 Elia Msegu1
Elia Msegu1 Eveline Konje2
Eveline Konje2 Teckla Tupa1
Teckla Tupa1 Namanya Basinda3*Mlemile S. Gwimile1Teddy Ngallaba4Fredy Marwa5
Namanya Basinda3*Mlemile S. Gwimile1Teddy Ngallaba4Fredy Marwa5- 1Weill-Bugando School of Medicine, Catholic University of Health and Allied Sciences, Mwanza, Tanzania
- 2Department of Epidemiology and Biostatistics, Catholic University of Health and Allied Sciences, Mwanza, Tanzania
- 3Department of Community Medicine, Catholic University of Health and Allied Sciences, Mwanza, Tanzania
- 4Department of Social Science, Wesley College, Mwanza, Tanzania
- 5Tanzania Health Promotion Support, Dar-es-salaam, Tanzania
Introduction: Community Health Workers (CHWs) are the first contact between the community and health services in multiple rural areas in Tanzania. Therefore, Community Health Workers are set to play a crucial role in emergencies and disasters. This cross-sectional study assessed the readiness of CHWs in Itilima concerning preventing the spread of COVID-19.
Methods: A total of 190 CHWs and 30 stakeholders were interviewed using quantitative and qualitative methods, respectively. Multivariate linear regression model was used for quantitative data while thematic analysis was used for qualitative data.
Results: The study revealed that 140/190 (73%) CHWs had adequate knowledge of COVID-19, with 126/190 (66.32%) after receiving on-job training on COVID-19. There was no association between demographic characteristics and CHWs' knowledge of COVID-19. In-depth interviews (IDIs) highlighted that the majority of the CHWs were equipped with PPEs and other working tools to aid their role in response to COVID-19. Challenges such as incentive inadequacy and insufficient working tools were among the major setbacks highlighted by the CHWs during the IDIs.
Conclusion: CHWs appear to be adaptable and provide relevant feedback thus can take part in emergencies and disasters when capacity building is done.
Background
Human resources for health in Tanzania, as it is in most African countries, is a major constraint to service delivery. Shortages of skilled health workers, particularly in underserved areas, have remained a key facet of the growing human resource crisis (1). In most sub-Saharan African countries with most of the population constituting rural communities, the first health personnel contact is the Community Health Care Workers (CHWs) (2). CHWs are one of the strategies proposed to address the health worker crisis in this setting (3). They provide a range of health promotion activities and act as a link between communities and health facilities (4, 5). Studies show the success of CHWs in addressing health problems at the community level. CHWs have been shown to contribute to reductions in child morbidity and mortality, increase immunization uptake, promote breastfeeding, and improve outcomes for tuberculosis patients and children suffering from acute respiratory infection or malaria (6).
Disasters and medical emergencies can happen in any country without any warning. Due to globalization, the spread of disease from country to country is fast. This is a case of the COVID-19 pandemic. Since the first case of COVID-19 was discovered In November 2019, in Wuhan, China, it was declared a Public Health Emergency of International Concern on 30th January 2020 and a global pandemic by 22nd March 2020 (7, 8). All countries took multiple steps in facing the pandemic. However, countries like Tanzania face challenges including inadequate workforce in healthcare (1, 2). In Tanzania, it is estimated that the workforce available is only half of the required number (1). To this end, CHWs were involved in multiple tasks from case identification to guiding home care for clients with COVID-19. CHWs provide a range of health promotion activities and act as a link between communities and health facilities (2, 5, 9, 10). Therefore, this study assessed whether CHWs are well-equipped with enough knowledge, have a positive attitude, and are willing to take up roles in the fight prevention of the spread of COVID-19 as an example of an emergency.
Methods
This study was carried out in the Itilima district Simiyu region. Itilima District, covering 4,690 km2 (1,810 sq mi), is one of the five districts in Simiyu that hosts part of the Serengeti National Park (11). It is bordered to the North by Bariadi District, the East by Ngorongoro District, the South by Maswa District and Meatu District, and the West by Magu District. Its population as of the 2022 census was 313,900 (12). The district has 102 villages with 361 CHWs working in the area.
This was a community-based cross-sectional study. Data collection included qualitative and quantitative methods to allow for triangulation and enhance the strength of the findings in the study particularly the readiness of CHWs to take part in emergencies (13). A representative sample of 190 Community Healthcare Workers (CHWs) was selected for quantitative data collection, calculated using the Yamane Taro formula from the total of 361 CHWs in the district. A list of CHWs was generated from the CHWs district coordinator, then the first CHW was selected by lottery, and every 2nd CHW from the list was recruited until the sample size was reached. A total of 30 Key Informant Interviews (KIIs) were done, a sufficient number to reach saturation (14, 15). The KIIs included the Council Health Management Team members, CHW supervisors, and local community leaders.
A questionnaire and interview guide for quantitative and qualitative approaches were developed using questions from related studies. They were then reviewed by three experts who looked at the contents of the questions and made recommendations. The tools were developed in English and then translated into Swahili. They were back-translated by another person conversant in both languages to ensure no loss to translation. The tools were pretested in Nyamagana district to sort out wording issues or difficult questions; thus, the questions were examined to see if they could measure what they were meant to measure. Tape recorders were used to collect qualitative data while quantitative data were collected using Open Data Kit (ODK) Collect.
Quantitative data analysis and processing were done through IBM SPSS statistics version 20 computer program. Categorical data were tabulated and their frequencies and percentages were computed. For the variables where the association was to be computed p-values were calculated. The variables with p-values below 0.05 were to be considered statistically significant.
Qualitative data analysis comprised several steps to ensure a comprehensive and insightful analysis. Initially, the audio recordings of interviews were transcribed verbatim. Subsequently, proficient translators conducted translations from Swahili to English, ensuring that meaning is retained. Familiarization with the data was done, involving repeated readings of the transcripts to gain a holistic understanding of the content. This immersion in the data facilitated the identification of patterns, themes, and areas of interest. Hybrid coding (that is deductive and inductive coding) strategy was applied to ensure comprehensive coding. Coding was performed by two people for the sake of quality control with the assistance of qualitative data analysis software (NVIVO 12). The development of themes came after coding. Commonalities and connections between different codes were identified, and similar codes were grouped to form broader themes. Major theme categories were reviewed numerous times by two social scientists to ensure that classification was adequate. Thematic coding allowed the two social scientists to undertake a grounded analysis. This hybrid approach allowed the data to direct the progression of the intended and emergent themes. Data analysis used explicit, systematic, and reproducible methods hence, validation and trustworthiness of the findings were established and conclusions drawn were grounded in evidence (16). In the paper, we cite actual data in verbatim quotes from interviewees as a prerequisite for findings to be independently and objectively verified (16). The study informants' age, sex, occupation, and settings are provided at the end of each quotation.
Results
Sociodemographic characteristics of respondents
A total of 190 community health workers were included in the study. The mean age of the study participants was 39.5 ± 10.4 years, with a minimum and maximum age of 18 and 59 years, respectively. More than half 132/190 (69.5%) of the participants were female, and most of the participants 155/190 (81.6%) were married. A total of 165/190 (88.2%) of participants were volunteers with the rest being trained CHWs. The majority of the participants 118/190 (62.1%) had a primary level of education. Table 1 describes the demographic characteristics of the study participants.
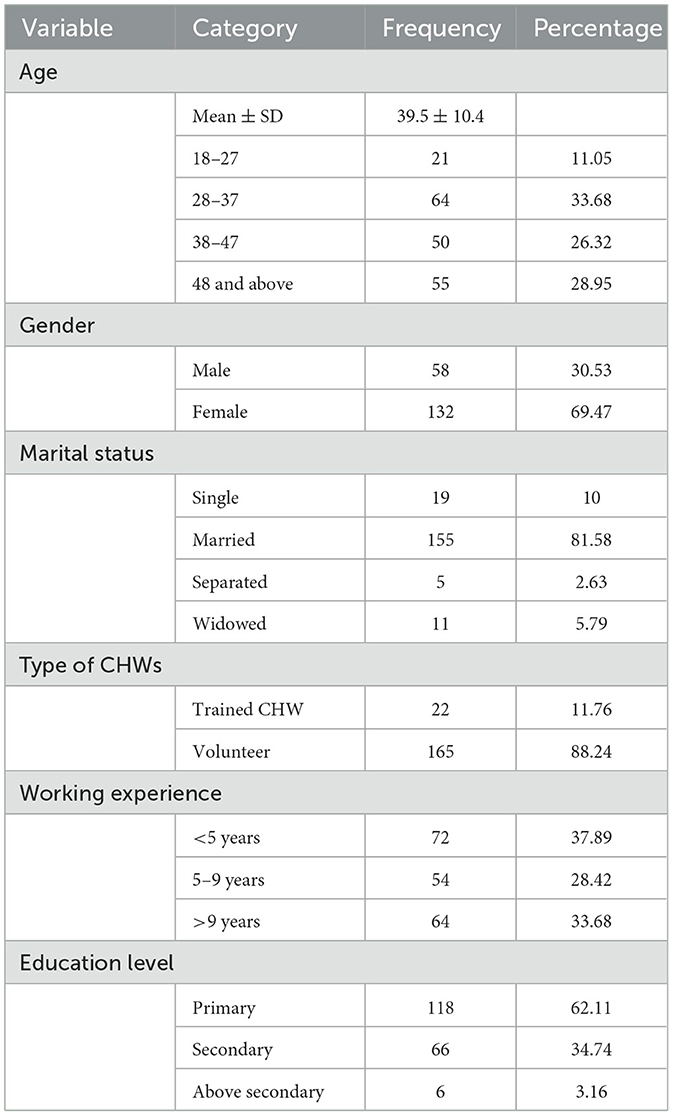
Table 1. Socio-demographic characteristics of study participants (n = 190).
Knowledge on COVID-19
More than half 140/190 (73%) health workers were knowledgeable about COVID-19. The response to 14 knowledge questions is summarized in Table 2. Around 98% knew that COVID-19 spreads mainly from person to person and spreads via the respiratory system (95%) and 84% had knowledge that people with respiratory conditions are at high risk if they get infected with COVID-19. However, CHWs did not answer certain questions correctly. Around 37% of CHWs responded children and young adults don't need to take preventative measures against COVID-19. Only (104/190) 54% of CHWs thought children under 10 years old are in high-risk categories of being affected by COVID-19. When asked whether warm weather would stop COVID-19, (90/190) 47% of CHWs thought so.
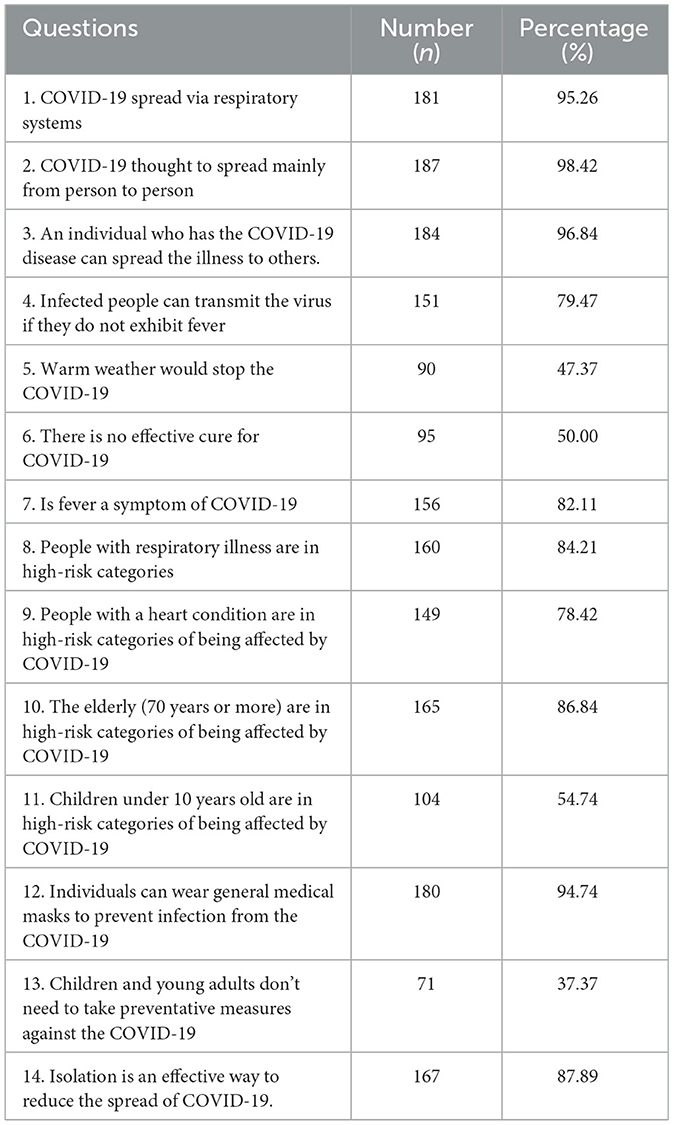
Table 2. Knowledge of COVID-19 among community health workers in Itilima district.
Preparedness
The response to 13 preparedness questions is summarized in Table 3. Around (176/190) 92% of respondents reported that supervisors took measures to keep staff informed with contemporary coronavirus information. About (170/190) 89% participated in emergency planning for COVID-19 in their community and (167/190) 87% of CHWs reported considering themselves prepared for managing the COVID-19 outbreak. On the other side (119/190) 62% of CHWs were aware of all the challenges in their community that may hinder the response to COVID-19. (126/190) 66% attended workshops or courses related to the COVID-19 outbreak and (119/190) 62% reported that PPEs are made available to them in case of contact with a COVID-19 patient.
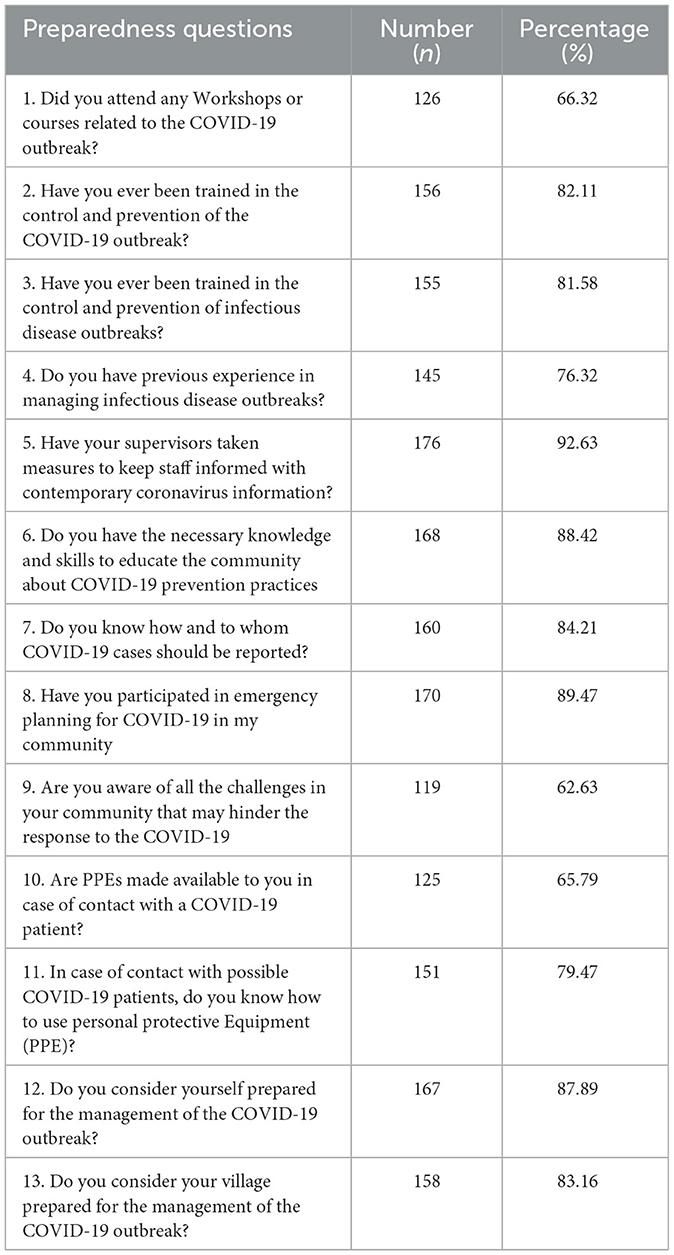
Table 3. Preparedness among CHW.
Factors associated with preparedness for COVID-19
Following univariate logistic regression to find the association between knowledge and social-demographic characteristics and between Preparedness and Social demographic characteristics, no social demographic characteristics were found to have a statistically significant association with either knowledge or preparedness as shown in Tables 4, 5, respectively.
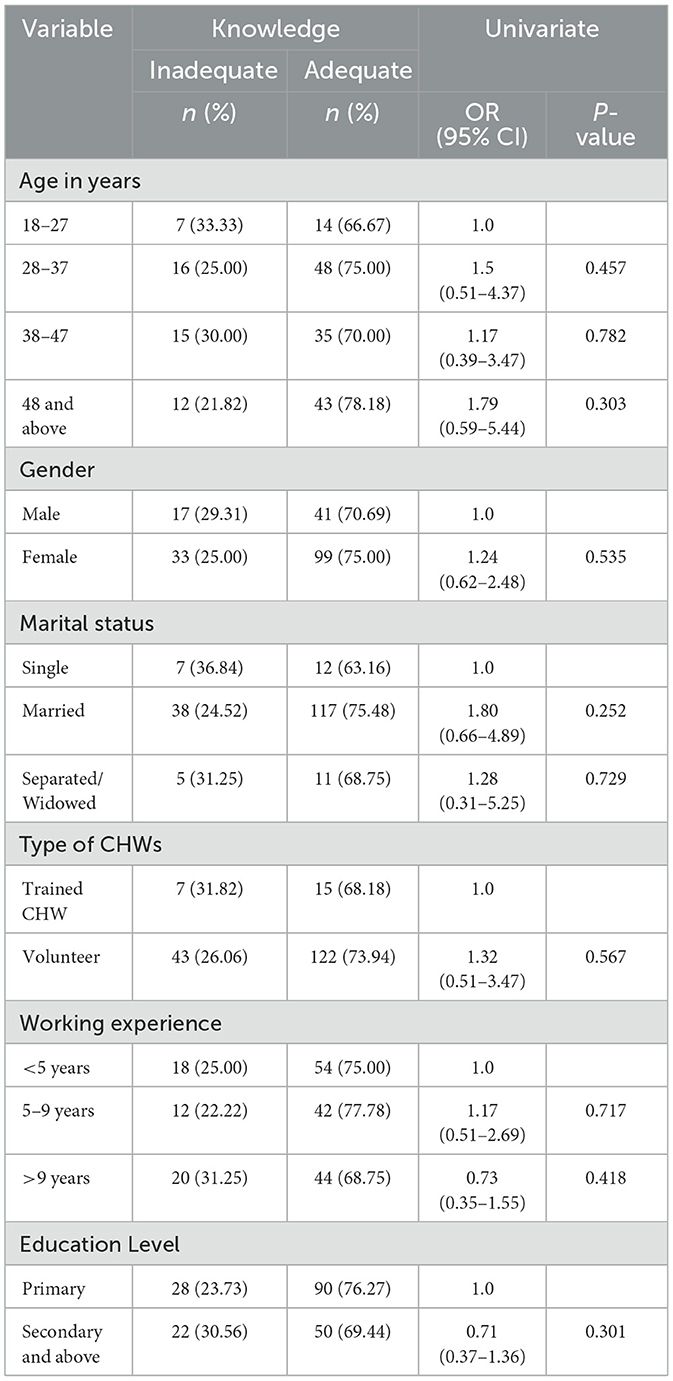
Table 4. Factors associated with knowledge of COVID-19.
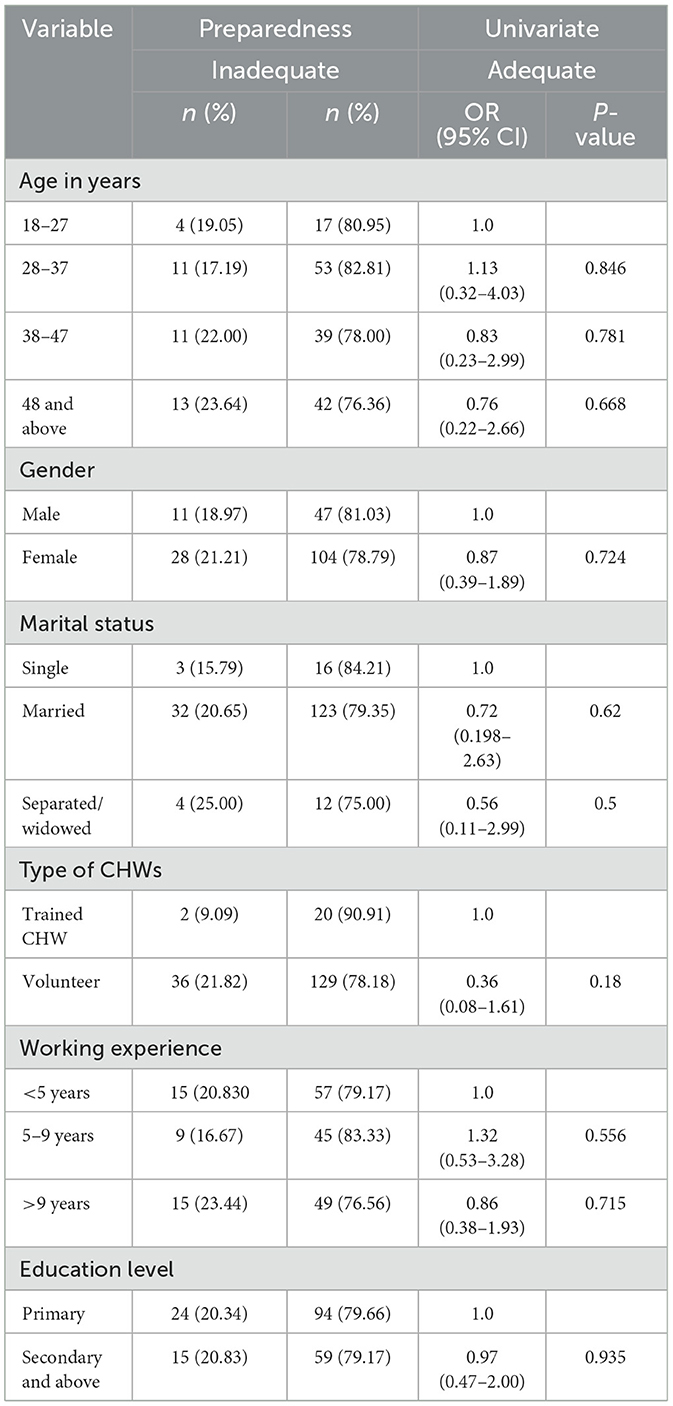
Table 5. Factors associated with preparedness for COVID-19.
Qualitative results
Thematic analysis of the interview data revealed three themes and five sub-themes as presented in Table 6.
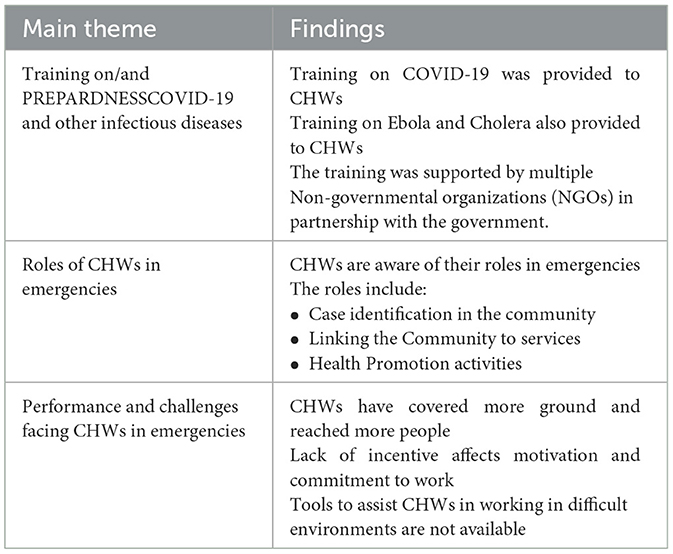
Table 6. Major themes.
Training and preparedness on COVID-19 and other infectious disease control
Most participants acknowledged that CHWs received training on response to COVID-19. This training was organized at the DMO's office with support from partners including Amref, Doctors with Africa Collegio Universitario Aspiranti Medici Missionari (CUAMM), Management and Development for Health (MDH), and Elizabeth Glaser Pediatric AIDS Foundation (EGPAF). The training focused on orienting CHWs toward prevention protocols against COVID-19. A male 72 years old respondent said, “All the CHWs were called at the DMO's office to receive training on COVID-19”. However, all CHWs have a history of being trained to recognize and report on various infectious diseases including Cholera and Ebola. A male 57 respondent reported, “CHW has received preparedness training to report on diseases such as Cholera and Ebola”. This training was provided in response to these diseases when they threatened the community.
All participants acknowledge that the training provided to CHWs was vital to helping them perform their roles. Participants are confident that CHWs have the necessary knowledge and skills to educate the community about COVID-19 preventive practices. A 57-year-old male respondent reported, “The trained CHWs have the basic knowledge and skills to educate the community about COVID-19 prevention”.
CHWs had received training on COVID-19 response activities. Most respondents shared their opinion that CHWs were prepared to respond and actively took part in their response. Working in collaboration with health facilities, they can take part in the response. A 34-year-old male respondent said, “Yes, they are prepared. The CHWs are prepared to take part in the response. They are trained and take part in the activities”.
In Itilima, CHWs have had previous experience working during an outbreak. This was in terms of a Cholera outbreak. Despite the differences in disease dynamics, working on an outbreak made the CHWs able to follow and learn outbreak protocols and procedures. A 32-year-old female respondent said, “We had a Cholera outbreak in the previous year, and CHWs participated actively in prevention strategy”.
CHWs were armored with personal protective equipment (PPE) during the COVID-19 response activities. They also received training on how to use these PPEs. This ensured their safety as they carried out their work. A 32-year-old female respondent reported, “During the pandemic, all CHWs were called for training at DMOs office. They were provided with PPEs which included masks and other items. They were also trained on proper use.”
Roles of CHWs in COVID-19 response
Participants described a vast array of roles that CHWs do as part of the COVID-19 response. These range from providing the community with health education to identifying and referring patients to health facilities for care and treatment. Other roles include encouraging handwashing and cleanliness for both hygiene improvement as well as cutting the COVID-19 transmission. A female 33-year-old respondent reported, “CHWs play a big role in linking the community to the facility by identifying cases and bringing them to the facility”. Another respondent, 26 years old male said, “The role of CHWs in the response to COVID-19 response was advocacy, health education, identification of suspects and support health care provider in vaccination activities”. Participants went on to acclaim the vital role CHWs played in increasing COVID-19 vaccine uptake. Most participants acknowledge that in the presence of CHWs, people accepted and were ready to get vaccinated than in their absence. This was because CHWs created trustworthiness of the health care services provided. A female 41-year-old participant reported, “The community trusts CHWs. When we went to provide vaccination services with CHWs, community members will only come to vaccinate if encouraged by CHWs”. This emphasizes the role CHWs play beyond just offering health services.
Further, respondents agree that CHWs know how to and can refer clients who are COVID-19 suspects to health facilities. This is an important activity in the prevention of spread and containment of the infection. A 30-year-old female respondent said, “Once they identify cases in the community, CHWs inform the facility personnel and escort the client to the facility for care. They also record and share information on the client with facility personnel for further intervention”.
Performance and challenges of COVID-19 activities in the community
All participants agree that CHWs are a key part of offering services to the community. Participants share their belief that CHWs offer a lot of services in the community. Acknowledged is the availability and willingness of CHWs to take part in health education activities. Participants note that CHWs perform this role and reach out to a lot of people to engage them in COVID-19 response including vaccination activities. A 41-year-old female respondent said, “CHWs have reached and covered great ground to provide COVID-19 education and prevention strategy. They go to places that HCWs cannot reach”. This depicts CHWs as a great arm of health services, reaching even remote communities and families.
That lack of incentive is the most highlighted issue reported by participants. All participants mentioned lack of incentive to motivate CHWs influences their desire to perform and provide services. General lack of funds from facility collections, the general district's budget leaves CHWs without any incentives in most cases.
A few other participants highlighted the lack of working tools including raincoats, boats, and torches that are relevant in working during rainy days and at night as one of the challenges facing CHWs. A female 30-year-old respondent said, “It is difficult for CHWs to offer services when called at night or during the rain because of lack of torches and raincoats or umbrellas”.
Discussion
One of the study's objectives was to assess the knowledge of CHWs regarding COVID-19. The finding from this study shows that more than half (73%) of health workers were knowledgeable about COVID-19. This is in line with other studies conducted in Nepal and Nigeria where the study showed that most participants (63.2%) and (67.4%), respectively, knew COVID-19 (17, 18). However, in this study, the authors argued that the higher knowledge contributed to higher levels of education of the participants. In this context, this argument differs from what was found in Itilima because most participants (62%) had only primary school education. The higher levels of knowledge on COVID-19 in Itilima could have contributed to the fact that CHWs received training on COVID-19 response. The training was prepared collaboratively between the DMO's office and partners especially Amref, Doctors of Africa CUAMM, MDH, and EGPAF as mentioned by participants. It was also found that CHWs have had a history of undergoing various training sessions in the past regarding infectious diseases including Cholera and Ebola.
All participants acknowledged the fact that these kinds of training sessions were vital in providing preparedness for CHWs to conduct their roles in responding to epidemics such as COVID-19. Studies show that on-the-job training has been identified as a key area to building knowledge and skills of health personnel, whilst delivering various health services (19–21). Furthermore, the role of the DMO's office in coordinating various stakeholders turned out to be vital in ensuring that the CHWs have enough knowledge related to COVID-19. This observation is evidenced by studies done in other places such as in Iran where the study shows that there are three thousand NGOs involved in controlling COVID-19 and the most important activities include training people (22).
However, this study's findings, showed that there were no social demographic characteristics were found to have a statistically significant association with knowledge. Other studies such as the one conducted by Saeed et al. (23) showed a significant association across socio-demographic characteristics such as gender, education level, marital status, and employment status. This could be because most of the participants in this study were mostly from the same locality and had comparatively similar demographic characteristics. Further, the training provided to take part in emergency responses could have influenced their level of knowledge altogether (24, 25).
The majority of the CHWs from the study through the IDIs claimed they were trained and equipped with PPEs at the same time and got similar incentives. A multicounty Interrupted Time Series Analysis shows that supported and received COVID-19 adopted protocols, training, and protective equipment were prepared for the pandemic and were able to maintain speed and coverage of community-delivered care during the pandemic period (26).
The study highlights various roles played by the CHW in response to COVID-19 these roles included providing the community with awareness regarding the pandemic, identifying and referring patients to health facilities for care and treatment, conducting COVID-19 surveillance at the community level, doing general community-based health data management where CHWs played a significant role in collecting COVID-related data at the community level and so simple analysis for sharing with the community and providing feedback to the community and distributing PPEs (especially sanitizers and soaps) to important public places such as schools and market places. These roles are consistent with other studies on the role played by the CHWs during the COVID-19 pandemic (6, 27–29).
From the study several challenges were put forward by CHWs and key informant respondents, these include little incentives available and not paid on time, lack of working and working and rain gear equipment, and the presence of few refresher pieces of training to match the dynamic trend of the COVID-19 virus. This assertion is also evidenced by other studies. The disruption of their routine work has meant less incentive-based income and may therefore, on balance, lead to income uncertainty (30). Lack of incentive or delay in paying CHWs incentives on time may hamper their performance. While they work voluntarily, incentives are an important motivation factor as evidenced by various studies (31, 32) furthermore lack of adequate working tools is consistent with other studies (33).
The study findings into the priority needs of CHWs which include the need to have clear and effective means of incentives in times such as COVID-19. This calls for local government authorities to plan well regarding CHW incentives in their Comprehensive Council Health Plans (CCHP). Additionally, CHWs need regular refresher training sessions to keep them up to date on the outbreak trend and any emerging issues. This will maintain CHWs' knowledge and skills in performing their roles.
The strength of the study lies in the fact that it used mixed design approaches ranging from qualitative and quantitative. This allowed triangulation of information for strengthening information generated by respondents. The study also involved multiple types of respondents ranging from CHWs, Health care workers, and community leaders' representatives. This gave room to get various opinions and get a clear picture of the state of affairs regarding the equipping of CHWs during times of epidemics including COVID-19. However, this was a cross-sectional study and could not assess the outcome or impact brought about by the actions of CHWs.
Conclusion
In conclusion, this study has highlighted the ability of the CHWs to adapt to Public Health Emergencies needs. These results underscore the importance of the adaptability of CHWs' knowledge, skills, and attitudes during public health emergencies. Moving forward, future research should focus on exploring the sustainability of utilizing CHWs in emergencies and their effectiveness. Further, a community-based study to assess the impact or outcome of the actions of CHWs could be relevant. This study provides insight into how CHWs can play a significant role in responding to Public Health emergency management in countries with limited medical resources.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving humans were approved by Joint CUHAS/BMC research and Ethics Review Committee. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
EM: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. EK: Conceptualization, Data curation, Formal analysis, Methodology, Supervision, Validation, Writing – original draft, Writing – review & editing. TT: Conceptualization, Data curation, Investigation, Project administration, Writing – original draft, Writing – review & editing. NB: Conceptualization, Data curation, Formal analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. MG: Data curation, Methodology, Supervision, Writing – original draft, Writing – review & editing. TN: Data curation, Methodology, Supervision, Writing – original draft, Writing – review & editing. FM: Data curation, Formal analysis, Funding acquisition, Writing – original draft, Writing – review & editing.
Funding
The author (s) declare that no financial support was received for the research, authorship, and/or publication of this article.
Acknowledgments
The authors would like to acknowledge the support from the Simiyu Regional Administrative Office, and the Regional Medical Officer for general information and practical guidance in working in the region. Further, the authors would like to thank the support of the Council Administration for link-ups and introductions to work in the communities.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. TTCIH. Addressing Tanzania's Health Workforce Crisis Through a Public-Private Partnership:The Case of TTCIH. (2016). Available at: https://www.globalhealthdelivery.org/files/ghd/files/ghd-034_ttcih_final.pdf (accessed June 24, 2024).
2. O'Donovan J. Community Health Workers Will be the Main Defense in Rural Uganda Against Coronavirus. (2020). Available at: https://www.statnews.com/2020/03/28/community-health-workers-lead-covid-19-fight-uganda/ (accessed June 24, 2024).
3. World Health Organization. Scaling Up, Saving Lives: Task Force for Scaling Up Education and Training for Health Workers. Global Health Workforce Alliance (2008). p. ix, 113–ix.
4. Greenspan JA, McMahon SA, Chebet JJ, Mpunga M, Urassa DP, Winch PJ. Sources of community health worker motivation: a qualitative study in Morogoro Region, Tanzania. Hum Resour Health. (2013) 11:52. doi: 10.1186/1478-4491-11-52
5. Nemcek MA, Sabatier R. State of evaluation: community health workers. Public Health Nurs. (2003) 20:260–70. doi: 10.1046/j.1525-1446.2003.20403.x
6. Lewin S, Munabi-Babigumira S, Glenton C, Daniels K, Bosch-Capblanch X, van Wyk BE, et al. Lay health workers in primary and community health care for maternal and child health and the management of infectious diseases. Cochr Database Syst Rev. (2010) CD004015. doi: 10.1002/14651858.CD004015.pub3
7. Zhou F, Yu T, Du R, Fan G, Liu Y, Liu Z, et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study. Lancet. (2020) 395:1054–62. doi: 10.1016/S0140-6736(20)30566-3
8. WHO. Director-General's Opening Remarks at the Media Briefing on COVID-19. (2020). Available at: https://wwwwhoint/director-general/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19-−11-march-2020 (accessed June 24, 2024).
9. Wadvalla B-A. Covid-19: decisive action is the hallmark of South Africa's early success against coronavirus. BMJ. (2020) 369:m1623. doi: 10.1136/bmj.m1623
10. Marahatta SB, Paudel S, Aryal N. COVID-19 pandemic: what can Nepal do to curb the potential public health disaster? J Karnali Acad Health Sci. (2020) 3:28374. doi: 10.3126/jkahs.v3i1.28374
11. Council ID. Itilima District Profile (2016). Available at: https://itilimadc.go.tz/profile (accessed June 24, 2024).
12. Ministry Ministry of Finance and Planning Office - Finance and Planning Zanzibar. The 2022 Population and Housing Census: Age and Sex Distribution Report. Tanzania (2022).
13. Bans-Akutey A, Tiimub BM. Triangulation in research. Acad Lett. (2021) 2:1–6. doi: 10.20935/AL3392
14. Hennink M, Kaiser BN. Sample sizes for saturation in qualitative research: a systematic review of empirical tests. Soc Sci Med. (2022) 292:114523. doi: 10.1016/j.socscimed.2021.114523
15. Fusch Ph D PI, Ness LR. Are We There Yet? Data Saturation in Qualitative Research. Fort Lauderdale, FL: TQR Publications (2015).
16. Greenhalgh T, Taylor R. How to read a paper: papers that go beyond numbers (qualitative research). BMJ. (1997) 315:740–3. doi: 10.1136/bmj.315.7110.740
17. Shrestha A, Thapa TB, Giri M, Kumar S, Dhobi S, Thapa H, et al. Knowledge and attitude on prevention of COVID-19 among community health workers in Nepal-a cross-sectional study. BMC Public Health. (2021) 21:1–13. doi: 10.1186/s12889-021-11400-9
18. Omoronyia O, Ekpenyong N, Ukweh I, Mpama E. Knowledge and practice of COVID-19 prevention among community health workers in rural Cross River State, Nigeria: implications for disease control in Africa. Pan Afr Med J. (2020) 37:24307. doi: 10.11604/pamj.2020.37.50.24307
19. Ajeani J, Mangwi Ayiasi R, Tetui M, Ekirapa-Kiracho E, Namazzi G, Muhumuza Kananura R, et al. A cascade model of mentorship for frontline health workers in rural health facilities in Eastern Uganda: processes, achievements and lessons. Glob Health Action. (2017) 10:1345497. doi: 10.1080/16549716.2017.1345497
20. Olateju Z, Olufunlayo T, MacArthur C, Leung C, Taylor B. Community health workers experiences and perceptions of working during the COVID-19 pandemic in Lagos, Nigeria—A qualitative study. PLoS ONE. (2022) 17:e0265092. doi: 10.1371/journal.pone.0265092
21. Perry H, Zulliger R. How Effective are Community Health Workers. An Overview of Current Evidence With Recommendations for Strengthening Community Health Worker Programs to Accelerate Progress in Achieving the Health-Related Millennium Development Goals. Baltimore, MD: Johns Hopkins Bloomberg School of Public Health (2012). 84 p.
22. Mohseni M, Azami-Aghdash S, Isfahani HM, Moosavi A, Fardid M. Role of nongovernmental organizations in controlling COVID-19. Disast Med Public Health Prepared. (2021) 1. doi: 10.1017/dmp.2021.60
23. Saeed BQ, Al-Shahrabi R, Bolarinwa OA. Socio-demographic correlate of knowledge and practice toward COVID-19 among people living in Mosul-Iraq: a cross-sectional study. PLoS ONE. (2021) 16:e0249310. doi: 10.1371/journal.pone.0249310
24. Atibioke OP, Adepoju-Olajuwon F, Ojomo OA, Oladeji AO, Oripeloye OB, Osinowo KA, et al. Knowledge, attitude and adherence to COVID-19 prevention among community health workers in Nigeria. Pan Afr Med J. (2022) 42:30791. doi: 10.11604/pamj.2022.42.307.30791
25. Schleiff MJ, Aitken I, Alam MA, Damtew ZA, Perry HB. Community health workers at the dawn of a new era: 6. Recruitment, training, and continuing education. Health Res Policy Syst. (2021) 19:1–28. doi: 10.1186/s12961-021-00757-3
26. Ballard M, Olsen HE, Millear A, Yang J, Whidden C, Yembrick A, et al. Continuity of community-based healthcare provision during COVID-19: a multicountry interrupted time series analysis. BMJ Open. (2022) 12:e052407. doi: 10.1136/bmjopen-2021-052407
27. Roy S, Kennedy S, Hossain S, Warren CE, Sripad P. Examining roles, support, and experiences of community health workers during the COVID-19 pandemic in Bangladesh: a mixed methods study. Global Health. (2022) 10:761. doi: 10.9745/GHSP-D-21-00761
28. Nanda P, Lewis TN, Das P, Krishnan S. From the frontlines to centre stage: resilience of frontline health workers in the context of COVID-19. Sex Reprod Health Matters. (2020) 28:1837413. doi: 10.1080/26410397.2020.1837413
29. Bhaumik S, Moola S, Tyagi J, Nambiar D, Kakoti M. Community health workers for pandemic response: a rapid evidence synthesis. BMJ Global Health. (2020) 5:e002769. doi: 10.1136/bmjgh-2020-002769
30. Singh D, Negin J, Otim M, Orach CG, Cumming R. The effect of payment and incentives on motivation and focus of community health workers: five case studies from low-and middle-income countries. Hum Resour Health. (2015) 13:1–12. doi: 10.1186/s12960-015-0051-1
31. Zulu JM, Perry HB. Community Health Workers at the Dawn of a New Era. Bethesda, MD: National Library of Medicine (2021). p. 1–5.
32. Nepomnyashchiy L, Dahn B, Saykpah R, Raghavan M. COVID-19: Africa needs unprecedented attention to strengthen community health systems. Lancet. (2020) 396:150–2. doi: 10.1016/S0140-6736(20)31532-4
Keywords: community health workers, COVID-19 pandemic, preparedness, emergency, medical emergencies, rural health care
Citation: Msegu E, Konje E, Tupa T, Basinda N, Gwimile MS, Ngallaba T and Marwa F (2024) The adaptability of rural healthcare workers' knowledge, skills, and attitudes during public health emergencies: insights from the COVID-19 response in Itilima district, Simiyu, Tanzania. Front. Disaster Emerg. Med. 2:1435585. doi: 10.3389/femer.2024.1435585
Received: 20 May 2024; Accepted: 09 August 2024;
Published: 25 September 2024.
Edited by:
Theodore Chan, University of California, San Diego, United StatesReviewed by:
Peggy Berry, Thrive at Life: Working Solutions, United StatesJan-Cedric Hansen, Centre d'Hébergement et d'Accompagnement Gérontologique (CHAG), France
Copyright © 2024 Msegu, Konje, Tupa, Basinda, Gwimile, Ngallaba and Marwa. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Namanya Basinda, ZHJiYXNpbmRhQHlhaG9vLmNvLnVr