 Naomi Ito1*
Naomi Ito1* Toyoaki Sawano1,2
Toyoaki Sawano1,2 Yuna Uchi1
Yuna Uchi1 Moe Kawashima3
Moe Kawashima3 Kemmei Kitazawa1
Kemmei Kitazawa1 Nobuaki Moriyama4
Nobuaki Moriyama4 Isamu Amir1Hiroki Yoshimura1Saori Nonaka1
Isamu Amir1Hiroki Yoshimura1Saori Nonaka1 Hiroaki Saito1,5
Hiroaki Saito1,5 Akihiko Ozaki6,7
Akihiko Ozaki6,7 Chika Yamamoto1
Chika Yamamoto1 Toshiki Abe1
Toshiki Abe1 Michio Murakami8†
Michio Murakami8† Mika Sato9Chihiro Matsumoto1
Mika Sato9Chihiro Matsumoto1 Momoka Yamamura1Tianchen Zhao1Mamoru Sakakibara10Kazuko Yagiuchi11Mako Otsuki12Tomoyoshi Oikawa13Shinichi Niwa14
Momoka Yamamura1Tianchen Zhao1Mamoru Sakakibara10Kazuko Yagiuchi11Mako Otsuki12Tomoyoshi Oikawa13Shinichi Niwa14 Masaharu Tsubokura1
Masaharu Tsubokura1- 1Department of Radiation Health Management, Fukushima Medical University School of Medicine, Fukushima, Japan
- 2Department of Surgery, Jyoban Hospital of Tokiwa Foundation, Iwaki, Japan
- 3ShirakawaKosei General Hospital, Shirakawa, Japan
- 4Department of Public Health, Fukushima Medical University School of Medicine, Fukushima, Japan
- 5Department of Internal Medicine, Soma Central Hospital, Fukushima, Japan
- 6Breast and Thyroid Center, Jyoban Hospital of Tokiwa Foundation, Iwaki, Japan
- 7Department of Thyroid and Endocrinology, Fukushima Medical University School of Medicine, Fukushima, Japan
- 8Department of Health Risk Communication, Fukushima Medical University School of Medicine, Fukushima, Japan
- 9Department of Health Nursing of International Radiation Exposure, Fukushima Medical University Graduate School of Medicine, Fukushima, Japan
- 10Reinstatement Support Center for Nurses, Incorporated Foundation of Tokiwa-Kai, Iwaki, Japan
- 11St. Olive Nursing Home, Fukushima, Japan
- 12Department of Nursing, Fukushima Medical University Hospital, Fukushima, Japan
- 13Department of Neurosurgery, Minamisoma Municipal General Hospital, Minamisoma, Japan
- 14Department of Psychiatry, Aizu Medical Center, Fukushima Medical University, Aizuwakamatsu, Japan
Introduction: Relocation after a disaster often has negative health effects on vulnerable people, particularly older adults. However, little is known about the number of repeated evacuations and relocations after disasters among those experienced disaster-related deaths. This case series aimed to summarize the secondary problems and mortality risks in patients involved in relocation after disasters.
Methods: We analyzed and summarized the data on 520 disaster-related deaths in Minamisoma City, a municipality near the Fukushima Daiichi Nuclear Power Plant, focusing on the number of relocations. Herein, we describe the cases of three individuals over 80 years old, who died after eight or more relocations, which were certified as disaster-related deaths.
Results: We discuss following three cases, which are (1) a female patient in her 90s who had a stroke and was completely disabled, (2) a female patient in her 80s whose cancer was detected later due to her failing to see her family doctor, and (3) a male patient in his 80s whose regular postoperative treatment was disrupted following cancer recurrence.
Discussion: Our findings indicate that evacuation led to the worsening of chronic diseases and eventually to post-disaster death. Prolonged wide-area evacuation and repeated relocation likely interrupted the continuum of care and led to the failure of adequate care provision. To reduce the loss of human life, it is necessary to review the number of wide-area evacuations and relocations over the medium to long term after large-scale disasters, including nuclear disasters, which may occur in the future. Simultaneously, it is important to establish a medical system at the evacuation site so that disaster victims can continue to receive medical care even after evacuation or relocation.
1 Introduction
The desire to continue living in a familiar place is a universal human desire (1, 2). This idea of aging in a familiar place represents a central concept of community living (3, 4). Living in a well-known area helps maintain and improve independence, dignity, and quality of life (5). However, it may not be possible to age in a usual place when other factors, such as disasters or illnesses, complicate matters. Despite the importance of this issue, appropriate measures are often not implemented during emergencies. Taking measures to facilitate aging in familiar places following such events is a significant concern for public health.
Disasters disturb the usual life of each individual, especially aging in familiar places. When a disaster happens, governments may issue evacuation orders, and severe damage to houses by disasters may prevent people from residing in the area. As the disaster frequency and scale have increased in recent years (6), there has been a growing national and international interest in ensuring the quality of life for residents while maintaining aging in familiar places in the event of prolonged post-disaster evacuation (7). Although essential during disasters, there is still not enough research on how to implement aging in familiar places during the post-disaster recovery process.
In the event of the Great East Japan Earthquake in 2011, 164,865 people were evacuated from Fukushima Prefecture not only because of the earthquake and tsunami but also because of the Fukushima Daiichi nuclear power plant (FDNPP) accident (8). The impact of the disaster was significant, resulting in 19,728 deaths nationwide (as of March 9, 2020) (9) and 3,789 disaster-related deaths (as of March 31, 2022) (10). For example, in Minamisoma City, located 13–38 km north of the FDNPP in Fukushima Prefecture (Figure 1), there were many deaths among the disaster-vulnerable people while evacuating (11, 12). Patients with underlying diseases die because of inadequate medical care in the wake of disasters (13–15). Many disaster victims have been forced to adapt to rapid environmental changes while living in evacuation centers, which may increase the mortality risk and disaster-related deaths (16, 17). Evacuation due to the nuclear accident forced evacuees to leave their homes for an extended period. They moved frequently to primary evacuation sites, temporary housing, and other locations, and were unable to return to their original homes. Recently, our research team conducted a survey of disaster-related deaths in Minamisoma City, Fukushima Prefecture, and found that people who had long-term care certification accounted for more than half of the deaths and that many died from cardiovascular and respiratory diseases during the early stages of the disaster (18). These results suggest that repeated evacuations likely increased the number of disaster-related deaths among disaster-vulnerable people, including those in need of care at medical institutions and older adult care facilities (19–21). Post-disaster (frequent) evacuations have caused deterioration in mental health, including psychological distress (22–24). However, the frequency of displacement, in terms of disaster-related deaths, has not yet been discussed.
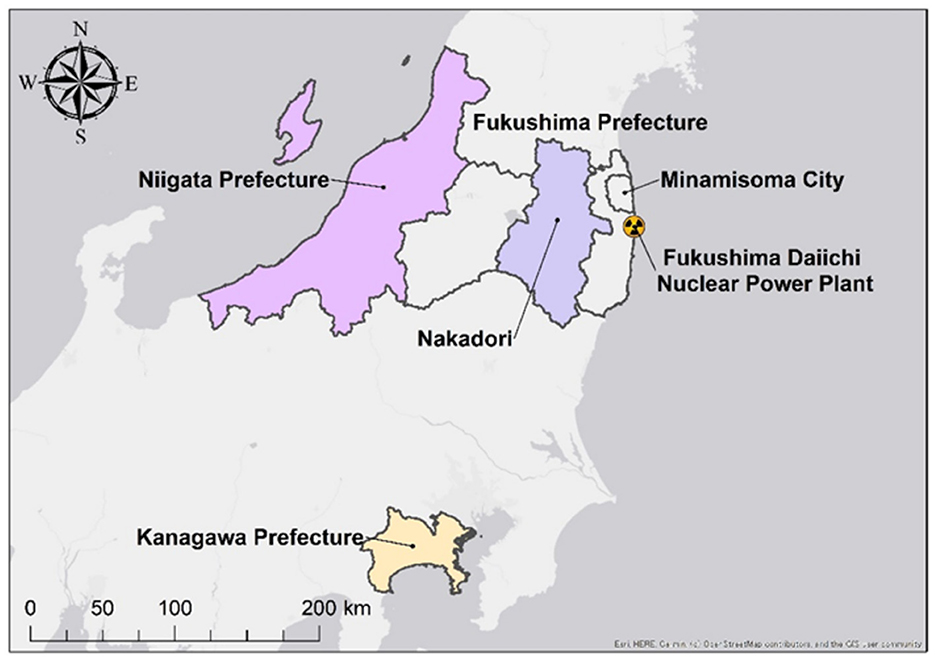
Figure 1. Location of Minamisoma City and relocation destinations for Case #1.
Herein, we report database-based cases of disaster-related deaths in Minamisoma City, Fukushima Prefecture, following the FDNPP accident, focusing on older residents who frequently relocated. This study aimed to examine the relationship between relocation and disaster-related deaths. By examining the characteristics of disaster-related deaths with a focus on relocation, more appropriate measures could be developed to reduce disaster-related deaths through identifying secondary problems associated with relocation in the event of similar disasters.
2 Materials and methods
2.1 Study design and setting
This is a retrospective observational study of residents of Minamisoma City, Fukushima Prefecture, who were identified as disaster-related deaths from March 11, 2011 to March 31, 2022. The tsunami caused by the Great East Japan Earthquake resulted in 636 deaths in Minamisoma City. The southern part of Minamisoma City was identified as an evacuation zone. As of February 14, 2022, 520 disaster-related deaths have occurred due to long-term evacuation (25).
2.2 Study subjects
The study examined 520 Minamisoma residents who died following the earthquake and were officially classified as disaster-related deaths by the city. Japan defines disaster-related deaths broadly, including those caused by conditions aggravated by the disaster or evacuation hardships. These deaths are certified by local committees based on family testimonies. However, there is no national standard for such certifications, and the process varies by municipality.
2.3 Data collection
Data on individuals officially recognized as disaster-related deaths in Minamisoma City were collected. This involved compiling application forms and supporting documents submitted by bereaved families to the city government.
Data on 520 people in Minamisoma City, whose deaths were certified as disaster-related, were collected from information obtained from the city hall in response to requests from bereaved families. Medical information from hospitals or other publicly available sources was not accessible during the data collection process.
2.4 Data analysis
Variables such as age, gender, time from disaster to death, area of residence, number of moves, number of evacuations, and reasons for certification were analyzed using descriptive statistics. In addition, qualitative analysis was conducted by focusing on and describing the subjects who moved more frequently.
2.5 Definition
Evacuation is a process of forced migration or relocation of populations from a hazardous area to a safer one, often necessitated by natural disasters, armed conflicts, or other man-made emergencies.
Relocation is defined as changing one's place of residence, which includes relocation due to evacuation and hospitalization for treatment (number of relocations > number of evacuations).
Disaster-related deaths are defined as deaths not due to direct damage from disasters such as collapsed buildings, fires, and tsunamis (direct deaths), but due to indirect factors such as deterioration of physical condition and psychological shock during the subsequent evacuation period.
2.6 Ethics statement
This study involving humans was approved by the Minamisoma Municipal General Hospital Ethics Committee (approval number: 2–21) and Fukushima Medical University Ethics Committee (reference number: 2020-297). The study was conducted in accordance with local legislation and institutional requirements. The need for informed consent was waived due to the retrospective and anonymized nature of the investigation.
3 Results
3.1 Data analysis and case description
The average age at death of all participants certified as having disaster-related deaths in Minamisoma City was 82.69 years (18). Of the 520 participants, we could obtain the relocation data (“number of relocations”) and the number of days from disaster to death (“number of days until death”) of 518. The average number of relocations between disaster and death was 3.03, and 66.2% of the participants relocated 0–3 times, which means that 33.8% of them relocated more than four times (Figure 2). In addition, the average number of days from the disaster to death was 230.6 for all participants, 161.4 for those who experienced three or fewer relocations (343 people), and 367 for those who experienced four or more relocations (175 people).
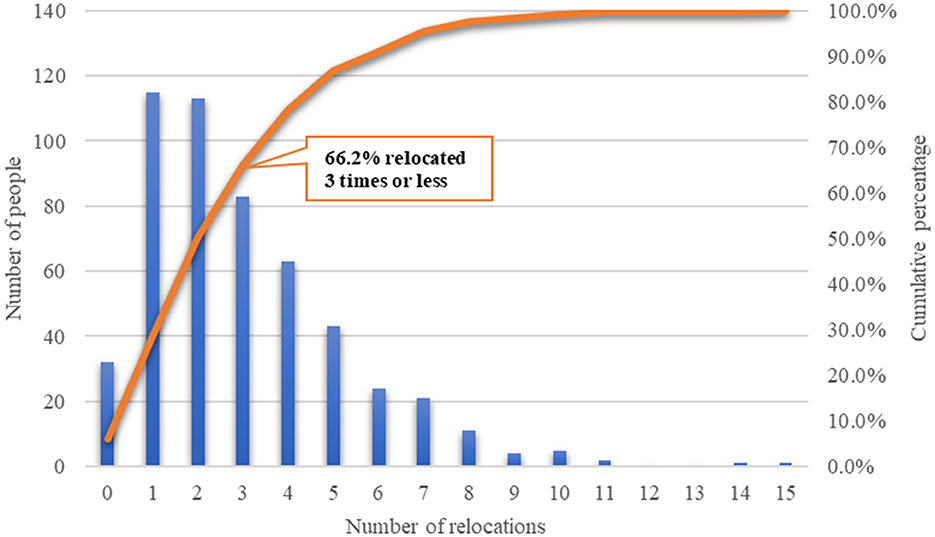
Figure 2. Number of relocations in the 518 cases of disaster-related deaths in Minamisoma City.
Herein, we describe three cases of patients aged over 80 years who required eight or more relocations, including evacuation, whose deaths were certified as disaster-related and reported each case below. These participants were selected, because this study focused on cases of extremely frequent post-disaster relocation in an aging society.
3.2 Case presentations
#1. Stress and illness due to frequent relocation
This was a case of a female patient, who was in her 90s and lived in Minamisoma. Her activity of daily living (ADL) score indicated functional independence at the time of the disaster. When the earthquake occurred, she went upstairs in her home to escape the tsunami. During her evacuation, her daily routine was to take walks; however, she stopped it in November 2011. She worried about her future, crying as she reminded her of her grandchildren and great-grandchildren. Seeing her house destroyed by the tsunami was a shock. The deaths of four individuals who were her associates and a friend in a senior citizen's group were also shocking to her. There was a strong fear that she would not be able to return home while still alive. After her home was damaged, she relocated to evacuation centers in the city, to several relatives' homes in Niigata Prefecture, and then to places in Kanagawa Prefecture and the Nakadori area in Fukushima Prefecture (Figure 1). She became depressed and mentally stressed. She experienced a cerebral infarction and required complete care. She was admitted to a facility but was hospitalized because of a high fever. The patient died of congestive heart failure 606 days after the disaster. Her death was disaster-related because evacuation and stress caused her heart and kidney failure. Retrospectively, the number of her relocations after the disaster was 10 times.
#2. Delayed medical examinations and early detection of cancer due to relocation
This was a case of a female patient, who was in her 80s and lived in Minamisoma. Her ADL score at the time of the disaster indicated functionally independence. After being evacuated, she continued to experience insomnia and loss of appetite due to stress. Although she had not been feeling well during her evacuation, she did not visit a doctor because her family doctor was not available at her evacuation destination. Later, she was diagnosed with gastric cancer and was repeatedly hospitalized. The patient died of gastric cancer 722 days after the disaster. Her death was recognized as disaster-related because the delayed detection of her gastric cancer was attributed to the long period of evacuation. Retrospectively, the number of her relocations after the disaster was 9.
#3. Interruption of treatment due to relocation
This was a case of a male patient, who was in his 80s and lived in Minamisoma. His ADL score at the time of the disaster indicated functionally independence. He had undergone surgery for gastric cancer 6 months prior to the disaster; thus, he had to divide his meals into several portions. Metastases were detected 1 year and 7 months after the surgery, which his doctor diagnosed as being caused by stress due to his lifestyle changes. Owing to the evacuation, he was unable to undergo a scheduled regular examination for gastric cancer. He did not have a letter of introduction and was unable to receive adequate treatment for his gastric cancer at the hospital to which he was evacuated. The patient died of respiratory failure 809 days after the disaster. His death was certified as disaster-related because the evacuation may have hastened his death. Retrospectively, the number of his relocations after the disaster was 8.
4 Discussion
This study showed that even amidst the generalized post-disaster health effects (22), repeated relocation over a long period after a nuclear power plant accident could result in reduced access to medical care, which poses fatal physical and psychological risks and damages to disaster-vulnerable people. This suggests that, although evacuation has benefits, such as reducing disaster risks, including radiation exposure and tsunami damage, the lack of careful post-treatment follow-up and psychological care due to relocation should be considered to worsen the physical and psychological prognosis.
Patients who frequently relocate might have an increased mental burden due to changes in their living environment, which may be associated with disaster-related deaths. In all the cases reported in this report, the patients were aged over 80 years, had relocated eight to 10 times, and died approximately 2 years after the disaster occurred. There was mental stress due to the disaster, evacuation, and completely changed living environments. They not only evacuated immediately after the disaster but also relocated frequently, as a secondary evacuation, to relatives' houses and medical facilities (#1, #2 and #3). Repeated relocation and changes in the environment can cause more stress, and it is highly likely that they will be unable to maintain their daily lives. Interruptions in self-care and regular medical checkups can easily lead to the deterioration of physical conditions (#2 and #3). There is certainly a secondary aspect to the loss of human connections, which is the inability to follow up on treatment and continue mental health care (#1, #2 and #3) (26). Many disaster-vulnerable people, including older adults, require support during disasters, and they are especially susceptible to evacuation. It means that evacuation brings about rapid changes in their living environments (27–29). Furthermore, even after evacuation, there is a risk of harm to health and loss of life (disaster-related deaths) (30). Therefore, in accordance with our own findings, relocation after a disaster has a negative impact on the health of people who were vulnerable to disasters, which requires more attention.
Repeated transfers result in the decline in ADLs, which increases vulnerability. This is not limited to the aging population but may also include people with disabilities receiving medical services and patients undergoing anticancer treatment, among others. Concerns about such situations due to relocation have also been raised. In the cases presented in this report, ADL scores indicated functional independence of the patients at the time of the disaster (#2 and #3). However, over time, their physical functions deteriorated owing to factors such as worsening chronic illnesses. Relocation has also been reported to cause declines in mental and physical function in older adults, even if no new illnesses occur (31). The cause and time of disaster-related deaths varied according to age. Many older adults die, with bedridden people dying within the first 1–2 months, followed by patients with low nursing care levels or dementia dying within the next 3 months (19, 32). After 1 year, depression, suicide, and alcohol use disorders are seen in young people (33).
The Fukushima nuclear accident resulted in marked confusion as evacuations were urgently planned and ordered far beyond the scope of the disaster prevention plan, forcing people to evacuate multiple times for long periods (34). This may require measures to reduce the number of relocations when the post-disaster evacuation is prolonged. This is because, due to multiple long-term and remote area evacuations, it is highly likely that continuity of care is interrupted and sufficient care cannot be provided. As in the cases shown in this report, moving eight times in the 2 years before death was not a reasonably calm life. Although the information was inconclusive, there may have been some relocations that could have been avoided. As a disaster countermeasure, it is possible to set up facilities nearby where people can stay so that they do not have to relocate to distant relatives' homes. At the same time, it is even more fatal if the medical and nursing care that they were previously receiving is interrupted or not available at all. It is important to continue sharing information and provide the same medical and nursing care even when they relocate. Therefore, it is necessary to establish a system that enables continuous support for individuals in the affected areas. In addition, an approach to building resilience is necessary even in the midst of an evacuation (35).
This study has some limitations. First, this case series utilized aggregated data of individuals with disaster-related deaths in Minamisoma City without additional information, such as medical records from hospitals or institutions. Therefore, we could not determine whether the deaths were due to relocation or natural causes. Second, the information was limited to a single local government. Since the number of cases were limited, we only described a few typical cases as a case series in this study. In the future, by obtaining information from other districts and from other sources, it would be possible to deepen our understanding.
5 Conclusion
According to a dataset of disaster-related deaths in one municipality near the FDNPP after the nuclear accident, more than 30% of disaster-related deaths involved four or more relocations. Repeated relocation over a long period accelerates the decline in mental and physical functions, and people often fail to receive regular health checkups or follow-up clinic visits. This occurs especially in people who are vulnerable to disasters, such as older adults and people with illnesses, as described here. Areas that were evacuated during the nuclear power plant accident experienced rapid aging and population decline. To prevent disaster-related deaths in future large-scale disasters, including nuclear disasters, it is important to take measures for disaster-vulnerable populations, taking into consideration the issue of relocation itself and the continuity of care under repeated relocation.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions. Data supporting the results of this study are available from third parties; however, restrictions apply to the availability of these data, which were used under license for this study and are not publicly available. Data are available from the authors upon reasonable request and with the permission of the third party. Requests to access these datasets should be directed to Minamisoma City Office.
Ethics statement
The studies involving humans were approved by Minamisoma Municipal General Hospital Ethics Committee (approval number: 2–21) and Fukushima Medical University Ethics Committee (reference number: 2020-297). The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin in accordance with the national legislation and institutional requirements.
Author contributions
NI: Writing – original draft, Writing – review & editing. TS: Writing – original draft, Writing – review & editing. YU: Data curation, Writing – review & editing. MK: Data curation, Writing – review & editing. KK: Data curation, Writing – review & editing. NM: Data curation, Writing – review & editing. IA: Data curation, Writing – review & editing. HY: Data curation, Writing – review & editing. SNo: Data curation, Writing – review & editing. HS: Data curation, Writing – review & editing. AO: Data curation, Writing – review & editing. CY: Data curation, Writing – review & editing. TA: Writing – review & editing. MM: Conceptualization, Writing – review & editing. MS: Writing – review & editing. CM: Writing – review & editing. MY: Writing – review & editing. TZ: Writing – review & editing. MS: Data curation, Writing – review & editing. KY: Data curation, Writing – review & editing. MO: Data curation, Writing – review & editing. TO: Writing – review & editing. SNi: Conceptualization, Writing – review & editing. MT: Supervision, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This work was financially supported by JST Grant Number JPMJPF2301 and the Program of the Network-type Joint Usage/Research Center for Radiation Disaster Medical Science.
Acknowledgments
We sincerely thank the research assistant Rika Ishizuka (Office for Diversity and Inclusion at Fukushima Medical University) for her assistance with manuscript preparation.
Conflict of interest
AO received personal fees from MNES, Kyowa Kirin Inc., Becton, Dickinson and Company, Pfizer, Daiichi Sankyo Inc and Taiho Pharmaceutical Co., Ltd., outside the scope of the submitted work.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Ivry J. Aging in place: the role of geriatric social work. Fam Soc. (1995) 76:76–85. doi: 10.1177/104438949507600202
2. Kelen J, Griffiths KA. Housing for the aged: new roles for social work. Int J Aging Hum Dev. (1983) 16:125–33. doi: 10.2190/LQ4J-6VEK-7AUU-ULAJ
3. Pynoos, J. Public policy and aging in place: Identifying the problems and potential solutions. in Aging in Place: Supporting the Frail Elderly in Residential Environments. Northbrook, IL: Scott Foresman & Company (1990). p. 167–208.
4. Rogers WA, Ramadhani WA, Harris MT. Defining aging in place: the intersectionality of space, person, and time. Innov Aging. (2020) 4:igaa036. doi: 10.1093/geroni/igaa036
5. Wiles JL, Leibing A, Guberman N, Reeve J, Allen RE. The meaning of “aging in place” to older people. Gerontologist. (2012) 52:357–66. doi: 10.1093/geront/gnr098
6. World_Disasters_Report_2022. (2022). Available at: https://www.ifrc.org/sites/default/files/2023-03/2022_IFRC-WDR_EN.0.pdf.pdf (accessed August 5, 2024).
7. Adams V, Kaufman SR, van Hattum T, Moody S. Aging disaster: mortality, vulnerability, and long-term recovery among Katrina survivors. Med Anthropol. (2011) 30:247–70. doi: 10.1080/01459740.2011.560777
8. Fukushima Prefecture. Evacuation Status in Fukushima Prefecture. Available at: https://www.pref.fukushima.lg.jp/uploaded/attachment/444563.pdf (accessed March 16, 2024).
9. Miyagi Prefecture. Overview of the Great East Japan Earthquake. (2020). Available at: https://www.pref.miyagi.jp/documents/38088/10_1.pdf (accessed March 16, 2024).
10. Reconstruction Agency. Number of earthquake-related deaths in the Great East Japan earthquake. (2022). Available at: https://www.reconstruction.go.jp/topics/main-cat2/sub-cat2-6/20220630_kanrenshi.pdf (accessed March 3, 2024).
11. Hayakawa M. Increase in disaster-related deaths: risks and social impacts of evacuation. Ann ICRP. (2016) 45:123–8. doi: 10.1177/0146645316666707
12. Nomura S, Gilmour S, Tsubokura M, Yoneoka D, Sugimoto A, Oikawa T, et al. Mortality risk amongst nursing home residents evacuated after the Fukushima nuclear accident: a retrospective cohort study. PLoS ONE. (2013) 8:e60192. doi: 10.1371/journal.pone.0060192
13. Sawano T, Senoo Y, Yoshida I, Ozaki A, Nishikawa Y, Hori A, et al. Emergency hospital evacuation from a hospital within 5 km radius of Fukushima Daiichi nuclear power plant: a retrospective analysis of disaster preparedness for hospitalized patients. Disaster Med Public Health Prep. (2022) 16:2190–3. doi: 10.1017/dmp.2021.265
14. Sonoda Y, Ozaki A, Hori A, Higuchi A, Shimada Y, Yamamoto K, et al. Premature death of a schizophrenic patient due to evacuation after a nuclear disaster in Fukushima. Case Rep Psychiatry. (2019) 2019:3284153. doi: 10.1155/2019/3284153
15. Sawano T, Nishikawa Y, Ozaki A, Leppold C, Takiguchi M, Saito H, et al. Premature death associated with long-term evacuation among a vulnerable population after the Fukushima nuclear disaster: a case report. Medicine. (2019) 98:e16162. doi: 10.1097/MD.0000000000016162
16. Morita T, Nomura S, Tsubokura M, Leppold C, Gilmour S, Ochi S, et al. Excess mortality due to indirect health effects of the 2011 triple disaster in Fukushima, Japan: a retrospective observational study. J Epidemiol Community Health. (2017) 71:974–80. doi: 10.1136/jech-2016-208652
17. Yasumura S. Evacuation effect on excess mortality among institutionalized elderly after the Fukushima Daiichi nuclear power plant accident. Fukushima J Med Sci. (2014) 60:192–5. doi: 10.5387/fms.2014-13
18. Kawashima M, Sawano T, Murakami M, Moriyama N, Uchi Y, Kitazawa K, et al. Association between the deaths indirectly caused by the Fukushima Daiichi nuclear power plant accident (disaster-related deaths) and pre-disaster long-term care certificated level; a retrospective observational analysis. (2023). doi: 10.2139/ssrn.4378009
19. Nomura S, Blangiardo M, Tsubokura M, Nishikawa Y, Gilmour S, Kami M, et al. Post-nuclear disaster evacuation and survival amongst elderly people in Fukushima: a comparative analysis between evacuees and non-evacuees. Prev Med. (2016) 82:77–82. doi: 10.1016/j.ypmed.2015.11.014
20. Sawano T, Shigetomi S, Ozaki A, Nishikawa Y, Hori A, Oikawa T, et al. Successful emergency evacuation from a hospital within a 5-km radius of Fukushima Daiichi nuclear power plant: the importance of cooperation with an external body. J Radiat Res. (2021) 62:i122–8. doi: 10.1093/jrr/rraa122
21. Yoshimura H, Sawano T, Murakami M, Uchi Y, Kawashima M, Kitazawa K, et al. Categorization of disaster-related deaths in Minamisoma City after the Fukushima nuclear disaster using clustering analysis. (2023). doi: 10.21203/rs.3.rs-3319395/v1
22. Uscher-Pines L. Health effects of relocation following disaster: a systematic review of the literature. Disasters. (2009) 33:1–22 doi: 10.1111/j.1467-7717.2008.01059.x
23. Horikoshi N, Iwasa H, Kawakami N, Suzuki Y, Yasumura S. Residence-related factors and psychological distress among evacuees after the Fukushima Daiichi nuclear power plant accident: a cross-sectional study. BMC Psychiatry. (2016) 16:420. doi: 10.1186/s12888-016-1134-9
24. Goto T, Wilson JP, Kahana B, Slane S. The Miyake Island volcano disaster in Japan: loss, uncertainty, and relocation as predictors of PTSD and depression. J Appl Soc Psychol. (2006) 36:2001–26. doi: 10.1111/j.0021-9029.2006.00091.x
25. Minamisoma_City. Damage and recovery from the Great East Japan Earthquake R4.2.14 Minamisoma City Disaster Countermeasures Headquarters members meeting materials. (2022). https://www.city.minamisoma.lg.jp/material/files/group/8/340_siryou1.pdf (accessed August 12, 2024).
26. Ozaki A, Nomura S, Leppold C, Tsubokura M, Tanimoto T, Yokota T, et al. Breast cancer patient delay in Fukushima, Japan following the 2011 triple disaster: a long-term retrospective study. BMC Cancer. (2017) 17:423. doi: 10.1186/s12885-017-3412-4
27. Tanida NJB. What happened to elderly people in the great Hanshin earthquake. BMJ. (1996) 313:1133–5 doi: 10.1136/bmj.313.7065.1133
28. Kawachi I, Aida J, Hikichi H, Kondo K. Disaster resilience in aging populations: lessons from the 2011 great east Japan Earthquake & Tsunami. J R Soc N Z. (2020) 50:263–78. doi: 10.1080/03036758.2020.1722186
29. Matsuoka Y, Haseda M, Kanamori M, Sato K, Amemiya A, Ojima T, et al. Does disaster-related relocation impact mental health via changes in group participation among older adults? Causal mediation analysis of a pre-post disaster study of the 2016 Kumamoto earthquake. BMC Public Health. (2023) 23:1982. doi: 10.1186/s12889-023-16877-0
30. Tsuboi M, Sawano T, Nonaka S, Hori A, Ozaki A, Nishikawa Y, et al. Disaster-related deaths after the Fukushima Daiichi nuclear power plant accident - definition of the term and lessons learned. Environ Adv. (2022) 8:100248. doi: 10.1016/j.envadv.2022.100248
31. Ferraro KF. The health consequences of relocation among the aged in the community. J Gerontol. (1983) 38:90–6. doi: 10.1093/geronj/38.1.90
32. Uchi Y, Sawano T, Kawashima M, Sakakibara M, Sudo M, Yagiuchi K, et al. Preliminary analysis of certified disaster-related death in the affected area of the Fukushima Daiichi nuclear power plant accident following the Great East Japan Earthquake: an observational study. ICRP. (2023) 52(S1):196–202. doi: 10.54320/PYOP3947
33. Kitazawa K, Sawano T, Uchi Y, Murakami M, Saito H, Ozaki A, et al. Disaster-related deaths with alcohol-related diseases after the Fukushima Daiichi nuclear power plant accident: case series. Front Public Health. (2024) 11:1292776. doi: 10.3389/fpubh.2023.1292776
34. Ohba T, Tanigawa K, Liutsko L. Evacuation after a nuclear accident: Critical reviews of past nuclear accidents and proposal for future planning. Environ Int. (2021) 148:106379. doi: 10.1016/j.envint.2021.106379
Keywords: relocation effects, disaster-related deaths, disaster, Fukushima nuclear accident, aging in place, evacuation, older people
Citation: Ito N, Sawano T, Uchi Y, Kawashima M, Kitazawa K, Moriyama N, Amir I, Yoshimura H, Nonaka S, Saito H, Ozaki A, Yamamoto C, Abe T, Murakami M, Sato M, Matsumoto C, Yamamura M, Zhao T, Sakakibara M, Yagiuchi K, Otsuki M, Oikawa T, Niwa S and Tsubokura M (2024) Multiple relocation cases in disaster-related deaths after the Fukushima nuclear accident. Front. Disaster Emerg. Med. 2:1434375. doi: 10.3389/femer.2024.1434375
Received: 17 May 2024; Accepted: 25 September 2024;
Published: 14 October 2024.
Edited by:
Ives Hubloue, Vrije University Brussels, BelgiumReviewed by:
Jan-Cedric Hansen, Centre d'Hébergement et d'Accompagnement Gérontologique (CHAG), FranceTakamitsu Kodama, Tajimi City Hospital, Japan
Copyright © 2024 Ito, Sawano, Uchi, Kawashima, Kitazawa, Moriyama, Amir, Yoshimura, Nonaka, Saito, Ozaki, Yamamoto, Abe, Murakami, Sato, Matsumoto, Yamamura, Zhao, Sakakibara, Yagiuchi, Otsuki, Oikawa, Niwa and Tsubokura. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Naomi Ito, aXRvbmFvbWlAZm11LmFjLmpw
†Present address: Michio Murakami, Center for Infectious Disease Education and Research, Osaka University, Suita, Japan