 Gwen Pollaris
Gwen Pollaris Frieda De Bondt2
Frieda De Bondt2
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Disaster Emerg. Med. , 04 December 2023
Sec. Disaster Medicine
Volume 1 - 2023 | https://doi.org/10.3389/femer.2023.1303809
This article is part of the Research Topic Recent Advances in Emergency Medicine View all 6 articles
Background: Many techniques to increase hospital surge capacity in the case of a mass casualty incident (MCI) have already been studied, but a new technique, reverse triage, has gained attention. The objective of this systematic review is to provide a comprehensive literature overview regarding the use of the reverse triage principle in emergency and disaster medicine.
Methods: A systematic literature review was carried out adhering to the Preferred Reporting Items for Systematic Reviews and Meta-Analysis guidelines. Publications up to May 2023 in the Medline, Embase, CENTRAL, CINAHL, and Web of Science databases were considered. The risk of bias was assessed using the Methodological Items for Non-Randomized Studies, the Risk of Bias Assessment Tool for Systematic Reviews, and Johanna Briggs Institute tools for observational, systematic reviews, and expert opinions respectively.
Results: The initial search identified 21,259 unique records, of which 16 were included, consisting of 2 reviews, 5 expert opinions, and 9 observational studies. Across studies, an overall surge capacity of 20–30% could be achieved by implementing reverse triage and even more when combined with other strategies. Furthermore, the American framework that comprehended a safe discharge protocol for inpatients is being used in the development of new reverse triage discharge protocols. The risk of developing a complication (adverse event) due to early discharge is rather low.
Discussion: Due to the heterogeneity of the included studies, the interpretation of the results should be taken with caution. The most prominent differences were related to study size, university affiliation, health care system, and patient characteristics. Nevertheless, implementing the reverse triage principle in MCIs to guide early discharge of adult inpatients can create additional surge capacity with a minor occurrence of adverse events. A final assessment by a multidisciplinary discharge team (nurses and physicians) remains crucial.
Systematic review registration: https://www.crd.york.ac.uk/prospero/display_record.php?ID=CRD42022294136, identifier: CRD42022294136.
Over time, mass casualty incidents (MCIs), such as natural disasters and global pandemics, are occurring more frequently. These high-consequence events easily overwhelm the local health care system and its limited resources, staff, and space. To increase hospitals' surge capacity, different interventions have been studied such as cancellation of elective surgeries, opening unstaffed beds, and converting non-clinical spaces for clinical use. Nevertheless, most of these interventions need increased medical staffing at a time they are needed to take care of casualties at the emergency department (ED) or at the disaster site itself (1). In 2005, the reverse triage (RT) principle was introduced (2). RT is a way to rapidly create inpatient surge capacity by identifying hospitalized patients who do not require major medical assistance for at least 96 h and who only have a small risk for serious complications resulting from early discharge (1). This technique will help make inpatient beds available on shorter notice without demanding more medical staff. In recent years, the principle of RT has gained significantly more interest. Research groups started to study potential RT applications within their own health care system. Following the COVID-19 pandemic, even moral and ethical considerations have been published regarding the implementation of RT protocols in the decision process to allocate scarce resources (3, 4).
To provide a comprehensive overview regarding the use of the RT principle in emergency and disaster medicine, we conducted a systematic literature search. The following research question was used: “What is the association between reverse triage implementation in adult inpatients and (1) hospitals' surge capacity, (2) prevalence of adverse events after early discharge, and (3) mortality rates during an MCI or ED crowding?”
The study protocol was registered in PROSPERO (registration number: CRD42022294136). The Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines were followed to report the results (5).
Studies were eligible if (1) the population of interest was hospitalized adult patients, (2) the intervention studied was “RT,” (3) the outcomes assessed were the effects of the intervention on hospital surge capacity and the prevalence of adverse events (AEs) in patients discharged early or mortality rate, and (4) they were reported in English, Dutch, or French.
In cooperation with an information specialist of the KU Leuven Libraries—Désiré Collen Learning Centre, a search strategy was designed (Table 1). Electronic searches were conducted in the Medline, CENTRAL, CINAHL, Embase, and Web of Science databases to identify relevant publications published up to May 2023. We searched for full-text manuscripts that adhered to the predefined eligibility criteria. Subsequently, we screened reference lists for additional eligible studies. Authors were not contacted for additional data as there was no need to.

Table 1. Search strings applied in different databases.
Using Rayyan Collaborative Systematic Review Software®, two reviewers (G.P & F.D.B) independently screened all titles, abstracts, and full-text publications of the manuscripts identified in the literature search as potentially relevant. Disagreements were resolved by consulting a third independent reviewer (M.S.). During the different stages of the selection process, references were managed using EndNote 20 (Clarivate Analytics, EndNote desktop, Version 20. 2021).
Data were extracted by one reviewer (G.P.) and checked by the second reviewer (F.D.B.). Data were extracted using specific marking colors to fit the outcomes of interest. Each color represented an outcome of interest. Doing so, it was transparent which article contained information on which outcome.
The risk of bias in the included studies was assessed by one reviewer (G.P.) and verified by the second reviewer (F.D.B.). Disagreements were resolved by consensus or by consulting the third reviewer (M.S.). Different sources were used to evaluate the quality of the reviewed literature. The systematic reviews were assessed by the Risk of Bias Assessment Tool for Systematic Reviews (ROBIS). The following aspects were evaluated to identify concerns with the review process: study eligibility criteria, methods of study identification and selection, data collection and study appraisal, synthesis, and findings (6).
The observational studies were assessed using the revised and validated version of the Methodological Items for Non-Randomized Studies (MINORS). The following items were included: clearly stated aim, inclusion of consecutive patients, prospective data collection, endpoints appropriate to the aim of the study, unbiased assessment of the study endpoints, follow-up period appropriate for the aim of the study, loss to follow-up <5%, and prospective calculation of the study size. In the case of a comparative study, the following additional criteria were assessed: adequate control group, contemporary groups, baseline equivalence, and adequate statistical analysis. The appraisal questions were rated “2” if the criterion was reported adequately, “1” when the criterion was reported but inadequately, “0” if the criterion was not met or not reported, and “N/A” when the criterion was not applicable for the assessed study. An overall score was calculated with a max of 16 or 24 points for non-comparative and comparative studies, respectively (7). For the quality assessment of the expert opinions, the Johanna Briggs Institute (JBI) Critical Appraisal Checklist for opinion papers was used. The following areas were evaluated: clear identification of the source, the field of expertise of the source, correlation of the central focus with outcomes of interest, sufficient congruency and logical analytical process, references to the extant literature, and logical defense of any incongruence with sources (8).
A narrative synthesis of the included systematic reviews and expert opinions was complemented with the descriptive statistics of the observational studies within each reported outcome: surge capacity, AEs, and mortality rates. No meta-analysis was performed.
The electronic literature search identified 21,259 unique records (Figure 1). After title and abstract screening, the full texts of 24 potentially eligible records were evaluated. Thirteen records were excluded. Of four studies, the full text could not be retrieved, six studies described no outcome of interest, and three studies assessed the wrong study population. The remaining 11 full-text publications met the inclusion criteria. By screening the reference lists, 5 additional studies were identified, resulting in a total of 16 included studies.
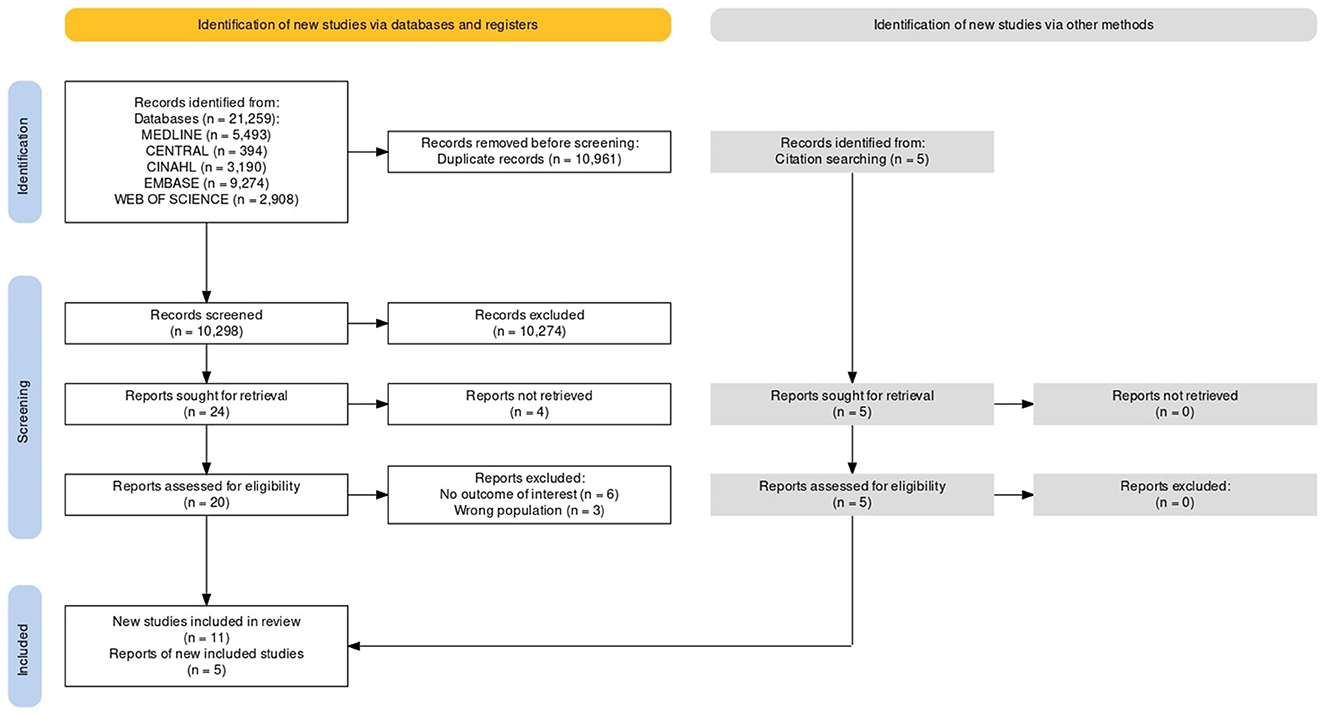
Figure 1. Study selection.
Two reviews, five expert opinions, and nine observational studies were included (Table 2). Of these, six studies were conducted in the United States, six in Europe, one in the United Kingdom, one in Iran, and two in Australia. Almost all studies covered the main outcome of “surge capacity,” five studies also “mortality,” and six studies also “AEs.” Of the observational studies, four studies had a cross-sectional design, and five studies had a longitudinal design. The sample sizes ranged from 150 to 1,352. For the longitudinal studies, the time points ranged from 2 to 6 days of data collection.
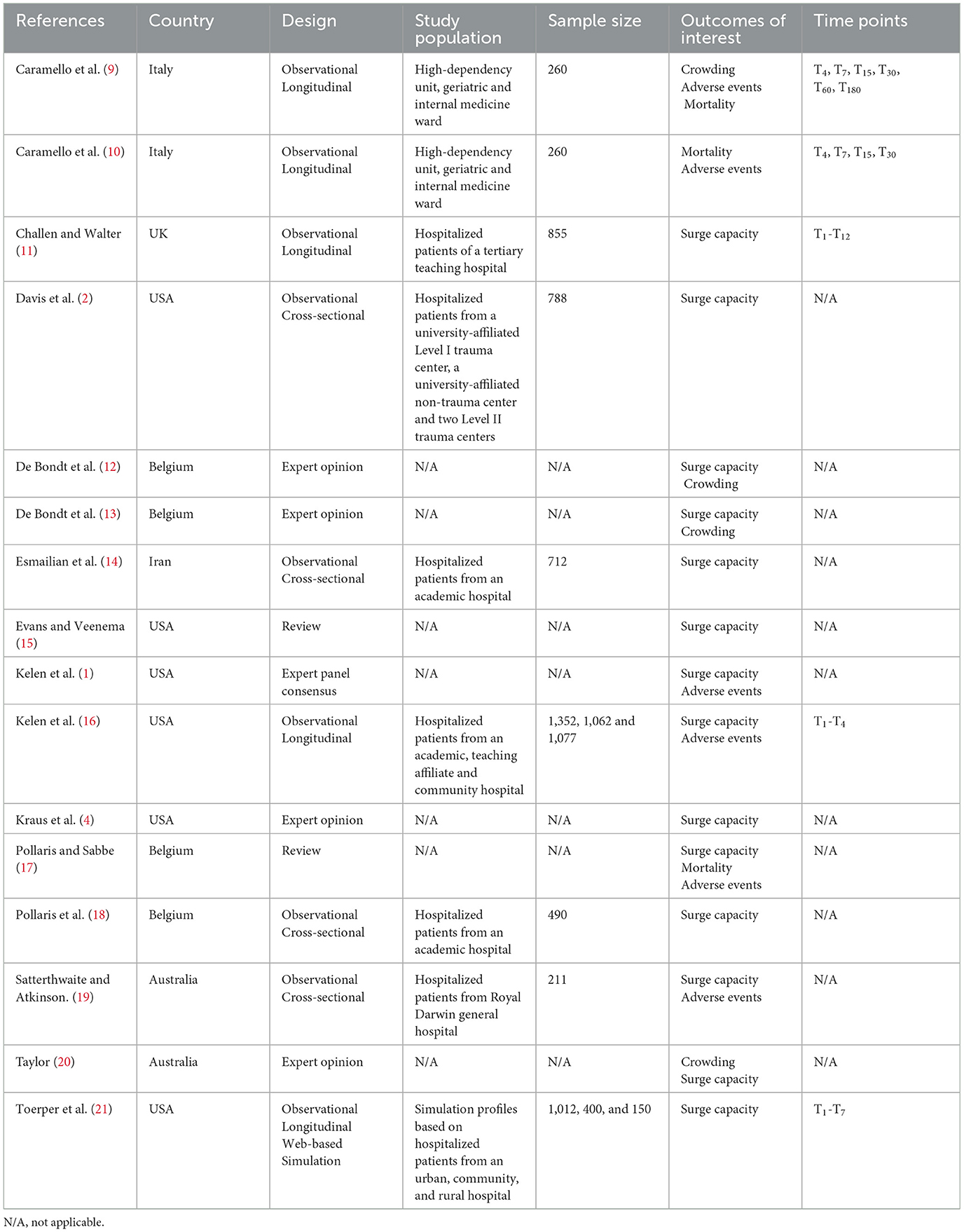
Table 2. Study characteristics.
With a mean score of 12, the overall risk of bias in the included observational studies (Table 3) was moderate. The following items were inadequately reported: “aim of the study” (n = 2), “appropriate endpoints” (n = 2), “assessment of the study endpoint” (n = 2), and “appropriate follow-up period” (n = 2). Only three studies adequately reported their loss to follow-up, and no study mentioned a prospective calculation of the study size. Of the systematic reviews, one study had an overall low concern on all the items of the ROBIS, while the other only showed a low concern regarding the specification of their eligibility criteria (Table 4). The overall risk-of-bias assessment of the expert opinions, using the JBI Critical Appraisal Checklist for opinion papers, was good. Every study met each criterion (Table 5).
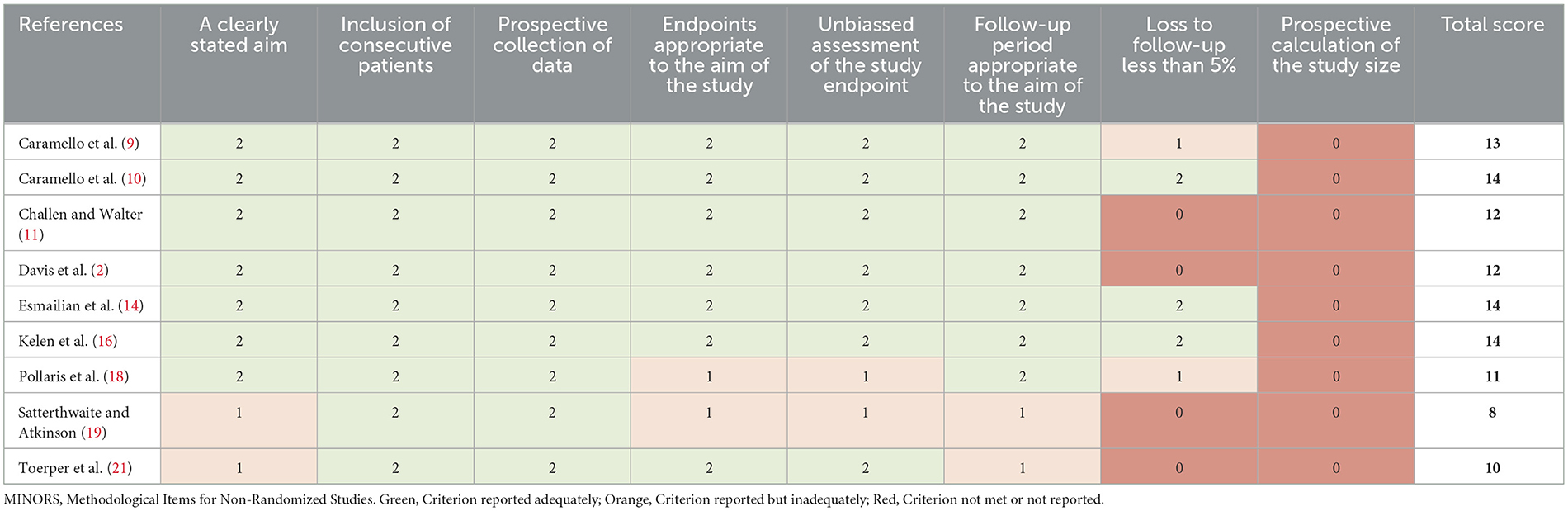
Table 3. Risk of bias observational studies (MINORS).
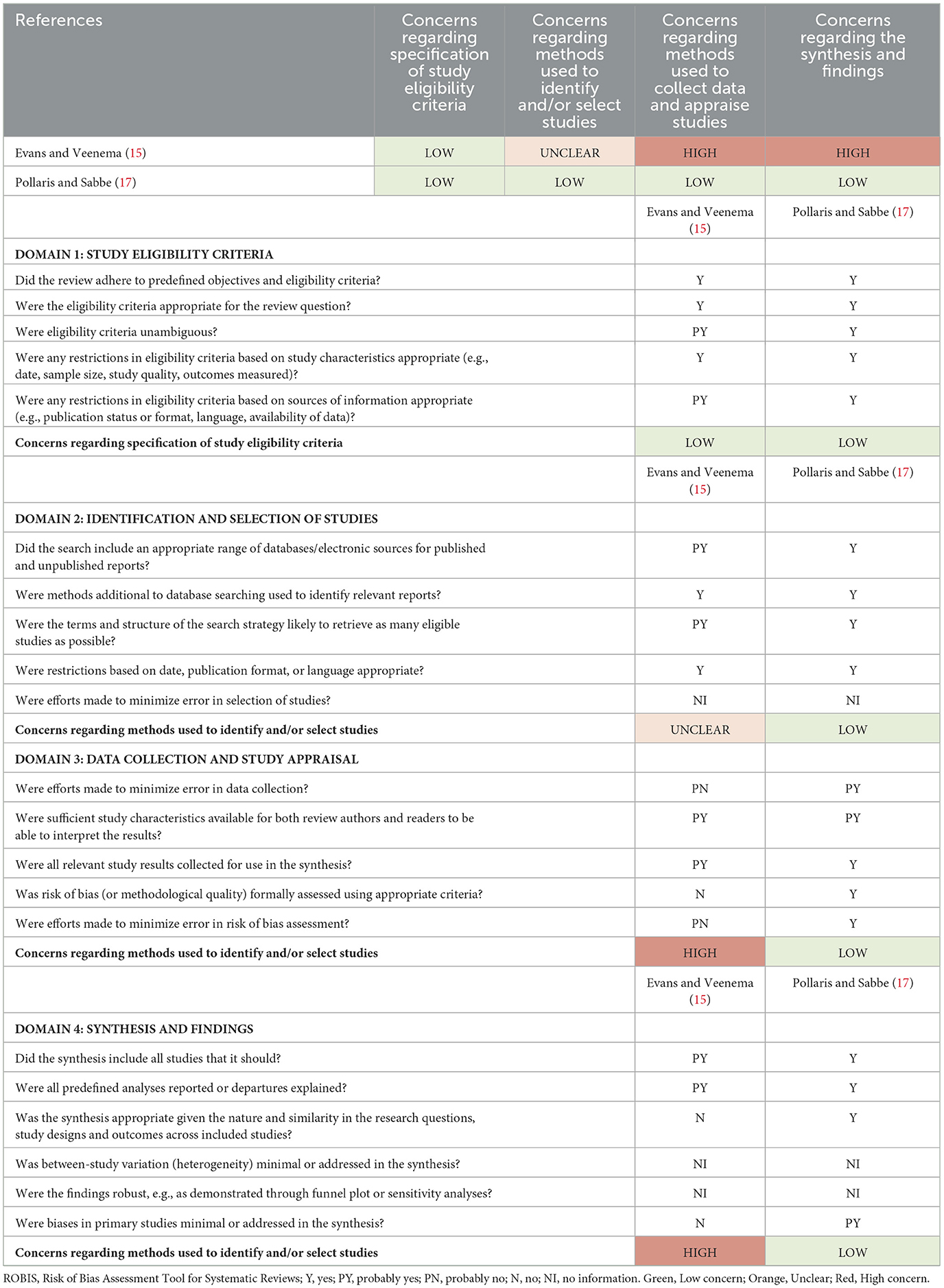
Table 4. Risk of bias systematic reviews (ROBIS).
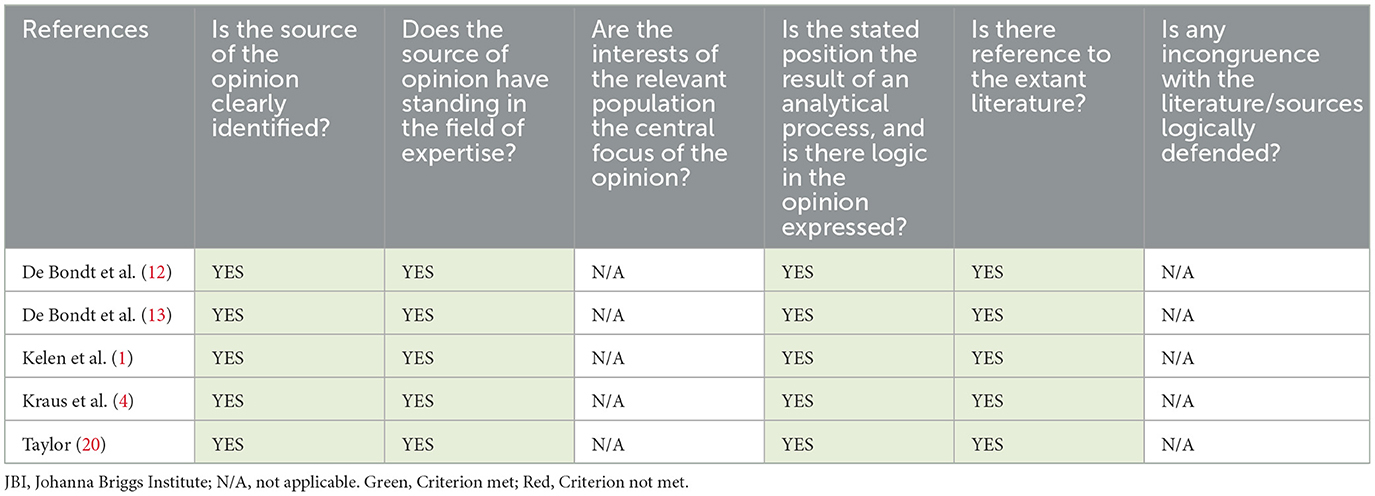
Table 5. Risk of bias expert opinions (JBI).
Before RT was civilianized into the health care system, a cross-sectional American study tried to determine the number of acute care beds that could be made available within four hospitals in the event of a theoretical MCI. Nurse managers and physicians assessed the inpatients' dischargability of a 360-bed university-affiliated Level I trauma center, a 120-bed university-affiliated non-trauma center, a 372-bed Level II trauma center, and another 280-bed Level II trauma center. The overall percentage of beds that could be made available was comparable for all hospitals. Approximately 33% was dischargeable within 24 h and 50% within 72 h. Of all patients, 25% were assessed to be transferable to a hypothetical on-site nursing facility whereas the rest were ready for early discharge home (2). Similar results were found for an 855-bed tertiary teaching hospital in the United Kingdom, where its discharge capacity was measured over a period of 12 days using a survey. Within 4 h, 147 beds could be made available, of which 35% were created by speeding up the discharge process for patients planned to be discharged later that day. Within 12 h, an additional 155 beds could be made available by transferring patients to their previous hospital (after specialized treatment), discharging those awaiting, carrying out investigations on an outpatient basis, or accelerating senior medical review. Interestingly, 55 of these additional beds could only be achieved if the UK Trust could arrange urgent placements for 25 patients in home care, 10 in nursing or residential care, and 20 in interim therapy-supported beds. So 302 beds (36% of total capacity) could be made available within 12 h by combining early discharge and cancellation of (semi-)elective admissions (11). Around the same time, in 2006, the American Joint Commission International stated that during an MCI, hospitals should be able to expand care and resources for incoming patients while continuing to care for their current inpatients for up to 96 h before outside assistance can be expected (16, 17). To address this capacity mismatch, an American RT framework was developed by 39 experts during a warfare analysis laboratory exercise. It comprehended to be a safe discharge protocol for inpatients and a reallocation of hospital resources to the incoming MCI patients who are in greater need of acute medical care. Patients who do not require major medical assistance for the upcoming 96 h and who only have a small risk of developing a complication due to their early discharge will be identified. This is based on a risk assessment for consequential medical events (CME). The consensus definition of a CME was “unexpected death, irreversible impairment, or reduction in function within 72 h of hospital discharge for which an in-hospital critical intervention would be initiated to stabilize or ameliorate the medical disorder.” The expert panel assembled a list of 28 critical interventions (CIVs) and weighted them on a 10-point Likert scale in order of criticalness and the possibility that the CIVs would lead to a CME if withdrawn or withheld from the patient (due to early discharge) (1). Furthermore, a five-category disposition classification system (minimum, low, moderate, high, and very high) was developed. Each category contains an upper limit of risk tolerance for a CME. For categories 1 through 5, the upper limits of risk tolerance were 3.8, 11.7, 33.1, 61, and 92.3%, respectively. This means that if category 1 holds 100 inpatients, it is tolerated by the expert panel that approximately four patients will develop a CME due to their early discharge. In February 2006, the inpatient disposition classification system was tested in a prospective study with a randomized block design. Controlling for day of the week, inpatient units from an academic center, a teaching affiliate, and a community hospital were included during a 19-week period, yielding a total of 3,491 included patients. As it would be unethical to withdraw or withhold CIV from patients for study purposes, a proxy was determined. Patients were considered to have a CIV if a continuous CIV, initiated before T0, remained in place or if any CIV occurred after T0. In the academic center, teaching affiliate, and community hospital, 33% (95% CI [29%, 36%]), 39% (95% CI [33%, 45%]), and 48% (95% CI [41%, 56%]) of beds, respectively, could be made available on T0 by applying the RT discharge protocol. Furthermore, applying the concept of RT created the majority (50, 55, and 59%, respectively) of the surge bed creation (16).
A few years later, the Royal Darwin Hospital responded to the Australian Ashmore Reef disaster. The 353-bed general hospital was asked to take on 30 casualties with blast injuries. Not only were all planned admissions canceled and the external disaster plan activated, but a multidisciplinary RT team was also set up to assess inpatients' suitability for (early) discharge and complete all necessary clinical and administrative requirements to do so. All patients with a planned discharge that day were discharged earlier in time, and an extra 19 patients were discharged at least 1 day earlier than planned. Combining all surge capacity strategies, 56 beds (16% of capacity) were made available to accommodate the blast victims (19).
In 2017, a Belgian study published the development of an information technology application, based on the original American RT framework, to guide clinical decision-making during the RT selection process. The application was set up to detect hospitalized patients who unequivocally cannot be discharged early in disaster circumstances. By doing so, the number of patients that need to be multidisciplinary assessed for early discharge can be reduced, making the RT selection process more efficient. During a 3-week period in March 2015, a pilot study was conducted at the University Hospitals of Leuven to test the performance of the Reverse Triage Tool Leuven (RTTL). Using the original framework as a gold standard in the contingency table, a χ2 of 12.024 (df = 1), with a p-value of 0.002, a specificity of 0.74, and a negative predictive value of 0.95, was achieved. The use of the RTTL reached a reduction of 63.9% of patients who needed a multidisciplinary evaluation for potential early discharge (18).
In 2018, a web-based simulation tool for emergency planners was made publicly available by the U.S. National Center for the Study of Preparedness and Catastrophic Event Response. Based on the emergency planners' input, a Monte Carlo simulation algorithm can forecast the hospital's surge capacity over a 7-day period. It is even possible to focus on a specific hospital service, intensive care unit (ICU), or inpatient ward. Multiple strategies to expand surge capacity can be individually selected and interactively evaluated. These strategies include the opening of unlicensed beds, canceling elective admissions, and implementing RT. Furthermore, the tool is sufficiently robust to allow self-definition and individualize the simulation for every hospital separately, with their own distinct characteristics. It is based on some fixed assumptions from previously published evidence (e.g., the estimated decrease of 25% of normal ED admissions during an MCI). To maximize the generalizability of the application, three representative profiles were created, based on real bed and patient flow of a 1,012-bed urban, a 400-bed community, and a 150-bed rural hospital. Throughout the sensitivity analysis (1,000 simulation runs per experiment setting) it was clear that exclusively performing RT for inpatient units (general wards) had a very limited impact on surge capacity for the small and medium-sized hospitals because the ICU is the limiting resource. Combining all surge capacity strategies, the relative maximal additional surge capacity was noted in the urban hospital (95% CI [14.1%, 16.6%]), followed by the community (95% CI [6.9%, 7.6%]), and the rural hospital (95% CI [4.9%, 6%]) (21).
Furthermore, in a 700-bed academic hospital in Iran, the potential role of RT to create additional surge capacity was also investigated. The 10 most common diseases within each ward (n = 41), including ICU and pediatric wards, were listed. Subsequently, an expert panel was appointed to agree on clinical decision rules, focused on the specialty of each ward, to reflect the possibility of early discharge. At the time of the study, the hospital had a mean bed occupancy rate (BOR) of 80% (140 vacant beds). By using their predefined RT protocol, an additional 108 hospitalized patients (20%) could be safely discharged early, resulting in a total of 248 vacant beds (14). Last, the role of nurses in the RT selection process was investigated in an American systematic review. Nurses have hourly contact with inpatients and could hold important clinical data for early discharge decision-making (e.g., functional status, resource needs, or acuity) (15).
Patients discharged early may experience a discontinuity in care as they transition, making them vulnerable to develop an AE. This could lead to a return visit to the ED for further assessment, treatment, and even readmission. These bounce-back patients will burden the already-strained EDs' and hospitals' limited resources, time, and staff (17).
To assess the risk of developing an AE due to early discharge, an American expert panel developed a five-category patient disposition classification system in 2006. It is based on a list of 28 CIVs that would lead to an AE if withheld or withdrawn from the patient. Patients with approximately the same risk of developing an AE due to their early discharge are grouped into a category. Furthermore, they added an upper limit of risk tolerance, respectively, 3.8, 11.7, 33.1, 61, and 92.3% for categories 1 through 5. The corresponding percentage of each category corresponds to the accepted number of patients that would develop an AE due to their early discharge (1).
In 2009, 50 inpatient units (excluding the ICU and pediatrics) of three capacity-constrained hospitals were prospectively assessed for theoretical early discharge. Patients who did not require any CIV for 4 consecutive days, were deemed suitable for early discharge. If a critical intervention had been initiated following theoretical discharge, this patient would have experienced an AE due to early discharge. Among those who were selected as “suitable for early discharge,” none required a critical intervention within 96 h post-discharge, whereas 8% required a critical intervention beyond 96 h (16).
In the response to the Ashmore Reef disaster in Australia, 19 patients were discharged earlier than planned, of which only one bounced back to the ED for continued treatment and readmission for his original condition (19).
To evaluate the risk of physiological deterioration due to early discharge, an Italian observational study prospectively assessed 260 inpatients of medical divisions at a Level II Italian hospital. An RT score, based on the original American framework, was calculated for each patient. If a patient needed more than one CIV, the CIV with the highest ranking was decisive for determining the RT score. This RT score was then compared with three other prognostic scores: the National Early Warning Score (NEWS), the Sequential Organ Failure Assessment (SOFA), and the Charlson Comorbidity Index (CCI). A positive correlation between the RT score and the NEWS (Spearman r 0.52, p < 0.001), SOFA score (Spearman r 0.29, p < 0.001), and CCI score (Spearman r 0.21, p < 0.001) was found. The need for resources (RT score) increased in parallel with an ascending risk of physiological deterioration (NEWS), severity of organ damage (SOFA), and clinical complexity (CCI). The RT score and NEWS were the most concordant. Subsequently, the same research group assessed 25 inpatients (9.6%) who were identified as suitable for early discharge (RT score <4) for death and readmission at 4, 7, 15, 30, and 60 days after the study visit (T0). The need for a CIV, transfer (back) to a higher level of care, or readmission at the ED was used as an ethical proxy to test the safety of the RT score. One patient (4%) died 10 days after T0, zero patients bounced back to the ED before T30, three patients (12%) needed a CIV in the ED between T30 and T60, and one patient (4%) got readmitted after T60 (9).
In the previous described Italian study, one patient out of 25 (4%) who were assessed as suitable for theoretical early discharge died 10 days after T0 (9). Furthermore, another study stated that RT could ameliorate the 30-day in-hospital mortality rate in daily crowding as the mortality risk increases by 53% once the patient processing time in the ED exceeds 4 h (17).
Applying RT selection to identifying inpatients who do not need in-hospital interventions for the coming days has been studied for MCIs before, but some have stated that it can be useful for coping with daily surges as well. By simultaneously prioritizing ED patients who need urgent medical care and hospitalized patients ready for discharge, a daily hospital surge capacity could be achieved (13). Nevertheless, early discharge could increase the risk of developing a CME which would require a readmission, an additional burden for the already-strained ED (10). Interestingly, it has been suggested that early discharge of inpatients could decrease the admission delay in EDs and therefore also could reduce crowding. However, today, no universal, safe early discharge criteria for non-MCI conditions exist. Caramello et al. (10) tried to fill the gap. They prospectively assessed 260 inpatients of medical divisions in a Level II Italian hospital. If inpatients had an RT score lower than 4 (9.6%, n = 25), they were identified as suitable for (hypothetical) early discharge after multidisciplinary evaluation. Those patients were discharged significantly earlier (3.5 vs. 8 days after T0, p = 0.0002). In addition, the Identification of Seniors At Risk, HOSPITAL score, and the Groningen Frailty Index readmission screening tools were applied to further increase the specificity of the RT cutoff for daily crowding. The HOSPITAL score showed the highest compliance with the RT score (84%). The RT score had a high specificity (95%) on its own, but it was even higher when associated with readmission screening tools (10). As the tolerated risk of 12% for developing a CME in a disaster setting will not be tolerable in ED crowding situations, a lower cutoff of <4% has been proposed for daily crowding (1, 13, 20). Furthermore, a Delphi study with a European expert panel recently discussed early discharge criteria within a universal patient disposition classification system that will be applicable for MCI and daily crowding (12, 13).
Using the Grading of Recommendations Assessment, Development and Evaluation approach, we found that the quality of evidence was high for the outcome surge capacity, moderate for adverse events, and very low for mortality (Table 6) (22).
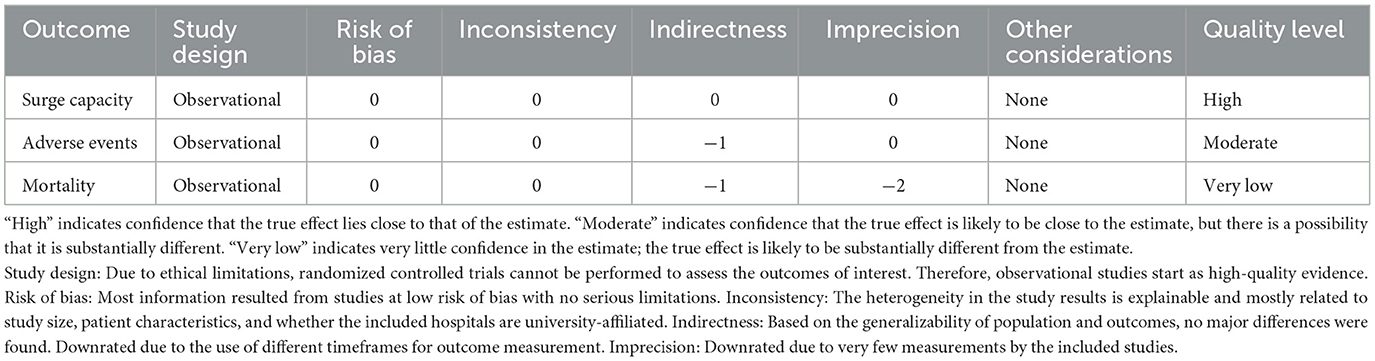
Table 6. Grading of recommendations, assessment, development, and evaluations for each outcome.
Throughout the studies, different methods were used to calculate the surge capacity that was made available due to the implementation of early discharge RT protocols. Some used the hospital's total bed capacity (occupied and empty beds) as the denominator, whereas others used only the initial number of occupied beds as the denominator. This should be taken into consideration when comparing results as it could lead to an overestimation of the effect of RT in certain studies. For example, the Al-Zahra Hospital had a BOR of 80% at the time of the study (140 out of 700 beds were vacant). Using RT, an additional 108 hospitalized patients (20%) could be discharged. Nevertheless, the study concluded that a total of 248 beds (35%) could be provided following RT discharge protocols (14). Across studies, the overall percentage of AEs and mortality rates due to early discharge are rather low. In the American study, no patient required a critical intervention within 96 h post-discharge, whereas only 8% required a critical intervention beyond 96 h (16). In the response to the Australian Ashmore Reef disaster, one patient bounced back to the ED for further treatment and readmission (19). In the Italian observational study, one patient (4%) died 10 days after T0, zero patients bounced back to the ED, three patients (12%) needed a CIV in the ED between T30 and T60, and one patient (4%) was readmitted after T60 (9). Notably in this latter study, only 25 of 260 patients (9.6%) had an RT score lower than 4 and were therefore considered eligible for discharge. This could be because the study population included 60% more patients from the high-dependency unit and geriatric wards than the internal medicine wards. Given the higher age and comorbidity prevalence in these populations, this probably results in an underestimation of the real proportion of patients who could be eligible for discharge. Furthermore, there was also a high number of denied informed consents due to cognitive impairment and unstable patient conditions. As these frail patients could not be included in the study, an underestimation of the AE and mortality ratio post-discharge is possible (9).
Moreover, the lack of available places in residential care is related to the shortage of free hospital beds in many hospitals. Therefore, patients stay hospitalized while they wait for a residential spot. This undermines the effect of the RT selection process. In the study of the 855-bed tertiary teaching hospital in the United Kingdom, an extra 55 patients (6.4% of total capacity) could be discharged immediately if the primary care trust could arrange an urgent placement for them in a home or residential care (11).
A crucial aspect of the RT selection process is the multidisciplinary discharge team members. They will have to make a final assessment of the patient's ability to be safely discharged with no or minimal negative consequences. When the assessments of nurse managers were compared with those of the attending physicians, interesting differences emerged. Because of their different points of view, both nurses and physicians should be part of the multidisciplinary discharge team as they are complementary (2).
Up to now, no universal or European consensus has existed concerning safe (early) discharge criteria for MCIs or daily crowding. It is of utmost importance that further investigation is to be continued to address this knowledge gap (13). Moreover, as medical data are progressively integrated into electronic health records, key prognostic variables (e.g., vital signs, comorbidities, and laboratory values) can be gathered and updated in real time. This way, a real-time discharge risk score could be calculated at the individual patient level. This risk-based disposition classification system could be used to guide clinical decision-making during MCIs or daily surges. In ascending order of risk, discharges would take place (1, 13).
Due to the heterogeneity of the included studies, the interpretation of the results should be taken with caution. The most prominent differences were related to study size, university affiliation, health care system, and patient characteristics. University-affiliated hospitals have a higher occupancy of critically ill patients and therefore potentially a higher care burden, resulting in a lower number of patients ready for early discharge. The differences in the U.S., U.K., and EU health care systems are also noteworthy. Not only does access to health care play an important role, but so, too, does the way health care is organized on a societal level. Last, the types of patients being assessed for early discharge vary slightly across studies. The different patient characteristics (e.g., comorbidities, age, and level of dependency) could influence the results.
Implementing the RT principle in MCIs to guide the early discharge of adult inpatients can create additional surge capacity with a minor occurrence of AEs due to their early discharge. A final assessment by a multidisciplinary discharge team, consisting of nurses and physicians, is crucial to ensure a minimal risk of developing a CME. Furthermore, a few already-published studies have elaborated the potential use of RT in daily ED crowding situations as well. Nevertheless, further research needs to be performed.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author.
GP: Conceptualization, Funding acquisition, Methodology, Project administration, Writing—original draft. FD: Writing—review & editing. MS: Conceptualization, Funding acquisition, Supervision, Writing—review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. KU Leuven and the Flemish Government by the Special Research Fund project C24M/21/034.8.
The authors wish to thank Krizia Tuand, the biomedical reference librarian of the KU Leuven Libraries—Désiré Collen Learning Centre (Leuven, Belgium), for her help in conducting the systematic literature search.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Kelen GD, Kraus CK, McCarthy ML, Bass E, Hsu EB, Li G, et al. Inpatient disposition classification for the creation of hospital surge capacity: a multiphase study. Lancet. (2006) 368:1984–90. doi: 10.1016/S0140-6736(06)69808-5
2. Davis DP, Poste JC, Hicks T, Polk D, Rymer TE, Jacoby I, et al. Hospital bed surge capacity in the event of a mass-casualty incident. Prehosp Disaster Med. (2005) 20:169–76. doi: 10.1017/S1049023X00002405
3. Emmerich N. Ought conscientious refusals to implement reverse triage decisions be accommodated? J. Bioeth Inq. (2020) 17:783–7. doi: 10.1007/s11673-020-10042-7
4. Kraus CK, Levy F, Kelen GD. Lifeboat ethics: considerations in the discharge of inpatients for the creation of hospital surge capacity. Disaster Med Public Health Prep. (2007) 1:51–6. doi: 10.1097/DMP.0b013e318065c4ca
5. Moher D, Liberati A, Tetzlaff J, Altman DG, PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. PLoS Med. (2009) 6:e1000097. doi: 10.1371/journal.pmed.1000097
6. Whiting P, Savović J, Higgins JP, Caldwell DM, Reeves BC, Shea B, et al. ROBIS: a new tool to assess risk of bias in systematic reviews was developed. J Clin Epidemiol. (2016) 69:225–34. doi: 10.1016/j.jclinepi.2015.06.005
7. Slim K, Nini E, Forestier D, Kwiatkowski F, Panis Y, Chipponi J, et al. Methodological index for non-randomized studies (minors): development and validation of a new instrument. ANZ J Surg. (2003) 73:712–6. doi: 10.1046/j.1445-2197.2003.02748.x
8. McArthur AKJ, Yan H, Florescu S. Chapter 4: systematic reviews of text and opinion In:E. Aromataris, Z. Munn, editors JBI Manual for Evidence Synthesis, Miami, FL: JBI (2020). doi: 10.46658/JBIRM-17-04
9. Caramello V, Marulli G, Reimondo G, Fanto' F, Boccuzzi A. Comparison of reverse triage with national early warning score, sequential organ failure assessment and charlson comorbidity index to classify medical inpatients of an Italian II level hospital according to their resource's need. Int Emerg Med. (2019) 14:1073–1082. doi: 10.1007/s11739-019-02049-9
10. Caramello V, Marulli G, Reimondo G, Fanto' F, Boccuzzi A. Inpatient disposition in overcrowded hospitals: is it safe and effective to use reverse triage and readmission screening tools for appropriate discharge? An observational prospective study of an Italian II level hospital. Int J Clin Pract. (2019) 73:e13281. doi: 10.1111/ijcp.13281
11. Challen K, Walter D. Accelerated discharge of patients in the event of a major incident: observational study of a teaching hospital. BMC Public Health. (2006) 6:108. doi: 10.1186/1471-2458-6-108
12. De Bondt F, Pollaris G, Sabbe M. How to reach European consensus on reverse triage? Acta Clin. Belg. (2021) 76:8–9.
13. De Bondt F, Pollaris G, Sabbe MB. Can a reverse triage clinical decision support tool create sufficient surge capacity and reduce emergency department crowding? Euro. J Emerg Med. (2022) 29:16–7. doi: 10.1097/MEJ.0000000000000855
14. Esmailian M, Salehnia MH, Shirani M, Heydari F. Reverse triage to increase the hospital surge capacity in disaster response. Adv J Emerg Med. (2018) 2:e17. doi: 10.22114/AJEM.v0i0.48
15. Evans CA, Veenema TG. The role of the nurse in reverse triage: a review of the literature. Health Emerg Disast Nurs. (2017) 4:5–11. doi: 10.24298/hedn.2016-0015
16. Kelen GD, McCarthy ML, Kraus CK, Ding R, Hsu EB, Li G, et al. Creation of surge capacity by early discharge of hospitalized patients at low risk for untoward events. Disaster Med Public Health Prep. (2009) 3:S10–S6. doi: 10.1097/DMP.0b013e3181a5e7cd
17. Pollaris G, Sabbe M. Reverse triage: more than just another method. Euro J Emerg Med. (2016) 23:240–7. doi: 10.1097/MEJ.0000000000000339
18. Pollaris G, Note S, Desruelles D, Sabbe M. Novel IT application for reverse triage selection: a pilot study. Disaster Med Public Health Prep. (2018) 12:599–605. doi: 10.1017/dmp.2017.115
19. Satterthwaite PS, Atkinson CJ. Using “reverse triage” to create hospital surge capacity: Royal Darwin Hospital's response to the Ashmore Reef disaster. Emerg Med J. (2012) 29:160–2. doi: 10.1136/emj.2010.098087
20. Taylor MD. Reverse triage: useful for day-to-day access block? Lancet. (2006) 368:1940–1. doi: 10.1016/S0140-6736(06)69785-7
21. Toerper MF, Kelen GD, Sauer LM, Bayram JD, Catlett C, Levin S, et al. Hospital surge capacity: a web-based simulation tool for emergency planners. Disaster Med Public Health Prep. (2018) 12:513–22. doi: 10.1017/dmp.2017.93
Keywords: reverse triage, surge capacity, adverse events, mass casualty incidents, crowding, patient discharge, risk assessment
Citation: Pollaris G, De Bondt F and Sabbe M (2023) Reverse triage: a systematic review of the literature. Front. Disaster Emerg. Med. 1:1303809. doi: 10.3389/femer.2023.1303809
Received: 28 September 2023; Accepted: 16 November 2023;
Published: 04 December 2023.
Edited by:
Derrick Tin, Beth Israel Deaconess Medical Center and Harvard Medical School, United StatesReviewed by:
Ramazan Aslan, Ardahan University, TürkiyeCopyright © 2023 Pollaris, De Bondt and Sabbe. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gwen Pollaris, Z3dlbi5wb2xsYXJpc0BrdWxldXZlbi5iZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.