 Md Shafiqur Rahman Jabin
Md Shafiqur Rahman Jabin
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Digit. Health, 14 March 2024
Sec. Health Informatics
Volume 6 - 2024 | https://doi.org/10.3389/fdgth.2024.1367431
This article is part of the Research TopicElectronic Patient-reported Outcomes for Patient Care ImprovementView all 11 articles
Despite many benefits, the extensive deployment of Health Information Technology (HIT) systems by healthcare organizations has encountered many challenges, particularly in the field of telemetry concerning patient monitoring and its operational workflow. These challenges can add more layers of complexity when an unplanned software security patching is performed, affecting patient monitoring and causing disruption in daily clinical operations. This study is a reflection on what happened associated with software security patching and why it happened through the lens of an incident report to develop potential preventive and corrective strategies using qualitative analyses—inductive and deductive approaches. There is a need for such analyses to identify the underlying mechanism behind such issues since very limited research has been conducted on the study of software patching. The incident was classified as a “software functionality” issue, and the consequence was an “incident with a noticeable consequence but no patient harm”, and the contributing factor was a software update, i.e., software security patching. This report describes how insufficient planning of software patching, lack of training for healthcare professionals, contingency planning on unplanned system disruption, and HIT system configuration can compromise healthcare quality and cause risks to patient safety. We propose 15 preventive and corrective strategies grouped under four key areas based on the system approach and social-technical aspects of the patching process. The key areas are (i) preparing, developing, and deploying patches; (ii) training the frontline operators; (iii) ensuring contingency planning; and (iv) establishing configuration and communication between systems. These strategies are expected to minimize the risk of HIT-related incidents, enhance software security patch management in healthcare organizations, and improve patient safety. However, further discussion should be continued about general HIT problems connected to software security patching.
“A software patch or fix is a quick-repair job for a piece of programming designed to resolve functionality issues, improve security, or add new features” (1). Software patching is a growing key aspect of today's computing environment (2), particularly in the healthcare environment (3) in which the volume, complexity, and number of configurations have increased considerably. A number of challenges associated with software security patching have been encountered in modern healthcare, including delayed patch applications (4), vulnerability scanning, assessment, and prioritization (5). The consequences of such problems due to software patching are enormous, such as causing delays in healthcare management and even risks to patient safety (4, 6). However, the underlying mechanism behind these issues is still unknown in most cases; for example, why and how delays occur while applying those patches (4). In addition, very limited research has been conducted on the study of software security patching, particularly in the context of healthcare.
HIT systems were deployed with the vision of making care delivery safer and more efficient by reducing adverse events and improving accuracy (7). The HITs have improved several dimensions of healthcare quality, such as enhancing the security and confidentiality of personal health information (8), improving patient safety, and increasing efficiency and effectiveness (9). Despite their numerous benefits, the introduction of HITs has encountered substantial problems, including planning, design, implementation, and management (10, 11).
Several studies of implementation science have indicated that the deployment of HIT systems might be successful in one setting but not in others (12). New and often unexpected problems arise, compromising the quality of healthcare and requiring diligent attention and awareness whenever a new technology or solution is introduced (13). Several pieces of evidence suggest that different HIT systems, such as radiology information systems (10, 11, 14) and e-prescribing systems (15), can pose serious consequences, ranging from workflow interruptions (16) and patient inconvenience (9) to multiple patient harm (17). Similarly, patient monitoring systems, such as an ECG monitoring system, can encounter various challenges, including system integration, complex computational needs, and patient/user resistance (18). While some studies suggested that the accuracy and reliability of remote patient monitoring systems can be questioned (19), others reported that security and privacy could also be the major challenges of these systems (20).
HIT systems, particularly those used in patient monitoring, such as central monitoring systems and alarm detectors, are commonly endorsed as the solution to many of the problems encountered by the Emergency Department or intensive care unit (21). Healthcare professionals, such as nurses, heavily depend on such systems, which allow them to monitor the vital signs of multiple patients on the same screen without being physically present in the patient room (22). While there is some evidence for the clinical benefits of this efficient system, there is reported evidence that patient monitoring systems can cause various challenges to patients, compromising healthcare quality (23).
The incident reporting process ensures reflection on what has happened, why it has happened, and how it might have been minimized (13). Sometimes, the incidents can act as an “early warning system” by identifying new issues before reaching the patient (24). They can be used as a basis for devising preventive and corrective strategies and strategies to prevent them from harming the patients (13). Incident reporting may also play a key role in improving the patient safety culture of a healthcare organization with the local follow-up of incidents (25). This necessitates qualitative analysis of the free-text narratives or anecdotes using inductive and deductive techniques. The inductive approach may include content analysis, whereas the deductive method may comprise the classification of the critical aspects of the qualitative data by feeding them into an existing framework, such as the HIT Classification System (HIT-CS) (26).
Since little research has been performed on software security patch management, there is an urgent need for qualitative analysis to explore the issue. Therefore, this case report will present how inappropriate planning of software patching can affect the patient monitoring system and cause disruption in day-to-day clinical operations and care delivery through the lens of an incident report. The report will also provide some useful insights for practitioners and researchers to understand what and where strategies are necessary to better support the patch management process.
The incident (presented in Box 1) was reported in an electronic incident management database for medical devices, i.e., the reidarMTP. The reidarMTP aims to make essential information on medical devices readily available for the healthcare environment, primarily in Sweden and the Nordic countries, such as Denmark, Norway, Finland, and Iceland. The reidarMTP is operated by a voluntary association of Clinical Engineering departments in Swedish hospitals and is handled by certified staff trained to report such information into an open database. The information in the web database is anonymous and freely available to all healthcare professionals for quality improvement, education, and training (27, 28).
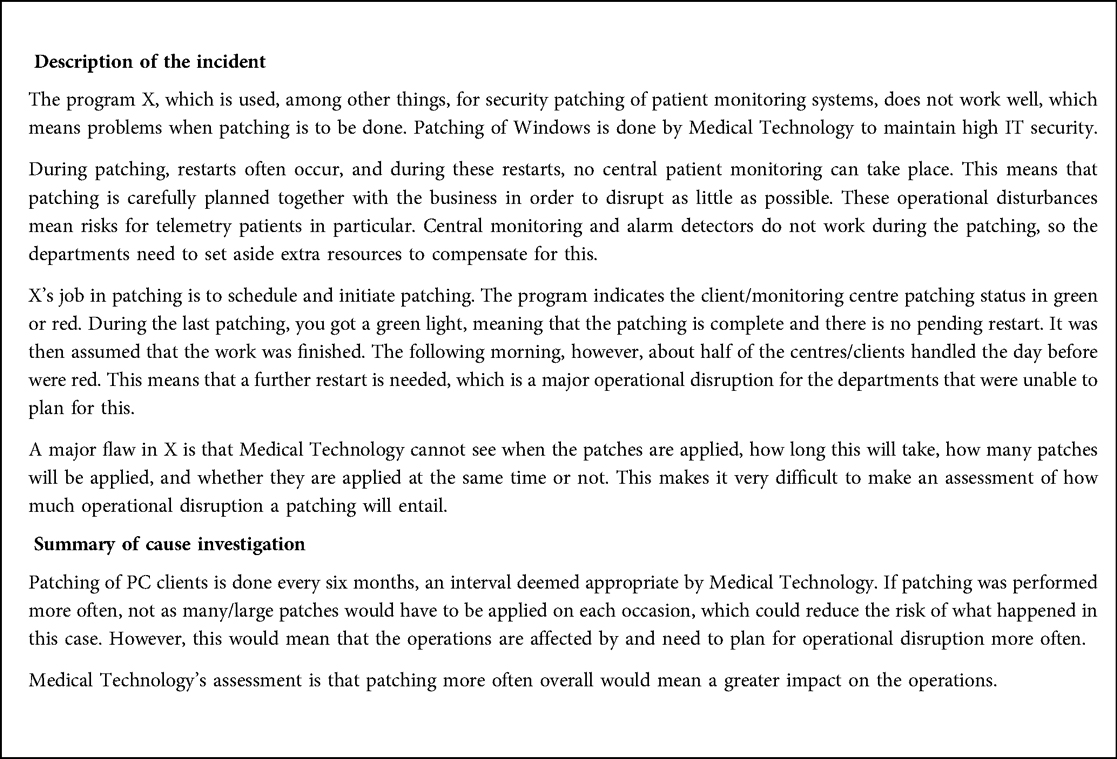
Box 1. This software security patching-related incident was reported to the reidarMTP by an anonymous user showing responses to the following categories of information.
The incidents are generally categorized into several different fields, entailing different sets of information. The first category includes the date, day, and time of events, an incident description with a short subject line, for example, “patching software for patient monitoring does not work well.” The second category is about the type of products involved in the incident, such as product name, manufacturer, software version, serial/batch number, etc. The third category comprises investigation, such as a summary of cause investigation, a summary of actions, and a summary of follow-up. The final and fourth categories consist of classification or risk assessment, including risk of medical damage and underlying cause.
The incident has been filtered and illustrated in Box 1 in two fields: “incident description,” which was reported by anonymous healthcare staff, and “summary of cause investigation,” i.e., an internal investigated narrative of the reported incident. The report was delivered in Swedish and translated into English by a linguistic expert who is proficient in both Swedish and English. The technical nature of the content through the translation process was taken into consideration with the help of consensus by the linguistic expert and the principal investigator. To maintain anonymity, the name of the software product has been masked by “X”.
The incident was analyzed using both deductive and inductive approaches. The deductive approach included an existing framework proposed by Magrabi et al., i.e., the HIT-CS (26). The HIT-CS has particularly been tailored to address the issues arising from HIT in healthcare for deconstructing incidents, classifying HIT-related issues, and extracting meaningful information. Issues can be classified based on human or technical-related problems, whereas technical challenges can be grouped into hardware and software-related problems (26). The HIT-CS was used to identify the type of software issue, the type of consequence, and the contributing (human) factor. The inductive approach involved content analysis. The application of the existing framework, i.e., HIT-CS and content extraction analyses, were managed on a semantic level—the exact content of the incident was taken into consideration, and no assumptions were made about the latent underpinnings of the incident report. Both of these approaches helped develop a set of preventive and corrective strategies that could potentially minimize future occurrences of these risks.
The HIT-CS was used for incident classification to enhance transparency and understanding. The incident was classified as a technical issue, i.e., “software functionality”, and the consequence of the incident was categorized as “incident with noticeable consequence but no patient harm”, and the contributing factor was “integration with clinical workflow”.
Using the content analysis, the contributing factors, mitigating factors, and patient/ organizational outcomes were identified. The contributing factor was identified to be the software update, i.e., software security patching. Although the incident did not cause any harm to patients directly, the operational disruption was clearly indicated in the incident description. To mitigate such software issues, one has to be mindful not to use many or large patches if security patching is to be done frequently, i.e., every six months. Another mitigating factor was identified, i.e., a contingency plan for frequent operation disruption. There was no patient outcome described in the narrative; however, the organizational outcome was determined to be severe disruptions in the clinical workflow for several weeks.
The issue of software patching and the coordination of different components have become a common phenomenon in modern healthcare systems. The outcomes of these issues can cause workflow disruptions or delays in healthcare delivery and serious risks to patient safety (4, 6). For example, an empirical investigation in the healthcare sector indicated delays in applying software security patches, particularly in the patch deployment phase, due to coordination delays relating to technology, people, and organization (4). Another study proposed a similar theory, i.e., a lack of in-depth understanding of socio-technical aspects of the patching process and patching decisions causing delays in applying security patches (29). To mitigate such delays and maintain a timely security patch management process, the studies recommended coordination and interdependent software/ hardware components and the decisions made by multiple stakeholders involved. The delays can also be minimized by designing and developing computer-aided supportive tools (4, 29).
Jabin et al. demonstrated in 2019 that HIT incidents occurred at each step of the medical imaging workflow process and that human and technical factors play a role in problems related to patient details (16). Such disruptions in the workflow process cause significant delays in patient treatments, patient inconvenience, and risks to patient safety, including repeat images resulting in unnecessary radiation and even additional workload for radiographers, i.e., repeat reconstruction of radiographic images. A recent study indicated that approximately 41% of the total sample of incidents had a staff/organization-related outcome with a clear indication that workflow disruptions resulted in additional system/service/resource use and delays in using facilities/service/systems (7). These delays in treatment or procedure further cause delayed diagnosis, treatment initiation, impact, and monitoring. Such delays can even cause delays in the decision-making process regarding further treatment options—continuation, discontinuation, or change in treatment. This means that once an incorrect shred of information or document is initiated into the HIT system, an “automation bias” tends to be considered correct (30).
A robust mechanism of system resilience and high-reliability organizations must address system flaws or software-related issues, including software patches, in a timely manner (31). Ensuring a robust mechanism means that similar types of errors are not repeated in the future, which will further guarantee that preventive and corrective interventions are applied at a system level (32). Therefore, such a system-wide approach and reliable systems can quickly identify and fix the issues related to HIT systems, minimize the stress and dissatisfaction of healthcare professionals, and thus improve healthcare quality (33).
Based on the system approach and through the lens of social-technical aspects of the patching process associated with HIT systems, such as the patient monitoring system, we propose the following 15 preventive and corrective strategies, which are grouped under four key areas (as outlined in Box 2). The key areas are (i) preparing, developing, and deploying patches; (ii) training the frontline operators; (iii) ensuring contingency planning; and (iv) establishing configuration and communication between systems.
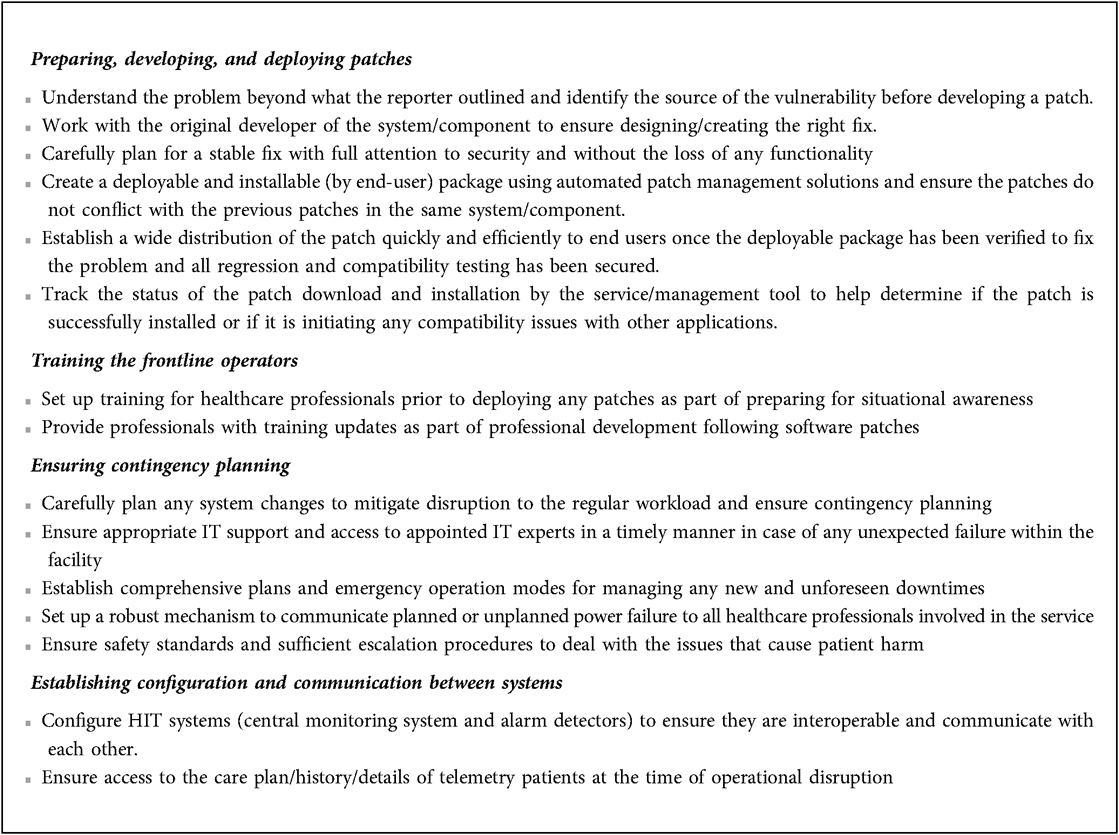
Box 2. Preventive and corrective strategies to mitigate and manage the risk of HIT incidents.
(i) Preparing, developing, and deploying patches—software security patch management in large and complex systems like healthcare is a challenging process that engages numerous stakeholders and involves multiple interdependent socio-technical decisions. A number of steps need to be followed systematically (as outlined in Box 2) in order to overcome patching security vulnerabilities. A systematic review of software security patch management based on 72 included studies identified 14 socio-technical challenges and 18 solution approaches, tools, and practices mapped into the process of software security patch management (5). The study drew some conclusions on various opportunities for practitioners to adopt new solutions to overcome common challenges and understand the variations of common practices.
We recommend that the readers use this systematic review as a guide or handbook for software security patch management—preparing, developing, and deploying patches. Figure 1 presents a mapping of the findings to enable the readers to identify the relationships between challenges and proposed solutions (5).
(ii) Training the frontline operators—providing training and education to healthcare professionals, ideally in cooperation with HIT vendors, prior to deploying any patches will mitigate the risk of patient harm.

Figure 1. A mapping of challenges onto solutions. Reprinted with permission from Dissanayake et al. (34), licensed under CC BY 4.0, https://doi.org/10.48550/arXiv.2012.00544.
Several studies suggest that training healthcare staff should be included in the planning process to effectively respond to a disruption. For example, a study on HIT risk and resilience states that “an organization's ability to effectively respond to a disruption not only depends on how effective it was in the planning process, but also how effective it was with its preparation, trials, and the training of their staff, which is often neglected” (35). Another study by Jabin et al. in 2019 identified the need to set up a process for initial and ongoing training of the operators to minimize the risks associated with human factors-related errors and workflow interruptions (13).
(iii) Ensuring contingency planning—a greater focus on stakeholder engagement in all aspects of healthcare practice, such as care providers, practice, quality, and/or departmental managers; accreditors, IT staff, and professional associations who set the standards of practice should be in place. This should include appropriate backup and emergency plans/measures to minimize disruption to regular care delivery, communicate unplanned power failure, and manage unexpected downtimes (33).
For example, a survey of US-based healthcare institutions focused on sharing HIT-related best practices and shared insight about Electronic Health Record (EHR)-related downtimes (36). The survey found that the majority of organizations experienced extended EHR-related downtimes, and most institutions implemented partial comprehensive contingency plans to mitigate the risks of unexpected EHR downtimes. The study concluded that “contingency planning” should be a routine part of all EHR-enabled healthcare organizations; we should eventually prepare for continuity of operations and ensure safe and effective healthcare.
(iv) Establishing configuration and communication between systems—configuration between different HIT systems, such as central monitoring systems and alarm detectors, should be considered at the time of design and purchase of systems (33).
Several other studies recommended to establish configuration and communication between systems as one of the strategies to overcome HIT-related issues and ensure safe and effective healthcare. For example, a study on e-prescribing-related challenges suggested ensuring software quality in an interfaced, networked healthcare environment since Lack of communication and appropriate configuration between systems was identified to be the major problem (15). Another similar study proposed that appropriate HIT configuration must be established to ensure access to prior studies, data integrity, and appropriate interfaces for record migration (17).
These strategies will be beneficial in improving healthcare quality and mitigating the risk of patient harm from issues with the HIT systems, such as the telemetry patient monitoring system. This recommendation guide will help set aside additional resources to compensate for any major operational disruptions; thus, the need for such a guide for healthcare professionals is urgent.
The major strength of this study is the use of both qualitative approaches, deductive (existing framework) and inductive (content analysis), permitting the investigator to obtain more detailed information from the incident report. Both of these approaches are most suitable due to their salient features for the qualitative data, i.e., free text narratives (17, 31); therefore, no other approach, such as Machine learning, could be applied. Although Machine learning could potentially extend the principle of qualitative analysis, offering a promising technique to scale up the coding process, one has to keep in mind that the study was on a single incident (not a set of incident reports) (37). Moreover, the application of both these approaches helps to minimize the potential subjective bias in devising 15 preventive and corrective strategies.
The incident report considered for this study was voluntary with its inherent limitations, including subjective bias, reporters’ lack of knowledge of the HIT systems/ software security patching, or inclination to provide a comprehensive report. In addition, a follow-up communication to glean additional information could not be conducted due to the anonymity of the reporter. Notwithstanding these limitations, the findings and the devised strategies can be considered as alerts to enlighten healthcare digitalization in Sweden to adopt the culture of digital safety and effectiveness. This also implies that the lessons learned from this case report can be useful and pertinent to adopt elsewhere for overall healthcare quality improvement and patient safety (7, 17, 32).
Major operational disruptions in the clinical workflow for several weeks may take place as a result of insufficient planning and complex processes (many/large/frequent patches) of software security patching. Such workflow interruptions occur due to inadequate training for frontline operators for unexpected system failure, lack of foresight, and poor understanding of HIT system integration into practice. To mitigate the identified risk, the software security patch management must be aligned with the context of clinical workflow. The first step of this alignment requires a proper understanding and consideration of proper planning, preparing, developing, and deploying patches. This should be followed by setting up the training process for healthcare professionals prior to any software patches and ensuring contingency planning to cope with any unexpected failures. The strategies should also include the configuration of HIT systems to ensure they are interoperable and communicate with each other.
As a multitude of settings, i.e., technology, people, and healthcare organizations, are potentially affected, it is challenging to specify in further detail. However, further discussion should be continued, emphasizing the need for adaptability in technology and healthcare practices and general HIT problems connected to software security patching. There is also a need to reinforce the necessity of systematic incident reporting as a fundamental practice for improving healthcare quality and patient safety.
The incident data has already been presented in Box 1. However, the data presented in this study are available on request from the corresponding author.
The studies involving humans were approved by Ethical Advisory Board in South East Sweden. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation was not required from the participants or the participants’ legal guardians/next of kin in accordance with the national legislation and institutional requirements.
MSRJ: Conceptualization, Data Collection, Formal Analysis, Investigation, Methodology, Writing – original draft, Writing – review & editing.
The author declares that financial support was received for the research, authorship, and/or publication of this article.
The research received no external funding. However, a publishing grant has been received from Linnaeus University as a part of the University Library's research support.
The author wish to thank Abdallah Hassoun, a Specialist in Medical Imaging and Functional Medicine of Region Gävleborg, and Max Birath, an M.Sc. student at the eHealth Institute, Linnaeus University.
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. TechTarget. Definition: Software Patch/Fix (2022). Available online at: https://www.techtarget.com/searchenterprisedesktop/definition/patch (accessed December 22, 2023).
2. Dadzie J. Understanding software patching: developing and deploying patches is an increasingly important part of the software development process. Queue. (2005) 3(2):24–30. doi: 10.1145/1053331.1053343
3. Srivastava AN, Schumann J. The case for software health management. 2011 IEEE Fourth International Conference on Space Mission Challenges for Information Technology; 2011 2-4 Aug (2011).
4. Dissanayake N, Zahedi M, Jayatilaka A, Babar MA. Why, how and where of delays in software security patch management: an empirical investigation in the healthcare sector. Proc ACM Hum-Comput Interact. (2022) 6(CSCW2):362. doi: 10.1145/3555087
5. Dissanayake N, Jayatilaka A, Zahedi M, Babar MA. Software security patch management—a systematic literature review of challenges, approaches, tools and practices. Inf Softw Technol. (2022) 144(C):21. doi: 10.1016/j.infsof.2021.106771
6. Meeks DW, Smith MW, Taylor L, Sittig DF, Scott JM, Singh H. An analysis of electronic health record-related patient safety concerns. J Am Med Inform Assoc. (2014) 21(6):1053–9. doi: 10.1136/amiajnl-2013-002578
7. Jabin MSR, Pan D, Nilsson E. Characterizing patient details-related challenges from health information technology-related incident reports from Swedish healthcare. Front Digit Health. (2024) 6. doi: 10.3389/fdgth.2024.1260521
8. Wager KA, Lee FW, Glaser JP. Health Care Information Systems: A Practical Approach for Health Care Management. Chichester, UK:John Wiley & Sons (2021).
9. Jabin MSR, Magrabi F, Hibbert P, Schultz T, Bessen T, Runciman W. Identifying and characterizing system issues of health information technology in medical imaging as a basis for recommendations. 2019 IEEE International Conference on Imaging Systems and Techniques (IST); 2019; Abu Dhabi: IEEE Xplore (2020).
10. Jabin MSR, Magrabi F, Hibbert P, Schultz T, Runciman W. Identifying and classifying incidents related to health information technology in medical imaging as a basis for improvements in practice. 2019 IEEE International Conference on Imaging Systems and Techniques (IST); 2019; Abu Dhabi: IEEE Xplore (2020).
11. Jabin MSR, Magrabi F, Hibbert P, Schultz T, Runciman W. Identifying clusters and themes from incidents related to health information technology in medical imaging as a basis for improvements in practice. 2019 IEEE International Conference on Imaging Systems and Techniques (IST); 2019; Abu Dhabi: IEEE Xplore (2020).
12. Chapman AK, Lehmann CU, Donohue PK, Aucott SW. Implementation of computerized provider order entry in a neonatal intensive care unit: impact on admission workflow. Int J Med Inform. (2012) 81(5):291–5. doi: 10.1016/j.ijmedinf.2011.12.006
13. Jabin MSR. Identifying and Characterising Problems Arising from Interactions Between Medical Imaging and Health Information Technology as a Basis for Improvements in Practice. Adelaide: University of South Australia (2019). Bibliographic ID: 9916366810901831
14. Jabin MSR, Schultz T, Mandel C, Bessen T, Hibbert P, Wiles L, et al. A mixed-methods systematic review of the effectiveness and experiences of quality improvement interventions in radiology. J Patient Saf. (2020) 18(1):e97–107. doi: 10.1097/PTS.0000000000000709
15. Jabin MSR, Hammar T. Issues with the Swedish e-prescribing system—an analysis of health information technology-related incident reports using an existing classification system. Digital Health. (2022) 8:20552076221131139. doi: 10.1177/20552076221131139
16. Jabin MSR, Mandel C, Schultz T, Hibbert P, Magrabi F, Runciman W. Identifying and characterizing the 18 steps of medical imaging process workflow as a basis for targeting improvements in clinical practice. 2019 IEEE International Conference on Imaging Systems and Techniques (IST); 2019; Abu Dhabi: IEEE Xplore (2020). doi: 10.1109/IST48021.2019.9010117
17. Jabin MSR, Pan D, Nilsson E. Characterizing healthcare incidents in Sweden related to health information technology affecting care management of multiple patients. Health Inform J. (2022) 28(2):14604582221105440. doi: 10.1177/14604582221105440
18. Serhani MA, El Kassabi TH, Ismail H, Nujum Navaz A. ECG Monitoring systems: review, architecture, processes, and key challenges. Sensors. (2020) 20(6):1796. doi: 10.3390/s20061796
19. Malasinghe LP, Ramzan N, Dahal K. Remote patient monitoring: a comprehensive study. J Ambient Intell Humaniz Comput. (2019) 10(1):57–76. doi: 10.1007/s12652-017-0598-x
20. Obogo J. Security and privacy challenges in healthcare iot devices for patient treatment and monitoring. (2020).
21. Kadhim KT, Alsahlany AM, Wadi SM, Kadhum HT. An overview of patient’s health Status monitoring system based on internet of things (IoT). Wireless Personal Commun. (2020) 114(3):2235–62. doi: 10.1007/s11277-020-07474-0
22. Bedfordshire Hospitals NHS Charity. Central Monitoring System 2023. Available online at: https://www.bedfordshirehospitals.nhs.uk/charity/support-our-hospitals/emergency-department-appeal/funded-projects/what-is-a-central-monitoring-system-and-why-we-need-your-help/ (accessed December 22, 2023).
23. Fagherazzi G, Goetzinger C, Rashid MA, Aguayo GA, Huiart L. Digital health strategies to fight COVID-19 worldwide: challenges, recommendations, and a call for papers. J Med Internet Res. (2020) 22(6):e19284. doi: 10.2196/19284
24. Runciman WB, Morris RW, Watterson LM, Williamson JA, Paix AD. Crisis management during anaesthesia: cardiac arrest. Qual Saf Health Care. (2005) 14(3):e14. doi: 10.1136/qshc.2002.004473
25. Woodward HI, Mytton OT, Lemer C, Yardley IE, Ellis BM, Rutter PD, et al. What have we learned about interventions to reduce medical errors? Annu Rev Public Health. (2010) 31:479–97. 1 p following 97. doi: 10.1146/annurev.publhealth.012809.103544
26. Magrabi F, Baker M, Sinha I, Ong MS, Harrison S, Kidd MR, et al. Clinical safety of England’s national programme for IT: a retrospective analysis of all reported safety events 2005 to 2011. Int J Med Inform. (2015) 84(3):198–206. doi: 10.1016/j.ijmedinf.2014.12.003
27. National Board of Health and Welfare (Sweden). Prerequisites for reprocessing and reusing disposable medical devices in Sweden. (2020).
28. Danko C. Traceability of medical devices used during surgeries (thesis). Stockholm: The Royal Institute of Technology (2020).
29. Dissanayake N, Zahedi M, Jayatilaka A, Babar MA. A grounded theory of the role of coordination in software security patch management. Proceedings of the 29th ACM Joint Meeting on European Software Engineering Conference and Symposium on the Foundations of Software Engineering; Athens, Greece: Association for Computing Machinery (2021). p. 793–805
30. Parasuraman R, Mouloua M, Hillsdale NJ. Automation and Human Performance: Theory and Applications. England: Lawrence Erlbaum Associates (1996).
31. Jabin MSR, Pan D. Software-related challenges in Swedish healthcare through the lens of incident reports: a desktop study. digital health. (2023) 9:20552076231203600. doi: 10.1177/20552076231203600
32. Jabin MSR, Steen M, Wepa D, Bergman P. Assessing the healthcare quality issues for digital incident reporting in Sweden: incident reports analysis. Digital Health. (2023) 9:20552076231174307. doi: 10.1177/20552076231174307
33. Schultz TJ, Hannaford N, Mandel C. Patient safety problems from healthcare information technology in medical imaging. BJR Case Rep. (2015) 2(2):20150107. doi: 10.1259/bjrcr.20150107
34. Dissanayake N, Jayatilaka A, Zahedi M, Babar MA. Software security patch management -- a systematic literature review of challenges, approaches, tools and practices. arXiv (2020). [Preprint]. doi: 10.48550/arXiv.2012.00544
35. Weil T, Murugesan S. IT risk and resilience—cybersecurity response to COVID-19. IT Prof. (2020) 22(3):4–10. doi: 10.1109/MITP.2020.2988330
36. Sittig DF, Gonzalez D, Singh H. Contingency planning for electronic health record-based care continuity: a survey of recommended practices. Int J Med Inf. (2014) 83(11):797–804. doi: 10.1016/j.ijmedinf.2014.07.007
Keywords: patient safety, healthcare quality improvement, software issue, training, system integration, system design, software update, workflow disruption
Citation: Jabin MSR (2024) Operational disruption in healthcare associated with software functionality issue due to software security patching: a case report. Front. Digit. Health 6:1367431. doi: 10.3389/fdgth.2024.1367431
Received: 8 January 2024; Accepted: 23 February 2024;
Published: 14 March 2024.
Edited by:
Suleman Atique, Norwegian University of Life Sciences, NorwayReviewed by:
Mohan Kumar Gajendran, University of Missouri–Kansas City, United States© 2024 Jabin. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Md Shafiqur Rahman Jabin bWRzaGFmaXF1ci5yYWhtYW5qYWJpbkBsbnUuc2U=; bWphYmluQGJyYWRmb3JkLmFjLnVr
†ORCID Md Shafiqur Rahman Jabin orcid.org/0000-0003-0197-8716
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.