 Yun-Ting Huang
Yun-Ting Huang Craig McCarthy1
Craig McCarthy1 Meghna Jani
Meghna Jani
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Drug Saf. Regul., 16 February 2023
Sec. Rheumatic Drug Safety
Volume 3 - 2023 | https://doi.org/10.3389/fdsfr.2023.1117674
Pain management has been a challenging issue for people living with rheumatic and musculoskeletal diseases (RMDs) and health professionals for decades. Pharmacological treatments remain a core element of pain management of inflammatory arthritis and osteoarthritis. Yet balancing the benefits/harms in pain management within RMDs can be difficult to navigate due to limited effective options, and emerging adverse events in a population where individual risk is important to consider due to patient multimorbidity, immunosuppression and polypharmacy. Paracetamol and non-steroidal anti-inflammatory drugs (NSAIDs) analgesics are widely used among RMD patients, however both classes of drugs have been associated with new safety concerns in the last two decades. Perhaps as a result in combination with multifactorial influences, opioid prescribing has increased from the 2000s–2010s in the majority of RMD focussed studies, accompanied with a rising trend of long-term opioid use, despite limited evidence on efficacy. Gabapentinoids have also shown increasing trends more recently, despite an unclear role in chronic pain management for RMDs within current guidelines. Antidepressants are recommended as the first line of pharmacological treatment of chronic primary pain (e.g., fibromyalgia) by the latest National Institute for Health and Care Excellence (NICE) guideline released in April 2021. This concise narrative review will discuss pharmacological options for pain management, based on the latest evidence that includes the main analgesic drug classes: paracetamol, NSAIDs, opioids, antidepressants, and gabapentinoids. We will discuss the efficacy of these analgesics in RMDs and emerging safety concerns to enable more informed shared decisions with patients commencing such medications.
Pain management in people living with RMDs has been a challenge to address for health professionals for decades. From the 2000s–2010s (i.e., 2010-2019), there has been a considerable increase in the prescriptions of antidepressants (Ivanova et al., 2011; John et al., 2016), gabapentinoids (Torrance et al., 2020; Kuehn, 2022), and opioids (Kalso et al., 2004; Jani et al., 2020; Anastasiou and Yazdany, 2022) for pain management, especially chronic pain, worldwide. Recommendations for chronic pain internationally can vary considerably and are heterogeneous, depending on underlying conditions. According to the European Alliance of Associations for Rheumatology (EULAR) recommendations, pharmacological treatments continue to remain important in pain management of inflammatory arthritis and osteoarthritis (OA). The recent NICE guideline from April 2021 places more emphasis on non-pharmacological treatments and recommends antidepressants as the first-line pharmacological treatment of chronic primary pain (e.g., fibromyalgia) (National Institute for Health and Care Excellence, 2021a). The strategy for chronic pain caused by an underlying condition [e.g., rheumatoid arthritis (RA)] however is unclear in this guideline. Balancing the benefits and harms of pain medications within different RMDs can be difficult due to limited effective therapeutic options. These need to be considered with emerging adverse events in a population where individual risk is especially important because of the presence of multimorbidity, immunosuppression and polypharmacy.
Despite the widespread use of paracetamol and NSAIDs for pain control, evidence of new safety concerns has emerged in the last two decades. Other analgesics such as opioids and antidepressants have also drawn many investigations and discussion, while a few research focuses on the use of gabapentinoids. This concise narrative review will discuss pharmacological options for pain management in RMDs based on the latest evidence, with an emphasis on efficacy, potential adverse effects and safety concerns. Five main drug classes are included in this review and introduced in the following order: paracetamol, NSAIDs, opioids, antidepressants and gabapentinoids.
Paracetamol is widely recommended for pain management, including by the World Health Organisation (WHO, 2019; Freo et al., 2021). Conditional recommendations of paracetamol are made by different organisations for pain conditions, including axial spondyloarthritis (AxSpA), low back pain (LBP), OA, musculoskeletal pain, headache, and cancer pain (Freo et al., 2021). For example, according to the NICE guideline, paracetamol is not recommended alone but is recommended in association with weak opioids for LBP (National Institute for Health and Clinical Excellence, 2016) (Table 1). For OA, both the American College of Rheumatology (ACR) and NICE recommend paracetamol to patients if NSAIDs and/or other pharmacological treatments fail (Kolasinski et al., 2019; National Institute for Health and Care Excellence, 2022a). Osteoarthritis Research Society International (OARSI), by contrast, does not recommend paracetamol in OA, given little to no efficacy with possible hepatotoxicity (Bannuru et al., 2019). Two geriatric societies—the American Geriatric Society (AGS) (American Geriatrics Society Panel on Pharmacological Management of Persistent Pain in Older Persons, 2009) and British Geriatric Society (BGS) (Abdulla et al., 2013)—recommend paracetamol for musculoskeletal pain in general among older adults (i.e., over 65 years). The two guidelines however have not been updated recently as they were released in 2009 and 2013 respectively.
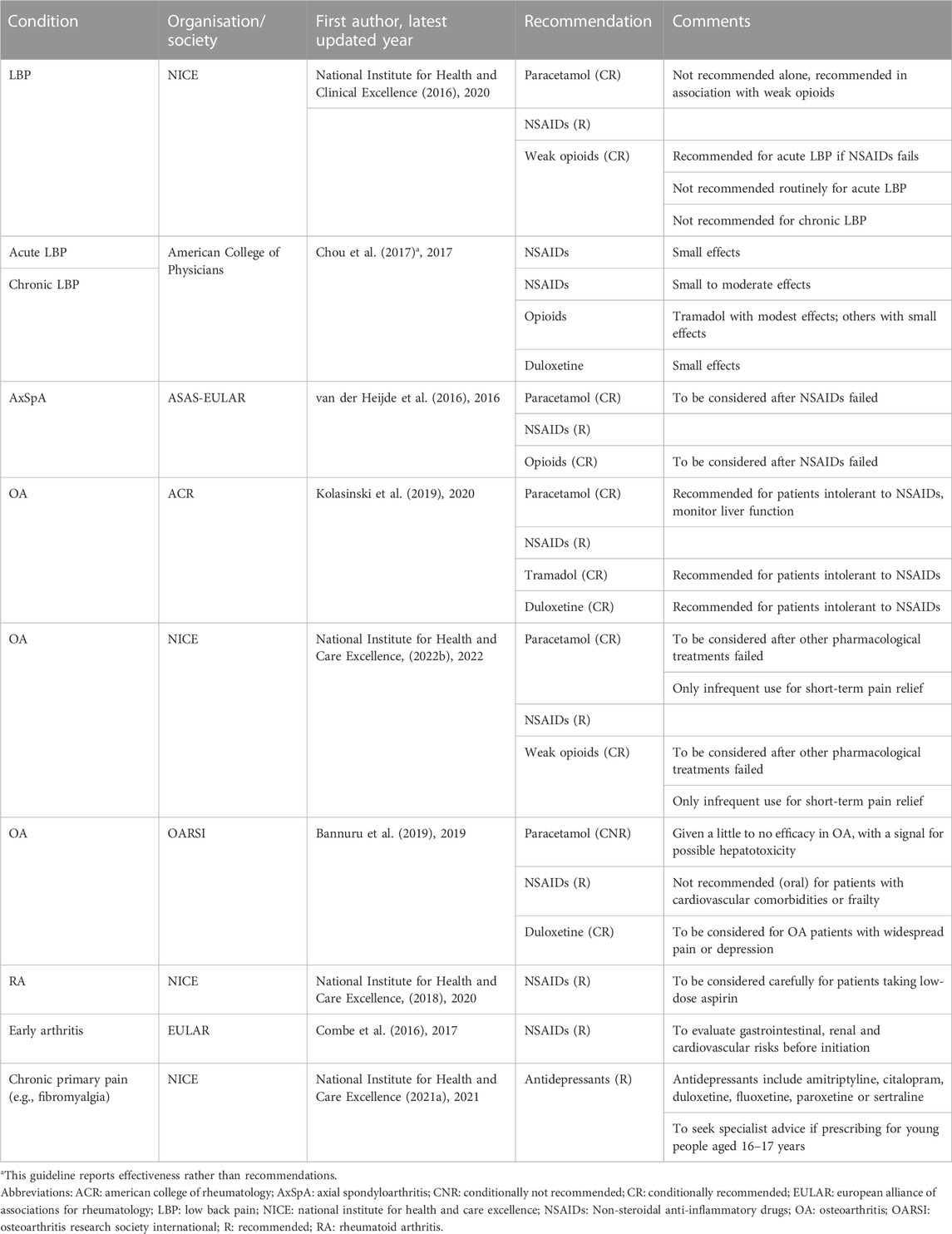
Table 1. Guidelines on the use of analgesics for RMDs published or updated in the past 5 years.
There has been questionable effectiveness about the long-term use of paracetamol (Freo et al., 2021), with limited evidence supporting the efficacy of long-term use of paracetamol in RMDs (Abdel Shaheed et al., 2021). A systematic review showed paracetamol (4 g/day for 3–12 weeks) provided modest pain relief by 3.23 points on a 0–100-point pain scale (95% CI = −5.43, −1.02) for people with knee or hip OA (Leopoldino et al., 2019). The rest of the RMDs, by contrast, lack high-quality evidence on efficacy, in which chronic LBP, RA, non-cancer pain in children and adolescents, and neuropathic pain are supported by very low-quality evidence. More importantly, the evidence from a previous Cochrane review concluded that paracetamol (up to 4 g/day for up to 12 weeks) was not effective in reducing acute LBP (Saragiotto et al., 2016). In light of a short follow-up ranging from a few hours to 2 weeks after administration, most systematic reviews assessed the immediate treatment effect, making the effectiveness of paracetamol for chronic pain management in RMDs difficult to thoroughly evaluate.
Whilst generally deemed fairly safe there has been emerging evidence of specific adverse effects in chronic use (McCrae et al., 2018). Regular long-term use at higher doses has been associated with an increased risk of gastrointestinal (GI) bleeding and a small increase in systolic blood pressure (BP) (2–4 mmHg) (Table 2). Regular use of daily doses of ≥2–3 g paracetamol was associated with a potentially increased risk of upper GI bleeding, with most being observational studies in participants aged 40 or older or in those with a history of ischemic stroke (García Rodríguez and Hernández-Díaz, 2001; González-Pérez and Rodríguez, 2006; Rahme et al., 2008; Doherty et al., 2011; Gonzalez-Valcarcel et al., 2016). An randomised controlled trial (RCT) also supported a decrease in haemoglobin (≥1 g/dl) at 13 weeks observed in 20.3% of participants on the treatment of paracetamol 3 g/day (Doherty et al., 2011). This effect was additive when combined with NSAIDs.

Table 2. Safety concerns about the use of analgesics.
BP increase has been another emerging concern with paracetamol (Turtle et al., 2013). The earliest study published in 1984 found an average of 4 mmHg increase in systolic BP when 3 g of paracetamol daily was administered for 4 weeks among patients with hypertension or OA (Chalmers et al., 1984). Subsequent RCTs had small sample sizes and showed inconsistent results, of which some supported an increase in BP (Radack et al., 1987; Sudano et al., 2010) but some against (Lewis et al., 1986). Similarly, most of the observational studies suggested that paracetamol in long-term use increased the risk of developing hypertension (Curhan et al., 2002; Dedier et al., 2002; Forman et al., 2007), with some conflicting evidence (Kurth et al., 2005; Dawson et al., 2013). Whilst several observational studies showed an association, the pain was often not measured and adjusted accordingly. An important confounding—uncontrolled pain could lead to high BP—of observational studies, however, would underestimate the association between paracetamol use and the change in BP, given the baseline BP might be higher. This could possibly explain the non-significant finding of the change in systolic BP in a cohort study (Dawson et al., 2013). The most recent NICE guideline defines hypertension as 140/90 mmHg and above, with a 10% or greater risk of developing cardiovascular disease (CVD) within the next 10 years (The Lancet, 2019; National Institute for Health and Care Excellence, 2019). A small increase in BP may be clinically important, especially for those with an increased baseline CVD risk. However, studies to date do not demonstrate these modest increase in BP has led to an increase in clinical endpoints such as stroke or myocardial infarctions (Table 2).
NSAIDs have been approved to be prescribed for a variety of conditions, including OA, RA, AxSpA, migraine, and mild to moderate acute/chronic pain, within different guidelines (Combe et al., 2016; National Institute for Health and Clinical Excellence, 2016; van der Heijde et al., 2016; National Institute for Health and Care Excellence, 2018; Bannuru et al., 2019; Kolasinski et al., 2019; Mei et al., 2020; National Institute for Health and Care Excellence, 2022b). The efficacy of NSAID treatments is indisputable, this review therefore will not put too much emphasis on it. Chronic NSAID use is defined as taking NSAIDs more than three times a week for more than 3 months. NSAIDs in chronic use have notably been reported for more than 29 million American adults (Zhou et al., 2014). The selection of an appropriate NSAID depends on patients’ profile, potential adverse effects, pharmacokinetic/pharmacodynamic properties, cost, and availability. The long-term use of NSAIDs has been associated with CV, GI, renal, skeletal muscle (e.g., interfere with muscle repair and fracture healing) and liver risks (Marcum and Hanlon, 2010; Sostres and Lanas, 2016; Mei et al., 2020). In recent years, there has been new evidence on the safety between COX2-selective and non-selective NSAIDs for chronic pain management, with a focus on GI and CV risks (Ho et al., 2018), which will be discussed in the next section.
The PRECISION study (Nissen et al., 2016) was the first study using NSAIDs in high-CV-risk patients with OA or RA to assess the CV risk of COX2-selective (i.e., celecoxib 200 mg/day) and non-selective NSAIDs (i.e., ibuprofen 1,800 mg/day or naproxen 750 mg/day) (Table 2). Similar CV-event rates were observed between celecoxib vs. naproxen and ibuprofen (hazard ratio (HR) for celecoxib vs. naproxen: 0.90, 95% CI = 0.71, 1.15; HR for celecoxib vs. ibuprofen: 0.81, 95% CI = 0.65, 1.02), but GI tolerability was better for celecoxib (serious GI events: HR for celecoxib vs. naproxen: 0.71, 95% CI = 0.54, 0.93; HR for celecoxib vs. ibuprofen: 0.65, 95% CI = 0.50, 0.85) (Nissen et al., 2016). The risk of renal events was significantly lower with celecoxib than with ibuprofen but not with naproxen. The MEDAL program (Combe et al., 2009) that evaluated long-term use of COX2-selective NSAIDs also reported no difference in risk of thrombotic CV events in arthritis patients on long-term therapy with etoricoxib (90 mg/day) compared to diclofenac (150 mg/day). Despite the reassuring results, an increase in BP was noticed in both groups, and the rate of discontinuation due to hypertension was higher in the etoricoxib group (Combe et al., 2009). The CONCERN study (Chan et al., 2017) assessed the risk of GI events between COX2-selective (i.e., celecoxib 200 mg/day) and non-selective NSAIDs (i.e., naproxen 1,000 mg/day), both in combination with a prophylactic proton pump inhibitor. This trial included arthritis patients who had cardiothrombotic diseases requiring low-dose aspirin and a history of upper-GI-tract bleeding and followed up recurrent upper-GI-tract bleeding for 18 months. Celecoxib was found to be associated with fewer adverse GI-tract events than naproxen (HR = 0.44, 95% CI = 0.23, 0.82).
Over the last two decades, an increase in CVD risk has been the major concern with NSAIDs especially following two COX2-selective NSAIDs, rofecoxib and valdecoxib, were withdrawn from the market in 2004 and 2005 and deemed unsafe (U.S. Food and Drug Administration, 2018). Additionally in 2013, following a Europe-wide review of CVD safety, diclofenac was issued safety warnings and contraindicated in patients with established ischaemic heart disease, peripheral arterial disease, cerebrovascular disease and congestive heart failure (Medicines and Healthcare products Regulatory Agency, 2014; Coxib and traditional NSAID Trialists' (CNT) Collaboration Emberson et al., 2013; Schmidt et al., 2018). Regarding the newer COX2-selective NSAIDs, reassuringly a meta-analysis (Bally et al., 2017) showed no significant difference in the rate of acute myocardial infarction between celecoxib and non-selective NSAIDs, and celecoxib was the only COX2-selective NSAID with a lower risk of adverse CV and GI events compared with non-selective NSAIDs. The risk was greatest during the first month of NSAID use and with higher doses. Summarising the latest evidence it indicates that long-term use of celecoxib 200 mg/day may be considered for patients at increased CV risk, given the comparable risk of CV events and favourable profile of GI adverse events compared to non-selective NSAIDs (Bally et al., 2017). The 2007 scientific statement from the American Heart Association, however, advised that COX2 inhibitors should be used at the lowest possible dose and for the shortest possible time to minimise the risk of CV events until more long-term data on CV safety is available (Antman et al., 2007). In patients where vascular risks are a concern, the safest option appears to be naproxen when compared to other NSAIDs (Coxib and traditional NSAID Trialists' (CNT) Collaboration Emberson et al., 2013), emphasising the need to personalise the approach to prescribing all analgesics based on an individual’s baseline risk.
Opioid prescribing is increasing for chronic non-cancer pain (CNCP) in high-income countries over the last few decades (Jani et al., 2020; Jani et al., 2021). Whilst use in acute pain has been well established, chronic/long-term use has been subject to considerable controversy in recent years due to its downstream adverse outcomes (Kalso et al., 2004).
Recent evidence from a meta-analysis suggests that opioid use was associated with statistically significant but small clinical improvements in pain and physical functioning/disability among people with CNCP, accompanied by a higher risk of adverse effects (Busse et al., 2018). Opioid use was associated with reduced pain [weighted mean difference (WMD) = −0.69 cm (95% CI = −0.82, −0.56) on a 10-cm visual analogue scale] and improved physical functioning [WMD = 2.04 points (95% CI = 1.41, 2.68) on the 100-point 36-item short form physical component score] compared to the placebo (Busse et al., 2018). Compared with non-opioid alternatives including NSAIDs, tricyclic antidepressants (TCAs), or anticonvulsants, opioids showed similar associations with improvements in pain and physical functioning, with low-to moderate-quality evidence only (Busse et al., 2018). Another meta-analysis focusing on chronic LBP reported the short-term (4–15 weeks) use of strong opioids might have clinically relevant reductions in pain compared to placebo (Nury et al., 2022). However even short-term use was associated with increases in GI and nervous system adverse events.
Despite frequent long-term opioid use for CNCP management in RMDs, there has been no scientific evidence to support its efficacy but with increasing evidence of adverse events in this population (Anastasiou and Yazdany, 2022). To date, there is limited evidence on the efficacy and safety of opioid use in RA and SLE, with scarce data in other RMDs (Anastasiou and Yazdany, 2022). Research on RA cohorts supported weak opioids in short-term (<6 weeks) use for pain control, with a relative risk (RR) = 1.40 (95% CI = 1.07, 1.85) that favours opioids over placebo (Whittle et al., 2013). Opioids were also superior to placebo in RA patient-reported global impression of change, with an absolute risk difference of 18% (95% CI = 1, 41), a relative percent change of 44% (95% CI = 3, 103), and numbers needed to treat (NNT) as 6 (95% CI = 3, 84) (Whittle et al., 2011). In OA, an RCT examining chronic opioid therapy for moderate to severe chronic back pain or hip or knee OA found no significant difference in pain-related function over 12 months (Krebs et al., 2018). The pain intensity was however significantly better in the non-opioid analgesic group which also had fewer adverse medication-related symptoms (Krebs et al., 2018). For inflammatory RMDs that require biologic disease-modifying antirheumatic drugs (DMARDs) treatments, early opioids may improve pain in the short term, resulting in delayed DMARD initiation or reduced DMARD use (Boytsov et al., 2019; Kimsey et al., 2019).
Opioid use was related to increased vomiting (RR = 2.50, 95% CI = 1.89, 3.30) among people with CNCP (Busse et al., 2018). Opioid treatments also showed 3 times higher odds of adverse events (OR = 2.94, 95% CI = 2.33, 3.72) and 4 times higher odds of treatment discontinuation due to adverse events (OR = 4.04, 95%CI = 3.10, 5.25) among older adults with musculoskeletal pain (Megale et al., 2018).
There has been limited RMD-specific research on opioid safety for pain management, in which RA and OA are the most commonly studied. For RA patients, opioids in short-term use were more likely to report adverse events such as nausea, vomiting, dizziness and constipation (OR = 3.90, 95% CI = 2.31, 6.56) (Whittle et al., 2011), but the risk of withdrawals due to adverse events was inconsistent between studies (Whittle et al., 2011; Whittle et al., 2013). Opioid use was also associated with an increased risk of fracture in the RA cohort, with a greater risk observed in strong opiates (HR = 1.53, 95% CI = 1.24, 1.88) than in weak opiates (HR = 1.37, 95% CI = 1.18, 1.59) (Ozen et al., 2019). Moreover, both RA and systemic lupus erythematosus (SLE) patients had a higher risk of hospital admissions due to opioid overdose compared to other hospitalisations (Anastasiou et al., 2019). Regarding OA, several RCTs have shown that patients receiving opioid treatments experience more adverse events and have higher proportions of dropout due to adverse events than those on placebo or non-opioids (Etropolski et al., 2014; Serrie et al., 2017; Krebs et al., 2018; Kawai et al., 2022). In the 12th month, patients on opioids had a significant increase in medication-related symptoms by 0.9 (95% CI = 0.3, 1.5) compared to those on non-opioid treatments (Krebs et al., 2018). Previous work also suggested that tapentadol PR seemingly had a better GI tolerability profile (GI adverse event = 47.3%) than oxycodone CR (GI adverse event = 65.4%) (Etropolski et al., 2014; Serrie et al., 2017) (Table 2).
To date, there are only a few studies investigating long-term opioid therapy for more than 6 months, with no study following up more than 1 year (Chou et al., 2015; Krebs et al., 2018; Nury et al., 2022). Long-term opioid therapy (defined in this study as ≥6 months) for CNCP appears not to be superior to non-opioids in improvements of pain, disability, or pain-related function but shows more adverse events, including treatment discontinuation, opioid abuse or dependence and all-cause mortality (Krebs et al., 2018; Nury et al., 2022). In addition, there is no study evaluating the long-term effectiveness of different opioid dosing strategies such as short- plus long-acting opioids vs. long-acting opioids alone (Chou et al., 2015). In light of a lack of evidence demonstrating consistently improved pain control with long-term opioid use in RMDs but with increased risks of adverse events, the current evidence strongly suggests that opioids do not have a routine role in the CNCP management of inflammatory rheumatic diseases (Anastasiou and Yazdany, 2022).
Antidepressants for the treatment of LBP (Ferraro et al., 2021) and OA (Ferreira et al., 2021) have been found associated with small reductions in pain intensity or disability scores but the effect on pain might not be clinically important. In the meta-analysis assessing LBP (Ferraro et al., 2021), antidepressants showed a reduction of 4.33 points (95% CI = −6.15, −2.50, on a 0–100 scale) in pain intensity but had increased odds of stopping treatment for any reason (OR = 1.27, 95% CI = 1.03, 1.56) or due to adverse effects (OR = 2.39, 95% CI = 1.71, 3.34). In the meta-analysis evaluating back pain and OA (Ferreira et al., 2021), serotonin and norepinephrine reuptake inhibitors (SNRIs) reduced back pain by 5.30 points (95% CI = −7.31, −3.30, on a 0–100 scale, moderate evidence level) and OA pain by 9.72 points (95% CI = −12.75, −6.69, low evidence level) at 3–13 weeks. SNRIs were also found to decrease disability from back pain at 3–13 weeks (−3.55, 95% CI = −5.22, −1.88) and disability due to OA at 2 weeks or less (−5.10, 95% CI = −7.31, −2.89), with moderate evidence level respectively (Ferreira et al., 2021). Despite the efficacy, SNRIs were related to a high risk of adverse effects (RR = 1.23, 95% CI = 1.16, 1.30). Adverse events in this meta-analysis referred to various symptoms such as nausea (most prevalent), somnolence, back pain, diarrhoea, dizziness, transient ischaemic attack, and myocardial infarction, because they were defined by each study and varied noticeably across trials (Skljarevski et al., 1976; Skljarevski et al., 2009; Ferreira et al., 2021). TCAs and other antidepressants, by contrast, did not reduce pain or disability from back pain and had no available information about the treatment of OA.
The current evidence on the efficacy of antidepressants for musculoskeletal pain appears conflicting, leading to the discrepancy in guideline recommendations. NICE does not recommend the use of antidepressants for LBP (National Institute for Health and Clinical Excellence, 2016), while the American College of Physicians guidance suggests considering duloxetine as a second-line drug treatment for chronic LBP (Chou et al., 2017). Similarly, NICE does not make a specific recommendation on antidepressants for OA (National Institute for Health and Care Excellence, 2022b) but OARSI guidance makes a conditional recommendation on duloxetine for people with OA and widespread pain or depression (Bannuru et al., 2019). Despite the small effects at the group level reported in the present evidence, some treated individuals may gain a worthwhile benefit from antidepressants. For example, absolute effect sizes for physical treatments for LBP are of similar magnitudes to those reported in the previous review (Ferreira et al., 2021) and translate into NNT of between 5 and 9 (Froud et al., 2009; Underwood and Tysall, 2021).
Antidepressants such as amitriptyline, citalopram, duloxetine, fluoxetine, paroxetine or sertraline are suggested by NICE guidelines to manage chronic primary pain (e.g., fibromyalgia) for adults (National Institute for Health and Care Excellence, 2021a). Most antidepressants are off-label use since, to date, only three pharmacological agents—pregabalin (i.e., gabapentinoids), duloxetine and milnacipran—approved by the United States Food and Drug Administration to treat fibromyalgia. A meta-analysis evaluated the efficacy and harms of antidepressants in the management of fibromyalgia syndromes (Hauser et al., 2012). The standardised mean differences of SNRIs, selective serotonin reuptake inhibitors (SSRIs), and TCAs on pain, sleep, fatigue, depression and health-related quality of life were all significant, despite only a small effect size reported. The NNT was estimated as 10.0 (95% CI = 8.0, 13.4) for SNRIs, 6.3 (95% CI = 4.1, 14.1) for SSRIs, and 4.9 (95% CI = 3.5, 8.0) for TCAs (Hauser et al., 2012). The RR of dropouts due to adverse events was higher for SNRIs (1.83, 95% CI = 1.53, 2.18) but was not statistically different for SSRIs and TCAs (Hauser et al., 2012). Although antidepressants are increasingly prescribed for fibromyalgia as per guideline recommendations, physicians and patients should be realistic about the balance between the benefits and harms of antidepressants.
The inconsistent recommendations of antidepressants across different guidelines are challenging, given the limited evidence on antidepressants’ efficacy for different RMDs. The current evidence indicates that for non-fibromyalgia RMDs, antidepressants have no important benefit that is less acceptable, less safe, and less tolerable (Ferraro et al., 2021).
There is well-established evidence supporting the use of gabapentin in people with postherpetic neuralgia and peripheral diabetic neuropathy for pain relief (Moore et al., 2014; Wiffen et al., 2017). Around 3-4 out of 10 participants achieved at least 50% pain intensity reduction with gabapentin, compared with 1-2 out of 10 for placebo (Wiffen et al., 2017). Evidence for chronic non-neuropathic pain conditions, however, is very limited, making it difficult to discuss the efficacy and safety of gabapentinoids thoroughly in this review. The previous RCT showed that gabapentin was not superior to placebo in the reduction in pain intensity and disability scores for chronic LBP (Atkinson et al., 2016). Despite the unclear efficacy of gabapentinoids in most pain conditions, its’ prescribing rate has increased drastically between 2006–2016 in Scotland, with a 4-fold increase for gabapentin and 16-fold for pregabalin (Torrance et al., 2020). The increasing prescribing is in line with the findings of gabapentinoids being increasingly abused or misused to self-medicate, in which opioid use disorder is the greatest risk factor (Evoy et al., 2021). Emerging evidence therefore reports the harms of gabapentinoids in terms of hospital utilisation and mortality risk (Evoy et al., 2021). People prescribed gabapentinoids had doubled the age-standardised death rate than that in the Scottish population (RR = 2.16, 95% CI = 2.08, 2.25) (Torrance et al., 2020). The increase in gabapentinoid prescribing, along with frequent co-prescriptions of opioids and/or benzodiazepines, also contributed to a higher rate of drug-related deaths (Torrance et al., 2020).
Gabapentinoids appear not to be recommended for RMDs by various guidelines given their unclear efficacy but do reveal an increasing prescribing rate and associations with poor health outcomes. The early evidence indicates some concerns regarding the appropriateness of gabapentinoids for chronic non-neuropathic pain management.
This narrative review incorporates heterogeneous study designs for RMDs with detailed interpretation and discussion, aiming to provide up-to-date and well-evidenced-based information to healthcare professionals on a topic with little evidence. Limitations of this work should also be acknowledged: 1) data unavailability due to no full-text, or a format of published abstract 2) incomparability of studies because of heterogeneous dose regimens, comparators, or outcomes.
In this review, we have discussed some of the challenges in interpreting the evidence and following current guidelines, which inevitably lead to variation in clinical practice when prescribing analgesics to patients with RMDs. The heterogeneity in the quality of clinical trials to assess the analgesic efficacy and a lack of key metrics such as NNT and number needed to harm, make the interpretability of evidence difficult. This subsequently makes communications with patients about the benefit/harm balance and shared decision-making more challenging. Whilst population-level estimates can help identify subgroups of patients at high risk of specific adverse outcomes, prescribing often requires a personalised approach that incorporates the baseline risk of the patient as well as patient preference. Long-term use of opioids, antidepressants and gabapentinoids prescribed frequently in RMDs is importantly associated with dependence, often with minimal clinical benefits in symptoms or function. Recognising these challenges, NICE has released helpful resources to consider when prescribing dependence-forming medicines or antidepressants (National Institute for Health and Care Excellence, 2022a) as well as on shared decision-making with patients (National Institute for Health and Care Excellence, 2021b). Resources for effective non-pharmacological options for pain, alongside quantitative safety estimates that can be easily communicated with patients, would allow more informed choices and better treatment stratification than is currently possible.
Y-TH and MJ conceived the study. MJ secured funding. Y-TH led the literature review with the support of CM’s Master’s Dissertation. Y-TH drafted the initial version of the manuscript. Y-TH and MJ critically reviewed the manuscript and contributed to revisions. All authors have read and approved the final manuscript.
MJ is funded by a National Institute for Health and Care Research (NIHR) Advanced Fellowship (NIHR301413). The views expressed in this publication are those of the authors and not necessarily those of the NIHR, NHS or the United Kingdom Department of Health and Social Care. This work is supported also by a FOREUM Career Research Grant (reference 125059) and Versus Arthritis (reference 22481).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abdel Shaheed, C., Ferreira, G. E., Dmitritchenko, A., McLachlan, A. J., Day, R. O., Saragiotto, B., et al. (2021). The efficacy and safety of paracetamol for pain relief: An overview of systematic reviews. Med. J. Aust. 214 (7), 324–331. doi:10.5694/mja2.50992
Abdulla, A., Adams, N., Bone, M., Elliott, A. M., Gaffin, J., Jones, D., et al. (2013). Guidance on the management of pain in older people. Age Ageing 42 (1), i1–i57. doi:10.1093/ageing/afs200
American Geriatrics Society Panel on Pharmacological Management of Persistent Pain in Older Persons (2009). Pharmacological management of persistent pain in older persons. J. Am. Geriatrics Soc. 57 (8), 1331–1346. doi:10.1111/j.1532-5415.2009.02376.x
Anastasiou, C., Li, J., Trupin, L., Schmajuk, G., and Yazdany, J. (2019). Opioid overdose hospitalizations in patients with systemic lupus erythematosus and rheumatoid arthritis. Arthritis Rheumatol. 71 (10), 670–677.
Anastasiou, C., and Yazdany, J. (2022). Review of publications evaluating opioid use in patients with inflammatory rheumatic disease. Curr. Opin. Rheumatol. 34 (2), 95–102. doi:10.1097/BOR.0000000000000868
Antman, E. M., Bennett, J. S., Daugherty, A., Furberg, C., Roberts, H., Taubert, K. A., et al. (2007). Use of nonsteroidal antiinflammatory drugs: An update for clinicians: A scientific statement from the American heart association. Circulation 115 (12), 1634–1642. doi:10.1161/CIRCULATIONAHA.106.181424
Atkinson, J. H., Slater, M. A., Capparelli, E. V., Patel, S. M., Wolfson, T., Gamst, A., et al. (2016). A randomized controlled trial of gabapentin for chronic low back pain with and without a radiating component. Pain 157 (7), 1499–1507. doi:10.1097/j.pain.0000000000000554
Bally, M., Dendukuri, N., Rich, B., Nadeau, L., Helin-Salmivaara, A., Garbe, E., et al. (2017). Risk of acute myocardial infarction with NSAIDs in real world use: Bayesian meta-analysis of individual patient data. Bmj 357, j1909. doi:10.1136/bmj.j1909
Bannuru, R. R., Osani, M. C., Vaysbrot, E. E., Arden, N. K., Bennell, K., Bierma-Zeinstra, S. M. A., et al. (2019). OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 27 (11), 1578–1589. doi:10.1016/j.joca.2019.06.011
Boytsov, N. N., Bhattacharya, R., Saverno, K., Dixon, L., Abbott, P. L., Zhang, X., et al. (2019). Health care effect of disease-modifying antirheumatic drug use on patients with rheumatoid arthritis. J. Manag. Care Spec. Pharm. 25 (8), 879–887. doi:10.18553/jmcp.2019.25.8.879
Busse, J. W., Wang, L., Kamaleldin, M., Craigie, S., Riva, J. J., Montoya, L., et al. (2018). Opioids for chronic noncancer pain: A systematic review and meta-analysis. JAMA 320 (23), 2448–2460. doi:10.1001/jama.2018.18472
Chalmers, J. P., West, M. J., Wing, L. M., Bune, A. J., and Graham, J. R. (1984). Effects of indomethacin, sulindac, naproxen, aspirin, and paracetamol in treated hypertensive patients. Clin. Exp. Hypertens. A 6 (6), 1077–1093. doi:10.3109/10641968409039582
Chan, F. K. L., Ching, J. Y. L., Tse, Y. K., Lam, K., Wong, G. L. H., Ng, S. C., et al. (2017). Gastrointestinal safety of celecoxib versus naproxen in patients with cardiothrombotic diseases and arthritis after upper gastrointestinal bleeding (CONCERN): An industry-independent, double-blind, double-dummy, randomised trial. Lancet 389 (10087), 2375–2382. doi:10.1016/S0140-6736(17)30981-9
Chou, R., Deyo, R., Friedly, J., Skelly, A., Weimer, M., Fu, R., et al. (2017). Systemic pharmacologic therapies for low back pain: A systematic review for an American College of physicians clinical practice guideline. Ann. Intern Med. 166 (7), 480–492. doi:10.7326/M16-2458
Chou, R., Turner, J. A., Devine, E. B., Hansen, R. N., Sullivan, S. D., Blazina, I., et al. (2015). The effectiveness and risks of long-term opioid therapy for chronic pain: A systematic review for a national institutes of health pathways to prevention workshop. Ann. Intern. Med. 162 (4), 276–286. doi:10.7326/M14-2559
Combe, B., Landewe, R., Daien, C. I., Hua, C., Aletaha, D., Álvaro-Gracia, J. M., et al. (2016). 2016 update of the EULAR recommendations for the management of early arthritis. Ann. Rheum. Dis. 76 (6), 948–959. doi:10.1136/annrheumdis-2016-210602
Combe, B., Swergold, G., McLay, J., McCarthy, T., Zerbini, C., Emery, P., et al. (2009). Cardiovascular safety and gastrointestinal tolerability of etoricoxib vs diclofenac in a randomized controlled clinical trial (The MEDAL study). Rheumatol. Oxf. 48 (4), 425–432. doi:10.1093/rheumatology/kep005
Curhan, G. C., Willett, W. C., Rosner, B., and Stampfer, M. J. (2002). Frequency of analgesic use and risk of hypertension in younger women. Arch. Intern Med. 162 (19), 2204–2208. doi:10.1001/archinte.162.19.2204
Dawson, J., Fulton, R., McInnes, G. T., Morton, R., Morrison, D., Padmanabhan, S., et al. (2013). Acetaminophen use and change in blood pressure in a hypertensive population. J. Hypertens. 31 (7), 1485–1490. doi:10.1097/HJH.0b013e328360f6f8
Dedier, J., Stampfer, M. J., Hankinson, S. E., Willett, W. C., Speizer, F. E., and Curhan, G. C. (2002). Nonnarcotic analgesic use and the risk of hypertension in US women. Hypertension 40 (5), 604–608. doi:10.1161/01.hyp.0000035856.77718
Doherty, M., Hawkey, C., Goulder, M., Gibb, I., Hill, N., Aspley, S., et al. (2011). A randomised controlled trial of ibuprofen, paracetamol or a combination tablet of ibuprofen/paracetamol in community-derived people with knee pain. Ann. Rheum. Dis. 70 (9), 1534–1541. doi:10.1136/ard.2011.154047
Coxib and traditional NSAID Trialists' (CNT) Collaboration Emberson, J., Merhi, A., Abramson, S., Arber, N., and Hawk, A. (2013). Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: meta-analyses of individual participant data from randomised trials. Lancet 382 (9894), 769–779. doi:10.1016/S0140-6736(13)60900-9
Etropolski, M., Kuperwasser, B., Flügel, M., Häufel, T., Lange, B., Rauschkolb, C., et al. (2014). Safety and tolerability of tapentadol extended release in moderate to severe chronic osteoarthritis or low back pain management: Pooled analysis of randomized controlled trials. Adv. Ther. 31 (6), 604–620. doi:10.1007/s12325-014-0128-6
Evoy, K. E., Sadrameli, S., Contreras, J., Covvey, J. R., Peckham, A. M., and Morrison, M. D. (2021). Abuse and misuse of pregabalin and gabapentin: A systematic review update. Drugs 81 (1), 125–156. doi:10.1007/s40265-020-01432-7
Ferraro, M. C., Bagg, M. K., Wewege, M. A., Cashin, A. G., Leake, H. B., Rizzo, R. R. N., et al. (2021). Efficacy, acceptability, and safety of antidepressants for low back pain: A systematic review and meta-analysis. Syst. Rev. 10 (1), 62. doi:10.1186/s13643-021-01599-4
Ferreira, G. E., McLachlan, A. J., Lin, C-W. C., Zadro, J. R., Abdel-Shaheed, C., O’Keeffe, M., et al. (2021). Efficacy and safety of antidepressants for the treatment of back pain and osteoarthritis: Systematic review and meta-analysis. Bmj 372, m4825. doi:10.1136/bmj.m4825
Forman, J. P., Rimm, E. B., and Curhan, G. C. (2007). Frequency of analgesic use and risk of hypertension among men. Arch. Intern Med. 167 (4), 394–399. doi:10.1001/archinte.167.4.394
Freo, U., Ruocco, C., Valerio, A., Scagnol, I., and Nisoli, E. (2021). Paracetamol: A review of guideline recommendations. J. Clin. Med. 10 (15), 3420. doi:10.3390/jcm10153420
Froud, R., Eldridge, S., Lall, R., and Underwood, M. (2009). Estimating the number needed to treat from continuous outcomes in randomised controlled trials: Methodological challenges and worked example using data from the UK back pain exercise and manipulation (BEAM) trial. BMC Med. Res. Methodol. 9 (1), 35. doi:10.1186/1471-2288-9-35
García Rodríguez, L. A., and Hernández-Díaz, S. (2001). Relative risk of upper gastrointestinal complications among users of acetaminophen and nonsteroidal anti-inflammatory drugs. Epidemiology 12 (5), 570–576. doi:10.1097/00001648-200109000-00018
González-Pérez, A., and Rodríguez, L. A. (2006). Upper gastrointestinal complications among users of paracetamol. Basic Clin. Pharmacol. Toxicol. 98 (3), 297–303. doi:10.1111/j.1742-7843.2006.pto_248.x
Gonzalez-Valcarcel, J., Sissani, L., Labreuche, J., Bousser, M. G., Chamorro, A., Fisher, M., et al. (2016). Paracetamol, ibuprofen, and recurrent major cardiovascular and major bleeding events in 19 120 patients with recent ischemic stroke. Stroke 47 (4), 1045–1052. doi:10.1161/STROKEAHA.115.012091
Hauser, W., Wolfe, F., Tolle, T., Uceyler, N., and Sommer, C. (2012). The role of antidepressants in the management of fibromyalgia syndrome: A systematic review and meta-analysis. CNS Drugs 26 (4), 297–307. doi:10.2165/11598970-000000000-00000
Ho, K. Y., Gwee, K. A., Cheng, Y. K., Yoon, K. H., Hee, H. T., and Omar, A. R. (2018). Nonsteroidal anti-inflammatory drugs in chronic pain: Implications of new data for clinical practice. J. Pain Res. 11, 1937–1948. doi:10.2147/JPR.S168188
Ivanova, J. I., Birnbaum, H. G., Schiller, M., Kantor, E., Johnstone, B. M., and Swindle, R. W. (2011). Real-world practice patterns, health-care utilization, and costs in patients with low back pain: The long road to guideline-concordant care. Spine J. 11 (7), 622–632. doi:10.1016/j.spinee.2011.03.017
Jani, M., Birlie Yimer, B., Sheppard, T., Lunt, M., and Dixon, W. G. (2020). Time trends and prescribing patterns of opioid drugs in UK primary care patients with non-cancer pain: A retrospective cohort study. PLoS Med. 17 (10), e1003270. doi:10.1371/journal.pmed.1003270
Jani, M., Girard, N., Bates, D. W., Buckeridge, D. L., Sheppard, T., Li, J., et al. (2021). Opioid prescribing among new users for non-cancer pain in the USA, Canada, UK, and taiwan: A population-based cohort study. PLoS Med. 18 (11), e1003829. doi:10.1371/journal.pmed.1003829
John, A., Marchant, A. L., Fone, D. L., McGregor, J. I., Dennis, M. S., Tan, J. O., et al. (2016). Recent trends in primary-care antidepressant prescribing to children and young people: An e-cohort study. Psychol. Med. 46 (16), 3315–3327. doi:10.1017/S0033291716002099
Kalso, E., Edwards, J. E., Moore, A. R., and McQuay, H. J. (2004). Opioids in chronic non-cancer pain: Systematic review of efficacy and safety. Pain 112 (3), 372–380. doi:10.1016/j.pain.2004.09.019
Kawai, S., Sobajima, S., Jinnouchi, M., Nakano, H., Ohtani, H., Sakata, M., et al. (2022). Efficacy and safety of tramadol hydrochloride twice-daily sustained-release bilayer tablets with an immediate-release component for chronic pain associated with knee osteoarthritis: A randomized, double-blind, placebo-controlled, treatment-withdrawal study. Clin. Drug Investig. 42 (5), 403–416. doi:10.1007/s40261-022-01139-5
Kimsey, L., Weissman, J. S., Patel, A., Drew, A., Koehlmoos, T., and Sparks, J. A. (2019). Delay in initiation of DMARD or anti-inflammatory therapy in patients newly diagnosed with rheumatoid arthritis: An analysis of United States Military Health System TRICARE beneficiaries. Semin. Arthritis Rheum. 48 (5), 821–827. doi:10.1016/j.semarthrit.2018.07.003
Kolasinski, S. L., Neogi, T., Hochberg, M. C., Oatis, C., Guyatt, G., Block, J., et al. (2019). 2019 American College of rheumatology/arthritis foundation guideline for the management of osteoarthritis of the hand, hip, and knee. Arthritis rheumatol. 72 (2), 220–233. doi:10.1002/art.41142
Krebs, E. E., Gravely, A., Nugent, S., Jensen, A. C., DeRonne, B., Goldsmith, E. S., et al. (2018). Effect of opioid vs nonopioid medications on pain-related function in patients with chronic back pain or hip or knee osteoarthritis pain: The SPACE randomized clinical trial. JAMA 319 (9), 872–882. doi:10.1001/jama.2018.0899
Kuehn, B. M. (2022). Gabapentin increasingly implicated in overdose deaths. JAMA 327 (24), 2387. doi:10.1001/jama.2022.10100
Kurth, T., Hennekens, C. H., Stürmer, T., Sesso, H. D., Glynn, R. J., Buring, J. E., et al. (2005). Analgesic use and risk of subsequent hypertension in apparently healthy men. Arch. Intern Med. 165 (16), 1903–1909. doi:10.1001/archinte.165.16.1903
Leopoldino, A. O., Machado, G. C., Ferreira, P. H., Pinheiro, M. B., Day, R., McLachlan, A. J., et al. (2019). Paracetamol versus placebo for knee and hip osteoarthritis. Cochrane Database Syst. Rev. 2, CD013273. doi:10.1002/14651858.CD013273
Lewis, R. V., Toner, J. M., Jackson, P. R., and Ramsay, L. E. (1986). Effects of indomethacin and sulindac on blood pressure of hypertensive patients. Br. Med. J. Clin. Res. Ed. 292 (6525), 934–935. doi:10.1136/bmj.292.6525.934-a
Marcum, Z. A., and Hanlon, J. T. (2010). Recognizing the risks of chronic nonsteroidal anti-inflammatory drug use in older adults. Ann. Longterm Care 18 (9), 24–27.
McCrae, J. C., Morrison, E. E., MacIntyre, I. M., Dear, J. W., and Webb, D. J. (2018). Long-term adverse effects of paracetamol - a review. Br. J. Clin. Pharmacol. 84 (10), 2218–2230. doi:10.1111/bcp.13656
Medicines and Healthcare products Regulatory Agency (2014). Diclofenac: New contraindications and warnings 2014. Available from: https://www.gov.uk/drug-safety-update/diclofenac-new-contraindications-and-warnings#fn:1.
Megale, R. Z., Deveza, L. A., Blyth, F. M., Naganathan, V., Ferreira, P. H., McLachlan, A. J., et al. (2018). Efficacy and safety of oral and transdermal opioid analgesics for musculoskeletal pain in older adults: A systematic review of randomized, placebo-controlled trials. J. Pain 19 (5), e1–e475. doi:10.1016/j.jpain.2017.12.001
Mei, J., Polyakova, O., Dhaliwall, S., McDonald, K., and Wong, A. Y. (2020). Safety and efficacy considerations for chronic use of NSAIDs for chronic Pain2020. Available from: https://www.thejournalofprecisionmedicine.com/the-journal-of-precision-medicine/safety-and-efficacy-considerations-for-chronic-use-of-nsaids-for-chronic-pain/.
Moore, R. A., Wiffen, P. J., Derry, S., Toelle, T., and Rice, A. S. (2014). Gabapentin for chronic neuropathic pain and fibromyalgia in adults. Cochrane Database Syst. Rev. 2014 (4), Cd007938. doi:10.1002/14651858.CD007938.pub2
National Institute for Health and Care Excellence (2021a). Chronic pain (primary and secondary) in over 16s: Assessment of all chronic pain and management of chronic primary pain 2021. Available from: https://www.nice.org.uk/guidance/ng193.
National Institute for Health and Care Excellence (2019). Hypertension in adults: Diagnosis and management 2019. Available from: https://www.nice.org.uk/guidance/ng136.
National Institute for Health and Care Excellence (2022a). Medicines associated with dependence or withdrawal symptoms: Safe prescribing and withdrawal management for adults 2022. Available from: https://www.nice.org.uk/guidance/ng215.
National Institute for Health and Care Excellence (2022b). Osteoarthritis in over 16s: Diagnosis and management 2022. Available from: https://www.nice.org.uk/guidance/ng226/chapter/Recommendations.
National Institute for Health and Care Excellence (2018). Rheumatoid arthritis in adults: Management. Available from: https://www.nice.org.uk/guidance/ng100.
National Institute for Health and Care Excellence (2021b). Shared decision making 2021. Available from: https://www.nice.org.uk/guidance/ng197.
National Institute for Health and Clinical Excellence (2016). Low back pain and sciatica in over 16s: Assessment and management 2016. Available from: https://www.nice.org.uk/guidance/ng59.
Nissen, S. E., Yeomans, N. D., Solomon, D. H., Lüscher, T. F., Libby, P., Husni, M. E., et al. (2016). Cardiovascular safety of celecoxib, naproxen, or ibuprofen for arthritis. N. Engl. J. Med. 375 (26), 2519–2529. doi:10.1056/NEJMoa1611593
Nury, E., Schmucker, C., Nagavci, B., Motschall, E., Nitschke, K., Schulte, E., et al. (2022). Efficacy and safety of strong opioids for chronic noncancer pain and chronic low back pain: A systematic review and meta-analyses. Pain 163 (4), 610–636. doi:10.1097/j.pain.0000000000002423
Ozen, G., Pedro, S., Wolfe, F., and Michaud, K. (2019). Medications associated with fracture risk in patients with rheumatoid arthritis. Ann. Rheum. Dis. 78 (8), 1041–1047. doi:10.1136/annrheumdis-2019-215328
Radack, K. L., Deck, C. C., and Bloomfield, S. S. (1987). Ibuprofen interferes with the efficacy of antihypertensive drugs. A randomized, double-blind, placebo-controlled trial of ibuprofen compared with acetaminophen. Ann. Intern Med. 107 (5), 628–635. doi:10.7326/0003-4819-107-5-628
Rahme, E., Barkun, A., Nedjar, H., Gaugris, S., and Watson, D. (2008). Hospitalizations for upper and lower GI events associated with traditional NSAIDs and acetaminophen among the elderly in Quebec, Canada. Am. J. Gastroenterol. 103 (4), 872–882. doi:10.1111/j.1572-0241.2008.01811.x
Saragiotto, B. T., Machado, G. C., Ferreira, M. L., Pinheiro, M. B., Abdel Shaheed, C., and Maher, C. G. (2016). Paracetamol for low back pain. Cochrane Database Syst. Rev. 2016 (6), Cd012230. doi:10.1002/14651858.CD012230
Schmidt, M., Sørensen, H. T., and Pedersen, L. (2018). Diclofenac use and cardiovascular risks: Series of nationwide cohort studies. Bmj 362, k3426. doi:10.1136/bmj.k3426
Serrie, A., Lange, B., and Steup, A. (2017). Tapentadol prolonged-release for moderate-to-severe chronic osteoarthritis knee pain: A double-blind, randomized, placebo- and oxycodone controlled release-controlled study. Curr. Med. Res. Opin. 33 (8), 1423–1432. doi:10.1080/03007995.2017.1335189
Skljarevski, V., Desaiah, D., Liu-Seifert, H., Zhang, Q., Chappell, A. S., Detke, M. J., et al. (1976). Efficacy and safety of duloxetine in patients with chronic low back pain. Spine (Phila Pa 35 (13), E578–E585. doi:10.1097/BRS.0b013e3181d3cef6
Skljarevski, V., Ossanna, M., Liu-Seifert, H., Zhang, Q., Chappell, A., Iyengar, S., et al. (2009). A double-blind, randomized trial of duloxetine versus placebo in the management of chronic low back pain. Eur. J. Neurol. 16 (9), 1041–1048. doi:10.1111/j.1468-1331.2009.02648.x
Sostres, C., and Lanas, Á. (2016). Appropriate prescription, adherence and safety of non-steroidal anti-inflammatory drugs. Med. Clin. Barc. 146 (6), 267–272. doi:10.1016/j.medcli.2015.09.022
Sudano, I., Flammer, A. J., Périat, D., Enseleit, F., Hermann, M., Wolfrum, M., et al. (2010). Acetaminophen increases blood pressure in patients with coronary artery disease. Circulation 122 (18), 1789–1796. doi:10.1161/CIRCULATIONAHA.110.956490
The Lancet (2019). NICE hypertension guidelines: A pragmatic compromise. Lancet 394 (10201), 806. doi:10.1016/S0140-6736(19)32042-2
Torrance, N., Veluchamy, A., Zhou, Y., Fletcher, E. H., Moir, E., Hebert, H. L., et al. (2020). Trends in gabapentinoid prescribing, co-prescribing of opioids and benzodiazepines, and associated deaths in Scotland. Br. J. Anaesth. 125 (2), 159–167. doi:10.1016/j.bja.2020.05.017
Turtle, E. J., Dear, J. W., and Webb, D. J. (2013). A systematic review of the effect of paracetamol on blood pressure in hypertensive and non-hypertensive subjects. Br. J. Clin. Pharmacol. 75 (6), 1396–1405. doi:10.1111/bcp.12032
Underwood, M., and Tysall, C. (2021). Antidepressants for musculoskeletal pain. Bmj 372, n80. doi:10.1136/bmj.n80
U.S. Food and Drug Administration (2018). COX-2 selective (includes bextra, celebrex, and vioxx) and non-selective non-steroidal anti-inflammatory drugs (NSAIDs) 2018. Available from: https://www.fda.gov/drugs/postmarket-drug-safety-information-patients-and-providers/cox-2-selective-includes-bextra-celebrex-and-vioxx-and-non-selective-non-steroidal-anti-inflammatory.
van der Heijde, D., Ramiro, S., Landewé, R., Baraliakos, X., Van den Bosch, F., Sepriano, A., et al. (2016). 2016 update of the ASAS-EULAR management recommendations for axial spondyloarthritis. Ann. Rheum. Dis. 76 (6), 978–991. doi:10.1136/annrheumdis-2016-210770
Whittle, S. L., Richards, B. L., and Buchbinder, R. (2013). Opioid analgesics for rheumatoid arthritis pain. JAMA 309 (5), 485–486. doi:10.1001/jama.2012.193412
Whittle, S. L., Richards, B. L., Husni, E., and Buchbinder, R. (2011). Opioid therapy for treating rheumatoid arthritis pain. Cochrane Database Syst. Rev. 11, Cd003113. doi:10.1002/14651858.CD003113.pub3
WHO (20192023). World health organization model list of essential medicines, 21st list. Geneva: World Health Organization. Available from: https://apps.who.int/iris/bitstream/handle/10665/325771/WHO-MVP-EMP-IAU-2019.06-eng.pdf?ua=1.
Wiffen, P. J., Derry, S., Bell, R. F., Rice, A. S., Tolle, T. R., Phillips, T., et al. (2017). Gabapentin for chronic neuropathic pain in adults. Cochrane Database Syst. Rev. 6, CD007938. doi:10.1002/14651858.CD007938.pub4
Keywords: rheumatic and musculoskeletal diseases (RMDs), pharmacological treatment, paracetamol (acetaminophen), non-steroidal anti-inflammatory drugs (NSAIDs), opioids, antidepressants, gabapentinoids
Citation: Huang Y-T, McCarthy C and Jani M (2023) Balancing the evidence: An update on analgesic use in rheumatic and musculoskeletal diseases. Front. Drug Saf. Regul. 3:1117674. doi: 10.3389/fdsfr.2023.1117674
Received: 06 December 2022; Accepted: 31 January 2023;
Published: 16 February 2023.
Edited by:
Enrique Roberto Soriano, Italian Hospital of Buenos Aires, ArgentinaReviewed by:
Dario Scublinsky, University of Buenos Aires, ArgentinaCopyright © 2023 Huang, McCarthy and Jani. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Meghna Jani, bWVnaG5hLmphbmlAbWFuY2hlc3Rlci5hYy51aw==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.