoint inhibitors: A pharmacovigilance study. Cancers 15, 240. doi:10.3390/cancers15010240
Yi, M., Jiao, D., Qin, S., Chu, Q., Wu, K., and Li, A. (2019). Synergistic effect of immune checkpoint blockade and anti-angiogenesis in cancer treatment. Mol. Cancer. 18, 60. doi:10.1186/s12943-019-0974-6
Keywords: atezolizumab, bevacizumab, cardiovascular toxicity, thromboembolism, adverse event
Citation: Niimura T, Goda M, Miyata K, Matsumoto J, Yoshioka T, Hamano H, Aizawa F, Yagi K, Izawa-Ishizawa Y, Zamami Y and Ishizawa K (2023) Evaluation of cardiovascular toxicity of the atezolizumab and bevacizumab combination. Front. Drug Saf. Regul. 3:1213771. doi: 10.3389/fdsfr.2023.1213771
Received: 28 April 2023; Accepted: 30 June 2023;
Published: 04 August 2023.
Edited by:
Miao Yan, Central South University, ChinaReviewed by:
Long Meng, First Affiliated Hospital of Chongqing Medical University, ChinaCopyright © 2023 Niimura, Goda, Miyata, Matsumoto, Yoshioka, Hamano, Aizawa, Yagi, Izawa-Ishizawa, Zamami and Ishizawa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Mitsuhiro Goda, bWdvZGFAdG9rdXNoaW1hLXUuYWMuanA=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.