 Jieqiong Zhang1†
Jieqiong Zhang1† Jun Jiang
Jun Jiang Yan Hua
Yan Hua
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Disaster Emerg. Med. , 28 August 2023
Sec. Emergency Health Services
Volume 1 - 2023 | https://doi.org/10.3389/femer.2023.1169851
This article is part of the Research Topic Advancements and Challenges in Mass Gathering Medicine: Enhancing Health Outcomes View all 6 articles
Background: Triage is an initial important step in emergency medical rescues for mass casualty incidents, and different triage systems are used in practice. However, quantitative analysis-based evidence comparing these triage systems in mass casualty incidents is limited.
Objective: To compare the performance of three triage systems, simple triage and rapid treatment (START), abbreviated scoring method for combat casualty (ASMcc), and sort assess lifesaving interventions treatment/transport (SALT) system, for simulated disaster patients, as assessed by medical undergraduate students.
Methods: Medical undergraduates were recruited and randomly divided into three groups to evaluate the performance of the three triage systems by using simulated disaster patient cards. The triage time, accuracy, and overtriage and undertriage rates were analyzed among groups. Furthermore, a questionnaire survey was used to investigate the responses of the participants regarding learning, practice, and satisfaction among the three triage systems.
Results: A total of 30 participants were included in the study. The participants were male medical undergraduate students with a mean age of 20.73 ± 0.45 years. ASMcc had the highest accuracy of 75% with the lowest over-triage rate of 20%, SALT had the lowest undertriage rate of 19%, and START had the shortest triage time of 12.68 ± 4.96 min (all P < 0.05). Furthermore, the results of the questionnaire survey showed that START was easy to learn and recall with high efficiency and, among the three systems, had the highest satisfaction ratings from the participants.
Conclusion: The results of the study showed that the three triage systems had their own characteristics and advantages, and they are all suitable for use in mass casualty incidents. Further studies involving more triage systems with data based on real conditions are recommended.
Triage is an initial and important step in emergency medical rescues for mass casualty incidents (MCIs) (1). In the case of limited medical resources such as medical personnel and emergency medications, the treatment order of the injured is differentiated according to the severity of the injury (2). If the triage is nonstandard and unreasonable, there may be undertriage or overtriage, and either of these will greatly reduce treatment efficiency (3). Therefore, it is important to develop an effective triage system for the rational application of first-aid resources and the optimization of the treatment process of the wounded (4).
Many triage systems have been used in practice for MCIs or disaster rescue worldwide, and they have the common goal of rapid classification of patients for efficient medical care (3). The well-known triage systems include the Simple Triage and Rapid Treatment (START) triage tool, the sort assess lifesaving interventions treatment/transport (SALT) system, the field triage score (FTS), the sequential evaluation method for Massive Hemorrhage, Airway, Respiration, Circulation and Hypothermia (MARCH), the abbreviated scoring procedure method for combat casualty (ASMcc), and the circulation, respiration, abdomen, motor and speech (CRAMS) scale (3–5). Among these systems, the START triage tool is simple and quick, which can be briefly explained as the “30-2-can-do” principle. Due to its simplicity in implementation, this method has been widely used in NATO armies, such as that of America, Australia, Israel (6). The SALT system includes overall evaluations and individual evaluations, which are easy to implement, easy to grasp, accurate and reliable, and it has been widely applied for the assessment of injuries in disaster rescue (7). The ASMcc method is widely used in the Chinese army and is included in the previous and updated Rules for Combat Casualty Care in China. The evaluation indicators for the ASMcc method include respiratory rate, systolic pressure, and Glasgow coma index (8, 9). In the AMSCC, the maximum score is 12. Those with a score of 5 or less are the most critically wounded, 6–9 have severe injuries, 10–11 have moderate injuries. Patients scoring 12 have minor injuries (10).
However, in practice, these triage systems may have many problems, such as parallel methods, different effects, population specificity, age limitations, and diversity of complexity. Furthermore, there is no general consensus on which triage system is better, and quantitative analysis-based evidence comparing these triage systems in mass casualty incidents is limited (5). Therefore, this study aimed to compare the performance of three triage systems, the START, SALT and ASMcc systems, for simulated disaster patients, as assessed by medical undergraduate students. Provide a basis for selecting MCIs classification methods through comparison of effectiveness and evaluation.
From May to June 2022, a total of 30 junior undergraduate students majoring in clinical medicine at a military medical school in China were recruited for the study. The inclusion criteria were junior undergraduate students majoring in clinical medicine who had learned certain basic medical and clinical knowledge; participating in the elective course “prehospital first aid technology”; and agreeing to participate in the study. Those who provided incomplete survey data or were not able to follow the study procedure were excluded from the study. The prerequisite courses for students include medical and clinical courses such as “Normal Human Morphology,” “Clinical Introduction,” and “Fundamentals of Diagnosis and Treatment,” with a certain knowledge background, which is essential for learning emergency medical rescues for mass casualty incidents.
The included participants were randomly and equally divided into three groups, A, B, and C, with 10 participants in each group, by using the random number method. The crossover study design was adopted for each group to use the three triage systems by randomized sequence to avoid potential bias on the results (Table 1) (11, 12).
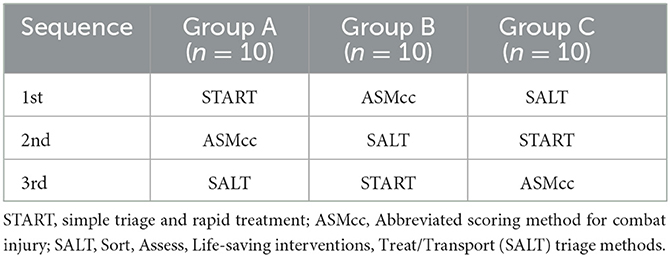
Table 1. Sequence procedure of the study.
A total of 30 typical cases of injuries in earthquake scenarios were simulated by using simulated disaster patient cards, which used the earthquake disaster of the Sichuan area as the background. The injuries were mainly crush injury, blast injury, impact injury, psychological stress. The injury positions included head, upper limbs, lower limbs, waist abdomen, chest, back, pelvis and perineum, neck, spinal cord. Furthermore, among the 30 casualties, the proportion of severe (Severe trauma, life-threatening, requiring immediate first aid.), moderate (The injury is not life-threatening temporarily, but needs prompt treatment.) and light (Clear awareness, no life danger, able to walk, no special treatment.) injuries was 1:3:6, which consisted of 3 severe, 9 moderate, and 18 light injuries, with a random order of the patient numbers from P1 to P30 (13). Furthermore, a preliminary experiment was conducted to test the feasibility of the triage process.
All participants systematically studied the three triage systems by a unified short course, and the instructors conducted unified training before teaching.
After learning the three triage systems, each group of participants examined and classified all 30 simulated patients by using the three triage systems, START, SALT, and ASMcc, in sequence according to the presupposed order. The triage results were recorded based on the criteria of the three triage systems, including patient number, triage times, triage outcome.
Undertriage will lead to the delay of initiation of emergency aid and treatment for the more severely wounded and increase the number of potentially preventable deaths. Over-triage will lead to the non-critical patients being classified as needing emergency aid and treatment which results in the consumption of limited medical resources that could have been otherwise utilized for patients that need the interventions. Overtriage has also been associated with increased fatality rate (14).
A self-developed questionnaire was used to investigate the general demographic information including gender, age and satisfaction of the participants with the three triage systems. The questions about satisfaction included “Q1: What is the level of ease of learning?”; “Q2: What is the level of memorability of the triage system?” and “Q3: What is your satisfaction level with the efficiency of this triage method?”. The answers for the questions used the five-stage scoring method of Linkage, ranking from 1 to 5 (1 is the lowest score for unsatisfied, 5 is the highest score for very satisfied).
Finally, all participants were interviewed face to face and recorded for the following two aspects: “What do you think are the advantages and disadvantages of the three methods? Which triage system is satisfactory?” and “Do you have any further suggestions about the triage system based on your experience?”.
All completed questionnaires were checked by the research staff and missing or unclear responses were clarified before the participants left.
IBM SPSS Statistics version 20 (Chicago, Illinois, USA) was used for statistical analysis. Data were presented as or frequency as suitable. The measurement data were compared among the three groups with one-way analysis of variance followed by the post hoc pairwise comparison method, and the comparison of enumeration data was performed using the Chi-square test followed by pairwise comparison adjusted by the Bonferroni method. P < 0.05 was considered statistically significant.
A total of 30 male participants who were junior clinical undergraduate students were included in the study. The average age of the participants was 20.73 ± 0.45 years old, and the age difference between the three groups was not statistically significant (F = 2.34, P = 0.116).
According to the triage results, the accuracies of the START, ASMcc, and SALT systems were 60.44%, 74.67%, and 70.22%, respectively. The accuracy of the ASMcc system was the highest, followed by the SALT system. Compared with the START system, the accuracy ratings of the ASMcc and SALT systems were statistically significantly higher (all P < 0.05). Furthermore, the differences in the over-triage rates of 39%, 20%, and 31% among the STRAT, ASMcc and SALT systems, respectively, were statistically significant (all P < 0.05); however, no significant difference was found among the three triage systems in the undertriage rates, which were 21%, 26%, and 19%, respectively. The triage times were 12.68 ± 4.96 min, 17.82 ± 5.13 min and 13.34 ± 3.58 min for the START, ASMcc and SALT groups, respectively, with no statistically significant differences (Table 2). The result data is the completion time of 30 injuries, with an average time of one thirtieth for a single injury. The triage times were 0.423 ± 0.165 min, 0.445 ± 0.119 min and 0.594 ± 0.171 min for the START, ASMcc and SALT groups.
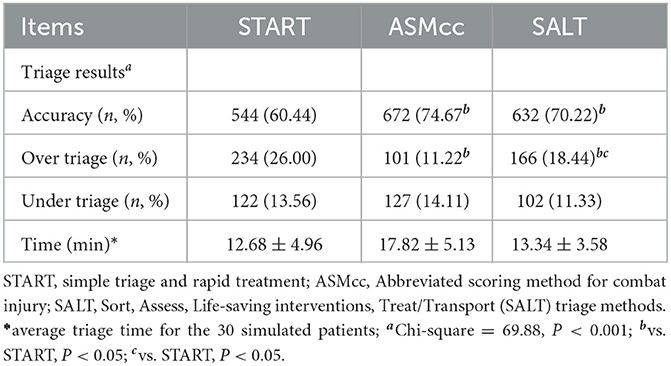
Table 2. The comparison results of triage practice among the three methods (n = 30).
From the results of the questionnaire survey, for the learning of the triage systems, START was the easiest system to learn compared to the other two systems (4.73 ± 0.59 vs. 3.33 ± 1.11 and 4.00 ± 1.13, P < 0.05). Furthermore, the START system had the highest score (4.60 ± 0.63, P < 0.05) for being easy to recall compared to ASMcc (3.27 ± 1.33) and SALT (3.80 ± 1.08). The participants also felt that START was more efficient than the other two triage systems (4.40 ± 0.83 vs. 3.29 ± 1.27 and 4.14 ± 0.86, P < 0.05) (Table 3).

Table 3. Results of the questionnaire survey on the use of the three triage systems (n = 30).
The results of the field interview showed further details on the usage experience of the triage systems from the participants. The participants mentioned that “the START system is fast and easy to use,” “the process of the START system is very clear,” “the ASMcc system is close to the actual situation of the injury,” “the ASMcc system is more complicated to learn,” “the ASMcc system takes longer time during triage,” “the SALT system is more comprehensive,” “when using the SALT system is relatively more challenging to judge.” According to these characteristics, the majority of the participants were most satisfied with the START system (18/30), followed by the SALT (9/30) and ASMcc systems (3/30). Regarding the suggestions for the triage systems for MCIs, some participants suggested that “if we can unify the standards of triage systems, it is not necessary to learn so many triage systems” and “it is hoped that the steps of triage evaluation can be simplified to make the classification faster and better.” They admitted that two of the most important features of a good triage system is its simplicity in performance and high reliability.
The results of the study on the performance evaluation of the three triage systems for simulated disaster patients with medical undergraduate students showed that the ASMcc triage system had the highest accuracy with the lowest over triage rate, the SALT system had the lowest under triage rate, and the START system had the shortest triage time. Furthermore, the START system was the easiest to learn and recall with the highest efficiency and satisfaction among the three systems (15).
For MCIs, the triage process is a dynamic procedure, and there is no fixed standard for the triage of mass casualties (16). Many different triage systems are available worldwide and can be classified into two main categories: algorithmic approaches and numerical approaches (17). The algorithmic approach places the injured person in a particular category through a check with each criterion, and if this criterion is normal, proceed to the next.
The numerical approach is to calculate the final score based on each criterion to classify the wounded (18, 19). Although both the START and SALT systems belong to the algorithm approach, their specific standards and the priority of evaluation are different. The ASMcc system is a numerical approach (10). Due to the diversity of triage systems, the triage results, such as accuracy and triage time, are different, which can be verified according to the results of the study. The performance of the three triage systems was compared under the same basis and conditions. From the perspective of the speed of triage, START was the fastest, and the participants in the study provided the viewpoint that it had the greatest simplicity among the three triage systems (4, 20). However, START had the lowest accuracy and the highest over-triage rate. This may be because START mainly utilizes manual operation without the use of sphygmomanometers and other medical equipment for auxiliary evaluation, which is simple but easy to overtriage (21), resulting in a lower accuracy rate.
Compared with the START system, the SALT system had a higher accuracy rate. It was not consistent with the results of a study in a similar earthquake scenario (7), which may be due to those participants having been experienced medical personnel or due to the differences in the conditions of the injuries (22). Due to the different medical and health knowledge reserves of the participants, the judgment on traumatic condition also differs. It is worth mentioning that SALT had the lowest undertriage rate, which may be because it classifies the wounded by simple instructions followed by individual evaluations. The SALT triage system is a dynamic and continuous process that is suitable for disaster rescue scenarios (23).
ASMcc had the longest triage time because it is more complicated and has more evaluation items. However, from the perspective of triage accuracy, ASMcc had the highest accuracy rate. This may be because the classification standard is specific, and it uses a quantitative method by calculating scores to improve accuracy. To improve the triage accuracy, it is necessary to conduct systematic physical examinations and close observations on the wounded, which will definitely take more time during triage (10, 24). A good triage system should balance many factors, including triage accuracy and time, and its developers might also consider its use under specific or diverse scenarios (25).
In MCIs, triage personnel may be professional medical staff, volunteers with basic first aid knowledge, and even displaced persons with no prior experience. Due to different factors, such as specialty and ability, the applicability of different triage systems to the population is also different (26). START uses simple medical knowledge to determine the extent of the injuries by noting if the patients are walking, breathing or conscious. In this study, the START method was more likely to be preferred by the students (with simple medical and health knowledge), because it can be grasped quickly and thus improve efficiency. A study compared START with the SALT system, and the results showed that males preferred START for being easier to learn, while females preferred the SALT system for being more logical, comprehensible, and consistent with traditional medical care (5). ASMcc is more specific and complex, involving respiratory rate, systolic blood pressure and consciousness (Glasgow coma index) (27), which is more suitable for professional medical personnel with clinical experience. In practice, the triage system users should not only consider the particularity of different people and training but also choose specific methods according to the scale and type of events. In addition, it is also necessary to consider the use of existing resources and treatment interventions and take appropriate methods of injury classification into account in clinical practice (28).
The study also had some limitations. First, the study evaluated the effectiveness of the three triage systems, but it did not cover other triage systems. Furthermore, the limitation of the cross-sectional study design and potential bias need to be considered. Therefore, in the study, a randomization method and crossover study design were used to avoid potential bias with quality control measures. Second, the study used a simulated traumatic condition card instead of real patients due to limited resources, which might differ from medical disaster rescue in practice. However, the traumatic condition and distribution of the simulated disaster patients were fully considered to simulate the real situation as much as possible. Third, the participants were recruited from junior undergraduates majoring in clinical medicine with only males included, which might have limited the representativeness of the study population. The junior undergraduate students of clinical medicine were recruited because they had finished relative medical courses according to the semester requirements, were fresh learners on triage of disaster patients and had no prehospital or clinical practice before. For the female participants, the study was limited because most of the undergraduates in military medical school were males. Therefore, further studies with more representative participants, including more triage systems, and evaluation in real practice are suggested.
In MCIs, an appropriate triage system is crucial to effectively classify the wounded, reduce the death and disability rate, and improve the overall treatment efficiency (29, 30). This study evaluated the effectiveness of three triage systems among undergraduate students, and it was noted that they all have their own characteristics and advantages and can be suitable in practice in MCIs. Further studies involving more triage systems with data based on real conditions are recommended.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The requirement of ethical approval was waived by Air Force Medical University for the studies involving humans because the sample used is anonymous. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants' legal guardians/next of kin because all protocols were in accordance with the ethical standards of our institution. Written informed consent was obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article.
YW and YH designed the study and directed its implementation. JZ, KL, RW, RC, and JJ performed and conducted the field works, data collection, and analysis. JZ, KL, JR, YH, and LL performed the statistical analysis and initial manuscript writing. All authors read and approved the final manuscript.
JZ was supported by the Shaanxi Provincial Natural Science Foundation (No. 2021SF-425). YW was supported by the Shaanxi Provincial Natural Science Foundation (No. 2017JM7008) and the Science Foundation of Fourth Military Medical University (Nos. 2019ZFB006, 21QNPY086). The funders had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
MCIs, mass casualty incidents; START, simple triage and rapid treatment; ASMcc, abbreviated scoring method for combat casualty; SALT, sort assess lifesaving interventions treatment/transport system; FTS, field triage score; MARCH, Massive Hemorrhage, Airway, Respiration, Circulation and Hypothermia; CRAMS, circulation, respiration, abdomen, motor and speech.
1. Liu SY, Chen HH, Li YZ. Establishment and management of OBU (On board Unit) for first-aid in mass casualty. China J Emerg Resuscit Disast Med. (2012) 7:359–62. doi: 10.3969/j.issn.1673-6966.2012.04.023
2. Zhang XR, Zhu R, Liu HY, Zhang JH. Research on emergency medical rescue considering the psychological status of wounded. Chinese J Manag Sci. (2017) 10:190–9. doi: 10.16381/j.cnki.issn1003-207x.2017.10.020
3. Disaster Rescue Branch of China Medical Rescue Association. Consensus of experts on emergency medical countermeasures to mass casualty. Chin J Emerg Med. (2016) 25:405–14. doi: 10.3760/cma.j.issn.1671-0282.2016.04.003
4. Pouraghaei M, Tabrizi JS, Moharamzadeh P, Ghafori RR, Rahmani F, Mirfakhraei BN.The effect of start triage education on knowledge and practice of emergency medical technicians in disasters. J Caring Sci. (2017) 6:119–25. doi: 10.15171/jcs.2017.012
5. Fink BN, Rega PP, Sexton ME, Carolina W. START vs. SALT triage: which is preferred by the 21st century health care student? Prehosp Disaster Med. (2018) 33:381–6. doi: 10.1017/S1049023X18000547
7. Zhai YC, Chen DM, Ren HQ, Dai L. A preliminary research on the application of SALT in disaster rescue. Chin J Pract Nurs. 34:1296–300. doi: 10.3760/cma.j.issn.1672-7088.2018.17.005
8. Wang, D. Research and Development of Intelligent Triage System. Tianjin: Institute of Medical Equipment, Academy of Military Medical Sciences. (2016).
10. Zong ZW, Zhang LY, Qin H, Chen SX, Zhang L, Yang L, et al. Expert consensus on the evaluation and diagnosis of combat injuries of the Chinese people's liberation army. Military Med Res. (2018) 5:7–16. doi: 10.1186/s40779-018-0152-y
11. Lim CY, In JY. Considerations for crossover design in clinical study. Korean J Anesthesiol. (2021) 74:293–9. doi: 10.4097/kja.21165
12. Wang T, Malone J, Fu H, Heilmann C, Qu Y, Huster WJ. Crossover design and its application in late-phase diabetes studies. J Diabetes. (2016) 8:610–8. doi: 10.1111/1753-0407.12412
13. Yang Z. Research on the Composition of Earthquake Disaster Injury Spectrum and Emergency Medical Rescue Force. Beijing: PLA Academy of Military Medical Sciences; Chinese People's Liberation Army Academy of Military Medical Sciences. (2017).
14. Hupert N, Hollingsworth E, Xiong W. Is overtriage associated with increased mortality? Insights from a simulation model of mass casualty trauma care. Disaster Med Public Health Prep. (2007) 14–24. doi: 10.1097/DMP.0b013e31814cfa54
15. Lin YK, Chen KC, Wang JH, Lai PF. Simple triage and rapid treatment protocol for emergency department mass casualty incident victim triage. Am J Emerg Med. (2022) 53:99–103. doi: 10.1016/j.ajem.2021.12.037
16. Mckee CH, Heffernan RW, Willenbring BW, Schwartz RB, Lerner EB. Comparing the accuracy of mass casualty triage systems when used in an adult population. Prehosp Emerg Care. (2019) 24:515–24. doi: 10.1080/10903127.2019.1641579
17. Yang J, Chen JH, Peng BB, Yang Y, Zhang XY, Zhao L, et al. A systematic review of primary injury classification techniques for large-scale casualties in China. Chin J Emerg Recov Dis Med. (2021) 16:7. doi: 10.3969/j.issn.1673-6966.2021.07.008
18. Bazyar J, Farrokhi M, Khankeh H. Triage systems in mass casualty incidents and disasters: a review study with a worldwide approach. Open Access Maced. J. Med. Sci. (2019) 7:482–94. doi: 10.3889/oamjms.2019.119
19. Zhao W. Review on the triage at the scene of disaster rescue qualitative and quantitative methods outside the hospital. China J Emerg Resuscit Disast Med. (2007) 2:291–4. doi: 10.3969/j.issn.1673-6966.2007.05.013
20. Hua Y, Lu P, Liao CF, Wang Q, Wang XD. Application of injury classification in pre hospital emergency treatment of group trauma. Public Med Forum Magaz. (2015) 25:67–116.
21. Baker MS. Creating order from chaos: part ii: tactical planning for mass casualty and disaster response at definitive care facilities. Mil Med. (2007) 3:237–43. doi: 10.7205/MILMED.172.3.237
22. Chen JH, Yang J, Yu Y, Zheng JC. Mass casualty incident primary triage methods in china. Chinese Med J. (2015) 128:2664–71. doi: 10.4103/0366-6999.166030
23. SALT SALT mass casualty triage: Concept Endorsed by the American College of Emergency Physicians American American College of Surgeons Committee on trauma American Trauma Society National National Association of EMS Physicians National Disaster Life Support Education Consort. Disaster Med Public Health Prep. (2008) 2:245–6. doi: 10.1097/DMP.0b013e31818d191e
24. Zhao JJ, Deng YX, Jiang L, Qin C. Improve the evaluation of the state of consciousness in the summary battle injury score of the Chinese army. Hospital Admin J Chinese People's Liberation Army. (2017) 24:128–9. doi: 10.16770/J.cnki.1008-9985.2017.02.009
25. Khorram-Manesh A, Nordling J, Carlstrm E, Goniewicz K, Faccincani R, Burkle FM. A translational triage research development tool: standardizing prehospital triage decision-making systems in mass casualty incidents. Scand J Trauma Resusc Emerg Med. (2021) 29:119. doi: 10.1186/s13049-021-00932-z
26. Wang DM, Zheng JC, Li XH. Triage in disaster medical rescue. Chinese J Dis Med. (2014) 2:186–90. doi: 10.3969/j.issn.2095-6275.2014.04.002
27. Geng F. Triage of examination in First-aid before Hospital–Quantitative Analysis Method and Procedure. Chin General Pract. (2012) 15:575–6. doi: 10.3969/j.issn.1007-9572.2012.05.037
28. Bhalla MC, Frey J, Rider C, Nord M, Hegerhorst M. Evaluation of simple triage algorithm and rapid treatment and sort, assess, lifesaving, interventions, treatment, and Transportation mass casualty triage methods for sensitivity, specificity, predictive values. Am J Emer Med. (2015) 33:1687–91. doi: 10.1016/j.ajem.2015.08.021
29. Marcussen CE, Bräuner KB, Alstrom H, Moller AM. Accuracy of prehospital triage systems for mass casualty incidents in trauma register studies—a systematic review and meta-analysis of diagnostic test accuracy studies. Injury. (2022) 53:2725–33. doi: 10.1016/j.injury.2022.05.006
Keywords: mass casualty incidents, triage, emergency medical service, START, ASMcc, SALT
Citation: Zhang J, Liu K, Chen R, Ren J, Wang R, Li L, Jiang J, Hua Y and Wan Y (2023) Assessment of three triage systems by medical undergraduate students using simulated disaster patients: a comparative study. Front. Disaster Emerg. Med. 1:1169851. doi: 10.3389/femer.2023.1169851
Received: 20 February 2023; Accepted: 03 August 2023;
Published: 28 August 2023.
Edited by:
Muhammad Waseem, Lincoln Medical Center, United StatesReviewed by:
Jabeen Fayyaz, University of Toronto, CanadaCopyright © 2023 Zhang, Liu, Chen, Ren, Wang, Li, Jiang, Hua and Wan. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yi Wan, d2FueWlAZm1tdS5lZHUuY24=; Yan Hua, aHVheWFuMTExMkAxMjYuY29t
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.