 Victòria Brugada-Ramentol
Victòria Brugada-Ramentol Amir Bozorgzadeh
Amir Bozorgzadeh Hossein Jalali
Hossein Jalali- Virtuleap, Lisbon, Portugal
Cognitive training systems aim to improve specific domains or global cognition by engaging users in cognitively demanding tasks. While screen-based applications can improve performance in the trained cognitive abilities, they are often criticized for their poor transferability to activities of daily living. These systems, however, exclude the user's body and motor skills, which invariably serves to restrict the user experience. Immersive Virtual Reality (IVR) systems, in contrast, present the user with body-related information, such as proprioceptive and visuomotor information, allowing for an immersive and embodied experience of the environment. This feature renders VR a very appealing tool for cognitive training and neurorehabilitation applications. We present Enhance VR, an IVR-based cognitive training and monitoring application that offers short daily cognitive workouts. The games are designed to train and monitor specific cognitive domains such as memory, task flexibility, information processing, orientation, attention, problem-solving, and motor control. The aim is to test whether cognitively demanding tasks, presented in an IVR setting, provide a naturalistic system to train and monitor cognitive capabilities.
1. Introduction
Cognitive decline, the gradual deterioration of cognitive abilities and functioning, progresses in parallel with age and becomes more pronounced in populations at risk of neurodegenerative diseases (Figure 1A). The deterioration of cognitive abilities has a direct influence on the execution of activities of daily living (ADLs) and negatively affects autonomy and wellbeing. As life expectancy continues to increase, the number of the senior population and, consequently, the prevalence of cognitive impairment is expected to increase (WHO Europe, n.d.). A combination of healthy diet, moderate exercise, and cognitive stimulation have been proposed as strategies to attempt to slow down the progression of cognitive decline (1–3). Among these, cognitive training systems aim to maintain an effective cognitive function through the structured practice of specific cognitive domains. Furthermore, when presented in a computerized form, the exercise difficulty can be adapted to the performance of the individual, which presents an advantage over pen-and-paper formats (4).
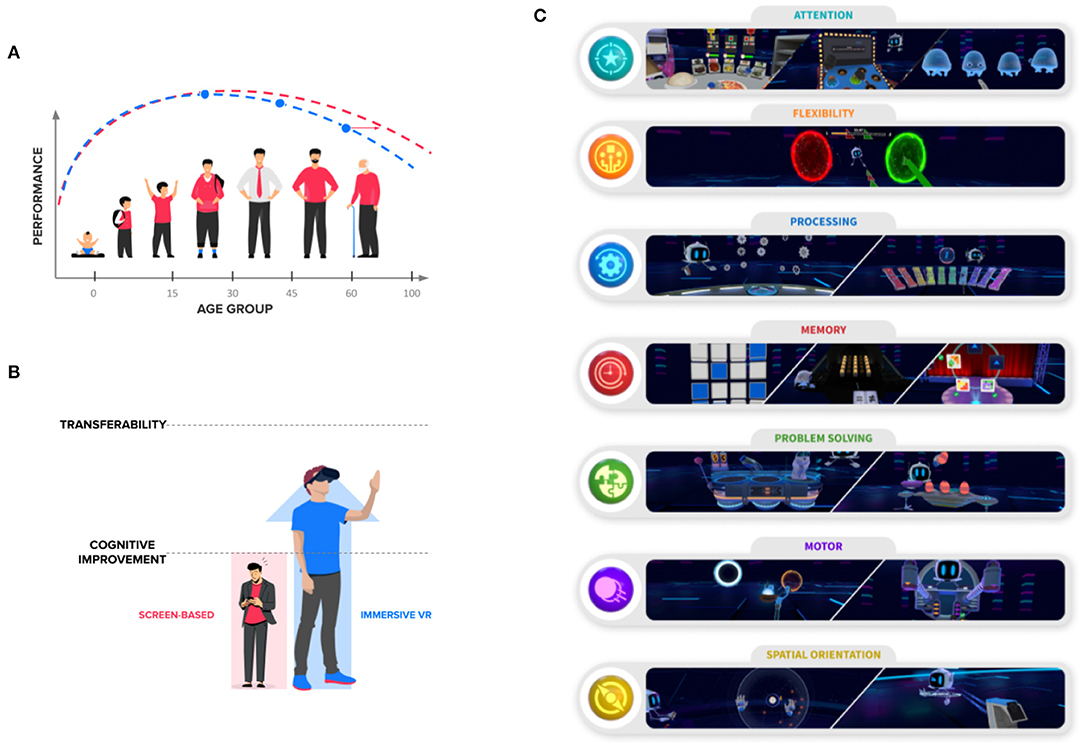
Figure 1. Enhance VR offers a library of cognitive exercises in virtual reality. (A) Cognitive abilities change across the lifespan of an individual. Cognitive training solutions, together with physical exercise and a healthy balanced diet, have shown potential improvement in the cognitive abilities of elderly. (B) Screen-based cognitive training solutions have shown potential improvement in the trained cognitive abilities, but the effects on global cognitive functioning and activities of daily living are still to be determined. Virtual reality systems present the user with an embodied experience of cognitive exercises, which can potentially increase the possibility of transfer of benefits. (C) The Enhance VR exercises span across seven cognitive categories (and their respective subcategories). Namely, attention, cognitive flexibility, information processing, memory, problem-solving, motor control, and spatial orientation. The latter being inherent to IVR environments.
Thus, computerized cognitive training (CCT) could potentially act as a non-pharmacological intervention to maintain cognitive functioning across the lifespan of healthy and cognitively impaired individuals. CCT has been shown to reduce cognitive decline in healthy aging (5), but with no clear effectiveness in delaying difficulties in instrumental ADLs. CCT programs have shown an improvement in trained cognitive abilities (i.e., memory, reasoning, or speed-of-processing) (6), which was maintained for 5 (7) or even 10 years (8). A meta-analysis found a small and significant effect on cognitive function in healthy older adults (9). Overall, CCT has shown promising, but heterogeneous results in global cognitive functioning (10). However, screen-based CCT solutions have failed to show transfer to untrained cognitive categories and tasks and iADLs (6, 11), thus failing to show transfer of benefits. Furthermore, computer-based interventions showed improvements in cognition and non-cognitive measures (e.g., mood), but failed to improve ADLs in people with dementia (12). A 12-week program showed improved capacities in early-stage Alzheimer's disease (AD), without positive effects on ADLs (13).
The lack of ecological validity in screen-based CCT could, in part, explain why these systems do not result in a transfer of benefits to ADLs and general cognition. While screen-based systems fail to provide body-related sensory information (e.g., proprioception), virtual reality (VR) environments provide it innately through multisensory embodied experiences (14). VR environments yield ecologically valid environment scenarios with precise control over the experimental variables (15, 16). VR has shown to be potentially relevant for cognitive training in the elderly population, as a result of many different features, such as the flexibility of the environments and the possibility to gather rich data, as a result of increased immersion (17). Thus, cognitive training in VR can potentially improve cognitive functioning in healthy and at-risk older adults and promote the transfer of benefits (Figure 1B).
2. Virtual Reality Environments as a Cognitive Training and Monitoring Tool
2.1. Advantages of Using VR Environments
VR scenarios offer many advantages over screen-based cognitive training methodologies. Traditional methodologies have to trade external validity (i.e., how the task accurately represents the measure in real life scenarios) and the internal validity of conducting the tasks in a controlled laboratory setting with controlled variables (18). VR, on the other hand, offer realistic scenarios with a high degree of control over desirable experimental variables (15), such as the stimuli, the presence of distractors, among others. Additional advantages of VR systems include the possibility to create situations that are adapted to the individuals needs or that are impossible to recreate in real life scenarios and collect precise measurements of physical movements, while sourcing large amounts of behavioral data (18).
Moreover, immersive VR (IVR) systems that are displayed through a head-mounted display with embedded head-tracking, which update the environment according to the movement of the participant, allow for a naturalistic interaction with the environment. In these scenarios, the behavior of the environment matches the expected physical and motor consequences of the action of the participant. This is also referred to as the plausibility illusion. Furthermore, IVR environments engage the sensorimotor system enhancing the illusion of embodiment over a virtual body or body part (19, 20). By providing immersive experiences of the scenarios, virtual environments provide the feeling that the virtual world is the real world and provide the feeling of actually “being” in the virtual environment (i.e., placement illusion). The feeling of presence in virtual environment has shown to increase motivation for learning and attention to the task (21) and it is dependent both on hardware and software (22). These three illusions contribute to the immersive experience of the environment (23).
Sensorimotor contingencies are, thus, important for the immersion. VR systems are particularly interesting for this matter, as they allow for the integration of proprioceptive, visual, and motor information (14). Ultimately, VR scenarios provide a high degree of realism that elicit naturalistic behaviors from participants (24). Together with the sense of presence and immersion in the virtual environment, the naturalistic interaction with the environment provides a higher degree of ecological validity than current screen-based or pen-and-paper solutions. As a result, VR systems become interesting tools for training and rehabilitation of cognitive functions in distinct populations (25).
2.2. Cognitive Training and Rehabilitation in VR
VR enables a stronger sensory immersion that promotes higher cognitive processing and learning and has found positive impacts on learning outcomes when analyzing the effects of VR-based games and simulations (21, 26, 27). In addition, VR enhances the learning and the application of information compared to screen-based systems (28). VR is increasingly being used in the field of cognitive rehabilitation, such as rehabilitation of post-stroke patients (25) and indicated potential applications for Parkinson's disease (29). Training in wayfinding paradigms in VR has shown improvement in the untrained memory category (30). Lastly, VR has proven itself useful in the study of postural instability in AD patients (31).
Exercises in semi-immersive VR representing a virtual supermarket mixed with physical activity (such as using a treadmill) has been proposed as an alternative that could ultimately translate to improvements in daily life activities (32). Evidence using a VR cognitive training system in patients with mild cognitive impairment (MCI), a prodromal state to AD, shows moderate effects in global cognitive functioning (33). Stroke rehabilitation using an ecological valid simulating ADLs scenario can have a positive impact in post-stroke individuals, showing larger improvements than conventional methods (34). Individuals with MCI and dementia have reported a preference for VR formats over the pen-and-paper versions, thus, suggesting the potential to increase engagement and adherence to non-pharmacological interventions (35). A VR cognitive training system, representing ADLs showed positive improvement in executing function and visual memory in elderly, and general cognitive (36). A program designed to train memory, attention, and executive function resulted in improvements in the healthy and MCI individuals (37).
The advantages of IVR are not only restricted to cognitive training, but also to provide immersive scenarios for cognitive assessment (38). As a result of the naturalistic interaction and the realistic scenarios, VR cognitive assessment offers the opportunity to accurately measure the cognitive performance of the individual.
3. Enhance VR, a Cognitive Training and Monitoring Tool in Virtual Reality
Enhance VR is a commercially available app consisting of a library of cognitive exercises (hereafter, games) developed by Virtuleap (Virtuleap, United States, virtuleap.com). The Enhance VR system takes advantage of the multisensory experience of immersive VR environments to train and monitor specific cognitive categories (i.e., memory, attention, task flexibility, information processing, orientation, and problem-solving) and motor control (Figure 1C).
The Enhance VR app is designed to be played regularly in the form of short workouts. Each workout is composed of three randomly chosen games. The mechanics of each game is motivated by the mechanics of validated neuropsychological principles. Every game stems from the collaboration between scientists and game designers to ensure that the mechanics of each test are maintained, while the experience is a gamified and engaging representation of the neuropsychological validated tests (Table 1). Every game starts with a benchmark session that aims to find the current level of the participant's performance. From there on, every session starts at the level where the user left off. The difficulty of the Enhance VR app is game dependent and controlled by adjusting the relevant parameters for each exercise. The Enhance VR is compatible with a wide range of commercially available headsets (https://virtuleap.com/download/).
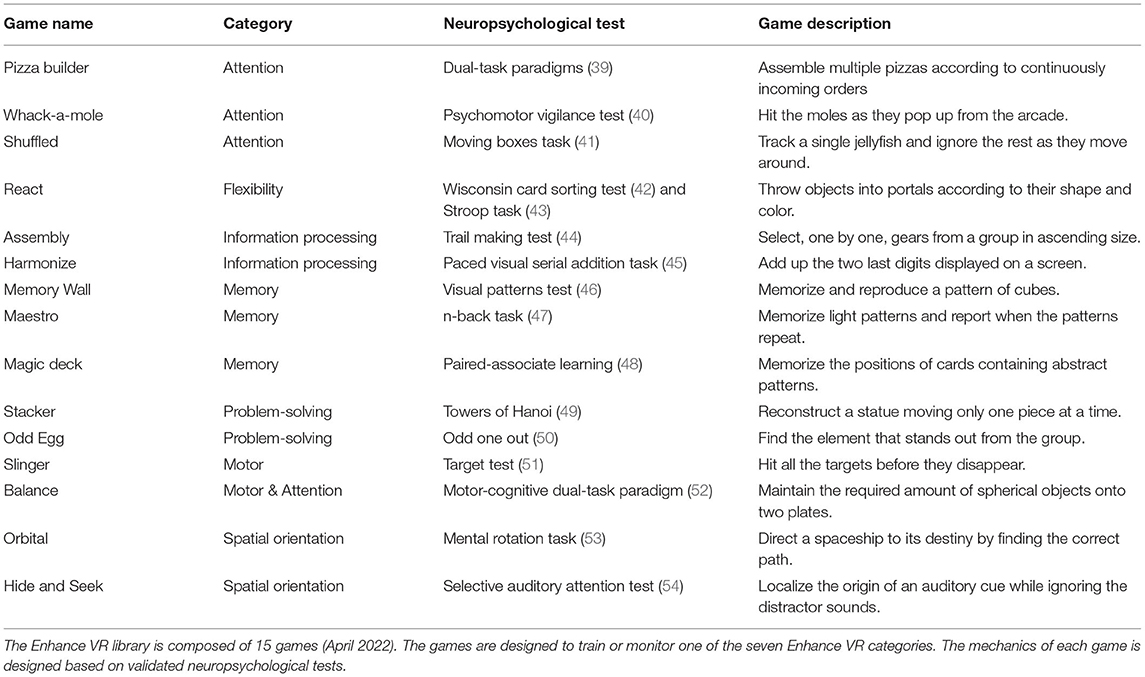
Table 1. Enhance VR game descriptions.
Individual progression is tracked by the Enhance VR Performance Index (EPI), calculated as an aggregate of weighted performance across all cognitive categories in addition to scores for each game, the main cognitive categories, and subcategories scores. The app collects data on self-reported mood and sleeping hours at the start of each workout. Most importantly, there are also game-play patterns that can be obtained from the collection of behavioral data obtained by game-specific events, ultimately allowing the Enhance VR system to calculate reaction times, accuracy, and other behavioral variables.
4. Discussion
With the extension of life expectancy and the aging of the population, the numbers of the elderly population affected with cognitive impairment and loss of autonomy are expected to increase. The number of older adults affected by AD is projected to reach 1.6 billion globally by 2050 (55). It is, therefore, crucial to develop and implement strategies that extend the autonomy and independence of individuals at risk of cognitive decline. Pharmacological interventions have yet to be proven fully useful in helping arrest cognitive and functional decline in those suffering from neurodegenerative diseases. Among potential non-pharmacological interventions, cognitive training presents an opportunity to extend the individual's autonomy and independence (2, 56).
Exposure to a multi-domain active video game itself has been shown to result in a transfer of benefits between tasks (57), which was maintained up to a six-month follow-up period. Thus, gaming environments are a promising tool for the transfer of benefits (58). Training in game-like IVR scenarios has been proposed as a means to increase engagement and motivation in neurorehabilitation (59). Furthermore, immersive VR scenarios offer an ecologically valid environment that can potentially improve global cognitive functions and have positive effects on untrained cognitive abilities. The Enhance VR app takes advantage of the immersive and ecological validity of VR environments to provide a structured and controlled setting for cognitive training. The Enhance VR app can be considered a cognitive training system that offers mentally challenging exercises that aim to train specific cognitive skills presented in a structured manner and extracts behavioral measures of cognitive fitness (60). The Enhance VR app has the potential to enable strong presence and high placement and plausibility illusion, which increases the ecological validity of its environment (61).
To this day, few studies have used IVR environments for cognitive training in healthy elderly (17, 62) or MCI (63) populations. Recent studies point toward positive attitudes displayed by the elderly population in the use of VR environments (64). Further, studies have shown promising results regarding the acceptability and usability in elderly individuals with subjective cognitive impairment and MCI (65) and patients with mild dementia (66), overall suggesting that structured and controlled environments for cognitive training pose a promising tool for elderly at risk of cognitive decline. We therefore propose that exposure to cognitively demanding, physically engaging, and sensory-rich immersive and gamified exercises, such as the ones offered through Enhance VR games, can potentially increase the transfer of benefits to iADLs and global cognitive functioning in populations at risk of cognitive decline.
IVR systems present a unique opportunity to collect potentially ecologically valid data (15) and cognitive assessment systems have shown to be useful in the assessment of cognitive functions (38). Therefore, the prolonged and regular engagement with the Enhance VR app enables the collection of longitudinal data that represents a naturalistic scenario. Thus, the Enhance VR app could also act as a cognitive monitoring tool. VR adaptations of the test have proven useful in the assessment of memory functions (67).
The design of each individual Enhance VR game can be compared to other workflows proposed for the design of cognitive assessment exercises (68). Whenever the need for a specific cognitive category is identified, different classical paradigms are selected and evaluated to maximize the training abilities in an IVR environment. Once the candidate paradigm has been identified, the extensive literature review identifies task requirements. Namely, (1) the mechanics of the paradigm, (2) the actions that are required from the participant, (3) the category and type of stimuli, (4) the outcome measures that are expected from the task that are critical to evaluate the cognitive ability, and (5) identify the parameters that can be modified to increase the difficulty of the task. Further evaluation of the Enhance VR app will require confirmation of the face and content validity of the tests since the inclusion of a strong motor component may add confounding variables despite careful co-design between scientific and development teams.
Additionally, VR scenarios offers the opportunity to assess cognitive function in realistic daily-life scenarios with increased ecological validity (38). For instance, VR paradigms enable testing of navigational skills in a supermarket and collecting ecologically relevant data, without exposing the participant to the dangers of navigating these actual scenarios (i.e., experimentally well-controlled) (68). The mechanics of the Enhance VR games derive from neuropsychological principles, such as the n-back task (47) or the Stroop task (43). We propose that the VR versions of the cognitive assessment tests could provide a naturalistic approach toward the measurement of cognitive capabilities since IVR promotes multisensory body-related information (69).
An additional advantage of IVR systems is the ability to collect large and varied behavioral datasets (17). As the participants engage with the Enhance VR games, the system not only collects the performance of the participants, but also a large number of game-related variables. Some of these variables include motor outputs (e.g., movement coordinates or hand preferences), and reaction times, among others. These data points could provide, when combined with supervised machine learning algorithms, novel non-invasive digital biomarkers of cognitive status by collecting characteristics from digital health technologies that could be used to monitor biological or pathogenic processes and assess responses to pharmacological interventions (70). The app thus affords, for an experimenter-independent monitoring of cognitive function, while allowing the researchers and clinical staff to access this data. The Enhance VR app is compliant with GDPR and HIPAA regulations to ensure that it can meet the criteria of data privacy (61).
The use of VR environments for cognitive training and monitoring (or assessment) presents some concerns that need to be addressed as their use is becoming more widespread (61, 68). Among these, the need to minimize adverse effects is of utmost importance. For instance, cybersickness can negatively affect the cognitive performance of the individuals (71). Efforts to minimize cybersickness can be implemented both in the hardware and software (61). First, the Enhance VR app takes advantage of the technical aspects of the hardware, supporting state of the art off-the-shelf headsets. The Enhance VR app is available for headsets with six degrees of freedom (6DoF), which provide a seemingly naturalistic interaction with the environment by the use of controllers (72). Additionally, the Enhance VR app provides high-quality software that can potentially help avoid cybersickness (61). Finally, the participant is not required to move within the virtual environment, which further helps reduce the potential for cybersickness. Future studies will assess the presence of adverse effects in VR environments (73).
The cost of the hardware has been reduced significantly in the last years and it is becoming more readily available for research and clinical purposes (23). However, the development of high quality immersive environments is time consuming and expensive (68). Thus, it is important to foster collaboration between enterprizes with the resources to develop the cognitive training software and research institutions with the means to validate these systems. The Enhance VR system is readily available for research purposes. Furthermore, it is accompanied by additional features that make it an interesting tool, such as a data dashboard that allows the monitoring of users within an organization; a remote control feature that allows for telehealth interventions; and a customizable survey system integrated within the Enhance VR system.
5. Conclusions
As the senior population continues to grow, it becomes crucial to implement strategies to maintain their autonomy and independence. Among the proposed strategies, cognitive training solutions provide a structured system to train multiple cognitive abilities in a scenario with an adaptive difficulty. While computerized cognitive training solutions have shown positive results, screen-based systems lack naturalistic interaction and show a limited transfer of benefits to activities of daily living and global cognitive functioning.
IVR systems, on the other hand, present the user with a multisensory environment, resulting in an immersive and embodied experience of the virtual scenario. By taking advantage of this feature, the Enhance VR app aims to train and monitor cognitive functions using cognitively demanding immersive games. The presentation of seemingly naturalistic environments could provide an advantage over screen-based systems, whereby Enhance VR can become a validated tool for cognitive monitoring and training.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author Contributions
All authors contributed to the manuscript writing, revision, and approval of the submitted version.
Conflict of Interest
AB and HJ are Chief Executive Officer and Chief Technical Officer, respectively, and founders at Virtuleap. VB-R was employed as Neuroscientist at Virtuleap.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
The authors would like to thank all of the Virtuleap team, who are making Enhance VR a reality, and Badoo.
References
1. Ngandu T, Lehtisalo J, Solomon A, Levälahti E, Ahtiluoto S, Antikainen R, et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): a randomised controlled trial. Lancet. (2015) 385:2255–63. doi: 10.1016/S0140-6736(15)60461-5
2. Klimova B, Valis M, Kuca K. Cognitive decline in normal aging and its prevention: a review on non-pharmacological lifestyle strategies. Clin Interv Aging. (2017) 12:903–10. doi: 10.2147/CIA.S132963
3. Lauenroth A, Ioannidis AE, Teichmann B. Influence of combined physical and cognitive training on cognition: a systematic review. BMC Geriatr. (2016) 16:141. doi: 10.1186/s12877-016-0315-1
4. Clare L, Woods RT. Cognitive training and cognitive rehabilitation for people with early-stage Alzheimer's disease: a review. Neuropsychol Rehabil. (2007) 14:385–401. doi: 10.1080/09602010443000074
5. Hertzog C, Kramer AF, Wilson RS, Lindenberger U. Enrichment effects on adult cognitive development: can the functional capacity of older adults be preserved and enhanced? Psychol Sci Publ Int. (2008) 9:1–65. doi: 10.1111/j.1539-6053.2009.01034.x
6. Ball K, Berch DB, Helmers KF, Jobe JB, Leveck MD, Marsiske M, et al. Effects of cognitive training interventions with older adults: a randomized controlled trial. J Am Med Assoc. (2002) 288:2271–81. doi: 10.1001/jama.288.18.2271
7. Willis SL, Tennstedt SL, Marsiske M, Ball K, Elias J, Koepke KM, et al. Long-term effects of cognitive training on everyday functional outcomes in older adults. J Am Med Assoc. (2006) 296:2805–14. doi: 10.1001/jama.296.23.2805
8. Rebok GW, Ball K, Guey LT, Jones RN, Kim HY, King JW, et al. Ten-year effects of the advanced cognitive training for independent and vital elderly cognitive training trial on cognition and everyday functioning in older adults. J Am Geriatr Soc. (2014) 62:16–24. doi: 10.1111/jgs.12607
9. Lampit A, Hallock H, Valenzuela M. Computerized cognitive training in cognitively healthy older adults: a systematic review and meta-analysis of effect modifiers. PLoS Med. (2014) 11:e1001756. doi: 10.1371/journal.pmed.1001756
10. Lasaponara S, Marson F, Doricchi F, Cavallo M. A scoping review of cognitive training in neurodegenerative diseases via computerized and virtual reality tools: what we know so far. Brain Sci. (2021) 11:528. doi: 10.3390/brainsci11050528
11. Owen AM, Hampshire A, Grahn JA, Stenton R, Dajani S, Burns AS, et al. Putting brain training to the test. Nature. (2010) 465:775–8. doi: 10.1038/nature09042
12. García-Casal JA, Loizeau A, Csipke E, Franco-Martín M, Perea-Bartolomé MV, Orrell M. Computer-based cognitive interventions for people living with dementia: a systematic literature review and meta-analysis. Aging Ment Health. (2017) 21:454–67. doi: 10.1080/13607863.2015.1132677
13. Polat BSA, Karadas O. Evaluation of a computer-based cognitive training program for early-stage Alzheimer's disease. Ann Clin Analyt Med. (2022) 13:175–179. doi: 10.4328/ACAM.20902
14. Sanchez-Vives MV, Slater M. From presence to consciousness through virtual reality. Nat Rev Neurosci. (2005) 6:332–9. doi: 10.1038/nrn1651
15. Bohil CJ, Alicea B, Biocca FA. Virtual reality in neuroscience research and therapy. Nat Rev Neurosci. (2011) 12:752–62. doi: 10.1038/nrn3122
16. Parsons TD. Virtual reality for enhanced ecological validity and experimental control in the clinical, affective and social neurosciences. Front Hum Neurosci. (2015) 9:660. doi: 10.3389/fnhum.2015.00660
17. Bauer A, Andringa G. The potential of immersive virtual reality for cognitive training in elderly. Gerontology. (2020) 66:614–23. doi: 10.1159/000509830
18. Martingano AJ, Persky S. Virtual reality expands the toolkit for conducting health psychology research. Soc Pers Psychol Compass. (2021) 15:e12606. doi: 10.1111/spc3.12606
19. Brugada-Ramentol V, Clemens I, de Polavieja GG. Active control as evidence in favor of sense of ownership in the moving Virtual Hand Illusion. Conscious Cogn. (2019) 71:123–35. doi: 10.1016/j.concog.2019.04.003
20. Sanchez-Vives MV, Spanlang B, Frisoli A, Bergamasco M, Slater M. Virtual hand illusion induced by visuomotor correlations. PLoS ONE. (2010) 5:e10381. doi: 10.1371/journal.pone.0010381
21. Bailenson JN, Yee N, Blascovich J, Beall AC, Lundblad N, Jin M. The use of immersive virtual reality in the learning sciences: digital transformations of teachers, students, and social context. J Learn Sci. (2008) 17:102–41. doi: 10.1080/10508400701793141
22. Garrett B, Taverner T, Gromala D, Tao G, Cordingley E, Sun C. Virtual reality clinical research: promises and challenges. JMIR Ser Games. (2018) 6:e10839. doi: 10.2196/preprints.10839
23. Slater M. Immersion and the illusion of presence in virtual reality. Br J Psychol. (2018) 109:431–3. doi: 10.1111/bjop.12305
24. Riva G, Wiederhold BK, Mantovani F. Neuroscience of virtual reality: from virtual exposure to embodied medicine. Cyberpsychol Behav Soc Netw. (2019) 22:82–96. doi: 10.1089/cyber.2017.29099.gri
25. Perez-Marcos D. Virtual reality experiences, embodiment, videogames and their dimensions in neurorehabilitation. J NeuroEng Rehabil. (2018) 15:113. doi: 10.1186/s12984-018-0461-0
26. Gamito P, Oliveira J, Pacheco J, Morais D, Saraiva T, Lacerda R, et al. Traumatic brain injury memory training: a virtual reality online solution. Int J Disabil Hum Dev. (2011) 10:309–12. doi: 10.1515/IJDHD.2011.049
27. Coughlan G, Coutrot A, Khondoker M, Minihane AM, Spiers H, Hornberger M. Toward personalized cognitive diagnostics of at-genetic-risk Alzheimer's disease. Proc Natl Acad Sci USA. (2019) 116:9285–92. doi: 10.1073/pnas.1901600116
28. Krokos E, Plaisant C, Varshney A. Virtual memory palaces: immersion aids recall. Virt Real. (2019) 23. doi: 10.1007/s10055-018-0346-3
29. Triegaardt J, Han TS, Sada C, Sharma S, Sharma P. The role of virtual reality on outcomes in rehabilitation of Parkinson's disease: meta-analysis and systematic review in 1031 participants. Neurol Sci. (2020) 41:529–36. doi: 10.1007/s10072-019-04144-3
30. Wais PE, Arioli M, Anguera-Singla R, Gazzaley A. Virtual reality video game improves high-fidelity memory in older adults. Sci Rep. (2021) 11:2552. doi: 10.1038/s41598-021-82109-3
31. Gago MF, Yelshyna D, Bicho E, Silva HD, Rocha L, Rodrigues ML, et al. Compensatory postural adjustments in an oculus virtual reality environment and the risk of falling in Alzheimer's disease. Dement Geriatr Cogn Disord Extra. (2016) 6:252–67. doi: 10.1159/000447124
32. Doniger GM, Beeri MS, Bahar-Fuchs A, Gottlieb A, Tkachov A, Kenan H, et al. Virtual reality-based cognitive-motor training for middle-aged adults at high Alzheimer's disease risk: a randomized controlled trial-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/ 4.0/). Transl Res Clin Interven. (2018) 4:118–29. doi: 10.1016/j.trci.2018.02.005
33. Zhong D, Chen L, Feng Y, Song R, Huang L, Liu J, et al. Effects of virtual reality cognitive training in individuals with mild cognitive impairment: a systematic review and meta-analysis. Int J Geriatr Psychiatry. (2021) 36:1829–47. doi: 10.1002/gps.5603
34. Faria AL, Andrade A, Soares L, i Badia SB. Benefits of virtual reality based cognitive rehabilitation through simulated activities of daily living: a randomized controlled trial with stroke patients. J NeuroEng Rehabil. (2016) 13:96. doi: 10.1186/s12984-016-0204-z
35. Manera V, Chapoulie E, Bourgeois J, Guerchouche R, David R, Ondrej J, et al. A feasibility study with image-based rendered virtual reality in patients with mild cognitive impairment and dementia. PLoS ONE. (2016) 11:e151487. doi: 10.1371/journal.pone.0151487
36. Gamito P, Oliveira J, Alves C, Santos N, Coelho C, Brito R. Virtual reality-based cognitive stimulation to improve cognitive functioning in community elderly: a controlled study. Cyberpsychol Behav Soc Netw. (2020) 23:150–6. doi: 10.1089/cyber.2019.0271
37. Maeng S, Hong JP, Kim WH, Kim H, Cho SE, Kang JM, et al. Effects of virtual reality-based cognitive training in the elderly with and without mild cognitive impairment. Psychiatry Invest. (2021) 18:619–27. doi: 10.30773/pi.2020.0446
38. Kourtesis P, Collina S, Doumas LAA, MacPherson SE. Validation of the virtual reality everyday assessment lab (VR-EAL): an immersive virtual reality neuropsychological battery with enhanced ecological validity. J Int Neuropsychol Soc. (2021) 27:181–96. doi: 10.1017/S1355617720000764
39. Tedstone D, Coyle K. Cognitive impairments in sober alcoholics: performance on selective and divided attention tasks. Drug Alcohol Depend. (2004) 75:277–86. doi: 10.1016/j.drugalcdep.2004.03.005
40. Dinges DF, Powell JW. Microcomputer analyses of performance on a portable, simple visual RT task during sustained operations. Ann GIS. (1985) 17:652–5. doi: 10.3758/BF03200977
41. Rivière J, Brisson J. Space-based visual attention: a marker of immature selective attention in toddlers? Dev Psychobiol. (2014) 56:1589–94. doi: 10.1002/dev.21240
42. Grant DA, Berg E. A behavioral analysis of degree of reinforcement and ease of shifting to new responses in a Weigl-type card-sorting problem. J Exp Psychol. (1948) 38:404–11. doi: 10.1037/h0059831
43. Stroop JR. Studies of interference in serial verbal reactions. J Exp Psychol. (1935) 18:643–62. doi: 10.1037/h0054651
44. Reitan RM. Validity of the Trail Making Test as an indicator of organic brain damage. Percept Motor Skills. (1958) 8:271. doi: 10.2466/PMS.8.7.271-276
45. Gronwall DMA. Paced auditory serial addition task: a measure of recovery from concussion. Percept Motor Skills. (1977) 44:367–73. doi: 10.2466/pms.1977.44.2.367
46. Sala SD, Gray C, Baddeley A, Wilson L. Visual Patterns Test. A Test of Short-Term Visual Recall. Bury St Edmunds: Thames Valley Test Company (1997).
47. Kirchner WK. Age differences in short-term retention of rapidly changing information. J Exp Psychol. (1958) 55:352–8. doi: 10.1037/h0043688
48. Sahakian BJ, Bruhl AB, Cook J, Killikelly C, Savulich G, Piercy T, et al. The impact of neuroscience on society: cognitive enhancement in neuropsychiatric disorders and in healthy people. Philos Trans R Soc B Biol Sci. (2015) 370:20140214. doi: 10.1098/rstb.2014.0214
49. Humes GE, Welsh MG, Retzlaff P, Cookson N. Towers of Hanoi and London: reliability and validity of two executive function tasks. Assessment. (1997) 4:249–57. doi: 10.1177/107319119700400305
50. Frearson W, Eysenck HJ. Intelligence, reaction time (RT) and a new 'odd-man-out' RT paradigm. Pers Individ Differ. (1986) 7:807–17. doi: 10.1016/0191-8869(86)90079-6
51. Borod JC, Koff E, Caron HS. The Target Test: a brief laterality measure of speed and accuracy. Percept Motor Skills. (1984) 58:743–8. doi: 10.2466/pms.1984.58.3.743
52. Fritz NE, Cheek FM, Nichols-Larsen DS. Motor-cognitive dual-task training in persons with neurologic disorders. J Neurol Phys Ther. (2015) 39:142–53. doi: 10.1097/NPT.0000000000000090
53. Shepard RN, Metzler J. Mental rotation of three-dimensional objects. Science. (1971) 171:701–3. doi: 10.1126/science.171.3972.701
54. Chermak GD, Montgomery MJ. Form equivalence of the Selective Auditory Attention Test administered to 6-year-old children. J Speech Hear Res. (1992) 35:661–5. doi: 10.1044/jshr.3503.661
55. He W, Goodkind D, Kowal P. An Aging World. (2016). Available online at: https://www.census.gov/content/dam/Census/library/publications/2016/demo/p95-16-1.pdf
56. Huckans M, Hutson L, Twamley E, Jak A, Kaye J, Storzbach D. Efficacy of cognitive rehabilitation therapies for mild cognitive impairment (MCI) in older adults: working toward a theoretical model and evidence-based interventions. Neuropsychol Rev. (2013) 23:63–80. doi: 10.1007/s11065-013-9230-9
57. Anguera JA, Boccanfuso J, Rintoul JL, Al-Hashimi O, Faraji F, Janowich J, et al. Video game training enhances cognitive control in older adults. Nature. (2013) 501:97–101. doi: 10.1038/nature12486
58. Boot WR, Blakely DP, Simons DJ. Do action video games improve perception and cognition? Front Psychol. (2011) 2:226. doi: 10.3389/fpsyg.2011.00226
59. Perez-Marcos D, Bieler-Aeschlimann M, Serino A. Virtual reality as a vehicle to empower motor-cognitive neurorehabilitation. Front Psychol. (2018) 9:2120. doi: 10.3389/fpsyg.2018.02120
60. Sala G, Aksayli ND, Tatlidil KS, Tatsumi T, Gondo Y, Gobet F. Near and far transfer in cognitive training: a second-order meta-analysis. Collabra. (2019) 5:18. doi: 10.1525/collabra.203
61. Kourtesis P, MacPherson SE. How immersive virtual reality methods may meet the criteria of the National Academy of Neuropsychology and American Academy of Clinical Neuropsychology: a software review of the Virtual Reality Everyday Assessment Lab (VR-EAL). Comput Hum Behav Rep. (2021) 4:100151. doi: 10.1016/j.chbr.2021.100151
62. Strong J. Immersive virtual reality and persons with dementia: a literature review. J Gerontol Soc Work. (2020) 63:209–26. doi: 10.1080/01634372.2020.1733726
63. Sayma M, Tuijt R, Cooper C, Walters K. Are we there yet? Immersive virtual reality to improve cognitive function in dementia and mild cognitive impairment. Gerontologist. (2020) 60:e502–12. doi: 10.1093/geront/gnz132
64. Syed-Abdul S, Malwade S, Nursetyo AA, Sood M, Bhatia M, Barsasella D, et al. Virtual reality among the elderly: a usefulness and acceptance study from Taiwan. BMC Geriatr. (2019) 19:8. doi: 10.1186/s12877-019-1218-8
65. Arlati S, Santo SGD, Franchini F, Mondellini M, Filiputti B, Luchi M, et al. Acceptance and usability of immersive virtual reality in older adults with objective and subjective cognitive decline. J Alzheimer's Dis. (2021) 80:1025–38. doi: 10.3233/JAD-201431
66. Yun SJ, Kang MG, Yang D, Choi Y, Kim H, Oh BM, et al. Cognitive training using fully immersive, enriched environment virtual reality for patients with mild cognitive impairment and mild dementia: feasibility and usability study. JMIR Ser Games. (2020) 8:e18127. doi: 10.2196/preprints.18127
67. Parsons TD, Rizzo AA. Initial validation of a virtual environment for assessment of memory functioning: virtual reality cognitive performance assessment test. CyberPsychol Behav. (2008) 11:17–25. doi: 10.1089/cpb.2007.9934
68. Krohn S, Tromp J, Quinque EM, Belger J, Klotzsche F, Rekers S, et al. Multidimensional evaluation of virtual reality paradigms in clinical neuropsychology: application of the VR-check framework. J Med Intern Res. (2020) 22:e16724. doi: 10.2196/16724
69. Kilteni K, Maselli A, Kording KP, Slater M. Over my fake body: body ownership illusions for studying the multisensory basis of own-body perception. Front Hum Neurosci. (2015) 9:141. doi: 10.3389/fnhum.2015.00141
70. Vasudevan S, Saha A, Tarver ME, Patel B. Digital biomarkers: convergence of digital health technologies and biomarkers. NPJ Digit Med. (2022) 5:36. doi: 10.1038/s41746-022-00583-z
71. Mittelstaedt JM, Wacker J, Stelling D. VR aftereffect and the relation of cybersickness and cognitive performance. Virt Real. (2019) 23:143–54. doi: 10.1007/s10055-018-0370-3
72. Figueiredo L, Rodrigues E, Teixeira J, Techrieb V. A comparative evaluation of direct hand and wand interactions on consumer devices. Comput Graph. (2018) 77:108–21. doi: 10.1016/j.cag.2018.10.006
Keywords: virtual reality, cognitive training, cognitive monitoring, immersion, multisensory integration, presence
Citation: Brugada-Ramentol V, Bozorgzadeh A and Jalali H (2022) Enhance VR: A Multisensory Approach to Cognitive Training and Monitoring. Front. Digit. Health 4:916052. doi: 10.3389/fdgth.2022.916052
Received: 08 April 2022; Accepted: 16 May 2022;
Published: 03 June 2022.
Edited by:
Lars Lau Raket, Novo Nordisk, DenmarkReviewed by:
Panagiotis Kourtesis, Inria Rennes—Bretagne Atlantique Research Centre, FranceCopyright © 2022 Brugada-Ramentol, Bozorgzadeh and Jalali. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Victòria Brugada-Ramentol, dmljdG9yaWFAdmlydHVsZWFwLmNvbQ==; Amir Bozorgzadeh, YW1pckB2aXJ0dWxlYXAuY29t; Hossein Jalali, aG9zc2VpbkB2aXJ0dWxlYXAuY29t