
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Drug Saf. Regul. , 15 August 2022
Sec. Advanced Methods in Pharmacovigilance and Pharmacoepidemiology
Volume 2 - 2022 | https://doi.org/10.3389/fdsfr.2022.970661
 Lucia Gozzo1
Lucia Gozzo1 Kenneth Paterson2Olivier Wong3Francis Megerlin4Jan Geldmacher5Patrizia Popoli6Claudio Jommi7Frank-Ulrich Fricke8Oriol De Solà-Morales9Isao Kamae10Guido Rasi11
Kenneth Paterson2Olivier Wong3Francis Megerlin4Jan Geldmacher5Patrizia Popoli6Claudio Jommi7Frank-Ulrich Fricke8Oriol De Solà-Morales9Isao Kamae10Guido Rasi11 Filippo Drago1,12,13*
Filippo Drago1,12,13*Health Technology Assessment (HTA) is a multidisciplinary process which supports policy “decision-making”, including those related to drug reimbursement and price negotiation based on comprehensive clinical and non-clinical evaluations. The discrepancies in HTA recommendations among European countries are related to the differences in health care systems and willingness to invest in health care, differences in assessment methodologies and appraisal practices, and variations in economic constraints, and may produce disparities in terms of patient access to medicines. The political discussion about the adoption of the European Regulation on HTA lasted for years due to concerns about its feasibility and its implications for national health care systems In this paper we highlighted the importance to harmonize HTA process in Europe and some critical issues emerged during the discussion among experts in the field carried out at the European Regulatory Conference.
The European Medicines Agency (EMA) has produced an efficient marketing authorisation system for human medicines, ensuring appropriate control and monitoring of medicinal products and adequate protection of patients. (EMA, 2020a).
The great majority of new medicines are approved through the centralised authorisation procedure; in particular it is mandatory for specific categories of drugs (e.g. new active substance to treat HIV/AIDS, cancer, neurodegenerative diseases, viral diseases, biotechnological products, advanced-therapy medicines, orphan medicines) (EMA., 2020b). The aim of the centralised procedure is to enable rapid, EU-wide authorisation of medicinal products.
A positive opinion supporting a marketing authorization is based on a benefit/risk assessment, which requires the evaluation of quality, nonclinical and clinical data on safety and efficacy submitted by the applicant, but which excludes any economic considerations.
Despite the unification of the European procedures for drug approval, each country retains its own jurisdiction over national market access, pricing and reimbursement agreements adapted to national health needs and local budgets.
The decision about new medicine reimbursement usually needs a Health Technology Assessment (HTA) performed at the national, and, in some countries, regional and hospital levels.
HTA is a multidisciplinary process whose purpose is to systematically evaluate new healthcare interventions based on clinical (efficacy and safety), economic, ethical, and organizational aspects in support of policy decision making about reimbursement and price negotiation (Drummond et al., 2008).
General criteria usually considered in order to issue HTA recommendations include unmet medical needs, relative effectiveness and safety of the new drug compared to the current standard of care if any, budget impact and cost-effectiveness (van Nooten et al., 2012). However, this step may produce disparities among European patients in terms of access, due to the heterogeneity of national assessments (Akehurst et al., 2017; Allen et al., 2017; Angelis et al., 2018; Gozzo et al., 2020; Gozzo et al., 2021a; Gozzo et al., 2021b), thereafter reflected in reimbursement decisions and pricing agreements (e.g. coverage or not, innovative medicine designation, treatment restrictions as regard to patients’ eligibility, Managed Entry Agreements application) (Angelis et al., 2018). Even where there is a general consensus on the way decisions should be taken, there are important differences across countries. For example, the way the principles of value-based pricing for medicines have been actually applied is still very different across countries (Jommi et al., 2020).
The discrepancies relate to differences in health care systems and willingness to invest in health care, differences in assessment methodologies and appraisal practices, and variations in the economic constraints. (Richardson and Schlander, 2019).
Moreover, in recent years marketing authorization is increasingly granted by EMA at earlier stages in the life-cycle of medicines, especially for high-unmet medical need or rare diseases, through accelerated assessment or conditional marketing authorisation before complete data are available, thus potentially leading to limitations of evidence needed for subsequent HTA (Akehurst et al., 2017; EMA; Moseley et al., 2020). Indeed, the conditional marketing authorisation is granted for medicines treating unmet medical needs, in particular seriously debilitating or life-threatening diseases, even if comprehensive clinical data are not available at the initial authorisation. To maintain the authorisation, the marketing authorisation holder must fulfill specific obligations, including the collection of additional data to confirm the benefit-risk balance. Therefore, even if the benefit risk profile should be positive to obtain the conditional approval, uncertainties associated with these products remain and cannot be solved before launch. Acceleration of drug approval might therefore not always translate into positive and/or equally rapid reimbursement decisions due to residual uncertainties around net clinical benefits and the expected high impact on healthcare system, hindering patient access in some countries (Ciani and Jommi, 2014; Akehurst et al., 2017; Allen et al., 2017; Richardson and Schlander, 2019; Jommi et al., 2020).
In this context, EU-wide harmonization of regulatory and HTA procedures (i.e. shared rules regarding in general national approval processes) across countries could support the timing alignment regarding access and reimbursement.
Such a harmonization requires above all national procedures of evidence assessment to become similar and/or aligned–at least interoperable - as a result of experience sharing, and the adoption of internationally recognized (new and old) standards and/or principles, adaptable to each local legal context.
To promote cooperation between HTA bodies, two Joint Actions (EUnetHTA JA) with the voluntary participation from EU Member States have been carried out and a third one (EUnetHTA Joint Action 3) is still ongoing, all supported by the European Commission (EUNETHA, 2020) (Figure 1). In particular, the third Joint Action focuses on developing common assessment methodologies, producing joint clinical assessments and full HTA reports, and on developing and maintaining common tools.
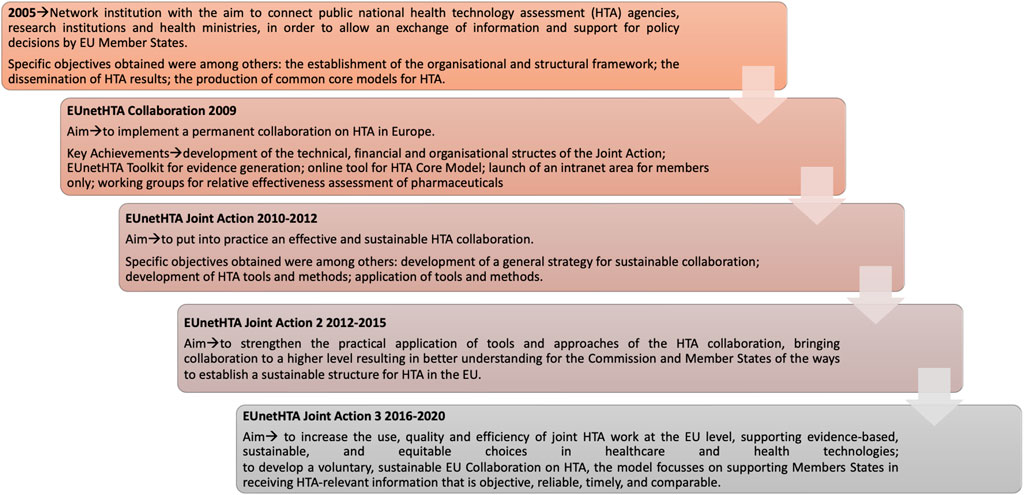
Figure 1. The institution of the EUnetHTA Project in Europe (EUnetHTA, 2008; EUnetHTA, 2013; EUnetHTA, 2018; EUNETHA, 2022).
Despite these achievements, a lot of issues have not been solved yet, and cannot be sufficiently addressed by the voluntary cooperation within a single project.
A number of stakeholders emphasised that EU cooperation beyond the EUnetHTA Joint Action 3 is needed “to ensure a constant exchange of information and knowledge between HTA institutions in Europe, to increase synergies between Member States, to streamline HTA methodologies, to increase transparency and evidence-based decision-making, as well as to ensure business predictability” (Council on health technology, 2018). A proposal for a Regulation of the European Parliament and of the Council on health technology assessment and amending Directive 2011/24/EU (Council on health technology, 2018) has been developed in 2018. Extensive consultation with stakeholders took place in the preparation of this proposal, which has been modified in 2021 (Council on health technology, 2021). The HTA Regulation [Regulation (EU) 2021/2282] entered into force in January 2022 and applies from January 2025.
The Regulation provides the basis for a permanent and sustainable cooperation on HTA at the EU level, covering four main HTA activities (Table 1):
1) joint clinical assessments;
2) joint scientific consultations whereby developers can seek advice from HTA authorities, also in parallel with European regulators;
3) horizon scanning;
4) continuing voluntary cooperation in areas not covered by joint clinical assessments in which individual EU countries will continue to be responsible (non-clinical aspects of health technologies, decisions on pricing and reimbursement).
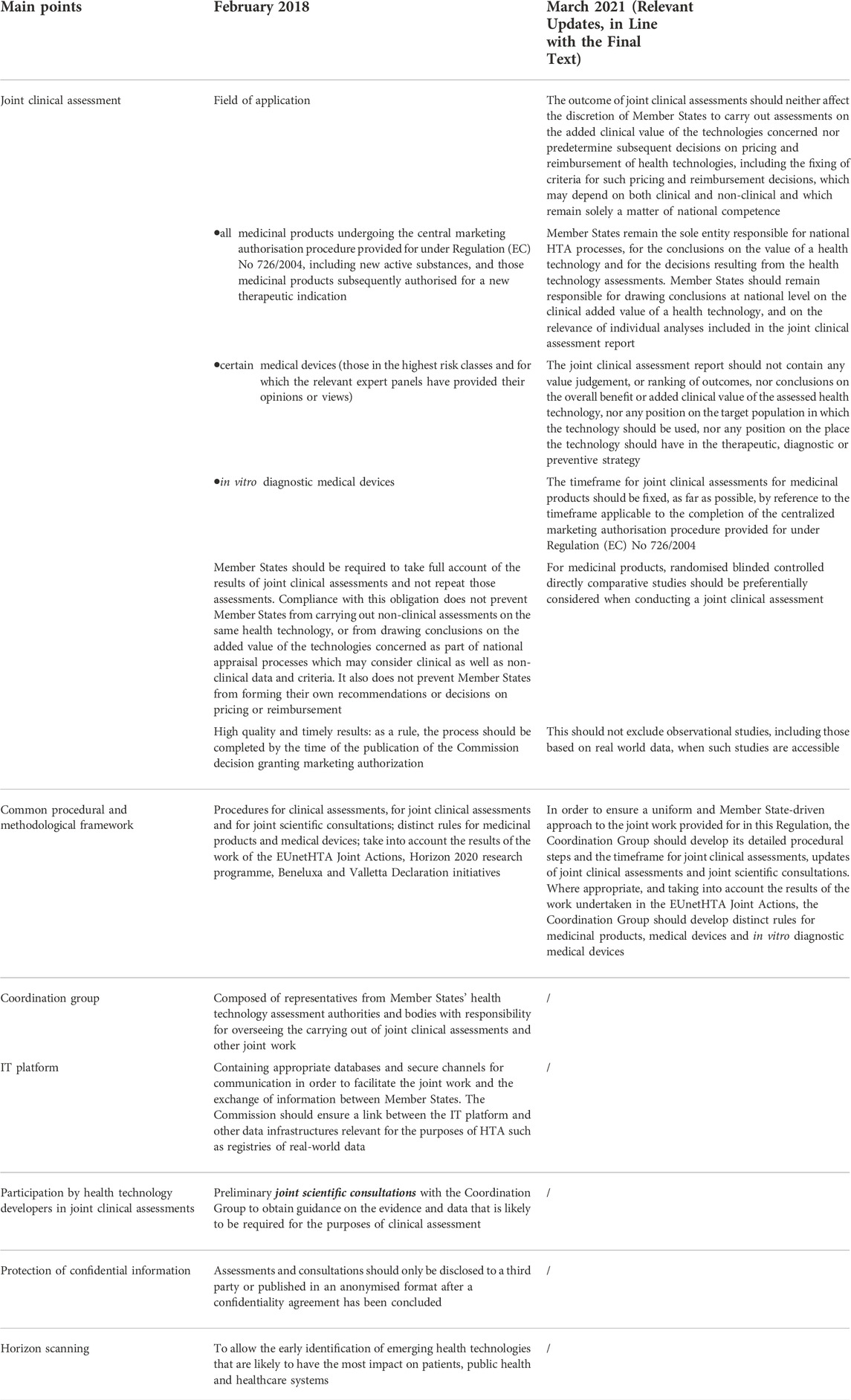
Table 1. Main features of the proposal for a Regulation of the European Parliament on health technology assessment and amending Directive 2011/24/EU (draft February 2018 and March 2021).
The discussion about amendments and final adoption of the proposal lasted for years due to concerns around its feasibility and its implications for national health care systems.
The first proposal was that Member States would take full account of the results of joint clinical assessments and would not repeat those assessments; however, they could carry out non-clinical assessments on the same health technology and draw conclusions on the added value within the national appraisal processes, forming their own recommendations on pricing and reimbursement.
The final version does not mention this obligation and stresses only the discretion of Member States to carry out assessments on the added clinical value and to take decisions on pricing and reimbursement, which may depend on both clinical and non-clinical features.
A recent survey showed the divergences of methodology among HTA bodies in 27 EU Member States and Norway (Kristensen, 2017). In order to achieve a real harmonization, an agreement among Member States should be developed on appropriate assessment methods as well as relevant outcome parameters, appropriate comparators and the relevant data sets for the assessments.
The joint clinical assessment under the umbrella of the new Regulation should notably be supported by reliable, practicable and justifiable parameters, shared and standardized by EU-HTA bodies and payers, using both clinical trial data and “real life data” collected in dedicated comparative registries or as part of routine healthcare provision.
Therefore, the following concepts should be universally defined in clear terms, within the HTA framework that has been designed by the new Regulation:
1) clinical value and added clinical value;
2) appropriate comparators, starting from what is mentioned in internationally recognized disease treatment guidelines, taking into account national restrictions on comparator therapies;
3) reliable and clinically relevant endpoints (& Key Performance Indicators, specific and measurable elements used to assess quality of care) and outcomes to be considered in the HTA processes using data from clinical trials and real-life settings;
4) acceptable quality of evidence, including the need to clearly define the role of post-approval evidence, indirect treatment comparisons and outcome registries, in particular when randomized clinical trial data are not available (e.g. due to the rarity of the disease or special access schemes);
5) defining the links between patient benefits and societal benefits - which may exceed the effect of drugs on individuals - and their systemic impact.
All the critical issues emerged were not addressed in the proposal nor in the final draft.
The final draft of the Regulation moves even further away from these goals. It provides that the detailed definition of procedures and timing for joint clinical assessments and joint scientific consultations will be subsequently established by the Coordination Group. While the preliminary draft stated that Member States should take full account of the results of the joint clinical assessments without the possibility of repeating them, the final version underline that Member States may carry out clinical assessments in order to define the therapeutic added value of the technologies and are the sole responsible for national HTA processes. Moreover, the joint clinical assessment reports should not contain conclusions on the overall benefit or added clinical value of the new technology, nor any opinion about the target population in which the technology should be used, probably to avoid influencing national decisions in terms of usage restrictions (eg eligibility criteria in AIFA monitoring register (Breccia et al., 2020; Olimpieri et al., 2020; Breccia et al., 2021; Gozzo et al., 2021c). Nevertheless, HTA is per definition an evidence-based process that allows to determine the relative effectiveness, and specifically the added value in comparison with other new or existing health technologies.
In addition, this is clearly in contrast to the European Parliament resolution of 2 March 2017 (EUROPARL, 2017), mentioned in the draft, which underlined the need for the creation of a European system for HTA as soon as possible, with transparent and harmonised HTA criteria “in order to assess the added therapeutic value of medicines compared with the best available alternative taking into account the level of innovation and value for the patients among others, to introduce compulsory relative effectiveness assessments at EU level as a first step for new medicines, and to put in place a European classification system to chart their therapeutic added value level”.
As regards to the quality of evidence, the Regulation partially addresses this issue, pointing out that direct comparison obtained through randomised blinded controlled trials are the standard to consider in the joint clinical assessment, although not excluding observational studies, including those based on real world data.
Reaching agreement on the points described in this document, and enhancing experience-sharing amongst the EU nations within this perspective and other domains (e.g. patient-reported outcome measures), would be useful to promote the real convergence of HTA methodologies, hopefully leading to reduced disparities in patient access to medicines across European countries.
The European harmonization would influence the HTA procedures in global communities beyond EU. For example, the Pharmaceuticals and Medical Devices Agency (PMDA) in Japan plans to promote and contribute to the international regulatory harmonization and global cooperation through the International Council for Harmonisation of Technical Requirements for Pharmaceuticals for Human Use (ICH) (PMDA). Moreover, the new launch of HTA 2019 in Japan employing value-based pricing (HTAsiaLink, 2020)might trigger and boost the HTAsiaLink, the HTA agencies’ networking in Asia (Teerawattananon et al., 2018; Kamae, 2019), to harmonize the HTA in the regions, learning from the EU initiatives. HTAsiaLink is a voluntary collaborative research network of HTA agencies in the Asia-Pacific region established in 2010. Actually, around 34 agencies from 17 different countries voluntarily join the network. The functions of HTAsiaLink network evolved from platform for sharing research findings to a vehicle for sharing awareness about the usefulness of HTA evidence for policy decisions. One of the goals of the Network is ‘avoiding duplication especially in reviewing safety and clinical efficacy of vaccines and medicines for HTA, facilitating learning, reducing wasteful resource use, and enhancing efficiency at organizational level through collaborative activities among the network’, similar in part to that of EU collaboration. Given that most of the network’s members are newly established HTA agencies with relatively few experienced and share cultural attributes and common policy challenges, the Asian harmonization could be probably easier than EU harmonization.
The views expressed in this article are the personal views of the authors (national experts, representatives of academic institutions and/or members of health organizations) and may not be understood or quoted as being made on behalf of or reflecting the position of the regulatory agency or organisations with which the authors are employed/affiliated.
The conclusions reported in this paper is the result of the discussion among the authors carried out at the European Regulatory Conference held in Catania in February 2020.
All authors contributed read, revised, and approved the submitted version.
OW was employed by the company Medi Quality Omega.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Akehurst, R. L., Abadie, E., Renaudin, N., and Sarkozy, F. (2017). Variation in health technology assessment and reimbursement processes in Europe. Value Health 20 (1), 67–76. doi:10.1016/j.jval.2016.08.725
Allen, N., Liberti, L., Walker, S. R., and Salek, S. (2017). A comparison of reimbursement recommendations by European HTA agencies: Is there opportunity for further alignment? Front. Pharmacol. 8, 384. doi:10.3389/fphar.2017.00384
Angelis, A., Lange, A., and Kanavos, P. (2018). Using health technology assessment to assess the value of new medicines: Results of a systematic review and expert consultation across eight European countries. Eur. J. Health Econ. 19 (1), 123–152. doi:10.1007/s10198-017-0871-0
Breccia, M., Celant, S., Olimpieri, P. P., Olimpieri, O. M., Pane, F., Iurlo, A., et al. (2021). Mortality rate in patients with chronic myeloid leukemia in chronic phase treated with frontline second generation tyrosine kinase inhibitors: A retrospective analysis by the monitoring registries of the Italian medicines agency (AIFA). Ann. Hematol. 100 (2), 481–485. doi:10.1007/s00277-021-04406-1
Breccia, M., Olimpieri, P. P., Olimpieri, O., Pane, F., Iurlo, A., Foggi, P., et al. (2020). How many chronic myeloid leukemia patients who started a frontline second-generation tyrosine kinase inhibitor have to switch to a second-line treatment? A retrospective analysis from the monitoring registries of the Italian medicines agency (AIFA). Cancer Med. 9 (12), 4160–4165. doi:10.1002/cam4.3071
Ciani, O., and Jommi, C. (2014). The role of health technology assessment bodies in shaping drug development. Drug Des. devel. Ther. 8, 2273–2281. doi:10.2147/DDDT.S49935
Council on health technology (2021). Proposal for a regulation of the European parliament and of the Council on health technology assessment and amending directive 2011/24/EU - partial mandate for negotiations with the European parliament. Brussels: General Secretariat of the Council.
Council on health technology (2018). Proposal for a regulation of the european parliament and of the council on health technology assessment and amending Directive 2011/24/EU. European Commission, Directorate-General for Health and Food Safety.
Drummond, M. F., Schwartz, J. S., Jonsson, B., Luce, B. R., Neumann, P. J., Siebert, U., et al. (2008). Key principles for the improved conduct of health technology assessments for resource allocation decisions. Int. J. Technol. Assess. Health Care 24 (3), 244–258. ; discussion 362-8. doi:10.1017/S0266462308080343
EMA EMA (2020a) Available at: http://www.ema.europa.eu/en/about-us/what-wedo/authorisation-medicines (Accessed April, 2022).
EMA. EMA (2020b) Available at: http://www.ema.europa.eu/en/about-us/what-wedo/authorisation-medicines-centralised-authorisation-procedure-section.
EMA. EMA. Available at: https://www.ema.europa.eu/en/human-regulatory/overview/support-early-access.
EUNETHA (2020) Eunethta. Available at: https://eunethta.eu/about-eunethta/.
EUNETHA (2022) JA3 archive (2016-2021).Accessed at: https://www.eunethta.eu/ja3-archive/
EUNETHTA (2018) EUnetHTA. Eunethta Joint Action 2 2012-2015 Final Technical Report. Available at: https://www.eunethta.eu/wp-content/uploads/2018/01/EUnetHTAJA2_FinalTechnicalReport_Executive-Summary_May2016.pdf?x69613&x50316 (Accessed at July, 2022. 2018).
EUNETHTA (2013) EUnetHTA joint action. European network for health technology assessment. Final Technical Report 2010-2012. Available at: https://www.eunethta.eu/wp-content/uploads/2013/01/EUnetHTA-JA-FinalTechnicalReport2010_2012FinalVersion20130531_0-1.pdf?x69613 (Accessed at July, 2022. 2013).
EUNETHTA (2008) EUnetHTA project. Overview of results. Available at: https://www.eunethta.eu/wp-content/uploads/2018/01/Overview-of-the-EUnetHTA-Project-Results-2006-2008_0.pdf?x69613 (Accessed by July 2022 2009)
EUnetHTA (2009) EUnetHTA Collaboration Key activities and achievements in 2009. Available at: https://www.eunethta.eu/wp-content/uploads/2018/01/EUnetHTA-Key-activities-and-achievements-in-2009.pdf?x69613 (Accessed at July 2022 2010.
EUROPARL (2017) European Parliament resolution of 2 March 2017 on EU options for improving access to medicines – 2016/2057(INI). Available at : https://www.europarl.europa.eu/doceo/document/TA-8-2017-0061_EN.html.
Gozzo, L., Di Lenarda, A., Mammarella, F., Olimpieri, P. P., Cirilli, A., Cuomo, M., et al. (2021). Starting dose and dose adjustment of non-vitamin K antagonist oral anticoagulation agents in a nationwide cohort of patients with atrial fibrillation. Sci. Rep. 11 (1), 20689. doi:10.1038/s41598-021-99818-4
Gozzo, L., Longo, L., Vitale, D. C., and Drago, F. (2020). The regulatory challenges for drug repurposing during the covid-19 pandemic: The Italian experience. Front. Pharmacol. 11, 588132. doi:10.3389/fphar.2020.588132
Gozzo, L., Romano, G. L., Brancati, S., Cicciu, M., Fiorillo, L., Longo, L., et al. (2021). Access to innovative neurological drugs in Europe: Alignment of health technology assessments among three European countries. Front. Pharmacol. 12, 823199. doi:10.3389/fphar.2021.823199
Gozzo, L., Romano, G. L., Romano, F., Brancati, S., Longo, L., Vitale, D. C., et al. (2021). Health technology assessment of advanced therapy medicinal products: Comparison among 3 European countries. Front. Pharmacol. 12, 755052. doi:10.3389/fphar.2021.755052
HTAsiaLink (2020) Available at: https://www.htasialink.org/about/overview.html.
Jommi, C., Armeni, P., Costa, F., Bertolani, A., and Otto, M. (2020). Implementation of value-based pricing for medicines. Clin. Ther. 42 (1), 15–24. doi:10.1016/j.clinthera.2019.11.006
Kamae, I. (2019). Health technology assessment in Japan - policy, pharmacoeconomic methods and guidelines, value, and beyond. Berlin, Germany: Springer Nature.
Kristensen, F. B. (2017) Mapping of HTA methodologies in EU and Norway. Available at: https://ec.europa.eu/health/sites/default/files/technology_assessment/docs/2018_mapping_methodologies_en.pdf.
Moseley, J., Vamvakas, S., Berntgen, M., Cave, A., Kurz, X., Arlett, P., et al. (2020). Regulatory and health technology assessment advice on postlicensing and postlaunch evidence generation is a foundation for lifecycle data collection for medicines. Br. J. Clin. Pharmacol. 86 (6), 1034–1051. doi:10.1111/bcp.14279
Olimpieri, P. P., Di Lenarda, A., Mammarella, F., Gozzo, L., Cirilli, A., Cuomo, M., et al. (2020). Non-vitamin K antagonist oral anticoagulation agents in patients with atrial fibrillation: Insights from Italian monitoring registries. Int. J. Cardiol. Heart Vasc. 26, 100465. doi:10.1016/j.ijcha.2019.100465
PMDA. PMDA. Available at: https://www.pmda.go.jp/english/int-activities/outline/0017.html (Accessed April, 2022).
Richardson, J., and Schlander, M. (2019). Health technology assessment (HTA) and economic evaluation: Efficiency or fairness first. J. Mark. Access Health Policy 7 (1), 1557981. doi:10.1080/20016689.2018.1557981
Teerawattananon, Y., Luz, K., Yothasmutra, C., Pwu, R. F., Ahn, J., Shafie, A. A., et al. (2018). Historical development of the htasialink network and its Key determinants of success. Int. J. Technol. Assess. Health Care 34 (3), 260–266. doi:10.1017/S0266462318000223
van Nooten, F., Holmstrom, S., Green, J., Wiklund, I., Odeyemi, I. A., and Wilcox, T. K. (2012). Health economics and outcomes research within drug development: Challenges and opportunities for reimbursement and market access within biopharma research. Drug Discov. Today 17 (11-12), 615–622. doi:10.1016/j.drudis.2012.01.021
Keywords: health technology assessment, recommendations, harmonization, european regulation, european regulatory conference
Citation: Gozzo L, Paterson K, Wong O, Megerlin F, Geldmacher J, Popoli P, Jommi C, Fricke F-U, De Solà-Morales O, Kamae I, Rasi G and Drago F (2022) Towards a European harmonization of health technology assessment recommendations executive paper of European regulatory conference focused on the EU commission proposal to harmonize HTA. Front. Drug Saf. Regul. 2:970661. doi: 10.3389/fdsfr.2022.970661
Received: 16 June 2022; Accepted: 20 July 2022;
Published: 15 August 2022.
Edited by:
Mina Tadrous, Women’s College Hospital, CanadaReviewed by:
Patricia Coelho de Soarez, University of São Paulo, BrazilCopyright © 2022 Gozzo, Paterson, Wong, Megerlin, Geldmacher, Popoli, Jommi, Fricke, De Solà-Morales, Kamae, Rasi and Drago. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Filippo Drago, Zi5kcmFnb0B1bmljdC5pdA==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.