
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Drug Saf. Regul. , 09 January 2023
Sec. Rheumatic Drug Safety
Volume 2 - 2022 | https://doi.org/10.3389/fdsfr.2022.1044696
 Pedro Santos-Moreno1*
Pedro Santos-Moreno1* Linda Ibatá2Susan Martínez2
Linda Ibatá2Susan Martínez2 Gabriel-Santiago Rodríguez-Vargas1Laura Villarreal1Pedro Rodríguez1Wilberto Rivero1
Gabriel-Santiago Rodríguez-Vargas1Laura Villarreal1Pedro Rodríguez1Wilberto Rivero1 Fernando Rodríguez-Florido1
Fernando Rodríguez-Florido1 Adriana Rojas-Villarraga3
Adriana Rojas-Villarraga3Introduction: The antimalarials chloroquine and hydroxychloroquine have been used for several decades in treating malaria and some autoimmune diseases—mainly rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE)—with excellent efficacy and safety. Due to the massive use of antimalarials worldwide for managing SARS-CoV-2/COVID-19 infection during the last 2 years and the consequent increase in cardiac arrhythmia, fear has risen about the safety of using antimalarials, especially for patients with increased cardiovascular risk.
Objective: To describe a real-life experience about the safety of antimalarials in the setting of a single rheumatological center in Colombia.
Methods: This is a cross sectional study that includes patients diagnosed with RA and treated with antimalarials between 2020 and 2021. Clinical follow-up information was gathered from the medical records, and all reported adverse events were described.
Results: A total of 957 patients were included, primarily women (79.2%). The most frequent comorbidities were hypertension and osteoporosis. Chloroquine use was more frequent than hydroxychloroquine (86.4% vs. 13.6%). During the observation period, 243 (25.4%) patients presented at least one adverse event, 72 (29.6%) had retinal toxicity, 85 (35%) dermatological events, and 81 (33.3%) gastrointestinal intolerance. Other adverse events reported less frequently (15.2%) included headache, dizziness, lipothymia, and elevated transaminases. There were no reports of cardiovascular events from the period of antimalarial use to the date of data collection despite the high frequency of previous metabolic or cardiovascular disease in this cohort.
Conclusion: This study reasserts the evidence of antimalarials safety profile for patients with rheumatological conditions such as RA. RA patients that were treated with antimalarials at doses recommended by the guidelines had no cardiovascular events.
The antimalarials initially used to manage Plasmodium spp infection have been used in recent decades to treat rheumatic diseases like rheumatoid arthritis (RA) and systemic lupus erythematosus (SLE) because they help control joint and skin manifestations (Plantone and Koudriavtseva, 2018). The mechanisms of action these medications have are not fully understood yet. However, their effects are known to modify the functionality of Toll-like receptors and reduce the secretion of interleukins (Rosenbaum et al., 2016). Nevertheless, they are commonly used and crucial in patients with RA or SLE to control the inflammatory disease activity (Schrezenmeier and Dörner, 2020).
In the 1990s, the safety of this pharmacological group began to be discussed due to reports of some adverse effects, mainly ophthalmological. However, over the years, several studies have shown that chloroquine (CQ) and hydroxychloroquine (HCQ) are safe for patients with rheumatic diseases. Therefore, considering the risk/benefit balance, people with these pathologies are currently treated with antimalarials following international guidelines (Mackenzie, 1983; Felson et al., 1990; Fries et al., 1993).
RA is a chronic, autoimmune, and systemic disease which is characterized by inflammation in the synovial membrane that causes swelling, pain, and stiffness in the joints. Illness could generate other extraarticular manifestations (Smolen et al., 2016). Treating diseases depends on disease activity and extraarticular compromise. Many studies demonstrate the usefulness of the antimalarials in controlling the disease and explained the importance of following the, mainly ocular, adverse events (Mackenzie, 1983).
In 2020, the coronavirus disease (COVID-19) pandemic caused by the SARS-COV2 led physicians to use multiple experimental pharmacological treatments, including HCQ and CQ combined with antibiotic agents (Wong et al., 2021). Unfortunately, the outcomes of clinical trials were not encouraging and showed high toxicity, mainly cardiovascular, with increased frequencies of QT interval prolongation and arrhythmias (Bansal et al., 2021). Once again, this finding raised questions about the safety of using antimalarials, especially in patients with increased cardiovascular risk. Likewise, this concern caused antimalarial treatment for patients with autoimmune diseases to be suspended, and this generated a higher frequency of disease relapses (Saldarriaga Rivera et al., 2020; Egeli et al., 2021).
Considering the frequency and the risks linked to using antimalarials, the purpose of the study is to describe the safety profile of these medications and, evaluate cardiotoxicity and other adverse events in patients with RA that were admitted to a specialized rheumatology center in a real-life experience.
This is a cross sectional study that included patients diagnosed with RA and treated with antimalarial agents, regardless of the treatment start date or duration. All the clinical records of patients that were seen at the rheumatological center from January 2020 to December 2021 were included.
The following were considered inclusion criteria: 1) Age of 18 or above 2) a confirmed diagnosis of RA [International Classification of Diseases (ICD): M069, M059, M060] based on the classification criteria of the American College of Rheumatology/European League Against Rheumatism (Aletaha et al., 2010) and 3) use of antimalarials during the follow-up period, regardless of the type (CQ 3.5–4 mg/kg daily/HCQ 6–6.5 mg/kg daily, according to the institution protocol and international guidelines) (Mackenzie, 1983; Felson et al., 1990). Conversely, the following were exclusion criteria: 1) Patients with a confirmed diagnosis of juvenile arthritis based on international criteria and 2) patients who did not have three or more visits during the follow-up period (for any reason, for example, administrative reasons, change of insurance, change of city, so on).
All patients are treated in a specialized multidisciplinary program, including experienced rheumatologists who determine the appropriate doses of medications. Additionally, the “treat to target, T2T″ management strategy is used for follow-up and outcomes (Smolen, 2016). Patients come on a monthly-bimonthly basis and are evaluated by a multidisciplinary team, including a nutritionist, a pharmaceutical chemist, and a psychologist.
All patients in the specialized multidisciplinary program received pharmaceutical care consisting of medication review follow-up based on Dáder’s method (DMet) (Sabater Hernadez et al., 2007), (Pharmaceutical Care Research Group, 2006). This is a systematic process developed by the Research Group of Pharmaceutical Care at the University of Granada, Spain that includes health education, help in adhering to treatment, registration of adverse drug reactions, and therapeutic drug monitoring of disease-modifying antirheumatic drugs (DMARDs).
Data were collected from medical records under strict confidential and anonymized information management criteria. Baseline clinical data, including the evaluation of RA activity by measuring disease activity using the disease activity score 28 joints (DAS28) (Prevoo et al., 1995) and the Health Assessment Questionnaire (HAQ) (Bruce and Fries, 2005), and follow-up data were gathered to analyze the hematologic, liver, and renal function and inflammatory activity. In addition, data regarding the medications used for the underlying disease and other laboratory test results of interest were collected. The primary outcome was the presence of antimalarial adverse events. These events were defined, reported on, and described by the treating physician and the pharmaceutical chemist (under the DMet program).
The Third Consensus of Granada (TCG) was used to classify drug-related problems (Comité de Consenso, 2007). This classification includes three categories. The first category is related to need, the second is related to efficacy, and the last one is related to adverse reactions to medications, and this is the one that we used to classify adverse events related to antimalarials. Each patient was registered and all adverse events that they had presented up until the data collection date were included. Additionally, the adverse drug reaction probability was assessed according to the Naranjo probability scale (Naranjo et al., 1981). Therefore, this probability was categorized by taking sum of the 10 questions and grouped as definite, probable, possible, or doubtful if the total score was ≥9, 5–8, 1–4, and 0 respectively.
Analyzes were done in R statistical software. Qualitative variables are presented through frequencies and percentages. The quantitative variables are presented as means and standard deviations, or medians and interquartile ranges, depending on their distribution based on the Kolmogorov-Smirnov test.
This research was approved by the Human Research Ethics Committee - Hospital de San José, Bogotá, Colombia (File 0317-2021, 1 June 2021) and follows the declaration of Helsinki’s guidelines and the ethical principles of human research.
Records of 957 patients from 1 January 2020, to 31 December 2021 were included in the study. The characteristics of these patients are described in Table 1. Metabolic and cardiovascular alterations were the main comorbidities found in the cohort; arterial hypertension (30.3%) was the most prevalent, followed by osteoporosis (27%) and diabetes mellitus (9.5%). Most of the patients evaluated were in remission (539, meaning 59.4%) or had low disease activity (141, meaning 15.5%). Moreover, the HAQ showed that the patients’ functionality, in general, was not compromised (see Table 1).
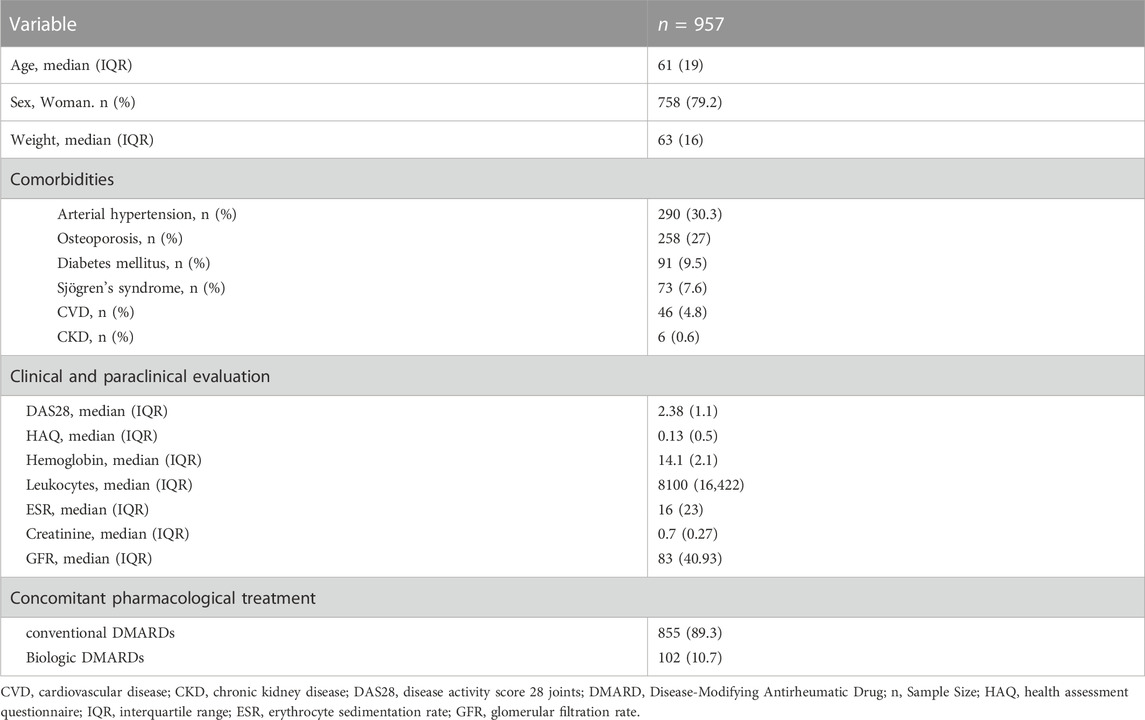
Table 1. Characteristics of the study cohort.
Regarding the pharmacological treatment of RA, 89.3% of patients received conventional synthetic DMARDs (csDMARDs), while 10.7% received treatment with biologic DMARDs. Two types of antimalarials were administered to patients: CQ with a dose of 250 mg/day in 86.4% of cases and HCQ with a dose of 200 mg/day in 13.6% of cases. During the follow-up, 67 (7%) patients had a therapeutic failure.
Based on the TCG classification criteria of the drug related problems exposed, we identified 275 adverse reactions to medications (third category of the TCG) attributed to antimalarials that were found in 243 (25.4%) patients. The most frequent events were dermatological events in 85 (35%) patients, followed by gastrointestinal intolerance in 81 (33.3%), and retinal toxicity in 72 (29.6%). Patients could present more than one pharmacological-related adverse event. The description of the adverse events is shown in Table 2. There were no reports of cardiovascular events at the time the data collection was completed. Based on Naranjo probability scale, 100% of dermatological, gastrointestinal intolerance, retinal toxicity and elevation of serum transaminases adverse events were classified as probable, the remaining adverse events were classified as possible (Table 2).
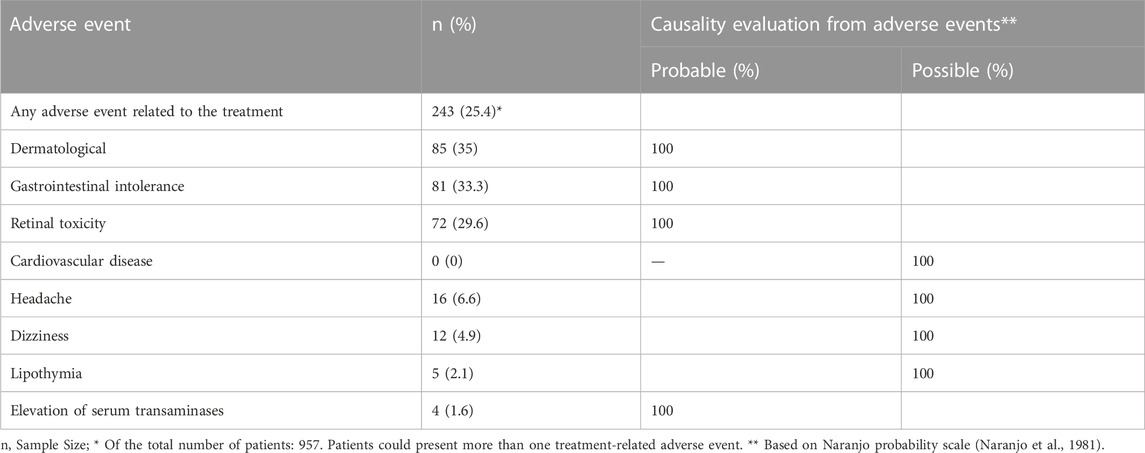
Table 2. Typification of adverse events due to antimalarials.
Antimalarial toxicity has been a concern among rheumatologists in the search for a balance between therapeutic effects and low toxicity. In 2-years of follow-up, this study showed a low prevalence of cardiotoxicity and other major events in RA patients. These medicines has been widely used over the years to fight malaria, treat rheumatic diseases, and recently in the treatment of COVID-19 based on its immunomodulatory, direct anti-inflammatory, and indirect antiviral properties (Vitte et al., 2020); however, they are no longer being used (Paliani and Cardona, 2020).
During the COVID-19 pandemic, publication of scientific articles increased due to the need for immediate information that would allow healthcare workers to make decisions about the care given to patients admitted to intensive care units. This urgent necessity undermined scientific accuracy, and in some cases, the information came from unclear sources and led to the retraction of several articles (Mehra et al., 2020; Lee et al., 2021). These COVID-19 studies concluded that the use of antimalarials increased cardiac arrhythmia in patients admitted to intensive care units. This premise was dangerous because patients with rheumatic diseases that were using antimalarials were the ones mainly affected by questioning of the safety of these drugs. It is noteworthy that in most of the COVID-19 studies, antimalarial doses were 1.5 to twice the dose used in the rheumatology setting (U.S. National Library of Medicine, 2022). Furthermore, although the administration period of antimalarials in such studies is shorter than the one used in RA treatment, in most, they have been used in conjunction with other medications such as antibiotics that are not frequently used in the rheumatology field.
This real-world study of evidence that included 957 patients identified a demographic of rheumatic diseases that is well-known: a predominance of women (Favalli et al., 2019). Similarly, the incidence of RA has been observed after the age of 50 as seen in this study which 75.4% of patients were over 40 years old (van der Woude and van der Helm-van Mil, 2018). The most common comorbidities in this group of patients were those related to metabolic syndromes like arterial hypertension and diabetes mellitus. The convergence between those comorbidities and RA has been extensively studied, and the conclusion was that these two entities share common pathophysiological pathways associated with pro-inflammatory states. In these states, cytokines, such as tumour necrosis factor (TNF) and interleukin-6 (IL-6), play a crucial role (Kerekes et al., 2014). Arterial hypertension was the main comorbidity in the cohort, with a prevalence of 30%, similar to that found in other studies (Romano et al., 2018). Osteoporosis was the second comorbidity found in our study. Several investigations have found a pathophysiological relationship between osteoporosis and autoimmune diseases. This relationship can be explained by a pro-inflammatory state where IL-6 and TNF increase osteoclast activity and osseous tissue damage (Adami and Saag, 2019). Diabetes mellitus was another prevalent disease in this group that also presents pro-inflammatory conditions and generates insulin resistance when simultaneously using corticosteroids (Romano et al., 2018). Thus, our population had characteristics of a typical real-life cohort with rheumatic involvement undergoing treatment. Remarkably, there were no cardiovascular adverse events despite the patients’ cardiometabolic context.
Regarding treatment, most patients remained under pharmacological treatment with csDMARDs based on the treatment guidelines and the disease activity as expected. The choice between CQ and HCQ depended on the disease’s activity, availability of medicine, and treating physician. In our study, 86% of patients received CQ, while in the report by Cabral et al. 55% of patients were treated with HCQ and 25% with CQ (Cabral et al., 2019).
This study found that dermatological adverse events were the most common, followed by gastrointestinal and ocular ones. These findings are similar to those reported by Mittal et al. (2018), where the main adverse event was dermatological, followed by gastrointestinal intolerance and neurological disorders. Visual disturbances are one of the most feared adverse effects, and the risk has been demonstrated to be greater in patients medicated with CQ (Mittal et al., 2018). These adverse effects were observed in 7.5% of our patients. It has been suggested that these disturbances are due to alterations in the retinal pigment epithelium that reduces central and night vision (Rosenbaum et al., 2016). Therefore, people on antimalarials should undergo routine examinations to detect visual disturbances, mainly visual field tests once a year after the fifth year of treatment (Peponis et al., 2010).
The results of the present study agree with those found by Majewski et al., who analysed 152 patients with rheumatic diseases (29 with RA) that were treated with antimalarials. Their study was done because of concerns generated about the use of these drugs in the context of COVID-19 and the possible cardiovascular risk they may cause. They found a frequency of 6.6% of adverse ophthalmological events and 22.4% of other adverse events but highlighted that no statistically significant correlation was found among adverse events, age, chronic heart or liver disease, or high blood pressure for both drugs (Majewski et al., 2021).
The cardiovascular effects linked to antimalarials are mainly those that compromise the cardiac conduction system followed by the ones that alter anatomy (Desmarais et al., 2021; Eveleens Maarse et al., 2022). In this regard, none of our patients presented adverse cardiovascular effects during the study period. This takes into account the fact that their treatment was carried out in a specialized multidisciplinary program by rheumatologists with a lot of experience and who are administering proper doses. In addition, patients were in a pharmaceutical program that follows a special methodology (DMet program). A systematic review by Chatre et al. showed that cardiovascular adverse events are rare but serious. Furthermore, her study showed that these adverse events were mainly related to CQ use over extended periods (median 7 years, minimum 3 days, maximum 35 years) and high cumulative doses (median 1,235 g for HQC and 803 g for CQ) (Chatre et al., 2018). Additionally, another systematic review evaluated the frequencies of serious adverse events such as retinopathy, and cardiac complications through randomized clinical trials of patients with malaria and non-malarial conditions. It was found that CQ and HCQ are unlikely to increase serious adverse events and such events are low in frequency in both malarial and non-malarial conditions (Souza Botelho et al., 2021).
Likewise, some studies have shown that the incidence of long QT syndrome and arrhythmia-related hospitalization is low for RA patients during the first year of treatment using HCQ or another non-biological DMARD. Furthermore, there was no evidence of a link between HCQ therapy and an increased risk of adverse cardiovascular events or death (Faselis et al., 2021). Indeed, some studies showed that the use of HCQ was not linked to the development of heart failure in patients with RA (Sorour et al., 2021). However, another study showed that HCQ and methotrexate had similar risks of sudden cardiac death, ventricular arrhythmia, or major adverse cardiovascular event in older RA patients. Therefore, those with a history of heart failure who started to take HCQ had higher risks of a major adverse cardiovascular event, cardiovascular mortality, all-cause mortality, and myocardial infarction (D’Andrea et al., 2022). Similarly, another study that involved patients with RA and SLE showed that the use of HCQ did not increase the risk of cardiac and ventricular arrhythmias regardless of the treatment duration (Lo et al., 2021a).
During the pandemic, research showed that arrhythmogenic effects were mainly due to pharmacological interactions with other drugs, such as azithromycin, and the use of HQC and CQ in critically ill patients (Bansal et al., 2021; Budhathoki et al., 2021). In this respect, the study carried out by Lozano-Cruz et al. showed that adverse events (including electrocardiographic alterations, such as prolongation of the corrected QT interval, p = .38 and ventricular arrhythmias, p = .058) in patients with COVID-19 treated with antimalarials were similar to those who did not receive antimalarials in medical centers with strict drug monitoring. Also, it should be noted that these drugs do not improve survival from COVID-19 in patients who receive optimal medical care.
On the other hand, the cardioprotective effect of antimalarials in inflammatory diseases that increase cardiovascular risk, such as rheumatic diseases, is well known. Thus, a meta-analysis involving patients with RA and SLE showed that using CQ/HCQ reduced the risk of cardiovascular disease in patients with rheumatic diseases (RR 0.72, 95% CI: 0.56–0.94, p = 0.013) (Liu et al., 2018) (Souza Botelho et al., 2021). Furthermore, studies after this meta-analysis have corroborated the results in patients with SLE (Lo et al., 2021b; Rúa-Figueroa et al., 2022).
Based on these studies, the concerns about the cardiovascular safety of antimalarials, and the findings of COVID-19 studies, the American College of Rheumatology issued a document called the American College of Rheumatology White Paper on Antimalarial Cardiac Toxicity that highlighted current data indicating that HCQ and CQ are invaluable drugs in the treatment for rheumatic and dermatologic diseases. Also, it stated that cardiac toxicity related to HCQ/CQ treatment for rheumatic diseases is rare. Still, it is slightly associated with QTc interval prolongation, especially for patients taking additional QTc prolonging drugs. Therefore, they suggest evaluating the safety profile of concomitant medications and the patient’s cardiovascular risk before prescribing these drugs and doing more research on this subject (Desmarais et al., 2021).
It is noteworthy that, like other drugs, toxic doses of antimalarials, described in cases of overdose, poisoning or suicidal attempt (Reddy and Sinna, 2000; Yanturali et al., 2004; Gunja et al., 2009), have been associated with fatal outcomes (Messant et al., 2004; White, 2007); mainly caused by hydroelectrolytic disbalance (i.e., severe hypokalemia) and cardiovascular effects, mostly life-threatening ventricular arrhythmias. Although cases of cardiomyopathies secondary to its chronic use have been described (Chatre et al., 2018), it is rare in patients with rheumatic diseases, where the drug doses used are those recommended by clinical practice and therefore the possibility of presenting this type of event is not expected. Therefore, these medications should be only based on guidelines management, being strictly monitored by multidisciplinary teams, and evaluating the risk-benefit of their use.
The main limitations in the present study are the fact that only frequencies of the adverse events are described, and sub-categories of adverse reactions are not differentiated by system. Also, validity can be questioned by the inherent limitations of the study design. Furthermore, these results cannot be generalized to populations other than those who are treated in a specialized multidisciplinary program under the T2T management strategy, therefore this circumstance can be considered an additional limitation of the study.
The use of antimalarials for patients with autoimmune diseases, especially RA, is effective during active disease. For some time, there were doubts about their safety and adverse effects, and these increased during the COVID-19 pandemic. This study found that the main alterations that developed were dermatological, gastrointestinal intolerance, and retinal toxicity. They were expected based on the known safety profile of these drugs, and no patient developed adverse cardiovascular effects. These findings reinforce the evidence that antimalarials are drugs with proven cardiovascular safety in rheumatic patients. It is crucial to continue researching pharmacovigilance to consolidate the safety profile of these drugs that are widely used and effective in treating patients with rheumatic diseases.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
The studies involving human participants were reviewed and approved by Human Research Ethics Committee—Hospital de San José, Bogotá, Colombia (File 0317-2021, 1 June, 2021). The patients/participants provided their written informed consent to participate in this study.
PS-M, LV, G-SR-V, AR-V, WR, and PR contributed to the concept and design of the study, LI, SM, and FR-F collected and organized the clinical database, LI, SM did the statistical analysis, PS-M, LI, SM, LV, G-SR-V, FR-F, PR, WR, and AR-V wrote the original draft. All authors contributed to manuscript revision, read, and approved the submitted version.
The authors declare that the research was done in the absence of any funding.
All the authors would like to thank Michael Cabrera for his participation and help with the data collection for this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Adami, G., and Saag, K. G. (2019). Osteoporosis pathophysiology, epidemiology, and screening in rheumatoid arthritis. Curr. Rheumatol. Rep. 21 (7), 34. doi:10.1007/s11926-019-0836-7
Aletaha, D., Neogi, T., Silman, A. J., Funovits, J., Felson, D. T., Bingham, C. O., et al. (2010). 2010 rheumatoid arthritis classification criteria: An American College of rheumatology/European League against rheumatism collaborative initiative. Arthritis Rheum. 62 (9), 2569–2581. doi:10.1002/art.27584
Bansal, P., Goyal, A., Cusick, A., Lahan, S., Dhaliwal, H. S., Bhyan, P., et al. (2021). Hydroxychloroquine: A comprehensive review and its controversial role in coronavirus disease 2019. Ann. Med. 53 (1), 117–134. doi:10.1080/07853890.2020.1839959
Bruce, B., and Fries, J. F. (2005). The health assessment Questionnaire (HAQ). Clin. Exp. Rheumatol. 23, S14–S18.
Budhathoki, P., Shrestha, D. B., Khadka, S., and Rawal, E. (2021). Is hydroxychloroquine with azithromycin a good combination in COVID-19 compared to hydroxychloroquine alone from cardiac perspective? A systematic review and meta-analysis. J. Nepal Health Res. Counc. 19 (1), 1–9. doi:10.33314/jnhrc.v19i1.3270
Cabral, R. T. S., Klumb, E. M., and Carneiro, S. (2019). Patients opinion and adherence to antimalarials in lupus erythematosus and rheumatoid arthritis treatment. J. Dermatol. Treat. 31 (3), 264–269. doi:10.1080/09546634.2019
Chatre, C., Roubille, F., Vernhet, H., Jorgensen, C., and Pers, Y. M. (2018). Cardiac complications attributed to chloroquine and hydroxychloroquine: A systematic review of the literature. Drug Saf. 41 (10), 919–931. doi:10.1007/s40264-018-0689-4
Comité de Consenso (2007). Tercer Consenso de Granada sobre Problemas Relacionados con Medicamentos (PRM) y Resultados Negativos asociados a la Medicación (RNM). Ars Pharm. (Internet) 48 (1), 5–17.
D’Andrea, E., Desai, R. J., He, M., Glynn, R. J., Lee, H., Weinblatt, M. E., et al. (2022). Cardiovascular risks of hydroxychloroquine vs methotrexate in patients with rheumatoid arthritis. J. Am. Coll. Cardiol. 80 (1), 36–46. doi:10.1016/j.jacc.2022.04.039
Desmarais, J., Rosenbaum, J. T., Costenbader, K. H., Ginzler, E. M., Fett, N., Goodman, S., et al. (2021). American College of rheumatology white paper on antimalarial cardiac toxicity. Arthritis Rheumatology 73 (12), 2151–2160. doi:10.1002/art.41934
Egeli, B. H., Sparks, J. A., Kim, A. H. J., and Liew, J. W. (2021). Hydroxychloroquine for the treatment of COVID-19 and its potential cardiovascular toxicity: Hero or villain? Best. Pract. Res. Clin. Rheumatol. 35 (1), 101658. doi:10.1016/j.berh.2020.101658
Eveleens Maarse, B. C., Graff, C., Kanters, J. K., van Esdonk, M. J., Kemme, M. J. B., In 't Veld, A. E., et al. (2022). Effect of hydroxychloroquine on the cardiac ventricular repolarization: A randomized clinical trial. Br. J. Clin. Pharmacol. 88 (3), 1054–1062. doi:10.1111/bcp.15013
Faselis, C., Zeng-Treitler, Q., Cheng, Y., Kerr, G. S., Nashel, D. J., Liappis, A. P., et al. (2021). Cardiovascular safety of hydroxychloroquine in US veterans with rheumatoid arthritis. Arthritis & Rheumatology. 73 (9), 1589–1600. doi:10.1002/art.41803
Favalli, E. G., Biggioggero, M., Crotti, C., Becciolini, A., Raimondo, M. G., and Meroni, P. L. (2019). Sex and management of rheumatoid arthritis. Clin. Rev. Allergy & Immunol. 56 (3), 333–345. doi:10.1007/s12016-018-8672-5
Felson, D. T., Anderson, J. J., and Meenan, R. F. (1990). The comparative efficacy and toxicity of second-line drugs in rheumatoid arthritis results of two metaanalyses. Arthritis Rheum. 33 (10), 1449–1461. doi:10.1002/art.1780331001
Fries, J. F., Williams, C. A., Ramey, D., and Bloch, D. A. (1993). The relative toxicity of disease-modifying antirheumatic drugs. Arthritis Rheum. 36 (3), 297–306. doi:10.1002/art.1780360303
Gunja, N., Roberts, D., McCoubrie, D., Lamberth, P., Jan, A., Simes, D. C., et al. (2009). Survival after massive hydroxychloroquine overdose. Anaesth. Intensive Care 37 (1), 130–133. doi:10.1177/0310057X0903700112
Kerekes, G., Nurmohamed, M. T., González-Gay, M. A., Seres, I., Paragh, G., Kardos, Z., et al. (2014). Rheumatoid arthritis and metabolic syndrome. Nat. Rev. Rheumatol. 10 (11), 691–696. doi:10.1038/nrrheum.2014.121
Lee, T. C., Senecal, J., Hsu, J. M., and McDonald, E. G. (2021). Ongoing citations of a retracted study involving cardiovascular disease, drug therapy, and mortality in COVID-19. JAMA Intern Med. 181 (11), 1535–1537. doi:10.1001/jamainternmed.2021.4112
Liu, D., Li, X., Zhang, Y., Kwong, J. S. W., Li, L., Zhang, Y., et al. (2018). Chloroquine and hydroxychloroquine are associated with reduced cardiovascular risk: A systematic review and meta-analysis. Drug Des. Devel Ther. 12, 1685–1695. doi:10.2147/DDDT.S166893
Lo, C. H., Wei, J. C. C., Wang, Y. H., Tsai, C. F., Chan, K. C., Li, L. C., et al. (2021a). Hydroxychloroquine does not increase the risk of cardiac arrhythmia in common rheumatic diseases: A nationwide population-based cohort study. Front. Immunol. 12, 631869. doi:10.3389/fimmu.2021.631869
Lo, C. H., Wang, Y. H., Tsai, C. F., Chan, K. C., Li, L. C., Lo, T. H., et al. (2021b). Association of hydroxychloroquine and cardiac arrhythmia in patients with systemic lupus erythematosus: A population-based case control study. PLoS One 16 (5), e0251918. doi:10.1371/journal.pone.0251918
Mackenzie, A. H. (1983). Antimalarial drugs for rheumatoid arthritis. Am. J. Med. 75 (6), 48–58. doi:10.1016/0002-9343(83)90474-6
Majewski, D., Majewska, K. A., Naskręcka, M., and Grygiel-Górniak, B. (2021). Chloroquine and hydroxychloroquine – safety profile of potential COVID-19 drugs from the rheumatologist’s perspective. Ann. Agric. Environ. Med. 28 (1), 122–126. doi:10.26444/aaem/127766
Mehra, M. R., Desai, S. S., Ruschitzka, F., and Patel, A. N. (2020). RETRACTED:Hydroxychloroquine or chloroquine with or without a macrolide for treatment of COVID-19: A multinational registry analysis. Lancet 395 (10240), 1820. doi:10.1016/S0140-6736(20)31180-6
Messant, I., Jérémie, N., Lenfant, F., and Freysz, M. (2004). Massive chloroquine intoxication: Importance of early treatment and pre-hospital treatment. Resuscitation 60 (3), 343–346. doi:10.1016/j.resuscitation.2003.11.007
Mittal, L., Zhang, L., Feng, R., and Werth, V. P. (2018). Antimalarial drug toxicities in patients with cutaneous lupus and dermatomyositis: A retrospective cohort study. J. Am. Acad. Dermatol 78 (1), 100–106. doi:10.1016/j.jaad.2017.09.061
Naranjo, C. A., Busto, U., Sellers, E. M., Sandor, P., Ruiz, I., Roberts, E. A., et al. (1981). A method for estimating the probability of adverse drug reactions. Clin. Pharmacol. Ther. 30 (2), 239–245. doi:10.1038/clpt.1981.154
Paliani, U., and Cardona, A. (2020). COVID-19 and hydroxychloroquine: Is the wonder drug failing? Eur. J. Intern Med. 78, 1–3. doi:10.1016/j.ejim.2020.06.002
Peponis, V., Kyttaris, V. C., Chalkiadakis, S. E., Bonovas, S., and Sitaras, N. M. (2010). Ocular side effects of anti-rheumatic medications: What a rheumatologist should know. Lupus 19 (6), 675–682. doi:10.1177/0961203309360539
Pharmaceutical Care Research Group (2006). Pharmaceutical care research group, university of Granada (Spain) pharmacotherapy follow-up: The dader method (3rd revision: 2005). Pharm. Pract. (Granada) 4 (1), 44–53.
Plantone, D., and Koudriavtseva, T. (2018). Current and future use of chloroquine and hydroxychloroquine in infectious, immune, neoplastic, and neurological diseases: A mini-review. Clin. Drug Investig. 38 (8), 653–671. doi:10.1007/s40261-018-0656-y
Prevoo, M. L. L., Van’T Hof, M. A., Kuper, H. H., Van Leeuwen, M. A., Van De Putte, L. B. A., and Van Riel, P. L. C. M. (1995). Modified disease activity scores that include twenty-eight-joint counts development and validation in a prospective longitudinal study of patients with rheumatoid arthritis. Arthritis Rheum. 38 (1), 44–48. doi:10.1002/art.1780380107
Reddy, V. G., and Sinna, S. (2000). Chloroquine poisoning: Report of two cases. Acta Anaesthesiol. Scand. 44 (8), 1017–1020. doi:10.1034/j.1399-6576.2000.440821.x
Romano, S., Salustri, E., Ruscitti, P., Carubbi, F., Penco, M., and Giacomelli, R. (2018). Cardiovascular and metabolic comorbidities in rheumatoid arthritis. Curr. Rheumatol. Rep. 20 (12), 81. doi:10.1007/s11926-018-0790-9
Rosenbaum, J. T., Mount, G. R., Youssef, J., and Lin, P. (2016). New perspectives in rheumatology: Avoiding antimalarial toxicity. Arthritis Rheumatology 68 (8), 1805–1809. doi:10.1002/art.39719
Rúa-Figueroa, I., Rúa-Figueroa, D., Pérez-Veiga, N., Anzola, A. M., Galindo-Izquierdo, M., Calvo-Alén, J., et al. (2022). Antimalarials exert a cardioprotective effect in lupus patients: Insights from the Spanish Society of Rheumatology Lupus Register (RELESSER) analysis of factors associated with heart failure. Semin. Arthritis Rheum. 52, 151946. doi:10.1016/j.semarthrit.2021.11.012
Sabater Hernadez, D., Silva Castro, M., and Faus Dader, M. J. (2007). Dader method: Guidelines for pharmacotherapy follow-up. 3. Granada: Pharmaceutical care research group. Granada: University of Granada.
Saldarriaga Rivera, L. M., Fernández Ávila, D., Bautista Molano, W., Jaramillo Arroyave, D., Bautista Ramírez, A. J., Díaz Maldonado, A., et al. (2020). Recommendations on the management of adult patients with rheumatic diseases in the context of SARS-CoV-2/COVID-19 infection. Colombian Association of Rheumatology. Reumatol. Clin. Engl. Ed. 27 (3), 230–241. doi:10.1016/j.rcreue.2020.10.001
Schrezenmeier, E., and Dörner, T. (2020). Mechanisms of action of hydroxychloroquine and chloroquine: Implications for rheumatology. Nat. Rev. Rheumatol. 16 (3), 155–166. doi:10.1038/s41584-020-0372-x
Smolen, J. S., Aletaha, D., and McInnes, I. B. (2016). Rheumatoid arthritis. Lancet 388 (10055), 2023–2038. doi:10.1016/S0140-6736(16)30173-8
Smolen, J. S. (2016). Treat-to-target as an approach in inflammatory arthritis. Curr. Opin. Rheumatol. 28 (3), 297–302. doi:10.1097/BOR.0000000000000284
Sorour, A. A., Kurmann, R. D., Shahin, Y. E., Crowson, C. S., Achenbach, S. J., Mankad, R., et al. (2021). Use of hydroxychloroquine and risk of heart failure in patients with rheumatoid arthritis. J. Rheumatol. 48 (10), 1508–1511. doi:10.3899/jrheum.201180
Souza Botelho, M., Bolfi, F., Leite, R. G. O. F., Leite, M. S. F., Banzato, L. R., Soares, L. T., et al. (2021). Systematic review and meta-analysis of the safety of chloroquine and hydroxychloroquine from randomized controlled trials on malarial and non-malarial conditions. Syst. Rev. 10 (1), 294–19. doi:10.1186/s13643-021-01835-x
U.S. National Library of Medicine (2022). Clinical trials hydroxychloroquine and COVID-19 studies. [Internet]. Available at: https://clinicaltrials.gov/ct2/home. https://clinicaltrials.gov/ct2/results?cond=COVID-19&term=hydroxychloroquine&cntry=&state=&city=&dist= (Accessed 11 2, 2022).
van der Woude, D., and van der Helm-van Mil, A. H. M. (2018). Update on the epidemiology, risk factors, and disease outcomes of rheumatoid arthritis. Best. Pract. Res. Clin. Rheumatol. 32 (2), 174–187. doi:10.1016/j.berh.2018.10.005
Vitte, J., Michel, M., Mezouar, S., Diallo, A. B., Boumaza, A., Mege, J. L., et al. (2020). Immune modulation as a therapeutic option during the SARS-CoV-2 outbreak: The case for antimalarial aminoquinolines. Front. Immunol. 11, 2159–15. doi:10.3389/fimmu.2020.02159
White, N. J. (2007). Cardiotoxicity of antimalarial drugs. Lancet Infect. Dis. 7, 549–558. doi:10.1016/S1473-3099(07)70187-1
Wong, A. O. T., Gurung, B., Wong, W. S., Mak, S. Y., Tse, W. W., Li, C. M., et al. (2021). Adverse effects of hydroxychloroquine and azithromycin on contractility and arrhythmogenicity revealed by human engineered cardiac tissues. J. Mol. Cell Cardiol. 153, 106–110. doi:10.1016/j.yjmcc.2020.12.014
Keywords: pharmacovigilance, antimalarials, rheumatoid arthritis, drug-related side effects, cardiotoxicity
Citation: Santos-Moreno P, Ibatá L, Martínez S, Rodríguez-Vargas G-S, Villarreal L, Rodríguez P, Rivero W, Rodríguez-Florido F and Rojas-Villarraga A (2023) Adverse events in rheumatoid arthritis patients under antimalarial treatment—Is there cardiovascular compromise?. Front. Drug Saf. Regul. 2:1044696. doi: 10.3389/fdsfr.2022.1044696
Received: 14 September 2022; Accepted: 23 December 2022;
Published: 09 January 2023.
Edited by:
Luis J. Jara, Independent Researcher, Mexico City, MexicoReviewed by:
Efe Eworuke, United States Food and Drug Administration, United StatesCopyright © 2023 Santos-Moreno, Ibatá, Martínez, Rodríguez-Vargas, Villarreal, Rodríguez, Rivero, Rodríguez-Florido and Rojas-Villarraga. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Pedro Santos-Moreno, cGVkcm9zYW50b3Ntb3Jlbm9AaG90bWFpbC5jb20=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.