 Dieter Hayn1,2*
Dieter Hayn1,2* Mahdi Sareban2,3
Mahdi Sareban2,3 Stefan Höfer4Fabian Wiesmüller1,2
Stefan Höfer4Fabian Wiesmüller1,2 Karl Mayr5Norbert Mürzl6Michael Porodko6Christoph Puelacher7Lisa-Marie Moser7Marco Philippi8Heimo Traninger9Josef Niebauer2,3
Karl Mayr5Norbert Mürzl6Michael Porodko6Christoph Puelacher7Lisa-Marie Moser7Marco Philippi8Heimo Traninger9Josef Niebauer2,3
- 1Center for Health & Bioresources, AIT Austrian Institute of Technology GmbH, Graz, Austria
- 2Ludwig Boltzmann Institute for Digital Health and Prevention, Salzburg, Austria
- 3University Institute of Sports Medicine, Prevention and Rehabilitation, Paracelsus Medical University, Salzburg, Austria
- 4Department of Psychiatry II, Medizinische Universität Innsbruck, Innsbruck, Austria
- 5CARDIOMED Kardiologisches Rehabilitationszentrum GmbH, Linz, Austria
- 6Institut für Präventiv- und Rehabilitationsmedizin, Cardio Vital Wels, Wels, Austria
- 7Reha Innsbruck, REHAmed-tirol GmbH, Innsbruck, Austria
- 8MedReha GmbH, Feldkirch, Austria
- 9ZARG Zentrum für ambulante Rehabilitation GmbH, Graz, Austria
Introduction: Cardiovascular diseases are the leading cause of death worldwide and are partly caused by modifiable risk factors. Cardiac rehabilitation addresses several of these modifiable risk factors, such as physical inactivity and reduced exercise capacity. However, despite its proven short-term merits, long-term adherence to healthy lifestyle changes is disappointing. With regards to exercise training, it has been shown that rehabilitation supplemented by a) home-based exercise training and b) supportive digital tools can improve adherence.
Methods: In our multi-center study (ClincalTrials.gov Identifier: NCT04458727), we analyzed the effect of supportive digital tools like digital diaries and/or wearables such as smart watches, activity trackers, etc. on exercise capacity during cardiac rehabilitation. Patients after completion of phase III out-patient cardiac rehabilitation, which included a 3 to 6-months lasting home-training phase, were recruited in five cardiac rehabilitation centers in Austria. Retrospective rehabilitation data were analyzed, and additional data were generated via patient questionnaires.
Results: 107 patients who did not use supportive tools and 50 patients using supportive tools were recruited. Already prior to phase III rehabilitation, patients with supportive tools showed higher exercise capacity (Pmax = 186 ± 53 W) as compared to patients without supportive tools (142 ± 41 W, p < 0.001). Both groups improved their Pmax, significantly during phase III rehabilitation, and despite higher baseline Pmax of patients with supportive tools their Pmax improved significantly more (ΔPmax = 19 ± 18 W) than patients without supportive tools (ΔPmax = 9 ± 17 W, p < 0.005). However, after adjusting for baseline differences, the difference in ΔPmax did no longer reach statistical significance.
Discussion: Therefore, our data did not support the hypothesis that the additional use of digital tools like digital diaries and/or wearables during home training leads to further improvement in Pmax during and after phase III cardiac rehabilitation. Further studies with larger sample size, follow-up examinations and a randomized, controlled design are required to assess merits of digital interventions during cardiac rehabilitation.
Introduction
Cardiovascular diseases (CVD) are the leading cause of death worldwide (1) with substantial micro- as well as macro-economic burden (1–3). Several modifiable risk factors contribute to the pathogenesis of CVD which can be addressed during cardiac rehabilitation (CR), i.e., a comprehensive multi-phased secondary prevention framework which has proven to reduce mortality in CVD patients (4) as well as lower its economic burden (5). Increasing physical activity (PA) and exercise capacity are one of the main goals during CR because they have favorable effects on multiple cardiovascular risk factors (6) and have shown to be strongly associated with lower mortality in CVD patients (7, 8). As a result, international secondary prevention guidelines advocate PA recommendations, i.e.,150–300 min of moderate intensity or 75–150 min of vigorous exercise each week (9), with higher exercise intensity and duration being associated with greater benefit (10). Notably, the greatest benefits to health and quality of life are likely to be achieved by increases in PA in otherwise sedentary subjects (7, 11), commonly defined as those with <14 METs h/week energy expenditure.
In order to achieve sustainable behavior change, enrollment in CR phase II should take place as soon as possible once a patient meets one of the well-established indications (12). CR phase II can be carried out as in- (IN-II) or outpatient (OUT-II) CR, depending on the severity of the diseases, patients’ preferences, and the availability of an outpatient CR facility in the vicinity. Following IN-II as well as OUT-II, an outpatient phase III (OUT-III) enrollment is offered with weekly visits at the outpatient CR facility to maintain short-term lifestyle changes.
Prior to and after OUT-III, detailed examinations are performed in the CR facilities, and include, among others, questionnaires, anthropometric assessment, blood tests, resting and exercise ECG.
Despite its proven merits, sustainable behavior change, i.e., long-term preservation of recommended PA volume and exercise capacity following completion of CR phase II, is disappointing (13, 14). This gap is addressed in recent recommendations (9), suggesting considering the use of consumer-based wearable activity trackers to increase PA participation and long-term adherence to healthy behaviors. Especially during OUT-III, supportive tools like digital training diaries and/or commercially available wearable devices might be of help for patients and clinicians to support patients during their home-training phase.
During CR, digital tools can be applied in numerous ways. Patients can use training diaries to document training sessions, receive reminders, etc., monitor vital parameters like heart rate during training sessions, monitor physical activity with activity trackers, or engage in comprehensive tele-rehabilitation programs. In the past decade, various studies and review articles concerning the effect of tele-rehabilitation and supportive tools during tele-rehabilitation on cardiac patients have been published. Recently, five review articles (15–19) analyzed 81 different original articles (four original articles were analyzed by four of the five reviews, four articles by three reviews, and 16 articles by two of the reviews). Tele-rehabilitation proofed to be feasible and acceptable, and it showed similar or superior effectiveness in terms of exercise capacity, physical activity, and/or adherence to CR. While there seem to be various benefits of tele-rehabilitation as compared to regular CR, tele-rehabilitation was found to bear only a very low risk for adverse events (20). Finally, tele-rehabilitation was found to be as cost-effective as center-based CR (21).
The studies described above applied digital support to patients in various settings and phases of CR. Only one study (22) assessed in these reviews included Austrian data. However, this study described a field experiment with 29 male patients in a specific test setting. Although we assume that the use of digital tools has a positive impact on cardiac rehabilitation in Austria, no evidence is available so far.
In our multi-center study, we analyzed the effect of digital tools on exercise capacity during OUT-III cardiac rehabilitation including a home training phase in Austria.
Materials and methods
Study design
We assessed the effect of multi-modal supportive tools on exercise capacity during OUT-III CR including home training in the multi-centric EPICURE study that was performed in five outpatient CR centers in Austria. In general, Austrian rehabilitation centers adhere to the latest national and international recommendations for center- and home-based exercise training (12). These recommendations emphasize the importance of personalized exercise training prescription after performing initial medical evaluations including exercise testing and risk assessment. The study protocol was approved by the ethics committee of Upper Austria (vote nr. 1165/2019) and registered at ClincalTrials.gov (Identifier: NCT04458727).
The primary objective was to investigate the effect of the patients’ preference-based choice of supportive tools (phone-based assessments, digital training diaries with/without adherence monitoring and with/without wearables) on the change of maximum power during ergometry pre and post CR phase OUT-III including home training. Secondary objectives included subgroup analyses concerning the effect of each of the supportive tools separately.
Since patients were recruited retrospectively, i.e., after OUT-III, blinding or randomization was not feasible.
Recruitment
Consecutive patients performing their examination post OUT-III including home training in one of the CR centers were screened for in- and exclusion criteria. In case of eligibility, willingness to participate in the study and after written informed consent was obtained, patients were included in the study and available data from the beginning of CR until inclusion into the study were analyzed.
The CR timeline, the time period analyzed for the primary hypothesis, and the timepoint for inclusion in the EPICURE study are illustrated in Figure 1.
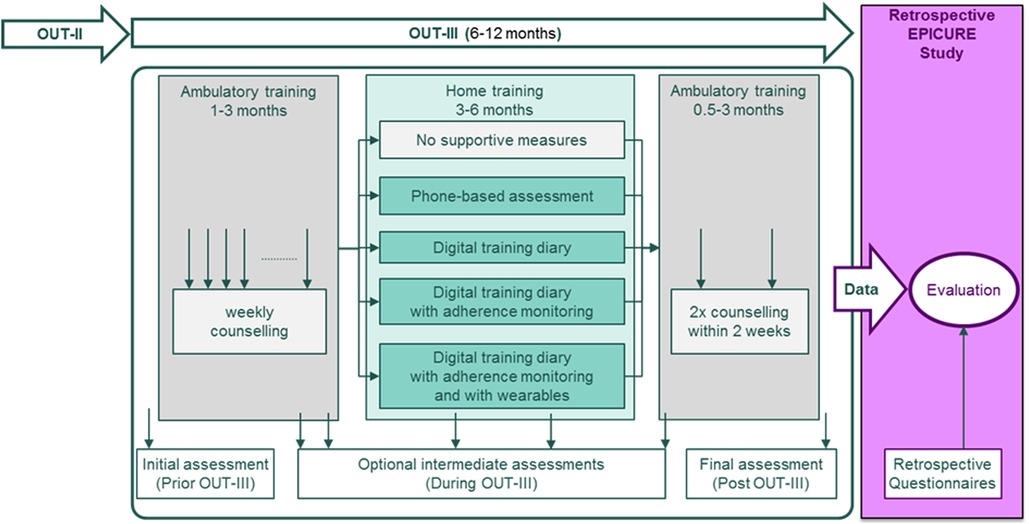
Figure 1. Illustration of the rehabilitation OUT-III phase and the timeline of the EPICURE study.
Inclusion criteria:
• Age ≥ 18 years.
• Participation in a phase III rehabilitation at one of the study sites.
• Documented cardiovascular disease.
• The patient is able to give consent to participate in the study.
• Written informed consent to participate in the study.
Exclusion criteria:
• none.
Each patient was assigned to one of two groups, based on their respective answers in the questionnaires:
• Patients who used at least one of the following supportive tools during their home training phase
○ Regular phone-based assessment.
○ Digital training diary with or without adherence monitoring and with or without wearables.
• Patients who used none of the above-mentioned supportive tools.
Data acquisition
Two types of data were recorded:
• Retrospective, pre-existing data as collected during CR, including demographic and clinical data, and quality of life according to MacNew-27 (23).
• Questionnaires concerning CR that were filled out by the patient after signing informed consent.
Statistical analysis
We analyzed the maximum workload Pmax [W] as achieved by patients during the exercise stress test at their regular assessments in the study centers. The difference ΔPmax [W] between Pmax at the end of OUT-III minus Pmax at the beginning of OUT-III was determined. If no data from the assessment prior to OUT-III was available, data from the assessment post phase II was taken instead. Normal distribution of the data was tested by using the Shapiro-Wilk test. A student t-test was applied to test for global differences between pre- to post CR (dependent t-test) and for differences between the groups (independent t-test). A value of alpha <0.05 was considered significant. Additionally, we applied ANCOVA statistics to correct on those variables that significantly differed in the two groups.
Primary hypothesis and sub-group analyses
The primary hypothesis was that ΔPmax [W] of patients who used any of the above-mentioned supportive tools was significantly higher (p < 0.05) as compared to ΔPmax [W] of patients without supportive tools.
In addition, we analyzed differences between sub-groups of patients with supportive tools to better understand the influence of regular phone-based assessments, digital training diaries alone and diaries in combination with adherence monitoring and wearables, i.e., heart rate monitoring during training and activity trackers. Therefore, we defined two sub-groups (A and B) per supportive tool and the group C without supportive tools:
A. Patients with digital training diary and with the respective supportive tool.
B. Patients with digital training diary and without the respective supportive tool.
C. Patients without supportive tools.
We compared patients with digital training diary and the respective supportive tool (group A) to (a) patients without a supportive tool (group C) and (b) all patients not included in group A (i.e., groups B + C). Therefore, ANCOVA was applied, taking into account all significantly different baseline parameters for the respective group assignment.
Power calculation
The effect size of 0.46 was derived from mean power and standard deviation at the end of a standard CR program (24). Assuming a minimal clinically important difference of 25 W (25), an α-error probability of 0.05, and a power (1-β error probability) of 0.8, the total sample size for the 2 groups analyzed by an unpaired t-test was determined as 150 participants, i.e., 75 per group.
Results
Patient characteristics
Details concerning patient characteristics of all recruited patients as recorded prior to OUT-III are presented in Table 1. Approximately two third of patients reported to have used supportive tools, as specified above, during their home training. This ratio was similar for men and women. Patients using supportive tools were significantly younger, fitter (in terms of Pmax), had a lower BMI and body weight, and reported a higher quality of life in all 4 aspects of the MacNew questionnaire prior to OUT-III.
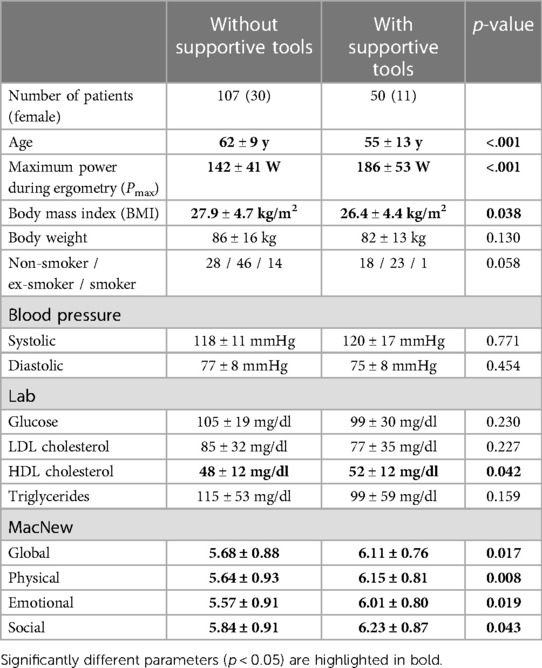
Table 1. Patient characteristics.
Exercise capacity pre and post OUT-III
Table 2 summarizes all exercise capacity data achieved pre and post OUT-III for patients with and without supportive tools, including differences and p-values.
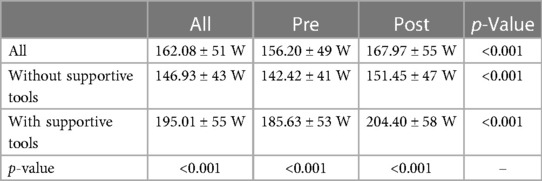
Table 2. Maximum power during ergometry (Pmax) pre and post OUT-III.
Figure 2 illustrates the maximum power achieved during ergometry pre and post OUT-III for both study groups. Pmax was higher post OUT-III as compared to pre OUT-III in patients with supportive tools, without supportive tools and for the whole study population. Pmax was higher in patients using supportive tools as compared to patients without supportive tools, prior to and post OUT-III and when combining results pre and post OUT-III.
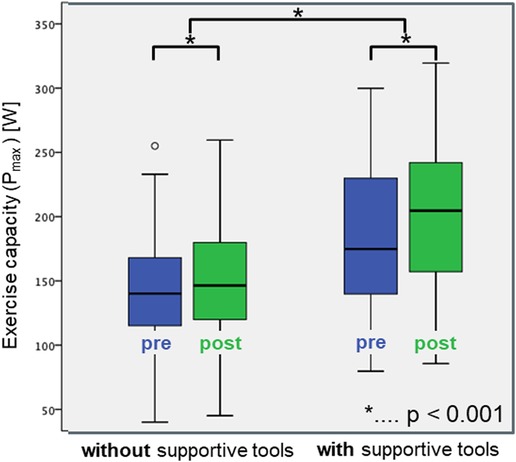
Figure 2. Boxplots of the maximum power during ergometry pre (blue) and post (green) OUT-III for patients with and without supportive measures.
Although patients with supportive tools already showed a higher exercise capacity prior to OUT-III, Pmax improved significantly more (19 ± 18 W) during OUT-III as compared to patients without supportive tools (9 ± 17 W, p < 0.005).
Five variables differed significantly between the two groups pre OUT-III: age, Pmax, HDL cholesterol, quality of life according to MacNew, and BMI. When adjusting for the difference of the variables between the two groups using analysis of covariance according to ANCOVA, the difference in ΔPmax between the groups was reduced to 5 ± 4 W and did no more reach statistical significance (p = 0.184). The change of exercise capacity for both groups with and without ANCOVA correction is illustrated in Figure 3 (results are plotted as mean +/- confidence intervals, since boxplots are not applicable after ANCOVA correction).
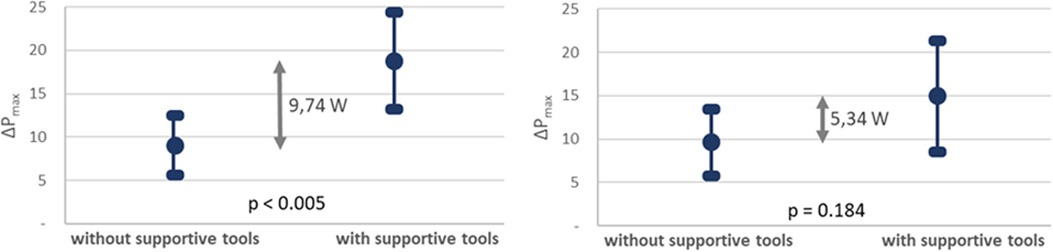
Figure 3. Mean value and confidence interval of the change of maximum power during ergometry pre and post OUT-III (ΔPmax) for patients with and without supportive measures without (left) and with (right) ANCOVA correction on co-variates.
Sub-group analyses
Details concerning sub-group analyses applied to the group with supportive tools are summarized in Table 3. None (0%) of the patients was monitored by regular phone-based assessments, while all 50 patients did use a digital training diary. 17 out of those 50 patients (34%) reported to have had adherence monitoring during home training. 46 out of 50 patients (92%) with a digital training diary were also using wearables. All these 46 patients monitored their heart rate during training. 41 out of 50 (82%) patients additionally used an activity tracker to monitor physical activity.
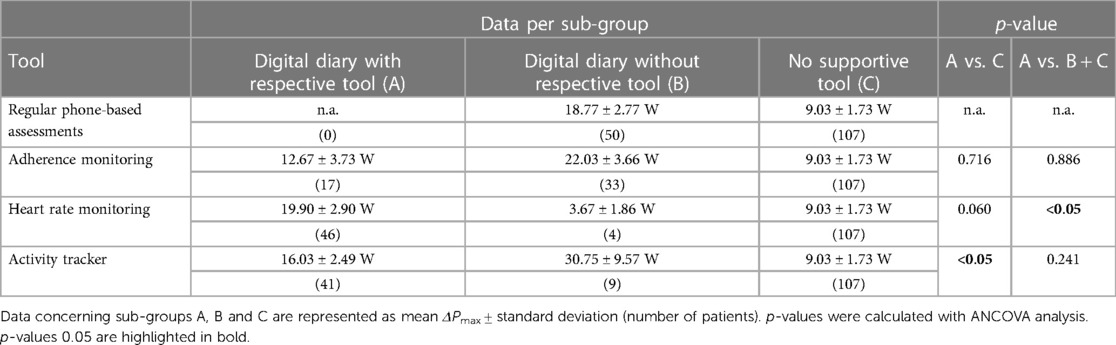
Table 3. Subgroup analysis including number of patients per subgroup A, B and C, p-value between subgroups for the change ΔPmax in the maximum power during ergometry (Pmax) at the end of OUT-III minus Pmax at the beginning of OUT-III.
We compared patients with digital training diaries and the respective supportive tool (group A) to (a) patients without a supportive tool (group C) and (b) all patients not included in group A (i.e., groups B + C). Adherence monitoring did not have a significant influence on ΔPmax in neither of these analyses.
A significant difference between patients using a digital training diary in combination with heart rate monitoring during training compared to all other patients (A vs. B + C, p < 0.05) was found. We also observed a trend in ΔPmax between patients with diary and heart rate monitoring as compared to those without digital training diaries, however, the difference did not reach statistical significance (A vs. C, p = 0.060).
ΔPmax significantly differed between patients with digital training diaries and activity tracker as compared to patients without digital training diaries (A vs. C, p < 0.05). No difference in ΔPmax between patients with digital training diaries and activity tracker as compared to all other patients was found (A vs. B + C, p 0.241).
Discussion
Patients in both groups significantly improved their exercise capacity during OUT-III including home-based training. Supportive tools were more frequently used by younger patients, with higher exercise capacity, lower HDL-cholesterol, lower BMI, and better quality of life prior to OUT-III. Patients who used supportive measures during the home training phase of OUT-III improved their exercise capacity more than patients who did not use any supportive measures. However, when applying ANCOVA to consider significant baseline differences in the study groups, the difference in ΔPmax between the two groups did no longer reach statistical significance.
Subgroup analyses revealed that digital training diaries in combination with heart rate monitoring during training or activity trackers led to significantly better improvement of exercise capacity in some subgroups (see Table 3). However, since in some groups, large variations between individual patients were identified, and since the number of patients in some sub-groups was low, further prospective studies in larger cohorts are indicated to analyse these effects.
Our results are in accordance with previous studies (15–19). However, to the best of our knowledge, the effect of using supportive tools during OUT-III that includes a home-based training phase has not been analysed so far. Our results confirm that OUT-III is effective. Additionally, the use of digital tools has the potential to support sustainable behaviour change and to further improve the exercise capacity of cardiac patients during CR, although our results did not reach statistical significance.
We did not check the use of digital tools but trusted in the patients’ respective answers and we did not consider whether adherence monitoring was really applied or the extent to which patients used supportive tools, which may have led to a rather heterogeneous group with digital tools. These facts need to be kept in mind when interpreting our results.
Although questionnaire data was recorded prospectively, most data in our study were analysed in a retrospective setting based on pre-existing routine-care data, including our primary outcome, i.e., maximum exercise capacity. Additionally, patients were not randomised to the two groups, but they declared within the questionnaire whether they used digital tools or not.
Initially, we planned to identify 50% of patients in the group with and 50% without digital tools. However, since no stratification or randomization was applied, we finally ended up with approx. one third with and two third of patients without digital tools, which reduced the power of our analyses. Therefore, since the number of patients using digital tools was rather low, additional studies with larger sample size may be indicated to confirm our results. To find out more about the effect of supportive tools as compared to the differences in baseline parameters on the training effect, a prospective study may be necessary, where patients are randomized to either a group with or without supportive tools, preferably including stratification on the above-mentioned baseline parameters.
Conclusion
Our results demonstrate an improvement in exercise capacity post OUT-III cardiac rehabilitation, which included a 3 to 6 months home-training phase as compared to pre OUT-III. Data from patients using supportive tools during OUT-III give first indications that an even greater increase in exercise capacity is possible, suggesting that supportive digital tools might help improve and/or maintain physical exercise capacity by supporting sustainable behaviour change.
Data availability statement
The datasets presented in this article are not readily available because based on study protocol, ethics approval and informed consent, we may only give access to the collected data to authorized personnel, as required for analyzing the data. Requests to access the datasets should be directed to DH, dieter.hayn@ait.ac.at.
Ethics statement
The studies involving human participants were reviewed and approved by the Ethics Committee of Upper Austria. The patients/participants provided their written informed consent to participate in this study.
Author contributions
DH had the main responsibility for setting up and conducting the study and for preparing the final manuscript and he contributed to the statistical analyses. MS and JN contributed to the study design, study preparation, and statistical analyses. SH contributed to the study design and performed the analyses. FW contributed to the statistical analyses. KM, NM, MPo, CP, L-MM, MPh, and HT contributed to the study design and conducted the study. All authors discussed the results, supervised the findings and contributed to the article and approved the submitted version.
Funding
The EPICURE study was funded by the Austrian Research Promotion Agency (FFG) under the grant number 865531.
Conflict of interest
Author KM is employed by heartfish GmbH and CARDIOMED Kardiologisches Rehabilitationszentrum GmbH and holds 20 % shares in both companies. Author NM is employed by Cardio Vital Wels. Author CP is employed by Reha Innsbruck, REHAmed-tirol GmbH and holds 100 % shares of the company. Author L-MM is employed by Reha Innsbruck, REHAmed-tirol GmbH. Author MPh is employed by MedReha GmbH and owns 100% shares of the company. Author HT is employed by ZARG Zentrum für ambulante Rehabilitation GmbH and holds 10 % shares of the company.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. Collaborators GDaI. Global burden of 369 diseases and injuries in 204 countries and territories, 1990–2019: a systematic analysis for the global burden of disease study 2019. Lancet. (2020) 396(10258):1204–22. doi: 10.1016/S0140-6736(20)30925-9
2. Jaspers L, Colpani V, Chaker L, van der Lee SJ, Muka T, Imo D, et al. The global impact of non-communicable diseases on households and impoverishment: a systematic review. Eur J Epidemiol. (2015) 30(3):163–88. doi: 10.1007/s10654-014-9983-3
3. Heidenreich PA, Trogdon JG, Khavjou OA, Butler J, Dracup K, Ezekowitz MD, et al. Forecasting the future of cardiovascular disease in the United States: a policy statement from the American Heart Association. Circulation. (2011) 123(8):933–44. doi: 10.1161/CIR.0b013e31820a55f5
4. Anderson L, Thompson DR, Oldridge N, Zwisler AD, Rees K, Martin N, et al. Exercise-based cardiac rehabilitation for coronary heart disease. Cochrane Database Syst Rev. (2016) 1:CD001800. doi: 10.1002/14651858.CD001800.pub3
5. Edwards K, Jones N, Newton J, Foster C, Judge A, Jackson K, et al. The cost-effectiveness of exercise-based cardiac rehabilitation: a systematic review of the characteristics and methodological quality of published literature. Health Econ Rev. (2017) 7(1):37. doi: 10.1186/s13561-017-0173-3
6. Niebauer J, Mayr K, Harpf H, Hofmann P, Müller E, Wonisch M, et al. Long-term effects of outpatient cardiac rehabilitation in Austria: a nationwide registry. Wien Klin Wochenschr. (2014) 126(5-6):148–55. doi: 10.1007/s00508-014-0527-3
7. Stewart RAH, Held C, Hadziosmanovic N, Armstrong PW, Cannon CP, Granger CB, et al. Physical activity and mortality in patients with stable coronary heart disease. J Am Coll Cardiol. (2017) 70(14):1689–700. doi: 10.1016/j.jacc.2017.08.017
8. Lear SA, Hu W, Rangarajan S, Gasevic D, Leong D, Iqbal R, et al. The effect of physical activity on mortality and cardiovascular disease in 130 000 people from 17 high-income, middle-income, and low-income countries: the PURE study. Lancet. (2017) 390(10113):2643–54. doi: 10.1016/S0140-6736(17)31634-3
9. Visseren FLJ, Mach F, Smulders YM, Carballo D, Koskinas KC, Bäck M, et al. 2021 ESC guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. (2021) 42(34):3227–337. doi: 10.1093/eurheartj/ehab484
10. Sattelmair J, Pertman J, Ding EL, Kohl HW, Haskell W, Lee IM. Dose response between physical activity and risk of coronary heart disease: a meta-analysis. Circulation. (2011) 124(7):789–95. doi: 10.1161/CIRCULATIONAHA.110.010710
11. Huber A, Höfer S, Saner H, Oldridge N. A little is better than none: the biggest gain of physical activity in patients with ischemic heart disease. Wien Klin Wochenschr. (2020) 132(23-24):726–35. doi: 10.1007/s00508-020-01767-x
12. Niebauer J, Mayr K, Tschentscher M, Pokan R, Benzer W. Outpatient cardiac rehabilitation: the Austrian model. Eur J Prev Cardiol. (2013) 20(3):468–79. doi: 10.1177/2047487312446137
13. Yu CM, Li LS, Ho HH, Lau CP. Long-term changes in exercise capacity, quality of life, body anthropometry, and lipid profiles after a cardiac rehabilitation program in obese patients with coronary heart disease. Am J Cardiol. (2003) 91(3):321–5. doi: 10.1016/S0002-9149(02)03159-4
14. Lear SA, Spinelli JJ, Linden W, Brozic A, Kiess M, Frohlich JJ, et al. The extensive lifestyle management intervention (ELMI) after cardiac rehabilitation: a 4-year randomized controlled trial. Am Heart J. (2006) 152(2):333–9. doi: 10.1016/j.ahj.2005.12.023
15. Wongvibulsin S, Habeos EE, Huynh PP, Xun H, Shan R, Porosnicu Rodriguez KA, et al. Digital health interventions for cardiac rehabilitation: systematic literature review. J Med Internet Res. (2021) 23(2):e18773. doi: 10.2196/18773
16. Batalik L, Filakova K, Batalikova K, Dosbaba F. Remotely monitored telerehabilitation for cardiac patients: a review of the current situation. World J Clin Cases. (2020) 8(10):1818–31. doi: 10.12998/wjcc.v8.i10.1818
17. Ashur C, Cascino TM, Lewis C, Townsend W, Sen A, Pekmezi D, et al. Do wearable activity trackers increase physical activity among cardiac rehabilitation participants? A SYSTEMATIC REVIEW AND META-ANALYSIS. J Cardiopulm Rehabil Prev. (2021) 41(4):249–56. doi: 10.1097/HCR.0000000000000592
18. Akinosun AS, Polson R, Diaz-Skeete Y, De Kock JH, Carragher L, Leslie S, et al. Digital technology interventions for risk factor modification in patients with cardiovascular disease: systematic review and meta-analysis. JMIR Mhealth Uhealth. (2021) 9(3):e21061. doi: 10.2196/21061
19. Hannan AL, Harders MP, Hing W, Climstein M, Coombes JS, Furness J. Impact of wearable physical activity monitoring devices with exercise prescription or advice in the maintenance phase of cardiac rehabilitation: systematic review and meta-analysis. BMC Sports Sci Med Rehabil. (2019) 11:14. doi: 10.1186/s13102-019-0126-8
20. Stefanakis M, Batalik L, Antoniou V, Pepera G. Safety of home-based cardiac rehabilitation: a systematic review. Heart Lung. (2022) 55:117–26. doi: 10.1016/j.hrtlng.2022.04.016
21. Batalik L, Filakova K, Sladeckova M, Dosbaba F, Su J, Pepera G. The cost-effectiveness of exercise-based cardiac telerehabilitation intervention: a systematic review. Eur J Phys Rehabil Med. (2023) 59(2):248–58. doi: 10.23736/S1973-9087.23.07773-0
22. Vogel J, Auinger A, Riedl R, Kindermann H, Helfert M, Ocenasek H. Digitally enhanced recovery: investigating the use of digital self-tracking for monitoring leisure time physical activity of cardiovascular disease (CVD) patients undergoing cardiac rehabilitation. PLoS One. (2017) 12(10):e0186261. doi: 10.1371/journal.pone.0186261
23. Oldridge N, Guyatt G, Jones N, Crowe J, Singer J, Feeny D, et al. Effects on quality of life with comprehensive rehabilitation after acute myocardial infarction. Am J Cardiol. (1991 May 15) 67(13):1084–9. doi: 10.1016/0002-9149(91)90870-q
24. Tschentscher M, Eichinger J, Egger A, Droese S, Schönfelder M, Niebauer J. High-intensity interval training is not superior to other forms of endurance training during cardiac rehabilitation. Eur J Prev Cardiol. (2016) 23(1):14–20. doi: 10.1177/2047487314560100
Keywords: mHealth, telehealth, cardiac rehabilitation, wearable, adherence
Citation: Hayn D, Sareban M, Höfer S, Wiesmüller F, Mayr K, Mürzl N, Porodko M, Puelacher C, Moser L-M, Philippi M, Traninger H and Niebauer J (2023) Effect of digital tools in outpatient cardiac rehabilitation including home training—results of the EPICURE study. Front. Digit. Health 5:1150444. doi: 10.3389/fdgth.2023.1150444
Received: 24 January 2023; Accepted: 3 July 2023;
Published: 14 July 2023.
Edited by:
Tom Foley, Newcastle University, United KingdomReviewed by:
Ladislav Batalik, University Hospital Brno, CzechiaEgidio Traversi, Scientific Clinical Institute Maugeri (ICS Maugeri), Italy
© 2023 Hayn, Sareban, Höfer, Wiesmüller, Mayr, Mürzl, Porodko, Puelacher, Moser, Philippi, Traninger and Niebauer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dieter Hayn ZGlldGVyLmhheW5AYWl0LmFjLmF0