 Giada Crescioli1,2†
Giada Crescioli1,2† Marco Finocchietti3†Silvia Cascini3Olga Paoletti4David Franchini5Emiliano Cappello6Giulia Valdiserra6
Marco Finocchietti3†Silvia Cascini3Olga Paoletti4David Franchini5Emiliano Cappello6Giulia Valdiserra6 Francesco Sciancalepore7
Francesco Sciancalepore7 Maria Grazia Celani8
Maria Grazia Celani8 Marco Tuccori6,9
Marco Tuccori6,9 Alfredo Vannacci1,2
Alfredo Vannacci1,2 Niccolò Lombardi1,2*‡Ursula Kirchmayer3‡ the CAESAR Study Group
Niccolò Lombardi1,2*‡Ursula Kirchmayer3‡ the CAESAR Study Group Antonio AddisAntonio AncidoniIlaria BacigalupoAnna Maria BargagliValeria BelleudiRoberto BonaiutiPaola BrunoriGiampaolo BucaneveTeresa Anna CantisaniSilvia CasciniMaria Grazia CelaniIrma ConvertinoGiada CrescioliMarco FinocchiettiRosa GiniGiulia HyeraciUrsula KirchmayerNiccolò LombardiOlga PaolettiRosalba Elisabetta RocchiMariangela RossiFrancesco SciancaleporeMarco TuccoriNicola VanacoreAlfredo Vannacci
Antonio AddisAntonio AncidoniIlaria BacigalupoAnna Maria BargagliValeria BelleudiRoberto BonaiutiPaola BrunoriGiampaolo BucaneveTeresa Anna CantisaniSilvia CasciniMaria Grazia CelaniIrma ConvertinoGiada CrescioliMarco FinocchiettiRosa GiniGiulia HyeraciUrsula KirchmayerNiccolò LombardiOlga PaolettiRosalba Elisabetta RocchiMariangela RossiFrancesco SciancaleporeMarco TuccoriNicola VanacoreAlfredo Vannacci- 1Department of Neurosciences, Psychology, Drug Research and Child Health, Section of Pharmacology and Toxicology, University of Florence, Florence, Italy
- 2Tuscan Regional Centre of Pharmacovigilance, Florence, Italy
- 3Department of Epidemiology, Latium Regional Health Service, Rome, Italy
- 4Regional Health Agency of Tuscany, Pharmacoepidemiology Unit, Florence, Italy
- 5Health ICT Service, Regional Health Authority of Umbria, Perugia, Italy
- 6Department of Clinical and Experimental Medicine, Unit of Pharmacology and Pharmacovigilance, University of Pisa, Pisa, Italy
- 7National Center for Disease Prevention and Health Promotion, Italian National Institute of Health, Rome, Italy
- 8Neurophysiopathology Unit, Perugia Hospital, Perugia, Italy
- 9Unit of Adverse Drug Reaction Monitoring, University Hospital of Pisa, Pisa, Italy
Background: This analysis describes the use of riluzole in amyotrophic lateral sclerosis (ALS) individuals with contraindications and off-label use for subjects with other motor neuron diseases (o-MND) in the Italian regions of Latium, Tuscany and Umbria.
Methods: A cohort of adults with ALS prescribed with riluzole during the years 2016–2019 was enrolled from administrative healthcare databases, excluding subjects with o-MND in the preceding 5 years. Being affected by ALS for more than 5 years, presence of tracheostomy, renal or hepatic failure were considered as contraindications to the use of riluzole. A cohort of adults with o-MND was enrolled in 2016–2019 for whom off-label use of riluzole was retrieved up to 4 years, analysing over the time differences related to sex.
Results: Among 206 ALS individuals prescribed with riluzole in Latium, 336 in Tuscany and 60 in Umbria, less than 1% were diagnosed with ALS for more than 5 years. Less than 2% were tracheotomised or affected by hepatic failure. Renal failure was documented for 1.9%, 2.7%, and 5.0% of ALS individuals in Latium, Tuscany and Umbria. The o-MND cohort comprised 264 subjects in Latium, 222 in Tuscany, and 66 in Umbria. Non-negligible off-label riluzole use was observed: 8.5%, 33.0%, and 4.2% in females, and 19.9%, 26.5% and 2.4% in males in Latium, Tuscany and Umbria.
Discussion: Riluzole use in ALS individuals in the presence of contraindications is rare, with slightly higher numbers in presence of renal failure. Off-label use in o-MND was found to be non-negligible, with variations between sexes.
Introduction
Riluzole is a drug indicated to improve survival and time free from invasive mechanical ventilation (or tracheostomy) in individuals with amyotrophic lateral sclerosis (ASL). Although the pathogenesis of ALS is not completely elucidated, recent advancements in ALS research suggest that genetic and/or environmental factors would be involved at some stage of the neurodegeneration of motor neurons, with the important contribution of many mechanisms to the manifestation of the disease, including mitochondrial dysfunction, dysfunction of axonal transport, toxic protein aggregation and propagation, impaired protein degradation systems, excitatory, oxidative stress, decreased neurotrophic support from neuronal cells, and RNA toxicity. Among them, glutamate-induced excitotoxicity is considered to play an important role for cell death in the disease.
Riluzole is proposed to act by inhibiting glutamate processes. Nevertheless, there is no evidence that riluzole exerts a therapeutic effect on motor function, lung function, fasciculations, muscle strength and motor symptoms (Andrews et al., 2020).
A Cochrane Systematic Review published in 2012 recommended the use of riluzole in individuals with probable and definite ALS who had a history of disease shorter than 5 years, and no history of tracheostomy. Riluzole 100 mg daily is reasonably safe, prolonging median survival by about 2–3 months in subjects with ALS (Miller et al., 2012). Andrews et al., in 2020 reported a review regarding the real-world evidence of riluzole effectiveness in treating ALS. This review indicates that riluzole treatment may extend survival by 6–19 months, which is substantially longer than the 2–3 months of survival benefit reported in clinical trials (Andrews et al., 2020). Moreover, clinical trials demonstrated that riluzole is generally safe and well tolerated, and there is little evidence for a difference in adverse events (AEs) rate between riluzole and placebo. The most frequently reported serious AEs are increased liver enzymes, nausea, vomiting, weakness, tachycardia, sedation, headache, dizziness, and paresthesia (Saitoh and Takahashi, 2020).
In ALS, riluzole use is contraindicated in the presence of renal and/or hepatic impairment, after tracheostomy, or in patients with an ALS history of more than 5 years, and during pregnancy and breastfeeding (EMA, 2016). In the latter stages of ALS, a medication review to evaluate the opportunity to discontinue treatment should be considered. Riluzole has been investigated in probable and definite ALS and for this reason should not be used in individuals with any other form of motor neuron diseases (o-MNDs). In this case, a riluzole-based treatment in o-MNDs can be defined as off-label use. Treatment with riluzole should only be started by a neurologist with experience in the management of MNDs (EMA, 2016).
To date, there are no drug utilisation studies investigating the pattern of riluzole use in a real-world setting in Italy, thus, this brief analysis describes the use of riluzole in ALS adult individuals with contraindications and its off-label use for adults with o-MND in the Italian regions of Latium, Tuscany and Umbria.
Material and methods
Data sources
This is a descriptive, retrospective cohort study, part of a multiregional Italian pharmacovigilance project on the comparative effectiveness and safety of drugs used in rare neuromuscular and neurodegenerative diseases (CAESAR project).
This brief analysis was performed on regional administrative healthcare data of three Italian regions (Latium, Tuscany, Umbria). Data referred to the years 2011–2019. The study protocol was registered on the EU PAS Register (EUPAS37983).
In Italy, healthcare is tax-funded and issues services to all residents, who are enrolled in the healthcare registries, covering around 95% of the population. Non-enrolment mainly refers to healthy young or middle-aged persons who can afford private medical care, whereas chronic patients are typically covered. For this population, all healthcare services issued by public or affiliated providers are recorded at an individual level. Specifically, administrative healthcare databases provide information regarding: 1) healthcare assistance (demographic and residence information registered in the regional health service, i.e., date, place, and cause of death, coded according to ICD-9-CM); 2) hospital discharge records (information regarding discharge from hospitals, i.e., primary and secondary diagnoses and procedures recorded at discharge, coded according to ICD-9-CM); 3) emergency department (ED) visits (i.e., up to five diagnoses coded according to ICD-9-CM, patient severity, triage code, and clinical parameters); 4) co-payment exemptions for patients with a confirmed diagnosis of a chronic or acute condition; 5) reimbursed drugs intended for outpatient use (coded according to the international Anatomical Therapeutic Chemical Classification System (ATC), claim date, number of pills).
All databases can be linked through an anonymous unique patient identifier, to create patient level records containing all information available in the different administrative registries, in line with the Italian privacy legislation.
Study population
The enrolment period covered the years 2016–2019, while the years 2011–2015 were needed to allow for a 5-year look-back period at the index date for all cohort members. Two different cohorts of subjects were considered.
The first cohort included individuals with a record of ALS from 1 January 2016, to 31 December 2019 (cohort A). Subjects were included if any of the following criteria was retrieved from the regional administrative databases: diagnosis of ALS from hospital discharge (primary diagnosis: ICD-9-CM 335.20); diagnosis of ALS from hospital discharge (secondary diagnosis: ICD-9-CM 335.20), with hospital discharge from neurology ward; ALS specific co-payment exemption (code RF0100); diagnosis of ALS from ED visits (primary diagnosis: ICD-9-CM 335.20). The date of the first signal was defined as the index date. Subjects were excluded if they met any of the following criteria: less than 5-year look-back period from the index date; no dispensing of riluzole (ATC code: N07XX02) after the index date and before 31 December 2019; dispensing of riluzole during the 5-year look-back period; diagnosis of o-MND (from hospital discharge or ED visits: ICD-9-CM 335.2, excl. 335.20); co-payment exemption codes of o-MND (i.e., codes RF0110, RF0390, RFG050) in the 5-year look-back period; age <18 years at index date; not resident/registered with a general practitioner in any of the regions of interest at index date.
The second cohort included individuals affected by o-MND (cohort B), namely progressive muscular atrophy, progressive bulbar palsy pseudobulbar palsy, primary lateral sclerosis, and all other motor neuron diseases. Subjects were included if any of the following criteria was retrieved from the regional administrative databases from 1 January 2016, to 31 December 2019: diagnosis of o-MND from hospital discharge (primary diagnosis: ICD-9-CM 335.2, excl. 335.20; diagnosis of o-MND from hospital discharge (secondary diagnosis: ICD-9-CM 335.2, excl. 335.20), with hospital discharge from neurology ward; o-MND specific co-payment exemption (i.e., codes RF0110, RF0390, RFG050); diagnosis of o-MND from ED visits (primary diagnosis: ICD-9-CM 335.2, excl. 335.20). The date of the first signal was defined as the index date. Subjects were excluded if they met any of the following criteria: less than 5-year look-back from the index date; prescriptions of riluzole in the 5-year look-back period; diagnosis of ALS (from hospital discharge or ED visits: ICD-9-CM 335.20) or co-payment exemption (code RF0100) in the 5-year look-back period; age <18 years at index date; not resident/assisted at index date.
Study outcomes
The use of riluzole in the presence of contraindications in individuals affected by ALS was identified according to its therapeutic indications (EMA, 2016). The occurrence of any of the following conditions in ALS individuals (cohort A) at first riluzole prescription was considered: more than 5 years from first diagnosis of ALS to first riluzole (ATC N07XX02) prescription; occurrence of any record of tracheostomy in the 5-year look-back period (ICD-9-CM codes 51900, 51901, 51902, 51909, V440, V550); occurrence of any record of impairment of renal function in the 5-year look-back period (ICD-9-CM codes 582, 583, 585, 586, 587 for chronic renal insufficiency; 250.4, 250.40, 250.41, 250.42, 250.43 for diabetic nephropathy; 403.xx, 404.xx for hypertensive nephropathy; 572.4, 580.xx, 584.xx, 580.0, 580.4, 580.89, 580.9, 582.4, 791.2, 791.3 for acute renal failure; 274.10, 440.1, 442.1, 453.3, 581.xx, 593.xx, 753.0, 753.3, 866.00, 866.01, 866.1 for other renal diseases); occurrence of any record of liver function impairment in the 5-year look-back period (ICD-9-CM codes 571, 570, 572, 573, 070, except 573.0).
The off-label use of riluzole, defined as its use in individuals affected by o-MND (cohort B), was also investigated.
Statistical analysis
The analysis of riluzole prescribing in the presence of contraindications in ALS individuals (cohort A) was performed, identifying any signal of one of the defined contraindications during the 5-year look-back period for every cohort member from administrative health data. For each specific contraindication, occurrence was calculated in terms of the number of subjects with at least one signal during the look-back period (numerator) in relation to the cohort of new riluzole users (denominator), and is presented in absolute numbers and percentages, stratified by region.
Off-label riluzole prescribing in individuals with o-MND (cohort B) was analysed, retrieving riluzole prescriptions after the index date of o-MND diagnosis throughout the end of 2019. Occurrence was calculated as the proportion of riluzole users in terms of at least one riluzole claim (numerator) with respect to the o-MND cohort (denominator), expressed in absolute numbers and percentages, stratifying by region, sex, and year of enrolment.
The present analysis is part of a research project (“CAESAR”) which will also investigate efficacy and safety of riluzole use in ALS patients. For this analysis we will use multivariate COX regression models, including sensitivity analysis. Regarding the ALS cohort, we have run a validation study which evaluated sensitivity and specificity of the algorithm we used to identify ALS patients from administrative data, and found good levels of both. This validation study is part of another scientific article on ALS incidence and prevalence which is currently on its way and will hopefully be published soon.
Results
Overall, 1,890 ALS individuals were identified. Applying the exclusion criteria, resident adults with incident ALS (cohort A), not affected by o-MND, and newly prescribed with riluzole after the index date accounted for 206 subjects in Latium, 336 in Tuscany, and 60 in Umbria, respectively (Table 1). In Latium and Umbria individuals were more frequently males. Mean age varied between 65.9 and 70.6 years at index date, reflecting the different characteristics of resident population in the three Italian regions. Riluzole was only sporadically prescribed for ALS in the presence of contraindications across the participating regions. Less than 1% had a recorded history of ALS of more than 5 years, less than 2% had undergone tracheostomy or were affected by liver impairment. Renal failure was documented for 1.9%, 2.7%, and 5.0% of ALS individuals in Latium, Tuscany, and Umbria, respectively (Table 2).
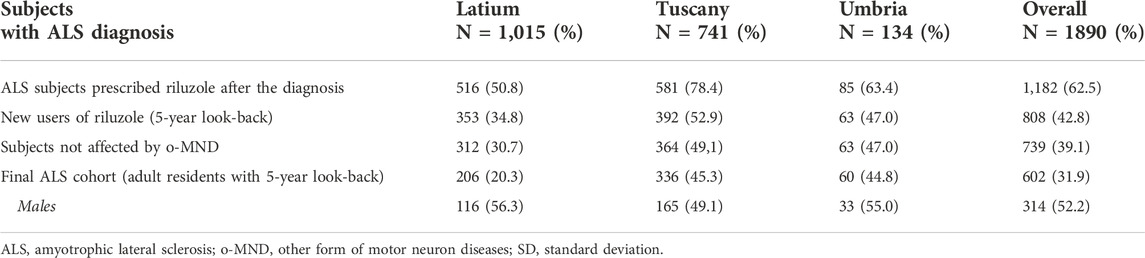
Table 1. The ALS cohorts in the three Italian regions (years 2016–2019).
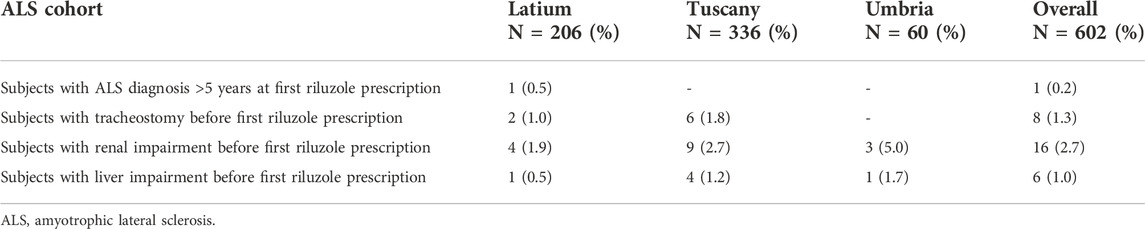
Table 2. Riluzole prescribing in presence of contraindications in the ALS cohort by region.
In the three regions, a total number of 1,230 subjects with o-MND were retrieved (cohort B). The cohorts contributing to our analysis included 264 individuals in Latium, 222 in Tuscany, and 66 in Umbria (Table 3). There was a higher proportion of males in all regions, and mean age was 58 3 years.

Table 3. The o-MND cohorts in the three Italian regions (years 2016–2019).
Off-label use of riluzole in o-MND individuals was observed, with differences between the three regions and sexes. Prevalence of riluzole use was 8.5% in females and 19.9% in males in Latium, 33.0% in females and 26.5% in males in Tuscany, and 4.2% in females and 2.4% in males in Umbria. Analysing time trends over the 4-year study period, prevalence of off-label riluzole use was generally stable, except in Tuscany, where some fluctuation was registered, ranging between 17.9% and 34.4% for males, and 26.7% and 50.0% for females (Figure 1).
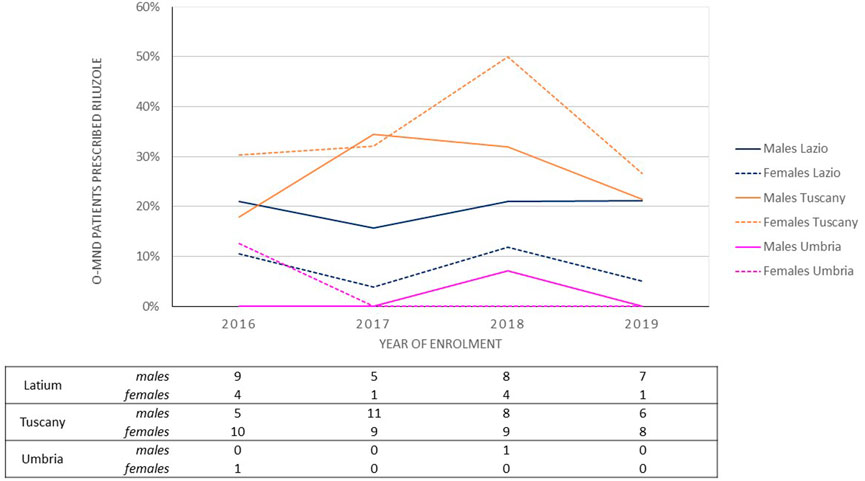
Figure 1. Off-label riluzole prescribing in o-MND subjects: proportions by region, sex and year of enrolment.
Discussion
Our data show that riluzole use in individuals with a diagnosis of ALS is generally in line with therapeutic indications. Riluzole therapy was only sporadically started in the presence of a contraindication, as more than 5 years from disease onset, after tracheostomy or in the presence of liver impairment, indicating that riluzole use in the Italian clinical practice can be considered as appropriate and safe as possible. A slightly higher but still modest use was observed in subjects suffering from renal impairment. Differences between the three regions included in the analysis are small and due to very small numbers are hard to interpret. However, this is the first drug utilisation study describing the pattern of riluzole use in a real-world setting in Italy, with a specific focus on its therapeutic indications.
Regarding the off-label use of riluzole to treat o-MND, for which riluzole is not officially authorised in Italy, we detected a non-negligible number of cases. This may certainly be explained to some extent by the absence of a therapeutic alternative for these conditions. Differences observed may be partly due to variations of drug policies or clinical guidelines over time and between regions, given that regional health authorities oversee reimbursement regulations for drugs in Italy (Prada et al., 2017). From a clinical point of view, these findings are of exceptional relevance to avoid safety problems potentially associated with the use of riluzole out of its therapeutic indications in neurology.
Even if evidence regarding the on- and off-label use of riluzole in clinical practice is scarce, some studies attempted to analyse its utilisation patterns. In the scientific literature there are some international studies that have already reported information regarding the use of riluzole in clinical practice. Nevertheless, no one reported information on the use of riluzole in presence of contraindications and/or its use in an off-label regimen. A descriptive observational retrospective study performed in Lisbon, characterised the use of riluzole in 77 ALS patients (63% men). Overall, the study estimated a mean adherence of 91.2% and a median survival of 10.1 months. Tracheostomy was registered in four patients (5%), but no information regarding riluzole withdrawal were reported in the paper (Paróla et al., 2018). A nationwide retrospective cohort study conducted in Sweden between 2007 and 2013 evaluated the use of prescription drugs over the course of the last year of life in older adults affected by ALS (Grande et al., 2017). Riluzole was found among the five most used active principles during the final months before death. On a total of 1,603 older adults (51.2% men; mean age 76.5 years), authors found a significant increase in the prescription of riluzole during the last year of life (26.7% at 12th month, 37.9% at 6th month, and 45.0% at final month). This pattern of use can be explained by riluzole efficacy in extending life or the time free from mechanical ventilation in patients with ALS. However, no information on the time from diagnosis of ALS, contraindications (i.e., liver or renal impairment), and tracheostomy were provided by the authors, making their analysis difficult to compare with our results.
A real-world cohort study published by Chen L. and colleagues in 2016 investigated the efficacy of riluzole in patients with sporadic ALS (Chen et al., 2016). Among 1,540 patients, 415 were administered with riluzole, 252 (60.7%) males. Authors observed that the prognosis of patients treated with a cumulative defined daily dose≥ 16,800 mg was significantly better than that of patients treated with lower doses of riluzole and better than that of patients not exposed to this medication. No information regarding the use of riluzole in presence of contraindication or of its off-label use was provided.
A descriptive cross-sectional study was conducted in Colombia in 2017 to determine the prescription pattern of riluzole in a population of patients with MND (Calvo-Torres et al., 2021). In the Colombian General Social Security Health System database, a total of 81 ALS patients receiving riluzole were found (48.1% men; mean age 60.8 years). Although the authors reported that 63% of ALS individuals were receiving medicines that reflect the presence of comorbidities, specific information on concomitant conditions were not retrievable from their analysis. In fact, comedication was used as a surrogate indicator of chronic disease. In this context, it could be very difficult to evaluate the use of riluzole in this subset, based on its contraindications.
Another study published in the United States in 2020 (Vu et al., 2020) monitored patients’ characteristics, utilisation and safety of edaravone cycles and riluzole use. This propensity score–matched cohort study used data on 369 patients with documented definite or probable ALS and compared edaravone (alone or with riluzole) with riluzole only. 71.3% of patients enrolled received edaravone with riluzole, while 669 patients used riluzole only. Among riluzole users, 97% were males. Tracheostomy was registered for 16 patients in the riluzole users group, along with 182 cases of death, and 35 cases of hospitalisation. Only 17 riluzole users recovered to mechanical ventilation. Also in this case, the off-label use of riluzole was not considered by the authors.
In his analysis (Kim, 2017), Yong-Jin Kim demonstrated that, in Ontario (Canada), riluzole prescriptions were influenced by the patient's age, moderate and moderate-severe cognitive impairment, marital status, and geographical locations. The majority of riluzole users were married males, more than 56 years old. The analysis demonstrated that the receipt of riluzole reduced the hazard of death and hospitalisation by 14%. Information on comorbidities, tracheostomy and/or other contraindications were not available.
In summary, in the last decade, several population-based studies from real-world settings were published on clinical ALS databases. All of them suggested significant enhancement of survival in riluzole-treated ALS individuals compared to those who did not receive riluzole with the effect most notable in patients who started the medication early in the disease (Hinchcliffe and Smith, 2017). Unfortunately, most of these real-world studies focused their analysis only on the efficacy of riluzole, not reporting direct information useful to better characterise its use in clinical practice, particularly in terms of contraindications in ALS patients and off-label use in o-MNDs. Consequently, the safety of riluzole use in the aforementioned clinical settings is still understudied.
Strengths and limitations
Several limitations of our study must be noted. In particular, they may derive from the use of administrative data sources. In fact, claims data could be associated with the risk of underestimation with respect to drug prescribing or retrieval of chronic conditions, such as renal or liver impairments. Consequently, we may have underestimated the phenomenon of riluzole prescribing in presence of contraindications in ALS. This may also have influenced the detection of patients affected by o-MNDs and treated with riluzole. Furthermore, due to the lack of information regarding individual doses prescribed to patients, it was not possible to investigate whether doses were reduced in patients with liver and renal impairment. Additionally, another important limitation could be represented by the lack of information on concomitant diseases and medications, thus not allowing us to investigate both the presence of potential drug-disease and drug-drug interactions, which may have somehow influenced the use of riluzole in this subset. More details about the other medications would also be helpful to understand the clinical complexity of subjects affected by ALS in Italy. Finally, for subjects diagnosed with ALS for more than 5 years, information regarding the onset of contraindications and the start of riluzole prescriptions were not considered. All these limitations may have different impacts in the three regions, because traceability of drug claims depends on the administrative procedures underlying drug registration under different reimbursement policies (Prada et al., 2017). Moreover, drugs administered to in-patients are generally not retrievable at patient level. On the contrary, our analysis is the only one that provided real-world data on the use of riluzole in ALS individuals considering for each subject the time from ALS diagnosis, presence of tracheostomy, liver and/or renal impairment, thus allowing us to better evaluate the use of riluzole in presence of contraindications. Furthermore, its off-label use was also described in o-MND individuals, making this analysis the first one of its kind.
Conclusion
This descriptive analysis highlights that riluzole use in ALS individuals in the presence of contraindications is rare in the 3 Italian regions, with slightly greater use in the presence of renal failure, especially in Umbria. Off-label riluzole use in o-MND was found to be non-negligible, with variations between sexes and regions. Our observations may be partially explained by the lack of specific disease modifying medications in o-MND, and differences between regional health policies.
Larger population-based studies are recommended to determine the use of riluzole in real-life conditions, improving our knowledge on both its patterns and safety of use in different clinical settings. In a next step, we will address the question whether riluzole can increase survival even in tracheostomies or in those who have been diagnosed for over 5 years.
CAESAR study group
Antonio Addis, Antonio Ancidoni, Ilaria Bacigalupo, Anna Maria Bargagli, Valeria Belleudi, Roberto Bonaiuti, Paola Brunori, Giampaolo Bucaneve, Teresa Anna Cantisani, Silvia Cascini, Maria Grazia Celani, Livia Convertino, Giada Crescioli, Marco Finocchietti, Rosa Gini, Giulia Hyeraci, Ursula Kirchmayer, Niccolò Lombardi, Olga Paoletti, Rosalba Elisabetta Rocchi, Mariangela Rossi, Francesco Sciancalepore, Marco Tuccori, Nicola Vanacore, Alfredo Vannacci
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Author contributions
Study design was contributed by GC, MF, MT, AV, NL, and UK, with assistance from the rest of the authors. MF and UK took the lead in data analysis. Data interpretation was performed by GC, MF, MT, AV, NL, and UK, with assistance from the other authors. The manuscript was written primarily by GC, MF, NL, and UK, with assistance from the other authors, and revised by all authors. All authors approved the final version of the manuscript.
Funding
This study is co-funded by a research grant from the Italian Medicines Agency (AIFA) in the multiregional pharmacovigilance call 2012-13-14. The funder of the study had no role in the collection, analysis, and interpretation of data, nor in the writing of the report, nor in the decision to submit the article for publication.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Andrews, J. A., Jackson, C. E., Heiman-Patterson, T. D., Bettica, P., Brooks, B. R., and Pioro, E. P. (2020). Real-world evidence of riluzole effectiveness in treating amyotrophic lateral sclerosis. Amyotroph. Lateral Scler. Front. Degener. 21, 509–518. doi:10.1080/21678421.2020.1771734
Calvo-Torres, L. F., Vera-Polania, F., Ayala-Torres, J. D., Solano-Atehortua, J. M., and Machado-Alba, J. E. (2021). Prescription patterns of riluzole in a population of patients with motor neuron disease. Acta Neurol. Colomb. 37, 57–62. doi:10.22379/24224022367
Chen, L., Liu, X., Tang, L., Zhang, N., and Fan, D. (2016). Long-term use of riluzole could improve the prognosis of sporadic amyotrophic lateral sclerosis patients: A real-world cohort study in China. Front. Aging Neurosci. 8, 246. doi:10.3389/fnagi.2016.00246
EMA (2016). Rilutek, annex I - summary of product characteristics. Available at: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/viewer.html?pdfurl=https%3A%2F%2Fwww.ema.europa.eu%2Fen%2Fdocuments%2Fproduct-information%2Frilutek-epar-product-information_en.pdf&clen=316213&chunk=true (Accessed March 24, 2022).
Grande, G., Morin, L., Vetrano, D. L., Fastbom, J., and Johnell, K. (2017). Drug use in older adults with amyotrophic lateral sclerosis near the end of life. Drugs Aging 34, 529–533. doi:10.1007/s40266-017-0469-3
Hinchcliffe, M., and Smith, A. (2017). Riluzole: Real-world evidence supports significant extension of median survival times in patients with amyotrophic lateral sclerosis. Degener. Neurol. Neuromuscul. Dis. 7, 61–70. doi:10.2147/dnnd.s135748
Kim, Y.-J. (2017). Cost effectiveness analysis of riluzole for ALS in Ontario home care setting. Available at: chrome-extension://efaidnbmnnnibpcajpcglclefindmkaj/viewer.html?pdfurl=https%3A%2F%2Fuwspace.uwaterloo.ca%2Fbitstream%2Fhandle%2F10012%2F12038%2FKim_Yong-Jin.pdf%3Fsequence%3D3&clen=1691891 (Accessed March 24, 2022).
Miller, R. G., Mitchell, J. D., and Moore, D. H. (2012). Riluzole for amyotrophic lateral sclerosis (ALS)/motor neuron disease (MND). Cochrane Database Syst. Rev. 2012 (3), CD001447. doi:10.1002/14651858.cd001447.pub3
Paróla, A., de Palhares Falcão, F. D. S. M., Farinha, H., Caetano, A., Santos, L., Medeiros, E., et al. (2018). Analysis of riluzole’s profile of use in a central hospital in Lisbon. Patient prefer. Adherence 12, 2357–2361. doi:10.2147/PPA.S167861
Prada, M., Ruggeri, M., Sansone, C., de Fazio, D., Tettamanti, A., and Mantovani, M. (2017). Timeline of authorization and reimbursement for oncology drugs in Italy in the last 3 years. Med. Access @ Point Care 1, maapoc.0000007. doi:10.5301/maapoc.0000007
Saitoh, Y., and Takahashi, Y. (2020). Riluzole for the treatment of amyotrophic lateral sclerosis. Neurodegener. Dis. Manag. 10, 343–355. doi:10.2217/nmt-2020-0033
Keywords: riluzole, amyotrophic lateral sclerosis, cohort study, off-label, clinical practice, neurology
Citation: Crescioli G, Finocchietti M, Cascini S, Paoletti O, Franchini D, Cappello E, Valdiserra G, Sciancalepore F, Celani MG, Tuccori M, Vannacci A, Lombardi N, Kirchmayer U and the CAESAR Study Group (2022) Riluzole use in presence of contraindications in adults affected by amyotrophic lateral sclerosis and its off-label use in other motor neuron diseases: Findings from an Italian multicentre study (the CAESAR project). Front. Drug Saf. Regul. 2:1041275. doi: 10.3389/fdsfr.2022.1041275
Received: 10 September 2022; Accepted: 13 October 2022;
Published: 25 October 2022.
Edited by:
Jeff Guo, University of Cincinnati, United StatesReviewed by:
Guillermo Alberto Keller, Universidad de Buenos Aires, ArgentinaKhaled Alamri, University of Cincinnati, United States
Copyright © 2022 Crescioli, Finocchietti, Cascini, Paoletti, Franchini, Cappello, Valdiserra, Sciancalepore, Celani, Tuccori, Vannacci, Lombardi, Kirchmayer and the CAESAR Study Group. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Niccolò Lombardi, bmljY29sby5sb21iYXJkaUB1bmlmaS5pdA==
†These authors share first authorship
‡These authors share last authorship