 Awole Seid
Awole Seid Desta Dugassa Fufa
Desta Dugassa Fufa Zebenay Workneh Bitew
Zebenay Workneh Bitew- 1Department of Adult Health Nursing, College of Medicine and Health Sciences, Bahir Dar University, Bahir Dar, Ethiopia
- 2Center for Food Science and Nutrition, Addis Ababa University, Addis Ababa, Ethiopia
- 3Haramaya Institute of Technology, Haramaya University, Dire Dawa, Ethiopia
- 4Saint Paul’s Hospital Millennium Medical College, Addis Ababa, Ethiopia
Introduction: Digital tools, such as mobile apps and the Internet, are being increasingly used to promote healthy eating habits. However, there has been inconsistent reporting on the effectiveness of smartphones and web-based apps in influencing dietary behaviors. Moreover, previous reviews have been limited in scope, either by focusing on a specific population group or by being outdated. Therefore, the purpose of this review is to investigate the impacts of smartphone- and web-based dietary interventions on promoting healthy eating behaviors worldwide.
Methods: A systematic literature search of randomized controlled trials was conducted using databases such as Google Scholar, PubMed, Global Health, Informit, Web of Science, and CINAHL (EBSCO). The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were followed to prepare the entire document. EndNote (version 20) was used for reference management. The risk of bias in the articles was assessed using the “Revised Cochrane Risk of Bias tool for randomized trials (RoB 2.0)” by the Cochrane Collaboration. Narrative synthesis, using text and tables, was used to present the results. The study was registered in PROSPERO under protocol number CRD42023464315.
Results: This review analyzed a total of 39 articles, which consisted of 25 smartphone-based apps and 14 web-based apps. The studies involved a total of 14,966 participants. Out of the 25 studies, 13 (52%) showed that offline-capable smartphone apps are successful in promoting healthier eating habits. The impact of smartphone apps on healthy adults has been inconsistently reported. However, studies have shown their effectiveness in chronically ill patients. Likewise, internet-based mobile apps, such as social media or nutrition-specific apps, have been found to effectively promote healthy eating behaviors. These findings were consistent across 14 studies, which included healthy adults, overweight or obese adults, chronically ill patients, and pregnant mothers.
Conclusion: Overall, the findings suggest that smartphone apps contribute to improving healthy eating behaviors. Both nutrition-specific and social media-based mobile apps consistently prove effective in promoting long-term healthy eating habits. Therefore, policymakers in the food system should consider harnessing the potential of internet-based mobile apps and social media platforms to foster sustainable healthy eating behaviors.
Introduction
The concept of digital access goes beyond simply having physical access to the Internet. It also includes the ability to search, evaluate, organize, and perform tasks using digital devices in various aspects of life, such as learning, work, and social interactions. The United Nations, through its Sustainable Development Goals (SDG 9), aims to improve digital literacy by setting targets to achieve universal and affordable internet access by 2030 (1, 2). Although more than 80% of people in developed countries use the Internet, 32% of Europeans lack basic digital skills (3–5). This indicates a significant gap in digital literacy within developed nations, and the adoption of digital technology is influenced by factors such as age, residence, socioeconomic status, education level, and others (6).
Digital technologies, like mobile health apps (mHealth), can be used for public health dietary education, promotion, and empowering individuals to take care of themselves (7). It has been indicated that advocating for people-centered health systems enabled by digital health is a strategic objective of WHO's global strategy on digital health 2020–2025 (8). Hence, to achieve this strategic objective, it is imperative to improve digital health literacy at the population level. This entails addressing attitudes, practices, and public awareness of digital health (8).
Unhealthy eating increases the risk of chronic diseases. However, many current strategies for promoting healthy eating are not sustainable in the long term (9). As a result, mobile apps are being used more frequently to deliver behavioral health interventions. These digital platforms can help people improve their food behavior over a longer period of time (10, 11). According to studies, digital tools such as mobile apps, the internet, and video games can promote healthy eating (12–14). Digital health technology is also receiving policy investment due to its ability to deliver healthcare to more people in a cost-effective manner.
One study indicated that the increase in lifestyle diseases, which are often linked to poor consumer food behavior, necessitates the need for accessible and efficient digital solutions (15). Although digital technologies (DTs) have been used to raise awareness and encourage the consumption of healthy foods, their effectiveness has not been consistently documented (16, 17). Furthermore, upon closer appraisal of previous reviews reveals certain limitations. These limitations include a limited number of included studies (18), studies conducted on a single population group (19–23), examination of different types of DTs together (24), the inclusion of articles conducted in a single country (25), the use of DT assessment to measure dietary intake instead of intervention (26), exclusion of recently published articles (9, 27, 28), and lack of assessment of specific interventional strategies, such as an artificial intelligence chatbot (29). It is important to note that the use of digital technology, especially smartphone apps, is still in an exploratory phase (30). Therefore, a comprehensive systematic review is needed to address a diverse population, cover various study periods, and include rigorous quality assessment. Lastly, this review aims to offer robust recommendations for practice, policy, and future research.
Review question
• What is the effect of smartphone apps and web-based dietary interventions on healthy eating behaviors?
The scope of the study and eligibility criteria were defined using the Population, Intervention, Comparison, Outcomes, and Study (PICOS) framework as follows, before conducting the article search (31).
• Population (P): Healthy adults, overweight adults, obese adults, children, adolescents, chronically ill patients, pregnant women, and breastfeeding mothers. Studies from all countries, regardless of their income level and development, were included.
• Intervention (I): Smartphone app-based dietary education, whether nutrition-specific or through social media, includes counseling for improving dietary adherence, maternal diet counseling, guidance on exclusive breastfeeding and complementary feeding, promoting the consumption of fortified foods and a diverse diet, counseling on healthy and sick child feeding, and any other intervention aimed at improving healthy dietary practices in the general public.
• Comparison (C): No digital technologies, as well as similar dietary interventions delivered through other digital technologies such as web-based platforms, phone calls, and text messages.
• Outcome (O): Healthy eating behaviors/practices:
- Increase consumption of fruits, vegetables, legumes (such as lentils and beans), nuts, and whole grains (such as unprocessed maize, millet, oats, wheat, and brown rice).
- Avoid or limit table sugar to less than 5% of total energy intake.
- Decrease salt intake to less than 5 g per day.
- Practice exclusive breastfeeding for the first 6 months of life.
- Introduce complementary feeding.
- Breastfeed optimally up to 2 years of age.
- Reduce saturated fats to less than 10% of total energy intake.
- Avoid industrially-produced trans-fats.
- Follow special diets like DASH and Mediterranean diet.
- Read nutrition labels.
- Prevent food contamination.
- Make mindful food choices.
- Make informed food purchases.
- Consume fortified foods, including the use of multiple micronutrient powders at home.
• Time: No time restriction.
• Language: Articles with abstracts written in English were included for articles retrieved from PubMed, while articles from other data sources were searched without language restrictions.
• Types of included studies: Randomized controlled trials (RCTs) that reported relevant outcomes of interest were included. However, systematic reviews and meta-analyses, observational studies, unpublished studies such as theses and dissertations, editorial comments, non-human studies, conference proceedings, case reports, case series, and duplicate publications using similar data were excluded from the current study.
Materials and methods
Data sources and search strategies
This document has been prepared based on the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines (32). In this study, articles published up to June 2022 were included. To retrieve articles, reputable database sources were explored independently by three authors. The following databases were explored comprehensively: PubMed (including Medline), Scopus, Web of Sciences, Embase, Global Health, Cumulative Index to Nursing and Allied Health Literature (CINAHL) (EBSCO), WHO's Institutional Repository for Information Sharing (IRIS), Informit Health Collection, Food Science and Technology Abstracts (FSTA) (EBSCO), and references of previously published reviews (snowball technique). Advanced searching was employed during the search process for those databases. The retrieved articles were exported to EndNote version 20 software, so the removal of duplicates and citations was performed using this software. Key terms were verified for appropriateness before the actual search. For instance, the following search strings were employed to search articles from PubMed (Table 1).

Table 1. Search terms used to access published studies in the pubMed database, 2022.
Data extraction procedure
The articles in this systematic review were assessed and selected by the three authors (ZWB, AS, and DD). The data extraction sheet was created using Microsoft Excel. The sheet includes authors' names, publication years, research titles, study settings and designs, study populations, sample sizes, types of smartphone apps, types of dietary interventions, assessment methods for outcome variables, duration of interventions or follow-ups, methods of intervention, main findings, and limitations. Any discrepancies during the extraction process were resolved through discussion among the authors.
Quality assessment of studies
In this study, the Cochrane Risk of Bias Assessment Tool Version 2 (RoB 2) was used to evaluate the quality of articles. The tool consists of components such as yes (Y), probably yes (PY), no (N), probably no (PN), and no information (NI). Bias can arise from various factors, including the randomization process, deviations from intended interventions, missing outcome data, measurement bias of the outcome, and selection bias in reporting results. The overall risk of bias is determined by three components: low risk, high risk, and some concerns. If all five components or domains are assessed as low risk, the overall risk of bias is classified as “low risk.” If one of the components has some concerns, the overall risk of bias is categorized as “some concerns.” On the other hand, if any of the five components are assessed as high risk or if any of the two domains have some concerns, the overall risk of bias is classified as “high risk” (33). The qualitative presentation of the overall risk of bias is represented by a visual graph with green, yellow, and red colors, indicating low risk, some concerns, and high risk, respectively.
Data synthesis
The results of the study are presented through text and tables. Since the effect measures reported in the study are varied, a quantitative summary or meta-analysis was not conducted. Furthermore, the results are summarized based on the following subgroups: type of smartphone apps, study population, type of public health dietary interventions, duration of intervention, and country income classification. To provide a narrative synthesis, vote counting and the direction of the effect were utilized (34). The findings are displayed using summary tables.
Results
Literature search and study selection
The search identified a total of 10,498 electronic records. After removing 10,248 records due to duplication and irrelevancy, 250 titles were screened for potential eligibility. Following the removal of 48 articles that were unrelated and five articles that could not be retrieved, a total of 58 articles remained. Among these, 11 were excluded as they were not randomized controlled trials (32, 35–44), 11 were reviews (18–22, 24, 26, 27, 29, 31, 45), six studies used other types of digital technologies (DTs) (46–51), 19 studies did not align with the review objective (52–70), and 11 studies were study protocols (71–76). Finally, a total of 39 studies were included in the review, of which 25 utilized smartphone apps that could function both online and offline, and the remaining 14 used web-based apps that required an internet connection to function (Figure 1).
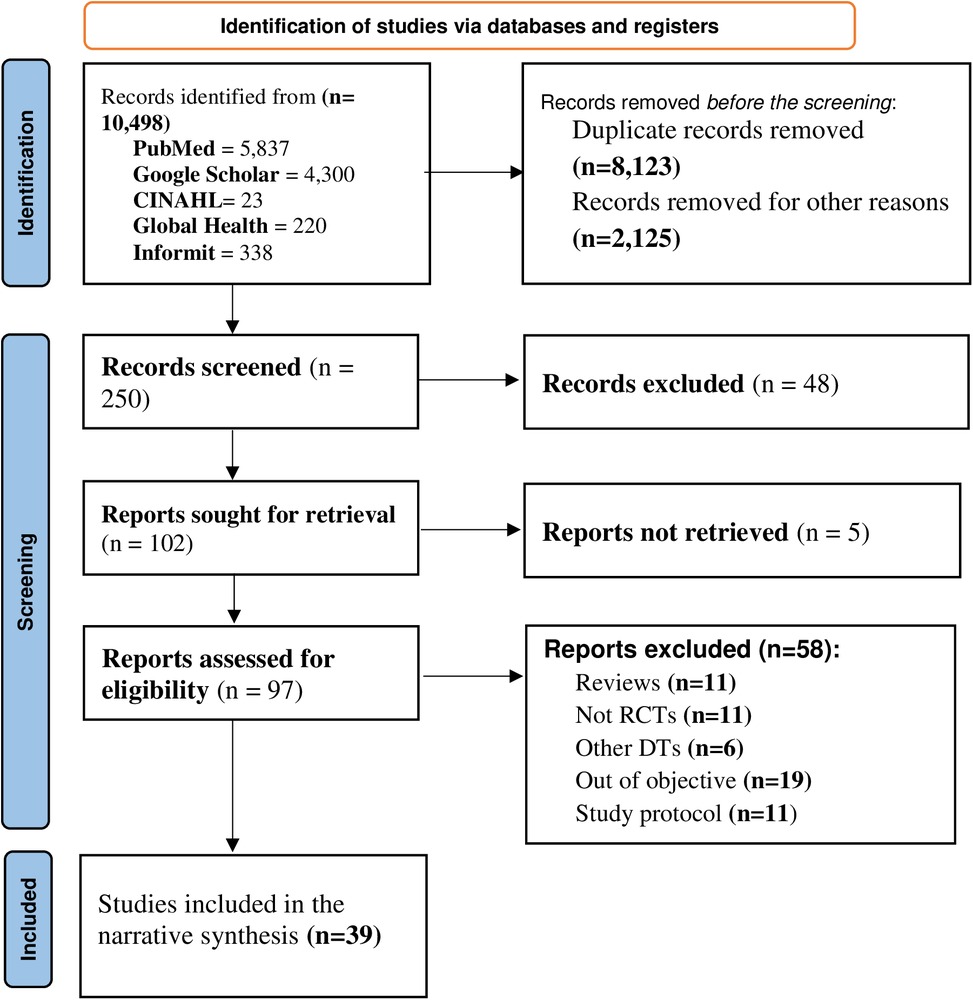
Figure 1. Study selection proces using the PRISMA flowchart, 2022.
Characteristics of the included articles
All 39 articles included in this systematic review were randomized controlled trials. The majority of the studies (31) were reported from high-income countries, while the remaining nine studies were reported from middle-income countries. Similarly, 16 of the studies were reported from European countries, 10 from the USA, and the remaining studies were reported from Asian countries. All of the included studies were published between 2011 and 2022. The sample sizes ranged from 24 to 1,859 participants. Regarding the study population, 12 studies were carried out in healthy adults, seven in overweight/obese adults, nine in chronically ill patients, six in pregnant mothers, and five in children. In addition, the duration of the intervention ranges from 10 days to 24 months. Regarding the type of interventions, 20 studies focused on comprehensive dietary interventions, nine studies targeted fruit and vegetable consumption, five studies focused on limiting salt or sodium intake, three studies focused on adherence to the Dietary Approaches to Stop Hypertension (DASH) and Mediterranean diets, two studies focused on promoting exclusive breastfeeding, and one study examined consumers' food choices.
Risk of bias of included studies
After the quality of studies was evaluated using Cochrane RoB 2, nine studies were identified as low-risk, 18 studies had some concerns, and 12 studies had a high risk of bias. This shows that the results should be interpreted cautiously (Figure 2).
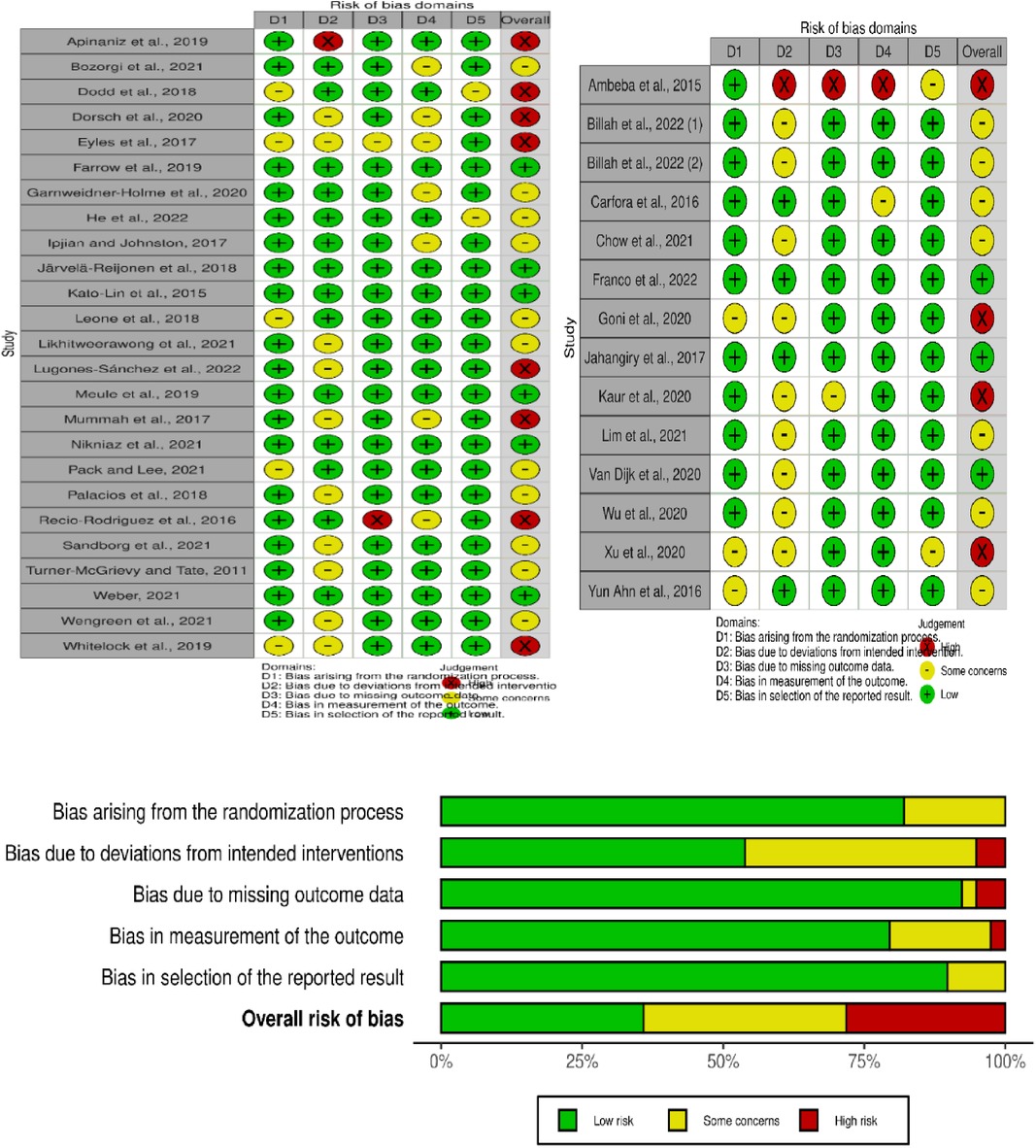
Figure 2. The overall risk of bias of included studies assessed with the cochrane risk of bias tool, 2022.
Effectiveness of interventions
The data is categorized into smartphone apps and web applications for better understanding. Smartphone apps are designed for mobile devices like smartphones and tablets. They can be accessed without an internet connection once installed. On the other hand, web apps are designed to run on web browsers across different devices, including desktops, laptops, and mobile devices. Web apps require an internet connection to access since they are hosted on remote servers and accessed through web browsers.
The effect of smartphone app-based interventions on healthy eating habits
Out of the 25 studies, 13 (52%) found that mobile apps encouraged healthier eating habits. The remaining 12 (48%) had mixed or no significant results. Smartphone app-based interventions were effective in promoting healthier eating habits among patients with chronic diseases. Only four studies involving healthy adults, two studies on children, and one study on pregnant women showed a significant change in eating behavior through smartphone apps.
The use of mobile apps to reduce sodium intake has been studied in various populations. Several studies, including Dorsch et al. (77), Eyles et al. (78), Hele et al. (74), He, et al. (79), Ipjian and Johnston (80) evaluated the effects of mobile apps such as LowSalt4Life, SaltSwitch, and MyFitnessPal on salt intake among different groups, including hypertensive patients, cardiovascular patients, schoolchildren and families, and healthy adults. These studies followed participants for periods ranging from 4 weeks to 12 months and found a significant reduction in dietary sodium intake as well as household purchases of salt. Moreover, the findings indicated that mobile apps were effective in providing salt restriction advice, even in restaurant and beverage settings.
Mobile apps have been shown to benefit adherence to the DASH diet and increase dietary self-efficacy among patients with hypertension and chronic kidney disease. A study conducted by Bozorgi et al. on 120 hypertensive patients over 8 weeks demonstrated that the use of smartphone apps improved adherence to the DASH and low-fat diets (81). In a study by Pack and Lee with 75 patients undergoing hemodialysis, a 30-minute face-to-face and online counseling program significantly increased the dietary self-efficacy of the patients (82).
The impact of smartphone apps on the eating behaviors of both healthy and overweight adults has been inconsistent. For example, Järvelä-Reijonen et al. conducted a study involving 219 overweight adults, which showed that a mobile app-based intervention delivered in a group session had a beneficial effect on improving dietary behavior (69). Similarly, Mummah et al. found that the use of a mobile app called “Vegatone” led to an improvement in daily vegetable consumption among overweight adults (83). In contrast to the previous results, several studies conducted on both healthy and overweight adults, with different sample sizes and study settings, did not find a significant impact on eating behavior. For example, a study by Kato Lin et al. involving 425 healthy adults in the USA found no improvement in users' engagement in tracking dietary patterns (84). Similarly, in Spain, a study conducted by Recio-Rodriguez et al. with 833 healthy adults showed no difference in adherence to the Mediterranean diet in the intervention groups (85). Likewise, a study by Meule et al. indicated that a smartphone-based approach did not affect the eating behaviors of adolescents (86). Further studies are needed to determine the cause of these disparate results.
Game-based mobile apps have been shown to significantly improve children's eating behaviors. A 3-month follow-up study by Wengreen et al. involved 1,859 children. The study found that presenting the smartphone app (FIT Game) as daily comic-book-formatted episodes, projected onto a large screen in the school cafeteria during lunchtime, led to an increase in the consumption of fruits and vegetables (87). Another study conducted by Farrow et al. involved 74 children between the ages of 3 and 6. The study revealed that playing a game-based mobile app called “Vegetable Maths Masters” led to an increase in both the preference for and consumption of vegetables (88) (Table 2).
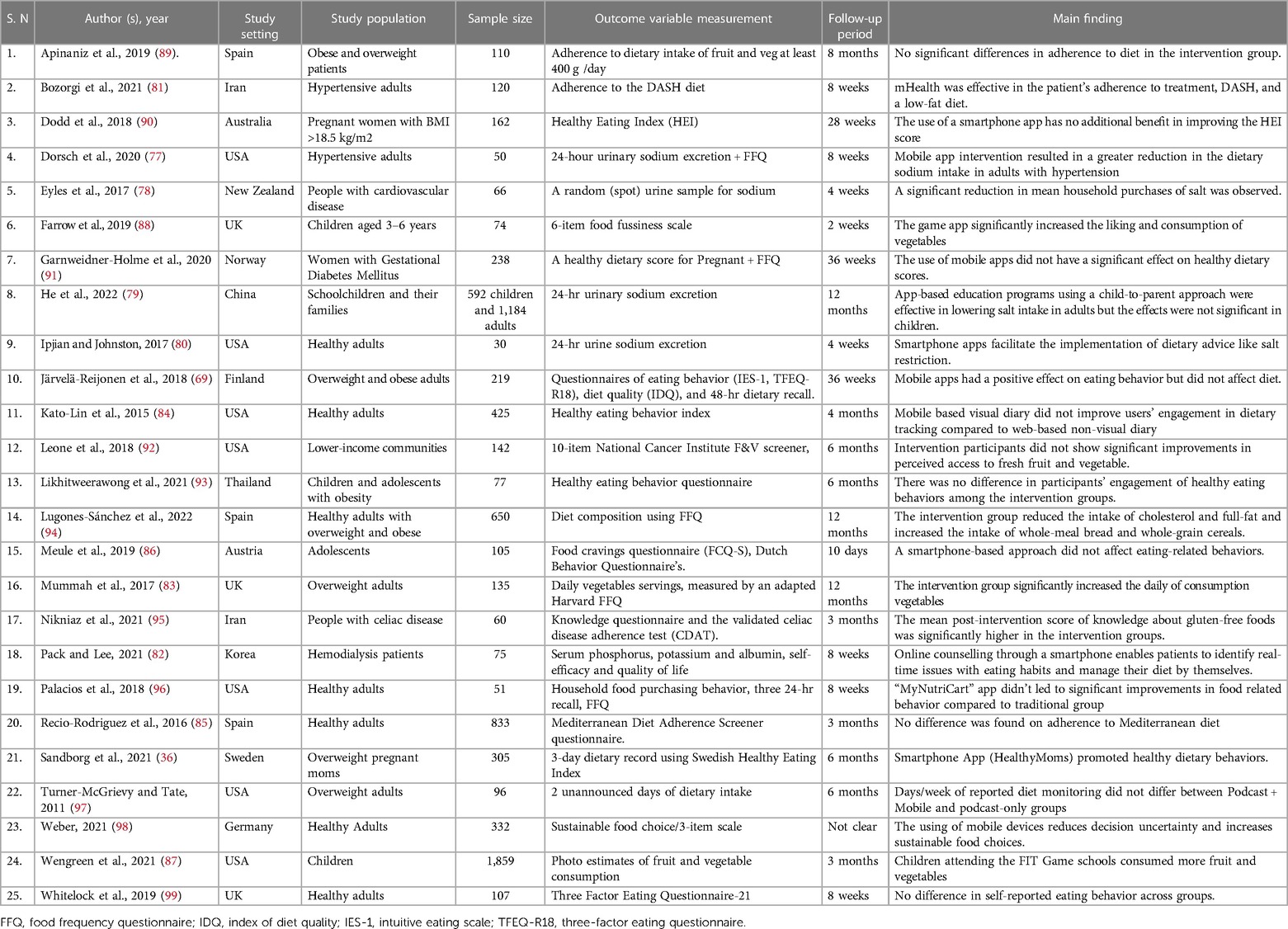
Table 2. Summary of randomized controlled studies on the effect of smartphone App-based interventions on healthy eating behaviors, 2022.
The effect of web-based mobile app interventions on healthy eating behavior
Out of the 34 studies included in the final narrative synthesis, 16 focused on the effects of web-based mobile applications on healthy eating behavior. These studies assessed behaviors such as reducing sugar and fat intake, increasing fruit and vegetable consumption, decreasing salt intake, and adherence to the Mediterranean diet. It was found that using social media or internet-connected nutrition apps, which allow users to share thoughts and receive personalized expert advice, encouraged the adoption of healthier eating habits.
Web-based smartphone apps promote healthy eating behaviors in individuals with chronic diseases. For example, apps like Healthwatch 360 and DHealth Bar (a WeChat applet) improve the eating behavior of cancer and diabetic patients. In cardiac patients, it increases adherence to the Mediterranean diet (100–103).
Internet-based mobile apps have had a significant impact on promoting desired feeding practices in pregnant women and children. For example, a study by Billah et al. involving 1,500 participants showed a 16% increase in exclusive breastfeeding and improved dietary diversity scores among children in the intervention group (104). Another study by Van Dijk et al. focused on pregnant women and found that smartphone-based interventions increased the consumption of fruits and vegetables while reducing the intake of unhealthy snacks (105).
Online mobile apps have had a positive impact on the eating habits of both healthy adolescents and adults. One study conducted in Italy, for instance, demonstrated that a two-week intervention utilizing text messages resulted in improved fruit and vegetable consumption among 623 participating adolescents (106). Moreover, Kaur et al. and Lim et al. conducted interventional studies on healthy and overweight adults, which demonstrated that SMART-eating effectively reduced fat, sugar, and salt intake while increasing fruit and vegetable consumption (105, 107) (Table 3).

Table 3. Summary of randomized controlled studies on the effect of internet-based mobile apps interventions on healthy eating behaviors, 2022.
Discussion
The widespread availability and affordability of smartphones, along with the influence of social media, have harnessed the extensive capabilities of technology to assist individuals in improving their healthy eating habits. This study sought to evaluate the effectiveness of smartphone app-based interventions in promoting healthy dietary behaviors among diverse populations and in different countries. The findings of this study indicate that the use of smartphone and web apps has a significant impact on enhancing healthy eating behaviors. However, it is worth noting that in certain studies, changes in dietary behaviors were only maintained for a short duration.
This study included 39 interventional studies that used smartphone and web-based apps to provide information to diverse populations. The study involved healthy adults, overweight or obese adults, chronically ill patients, pregnant mothers, and children of different age groups.
Among the 14-smartphone app-based studies conducted on healthy adults (with the offline capability), the majority (10) did not show a positive impact on modifying healthy eating behaviors. However, all four studies involving patients with chronic diseases indicated that the use of smartphone apps improved adherence to healthy dietary behaviors. Additionally, the findings regarding pregnant women and children showed mixed results. The hesitance of healthy adults to use smartphone apps can be attributed to the health belief model, which emphasizes the significance of factors such as perceived susceptibility, perceived severity, and perceived benefits in promoting healthy behavioral changes (114). This suggests that policy engagement is still necessary to promote the adoption of health maintenance behaviors among healthy adults. In contrast, using smartphone apps to convey dietary messages had a significant positive impact on the eating behavior of patients with chronic diseases. Altering one's eating habits is crucial for effectively managing chronic diseases. Patients are well aware of the negative consequences that can arise from making irresponsible food choices. Moreover, smartphone apps designed to help reduce salt or sodium consumption can serve as a platform to achieve the WHO's goal of reducing the global population's sodium intake by 30% by 2025 (115). The finding regarding the role of smartphone app-based interventions in healthy adults aligns with previous systematic reviews (12, 29). However, this finding contradicted a review of trials involving overweight adults. The review found that the use of smartphone apps improved adherence to diets that included lower-calorie, low-fat, and high-fiber foods (116). The discrepancy may be attributed to variations in the scope of the reviews, eligibility criteria for study selection, and the number of studies included in the review, all of which can impact the conclusions drawn. The effects of smartphone app-based dietary interventions on both healthy and overweight adults were inconsistent in the studies included. It is worth noting that these inconsistencies were not due to variations in sample size, intervention duration, or study settings. These findings underscore the significance of carefully identifying the target consumers when designing smartphone app-based interventions. The main finding from all 14 studies was that web-based mobile apps effectively encouraged the development of healthy eating habits in various groups of people, such as healthy adults, overweight or obese adults, pregnant women, and individuals with chronic diseases. The positive outcome can be attributed to intervention methods that involved receiving regular messages and feedback from professionals. Additionally, the use of educational videos was effective in conveying information. These strategies successfully engaged participants and facilitated changes in their healthy eating behaviors. Visual content, such as images and videos, is highly appealing to consumers, particularly in the current age of social media platforms like TikTok. As consumers have limited time and patience for reading lengthy texts, they prefer information that engages multiple senses and is presented in a concise format (117). A meta-analysis study also indicated that using pictorial health information significantly increases knowledge and understanding, especially for populations with lower health literacy. Furthermore, the use of icons with minimal accompanying words is found to be highly effective in conveying health information (118). Furthermore, our study emphasized the importance of not just the presentation format of the message but also the consistency and professional feedback provided through online platforms as vital elements of web-based dietary interventions. Our findings align with a study that demonstrates the significant positive impact of using web-based apps on weight loss and calorie reduction. Furthermore, the study highlights that tailored interventions are considerably more effective than non-tailored interventions (20). Our results are consistent with a previous review that highlighted the significance of integrating digital-based interventions with personalized feedback and counseling to achieve long-lasting, desired dietary behavior (45). Furthermore, this study aligns with a review that highlights the efficacy of digital technology, particularly apps, in improving stakeholder relationships within the agro-food chain and advancing urban and regional food systems (119). The result can be better elucidated by considering the concepts of social and behavioral change communication (SBCC) and health belief models (HBM). According to these models, individuals require repetitive communication through channels that are suitable and preferred within their community to effectively promote desired changes in behavior (120). Meanwhile, the results of our study have global implications for improving countries' efforts to expand internet infrastructure, making smartphones more affordable, and promoting digital literacy. These combined efforts will enhance the effectiveness of public-health dietary interventions.
The strength of this study lies in its inclusion of only randomized controlled trials and the assessment of article quality using the Cochrane risk-of-bias tool. This enhances the credibility of the results. However, this review has some limitations. The extensive scope of this study, which includes a wide range of study populations and dietary interventions, hinders the ability to carry out a meta-analysis. Furthermore, the lack of studies conducted in low-income countries, the disparities in digital access both within and between affluent countries, and the increasing prices of healthy food could impact the generalizability of the findings.
Conclusion
In general, the use of smartphone apps (offline or web-based) has led to positive changes in healthy eating habits among different populations and individuals with varying health conditions. Both platforms of smartphone apps contribute to promoting healthy dietary behaviors among patients with chronic diseases. Similarly, the impact of tailored messages, along with professional feedback through web-based app platforms, on promoting public health dietary interventions has been significant. However, there is no consistent reporting on the effectiveness of non-internet-based smartphone apps on the dietary behavior of healthy adults.
Recommendation
The use of mobile apps, including social media, to deliver public health dietary interventions should be a top policy priority. Furthermore, it is important to identify target consumers before developing digital technologies, as their effectiveness can vary among different populations. Continued efforts are needed to improve smartphone and internet accessibility for a wider range of population groups. It is recommended to conduct more large-scale randomized controlled trials (RCTs) in low- and middle-income countries to gather more comprehensive evidence. Meta-analysis studies that examine specific dietary interventions in single population groups are also recommended. Further studies that specifically target healthy adults and adolescents are necessary.
Author contributions
AS: Conceptualization, Data curation, Formal Analysis, Writing – original draft, Writing – review & editing. DF: Conceptualization, Data curation, Formal Analysis, Writing – original draft, Writing – review & editing. ZB: Conceptualization, Data curation, Formal Analysis, Writing – original draft, Writing – review & editing.
Funding
This systematic review was funded by the World Health Organization (WHO) with grant number 202884789.
Acknowledgments
We are grateful to WHO and Nutrition International for sponsoring and technical support of this project.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. GGI. Digital Access: Bridging the Digital Divide for Inclusive Connectivity. 2023. Available at: https://www.graygroupintl.com/blog/digital-access (Accessed December 20, 2023).
2. Taskin B, Ok C. Impact of digital literacy and problematic smartphone use on life satisfaction: comparing Pre- and post-COVID-19 pandemic. Eur J Investig Health Psychol Educ. (2022) 12:1311–22. doi: 10.3390/ejihpe12090091
3. van Kessel R, Wong BLH, Rubinić I, O’Nuallain E, Czabanowska K. Is Europe prepared to go digital? Making the case for developing digital capacity: an exploratory analysis of eurostat survey data. PLOS Digit Health. (2022) 1:e0000013. doi: 10.1371/journal.pdig.0000013
5. Blazhevska V. Sustainable Development Goal 9: Investing in ICT access and quality education to promote lasting peace. United Nations Sustainable Development. 2017. Available at: https://www.un.org/sustainabledevelopment/blog/2017/06/sustainable-development-goal-9-investing-in-ict-access-and-quality-education-to-promote-lasting-peace/ (Accessed December 21, 2023).
6. Lee H, Lim J-A, Nam H-K. Effect of a digital literacy program on older adults’ digital social behavior: a quasi-experimental study. Int J Environ Res Public Health. (2022) 19(12404):12404. doi: 10.3390/ijerph191912404
7. Alain L, Smisha A, Tigest T, Garrett M. WHO Digital health guidelines: a milestone for global health. NPJ Digit Med. (2020) 3:120. doi: 10.1038/s41746-020-00330-2
9. McCarroll R, Eyles H, Ni Mhurchu C. Effectiveness of mobile health (mHealth) interventions for promoting healthy eating in adults: a systematic review. Prev Med. (2017) 105:156–68. doi: 10.1016/j.ypmed.2017.08.022
10. Lucassen DA, Lasschuijt MP, Camps G, Van Loo EJ, Fischer AR, de Vries RA, et al. Short and long-term innovations on dietary behavior assessment and coaching: present efforts and vision of the pride and prejudice consortium. Int J Environ Res Public Health. (2021) 18:7877. doi: 10.3390/ijerph18157877
11. McGloin AF, Eslami S. Digital and social media opportunities for dietary behavior change. Proc Nutr Soc. (2015) 74:139–48. doi: 10.1017/S0029665114001505
12. Paramastri R, Pratama SA, Ho DKN, Purnamasari SD, Mohammed AZ, Galvin CJ, et al. Use of mobile applications to improve nutrition behavior: a systematic review. Comput Methods Programs Biomed. (2020) 192:105459. doi: 10.1016/j.cmpb.2020.105459
13. Watanabe-Ito M, Kishi E, Shimizu Y. Promoting healthy eating habits for college students through creating dietary diaries via a smartphone app and social media interaction: online survey study. JMIR MHealth UHealth. (2020) 8:e17613. doi: 10.2196/17613
14. Samoggia A, Riedel B. Assessment of nutrition-focused mobile apps’ influence on consumers’ healthy food behavior and nutrition knowledge. Food Res Int. (2020) 128:108766. doi: 10.1016/j.foodres.2019.108766
15. Rich E, Miah A. Understanding digital health as public pedagogy: a critical framework. Societies. (2014) 4:296–315. doi: 10.3390/soc4020296
16. Milne-Ives M, Lam C, De Cock C, Van Velthoven MH, Meinert E. Mobile apps for health behavior change in physical activity, diet, drug and alcohol use, and mental health: systematic review. JMIR MHealth UHealth. (2020) 8:e17046. doi: 10.2196/17046
17. Kankanhalli A, Shin J, Oh H. Mobile-based interventions for dietary behavior change and health outcomes: scoping review. JMIR MHealth UHealth. (2019) 7:e11312. doi: 10.2196/11312
18. Villinger K, Wahl DR, Boeing H, Schupp HT, Renner B. The effectiveness of app-based mobile interventions on nutrition behaviors and nutrition-related health outcomes: a systematic review and meta-analysis. Obes Rev. (2019) 20:1465–84. doi: 10.1111/obr.12903
19. Mieso B, Neudecker M, Furman L. Mobile phone applications to support breastfeeding among African-American women: a scoping review. J Racial Ethn Health Disparities. (2022) 9:1–20. doi: 10.1007/s40615-020-00927-z
20. Berry R, Kassavou A, Sutton S. Does self-monitoring diet and physical activity behaviors using digital technology support adults with obesity or overweight to lose weight? A systematic literature review with meta-analysis. Obes Rev. (2021) 22:e13306. doi: 10.1111/obr.13306
21. Duan Y, Shang B, Liang W, Du G, Yang M, Rhodes RE. Effects of eHealth-based multiple health behavior change interventions on physical activity, healthy diet, and weight in people with noncommunicable diseases: systematic review and meta-analysis. J Med Internet Res. (2021) 23:e23786. doi: 10.2196/23786
22. Akinosun AS, Polson R, Diaz-Skeete Y, De Kock J, Carragher L, Leslie S. Digital technology interventions for risk factor modification in patients with cardiovascular disease: a systematic literature review and meta-analysis. Prepr JMIR MHealth UHealth Internet. 2020.
23. Salas-Groves E, Galyean S, Alcorn M, Childress A. Behavior change effectiveness using nutrition apps in people with chronic diseases: scoping review. JMIR MHealth UHealth. (2023) 11:e41235. doi: 10.2196/41235
24. Robinson A, Husband AK, Slight RD, Slight SP. Digital technology to support lifestyle and health behavior changes in surgical patients: systematic review. BJS Open. (2021) 5:zraa009. doi: 10.1093/bjsopen/zraa009
25. Yang X, Kovarik CL. A systematic review of mobile health interventions in China: identifying gaps in care. J Telemed Telecare. (2021) 27:3–22. doi: 10.1177/1357633X19856746
26. Porter J, Huggins CE, Truby H, Collins J. The effect of using mobile technology-based methods that record food or nutrient intake on diabetes control and nutrition outcomes: a systematic review. Nutrients. (2016) 8:815. doi: 10.3390/nu8120815
27. Han M, Lee E. Effectiveness of mobile health application used to improve health behavior changes: a systematic review of randomized controlled trials. Healthc Inform Res. (2018) 24:207–26. doi: 10.4258/hir.2018.24.3.207
28. Schoeppe S, Alley S, Van Lippevelde W, Bray NA, Williams SL, Duncan MJ, et al. Efficacy of interventions that use apps to improve diet, physical activity, and sedentary behavior: a systematic review. Int J Behav Nutr Phys Act. (2016) 13:127. doi: 10.1186/s12966-016-0454-y
29. Oh YJ, Zhang J, Fang M-L, Fukuoka Y. A systematic review of artificial intelligence chatbots for promoting physical activity, healthy diet, and weight loss. Int J Behav Nutr Phys Act. (2021) 18:160. doi: 10.1186/s12966-021-01224-6
30. Hedin B, Katzeff C, Eriksson E, Pargman D. A systematic review of digital behavior change interventions for more sustainable food consumption. Sustainability. (2019) 11:2638. doi: 10.3390/su11092638
31. Amir-Behghadami M, Janati A. Population, intervention, comparison, outcomes and study (PICOS) design as a framework to formulate eligibility criteria in systematic reviews. Emerg Med J. (2020) 37:387–00. doi: 10.1136/emermed-2020-209567
32. Nakamura M, Shirai Y, Sakuma M. Dietary changes during the COVID-19 pandemic: a longitudinal study using objective sequential diet records from an electronic purchase system in a workplace cafeteria in Japan. Nutrients. (2021) 13:1606. doi: 10.3390/nu13051606
33. Eldridge S, Campbell M, Campbell M, Dahota A, Giraudeau B, Higgins J, et al. Revised cochrane risk of bias tool for randomized trials (RoB 2.0): additional considerations for cluster-randomized trials. Cochrane Methods Cochrane Database Syst Rev. (2016) 10.
34. Boon MH, Thomson H. The effect direction plot revisited: application of the 2019 cochrane handbook guidance on alternative synthesis methods. Res Synth Methods. (2021) 12:29–33. doi: 10.1002/jrsm.1458
35. Caon M, Prinelli F, Angelini L, Carrino S, Mugellini E, Orte S, et al. PEGASO e-diary: user engagement and dietary behavior change of a mobile food record for adolescents. Front Nutr. (2022) 9:727480. doi: 10.3389/fnut.2022.727480
36. Sandborg J, Söderström E, Henriksson P, Bendtsen M, Henström M, Leppänen MH, et al. Effectiveness of a smartphone app to promote healthy weight gain, diet, and physical activity during pregnancy (HealthyMoms): randomized controlled trial. JMIR MHealth UHealth. (2021) 9:e26091. doi: 10.2196/26091
37. Pagoto S, Tulu B, Waring ME, Goetz J, Bibeau J, Divito J, et al. Slip buddy app for weight management: a randomized feasibility trial of a dietary lapse tracking app. JMIR MHealth UHealth. (2021) 9:e24249. doi: 10.2196/24249
38. Doub AE, Levin A, Heath CE, LeVangie K. Mobile appetite: consumer attitudes towards and use of mobile technology in the context of eating behavior. J Direct Data Digit Mark Pract. (2015) 17:114–29. doi: 10.1057/dddmp.2015.44
39. Appleton K, Passmore D, Burn I, Pidgeon H, Nation P, Boobyer CA, et al. An interactive mobile phone application, smart 5-a-day, for increasing knowledge of and adherence to fruit and vegetable recommendations: development and randomized controlled test. JMIR MHealth UHealth. (2019) 7. doi: 10.2196/14380
40. Ifejika NL, Bhadane M, Cai CC, Noser EA, Grotta JC, Savitz SI. Use of a smartphone-based mobile app for weight management in obese minority stroke survivors: a pilot randomized controlled trial with an open blinded endpoint. JMIR MHealth UHealth. (2020) 8:e17816. doi: 10.2196/17816
41. Kakoschke N, Hawker C, Castine B, de Courten B, Verdejo-Garcia A. Smartphone-based cognitive bias modification training improves healthy food choice in obesity: a pilot study. Eur Eat Disord Rev. (2018) 26:526–32. doi: 10.1002/erv.2622
42. Seto E, Hua J, Wu L, Shia V, Eom S, Wang M, et al. Models of individual dietary behavior based on smartphone data: the influence of routine, physical activity, emotion food environment. PLoS One. (2016) 11:04. doi: 10.1371/journal.pone.0153085
43. Skouw S, Suldrup A, Olsen A. A serious game approach to improve food behavior in families—a pilot study. Nutrients. (2020) 12:1415. doi: 10.3390/nu12051415
44. Zang J, Song J, Wang Z, Yao C, Ma J, Huang C, et al. Acceptability and feasibility of smartphone-assisted 24-hour recalls in the Chinese population. Public Health Nutr. (2015) 18:3272–7. doi: 10.1017/S1368980015000907
45. Chen Y, Perez-Cueto FJ, Giboreau A, Mavridis I, Hartwell H. The promotion of eating behavior change through digital interventions. Int J Environ Res Public Health. (2020) 17:7488. doi: 10.3390/ijerph17207488
46. Markert J, Herget S, Petroff D, Gausche R, Grimm A, Kiess W, et al. Telephone-based adiposity prevention for families with overweight children (TAFF-study): one-year outcome of a randomized, controlled trial. Int J Environ Res Public Health. (2014) 11:10327–44. doi: 10.3390/ijerph111010327
47. Chapman CD, Nilsson VC, Thune HÅ, Cedernaes J, Le Grevès M, Hogenkamp PS, et al. Watching TV and food intake: the role of content. PLoS One. (2014) 9:e100602. doi: 10.1371/journal.pone.0100602
48. Norman GJ, Kolodziejczyk JK, Adams MA, Patrick K, Marshall SJ. Fruit and vegetable intake and eating behaviors mediate the effect of a randomized text-message based weight loss program. Prev Med. (2013) 56:3–7. doi: 10.1016/j.ypmed.2012.10.012
49. Kim J-W, Ryu B, Cho S, Heo E, Kim Y, Lee J, et al. Impacts of personal health records and wearables on health outcome and sustainable use: 3-arm-based randomized controlled trial. J Med Internet Res. (2018) 7(1):e12070. doi: 10.2196/preprints.12070
50. Kelders SM, Van Gemert-Pijnen JE, Werkman A, Nijland N, Seydel ER. Effectiveness of a web-based intervention aimed at healthy dietary and physical activity behavior: a randomized controlled trial about users and usage. J Med Internet Res. (2011) 13:e1624. doi: 10.2196/jmir.1624
51. Gage R, Girling-Butcher M, Joe E, Smith M, Ni Mhurchu C, McKerchar C, et al. The frequency and context of snacking among children: an objective analysis using wearable cameras. Nutrients. (2020) 13:103. doi: 10.3390/nu13010103
52. Lowe B, Fraser I, Souza-Monteiro DM. A change for the better? Digital health technologies and changing food consumption behaviors. Psychol Mark. (2015) 32:585–600. doi: 10.1002/mar.20802
53. Annosi MC, Brunetta F, Bimbo F, Kostoula M. Digitalization within food supply chains to prevent food waste. Drivers, barriers and collaboration practices. Ind Mark Manag. (2021) 93:208–20. doi: 10.1016/j.indmarman.2021.01.005
54. Fuchs KL, Lian J, Michels L, Mayer S, Toniato E, Tiefenbeck V. Effects of digital food labels on healthy food choices in online grocery shopping. Nutrients. (2022) 14:2044. doi: 10.3390/nu14102044
55. Ng WWM, Wong ASW, Cheung K. A cluster randomized controlled trial feasibility study of a WhatsApp-delivered intervention to promote healthy eating habits in male firefighters. Int J Environ Res Public Health. (2021) 18:6633. doi: 10.3390/ijerph18126633
56. Hernández-Reyes A, Cámara-Martos F, Recio GM, Molina-Luque R, Romero-Saldaña M, Rojas RM. Push notifications from a mobile app to improve the body composition of overweight or obese women: randomized controlled trial. JMIR MHealth UHealth. (2020) 8:e13747. doi: 10.2196/13747
57. Agarwal P, Mukerji G, Desveaux L, Ivers NM, Bhattacharyya O, Hensel JM, et al. Mobile app for improved self-management of type 2 diabetes: multicenter pragmatic randomized controlled trial. JMIR Mhealth Uhealth. (2019) 7(1):e10321. doi: 10.2196/10321
58. Brindal E, Hendrie GA, Freyne J, Noakes M. A mobile phone app designed to support weight loss maintenance and well-being (MotiMate): randomized controlled trial. JMIR MHealth UHealth. (2019) 7:e12882. doi: 10.2196/12882
59. Lee K-W, Kim H-B, Lee S-H, Ha H-K. Changes in weight and health-related behavior using smartphone applications in patients with colorectal polyps. J Nutr Educ Behav. (2019) 51:539–46. doi: 10.1016/j.jneb.2019.02.002
60. Bi T, Bambling M, Edirippulige S. The Mindfulness App Trial for Weight, Weight-Related Behaviors, and Stress in University Students: Randomized Controlled Trial.
61. Stephens JD, Yager AM, Allen J. Smartphone technology and text messaging for weight loss in young adults: a randomized controlled trial. J Cardiovasc Nurs. (2017) 32:39. doi: 10.1097/JCN.0000000000000307
62. Ojeda-Rodríguez A, Zazpe I, Morell-Azanza L, Chueca MJ, Azcona-Sanjulian MC, Marti A. Improved diet quality and nutrient adequacy in children and adolescents with abdominal obesity after a lifestyle intervention. Nutrients. (2018) 10:1500. doi: 10.3390/nu10101500
63. Bijlholt M, Ameye L, Van Uytsel H, Devlieger R, Bogaerts A. The inter-act e-health supported lifestyle intervention improves postpartum food intake and eating behavior, but not physical activity and sedentary behavior—a randomized controlled trial. Nutrients. (2021) 13:1287. doi: 10.3390/nu13041287
64. Spring B, Pellegrini CA, Pfammatter A, Duncan JM, Pictor A, McFadden HG, et al. Effects of an abbreviated obesity intervention supported by mobile technology: the ENGAGED randomized clinical trial. Obesity. (2017) 25(7):1191–8. Altern TEXT Fig. 1. doi: 10.1002/oby.21842
65. Bonn SE, Alexandrou C, Hjörleifsdottir Steiner K, Wiklander K, Östenson C-G, Löf M, et al. App-technology to increase physical activity among patients with diabetes type 2-the DiaCert-study, a randomized controlled trial. BMC Public Health. (2018) 18:119. doi: 10.1186/s12889-018-5026-4
66. Ek A, Delisle Nyström C, Chirita-Emandi A, Tur JA, Nordin K, Bouzas C, et al. A randomized controlled trial for overweight and obesity in preschoolers: the more and less Europe study-an intervention within the STOP project. BMC Public Health. (2019) 19:1–13. doi: 10.1186/s12889-018-6343-3
67. Eisenhauer CM, Brito F, Kupzyk K, Yoder A, Almeida F, Beller RJ, et al. Mobile health assisted self-monitoring is acceptable for supporting weight loss in rural men: a pragmatic randomized controlled feasibility trial. BMC Public Health. (2021) 21:1–16. doi: 10.1186/s12889-021-11618-7
68. Boels AM, Rutten G, Zuithoff N, De Wit A, Vos R. Effectiveness of diabetes self-management education via a smartphone application in insulin treated type 2 diabetes patients–design of a randomised controlled trial (‘TRIGGER study’). BMC Endocr Disord. (2018) 18:1–10. doi: 10.1186/s12902-018-0304-9
69. Järvelä-Reijonen E, Karhunen L, Sairanen E, Muotka J, Lindroos S, Laitinen J, et al. The effects of acceptance and commitment therapy on eating behavior and diet delivered through face-to-face contact and a mobile app: a randomized controlled trial. Int J Behav Nutr Phys Act. (2018) 15:1–14. doi: 10.1186/s12966-018-0654-8
70. Kennelly MA, Ainscough K, Lindsay KL, O’Sullivan E, Gibney ER, McCarthy M, et al. Pregnancy exercise and nutrition with smartphone application support: a randomized controlled trial. Obstet Gynecol. (2018) 131:818–26. doi: 10.1097/AOG.0000000000002582
71. Chagas CMDS, Pontes e Silva TB, Reffatti LM, Botelho RBA, Toral N. Rango cards, a digital game designed to promote a healthy diet: a randomized study protocol. BMC Public Health. (2018) 18:910. doi: 10.1186/s12889-018-5848-0
72. Sutherland R, Brown A, Nathan N, Janssen L, Reynolds R, Walton A, et al. Protocol for an effectiveness- implementation hybrid trial to assess the effectiveness and cost-effectiveness of an m-health intervention to decrease the consumption of discretionary foods packed in school lunchboxes: the ’SWAP IT’ trial. BMC Public Health. (2019) 19:1510. doi: 10.1186/s12889-019-7725-x
73. Pieniak Z, Żakowska-Biemans S, Kostyra E, Raats M. Sustainable healthy eating behaviour of young adults: towards a novel methodological approach. BMC Public Health. (2016) 16:1–9. doi: 10.1186/s12889-016-3260-1
74. Helle C, Hillesund ER, Wills AK, Øverby NC. Evaluation of an eHealth intervention aiming to promote healthy food habits from infancy-the Norwegian randomized controlled trial early food for future health. Int J Behav Nutr Phys Act. (2019) 16:1–16. doi: 10.1186/s12966-018-0763-4
75. Van Lippevelde W, Vangeel J, De Cock N, Lachat C, Goossens L, Beullens K, et al. Using a gamified monitoring app to change adolescents’ snack intake: the development of the REWARD app and evaluation design. BMC Public Health. (2016) 16:1–11. doi: 10.1186/s12889-016-3286-4
76. Boh B, Lemmens LH, Jansen A, Nederkoorn C, Kerkhofs V, Spanakis G, et al. An ecological momentary intervention for weight loss and healthy eating via smartphone and internet: study protocol for a randomised controlled trial. Trials. (2016) 17:1–12. doi: 10.1186/s13063-015-1128-9
77. Dorsch MP, Cornellier ML, Poggi AD, Bilgen F, Chen P, Wu C, et al. Effects of a novel contextual just-in-time mobile app intervention (LowSalt4Life) on sodium intake in adults with hypertension: pilot randomized controlled trial. JMIR MHealth UHealth. (2020) 8:e16696. doi: 10.2196/16696
78. Eyles H, McLean R, Neal B, Jiang Y, Doughty RN, McLean R, et al. A salt-reduction smartphone app supports lower-salt food purchases for people with cardiovascular disease: findings from the SaltSwitch randomised controlled trial. Eur J Prev Cardiol. (2017) 24:1435–44. doi: 10.1177/2047487317715713
79. He FJ, Zhang P, Luo R, Li Y, Sun Y, Chen F, et al.. app based education programme to reduce salt intake (AppSalt) in schoolchildren and their families in China: parallel, cluster randomised controlled trial. Br Med J. (2022):376. doi: 10.1136/bmj-2021-066982
80. Ipjian ML, Johnston CS. Smartphone technology facilitates dietary change in healthy adults. Nutrition. (2017) 33:343–7. doi: 10.1016/j.nut.2016.08.003
81. Bozorgi A, Hosseini H, Eftekhar H, Majdzadeh R, Yoonessi A, Ramezankhani A, et al. The effect of the mobile “blood pressure management application” on hypertension self-management enhancement: a randomized controlled trial. Trials. (2021) 22:413. doi: 10.1186/s13063-021-05270-0
82. Pack S, Lee J. Randomised controlled trial of a smartphone application-based dietary self-management program on haemodialysis patients. J Clin Nurs. (2021) 30:840–8. doi: 10.1111/jocn.15627
83. Mummah S, Robinson TN, Mathur M, Farzinkhou S, Sutton S, Gardner CD. Effect of a mobile app intervention on vegetable consumption in overweight adults: a randomized controlled trial. Int J Behav Nutr Phys Act. (2017) 14:1–10. doi: 10.1186/s12966-017-0563-2
84. Kato-Lin Y-C, Padman R, Downs J, Abhishek V. Evaluating consumer m-health services for promoting healthy eating: a randomized field experiment. In: AMIA Annual Symposium Proceedings. Pittsburgh, Pennsylvania: American Medical Informatics Association (2015). p. 1947.
85. Recio-Rodriguez JI, Agudo-Conde C, Martin-Cantera C, González-Viejo MN, Fernandez-Alonso MDC, Arietaleanizbeaskoa MS, et al. Short-term effectiveness of a mobile phone app for increasing physical activity and adherence to the Mediterranean diet in primary care: a randomized controlled trial (EVIDENT II study). J Med Internet Res. (2016) 18:e331. doi: 10.2196/jmir.6814
86. Meule A, Richard A, Dinic R, Blechert J, Meule A. Effects of a Smartphone-Based Approach–Avoidance Intervention on Chocolate Craving and Consumption. JMIR MHealth UHealth Press (2019).
87. Wengreen HJ, Joyner D, Kimball SS, Schwartz S, Madden GJ. A randomized controlled trial evaluating the FIT game’s efficacy in increasing fruit and vegetable consumption. Nutrients (2021) 13:2646. doi: 10.3390/nu13082646
88. Farrow C, Belcher E, Coulthard H, Thomas JM, Lumsden J, Hakobyan L, et al. Using repeated visual exposure, rewards and modelling in a mobile application to increase vegetable acceptance in children. Appetite. (2019) 141:104327. doi: 10.1016/j.appet.2019.104327
89. Apiñaniz A, Cobos-Campos R, Sáez de Lafuente-Moríñigo A, Parraza N, Aizpuru F, Pérez I, et al. Effectiveness of randomized controlled trial of a mobile app to promote healthy lifestyle in obese and overweight patients. Fam Pract. (2019) 36:699–705. doi: 10.1093/fampra/cmz020
90. Dodd JM, Louise J, Cramp C, Grivell RM, Moran LJ, Deussen AR. Evaluation of a smartphone nutrition and physical activity application to provide lifestyle advice to pregnant women: the SNAPP randomised trial. Matern Child Nutr. (2018) 14:e12502. doi: 10.1111/mcn.12502
91. Garnweidner-Holme L, Henriksen L, Torheim LE, Lukasse M. Effect of the pregnant+ smartphone app on the dietary behavior of women with gestational diabetes mellitus: secondary analysis of a randomized controlled trial. JMIR MHealth UHealth. (2020) 8:e18614. doi: 10.2196/18614
92. Leone LA, Tripicchio GL, Haynes-Maslow L, McGuirt J, Grady Smith JS, Armstrong-Brown J, et al. Cluster randomized controlled trial of a mobile market intervention to increase fruit and vegetable intake among adults in lower-income communities in North Carolina. Int J Behav Nutr Phys Act. (2018) 15:1–11. doi: 10.1186/s12966-017-0637-1
93. Likhitweerawong N, Boonchooduang N, Kittisakmontri K, Chonchaiya W, Louthrenoo O. Effectiveness of mobile application on changing weight, healthy eating habits, and quality of life in children and adolescents with obesity: a randomized controlled trial. BMC Pediatr. (2021) 21:1–9. doi: 10.1186/s12887-021-02980-x
94. Lugones-Sánchez C, Recio-Rodríguez JI, Menéndez-Suárez M, Saz-Lara A, Ramirez-Manent JI, Sánchez-Calavera MA, et al. Effect of a multicomponent mHealth intervention on the composition of diet in a population with overweight and obesity—randomized clinical trial EVIDENT 3. Nutrients. (2022) 14:270. doi: 10.3390/nu14020270
95. Nikniaz Z, Shirmohammadi M, Namvar ZA. Development and effectiveness assessment of a Persian-language smartphone application for celiac patients: a randomized controlled clinical trial. Patient Educ Couns. (2021) 104:337–42. doi: 10.1016/j.pec.2020.08.014
96. Palacios C, Torres M, López D, Trak-Fellermeier MA, Coccia C, Pérez CM. Effectiveness of the nutritional app “mynutricart” on food choices related to purchase and dietary behavior: a pilot randomized controlled trial. Nutrients. (2018) 10:1967. doi: 10.3390/nu10121967
97. Turner-McGrievy G, Tate D. Tweets, apps, and pods: results of the 6-month Mobile pounds off digitally (Mobile POD) randomized weight-loss intervention among adults. J Med Internet Res. (2011) 13:e120. doi: 10.2196/jmir.1841
98. Weber A. Mobile apps as a sustainable shopping guide: the effect of eco-score rankings on sustainable food choice. Appetite. (2021) 167:105616. doi: 10.1016/j.appet.2021.105616
99. Whitelock V, Kersbergen I, Higgs S, Aveyard P, Halford JC, Robinson E. A smartphone based attentive eating intervention for energy intake and weight loss: results from a randomised controlled trial. BMC Public Health. (2019) 19:1–11. doi: 10.1186/s12889-019-6923-x
100. Chow EJ, Doody DR, Di C, Armenian SH, Baker KS, Bricker JB, et al. Feasibility of a behavioral intervention using mobile health applications to reduce cardiovascular risk factors in cancer survivors: a pilot randomized controlled trial. J Cancer Surviv. (2021) 15:554–63. doi: 10.1007/s11764-020-00949-w
101. Goni L, de la O V, Barrio-López MT, Ramos P, Tercedor L, Ibañez-Criado JL, et al. A remote nutritional intervention to change the dietary habits of patients undergoing ablation of atrial fibrillation: randomized controlled trial. J Med Internet Res. (2020) 22:e21436. doi: 10.2196/21436
102. Xu Z, Geng J, Zhang S, Zhang K, Yang L, Li J, et al. A mobile-based intervention for dietary behavior and physical activity change in individuals at high risk for type 2 diabetes mellitus: randomized controlled trial. JMIR MHealth UHealth. (2020) 8:e19869. doi: 10.2196/19869
103. Ahn Y, Bae J, Kim H-S. The development of a mobile u-health program and evaluation for self-diet management for diabetic patients. Nutr Res Pract. (2016) 10:342–51. doi: 10.4162/nrp.2016.10.3.342
104. Billah SM, Ferdous TE, Kelly P, Raynes-Greenow C, Siddique AB, Choudhury N, et al. Effect of nutrition counselling with a digital job aid on child dietary diversity: analysis of secondary outcomes from a cluster randomised controlled trial in rural Bangladesh. Matern Child Nutr. (2022) 18:e13267. doi: 10.1111/mcn.13267
105. Kaur J, Kaur M, Chakrapani V, Webster J, Santos JA, Kumar R. Effectiveness of information technology–enabled ’SMART eating’health promotion intervention: a cluster randomized controlled trial. PloS One. (2020) 15:e0225892. doi: 10.1111/mcn.13286
106. Carfora V, Caso D, Conner M. Randomized controlled trial of a messaging intervention to increase fruit and vegetable intake in adolescents: affective versus instrumental messages. Br J Health Psychol. (2016) 21:937–55. doi: 10.1111/bjhp.12208
107. Lim SL, Ong KW, Johal J, Han CY, Yap QV, Chan YH, et al. Effect of a smartphone app on weight change and metabolic outcomes in Asian adults with type 2 diabetes: a randomized clinical trial. JAMA Netw Open. (2021) 4:e2112417–e2112417. doi: 10.1001/jamanetworkopen.2021.12417
108. Ambeba EJ, Ye L, Sereika SM, Styn MA, Acharya SD, Sevick MA, et al. The use of mHealth to deliver tailored messages reduces reported energy and fat intake. J Cardiovasc Nurs. (2015) 30:35–43. doi: 10.1097/JCN.0000000000000120
109. Billah SM, Ferdous TE, Siddique AB, Raynes-Greenow C, Kelly P, Choudhury N, et al. The effect of electronic job aid assisted one-to-one counselling to support exclusive breastfeeding among 0–5-month-old infants in rural Bangladesh. Matern Child Nutr. (2022) 18:e13377. doi: 10.1111/mcn.13377
110. Zenun Franco R, Fallaize R, Weech M, Hwang F, Lovegrove JA. Effectiveness of web-based personalized nutrition advice for adults using the eNutri web app: evidence from the EatWellUK randomized controlled trial. J Med Internet Res. (2022) 24:e29088. doi: 10.2196/29088
111. Inauen J, Bolger N, Shrout PE, Stadler G, Amrein M, Rackow P, et al. Using smartphone-based support groups to promote healthy eating in daily life: a randomised trial. Appl Psychol Health Well-Being. (2017) 9:303–23. doi: 10.1111/aphw.12093
112. van Dijk MR, Koster MP, Oostingh EC, Willemsen SP, Steegers EA, Steegers-Theunissen RP. A mobile app lifestyle intervention to improve healthy nutrition in women before and during early pregnancy: single-center randomized controlled trial. J Med Internet Res. (2020) 22:e15773. doi: 10.2196/15773
113. Wu Q, Huang Y, Liao Z, van Velthoven MH, Wang W, Zhang Y. Effectiveness of WeChat for improving exclusive breastfeeding in Huzhu County China: randomized controlled trial. J Med Internet Res. (2020) 22:e23273. doi: 10.2196/23273
114. NCI. Theory at a Glance—A Guide For Health Promotion Practice (Second Edition) | Demand Generation I-Kit for Underutilized, Life Saving Commodities. 2005. Available at: https://sbccimplementationkits.org/demandrmnch/ikitresources/theory-at-a-glance-a-guide-for-health-promotion-practice-second-edition/ (Accessed August 19, 2023).
115. WHO WH. WHO global report on sodium intake reduction. In: WHO global report on sodium intake reduction. 2023.
116. Coughlin SS, Whitehead M, Sheats JQ, Mastromonico J, Hardy D, Smith SA. Smartphone applications for promoting healthy diet and nutrition: a literature review. Jacobs J Food Nutr. (2015) 2:021. doi: 10.1186/s12889-019-6923-x
117. Li Y, Guan M, Hammond P, Berrey LE. Communicating COVID-19 information on TikTok: a content analysis of TikTok videos from official accounts featured in the COVID-19 information hub. Health Educ Res. (2021) 36:261–71. doi: 10.1093/her/cyab010
118. Schubbe D, Scalia P, Yen RW, Saunders CH, Cohen S, Elwyn G, et al. Using pictures to convey health information: a systematic review and meta-analysis of the effects on patient and consumer health behaviors and outcomes. Patient Educ Couns. (2020) 103:1935–60. doi: 10.1016/j.pec.2020.04.010
119. Samoggia A, Monticone F, Bertazzoli A. Innovative digital technologies for purchasing and consumption in urban and regional agro-food systems: a systematic review. Foods. (2021) 10:208. doi: 10.3390/foods10020208
120. Mahumud RA, Uprety S, Wali N, Renzaho AM, Chitekwe S. The effectiveness of interventions on nutrition social behaviour change communication in improving child nutritional status within the first 1000 days: evidence from a systematic review and meta-analysis. Matern Child Nutr. (2022) 18:e13286. doi: 10.1111/mcn.13286
Keywords: smartphone apps, healthy eating behavior, systematic review, RCTs, web based applications
Citation: Seid A, Fufa DD and Bitew ZW (2024) The use of internet-based smartphone apps consistently improved consumers' healthy eating behaviors: a systematic review of randomized controlled trials. Front. Digit. Health 6:1282570. doi: 10.3389/fdgth.2024.1282570
Received: 24 August 2023; Accepted: 2 January 2024;
Published: 12 January 2024.
Edited by:
Edmund W. J. Lee, Nanyang Technological University, SingaporeReviewed by:
Maija Kale, University of Latvia, LatviaJed Senthil, Nanyang Technological University, Singapore
© 2024 Seid, Fufa and Bitew. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Awole Seid c2F3bGF5ZWh1QGdtYWlsLmNvbQ==