 Laura Gosselin1,2*
Laura Gosselin1,2* Romain Leguillon1,2,3
Romain Leguillon1,2,3 Laetitia Rollin3,4Emeline Lejeune1Stéfan J. Darmoni1,3Julien Grosjean1,3
Laetitia Rollin3,4Emeline Lejeune1Stéfan J. Darmoni1,3Julien Grosjean1,3
- 1Department of Digital Health, Rouen University Hospital, Rouen, France
- 2Department of Pharmacy, Rouen University Hospital, Rouen, France
- 3Laboratoire D'Informatique Médicale et D'Ingénierie des Connaissances en e-Santé (LIMICS), U1142, INSERM, Sorbonne Université, Paris, France
- 4Institute of Occupational Medicine, Rouen University Hospital, Rouen, France
Background: Drug-related problems (DRPs) can lead to serious health issues and have significant economic impacts on healthcare systems. One solution to address this issue is the use of computerized physician order entry systems (CPOE), which can help prevent DRPs by reducing the risk of medication errors.
Objective: The purpose of this study is to provide an analysis on scientific production of the past 20 years in order to describe trends in academic publishing on CPOE and to identify the major topics as well as the predominant actors (journals, countries) involved in this field.
Methods: A PubMed search was carried out to extract articles related to computerized provider order entry during the period January 1st 2003– December 31st 2022 using a specific query. Data were downloaded from PubMed in Extensible Markup Language (XML) and were processed through a dedicated parser.
Results: A total of 2,946 articles were retrieved among 623 journals. One third of these articles were published in eight journals. Publications grew strongly from 2002 to 2006, with a dip in 2008 followed by an increase again in 2009. After 2009, there follows a decreasing until 2022.The most producing countries are the USA with 51.39% of the publication over the period by France (3.80%), and Canada (3.77%). About disciplines, the top 3 is: “medical informatics” (21.62% of articles), “pharmacy” (19.04%), and “pediatrics” (6.56%).
Discussion: This study provides an overview of publication trends related to CPOE, which exhibited a significant increase in the first decade of the 21st century followed by a decline after 2009. Possible reasons for this decline include the emergence of digital health tools beyond CPOE, as well as healthcare professionals experiencing alert fatigue of the current system.
Conclusion: Future research should focus on analyzing publication trends in the field of medical informatics and decision-making tools to identify other areas of interest that may have surpassed the development of CPOE.
Background
Drug-related problems (DRPs) are a significant public health issue that affects patients worldwide. DRPs refer to any unwanted or harmful event associated with the use of medications, including adverse drug reactions, medication errors, and drug interactions. DRPs can result in hospitalization, disability, and even death, and they have a significant economic impact on healthcare systems (1, 2).
To address this issue, there are several solutions, including the use of computerized physician order entry (CPOE) systems to secure medication prescriptions (3). CPOE comes in two main types: hospital CPOE, which is used in healthcare institutions and limits drug choices to define lists, and ambulatory medicine CPOE. By using CPOE systems, healthcare professionals can help prevent DRPs by reducing the risk of medication errors, including incorrect dosages or medication interactions.
This study aims to assess the current trends in academic publishing on computerized physician order entry (CPOE) through proven bibliographic methods (4, 5). Specifically, it involves conducting a mapping review to identify the key contributors to the field (e.g., journals, countries), the most advanced medical disciplines on the subject, the prevalent themes, and the evolution of published articles since the inception of CPOE.
To our knowledge, no bibliometric analysis of CPOE has been carried out. It is important to conduct this research to map and analyze publications related to CPOE. This analysis can help identify weaknesses and improve CPOE research. Other works have consisted in drawing up a history of CPOEs but without a macroscopic vision or in a way that is too descriptive of the very principles of the discipline (6, 7). More methodologically similar studies have appeared but only on topics such as drug errors and adverse drug reactions in 2019 (8).
Methods
Bibliographic research
This study utilized the MEDLINE bibliographic database, which contains a vast collection of scientific articles from the biomedical field spanning several decades. The database's search engine, PubMed, enables the use of MeSH thesaurus keywords for precise indexing of articles, and it also permits searching for terms in unstructured fields such as article titles and abstracts. Additionally, the Boolean-compatible syntax, featuring the use of operators such as AND, OR, and NOT, provides exceptional flexibility for conducting queries.
The following query was constructed with the help of a medical librarian (EL) to select articles indexed with the keywords “Computerized Physician Order Entry” (MeSH identifier D050316) between 2003 and 2022 (a period of 20 completed years). To increase recall, the terms “CPOE”, “Computerized Physician Order Entry”, “computerized physician order entry system”, “computerized Provider Order Entry”, “Computerized Provider Order Entry System”, “prescription tool”, “prescription support tool”, and “medication alert system” were searched in the title. In order to minimize noise (false positives), some terms were excluded such as “laboratory test” or “laboratory”. The final equation is as follows:
“medical order entry systems"[MH] OR “medical order entry system*"[TW] OR CPOE[TW] OR “Computerized Physician Order Entry"[TW] OR “computerized physician order entry system"[TW] OR “computerized Provider Order Entry"[TW] OR “Computerized Provider Order Entry System"[TW] OR “prescription tool*"[TW] OR “prescription support tool*"[TW] OR “medication alert system*"[TW] NOT “laboratory test*"[TW] NOT “laboratory"[TW]
Extraction and processing of data
The bibliographic references retrieved from PubMed through the query are in XML (eXtensible Markup Language) format. A specialized program is used to extract relevant data from selected metadata, including the year of publication, author names and affiliations, journal, MeSH keywords, publication type, and language.
Two additional metadata were automatically added using specialized algorithms. First, the country of publication was inferred from the affiliation of the first author, which is typically the most informed and representative of the article's content. A computer program utilizing the Google Maps API and a dedicated database was used to identify the country from the author's email domain or location. Second, medical specialties were assigned to each reference based on the MeSH keywords using a categorization algorithm developed previously (9). The algorithm leverages the MeSH hierarchy and relations defined by domain experts to associate each keyword with one or more medical specialties (10). We conducted a human verification of a random sample of 100 articles related to CPOE (evaluation, design, and use of CPOE) by two individuals (LG and JG). This verification involved assessing the titles and abstracts of the articles to ensure that the retrieved results are relevant to CPOE.
Further information on the yearly publication count in MEDLINE was directly obtained from PubMed. Moreover, the total number of publications from these journals during the study period was compiled in the data table sourced from PubMed. Population data, including population size and Gross Domestic Product (GDP) per capita by country, were sourced from the World Population Review (http://worldpopulationreview.com) and the World Bank (https://data.worldbank.org/indicator).
Bradford's law was used to rank the journals. Bradford's law is also known as Bradford's law of scattering or the Bradford distribution, as it describes how the articles on a particular subject are scattered throughout the mass of periodicals (11).
The data were compiled into a table, enabling the creation of sub-tables and corresponding graphs.
Analyse of datas
The different data were extracted from our tool in the form of an Excel® spreadsheet. The columns ID MeSH, type of publication, N, and proportion of articles (%) were extracted directly.
Results
PubMed query yielded a total of 2,946 articles. Out of the 100 articles in the sample, 100% were found to be related to CPOE. As shown in Figure 1, there was significant growth from 2002 to 2006, followed by a decline in 2008 and subsequent increase in 2009. However, from 2009 onwards, there was a downward trend until 2022, with the highest number of articles (212 references) published in 2009 and only 67 articles published in 2022. The average annual increase in articles on the subject was 1.27% [−0.36; 23.00].
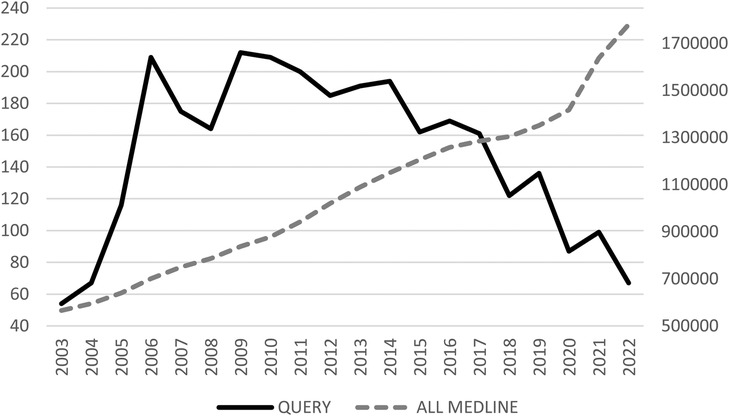
Figure 1. Evolution of the number of articles per year for MEDLINE and for the query.
Journals
Out of the 623 journals that published at least one article identified by the query, only five published over 100 articles, and 13 published more than 30 articles. Bradford's law was used to rank the journals, with eight journals publishing one third of the identified articles (1.8% of the journals), 59 journals publishing the second third (9.47% of the journals), and the rest of the journals publishing the final third, representing the vast majority (89.24%). Among the 13 journals that published more than 30 articles, 7 (53.85%) were specialized in the field of medical informatics. Table 1 shows that none of the main journals identified had a proportion of articles exceeding 10%. The Journal of the American Medical Informatics Association (JAMIA) had the highest proportion of articles at 7.71%.
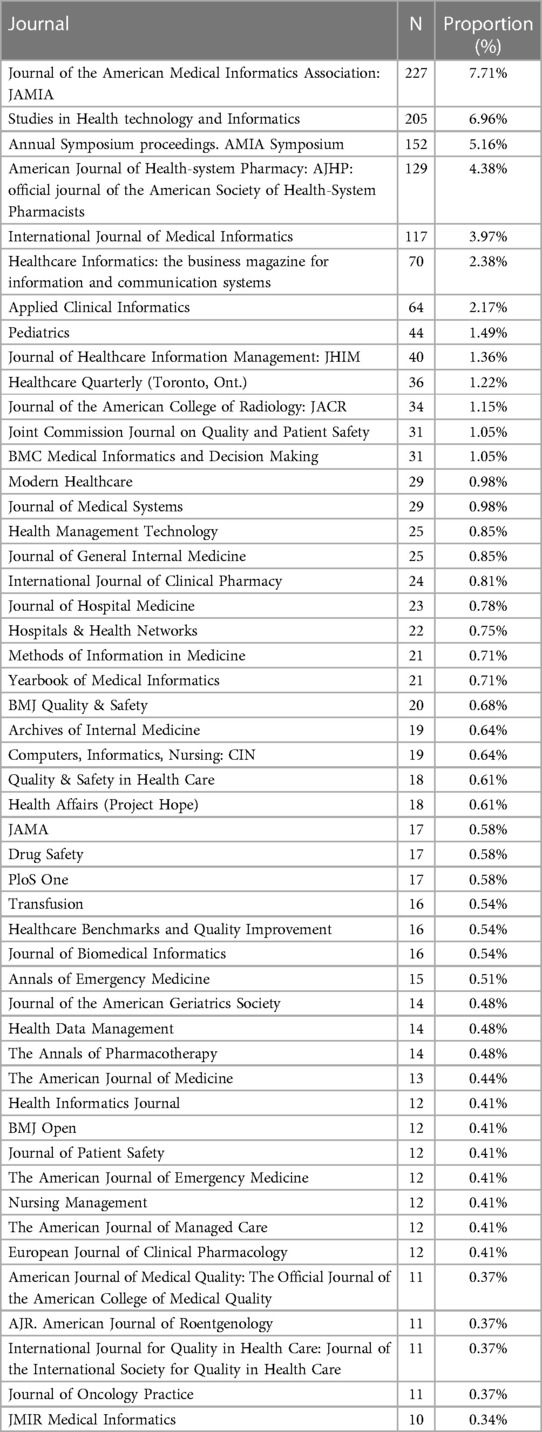
Table 1. Top 50 journals that published the articles identified by the query.
Languages
Most of the articles were written in English (96.9%), with Spanish and French, as well as German and Danish, accounting for 0.8% to 0.4% of the articles, respectively (Table 2). In MEDLINE, English was the predominant language at 97.89%, followed by Chinese at 0.62% and German at 0.52%. Nowadays, English is the predominant language for writing scientific articles, so the trend is quite normal.
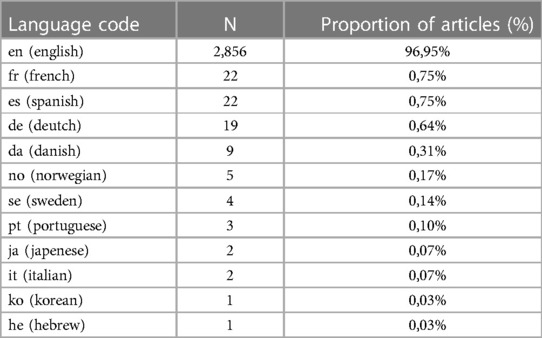
Table 2. Language distribution of the articles identified by the query.
Countries
Out of the 2,946 articles, 2,516 (85.4%) had a first author affiliation that identified a country. Table 3 provides a breakdown of the number of articles and ratios according to population size and GDP per capita (PPP, in international dollars). The United States of America led with 51.39% of the articles (among countries identified), followed by France (3.80%), Canada (3.77%), Australia (3.36%), and the United Kingdom (3.12%). The top 5 countries with the highest number of articles per 100,000 inhabitants were Australia (1.1), Switzerland (0.59), the United States of America (0.46), the Netherlands (0.45), and Denmark (0.36). Meanwhile, the top 5 countries with the highest number of articles per GDP (in PPP per 1,000 international dollars) were the United States of America (23.95), France (2.38), Canada (2.38), Australia (1.86), and the United Kingdom (1.66).
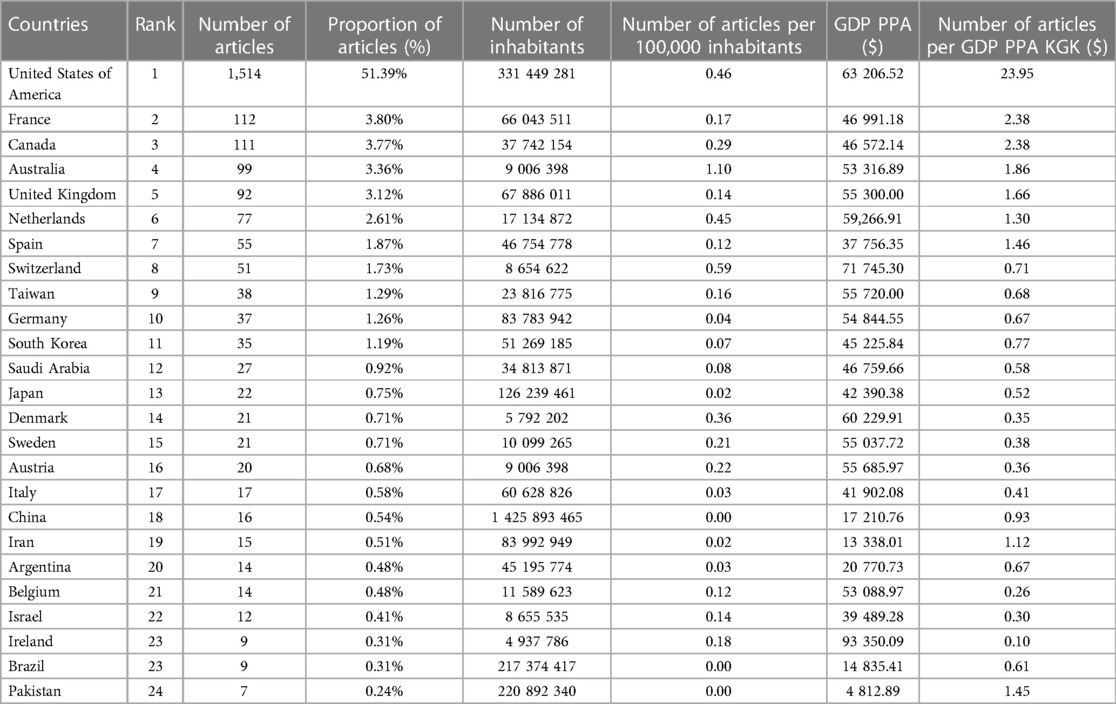
Table 3. Top 25 countries associated with the items identified by the query.
Types of publication
To filter out uninformative types such as grant-related publication types like “non-U.S. government research grant”, “NIH extramural research grant”, “U.S. government PHS research grant”, and “NA”, we retained 36 relevant publication types. The top 15 publication types account for almost all articles (see Table 4). These include journal article (93.73% of the relevant publication types), literature reviews (5.23%), comparative studies (3.36%), evaluation studies (2.47%), and commentaries (2.16%). The data in Table 4 are raw, and an article can have multiple types of publication.
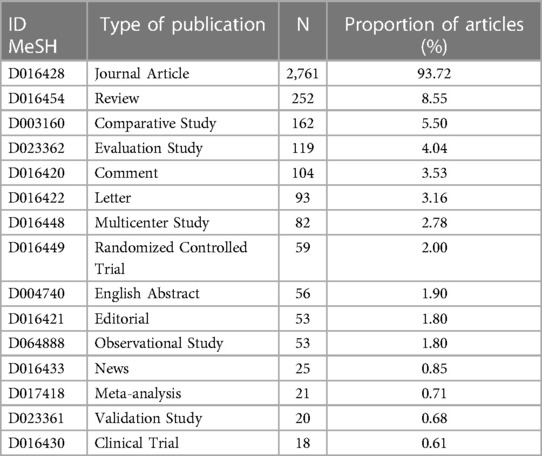
Table 4. Top 15 publication types (MeSH) of articles identified by the query.
MeSH terms
In total, 2,946 articles were identified in the study, which were indexed with 1,788 unique MeSH keywords. Check tags were excluded from the analysis as they did not provide any useful information. Table 5 presents the top 50 most frequently occurring keywords. The most common keywords were «Medical order entry systems» (68.53%), «Medication errors» (28.89%), «clinical decision support systems» (20.88%), and «United States» (16.63%).
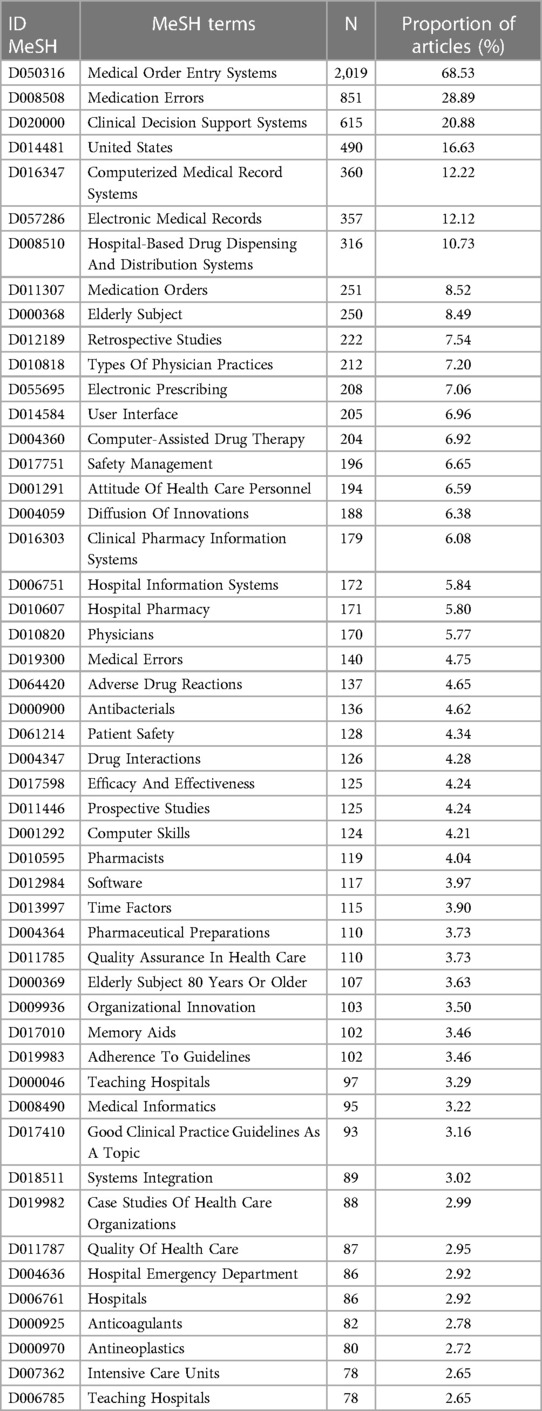
Table 5. Top 50 MeSH keywords that index the identified articles.
Medical specialties
The categorization algorithm is grounded on MeSH keywords to infer broad categories, particularly in the field of health, medicine, or paramedical disciplines. As a result, a total of 85 disciplines were identified among the articles (representing 60.28% out of 141 disciplines in total) as presented in Table 6. The top 5 disciplines include “medical informatics” accounting for 21.62% of the articles, followed by “pharmacy” at 19.04%, “pediatrics” at 6.56%, “medicine” at 5.45%, and “geriatrics” at 4.49%.
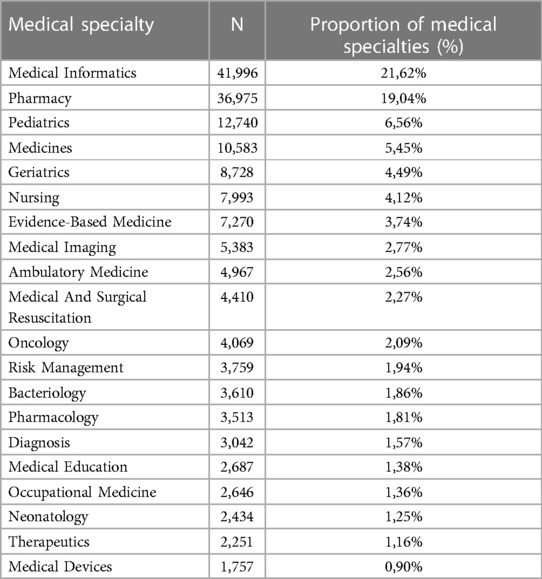
Table 6. Health disciplines calculated via the categorization algorithm from the MeSH keywords indexing the identified articles.
Discussion
The main results of this study provide us with trends in publications related to CPOE. Indeed, the first decade of the 21st century was marked by an increase in publications each year, which is correlated with the implementation of health information systems. Today, whether for hospital or primary care, CPOE systems are widely implemented in the daily practices of different healthcare professionals.
However, after 2009, there has been a clear decrease in the number of publications regarding CPOE, despite strong pressure from public authorities to continue digitizing healthcare systems. One possible line of thought that can be suggested is that the digitization of health tools is not only through CPOE (artificial intelligence, decision support, etc.) but also through a certain exhaustion of professionals towards CPOE. On the other hand, CPOE are now totally integrated in most hospital information systems and in software in primary care, as well as in some health information systems (at a national level, e.g., Israel, Denmark, Taiwan, Singapore).
Regarding Figure 1, the curve of our query decreases from 2009 while the trend of articles published on Medline only increases. Over the course of the past 20 years, the field of Computerized Physician Order Entry (CPOE) has witnessed a significant evolution, transitioning from an innovative technology to a mature one. This shift can be attributed to several factors.
Initially, when CPOE was introduced, it was considered a groundbreaking technology with the potential to revolutionize healthcare systems. Its implementation was met with enthusiasm and high expectations for improving patient safety, reducing medication errors, and enhancing overall workflow efficiency. Researchers and practitioners were eager to explore its capabilities and document its impact through academic publications.
As CPOE became more widely adopted and integrated into healthcare organizations, the initial wave of excitement and novelty subsided. With increased implementation, researchers began to shift their focus from simply exploring the technology's benefits to evaluating its real-world effectiveness and identifying areas for improvement. This transition from exploration to evaluation is characteristic of the maturation process.
Moreover, as CPOE became more commonplace, it started to be considered a standard practice rather than an innovative solution. Healthcare organizations began to expect its implementation as part of their electronic health record (EHR) systems. Consequently, the emphasis shifted from proving the concept to refining and optimizing the existing implementations. This shift in focus led to a decline in the number of publications specifically addressing the “acceptance” and “implementation” of CPOE.
Concerning the journals of publication and the medical specialties most found, medical informatics and digital health is predominant (e.g., JAMIA). Finally, few other specialties are interested or at least publish on this subject, except for pharmacy (concerned with drug prescribing and prescription analysis (e.g., AJHP), and care units such as pediatrics and geriatrics in which drug errors are more likely to occur.
Despite the ongoing issues of medication errors, the first impression is that researchers have come full circle about CPOE. This topic is becoming obsolete despite the fashion for artificial intelligence (AI) and all the possibilities for improving these CPOE coupled with AI.
Some countries, such as Canada, the United Kingdom (12) and Australia (13), are known to have a highly developed clinical pharmacy activity. This activity is based on good IT tools and good CPOE. Along with the United States and France, they are the countries that publish the most (in terms of the number of articles per 100,000 inhabitants).
It should be emphasized that CPOE are programmed with pre-established rules, which is called symbolic artificial intelligence. Today, there is shift towards digital artificial intelligence that is taking over thanks to all the health data that has been digitized. These two types of artificial intelligence deserve to be brought together in order to build a more efficient and personalized CPOE based on the prescriber and their prescribing habits.
Several studies highlight that the alert system of CPOE leads to a certain weariness of healthcare professionals who eventually stop using these tools in their entirety (14, 15).
Finally, another of our hypotheses concerning the decline in publications in this field is the change in research and economic models. Indeed, the research and publication field are mainly public, while it is the private software industry that creates the CPOE. The research and development sector of private industries is in sharp decline, and start-ups that create upstream software models are bought and developed by large software companies, which may tend to a decrease in scientific publication.
CPOE systems help reduce medication prescribing errors, such as dosage errors, potential drug interactions, and drug allergies. They facilitate communication among different healthcare professionals involved in patient care, thereby reducing communication errors and misunderstandings. Additionally, they can provide alerts and clinical guidance based on best practices and drug information, assisting prescribers in making more informed decisions and avoiding errors. Lastly, CPOE systems allow for tracking of medical orders, thereby facilitating monitoring of administered medications, detection of potential errors, and evaluation of therapeutic regimens. For future research, researchers could build upon the findings of our bibliometric analysis to design more effective and user-friendly CPOE systems. Indeed, alert fatigue remains a major usability barrier for CPOE systems, as described earlier. Additionally, some countries may consider investing in research on CPOE to mitigate medication prescribing errors.
It should be noted that our study is limited by the fact that it is based solely on Pubmed and not on all other search engines that may contain articles on CPOE, which may underestimate the number of publications in the field. Secondly, the tool used to perform this query is based on the categories and indexations of PubMed, which may not be indicated or may not appear in some articles. Then, one limitation of the article is the absence of subsequent examination of the included publications. As a result, our observation of a decrease in original articles or editorials/perspectives/letters published after 2009 lacks precision. This type of study aims to provide a comprehensive overview of the subject and pave the way for further investigations. One perspective that could be undertaken is to study trends in publication in the literature in the field of medical informatics and prescription and/or decision support tools. This would allow us to know if there is another area of interest that has taken over the development of CPOE.
Conclusion
In conclusion, we can observe that research concerning CPOE is uneven across countries. The disciplines with the highest publication rates are those with the most interest in CPOE, such as pharmacy and pediatrics. Possible reasons for the decline of publication trends related to CPOE after 2009 include the emergence of digital health tools beyond CPOE, as well as healthcare professionals experiencing fatigue with the alert functions of the current system. Moreover, changes in the research and development sector may have contributed to the decrease in scientific publications. Future research should focus on analyzing publication trends in the field of medical informatics and decision-making tools to identify other areas of interest that may have surpassed the development of CPOE.
Author contributions
All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Rodríguez-Monguió R, Otero MJ, Rovira J. Assessing the economic impact of adverse drug effects. Pharmacoeconomics. (2003) 21(9):623–50. doi: 10.2165/00019053-200321090-00002
2. Gyllensten H, Jönsson AK, Rehnberg C, Carlsten A. How are the costs of drug-related morbidity measured?: a systematic literature review. Drug Saf. (2012) 35(3):207–19. doi: 10.2165/11597090-000000000-00000
3. Institute of Medicine (US) Committee on Quality of Health Care in America. Crossing the quality chasm: A new health system for the 21st century. Washington (DC): National Academies Press (US) (2001). Available at: http://www.ncbi.nlm.nih.gov/books/NBK222274/ (cited 2023 Feb 24).
4. Siedlecki C, Griffon N, Kerdelhué G. Thèmes et tendances des publications en médecine générale dans PubMed. Rev Francoph Médecine Générale. (2017) 130:70–1.
5. Gehanno JF, Gehanno B, Schuers M, Grosjean J, Rollin L. Analysis of publication trends in childhood obesity research in PubMed since 1945. Child Obes Print. (2019) 15(4):227–36. doi: 10.1089/chi.2018.0276
6. Chien SC, Chen YL, Chien CH, Chin YP, Yoon CH, Chen CY, et al. Alerts in clinical decision support systems (CDSS): a bibliometric review and content analysis. Healthc Basel Switz. (2022) 10(4):601. doi: 10.3390/healthcare10040601
7. Hackl WO, Ganslandt T. New problems—new solutions: a never ending story. Findings from the clinical information systems perspective for 2015. Yearb Med Inform. (2016) 25(1):146–51. doi: 10.15265/IY-2016-054
8. Huang HC, Wang CH, Chen PC, Lee YD. Bibliometric analysis of medication errors and adverse drug events studies. J Patient Saf. (2019) 15(2):128–34. doi: 10.1097/PTS.0000000000000205
9. Darmoni SJ, Névéol A, Renard JM, Gehanno JF, Soualmia LF, Dahamna B, et al. A MEDLINE categorization algorithm. BMC Med Inform Decis Mak. (2006) 6:7. doi: 10.1186/1472-6947-6-7
10. Thirion B, Darmoni SJ. Simplified access to MeSH tree structures on CISMeF. Bull Med Libr Assoc. (1999) 87(4):480–1. PMID: 1055003510550035
11. Nash-Stewart CE, Kruesi LM, Del Mar CB. Does Bradford's law of scattering predict the size of the literature in cochrane reviews? J Med Libr Assoc JMLA. (2012) 100(2):135–8. doi: 10.3163/1536-5050.100.2.013
12. Ampe E. La pharmacie clinique : un développement récent de l’activité des pharmaciens pour une prise en charge otpimisée des patients du point de vue médicamenteux. Brussels, Belgium: Louvain Medical (2006).
13. Jackson T, Nissen L, Jessup R. Clinical pharmacy in Australia: transforming patient care in a rapidly evolving healthcare system. Res Social Adm Pharm. (2016) 12(numéro 2):285–9.
14. Orenstein EW, Kandaswamy S, Muthu N, Chaparro JD, Hagedorn PA, Dziorny AC, et al. Alert burden in pediatric hospitals: a cross-sectional analysis of six academic pediatric health systems using novel metrics. J Am Med Inform Assoc JAMIA. (2021) 28(12):2654–60. doi: 10.1093/jamia/ocab179
Keywords: bibliometric, bibliometric analysis, CPOE (computerized physician order entry), CPOE (computerized prescriber order entry), medical order entry systems
Citation: Gosselin L, Leguillon R, Rollin L, Lejeune E, Darmoni SJ and Grosjean J (2023) Trends in computerized provider order entry: 20-year bibliometric overview. Front. Digit. Health 5:1217694. doi: 10.3389/fdgth.2023.1217694
Received: 5 May 2023; Accepted: 28 June 2023;
Published: 11 July 2023.
Edited by:
Daniel B. Hier, Missouri University of Science and Technology, United StatesReviewed by:
Xia Jing, Clemson University, United StatesNahid Tavakoli, Isfahan University of Medical Sciences, Iran
© 2023 Gosselin, Leguillon, Rollin, Lejeune, Darmoni and Grosjean. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Laura Gosselin bGF1cmEtZ29zc2VsaW5AaG90bWFpbC5mcg==