 Marina A. Malikova1,2*
Marina A. Malikova1,2* Gianluca Trifirò3
Gianluca Trifirò3 Giorgio Racagni4Dennis Van Liew5Peggy Webster6Tejal S. Brahmbhatt1,2
Giorgio Racagni4Dennis Van Liew5Peggy Webster6Tejal S. Brahmbhatt1,2- 1Department of Surgery, School of Medicine, Boston University, Boston, MA, United States
- 2Boston Medical Center, Boston, MA, United States
- 3Department of Diagnostics and Public Health, University of Verona, Verona, Italy
- 4Department of Pharmacological and Biomolecular Sciences, Faculty of Pharmacy, University of Milan, Milan, Italy
- 5Red Nucleus, Waltham, MA, United States
- 6Glaxo SmithKline, Cambridge, MA, United States
Introduction
When the first cases of what would become the COVID-19 pandemic occurred in late 2019, many would not have predicted the massive widespread impact the pandemic would have. According to the European Centre for Disease Prevention and Control, as of 16 June 2020 there were 8,000,847 reported cases of COVID-19 globally with a breakdown of 3,907,668 cases from the Americas, 2,202,063 cases from Europe and 1,630,329 cases from Asia (European Centre). (European Centre for Disease Prevention and Control, 2020). With accelerated drug development timelines, vaccines have been developed to combat propagation of the virus. Originally, in the absence of a vaccine or cure, public health measures such as social distancing and contact tracing helped to flatten the case curve but even these were not sufficient. (Matrajt and Leung, 2020). Therefore, one of the options employed involved the accelerated repurposing of already approved drugs, mostly based on potential scientific evidence by an understanding of mechanisms of action. However, in the race to discover an already approved treatment which may also be effective in treating COVID-19 patients, it is important to note that the known safety profile of pharmacological treatments is an essential component of the risk-benefit assessment fundamental to decision-making.
Central to this is creating a contentious approach for any institution to how emerging information will be understood and applied. With modern day advances of communication, information can literally be transmitted and disseminated instantaneously within global medical community. On a down side, this creates an uncontrolled avalanche of information that could be misinterpreted and misused. Institutional leadership needs to be organized in a manner to best utilize the available resources, namely experts in basic science and the clinical care.
An appointed team which can critically review the onslaught of emerging literature is essential. Social and journal media should be reviewed with a critical eye as they can be rooted and driven by sensationalistic stories that in actuality do not bear any actionable clinical information. One of the key components that became very apparent during the early days of the COVID-19 pandemic was the poor implementation of the understanding of correlative versus causative data. Deciphering relevancy is important. Identifying information that is simply correlative is important so that incorrect assertions and conclusions do not drive institutional changes to combat a disease that has just begun to be understood.
Using an approved drug for an unapproved indication, off-label use, when there is some evidence that the drug may work, is not a new practice in the healthcare setting (FDA, 2018 Understanding unapproved). The large numbers of COVID-19 cases not only placed stress on Health Care Providers and the healthcare system, but was exacerbated by the rapid progression of the disease. Additionally, the increased proliferation of conflicting and sometimes confusing information created a sense of helplessness for both Health Care Providers and patients, a situation worsened by a sense of fear, uncertainty and desperation. In this state of urgency, and with the increased use of off-label medications for COVID-19, the Hippocratic aphorism of “first do no harm” is critical. (Stevenson, 1994). As the COVID-19 pandemic progresses, data is constantly evolving and various approved medications will continue to be tested for their efficacy in treating COVID-19. Some of the more recent medications being used off-label or for emergency use in COVID-19 include hydroxychloroquine, chloroquine, azithromycin and remdesivir. (Rosenberg et al., 2020).
Systems approach to drug repurposing
Systems thinking implies the ability and skills to perform problem solving in complex systems such as healthcare organizations. (Reason, 1990; Reason, 1997). This approach involves expanding boundaries of the problem one is trying to solve beyond one healthcare provider, service, clinic, or department to the entire healthcare system. (Wachter, 2013). Implications of changes on decision making and subsequent actions versus unintended consequences should be taken into account. (Wachter, 2013). The elements of the existing organizational structure (e.g. hospital’s formal policies and procedures, performance measures, rewards system, information availability and visibility, informal practices and cultural norms, mental models) must be considered when implementing systemic changes. The core strategies to optimize system shifting to drug repurposing should include the following elements: collaboration, innovation, and data-driven decision making (e.g. estimating safety stock pile of drugs/pharmaceutical supplies needed based on average usage on a monthly basis).
For drug repurposing, existing medications were utilized and algorithms needed to be developed quickly to ensure that proper drugs were dispensed based on specific symptoms. In ongoing pandemic pharmacies’ and hospitals’ experiences, significant contracts with a “just in time” supplies concept were employed when many hospitals in the US had only limited amount of supplies on the premises. (Wysocki and Lueck, 2006). Diversification of the shortage of medications risks can be achieved by shifting ordering/sourcing strategies form single supplier to multiple suppliers and looking into substitutes (i.e. using generics or biosimilars instead of innovator products). Developing flexible infrastructure to be more agile in healthcare service delivery, building cross functional teams with pharmacy input, and forecasting of supplies/drugs needed is critical for successful execution of drug repurposing protocols in the public health emergency state.
Looking at drug repurposing through the lens of a “systems approach” has allowed us to derive lessons learned that are worth mentioning:
• Independence between parties involved can lead to forming silos. Optimization of system’s performance on the organizational level rather than optimization of individual, separate parts/processes needs be considered and implemented.
• It is a non-linear process as small changes can have large effects.
• It is difficult to trace results of actions due to delays between the actions and measurable outcomes, and changes of practices can have unintended consequences (i.e. lack of efficacy of repurposed medication, new safety concern/adverse drug reaction).
• Points of leverage—consider upstream factors on organizational level to reinforce repurposing of drugs.
• Apply for federal and state grants to cover costs in emergency situations.
• Take into account conditions/requirements for reimbursements/payments for medications and services delivered by insurance carriers in value-based healthcare environment. (Wachter et al., 2008).
• Holistic systematic approach to patient monitoring/assessments, building treatment algorithms with repurposed drugs, complexity of operating system, taking into account social determinants of health (i.e. technical and social aspects).
Institutional response to the need for drug repurposing
As mentioned above, conscientious, streamlined approach is necessary on institutional or organizational level to properly perform drug repurposing that is equitable, safe, and insures quality assessment. Key stakeholders are important to identify (Figure 1). Leadership should include a governing clinician. This clinician, ideally, already holds an institutional leadership role, such as a chief medical officer or chief operations officer. The panel should then include clinicians and pharmacists who will be involved directly in the care of these patients (Figure 1). These clinicians and pharmacists should have a demonstrated track of being able to critically review the emerging literature and offer a non-biased assessment of any pharmaceutical agents that could be repurposed.
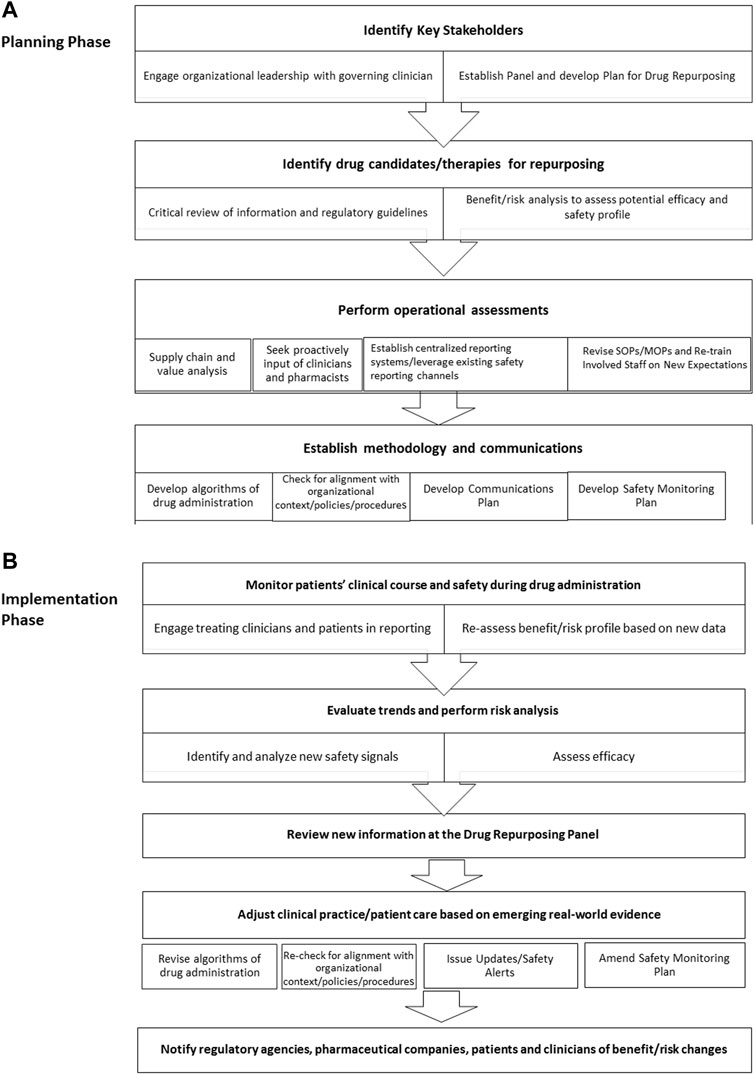
Figure 1. Establishing process for patient safety monitoring and risk/benefit assessments for drug repurposing for treatment of COVID-19 during healthcare emergency should roll out in phases; and involve engagement of key stakeholders, assessment of resources/supply channels, evaluation of drug candidates for repurposing and effective utilization of communication modalities.
COVID-19 pandemic highlighted further importance of healthcare access. Social factors, which have tremendous influence on patient care should be emphasized in the decision making process. These factors can guide development of relevant algorithms of medical treatment and policies, and also they should be promoted as high priority.
Based on information available (e.g. published literature, package inserts, individual case studies, real-world evidence, safety databased) the panel assesses and reviews potential efficacy for condition/disease to treat with re-purposed drugs, discuss safety profiles, perform risk assessments and establish risk/benefit ratios for new indications. Once agents have been identified, supplements to this panel should include supply chain officers and value-analysis analysists to provide institutional perspectives (Figure 1).
Once agents have been vetted and supply/availability understood, the panel should return to the table to create an algorithm for administration within the learned institutional/organizational context (Figure 1). Once approved, multiple modalities of communication need to be identified and utilized to disseminate the repurposing plan. Communication modalities can include (but not exclusively) email, internal media, individual departmental correspondences, and centrally accessible internal electronic repositories. Additional methods can include work modules to insure that designated clinicians understand the decided upon process, indications, and system set up for the repurposed drug. Mindfulness should be heeded that unorganized information overload can be detrimental to the dissemination of correct and up-to-date information.
Shared decision making
As with the case of any therapy, studies have demonstrated that the model of shared decision making engages the patient in their own care, empowers them to make decisions on treatment modalities that directly impact their health, and allows for a more appropriate set of expectations form the patient about their recovery. One such model that is widely utilized is a three step process popularized by (Elwyn et al., 2012). In the case of repurposed pharmaceuticals for off label use, this involves introducing a choice in therapy, then describing the options and what is understood to be the benefits of the repurposing with what is known about the risks in the drug profile, and then helping the patients explore the preferences within the context of their own goals. This approach would further enhance compliance and trust with the clinician given so many unknowns about a disease such as COVID-19 and its possible treatments.
Discussion
Pharmacovigilance after implementation
The pharmacovigilance discipline plays a crucial role in the expedient evaluation of new uses for existing therapies and enhances public health. In addressing the previously mentioned medications from a pharmacovigilance perspective, it is first important to understand the medication’s already established safety profile in its approved indications. Secondly, consistent monitoring of new safety data is integral in adequately determining the benefit-risk profile for off-label use of some therapies. For example, in the case of hydroxychloroquine and azithromycin, both drugs have been available on the market for years and both individually have, among other known safety risks, the labeled cardiovascular side effect of QT prolongation (FDA Highlights of prescribing information Zithromax, Hydroxychloroquine Sulfate tablets). (Food and Drug Administration (US), 2019; Food and Drug Administration (US), 2017). Thus, when administered as a combination treatment, which was done in several COVID-19 cases, the cardiovascular risk can be compounded. This synergistic effect was made evident in a retrospective multicenter study highlighted by the American College of Cardiology which found the “combination of hydroxychloroquine and azithromycin was associated with higher risk of cardiac arrest”. (Rosenberg et al., 2020). With this in mind, continued monitoring of emerging safety data will be paramount in making a definite conclusion on the use of hydroxychloroquine/chloroquine (plus azithromycin) in COVID-19.
As more data are generated for off-label and emergency use of medications for COVID-19, the data science engagement could be more emphasized in pharmacovigilance as a key factor for future pandemic responses. As Real World Data (RWD) and Real World Evidence (RWE) (e.g. data from Electronic Health Records/EHR systems) become increasingly utilized in drug safety monitoring, the need for more mature technical and methodological approaches in pharmacovigilance should also be emphasized. Noteworthy, based on the experience of COVID-19 pandemic, international data registries played a key role for policy decision making and we would expect them to be even more important in public health emergencies and/or future pandemics. However, utilization of RWD for PV purposes is still evolving, and more effort is required in the technical infrastructure availability and methodology to more fully mature acceptance of this approach.
Monitoring modalities need to be established prior to rolling out any form of repurposing. These need to involve a direct line of accessibility to patient care. Clinicians need to be involved to help organize and roll-out how information will be reported. Some institutions have implemented direct monitoring panels which monitor a patient’s clinical course during the administration of repurposed medications and their clinical progress afterwards. This would require resources that certain institutions may not have. Additionally, resource limited institutions could consider utilizing already in place electronic infrastructure where clinicians can report adverse events electronically that is then cataloged and monitored by the supervisory panel that decided on a drug’s original repurposing.
Pharmacovigilance will also play an important role by establishing close partnerships between drug regulatory agencies, healthcare professionals and pharmaceutical companies to provide real-time safety data through expedited safety reporting and other safety monitoring activities. This has been particularly important in the case of remdesivir which was granted Emergency Use Authorization for COVID-19 by the FDA on 1 May 2020 (FDA issues emergency use authorization, FDA News Release, Emergency use authorization (EUA)). (EUA, 2019; Food and Drug Administration (US), 2020b; FDA, 2020). Remdesivir is an investigational drug initially designed for hepatitis C and respiratory syncytial virus which was later studied in Ebola but did not prove to be as efficacious as other treatments (Gilead). (Gilead, 2020). Although remdesivir has been approved for Emergency Use in COVID-19, the safety profile was not well-established and the only known side effects at the time or repurposing, as reported in the approved indication, include infusion related reactions and increases in liver enzymes (FDA Fact sheet for patients). (Food and Drug Administration (US), 2020a). Thus, it has been critical that safety data from all possible sources be shared in a timely manner to ensure that any potential serious risks are identified and assessed promptly to ensure patient safety and prevent widespread harm.
In conclusion, as more data emerges during this pandemic, one can presume other medications for off-label use in COVID-19 will have been identified. Therefore, it is important that increased attention and awareness is created regarding drug safety and the potential harm these medications may have on an individual and re-affirm the critical role of pharmacovigilance expertise.
Author contributions
All authors listed have made a substantial, direct, and intellectual contribution to the work and approved it for publication.
Conflict of interest
PW: International Society of Pharmacovigilance (ISOP)/ NASoP member and employee of Glaxo SmithKline (GSK), Cambridge, MA, USA.; GT: Professor of Pharmacology, University of Verona, Italy. Member of the Italian Society of Pharmacology (SIF); DVL: International Society of Pharmacovigilance (ISOP)/NASoP member and partner at Red Nucleus.; GR: Department of Pharmacological and Biomolecular Sciences, University of Milan. Member of the Italian Society of Pharmacology (SIF).
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Elwyn, G., Frosch, D., Thomson, R., Joseph-Williams, N., Lloyd, A., Kinnersley, P., et al. (2012). Shared decision making: A model for clinical practice. J. Gen. Intern. Med. 27 (10), 1361–1367. doi:10.1007/s11606-012-2077-6
EUA (2019). Emergency use authorization (EUA) for remdesivir, an unapproved product center for drug evaluation and research (CDER) review. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/nda/2020/EUA%20Review%20Remdesivir_050120.pdf.
European Centre for Disease Prevention and Control (2020). COVID-19 situation update worldwide as of June 9th. Available at: https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases<https://www.ecdc.europa.eu/en/geographical-distribution-2019-ncov-cases>.
FDA (2020). FDA COVID-19 update: FDA broadens emergency use authorization for veklury (remdesivir) to include all hospitalized patients for treatment of COVID-19. August. Available at: https://www.fda.gov/news-events/press-announcements/covid-19-update-fda-broadens-emergency-use-authorization-veklury-remdesivir-include-all-hospitalized.
Food and Drug Administration (US) (2018). Understanding unapproved use of approved drugs “off label”. US Food and Drug Administration. Available at: https://www.fda.gov/patients/learn-about-expanded-access-and-other-treatment-options/understanding-unapproved-use-approved-drugs-label.
Food and Drug Administration (US) (2020). Coronavirus (COVID-19) update: FDA issues emergency use authorization for potential COVID-19 treatment. US Food and Drug Administration. Available at: https://www.fda.gov/news-events/press-announcements/coronavirus-covid-19-update-fda-issues-emergency-use-authorization-potential-covid-19-treatment.
Food and Drug Administration (US) (2020). Fact sheet for patients and parent/caregivers emergency use authorization (EUA) of remdesivir for coronavirus disease 2019 (COVID-19). US Food and Drug Administration. Available at: https://www.fda.gov/media/137565/download<https://www.fda.gov/media/137565/download>.
Food and Drug Administration (US) (2019). Highlights of prescribing information Zithromax US. Food and Drug Administration. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2019/050710s049,050711s047,050784s034lbl.pdf.
Food and Drug Administration (US) (2017). Hydroxychloroquine sulfate tablets, USP. US; Food and drug administration; nov. Available at: https://www.accessdata.fda.gov/drugsatfda_docs/label/2020/040133Orig1s029,%20s030lbl.pdf.
Gilead (2020). Development, Gilead.of remdesivir gilead. Available at: https://www.gilead.com/-/media/gilead-corporate/files/pdfs/covid-19/gilead_rdv-development-fact-sheet-2020.pdf.
Matrajt, L., and Leung, T. (2020). Evaluating the effectiveness of social distancing interventions to delay or flatten the epidemic curve of coronavirus disease. Emerg. Infect. Dis. 26 (8), 1740–1748. doi:10.3201/eid2608.201093
Reason, J. T. (1997). Managing the risks of organizational accidents. Aldershot, Hampshire: Ashgate.
Rosenberg, E., Dufort, E., Udo, T., Wilberschied, L., Kumar, J., Tesoriero, J., et al. (2020). Association of treatment with hydroxychloroquine or azithromycin with in-hospital mortality in patients with COVID-19 in New York State. JAMA2020 323 (24), 2493–2502. doi:10.1001/jama.2020.8630
Stevenson, D. (1994). Aphorisms: The Internet classic archives. Available at: http://classics.mit.edu/.
Wachter, R. M., Foster, N. E., and Dudley, R. A. (2008). Medicare's decision to withhold payment for hospital errors: The devil is in the det. Jt. Comm. J. Qual. Patient Saf. 34, 116–123. doi:10.1016/s1553-7250(08)34014-8
Wachter, R. M. (2013). Personal accountability in healthcare: Searching for the right balance. BMJ Qual. Saf. 22, 176–180. doi:10.1136/bmjqs-2012-001227
Wysocki, B., and Lueck, S. (2006). Just-in-Time inventories make U.S. Vulnerable in a pandemic. New York, NY: Dow Jones and Company, a division of News Corp. Available at: https://www.wsj.com/articles/SB113703203939544469.
Keywords: patient safety, systems approach, drug repurposing, emergency medical use, off-label medication use
Citation: Malikova MA, Trifirò G, Racagni G, Van Liew D, Webster P and Brahmbhatt TS (2022) Establishing patient safety monitoring in the benefit-risk paradigm for off-label and emergency use of medications for COVID-19: A pharmacovigilance perspective. Front. Drug Saf. Regul. 2:1038235. doi: 10.3389/fdsfr.2022.1038235
Received: 06 September 2022; Accepted: 29 September 2022;
Published: 26 October 2022.
Edited by:
Sengwee Toh, Harvard Medical School and Harvard Pilgrim Health Care Institute, United StatesReviewed by:
Pantelis Natsiavas, Centre for Research and Technology Hellas, GreeceCopyright © 2022 Malikova, Trifirò, Racagni, Van Liew, Webster and Brahmbhatt. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Marina A. Malikova, bW1hbGlrb3ZAYnUuZWR1