 Soumya Kini
Soumya Kini Dave Duluk2,†
Dave Duluk2,† Joshua Weinstein
Joshua Weinstein- 1Principal Health Systems Engineer at The MITRE Corporation, Mclean, VA, United States
- 2Lead Data Scientist at The MITRE Corporation, Mclean, VA, United States
- 3Department of Health Policy and Management, Gillings School of Global Public Health, University of North Carolina at Chapel Hill, Chapel Hill, NC, United States
The All of Us Research Program (All of Us or Program) is an ongoing longitudinal data collection operated by the National Institutes of Health (NIH). The Program aims to improve healthcare for all through the development of a biomedical research resource reflective of the diversity of the United States that includes Underrepresented in Biomedical Research (UBR) groups. Federally Qualified Health Centers (FQHCs) are a key recruitment stream of UBR participants, which are community based and provide primary care and preventive services in medically underserved areas. Over 90% of FQHC patients enrolled in All of Us to date are UBR. The COVID-19 pandemic caused a pause in All of Us activities. Re-starting the activities was a challenge, especially due to the digital divide faced by FQHC participants, and that most Program activities are primarily completed via web-based portal from a computer or a mobile device. This paper investigates the extent to which digital readiness impacted recruitment and sustainment of a pre-pandemic sample of 2,791 FQHC participants to the Program. Digital readiness was defined by access to home-based or other internet-accessing devices, and participants’ comfort level using such devices. Results from multivariable logistic regression models showed that lower age, more education, female gender identity, and higher income were associated with higher digital readiness (p ≤ 0.01). Race, rurality, and sexual orientation status were not significant factors associated with digital readiness. Older participants had higher odds of completing Program activities, even though less digitally ready than their younger peers, as they often completed the activities during their in-person clinical visits. A subsequent weighted model demonstrated that FQHC participants who were digitally ready had 27% higher odds of completing Program activities than those not digitally ready. The data highlight the need for improved connectivity and sustainment between longitudinal data collection, research programs, and UBR participants, particularly among those facing the digital divide. Quantifying digital challenges provide operational insights for longitudinal data collection (All of Us, or others), and broadly, other aspects of digital medicine such as telehealth or patient portals by recognizing digital readiness of participants and patients, and the level of support required for success.
1. Introduction
The All of Us Research Program (All of Us or Program) is an ongoing longitudinal data collection operated by the National Institutes of Health (NIH) to collect lifestyle, health, socioeconomic, environmental, and biological data from 1 million United States-based participants (1). Diversity is a core tenet of the Program, which aims to ensure those who are typically Underrepresented in Biomedical Research (UBR) are the majority of those enrolled and retained (2).
The Program has defined specific UBR categories that include racial identity, age when consented to Program participation, biological sex at birth, sexual orientation, gender identity, income, educational attainment, access to care, disability and rurality. Three site types are responsible for enrolling and retaining these participants: Regional Medical Centers, Veterans Administration Medical Centers, and Federally Qualified Health Centers (FQHCs). FQHCs are a key recruitment stream of UBR participants and are centrally coordinated and supported by The MITRE Corporation (MITRE) (3). FQHCs are community based and provide primary care and preventive services in medically underserved areas regardless of ability to pay (4). Over 90% of the FQHC patients are low income, over 80% are publicly insured or uninsured, and the majority are members of racial and ethnic minority groups (5). Individuals and families served by FQHCs are among the most economically vulnerable in the nation and often have complex health and social challenges. Enrollment activities for the Program are primarily completed via a web-based portal from a computer or a mobile device. Therefore, digital readiness plays a key role in the FQHC All of Us team's ability to enroll and retain participants in the Program. Barriers for utilizing digital devices among patients at FQHCs include cost and lack of information, access to technology, and broadband connection. Digital health device adoption at FQHCs requires education, investment, and high-touch methods (6).
While the Program intends to ensure enrichment of UBR populations, historically the recruitment of UBR populations (particularly racial and ethnic minorities, and low-income communities) to clinical studies is largely viewed as a challenge (7). For example, where race and ethnicity are concerned, though African Americans and Hispanics represent 13% and 16% of the United States population, respectively, only 5% of clinical trial participants are African American and 1% of participants are Hispanic (8). Socially and economically disadvantaged groups are least likely to have access to a smartphone, computer, home broadband, or internet. For example, a 2021 study published by the Pew Research Center found that 13% of low-income adults do not have access to a smartphone, computer, or home broadband, in comparison to 1% of those with incomes over $100,000 (9). Populations that discontinue internet use due to cost and disability are more likely to be Hispanic, Black, or low income. Telemedicine is also less adopted by UBR groups, including those who are older, are racial and ethnic minorities, have a rural residence, and are publicly insured (10). A Brookings Institute report published in 2020 found that, when examining the issue by income groups, 38% of households earning less than $20,000 lack a broadband subscription (11). This is a typical manifestation of the digital divide, defined as the gap between those who have and those who do not have access to information technology. Digital exclusion can limit participation in clinical research studies, innovative clinical trial design, and the collection of patient-reported outcomes. Furthermore, while digital exclusion is concentrated among the poorest, least educated, disabled, and socially isolated, these groups also gain less benefit from the use of digital technology in their health outcomes than do their more privileged peers. In this manner, digital exclusion compounds poor health outcomes, and is now termed a new social determinant of health (12–16).
This paper investigates the extent to which digital readiness impacts recruitment and sustainment of participants to the Program who are patients at FQHCs, particularly among UBR groups. Analyses contained in this paper provide operational insights for NIH, healthcare providers, and researchers on developing and adopting a digital inclusion-informed strategy that recognizes the digital readiness of participants and patients, and the level of staff support required for a broad range of activities, such as recruiting for longitudinal data collection and studies, telehealth, telemedicine, or patient portals.
2. Methods
The analyses utilize quantitative data on adult FQHC patients who are All of Us participants; data are housed at the Data and Research Center (DRC) Program Data Repository. The DRC is located at Vanderbilt University Medical Center and is funded by the NIH Program (17). Quantitative data used in this paper include participant demographics, All of Us operational data, and a participant survey questionnaire called the Minimum Common Metrics (MCM) collected by the following six FQHCs from across the country that reflect the diversity of the United States: Community Health Center, Inc. located in Connecticut; Cherokee Health Systems located in Tennessee; Cooperative Health located in South Carolina; Jackson-Hinds Comprehensive Health Center located in Mississippi; Sun River Health located in New York, and San Ysidro Health located in California. Two additional FQHCs located in Hawaii and Puerto Rico have since been added in 2021 and 2022, respectively. These two FQHCs had not begun collecting MCM data at the time of writing this paper and are therefore excluded from the analysis.
On March 16, 2020, NIH paused in-person Program activities to assist in preventing the spread of COVID-19 (23). UBR participants were disproportionality impacted during the COVID-19 pause of in-person activities. FQHCs adopted virtual strategies using Computer Assisted Telephone Interviewing (CATI), which was launched by All of Us in January 2021. CATI has presented a new opportunity for FQHCs to contact participants via phone and record participant responses to surveys in real time. Follow-up research is underway to characterize the All of Us participants who utilized CATI at FQHCs as well as to explore the relationship between retention activities via CATI and UBR status. The quantitative data collection methods were performed in accordance with relevant guidelines and regulations and approved by All of Us Research Program Institutional Review Board (IRB00010472). The participants included in this paper have provided consent to having their data used for research. All data used were derived from participants who provided written consent on or before April 28, 2022, which is the freeze date for the dataset used in this study. Variables in the dataset are described in the sections below.
2.1. Participant demographics and recruitment data
Participant demographics include data that the Program considers for determining UBR and are collected from FQHC patients at the time of registration. They include racial identity, age when consented to Program participation, biological sex at birth, sexual orientation, gender identity, income, educational attainment, and rurality at the time of writing this paper. Participants are considered UBR if one or more of the definitions provided in Table 1 is true.
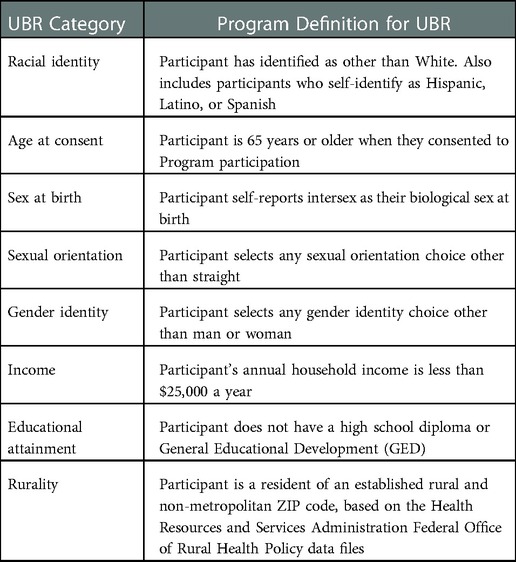
Table 1. All of Us definitions for participants that are Underrepresented in Biomedical Research (UBR).
Recruitment data include participants who are considered retained per the Program definition at the time of writing this paper, by completing the activities outlined in Table 2. In All of Us, retained participants complete follow-up surveys at least once every 18 months after their enrollment. In this context, retention provides a measure for the ability of the FQHCs to sustain engagement with participants after recruitment to the Program. All activities, except submitting bio samples to the Biobank, are completed by participants on a web-based portal when they come in-person to the FQHCs or virtually from a computer or a mobile device.
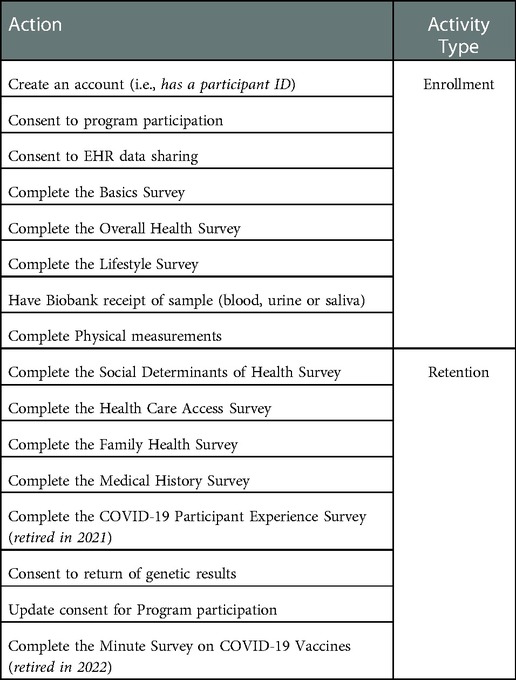
Table 2. Required Actions to be Completed by the Participant in the All of Us Research Program.
2.2. Minimum common metrics data
MCM is an Institutional Review Board (IRB)-approved questionnaire collected by FQHCs for MITRE. It contains participant responses on their enrollment experience, digital readiness, access to a fitness tracker, and level of FQHC staff assistance required for completing All of Us activities. Answers to these questions are collected throughout the participant journey (Table 2), with a goal of understanding FQHC participant experiences and resources available for them to participate in the Program. Table 3 provides all questions asked of participants in the MCM data at the time of writing this paper. The MCM survey questions were asked by FQHC staff to all participants at their time of enrollment in All of Us. However, per the IRB requirements, participants were given a choice to decline responding to the MCM survey entirely or skip any of the questions. A subset of responses to the MCM questions that pertain to participants' digital readiness were used in the analysis contained in this paper.
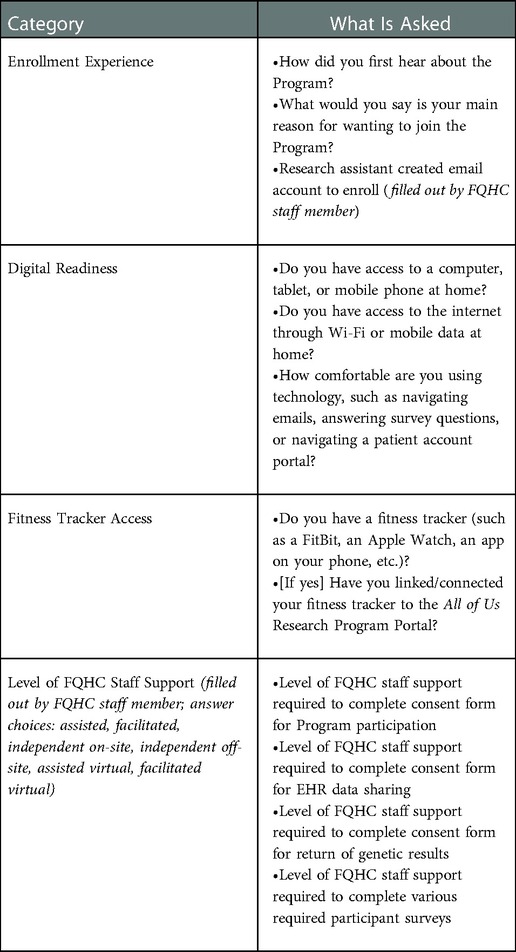
Table 3. FQHC MCM questionnaire.
2.3. Qualitative data from FQHCs
In addition to quantitative data described in the previous sections, the MITRE team engaged the FQHC staff to collect qualitative data about their experiences and strategies in engaging population groups for retention activities. The MITRE team held a focus group with the FQHC staff in June 2022 to gather inputs. All of Us staff members from all six FQHCs participated in the focus group. Focus group discussion included open-ended conversations on the following topics: strategies FQHCs used to retain participants with low digital readiness into All of Us, and data sources FQHCs utilized to be better informed and to develop strategies for engaging population groups with low digital readiness. The discussions were focused on pre-pandemic scenario, given the scope of this paper. The MITRE team recorded the conversation upon consent from the FQHC staff members participating in the meeting and transcribed notes summarizing the conversations. Information collected from these questions were analyzed alongside quantitative results to develop insights on whether specific population groups that the model found significant for indicating low digital readiness influenced the FQHC engagement strategy.
2.4. Study population
The study population included 2,897 All of Us participants who responded to questions on digital readiness (three questions, Table 3) for the time-period between June 2019 and March 2020 when they completed required actions to become an enrolled participant (Table 2). This time-period was selected based on when the digital readiness questions were first asked by FQHCs (June 2019) to newly enrolled participants until the start of the COVID-19 pandemic (March 2020). The COVID-19 pandemic significantly changed the operational workflow at the FQHCs when NIH paused in-person All of Us activities. Therefore, data collected during the COVID-19 pandemic were not included in this analysis. Demographic variables, retention data, and participant responses to the MCM technology access questions were additional fields associated with the participants in the study sample.
2.5. Analytical methods
For purposes of this study, digital readiness was defined by access to home-based or other internet-accessing devices (computers, tablets, mobile phones, and other devices) and participants' comfort level using such devices. Responses to the three MCM technology access questions shown in Table 4 were utilized to define digital readiness. Participants who skipped or selected the “Prefer not to answer” option to any of the three questions were excluded from the analytic sample within the study time-period range since it was not possible to infer the digital readiness disposition for these participants. This reduced the final analytic sample from 2,897 to 2,791 participants. FQHC participant demographic distributions of those included in the analytic sample were compared with those who were excluded from the study sample to verify that the analytic sample was not a biased set relative to the larger FQHC All of Us population. All analyses in this paper were conducted using R and RStudio (18, 19). Any group with less than 20 participants were included in “Other” group to stay consistent with the Program data suppression levels to support data privacy.
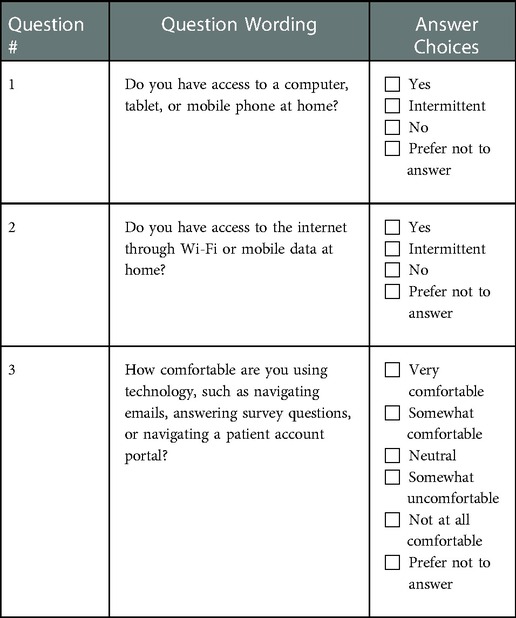
Table 4. Answer choices for the MCM technology access questions.
Participants who responded with a “Yes” or “Intermittent” to Questions 1 and 2, and “Very comfortable,” “Somewhat comfortable,” or “Neutral” to Question 3 were considered as digitally ready and transformed as such in the analytical data set. Participants who responded with a “No” to Questions 1 or 2 or “Somewhat uncomfortable” or “Not at all comfortable” to Question 3 were considered as not digitally ready and transformed as such in the analytical data set.
Retention data was transformed into a Boolean (1 or 0) variable, which was equal to 1 if the participant had ever been retained by completing the required activities outlined in Table 2 at some point during their involvement in the Program, and a 0 if the Participant was never retained because they did not complete any of the required activities since becoming an enrolled Participant during the study period.
2.5.1. Characteristics of digitally ready groups in the program at FQHCs
The characteristics of the All of Us groups that are digitally ready (vs. not digitally ready) at FQHCs were explored using a multivariable logistic regression model (Model 1) with UBR variables of racial identity, age at consent, sex at birth, sexual orientation, gender identity, income, educational attainment, and rurality.
2.5.2. Digital readiness impact on the retention of participants in the program at FQHCs
The effect of digital readiness on retention was measured using a second multivariable logistic regression model (Model 2). Inverse probability of treatment weights (IPTW) propensity score methods were used to create a weighted synthetic population. IPTW utilizes propensity scores to balance baseline characteristics in exposed and unexposed groups. Applied to the current study, IPTW balances UBR characteristics in the digitally ready and not digitally ready groups, therefore minimizing the impact of confounding due to those measured UBR characteristics (20). With this approach, one cannot attribute differences in retention outcomes due to differences in UBR characteristics between individuals who are digitally ready and those who are not digitally ready.
UBR variables significant at the 0.05 level from Model 1 were used in the propensity score model. Multivariable logistic regression was used to model participants' probability of retention as weighted by the previously described IPTW. Propensity score modeling was conducted using the WeightIt and Survey R packages (21, 22). Results from both weighted and unweighted models are included in the results.
3. Results and discussion
3.1. Digital readiness landscape of the program participants at FQHCs
The analytic sample included 2,791 All of Us participants who responded to the three MCM digital readiness questions between June 2019 and March 2020 when they completed the required actions to become an enrolled Participant. Applying the definition of digital readiness described earlier in this paper to this sample resulted in 1,527 participants who were considered digitally ready and 1,264 participants who were considered not digitally ready, as shown in Figure 1.
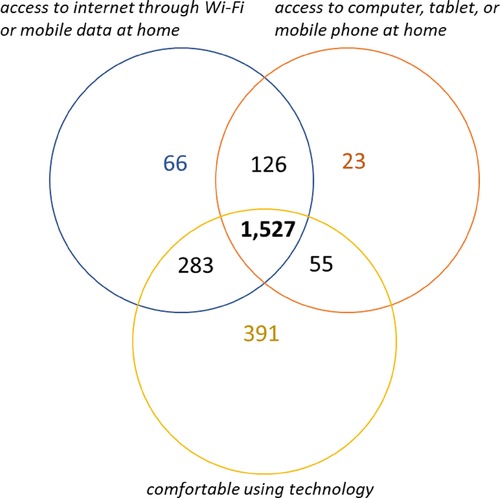
Figure 1. Digital readiness disposition among the All of Us participants at FQHCs. [Total number of participants = 2,791. Digital readiness was defined by access to home-based or other internet-accessing devices (computers, tablets, mobile phones, and other devices) and participants’ comfort level using such devices].
Figure 1 indicates that, among the 1,264 Program participants who were not digitally ready, about 31% (391) were comfortable using technology but did not have access to the internet or a computer at home; and 22% (283) of participants were comfortable using technology and had access to the internet but did not have a computer, tablet, or mobile phone at home. These observations indicate that a majority of the participants (53%) were not digitally ready due to lack of a device, which they may not have been able to afford considering that over 90% of FQHC patients are low income (5).
Prior to setting up the model, FQHC participant demographic distributions of those included in the analytic sample were compared with those who were excluded to verify that the analytic sample was not a biased set relative to the larger FQHC All of Us population. The two groups were very similar in distribution (χ2 test p ≥ 0.13 for all comparison groups), indicating that specific demographic groups were not over- or under-represented in the analytic sample. Examination of demographic characteristics, to the extent they might result in collinearity, showed that gender identity and sex at birth were strongly associated (Cramer's V = 0.65). Therefore, gender identity was used in the final model as it represented the participant's self-identification; sex at birth was excluded.
Results from a multivariable logistic regression model relating to characteristics of groups that are not digitally ready at FQHCs are shown in Figure 2 (Model 1). A complete table containing Odds Ratios (OR) and 95% Confidence Interval (CI) values is included in the Supplementary Table S1 of this paper.
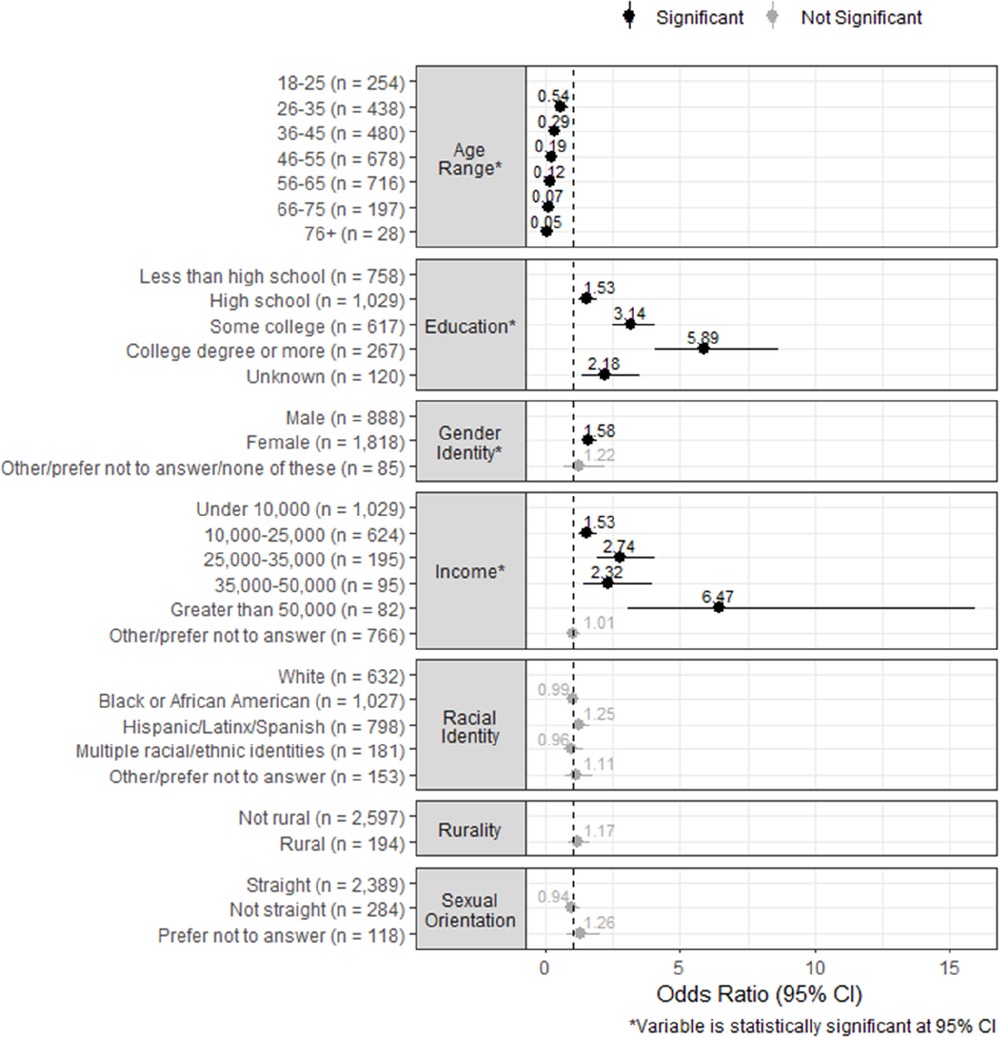
Figure 2. Results from the model to understand characteristics of groups that are not digitally ready at FQHCs. (Outcome variable: Digital Readiness. Coded as 1 if the participant was digitally ready, and 0 if the participant was not digitally ready. Digital readiness was defined by access to home-based or other internet-accessing devices (computers, tablets, mobile phones, and other devices) and participants' comfort level using such devices).
Age at consent, gender identity, income, and educational attainment were the significant variables associated with digital readiness (p ≤ 0.01). Race, rurality, and sexual orientation status were not significant factors associated with digital readiness. Participants who were 26–35 years of age when completing their primary consent had 46% lower odds of being digitally ready (OR 0.54) compared with their 18- to 25-year-old peers. This trend continued with every decade of age at consent increase. For example, participants who were 36–45 years of age at consent had 71% lower odds (OR 0.29) and those 46–55 years of age at consent had 81% lower odds (OR 0.19), peaking at 76 years or older of age at consent, who had 95% lower odds (OR 0.05) to be digitally ready.
Participants who identified as females had 60% higher odds of being digitally ready (OR 1.58) than those that identified as males. Further analyses showed that FQHC All of Us participants who identified as females were more digitally ready than males at all age groups, races, rurality, incomes, and education levels (data not shown).
Higher income levels were associated with higher digital readiness; participants with income levels greater than $50,000 had 6.5 times higher odds of being digitally ready (OR 6.47) than those with incomes under $10,000. This was the highest OR among all the other demographics included in the study. Educational attainment followed a similar trend as income levels. Participants with a high school degree had 53% higher odds of being digitally ready (OR 1.53) than those without a high school degree, and those with a college degree or more had five times higher odds of being digitally ready (OR 5.89) compared with their less-than-high-school participants.
3.2. Digital readiness impact on retention of participants in the program at FQHCs
As described earlier, most of activities required by All of Us that qualify a participant to be considered retained (except submitting bio samples to Biobank) are completed on a web-based portal. The online portal can be accessed by the participants when they come in-person to the FQHCs or virtually from a computer or a mobile device. The instructions for participants to complete the retention activities are often sent via mail as paper copies, or electronically by email or text messages, based on the participant's preferences indicated when joining the Program. Therefore, digital readiness plays a key role in the ability to retain participants in the Program.
Results showing the retention impact of digital readiness on FQHC participants in All of Us are shown in Figure 3 (Model 2). Significant variables from Model 1, which included age when consenting to the Program, income, educational attainment, and gender identity, were used for propensity score weighting in Model 2. Results from both unweighted and weighted (using IPTW propensity score methodology) models are shown. A complete table containing OR and 95% CI values for both unweighted and weighted models is included in the Supplementary Table S2 of this paper.
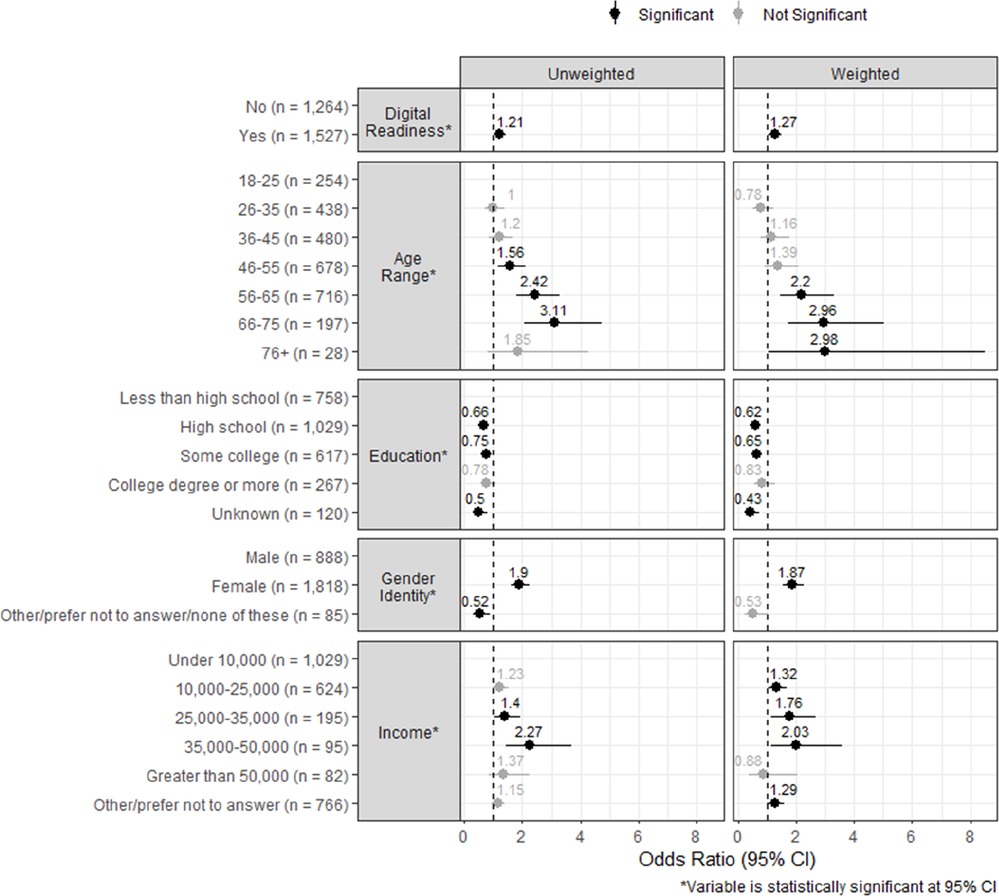
Figure 3. Results from weighted and unweighted models to understand the impact of digital readiness on retaining participants at FQHCs. (Outcome variable: Retention Status. Coded as 1 if the participant was retained, and 0 if the participant was never retained. Retained participants complete follow-up surveys on a web-based portal at least once every 18 months after their enrollment, indicating sustained engagement after recruitment to the Program).
Digital readiness significantly increased the odds of a participant being retained in the Program; the odds were 21% higher with the unweighted model (OR 1.21) and 27% higher in the case of IPTW model (OR 1.27). Additionally, the odds of never being retained were significantly associated with lower age at consent, lower income, and participants identifying as male.
The odds of being retained in the Program overlapped with participant groups with higher digital readiness (i.e., higher income and participants identifying as female), except for age at consent and educational attainment. Older participants had higher odds of being retained, even though they were less digitally ready than their younger peers. Participants who were 56–65 years of age at consent had two times higher odds of being retained (OR 2.2) than those who were 18–25 years of age at consent; at 66–75 years of age at consent, they had three times higher odds (OR 2.96). This observation suggests that older participants often completed retention activities through in-person appointments with FQHC staff during their clinical visits. Older participants might be making more frequent in-person clinical visits to the FQHCs and/or may have more time available, thereby providing more opportunities for the All of Us staff to engage them in-person for completing retention activities. Increase in education level did not increase the odds of being retained.
Findings from Models 1 and 2 indicate that participants who were digitally ready had 27% higher odds of being retained in the Program than those who were not digitally ready. Participants with higher income, higher educational attainment, and from lower age groups were all associated with digital readiness. While the odds of digital readiness increased with increase in education level, it did not increase the odds of being retained. Participants who were not digitally ready, such as those from older age groups, but made in-person clinical visits to the FQHCs benefited from All of Us staff supporting them in completing retention activities, thereby compensating for their lack of digital readiness. The models also suggest that younger participants, despite their association with being digitally ready, had lower odds of ever being retained, indicating that motivating participants from younger age groups to complete the Program retention activities at FQHCs is a significant challenge, particularly as they may be making less frequent visits for healthcare.
3.3. Qualitative findings on the strategies FQHCs are using for retaining participants in All of Us
In June 2022, 11 FQHC All of Us staff members participated in a focus group to share their strategies for retaining participants in the Program. The strategies were focused on pre-pandemic scenarios given the scope of the analysis included in this paper, but some of the findings could be applicable during the pandemic. The key takeaways are summarized in Table 5.
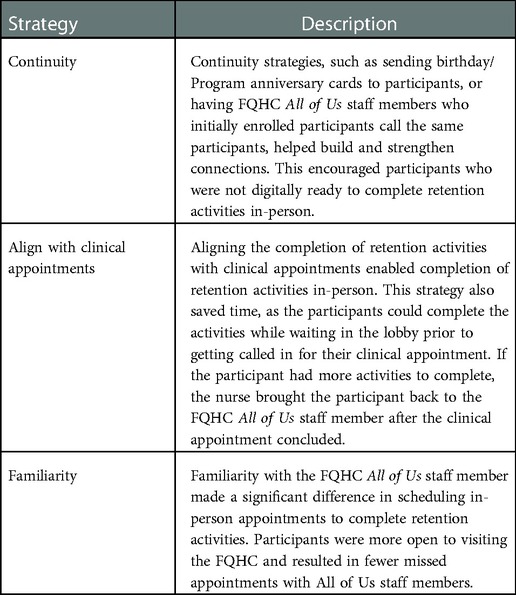
Table 5. Summary of Strategies used by FQHCs for Retaining Participants in All of Us.
Many of the strategies described in Table 5 further strengthen the findings from quantitative analyses. FQHC focus group members shared that aligning All of Us activities with clinical appointments was an especially effective strategy for older participants since they typically made more frequent in-person visits to FQHCs. They added that older participants enjoyed the company of having someone to talk to, liked to stay longer, and appreciated the service and personalized attention. This point further strengthens findings from the quantitative analysis that digital accessibility disposition for older participants had low to no impact on being retained into the Program at FQHCs.
Familiarity with a participant's digital readiness was another strategy that provides additional insights on the quantitative results. FQHCs shared that the All of Us staff recorded detailed notes from prior appointments about whether the participant completed all retention activities independently (vs. needing staff assistance) and their comfort using technology to determine the level of assistance needed. This allowed for the staff to be well prepared to support participant needs for completing Program activities.
4. Conclusions
The data presented in this paper demonstrate significant overlap between participants who are not digitally ready and those with low income, who are less educated, and of increased age. The representation of these UBR groups in clinical trials, along with longitudinal data collection, is critical to designing medical countermeasures that benefit the entire United States population and can potentially provide inference for populations around the globe. Longitudinal data collection efforts can embed measures to mitigate this disproportionate impact on UBR populations. Opportunities exist in the provision of culturally sustaining outreach and engagement to support retention, mitigating lack of digital readiness by ancillary services that bridge the gap between All of Us and participants who are not digitally ready, or provision of internet or internet-accessing devices to vulnerable groups.
5. Limitations
There were some limitations to this study, primarily due to constraints on the study design. The MCM survey questionnaire was not developed specifically for this research study. It was developed to understand the general characteristics of the population groups that FQHCs enroll. Therefore, our study was limited by the data that was already collected.
The MCM survey questions were asked by FQHC staff to all participants at their time of enrollment in All of Us. However, per the IRB requirements, participants were given a choice to decline responding to the MCM survey entirely or skip any of the questions. This may have introduced bias in our study sample. Out of a total of 3,552 participants enrolled by FQHCs during the study time-period, 2,897 participants chose to respond to MCM survey (82% response rate). Of the 2,897 that responded, 106 participants skipped one or more of the three MCM technology questions and were excluded (3.6%), potentially introducing selection bias. For example, these participants could have skipped the questions because they may not have access to technology devices (computers, tablets, mobile phones, and other devices) and were not comfortable stating it on the survey. Had these limitations not existed, we hypothesize that the magnitude of the quantified impact would only be greater.
The three MCM questions on technology access and participants' comfort level to using technology were used to develop a definition for digital readiness. While there is no universally established definition for digital readiness, the definition used in the study deviates from previous studies, which may limit the study's comparability with others. Some studies have used the term “digital divide”, focused on the gap between those who do and do not have access to information technology, regardless of their comfort with technology (24). Another definition of digital readiness is based on technology access, comfort level and trust (25).
Finally, the results of this study must be considered in the context of this longitudinal data collection effort, and may not generalize to other research efforts, each of which has its own definition of retention, incentive structure, and may have a vastly different study population. However, despite the limitations, the study provides timely and insightful contribution by quantifying the impact of digital readiness in recruiting and sustaining UBR population groups in longitudinal data collection.
Data availability statement
The data analyzed in this study is subject to the following licenses/restrictions: The datasets generated during and/or analyzed in this study are available from the corresponding author on reasonable request, and subject to approval from NIH. Requests to access these datasets should be directed toc2tpbmlAbWl0cmUub3Jn.
Ethics statement
The studies involving human participants were reviewed and approved by All of Us (AoU) Institutional Review Board (IRB). AoU IRB Protocol Number: 2017-06. The patients/participants provided their written informed consent to participate in this study.
Author contributions
SK and DD: contributed to conceiving the study, authored the manuscript and are equal contributors. SK: led the data analytics team, engaged FQHCs for qualitative inputs on retention strategies, and wrote the manuscript. DD: led the data clean up, validated study population, and contributed to model development. JW: contributed to the Propensity Score Weighted Model methodology development. All authors contributed to the article and approved the submitted version.
Funding
The authors disclose receipt of the following financial support for the research, authorship, and/or publication of this article: The work reported in this article was supported by the U.S. Department of Health and Human Services Contract 75FCMC18D0047, Task Order 75N98019F01202. Approved for Public Release; Distribution Unlimited. Public Release Case Number: 22-2696.
This (software/technical data) was produced for the U. S. Government under Contract Number 75FCMC18D0047, and is subject to Federal Acquisition Regulation Clause 52.227-14, Rights in Data-32 General.
No other use other than that granted to the U. S. Government, or to those acting on behalf of the U. S. Government under that Clause is authorized without the express written permission of The MITRE Corporation.
For further information, please contact The MITRE Corporation, Contracts Management Office, 7515 Colshire Drive, McLean, VA 22102-7539, (703) 983-6000.
Acknowledgments
The authors wish to acknowledge the members of the All of Us Research Program at the MITRE Corporation, led by Jessica Burke and Derek Inokuchi. The authors acknowledge Shmona Simpson on the initial conceptualization and drafting of the manuscript. Other members of the MITRE project team that contributed to the development of this paper include Maureen Leahy and Matthew McQueen. The authors thank the NIH Program Officer, Sarra Hedden for her leadership and support. The authors would also like to thank the All of Us Research Program team at each FQHC for their dedication to our participants and the Program. A huge debt of gratitude is owed to the participants of the All of Us Research Program, past and present, who voluntarily give their time to support this longitudinal data collection.
Conflict of interest
SK, DD and JW were employed by The MITRE Corporation when this work was carried out. The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. All of Us Research Program Investigators, Denny JC, Rutter JL, Goldstein DB, Philippakis A, Smoller JW, Jenkins G, et al. The “All of Us” research program. N Engl J Med. (2019) 381:668–76. doi: 10.1056/NEJMsr1809937
2. Mapes BM, Foster CS, Kusnoor SV, Epelbaum MI, AuYoung M, Jenkins G, et al. Diversity and inclusion for the All of Us research program: a scoping review. PLoS One. (2020) 15:e0234962. doi: 10.1371/journal.pone.0234962
3. The All of Us Research Program at The MITRE Corporation. Centrally coordinated federally qualified health centers recruit and retain the underrepresented in biomedical research to the All of Us research program. In progress (2022).
4. National Association of Community Health Centers. Available at: https://www.nachc.org/wp-content/uploads/2021/10/NACHC-Brochure-10.8.21.pdf (Accessed June 29, 2022).
5. National Association of Community Health Centers. Available at: https://www.nachc.org/research-and-data/research-fact-sheets-and-infographics/americas-health-centers-2021-snapshot/ (Accessed June 29, 2022).
6. Holko M, Litwin TR, Munoz F, Theisz KI, Salgin L, Jenks NP, et al. Wearable fitness tracker use in federally qualified health center patients: strategies to improve the health of all of us using digital health devices. npj Digit Med. (2020) 5:53. doi: 10.1038/s41746-022-00593-x
7. Fisher ER, Pratt R, Esch R, Kocher M, Wilson K, Lee W, et al. The role of race and ethnicity in views toward and participation in genetic studies and precision medicine research in the United States: a systematic review of qualitative and quantitative studies. Mol Genet Genomic Med. (2020) 8(2):e1099. doi: 10.1002/mgg3.1099
8. U.S. Food and Drug Administration. Office of women’s health; the society for women’s health research. Data presented by Tierney, J. & Sanders, P., in Dialogues on Diversifying Clinical Trials. Washington, DC. Available at: https://www.fda.gov/downloads/ScienceResearch/SpecialTopics/WomensHealthResearch/UCM334959.pdf (September 22, 2011).
9. Vogen EA. Digital divide persists even as Americans with lower incomes make gains in tech adoption. Pew Research Center (2021). Available at: https://www.pewresearch.org/fact-tank/2021/06/22/digital-divide-persists-even-as-americans-with-lower-incomes-make-gains-in-tech-adoption/
10. Tappen RM, Cooley ME, Luckmann R, Panday S. Digital health information disparities in older adults: a mixed methods study. J Racial Ethn Health Disparities. (2021) 9(1):82–92. doi: 10.1007/s40615-020-00931-3
11. Tomer A, Fishbane L, Siefer A, Callahan B. Digital prosperity: How broadband can deliver health and equity to all communities. Washington, DC: Metropolitan Infrastructure Initiative: Brookings Institution (2020).
12. Sieck CJ, Sheon A, Ancker JS, Castek J, Callahan B, Siefer A. Digital inclusion as a social determinant of health. npj Digit Med. (2021) 4(52). doi: 10.1038/s41746-021-00413-8
13. Nebeker C, Murray K, Holub C, Haughton J, Arredondo EM. Acceptance of mobile health in communities underrepresented in biomedical research: barriers and ethical considerations for scientists. JMIR Mhealth Uhealth. (2017) 5(6):e87. doi: 10.2196/mhealth.6494
14. Bender MS, Choi J, Arai S, Paul SM, Gonzalez P, Fukuoka Y. Digital technology ownership, usage, and factors predicting downloading health apps among Caucasian, Filipino, Korean, and Latino Americans: the digital link to health survey. JMIR Mhealth Uhealth. (2014) 2(4):e43. doi: 10.2196/mhealth.3710
15. Choi NG, Dinitto DM. The digital divide among low-income homebound older adults: internet use patterns, eHealth literacy, and attitudes toward computer/internet use. J Med Internet Res. (2013) 15(5):e93. doi: 10.2196/jmir.2645.23639979
16. Montague E, Perchonok J. Health and wellness technology use by historically underserved health consumers: systematic review. J Med Internet Res. (2012) 14(3):e78. doi: 10.2196/jmir.2095
17. National Institutes of Health All of Us Research Program. Data and research center. Available at: https://allofus.nih.gov/funding-and-program-partners/data-and-research-center (Accessed September 9, 2021).
18. R Core Team. R: A language and environment for statistical computing. Vienna, Austria: R Foundation for Statistical Computing (2021). Available at: https://www.r-project.org.
19. RStudio Team. RStudio: Integrated development for R. Boston, MA: RStudio, Inc. (2018). Available at: https://www.rstudio.com.
20. Ellis AR, Brookhart MA. Approaches to inverse-probability-of-treatment—weighted estimation with concurrent treatments. J Clin Epidemiol. (2013) 66(8 Suppl):S51–6. doi: 10.1016/j.jclinepi.2013.03.020
21. Greifer N. WeightIt: Weighting for covariate balance in observational studies. R package version 0.12.0 (2022). Available at: https://cran.r-project.org/web/packages/WeightIt/index.html.
23. Hedden SL, McClain J, Mandich A, Baskir A, Caulder MS, Denny JC, et al. The impact of COVID-19 on the All of Us research program. Am J Epidemiol. (2022). In press. doi: 10.1093/aje/kwac169
24. Hoffman DL, Novak TP, Schlosser AE. Evolution of the digital divide: how gaps in internet access may impact electronic commerce. J Comput Mediat Commun. (2001) 5(3). doi: 10.1111/j.1083-6101.2000.tb00341.x. Available at: https://academic.oup.com/jcmc/article/5/3/JCMC534/4584185.
25. Horrigan J. Digital readiness gaps. Pew Research Center (2016). Available at: https://www.pewresearch.org/internet/2016/09/20/digital-readiness-gaps/.
Keywords: longitudinal data collection, underrepresented in biomedical research (UBR), national institutes of health (NIH), diversity, All of Us research program, healthcare, health disparities, health equity, digital readiness
Citation: Kini S, Duluk D and Weinstein J (2023) Modeling the impact of digital readiness in recruiting and sustaining underrepresented groups: Data from the All of Us research program. Front. Digit. Health 4:1082098. doi: 10.3389/fdgth.2022.1082098
Received: 27 October 2022; Accepted: 13 December 2022;
Published: 13 April 2023.
Edited by:
Adrian Aguilera, University of California, United StatesReviewed by:
Moom Rahman Roosan, Chapman University, United StatesAldenise P. Ewing, The Ohio State University, United States
© 2023 Kini, Duluk and Weinstein. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Soumya Kini c2tpbmlAbWl0cmUub3Jn
†These authors have contributed equally to this work
Specialty Section: This article was submitted to Human Factors and Digital Health, a section of the journal Frontiers in Digital Health