 Rinat Meerson1,2
Rinat Meerson1,2 Hanna Buchholz1
Hanna Buchholz1 Klaus Kammerer3Manuel Göster3
Klaus Kammerer3Manuel Göster3 Johannes Schobel4
Johannes Schobel4 Christoph Ratz5,6
Christoph Ratz5,6 Rüdiger Pryss3Regina Taurines1
Rüdiger Pryss3Regina Taurines1 Marcel Romanos1,6
Marcel Romanos1,6 Matthias Gamer7
Matthias Gamer7 Julia Geissler1,6*
Julia Geissler1,6*
- 1Department of Child and Adolescent Psychiatry, Psychosomatics and Psychotherapy, Center of Mental Health, University Hospital of Wuerzburg, Wuerzburg, Germany
- 2Department of Communication, University of Vienna, Vienna, Austria
- 3Institute of Clinical Epidemiology and Biometry (IKEB), University of Wuerzburg, Wuerzburg, Germany
- 4DigiHealth Institute, Neu-Ulm University of Applied Sciences, Neu-Ulm, Germany
- 5Chair of Special Education IV—Education for People with Intellectual and Developmental Disabilities, University of Wuerzburg, Wuerzburg, Germany
- 6German Centre of Prevention Research in Mental Health, University and University Hospital Wuerzburg, Wuerzburg, Germany
- 7Department of Psychology, University of Wuerzburg, Wuerzburg, Germany
Introduction: Challenging behaviour (CB) is a common issue among children with autism spectrum disorder or intellectual and developmental disability. Mental health applications are low-threshold cost-effective tools to address the lack of resources for caregivers. This pre-post study evaluated the feasibility and preliminary effectiveness of the smartphone app ProVIA-Kids using algorithm-based behaviour analysis to identify causes of CB and provide individualized practical guidance to manage and prevent CB.
Methods: A total of 18 caregivers (M = 38.9 ± 5.0) of children with a diagnosis of autism spectrum disorder (44%), intellectual and developmental disabilities (33%) or both (22%) aged 4–11 years (M = 7.6 ± 1.8) were included. Assessments were performed before and after an 8-week intervention period. The primary outcome was the change in parental stress. Caregiver stress experience due to CB was also rated daily via ecological momentary assessments within the app. Secondary outcomes included the intensity of the child's CB, dysfunctional parenting, feelings of parental competency as well as caregivers' mood (rated daily in the app) and feedback on the app collected via the Mobile Application Rating Scale.
Results: We observed increases in parental stress in terms of conscious feelings of incompetence. However, we also saw improvements in parental stress experience due to CB and overreactive parenting, and descriptive improvements in CB intensity and caregiver mood.
Discussion: ProVIA-Kids pioneers behaviour analysis in a digital and automated format, with participants reporting high acceptance. Pilot results highlight the potential of the ProVIA-Kids app to positively influence child behaviour and caregiver mental health over a longer intervention period.
Registration: The study was registered at https://www.drks.de (ID = DRKS00029039) on May 31, 2022.
1 Introduction
Behaviour “can be described as challenging when it is of such an intensity, frequency, or duration as to threaten the quality of life and/or the physical safety of the individual or others and it is likely to lead to responses that are restrictive, aversive or result in exclusion” (1). Challenging behaviour (CB) in children encompasses, e.g., verbal and physical aggression towards others, auto-aggression, or non-compliance (2–4).
CB poses a significant obstacle to independence, learning, community integration, socialization, and public perception for individuals with mental disorders such as autism spectrum disorder (ASD) or intellectual and developmental disabilities (IDD), thus placing a substantial strain on the individuals themselves and on their caregivers (5, 6). Furthermore, managing CB comes at a high cost and often results in a significant burden of care, for example requiring special education and training for caregivers, and involvement of specialized health services (4, 7, 8). Research has identified CB as the best predictor of parental stress (5, 9–11).
Approximately 1% of the population has an IDD (IQ < 70), ranging from mild to profound degrees of impairment in conceptual, social and practical abilities (12). ASD has a prevalence of 2.8% and core symptoms comprise difficulties in social interaction and verbal and non-verbal communication as well as limited, repetitive and stereotyped patterns of behaviour, interests and activities. Among children with ASD, approximately 38% also have a diagnosis of IDD (13). A representative study in Germany found prevalence rates of approximately 52% for CB in students with IDD (14). The risk for CB increases further when IDD is accompanied by ASD (15). In children with ASD, the prevalence of CB is even higher at around 95% (16). Numerous studies have reported positive associations between the extent of CB and caregiver variables such as parental stress, depressive symptoms, and anxiety in families of children with ASD and/or IDD (17–21).
The risk factors for CB show considerable overlap between children with ASD and IDD. CB can arise from individual and/or environmental factors. Communication impairments constitute an important individual risk factor (22, 23) alongside insufficient adaptive problem-solving, and self-help abilities (24), sensory hypersensitivities (4), self-stimulation (3), physical discomfort or pain (25), symptom severity (26), comorbid psychiatric disorders (27), or intense need for care (14). Environmental factors are, e.g., punitive parenting (28), or an inadequate residential setting (e.g., lack of respectful communication or treatment, lack of autonomy) (29). Furthermore, CB can develop and persist due to operant learning processes and reinforcement (2, 30). The bidirectional relationship of child's CB, parental stress and parenting practices is described in the transactional model by Hastings, in which CB initiates parental stress, leading to dysfunctional parenting practices, which further exacerbate CB (31).
Behavioural interventions can be effective in reducing CB in individuals with ASD and/or IDD (32, 33). A meta-analysis on 8 randomized controlled trials (RCTs) including 653 children with ASD found a moderate effect of behavioural parent-training programs on children's disruptive behaviour (34). A recent meta-analysis by Groves et al. included 42 studies on non-pharmacological and 40 studies on pharmacological interventions for CB in individuals with IDD. The authors reported overall small effects, with no differences between non-pharmacological and pharmacological interventions. However, these results should be treated with caution as there were indications of a large number of studies supporting the null hypothesis (35). A meta-analysis by Ruane and Carr found a large effect of the behavioural parent program Stepping Stones Triple P on parenting style, moderate effects on parent-reported child problems, researcher observed child behaviour and parenting satisfaction and self-efficacy, as well as small effects on parental adjustment and parental relationship in families of children with developmental disabilities (36). However, the evidence remains inconclusive due to small effect sizes and a lack of high-quality studies along with great heterogeneity of behavioural interventions in terms of, e.g., contents, specificity and delivery. It may also be important to consider different types of CB that might have specific antecedents (e.g., pain as a trigger for self-injury). More nuanced and targeted therapeutic approaches, accounting for biological factors, may be necessary (37).
Addressing the question whether guidance by a healthcare professional is required, a meta-analysis showed that self-directed (i.e., without involvement of a therapist or other healthcare provider) parenting interventions for children with externalizing problem behaviour had a large effect on reducing parent-reported externalizing behaviour and moderate effects on reducing harsh or inconsistent discipline practices and reducing self-reported lax or dismissive discipline practices (38). Additionally, self-directed interventions had a small but significant effect on reducing parental stress, and a large effect on increasing parenting efficacy. Interestingly, the study found that self-directed interventions were comparable to therapist-led interventions in improving child behaviour as perceived by parents. Thus, self-directed parenting interventions not only have the potential to improve both child behaviour and parental well-being, but also can be a viable alternative for parents who face barriers to accessing therapist-led interventions.
Given the bidirectional relationship between CB and parental stress, interventions that aim to reduce parental stress can also lead to positive changes in child's CB (39). Hence, reducing parental stress can strengthen a family's functioning and balance, which in turn, moderates the effect of CB (40). Lewallen and Neece investigated changes in social skills of 24 children with IDD after parents participated in an 8-week mindfulness-based stress reduction intervention and found that the variance in child self-control was significantly accounted for by changes in parental attachment and discipline practices (41).
Overall, the literature emphasizes the need for interventions that focus not only on managing the child's CB but also on reducing parental stress and enhancing parental well-being (42).
However, there is a considerable shortage of resources addressing caregivers of children displaying CB. Insufficient healthcare resources and limited parent-training programs hinder access to professional support for families of children with ASD and/or IDD. Long waiting times, low access to specialized services and underrepresentation of children and adolescents with IDD in clinics contribute to the challenges faced (4, 43–46).
The increasing demand for accessible and low-threshold (i.e., freely available and easily accessible without relying on the resources of the healthcare system) interventions has driven the development of a growing number of mental health applications (MHAs) for children with ASD and/or IDD and their caregivers (47). However, empirical evidence for MHAs in the context of ASD and/or IDD is highly heterogeneous (48). Kim et al. showed that out of 695 apps listed by the nonprofit organisation “autism speaks” in 2017, 95% were not supported by any clinical evidence (49). Several studies indicate beneficial effects of MHAs for ASD, with the majority targeting a range of outcomes such as social and communication skills in children (48, 50, 51). Although scarce, there are some MHAs targeting CB in individuals with ASD and/or IDD. A narrative review by Sheehan and Hassiotis highlights that digital health interventions can support individuals with IDD and CB by providing augmented communication, facilitating behaviour analysis by monitoring apps, and supporting families through online forums (52). Johnson et al. found that children with ASD who used a social script iPad app before a neuroimaging procedure (n = 16) exhibited less externalizing CB during the procedure and parents showed lower levels of anxiety compared to the control group (53). Another study showed that an app used by parents can be effective to reduce stereotypy in children with ASD (n = 7) by implementing a personalized behavioural intervention (54). The app Smartautism by Bonnot et al. lets caregivers of children with ASD record the child's behaviour and daily routines via ecological momentary assessments (EMAs) and displays a graphical representation of the data, but offers no guidance or recommendations. The study only explored the usability and usage intention in a prospective longitudinal exploratory open study (n = 65) without examining efficacy. In conclusion, MHAs hold great potential for supporting caregivers of children with ASD and/or IDD (55). However, there is a notable scarcity of evidence-based MHAs that specifically target caregivers of children displaying CB as both users and beneficiaries.
The ProVIA project aimed at providing an evidence-based, low-threshold tool for caregivers of children with ASD and/or IDD to improve their understanding of CB and guide them in the modification of the child's behaviour via the app ProVIA-Kids. ProVIA-Kids is the first app to automate behaviour analysis to provide individualized feedback on risk factors of CB and suitable recommendations to caregivers. Additionally, ProVIA-Kids emphasizes the strengthening of caregivers' resources to reduce stress and positively influence the child's behaviour. The aim of this pilot study was to investigate the feasibility and preliminary effectiveness of using the ProVIA-Kids app for caregivers of children with ASD and/or IDD showing challenging behaviour. We hypothesized that the use of the ProVIA-Kids app would reduce parental stress over an eight-week intervention period. As secondary outcomes, we expected to find improvements in terms of child's CB, dysfunctional parenting, parental mood and parental competence.
2 Materials and methods
2.1 Experimental design and recruitment
Data for this pre-post study without control group were collected before (T0) and after eight weeks of using the ProVIA-Kids app (T1). Follow-up data collection is ongoing. The app generated a unique code under which data were transmitted to the university. Participants provided this code to the study team, who kept a paper list containing the study ID and the corresponding app code to link data from questionnaires to data transmitted from the app. All data was encrypted before transmission to prevent unauthorised access to confidential information. Access to the patient identification list was limited to the principal investigators. The study was approved by the ethics committee of the Medical Faculty of the University of Wuerzburg, Germany (AZ 233/21-me) on May 11, 2022 and registered on May 31, 2022 at the German Clinical Trials Register (https://drks.de/search/de/trial/DRKS00029039). The project was funded by the Bavarian Ministry for Family, Labor and Social Affairs.
Participants were mainly recruited from the general outpatient clinic at the Department of Child and Adolescent Psychiatry, Psychosomatics and Psychotherapy of the University Hospital of Wuerzburg between June 2022 and November 2022. Information about the study and contact details of the study team (email address and phone number) were additionally distributed via medical and care institutions, a podcast and a press release.
2.2 Trial flow
Families who contacted the study team via email or phone expressing interest in participating were extensively informed about the purpose of the study as well as their rights (verbally and via written participant information documents) and were provided a consent form. They were given sufficient time to decide on their voluntary participation. After all primary caregivers had signed the consent form, families fulfilling all inclusion criteria (for an overview, see Table 1) were enrolled. Participants had the right to revoke their consent at any point without giving a reason or facing any negative consequences. At the baseline assessment (T0), participants received questionnaires and provided additional sociodemographic information in an interview (face-to-face or via phone). Participants were then given access to the smartphone app ProVIA-Kids and instructed to use it over a period of eight weeks. One week after the baseline interview, a brief check-in phone call was scheduled to address any potential technical issues. During the eight-week intervention period, participants were encouraged to explore different app features, recommended to complete behaviour analyses after each occurrence of CB and fill out the daily mood diary for the duration of the intervention period. Especially in the first two weeks, the participants were encouraged to primarily observe the CB and fill out the behaviour analyses to identify the most common causes of CB. After those two weeks, participants were additionally encouraged to start implementing the recommended strategies for those risk factors for CB. After the intervention (T1), participants again received questionnaires and were interviewed about changes in the child's treatments and potential side effects of the app use.
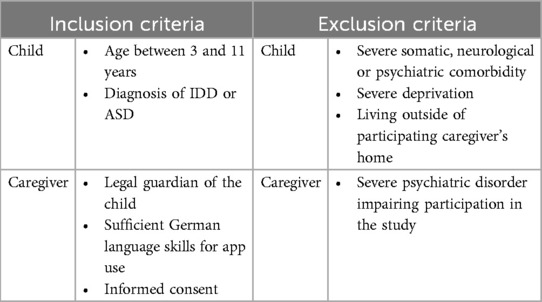
Table 1. Summary of eligibility criteria.
2.3 Sample description
Of N = 23 enrolled families, 3 dropped out during the study due to personal circumstances. Two families had stated their intention to return the T1 questionnaires they filled out, however, the study team did not yet receive them. The final analysis sample comprised N = 18 caregivers of children with a diagnosis of ASD (44%), IDD (33%) or both (22%). For analyses of data directly transmitted via the app, the two participants with missing T1 questionnaires were included. Of all enrolled children aged 4–11 years (M = 7.6 ± 1.8), 66% were male and 67% were diagnosed with comorbid psychiatric disorders and 72% lived with both biological parents. Sociodemographic characteristics of all children are presented in Table 2.
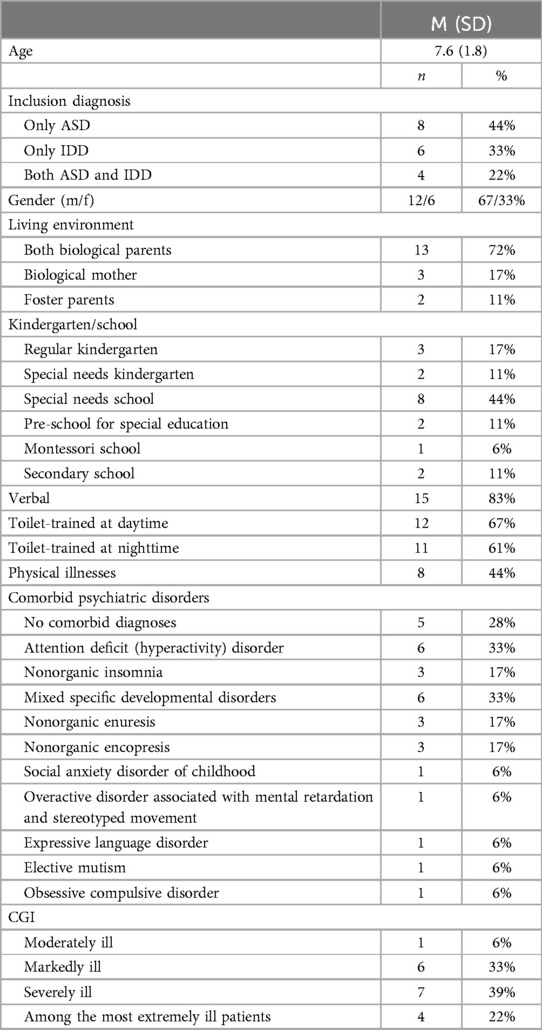
Table 2. Sociodemographic data regarding the children (ITT sample).
All app users (referred to as “study participants”) were female between 28 and 51 years (M = 38.9 ± 5.0) with 39% having a psychiatric diagnosis, and 6% having had a clinical visit due to psychiatric symptoms. Chronic illness was present in 28% of the main app users. In 44% of cases, study participants reported a higher education entrance qualification, 61% worked part-time and 11% worked full-time. All co-parents worked either full-time (94%) or part-time (6%). Sociodemographic characteristics of all caregivers are presented in Table 3.
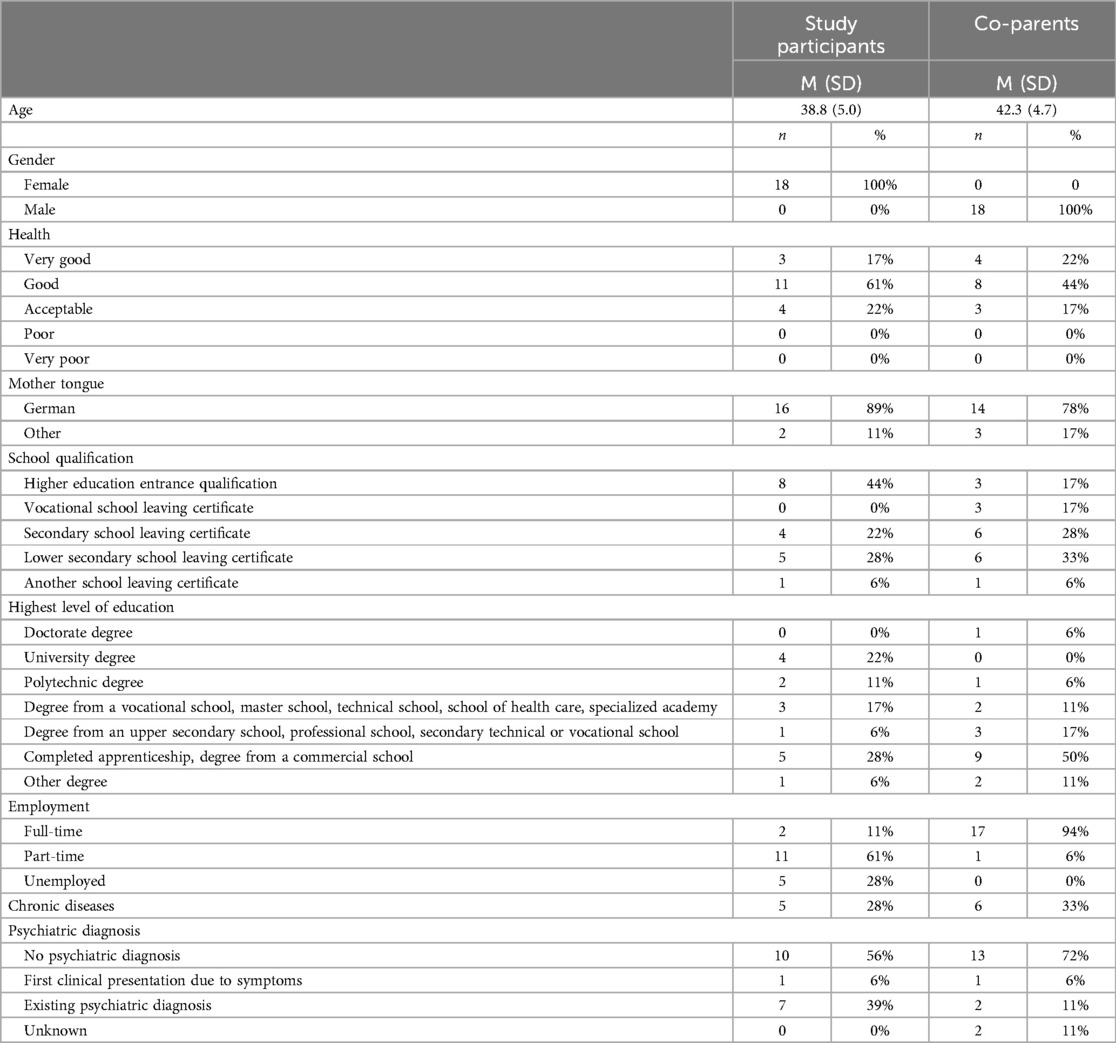
Table 3. Sociodemographic data regarding study participants and co-parents (ITT sample).
There was no difference between study completers and dropouts regarding initial parental stress (EBI total score; p = .182) with the exception of the subscale “parental attachment”, which revealed higher scores in completers than in the dropouts, t(21) = 2.86, p = .005. Among dropouts, 80% reported a psychiatric diagnosis whereas this was the case for only 40% of the study completers. For a comparison of baseline characteristics of completers and dropouts, see Supplementary Table S1.
2.4 Intervention
The ProVIA-Kids app was developed in cooperation with Prof. Dr. Rüdiger Pryss, Professor of Medical Informatics at the Institute for Clinical Epidemiology and Prof. Dr. Christoph Ratz, Chair of Special Education IV—Education for People with Developmental and Intellectual Disabilities at the University of Wuerzburg. ProVIA-Kids was developed for the Apple iOS and Android mobile operating systems. An overview of the menu items is shown in Figure 1. The app has a strong psychoeducational focus while also applying and teaching basic techniques used in cognitive behavioural therapy (CBT), such as behaviour analysis or contingency management.
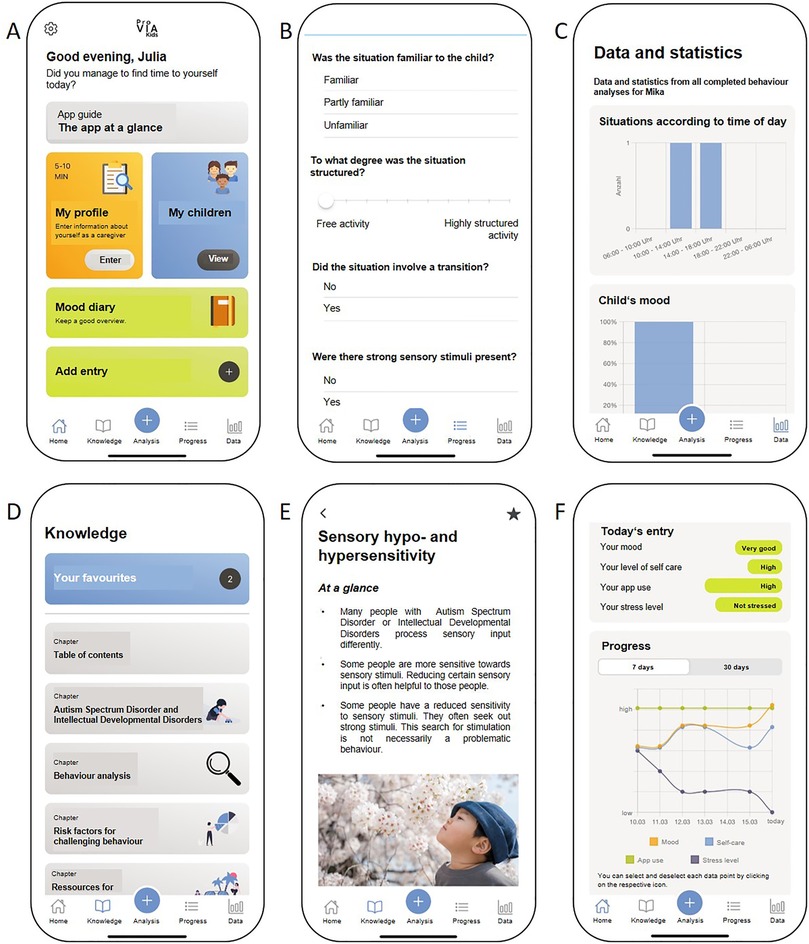
Figure 1. Features of the ProVIA-kids app. (A) Home screen including child and caregiver profiles, (B) behavioural analysis, (C) data and statistics, (D) psychoeducational chapters, (E) chapter example, (F) mood diary. The illustration is taken from the publication of the study protocol (56).
ProVIA-Kids examines potential risk factors for CB based on a behaviour analysis algorithm and provides caregivers with appropriate recommendations, while also emphasizing strengthening caregivers' resources.
To identify cross-situational risk factors, users complete profiles for themselves and the child. The caregiver profile comprises 20 items related to physical needs (e.g., sufficient sleep, hydration and food intake), social support, relationship with the child, stress experience and depressive symptoms (based on the PHQ-9) (57). The child's profile comprises 69 items relating to physical and emotional needs, communications skills and sensory processing. Based on the answers, the app identifies cross-situational risk factors for each individual and provided appropriate psychoeducational information and recommendations. For example, in response to the question “Is the child”s daily schedule predictable and well-structured for the child?”, answering “no” leads to “lack of structure” being flagged as a potential risk factor and triggers recommendations for providing adequate structure.
To identify situation-specific risk factors, users complete a behaviour analysis after CB had occurred in a specific situation. The app asks a series of single- or multiple-choice questions regarding the nature of the situation (time of day, presence of other people, novelty/structuredness of the situation, presence of strong sensory stimuli), the child's physical and mental state (mood, pain, frustration), the consequences of the behaviour (positive, negative or both) and the regularity of these consequences (first-time, intermittent, always), thereby following the SORKC principle used in cognitive behavioural therapy (58). For each question, specific answers (e.g., “Yes, the child was frustrated.” or “The situation had a low degree of structuredness.”) are marked as pathological. Upon completion of the behaviour analysis, users receive a summary of all identified situation-specific risk factors. For each identified risk factor, the users are provided with an explanation as to why it poses a potential problem for people with ASD and/or IDD and why it can lead to CB as well as brief suggestions on how to moderate the factor and thus prevent the CB in the future. Each short recommendation contains links to psychoeducational knowledge chapters within the app with more in-depth background information about that risk factor and more detailed practical recommendations.
All conducted behaviour analyses are stored in the app, allowing users to review the data at their own pace. In addition, the risk factors identified across all behaviour analyses are aggregated and their relative frequency was illustrated graphically. This allows users to recognize and understand recurring patterns in the CB (e.g., in 75% of the situations entered, there had been a change in the child's daily routine beforehand).
Independently of behaviour analyses and profiles, users can read psychoeducational chapters on risk factors for challenging behaviour and resources for caregivers included in the app.
Finally, the app features a “mood diary”, where users can voluntarily rate their daily mood, self-care, app use and stress experience due to CB on a 6-point scale. The input is used to create a graph with four trend curves to visualize changes over time as well as interactions (e.g., stress experience decreases as self-care increases).
2.5 Outcomes
All outcomes were assessed at T0 and T1. A complete description can be found in the published study protocol (56). For each family, outcomes measures were completed by the caregiver who primarily participated in the intervention.
The primary outcome parental stress was assessed with the “Eltern-Belastungs-Inventar” (EBI (59), the German version of the “Parenting Stress Index” (60) with 48 items using a 5-point Likert scale (1 = “does not apply at all” to 5 = “fully applies”). Higher scores represent greater parental stress. The EBI differentiates between two main sources of parental stress: impairment in parental function and child's characteristics and behaviour. The parenting domain contains seven subscales (parental attachment, isolation, competence, depression, health, role restriction, spouse; e.g., “Sometimes I find it difficult to empathize with my child.”, “In order to meet my child's needs, I have to restrict myself more than I had expected.”) and the child domain contains five subscales (distractibility/hyperactivity, acceptability, demandingness, adaptability, and mood; e.g., “My child does several things that bother me.”, “My child sometimes has difficulties adjusting to changes in the daily routine or home environment.”). The EBI shows excellent internal consistency for the total scale (Cronbach's Alpha, α = 0.95), the parent subscale (α = 0.93) and the child subscale (α = 0.91).
As secondary outcomes, all participants were prompted once daily at a prespecified time by the app to indicate their parental stress due to CB (using 6-point scale with the anchors “not stressed at all” to “highly stressed”) and parental mood (using 6-point scale with the anchors “very bad” to “very good”), assessed via EMA. Participants could only fill out the mood diary once per day. It was not possible to retrospectively fill out the mood diary for previous days.
Additional secondary outcomes were changes in the intensity of the child's CB (assessed on a self-constructed 5-point scale), experienced parenting competence (assessed with the “Fragebogen zum Kompetenzgefühl von Eltern” (61)) and dysfunctional parental practices (assessed with the short form of the “Erziehungsfragebogen” (62)). The technical aspects of the app were evaluated using the user version of the Mobile Application Rating Scale (uMARS).
2.6 Data analysis
For the statistical analysis IBM SPSS Statistics 28.0 (IBM Corp., 2020) was used. The significance level was set to α = .05 and in order not to lose statistical power, no adjustment for multiple testing was applied. To examine pre-post changes (T0 to T1) in parental stress, CB intensity and parenting practices, paired sample t-tests or nonparametric Wilcoxon sign-rank tests or sign tests were performed as applicable. Pre-post-changes in caregivers' mood and stress experience due to CB were evaluated using a paired sample t-test. Correlations (Pearson's r) were calculated to examine the relationship between the change in caregiver's mood (difference in pre- and post-scores of caregiver's mood, calculated by subtracting the pre-score from the post-score) and the change in the caregiver's stress experience due to CB (difference in pre- and post-scores of stress experience, calculated by subtracting the pre-score from the post-score). Effect sizes were calculated with Cohen's d for mean-based analyses or Eta-squared (η2) for median-based analyses. Per protocol (PP) and intention-to-treat (ITT) analyses were conducted for the pre-post changes in parental stress, CB intensity and parenting practices. The primary analysis is based on ITT, where all participants are included in the analysis regardless of whether they completed the intervention as instructed (i.e., no minimum usage of the ProVIA-Kids app). PP analyses only included participants who (1) provided at least 15 behaviour analyses or mood diary entries and (2) used the mood diary for at least six weeks with at least one entry per week. To identify potential factors leading to dropouts, differences in initial parental stress and CB between study completers and dropouts were calculated using independent t-tests or nonparametric Mann-Whitney U-tests, as applicable. Differences in single parenthood were calculated using Fisher's exact test and differences in employment and psychiatric diagnoses were calculated using Fisher-Freeman-Halton exact tests.
3 Results
3.1 User satisfaction with app quality
Mean treatment satisfaction (1 = “strongly disagree” to 5 = “strongly agree”) was M = 3.1 ± 0.8. The quality of the app (Figure 2) was rated as high in terms of functionality (M = 4.4 ± 0.1), aesthetics (M = 4.0 ± 0.2) and information content (M = 4.3 ± 0.1) and average in terms of engagement (M = 3.4 ± 0.2). The willingness to change health behaviour (M = 3.8 ± 0.2) resulting from app use was also high.
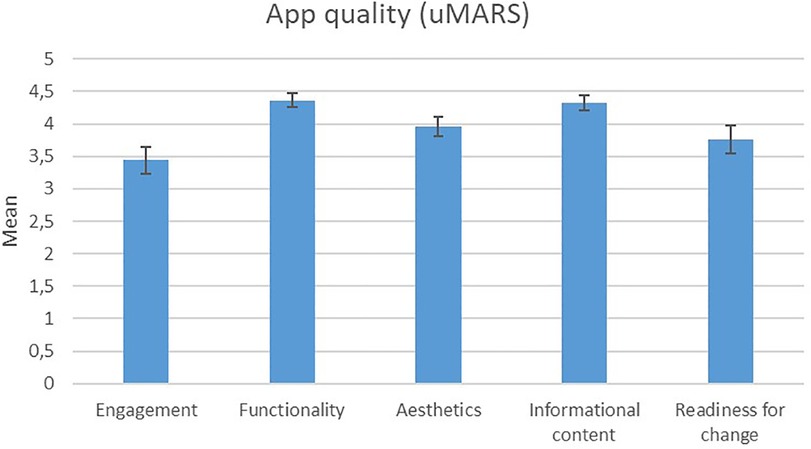
Figure 2. Ratings regarding app quality with the uMARS questionnaire.
3.2 Evaluation of the knowledge chapters
We received 113 ratings on 37 knowledge chapters from study participants via the app. For an overview of the ratings regarding overall article quality, comprehensibility of the information, usefulness of the recommendations, time taken to read knowledge articles, frequency of applying the recommendations in everyday life and readiness to change health behaviour, see Table 4.
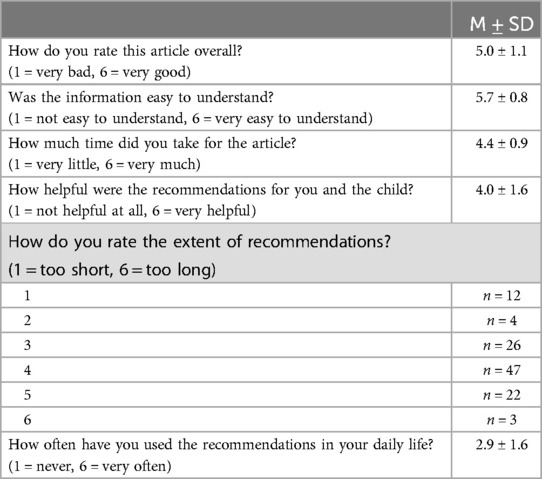
Table 4. Feedback for the knowledge chapters (n = 113 ratings).
3.3 Frequency of identified causal factors for CB
A total of 213 behaviour analyses were conducted with the ProVIA-Kids app. On average, 10.7 ± 11.1 (range 1–36) behaviour analyses were carried out by the 18 participants of the ITT sample. In most cases, the caregivers were able to state that the challenging behaviour was accompanied by positive consequences for the child (73%). In 95% of the situations, at least one other person was present and in 58% of situations at least one instruction was given. Changes in the daily routine were present in 49% of the situations. The strength of the child's feeling in the situation was reported as moderately strong (M = 6.0 ± 1.8; scale 1–10). An overview of the frequency of all potential causal factors can be found in Table 5.
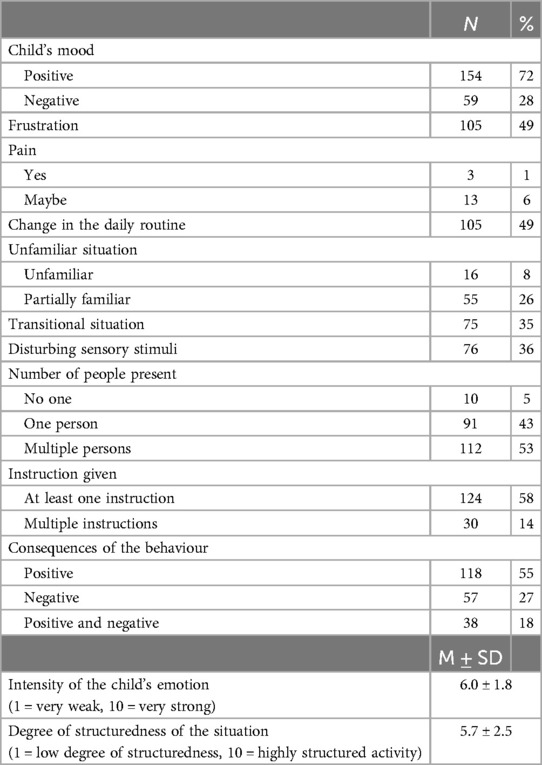
Table 5. Frequency of the identified causal factors across N = 213 behavioural analyses.
3.4 Increase in questionnaire-based parental stress
Contrary to our hypothesis, the ITT analysis showed a significant increase in total EBI scores and thus parental stress from baseline to the post-assessment, t(17) = −2.19, p = .021, d = 0.52. In the PP analysis, no significant difference in the total EBI scores was found, t(12) = −1.28, p = .112.
Additionally, in the ITT analysis, there was a significant effect in the parent domain with higher scores after the treatment, t(17) = −3.07, p = .003, d = 0.73. This effect was descriptively smaller in the PP analysis, t(17) = −2.14, p = .027, d = 0.59.
Figure 3 shows the changes in the EBI parent and child domains and total score from pre to post treatment.
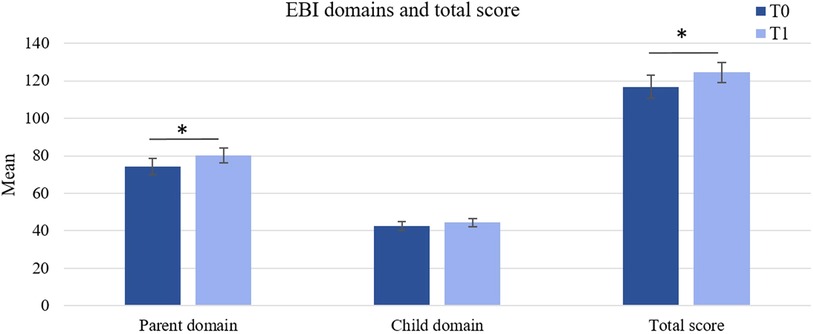
Figure 3. Changes in parental stress between T0 and T1 (ITT sample). Error bars represent standard errors of the mean. *p ≤ .05. **p ≤ .01.
ITT analyses of EBI subscales showed that participants were scoring higher on the parent domain subscale “attachment” after the treatment, t(17) = −1.79, p = .046, d = 0.42. However, in the PP analysis, no significant difference in the “attachment” scores could be found (p = .101).
Significant increases were observed in the parent domain subscale “competence”, t(17) = −2.07, p = .027, d = 0.49. This effect was also observed in the PP sample, t(17) = −1.92, p = .040, d = 0.53.
The PP analysis furthermore showed a significant increase in the parent domain “isolation” scores, t(17) = −1.96, p = .037, d = 0.55. Changes in the EBI subscales scores for all parent and child subscales between pre- and post-treatment are shown in Figure 4.
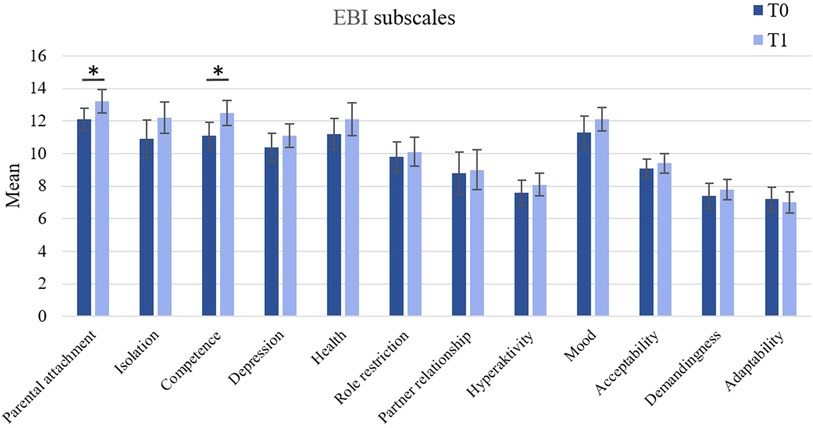
Figure 4. Changes in parental stress between T0 and T1 (ITT sample). Error bars represent standard errors of the mean. *p ≤ .05.
3.5 Descriptive decrease in intensity of the child's CB
Despite a descriptive decrease for all types of CB from T0 to T1 (as shown in Figure 5), no significant pre-post effects were found. Similarly, in the PP analyses there were no significant differences between the pre- and post-scores across all subscales.
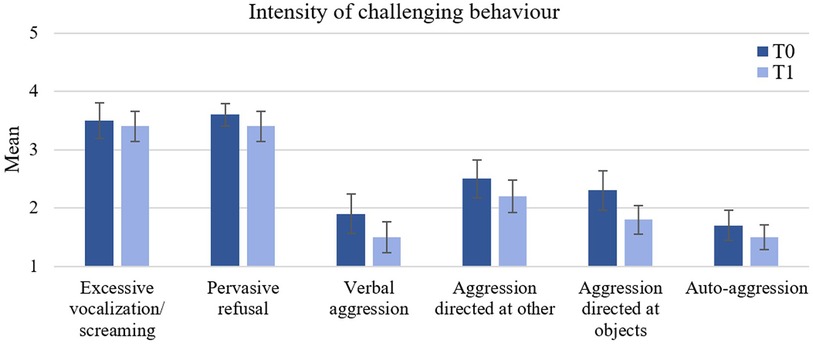
Figure 5. Changes in the child's challenging behaviour between T0 and T1 (ITT sample). Error bars represent standard errors of the mean.
3.6 Improvements in parenting practices despite decrease in subjective parental competence
There was no significant difference in total EFB-K scores before and after the treatment, t(16) = 1.37, p = .096, d = 0.33. However, participants scored significantly lower on the “overreactivity” subscale following the intervention, t(16) = 1.92, p = .036, d = 0.47. There was no significant difference in the “laxness” scores, z = −0.68, p = .495, η2 = 0.03. In contrast to the ITT analyses, the PP analyses showed no significant effects.
Regarding parental feeling of competence, there was a significant decrease in total FKE scores, t(167) = 3.72, p < .001, d = 0.88, carried by a decrease in self–efficacy, t(17) = 5.79, p < .001, d = 1.37.
3.7 Decrease in EMA-based parental stress and descriptive improvement of parental mood
EMA-based parental stress and mood were analysed for participants who had used the mood diary for at least six weeks, had made at minimum one entry per week and had available values in week 1 and week 8, resulting in a sample size of N = 13 (Figure 6). To examine whether the mean scores between week 1 and week 8 differed significantly, paired t-tests were conducted.
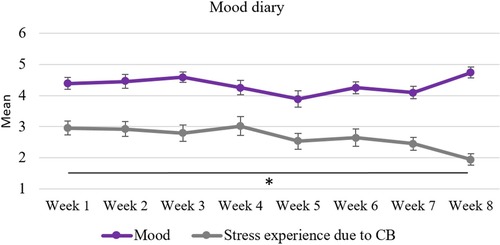
Figure 6. Caregiver's mood diary over the course of 8 weeks: changes in mood and stress experience due to challenging behaviour. Error bars represent standard errors of the mean. All available data sets were included which resulted in a sample size up to N = 20. **p ≤ .01.
A statistically significant decrease in the EMA-based subjective stress experience due to CB between week 1 (M = 2.8 ± 0.9) and week 8 (M = 2.0 ± 0.8) was observed, t(12) = 3.29, p = .003, d = 0.91. Descriptively, a slight non-significant increase in mood scores can be seen between week 1 (M = 4.5 ± 0.9) and week 8 (M = 4.6 ± 0.7) with fluctuations in scores over time (p = .313).
There was no significant correlation between the change in parental mood and the change in the parental stress experience due to CB (r = −.381, p = .199). The correlations between the change in app-use and the changes in self-care (r = .034, p = .912), parental mood (r = .117, p = .705) and parental stress experience due to CB (r = .011, p = .972) were not significant. However, there was a significant correlation between change in parental mood and change in self-care (r = .593, p = .032).
For an overview of the ITT and PP results for all primary and secondary outcomes, please refer to Table 6.
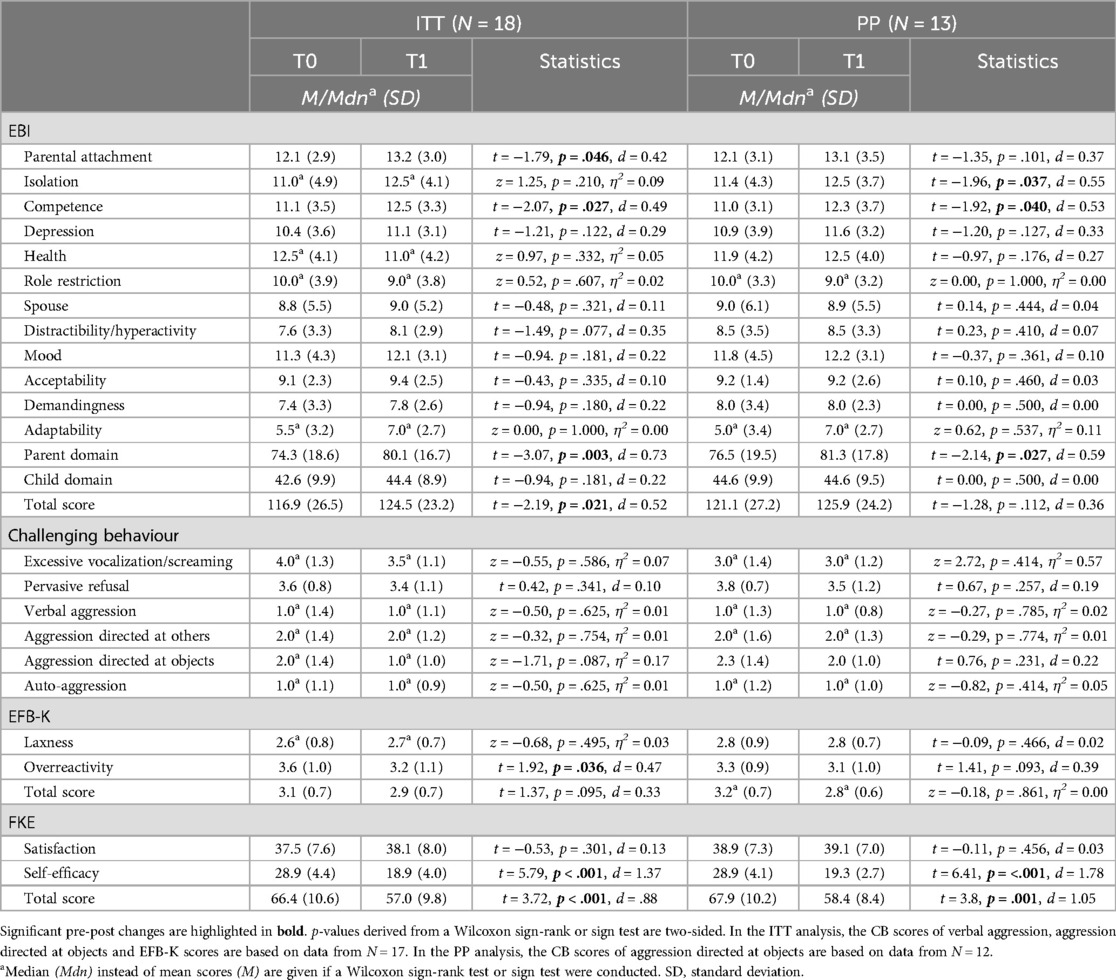
Table 6. Primary and exploratory outcomes at baseline (T0) and after treatment (T1) divided by intention-to-treat (ITT) and per-protocol (PP) analysis.
4 Discussion
ProVIA investigated the feasibility and preliminary effectiveness of an 8-week CBT-based smartphone intervention with a strong psychoeducational focus for caregivers of children with ASD and/or IDD showing challenging behaviour. We expected to see reductions in parental stress, the intensity of child's CB and dysfunctional parenting practices, and an increase of parental mood and parental feeling of competence from pre- to post-intervention. The results of the study revealed a high level of acceptance and mixed effects of the intervention on the quantitative outcomes.
Regarding the feasibility of targeting CB via a smartphone application, users reported high satisfaction with the ProVIA-Kids app, especially in terms of information content, functionality and psychoeducational chapters. Only very few minor technical difficulties were reported, none of which interfered substantially with app usage. The positive feedback underscores not only the suitability of the app for addressing the targeted behavioural issues but also indicates a demand for this accessible, free tool among a high-need under-supported group of patients. While user engagement as measured by the uMARS was rated as average, it is worth noting that this scale primarily focuses on entertainment value and interactivity. These dimensions will be expanded in future iterations of the app based on extensive qualitative feedback gathered after the testing phase, ensuring that updates align with the specific needs of the target audience.
Regarding the intervention's preliminary effectiveness, we found mixed results. In contrast to our hypothesis, we saw an increase in parental stress from pre-treatment to post-treatment in the ITT analysis (EBI). Increases occurred in the parent domain in the subscales “parental attachment” and “competence”. While this finding is inconsistent with studies showing a reduction in parental stress via therapist-led parent-training programs for parents of children with ASD (63–65) or IDD (66, 67), as well as self-directed interventions for parents of children displaying CB (68, 69), other studies also reported an increase in parental stress after a 12-month therapist-led training program for parents of children with ASD (70, 71), IDD (72–74) and/or CB (75).
Furthermore, parental stress was measured heterogeneously in the aforementioned studies. While five studies used the “Parenting Stress Index (PSI)”, which was also used in our study, the remaining studies utilized the “Depression Anxiety Stress Scales (DASS)” (76), the “Parental Stress Scale (PSS)” (77) or the “Elternstressfragebogen” (78), thus making it difficult to compare the findings. DASS does not specifically focus on stress within the parenting context, but rather measures general emotional distress. Moreover, compared to our study, the studies using PSI showed lower baseline scores, suggesting that initial stress levels can moderate the efficacy of the intervention. A closer examination of the EBI subscales carrying the significant results provides a possible explanation as the increase in parental stress was driven by higher post-treatment scores in the two subscales “isolation” and “competence”. Caregivers who score high on the “competence” subscale feel uncertain about their decision-making abilities and lack confidence in solving parenting issues (example item: “Some things in raising my child are harder for me than I expected.”) (59). Thus, as the ProVIA-Kids app encourages caregivers to reflect on their own behaviour and try new strategies in managing and preventing CB via psychoeducational chapters and practical recommendations, this at first may have led to heightened feelings of incompetence when these strategies did not yield immediate positive outcomes. This is in line with research suggesting that parents require time to try new strategies at home and adapt them to their unique circumstances, thus becoming more confident in dealing with the child's CB over time (71). High scores on the “isolation” subscale, on the other hand, indicate limited integration of parents into a social network, resulting in a lack of social support and overwhelming demands of child-rearing (example item: “Since I became a mother/father, it is more difficult for me to make new contacts”) (59). However, while it is unlikely for the extent of social integration to diminish over the short period of 8 weeks, it is much more likely that the ProVIA-Kids app drew the caregiver's attention to their lack of social support. A further possible explanation for the results in the primary outcome could be that during the first weeks after baseline, EBI scores may have initially shown a greater increase due to the abundance of information provided by the ProVIA-Kids app that may at first have left the caregivers feeling overwhelmed and less competent. At T1, EBI scores may have already started to decline again but were still elevated compared to baseline. However, as there was no measurement between T0 and T1, this assumption cannot be tested. Follow-up data will shed some light on this question, if a sufficient number of participants from the small sample participates. Based on these considerations it can be concluded that future studies should include additional measurement points as well as an alternative outcome measure for examining parental stress to better understand potential changes and underlying mechanisms in the observed changes in parental stress over time.
Considering the short intervention period of 8 weeks, substantial alterations in children's CB and parenting practices were not expected. Despite a lack of significant differences between pre- and post-intervention, we could descriptively see a decrease in the intensity of all types of CB both in the ITT and PP group, indicating a potential benefit of the intervention given more time. This result is in line with previous research on parent training programs for parents of children with ASD (63, 64, 71) or IDD (66, 67, 74), which consistently revealed a reduction in CB after the intervention. This also holds true for studies on self-directed interventions for parents of children displaying CB (68, 69, 75, 79). However, it is important to note that compared to these parent interventions which last ten weeks (68), three months (65), one year (70) or even longer (64, 80), the 8-week intervention period of our study was relatively short. Moreover, research has shown a delayed effect of parent trainings on parental stress, parenting practices, and child's CB, with studies reporting significant improvements not directly after the intervention, but only 3–12 months after the intervention (65). This “sleeper effect” emerges as the techniques learned in parent trainings gradually accumulate and prove to be effective in daily life.
With regards to dysfunctional parenting practices, our study showed that while there was no significant difference in total EFB-K scores and scores in the “laxness” subscale before and after the intervention, a significant reduction was found in the “overreactivity” subscale in the ITT analysis. This pattern of findings is in agreement with prior research on parent trainings for parents of children with ASD, which consistently reported a decrease in overreactivity but no (81, 82) or a delayed follow-up (65) effect on laxness, suggesting that compared to overreactive parenting practices, lax parenting practices may be more resistant to change. However, it has to be noted that there have been studies reporting both a reduction in laxness and overreactivity after a parent training for parents of children with ASD (83) or IDD (67) or no effect on parenting practices at all (71). Thus, the significant effect on “overreactivity” may also indicate that the ProVIA-Kids app addressed this parenting practice more explicitly, e.g., through knowledge chapters and recommendations following behaviour analyses. The “overreactivity” subscale captures parenting mistakes such as displaying anger, irritability, or hostility, and reacting strongly emotionally in situations where calm and assertive parenting would be more appropriate [item example: “When my child is misbehaving or acting inappropriately, I raise my voice or yell at my child (vs. talk calmly to my child.)”] (61). Hence, it is possible that the intervention helped caregivers better understand the underlying reasons for their child's behaviour and manage it effectively without overreacting. Also, the “overreactivity” scores were higher than the “laxness” scores both before and after the intervention which is in line with research indicating that caregivers of children with ASD exhibit more negative parenting behaviour, including excessive control, hostility, and poor communication, than parents of typically developing children (84). However, it is important to note that at baseline the EFB-K scores in this study were below the thresholds that indicate markedly dysfunctional parenting practices (cut-offs: total score = 3.59, overreactivity = 4.34, laxness: 3.43; for an overview of mean scores of all primary and exploratory outcomes, see Supplementary Table S2).
Regarding outcomes measured via ecological momentary assessments, the hypothesis of a decline in stress experience due to CB could be confirmed. Additionally, there was a trend-level improvement in mood scores, providing hints regarding the positive impact of the intervention on parental mental health. In comparison to parental stress and dysfunctional parenting practices assessed via questionnaires once before and after the intervention, parental mood and stress experience were reported daily in the ProVIA-Kids app, thus avoiding reliance on retrospective reports which are prone to memory errors and biases and increasing ecological validity as data were collected in the moment of experience. It is more likely to remember information or events that are consistent with one's current emotional state (85). Generally, more weight or attention is given to negative experiences, emotions, or information, than to positive or neutral ones, even when the negative experiences may be less significant (86). Hence, while the EBI scores at T1 may not yet have decreased below the scores at T0, the stress experience measured via EMA already showed a significant decline, suggesting that participants may not have noticed the actual improvement themselves when reflecting on the entirety of the intervention period retrospectively or may have viewed the experience in a more negative light due to singular difficult situations. In conclusion, the promising results from the EMA data support the potential efficacy of the ProVIA-Kids app, as it offers a more nuanced understanding of caregivers' experiences. This of course needs to be verified with a randomized controlled trial.
Baseline characteristics indicate that both caregivers and children were highly burdened before the intervention. 39% of study participants had a psychiatric diagnosis and 28% were affected by a chronic illness. Most of the children were rated as severely (39%) or markedly (33%) ill and 22% were considered among the most extremely ill patients. Furthermore, parental stress scores in the subscales “parental attachment”, “isolation”, “competence”, “depression”, “health” and “mood” in the ITT sample were clinically elevated compared with normative data from a combined sample of 538 mothers (age: 20–53 years, M = 34.9 ± 5.5) of children aged 1–6 years (see Supplementary Table S3) (59), which is consistent with many previous studies reporting that caregivers of children with ASD and/or IDD experience more parental stress compared to caregivers of typically developing children (40). However, interpretations of the EBI scores can only be made with reservation as the normative sample comprised mothers of younger children than those included in our study. The high levels of parental stress may have impaired the caregivers' ability to engage fully in the intervention. In turn, low treatment adherence due to time constraints, lack of motivation and inconsistent implementation of learned techniques can hinder an intervention's efficacy (87, 88). Moreover, it is possible that the ProVIA-Kids app is more effective in supporting less burdened families whereas a more time-intensive parent program could be better suited to reduce parental stress in a more clinically affected sample (65). This consideration is further reinforced when taking into account that 80% of dropouts had an existing psychiatric diagnosis, which is roughly twice the rate of completers (39%), thus indicating that the presence of a mental disorder can pose an obstacle to study participation and probably to appropriate app use. Interestingly, completers scored significantly higher on the EBI subscale “parental attachment” in comparison to dropouts. High scores on this subscale indicate difficulties in reliably assessing the child's needs (example item: “I sometimes have a hard time figuring out what my child needs.”) (59). Consequently, a possible explanation could be that caregivers, who have greater conscious difficulties understanding and empathizing with their child experience greater distress and are therefore more willing to invest in understanding their child better through participating in the study.
5 Limitations and outlook
The present study has several limitations that must be taken into consideration when interpreting the results.
Firstly, the sample size was relatively small, limiting the ability to detect small to medium treatment effects due to reduced statistical power. Additionally, due to the small sample size, the study did not include subgroup analyses according to child's primary diagnosis (ASD only, IDD only, ASS + IDD), which may have provided important insights into who may benefit most from this type of intervention. Moreover, given the broad age range of the children included in this study (4–11 years), future studies should assess the efficacy of the intervention for specific age groups.
Secondly, the absence of a control group prevents attributing changes in parental and child outcomes solely to the intervention as other factors, such as, e.g., natural variations or child maturation, could also contribute to the changes. It would be valuable to further investigate whether especially caregivers with limited access to professional resources and less familiarity with their child's diagnosis experience greater benefits from the intervention. Thus, future studies should conduct an RCT with a larger sample size to allow for more robust and nuanced analyses of efficacy including moderators and mediators.
Thirdly, due to the unpredictability of the frequency of CB episodes and the number of identified causal factors for CB for each participant, it was not possible to prescribe a set treatment dosage (e.g., how often behavioural analyses should be performed, how many techniques should be put into practice, how much time should be spent reading knowledge chapters etc.), which may have led to considerable heterogeneity in terms of treatment intensity.
Furthermore, it was not monitored whether participants were able to successfully perform behaviour analyses and implement the rather complex recommendations. A therapist-led introduction to the ProVIA-Kids app and joint implementation of the first few behavioural analyses may increase caregivers' understanding of the rationale of behavioural analyses and enhance their ability to accurately interpret the results. Therefore, future studies should include an intervention group involving (initial) therapist guidance to assess whether this can significantly increase the efficacy of the intervention.
For the EMA-based analyses, we set very liberal criteria for who was included (used the mood diary for at least six weeks, had made at minimum one entry per week and had available values in week 1 and week 8). In a study investigating efficacy, it would be necessary to define rules regarding missing assessments and set the threshold higher than in our pilot study.
Another limitation concerns the lack of representation of male caregivers in our sample. Although families could freely choose which caregiver primarily used the app, only female caregivers enrolled as study participants. Meta-analyses show that including fathers in parent training significantly enhances positive changes in children's behaviour and parenting practices (89), although fathers are consistently underrepresented in parenting interventions (90). Future studies should strive to engage both caregivers as app users and investigate the efficacy of the ProVIA-Kids app separately by sex of the caregivers.
A further limitation of the study is the dependence on caregiver report to evaluate both parental stress and parenting practices as well as children's CB. Relying on a single source of information can lead to biases and inaccuracies in the collected data. In order to reach a deeper understanding of the outcome variables and increase validity and generalizability of the results, a multi-informant approach should be applied in future studies. Furthermore, since a single informant does not possess a comprehensive knowledge about the child's behaviour in various settings and contexts, a jointly usable version of the ProVIA-Kids app should be developed which aggregates data from all persons involved in the child's care. However, this, in turn, presents a challenge as all parties involved need to consistently use the app and coordinate in implementing the recommendations to achieve improvements in the child's CB.
Lastly, in order to improve treatment adherence and app engagement, interactive gamification elements could be incorporated in the app, which could not be realized in the present study due to time and monetary constraints.
6 Conclusion
The present study highlights the potential benefits of self-directed interventions in improving child CB and parental well-being in families of children with ASD and/or IDD. Even over a short period of 8 weeks, the ProVIA-Kids app shows promise for reducing overreactive parenting practices and participants report a reduction of EMA-based parental stress experience due to child's CB. Descriptive results indicate a potential benefit in terms of children's CB, which may take longer to fully manifest. Thus, the study addresses the high demand for evidence-based, accessible, cost-effective, and low-threshold tools for caregivers of children with ASD and/or IDD who display CB. Pioneering the translation of structured behaviour analysis into a digital and automated context, ProVIA-Kids presents a promising approach for guiding caregivers in systemically modifying the causes and thus preventing their child's CB. Future research should revise the app by incorporating gamification elements and conduct an RCT with a larger sample size and an extended intervention period with the aim to gain a deeper insight into moderators and mediators. Prospectively, ProVIA-Kids could be adapted for group and team settings such as kindergartens, school, and residential facilities by e.g., allowing joint use by multiple caregivers.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Medizinische Ethikkommission an der Julius-Maximilians-Universität Würzburg, Josef-Schneider-Str. 4, 97080 Würzburg, Germany. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
Author contributions
RM: Data curation, Formal Analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. HB: Writing – original draft, Writing – review & editing. KK: Data curation, Project administration, Software, Writing – review & editing, Writing – original draft. MG: Software, Writing – review & editing, Data curation, Project administration. JS: Writing – review & editing, Software. CR: Funding acquisition, Methodology, Writing – review & editing, Conceptualization. RP: Writing – review & editing, Funding acquisition, Methodology, Supervision, Writing – original draft. RT: Writing – review & editing, Conceptualization. MR: Writing – review & editing, Funding acquisition. MG: Supervision, Writing – review & editing. JG: Writing – original draft, Writing – review & editing, Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The ProVIA trial was funded by the Bavarian State Ministry of Family, Labour and Social Affairs. This grant provided the financial means for study coordination, development of the intervention and programming of the smartphone application. The funding source had no role in the trial design of this study and will play no role in its execution, analyses and interpretation of the data, or the decision to publish results.
Acknowledgments
We thank Tim Güntzel for supporting content development with his extensive experience as senior physician in the Klinik am Greinberg, a specialized clinic for children with intellectual disabilities and mental disorders. We thank Theresa Breitner, Valentina Raba and Verena Schellein for translating the psychoeducational content into plain language and thus making ProVIA-Kids more widely accessible, Jakob Bartels for providing photographs to illustrate the psychoeducational content and Alexander Schmitt for providing audio recordings for resource building and relaxation.
Finally, we thank all families who participated in our study and supported out research.
Conflict of interest
RP is a partner in Lenox UG, which has set itself the goal of translating scientific findings into digital health applications. Lenox UG holds shares in Health Study Club GmbH. RP received consulting fees, reimbursements for congress attendance and travel expenses as well as payments for lectures in the context of diabetes topics and in connection with mobile health and e–mental health topics.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fdgth.2024.1462682/full#supplementary-material
References
1. Psychiatrists RCo. Challenging Behaviour: A Unified Approach. London, UK: Royal College of Psychiatrists (2007).
2. Newcomb ET, Hagopian LP. Treatment of severe problem behaviour in children with autism spectrum disorder and intellectual disabilities. Int Rev Psychiatry. (2018) 30(1):96–109. doi: 10.1080/09540261.2018.1435513
3. NICE. Challenging Behaviour and Learning Disabilities: Prevention and Interventions for People with Learning Disabilities Whose Behaviour Challenges. Clinical Guideline no. 11. National Institute for Health and Care Excellence (2015).
4. NICE. The Management and Support of Children and Young People on the Autism spectrum. Clinical Guideline no. 170. National Institute for Health and Care Excellence (2013).
5. Baker BL, Blacher J, Olsson MB. Preschool children with and without developmental delay: behaviour problems, parents’ optimism and well-being. J Intellect Disabil Res. (2005) 49(Pt 8):575–90. doi: 10.1111/j.1365-2788.2005.00691.x
6. Emerson E, Einfeld S, Stancliffe RJ. The mental health of young children with intellectual disabilities or borderline intellectual functioning. Soc Psychiatry Psychiatr Epidemiol. (2010) 45(5):579–87. doi: 10.1007/s00127-009-0100-y
7. Allen DG, Lowe K, Moore K, Brophy S. Predictors, costs and characteristics of out of area placement for people with intellectual disability and challenging behaviour. J Intellect Disabil Res. (2007) 51(Pt. 6):409–16. doi: 10.1111/j.1365-2788.2006.00877.x
8. Felce D, Lowe K, Perry J, Baxter H, Jones E, Hallam A, et al. Service support to people in Wales with severe intellectual disability and the most severe challenging behaviours: processes, outcomes and costs. J Intellect Disabil Res. (1998) 42(Pt 5):390–408. doi: 10.1046/j.1365-2788.1998.00153.x
9. Beck A, Daley D, Hastings RP, Stevenson J. Mothers’ expressed emotion towards children with and without intellectual disabilities. J Intellect Disabil Res. (2004) 48(7):628–38. doi: 10.1111/j.1365-2788.2003.00564.x
10. Bonis S. Stress and parents of children with autism: a review of literature. Issues Ment Health Nurs. (2016) 37(3):153–63. doi: 10.3109/01612840.2015.1116030
11. Fidler DJ, Hodapp RM, Dykens EM. Stress in families of young children with down syndrome, williams syndrome, and smith-magenis syndrome. Early Educ Dev. (2000) 11(4):395–406. doi: 10.1207/s15566935eed1104_2
12. Häßler F, Caby F, Hoffmann KH, Irblich D, Mall V, Mendes U, et al. S2k Praxisleitlinie Intelligenzminderung. AWMF-Register Nr. 028-042. AWMF (2021).
13. Saemundsen E, Magnússon P, Georgsdóttir I, Egilsson E, Rafnsson V. Prevalence of autism spectrum disorders in an Icelandic birth cohort. BMJ Open. (2013) 3(6):e002748. doi: 10.1136/bmjopen-2013-002748
14. Dworschak W, Ratz C, Wagner M. Prevalence and putative risk markers of challenging behavior in students with intellectual disabilities. Res Dev Disabil. (2016) 58:94–103. doi: 10.1016/j.ridd.2016.08.006
15. Matson JL, Wilkins J, Macken J. The relationship of challenging behaviors to severity and symptoms of autism spectrum disorders. J Ment Health Res Intellect Disabil. (2008) 2(1):29–44. doi: 10.1080/19315860802611415
16. Tsiouris JA, Kim SY, Brown WT, Cohen IL. Association of aggressive behaviours with psychiatric disorders, age, sex and degree of intellectual disability: a large-scale survey. J Intellect Disabil Res. (2011) 55(7):636–49. doi: 10.1111/j.1365-2788.2011.01418.x
17. Argumedes M, Lanovaz MJ, Larivée S. Brief report: impact of challenging behavior on parenting stress in mothers and fathers of children with autism spectrum disorders. J Autism Dev Disord. (2018) 48(7):2585–9. doi: 10.1007/s10803-018-3513-1
18. Blacher J, McIntyre LL. Syndrome specificity and behavioural disorders in young adults with intellectual disability: cultural differences in family impact. J Intellect Disabil Res. (2006) 50(3):184–98. doi: 10.1111/j.1365-2788.2005.00768.x
19. Eisenhower AS, Baker BL, Blacher J. Preschool children with intellectual disability: syndrome specificity, behaviour problems, and maternal well-being. J Intellect Disabil Res. (2005) 49(9):657–71. doi: 10.1111/j.1365-2788.2005.00699.x
20. Zeedyk SM, Cohen SR, Blacher J. Syndrome-Specific impact on parental well-being: autism compared. In: Patel VB, Preedy VR, Martin CR, editors. Comprehensive Guide to Autism. New York, NY: Springer New York (2014). p. 625–50.
21. Giovagnoli G, Postorino V, Fatta LM, Sanges V, De Peppo L, Vassena L, et al. Behavioral and emotional profile and parental stress in preschool children with autism spectrum disorder. Res Dev Disabil. (2015) 45–46:411–21. doi: 10.1016/j.ridd.2015.08.006
22. Emerson E, Bromley J. The form and function of challenging behaviours. J Intellect Disabil Res. (1995) 39(5):388–98. doi: 10.1111/j.1365-2788.1995.tb00543.x
23. McClintock K, Hall S, Oliver C. Risk markers associated with challenging behaviours in people with intellectual disabilities: a meta-analytic study. J Intellect Disabil Res. (2003) 47(Pt 6):405–16. doi: 10.1046/j.1365-2788.2003.00517.x
24. Didden R, Korzilius H, van Oorsouw W, Sturmey P. Behavioral treatment of challenging behaviors in individuals with mild mental retardation: meta-analysis of single-subject research. Am J Ment Retard. (2006) 111:290–8. doi: 10.1352/0895-8017(2006)111[290:BTOCBI]2.0.CO;2
25. Oliver C, McClintock K, Hall S, Smith M, Dagnan D, Stenfert-Kroese B. Assessing the severity of challenging behaviour: psychometric properties of the challenging behaviour interview. J Appl Res Intellect Disabil. (2003) 16(1):53–61. doi: 10.1046/j.1468-3148.2003.00145.x
26. Holden B, Gitlesen JP. A total population study of challenging behaviour in the county of Hedmark, Norway: prevalence, and risk markers. Res Dev Disabil. (2006) 27(4):456–65. doi: 10.1016/j.ridd.2005.06.001
27. Kearney DS, Healy O. Investigating the relationship between challenging behavior, co-morbid psychopathology and social skills in adults with moderate to severe intellectual disabilities in Ireland. Res Dev Disabil. (2011) 32(5):1556–63. doi: 10.1016/j.ridd.2011.01.053
28. Peters-Scheffer N, Didden R. Chapter 4—functional analysis methodology in developmental disabilities. In: Sturmey P, editor. Functional Analysis in Clinical Treatment. 2nd ed. San Diego: Academic Press (2020). p. 75–95.
29. Sjgafoos J, Elkins J, Kerr M, Attwood T. A survey of aggressive behaviour among a population of persons with intellectual disability in Queensland. J Intellect Disabil Res. (1994) 38(4):369–81. doi: 10.1111/j.1365-2788.1994.tb00417.x
30. Matson JL, Williams LW. Functional assessment of challenging behavior. Curr Dev Disord Rep. (2014) 1(2):58–66. doi: 10.1007/s40474-013-0006-y
31. Hastings RP. Parental stress and behaviour problems of children with developmental disability. J Intellect Dev Disabil. (2002) 27(3):149–60. doi: 10.1080/1366825021000008657
32. Harvey ST, Boer D, Meyer LH, Evans IM. Updating a meta-analysis of intervention research with challenging behaviour: treatment validity and standards of practice. J Intellect Dev Disabil. (2009) 34(1):67–80. doi: 10.1080/13668250802690922
33. Heyvaert M, Maes B, Onghena P. A meta-analysis of intervention effects on challenging behaviour among persons with intellectual disabilities. J Intellect Disabil Res. (2010) 54(7):634–49. doi: 10.1111/j.1365-2788.2010.01291.x
34. Postorino V, Sharp WG, McCracken CE, Bearss K, Burrell TL, Evans AN, et al. A systematic review and meta-analysis of parent training for disruptive behavior in children with autism spectrum disorder. Clin Child Fam Psychol Rev. (2017) 20(4):391–402. doi: 10.1007/s10567-017-0237-2
35. Groves L, Jones C, Welham A, Hamilton A, Liew A, Richards C. Non-pharmacological and pharmacological interventions for the reduction or prevention of topographies of behaviours that challenge in people with intellectual disabilities: a systematic review and meta-analysis of randomised controlled trials. Lancet Psychiatry. (2023) 10(9):682–92. doi: 10.1016/S2215-0366(23)00197-9
36. Ruane A, Carr A. Systematic review and meta-analysis of stepping stones triple P for parents of children with disabilities. Fam Process. (2019) 58(1):232–46. doi: 10.1111/famp.12352
37. Hassiotis A. Time to rethink behaviours that challenge in people with intellectual disabilities. Lancet Psychiatry. (2023) 10(9):654–5. doi: 10.1016/S2215-0366(23)00253-5
38. Tarver J, Daley D, Lockwood J, Sayal K. Are self-directed parenting interventions sufficient for externalising behaviour problems in childhood? A systematic review and meta-analysis. Eur Child Adolesc Psychiatry. (2014) 23(12):1123–37. doi: 10.1007/s00787-014-0556-5
39. Neece CL, Green SA, Baker BL. Parenting stress and child behavior problems: a transactional relationship across time. Am J Intellect Dev Disabil. (2012) 117(1):48–66. doi: 10.1352/1944-7558-117.1.48
40. Hayes SA, Watson SL. The impact of parenting stress: a meta-analysis of studies comparing the experience of parenting stress in parents of children with and without autism spectrum disorder. J Autism Dev Disord. (2013) 43(3):629–42. doi: 10.1007/s10803-012-1604-y
41. Lewallen AC, Neece CL. Improved social skills in children with developmental delays after parent participation in MBSR: the role of parent–child relational factors. J Child Fam Stud. (2015) 24(10):3117–29. doi: 10.1007/s10826-015-0116-8
42. Frantz R, Hansen SG, Machalicek W. Interventions to promote well-being in parents of children with autism: a systematic review. Rev J Autism Dev Disords. (2018) 5(1):58–77. doi: 10.1007/s40489-017-0123-3
43. Päckert J. Stationäre und Ambulante Versorgung von Menschen mit Intelligenzminderung und Psychischen StörUngen in den Kliniken für Kinder- und Jugendpsychiatrie / Psychotherapie in Deutschland. Rostock, Germany: Universität Rostock (2019).
44. Soltau B, Biedermann J, Hennicke K, Fydrich T. Mental health needs and availability of mental health care for children and adolescents with intellectual disability in Berlin. J Intellect Disabil Res. (2015) 59(11):983–94. doi: 10.1111/jir.12185
45. Riedel A, Biscaldi M, Tebartz van Elst L. Autismus und Asperger - Welche Rolle spielt der Hausarzt? Der Allgemeinarzt. (2017) 39(14):44–7.
46. Bachmann C, Hoffmann F. Autismus-Spektrum-Störungen in deutschland: diagnoseprävalenz, medizinische versorgung und zeitliche trends. In: Klauber J, Günster C, Gerste B, Robra BP, Schmacke N, editors. Versorgungs-Report 2015/2016 Schwerpunkt: Kinder und Jugendliche. Stuttgart: Schattauer (2015). p. 167–84.
47. Shic F, Goodwin M. Introduction to technologies in the daily lives of individuals with autism. J Autism Dev Disord. (2015) 45(12):3773–6. doi: 10.1007/s10803-015-2640-1
48. Whitehouse AJO, Granich J, Alvares G, Busacca M, Cooper MN, Dass A, et al. A randomised controlled trial of an iPad-based application to complement early behavioural intervention in autism spectrum disorder. J Child Psychol Psychiatry. (2017) 58(9):1042–52. doi: 10.1111/jcpp.12752
49. Kim JW, Nguyen T-Q, Gipson SY-MT, Shin AL, Torous J. Smartphone apps for autism Spectrum disorder—understanding the evidence. Journal of Technology in Behavioral Science. (2018) 3(1):1–4. doi: 10.1007/s41347-017-0040-4
50. An S, Feng X, Dai Y, Bo H, Wang X, Li M, et al. Development and evaluation of a speech-generating AAC mobile app for minimally verbal children with autism spectrum disorder in mainland China. Mol Autism. (2017) 8(1):52. doi: 10.1186/s13229-017-0165-5
51. Moon S, Hwang J, Hill H, Kervin R, Brown Birtwell K, Torous J, et al. Mobile device applications and treatment of autism spectrum disorder: a systematic review and meta-analysis of effectiveness. Arch Dis Child. (2020) 105(5):458. doi: 10.1136/archdischild-2019-318258
52. Sheehan R, Hassiotis A. Digital mental health and intellectual disabilities: state of the evidence and future directions. Evid Based Mental Health. (2017) 20(4):107. doi: 10.1136/eb-2017-102759
53. Johnson N, Bree O, Lalley EE, Rettler K, Grande P, Gani MO, et al. Effect of a social script iPad application for children with autism going to imaging. J Pediatr Nurs. (2014) 29(6):651–9. doi: 10.1016/j.pedn.2014.04.007
54. Trudel L, Lanovaz MJ, Préfontaine I. Brief report: mobile technology to support parents in reducing stereotypy. J Autism Dev Disord. (2021) 51(7):2550–8. doi: 10.1007/s10803-020-04735-6
55. Bonnot O, Adrien V, Venelle V, Bonneau D, Gollier-Briant F, Mouchabac S. Mobile app for parental empowerment for caregivers of children with autism Spectrum disorders: prospective open trial. JMIR Ment Health. (2021) 8(9):e27803. doi: 10.2196/27803
56. Geissler J, Buchholz H, Meerson R, Kammerer K, Göster M, Schobel J, et al. Smartphone-based behaviour analysis for challenging behaviour in intellectual and developmental disabilities and autism spectrum disorder—study protocol for the ProVIA trial. Front Neurosci. (2022) 16:984618. doi: 10.3389/fnins.2022.984618
57. Kroenke K, Spitzer RL, Williams JBW. The PHQ-9. J Gen Intern Med. (2001) 16(9):606–13. doi: 10.1046/j.1525-1497.2001.016009606.x
58. Kanfer FH, Saslow G. Behavioral diagnosis. In: Franks C, editor. Behavior Therapy. Appraisal and status: McGraw-Hill (1969). p. 417–44.
59. Tröster H. Eltern-Belastungs-Inventar (EBI). Deutsche Version des Parenting Stress Index (PSI) von R.R. Abidin. Göttingen: Hogrefe (2011).
60. Abidin RR. Parenting Stress Index. Professional Manual. Odessa, FL: Psychological Assessment Resources (1995).
61. Miller Y. Erziehung von Kindern im Kindergartenalter: Erziehungsverhalten und Kompetenzüberzeugungen von Eltern und der Zusammenhang zu Kindlichen Verhaltensstörungen. Braunschweig, Germany: Technische Universität Braunschweig (2001).
62. Naumann S, Bertram H, Kuschel A, Heinrichs N, Hahlweg K, Dopfner M. The erziehungsfragebogen (EFB): an instrument to assess parental behavioral tendencies in discipline situations with her children. Diagnostica. (2010) 56(3):144–57. doi: 10.1026/0012-1924/a000018
63. Leung C, Chan S, Lam T, Yau S, Tsang S. The effect of parent education program for preschool children with developmental disabilities: a randomized controlled trial. Res Dev Disabil. (2016) 56:18–28. doi: 10.1016/j.ridd.2016.05.015
64. Iadarola S, Levato L, Harrison B, Smith T, Lecavalier L, Johnson C, et al. Teaching parents behavioral strategies for autism Spectrum disorder (ASD): effects on stress, strain, and competence. J Autism Dev Disord. (2018) 48(4):1031–40. doi: 10.1007/s10803-017-3339-2
65. Schrott B, Kasperzack D, Weber L, Becker K, Burghardt R, Kamp-Becker I. Effectiveness of the stepping stones triple P group parenting program as an additional intervention in the treatment of autism Spectrum disorders: effects on parenting variables. J Autism Dev Disord. (2019) 49(3):913–23. doi: 10.1007/s10803-018-3764-x
66. Kong M-y, Au T-f. The incredible years parent program for Chinese preschoolers with developmental disabilities. Early Educ Dev. (2018) 29(4):494–514. doi: 10.1080/10409289.2018.1461987
67. Leung C, Fan A, Sanders MR. The effectiveness of a group triple P with Chinese parents who have a child with developmental disabilities: a randomized controlled trial. Res Dev Disabil. (2013) 34(3):976–84. doi: 10.1016/j.ridd.2012.11.023
68. Kierfeld F, Ise E, Hanisch C, Gortz-Dorten A, Dopfner M. Effectiveness of telephone-assisted parent-administered behavioural family intervention for preschool children with externalizing problem behaviour: a randomized controlled trial. Eur Child Adolesc Psychiatry. (2013) 22(9):553–65. doi: 10.1007/s00787-013-0397-7
69. Sanders MR, Baker S, Turner KMT. A randomized controlled trial evaluating the efficacy of triple P online with parents of children with early-onset conduct problems. Behav Res Ther. (2012) 50(11):675–84. doi: 10.1016/j.brat.2012.07.004
70. Rivard M, Morin M, Mercier C, Terroux A, Mello C, Lépine A. Social validity of a training and coaching program for parents of children with autism spectrum disorder on a waiting list for early behavioral intervention. J Child Fam Stud. (2017) 26(3):877–87. doi: 10.1007/s10826-016-0604-5
71. Medda JE, Kitzerow J, Schlitt S, Berndt K, Schwenck C, Uhlmann L, et al. Prä-post-Effekte des autismus-spezifischen psychoedukativen elterntrainings FAUT-E. Z Kinder Jugendpsychiatr Psychother. (2020) 49(2):134–43. doi: 10.1024/1422-4917/a000781
72. Bagner DM, Eyberg SM. Parent–child interaction therapy for disruptive behavior in children with mental retardation: a randomized controlled trial. J Clin Child Adolesc Psychol. (2007) 36(3):418–29. doi: 10.1080/15374410701448448
73. Küçüker S. The family-focused early intervention programme: evaluation of parental stress and depression. Early Child Dev Care. (2006) 176(3–4):329–41. doi: 10.1080/03004430500206957
74. Plant KM, Sanders MR. Reducing problem behavior during care-giving in families of preschool-aged children with developmental disabilities. Res Dev Disabil. (2007) 28(4):362–85. doi: 10.1016/j.ridd.2006.02.009
75. Markie-Dadds C, Sanders MR. Self-Directed triple P (positive parenting program) for mothers with children at-risk of developing conduct problems. Behav Cogn Psychother. (2006) 34(3):259–75. doi: 10.1017/S1352465806002797
76. Lovibond SH, Lovibond PF. Manual for the Depression Anxiety Stress Scales. 2nd ed. Sydney, Australia: Psychology Foundation of Australia (1995).
77. Berry JO, Jones WH. The parental stress scale: initial psychometric evidence. J Soc Pers Relat. (1995) 12(3):463–72. doi: 10.1177/0265407595123009
79. Piotrowska PJ, Tully LA, Collins DAJ, Sawrikar V, Hawes D, Kimonis ER, et al. Parentworks: evaluation of an online, father-inclusive, universal parenting intervention to reduce child conduct problems. Child Psychiatry Hum Dev. (2020) 51(4):503–13. doi: 10.1007/s10578-019-00934-0
80. Tonge B, Brereton A, Kiomall M, Mackinnon A, King N, Rinehart N. Effects on parental mental health of an education and skills training program for parents of young children with autism: a randomized controlled trial. J Am Acad Child Adolesc Psychiatry. (2006) 45(5):561–9. doi: 10.1097/01.chi.0000205701.48324.26
81. Sofronoff K, Jahnel D, Sanders M. Stepping stones triple P seminars for parents of a child with a disability: a randomized controlled trial. Res Dev Disabil. (2011) 32(6):2253–62. doi: 10.1016/j.ridd.2011.07.046
82. Whittingham K, Sofronoff K, Sheffield J, Sanders MR. Stepping stones triple P: an RCT of a parenting program with parents of a child diagnosed with an autism Spectrum disorder. J Abnorm Child Psychol. (2009) 37(4):469–80. doi: 10.1007/s10802-008-9285-x
83. Tellegen CL, Sanders MR. A randomized controlled trial evaluating a brief parenting program with children with autism spectrum disorders. J Consult Clin Psychol. (2014) 82:1193–200. doi: 10.1037/a0037246
84. Ku B, Stinson JD, MacDonald M. Parental behavior comparisons between parents of children with autism spectrum disorder and parents of children without autism Spectrum disorder: a meta-analysis. J Child Fam Stud. (2019) 28(6):1445–60. doi: 10.1007/s10826-019-01412-w
85. Gorin A, Stone A. Recall biases and cognitive errors in retrospective self reports: a call for momentary assessments. Handb Health Psychol. (2001) 23:405–13.
86. Kanouse D, Hanson L. Negativity in evaluations. In: Jones E, editor. Attribution. Perceiving the Causes of Behavior: General Learning Press (1972). p. 1173–84.
87. Moore TR, Symons FJ. Adherence to behavioral and medical treatment recommendations by parents of children with autism Spectrum disorders. J Autism Dev Disord. (2009) 39(8):1173–84. doi: 10.1007/s10803-009-0729-0
88. Detrich R. Increasing treatment fidelity by matching interventions to contextual variables within the educational setting. Sch Psychol Rev. (1999) 28(4):608–20. doi: 10.1080/02796015.1999.12085988
89. Lundahl BW, Tollefson D, Risser H, Lovejoy MC. A meta-analysis of father involvement in parent training. Res Soc Work Pract. (2007) 18(2):97–106. doi: 10.1177/1049731507309828
Keywords: autism spectrum disorder, challenging behaviour, behaviour analysis, mental health application, cognitive behaviour therapy, parent training, parental stress, intellectual and development disabilities
Citation: Meerson R, Buchholz H, Kammerer K, Göster M, Schobel J, Ratz C, Pryss R, Taurines R, Romanos M, Gamer M and Geissler J (2024) ProVIA-Kids - outcomes of an uncontrolled study on smartphone-based behaviour analysis for challenging behaviour in children with intellectual and developmental disabilities or autism spectrum disorder. Front. Digit. Health 6:1462682. doi: 10.3389/fdgth.2024.1462682
Received: 10 July 2024; Accepted: 26 August 2024;
Published: 13 September 2024.
Edited by:
Hui Zheng, Zhejiang Normal University, ChinaReviewed by:
Daniel Z. Q. Gan, The University of Melbourne, AustraliaPaula Sophia Sterkenburg, VU Amsterdam, Netherlands
Copyright: © 2024 Meerson, Buchholz, Kammerer, Göster, Schobel, Ratz, Pryss, Taurines, Romanos, Gamer and Geissler. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Julia Geissler, Z2Vpc3NsZXJfakB1a3cuZGU=