 Jorge M. Rodríguez-Fernández
Jorge M. Rodríguez-Fernández Jeffrey A. Loeb
Jeffrey A. Loeb Daniel B. Hier
Daniel B. Hier
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
PERSPECTIVE article
Front. Digit. Health, 28 November 2022
Sec. Health Informatics
Volume 4 - 2022 | https://doi.org/10.3389/fdgth.2022.1063141
This article is part of the Research TopicThe Digitalization of NeurologyView all 13 articles
Succinct clinical documentation is vital to effective twenty-first-century healthcare. Recent changes in outpatient and inpatient evaluation and management (E/M) guidelines have allowed neurology practices to make changes that reduce the documentation burden and enhance clinical note usability. Despite favorable changes in E/M guidelines, some neurology practices have not moved quickly to change their documentation philosophy. We argue in favor of changes in the design, structure, and implementation of clinical notes that make them shorter yet still information-rich. A move from physician-centric to team documentation can reduce work for physicians. Changing the documentation philosophy from “bigger is better” to “short but sweet” can reduce the documentation burden, streamline the writing and reading of clinical notes, and enhance their utility for medical decision-making, patient education, medical education, and clinical research. We believe that these changes can favorably affect physician well-being without adversely affecting reimbursement.
A crisis in physician well-being and the mounting burden of clinical documentation drives the need for neurologists to change their documentation philosophy. Burnout is prevalent among all healthcare professionals (1) and neurologists in particular (2, 3). Documentation is a known contributor to burnout (1, 4, 5). An estimated 40% of physician time in the electronic health record (EHR) is devoted to documentation (6). In 2015, the American College of Physicians (7) emphasized the importance of writing “concise, history-rich notes” that prioritize information relevant to medical decision-making (MDM). Responding to physician complaints about the burden of EHR documentation, the AMA Current Procedural Terminology Editorial Panel recommended changes to evaluation and management (E/M) documentation guidelines that would reduce the clerical burden (8). On January 1, 2021, the Center for Medicare and Medicaid Services (CMS) updated E/M coding guidelines for outpatient visits that would allow physicians to select a billing level based on the time or complexity of MDM and would reduce documentation requirements for the history and physical examination (including the unpopular bullet point requirements). These requirements were seen as both tedious and time-consuming. Furthermore, they were seen as reducing the time available for direct patient care (6). CMS plans to extend these changes to the inpatient setting (hospital inpatient, hospital observation, emergency department, and cognitive impairment assessment) by January 1, 2023 (9).
Time-based coding allows physicians to bill for time spent outside the patient visit on the day of evaluation, even if the patient is absent (chart review, documentation, orders, coordinating care, etc.) The complexity of medical decision-making (the main driver of billing level) is determined by the number and complexity of the problems addressed, the risk of complications (morbidity and mortality), and the complexity of the data reviewed. These changes simplify setting the correct level of service for billing purposes. For example, a patient with migraine headaches who is started on single-drug therapy has a low level of MDM; a patient with new-onset seizures who needs adjustments of anti-epileptic medications and imaging has a moderate level of MDM; and a patient with epilepsy and poorly-controlled seizures, a structural brain lesion, and who needs neuroimaging, extended electroencephalographic testing, and a surgical consultation has a high-level of MDM.
Initial studies suggest that these CMS changes will enhance reimbursement for Evaluation and Management (E/M) services (10) provided by non-surgical specialties but not by surgical specialties (11). Improvements have not yet been noted in time spent documenting in the EHR (10). Furthermore, to date, no study has determined that these changes in documentation guidelines have lightened provider documentation burden.
In the US, the volume of clinical documentation has increased over the past two decades. It is estimated that US clinicians do three times more documentation than clinicians in other medically advanced countries (12). The are several reasons for the bulkiness of our clinical notes in the US.
• We have been reimbursed more for bulkier notes. Since 1995, the level of service and reimbursement was linked to the number of coding elements (also known as “bullet points”) documented (9).
• It’s too easy to add bulk. Copy and paste functionality in electronic health records makes it easy to add bulk. Hyperlinks make it possible to add laboratory results, radiology findings, problem lists, medication lists, and other chart elements to a note with a single mouse click. One study of over 26,000 physician notes found that only 18% of the text was entered by the physician, 46% was copied from elsewhere in the EHR, and 35% was imported from other sections of the EHR (13). Copy and paste may document care that was never rendered or examinations that were never performed (14).
• We are trained to document negative findings. As Sinsky has observed, we need to move away from the dictum that “If it wasn’t documented, it wasn’t done” (15). Or, as Postal has wondered, do we have the time and energy to document all the negatives or should we stick to the salient positives (16)?
• We continue to document based on reimbursement and tradition rather than scientific evidence. In their essay subtitled “A farewell to the review of systems,” Barry and Tseng argue for deleting the traditional review of systems and that documentation should be based on scientific evidence (17).
A change in documentation philosophy is needed to slim down bloated notes that are hard to read, hard to write, and often inaccurate (Table 1). Copying and pasting text from one note into another fosters bloat, redundancies, and inaccuracies. When long pre-completed templates are used to document the neurological exam, parts of the neurological examination may be documented as normal when these parts were not examined. These documentation practices open the door to litigation. When test results (imaging, electroencephalography, electromyographic, etc.) are added to clinical notes, they should be addressed, discussed, and made relevant to the MDM.
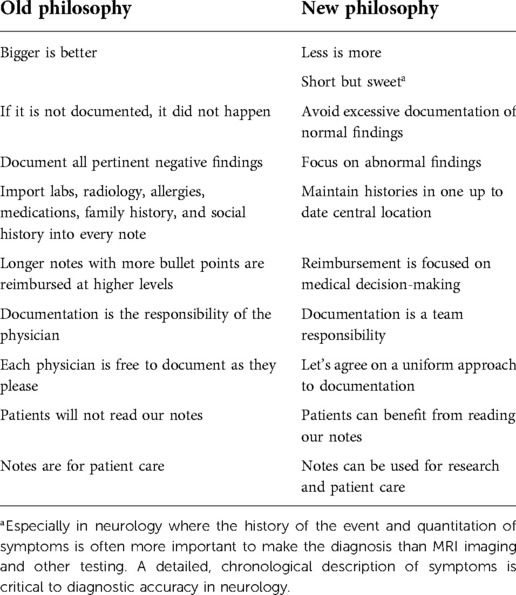
Table 1. Suggested changes in documentation philosophy.
Documentation needs to be clear, accurate, and concise. The emphasis should be on optimal patient care, not maximizing the billable level of care. Neurology departments need to discourage clinicians from the redundant documentation of information. We argue that certain types of medical data (e.g., social history, past medical history, allergies, surgical history, medication lists, laboratory results, and radiology results) are best housed in a central location in the EHR and should not be added to a note unless relevant to MDM. Clinicians need to be trained to document allergies, medications, past medical history, and social history in the appropriate place in the EHR and not redundantly in each note. This practice has multiple advantages: it allows patient care team members to share the work of documentation, it reduces duplicate work, and it reduces multiple and inconsistent versions of the same data.
Notes that have a consistent structure across the organization make notes easier to read and more predictable. Having a single consolidated note template for each department or subspeciality facilitates note maintenance. Detailed documentation of the history or the condition needed by a subspecialist can be collapsed in the EHR or linked elsewhere to not overwhelm the generalist user. In addition to text, developing innovative ways to visualize changes quantitatively in symptoms over time and their response to treatments can enhance the clinician’s perspective on the disease course. An additional benefit of a single template is the option of providing organizational updates or reminders to all template users.
The general SOAP (subjective-objective-assessment-plan) format has been well accepted. With the growing emphasis on MDM, the APSO (assessment-and-subjective-objective) format has grown in popularity. We additionally recommend the following:
• Create an institutional culture that values concise information-rich notes.
• Encourage clinicians to use collapsible sections in their notes to prioritize which sections are visible.
• Standardize the adoption of the SOAP or APSO note format at the organizational level.
• Encourage providers to document pertinent negative and positive findings through direct entry into the EHR rather than by template or copy and paste.
• Discourage providers from using hyperlinks in the EHR to add laboratory and ancillary testing results to notes with unnecessary redundancy when not relevant to MDM.
• Encourage providers to focus on adding those findings to notes that are pertinent to medical decision-making.
• Implement “vanishing text” that allows clinicians to view findings in their notes to support note creation and have it deleted when the note is finalized.
• Discourage the use of pre-completed examination templates with all findings marked as “normal.”
• If radiology or other reports are incorporated into a note, encourage the insertion of the “Impression” paragraph only.
• Look for help from the facility informatics department to create space-saving ways to represent bulky laboratory results as “fish bones” and other laboratory diagrams.
• Use hyperlinks, rather than text insertion, to connect notes to discrete data such as advanced directives or resuscitation status.
• Develop and implement policies that control copy and paste functionality, including highlighting of text that has been pasted into the note (14, 18).
• Use EHR metrics such as note length, time in chart, etc., to track changes in documentation practices by clinicians.
The implementation of these recommendations depends upon proper organizational support. The engagement of key stakeholders, including departmental leadership, compliance officers, billing, coders, clinicians, and clinical informaticians, is critical. Principles and objectives for documentation change must be developed, agreed upon, and implemented. Documentation metrics are crucial to evaluating project success. Key documentation metrics include clinician time in the EHR, clinician time spent documenting outside of regular work hours, and time spent writing notes (19). We additionally suggest tracking mean note length over time. These metrics can demonstrate project success tangibly to leadership and clinicians.
The use of sprints or PDSA (plan-do-study-act) cycles can address implementation barriers before and after project roll-out. Departmental support is critical to assisting physicians in adjusting to new documentation methods. Iterative sprints and cycles are recommended to foster change. Although some documentation changes are driven by CMS, other regulatory agencies might have specific documentation requirements that require compliance, such as quality measures related to stroke (20). Interdisciplinary teams tasked with documentation change must address documentation compliance issues for each sub-specialty.
OpenNotes is coming. Federal legislation under the 21st Century Cures Act provides patients access to notes without delay and charge by April 5, 2021 (21). The OpenNotes initiative seeks to provide patients with access to their medical records (22) to improve their understanding of their condition and give patients more control of their treatment plan. Open communication with the patient during the visit combined with succinct understandable notes supports co-ownership of medical problems by patient and clinician (23–28). Long-term outcomes from the OpenNotes initiative on patient satisfaction and patient condition are still being evaluated.
As neurologists, we must recognize that patients will be reading our notes. For some sensitive conditions, this may be problematic. For example, in neurology, we often evaluate patients with functional disorders who have a limited understanding of the causes and nature of their condition. Neurologists must be open and should provide transparent communication with the patient at the time of evaluation and while creating their notes. Patients with functional disorders may find terms such as “non-physiological” or “no neurological correlate” confusing. These patients deserve a clear explanation of their symptoms in the office and in our notes (29, 30) Lastly, concerns on disclosure and result interpretation of sensitive testing for diseases such as Alzheimer’s disease have been raised, and efforts to develop ethical and patient-centered policies for disclosure are needed (31).
The goal of team-based documentation is to offload some of the documentation work from the physician to other team members. Team-based documentation may variably involve scribes, nurses, pharmacists, medical assistants, or artificial intelligence-based dictation devices (32). Some team-based care models distribute specific documentation tasks such as recording allergies, documenting past medical history, and reconciling medication to specific team members (33). When these tasks are done before the initial interaction between patient and clinician, clinician time and effort are conserved. Other team-based documentation models use scribes to free up clinician time at the point of patient contact (32).
Clinical documentation is central to the education of medical students, residents, and fellows (34). Although uniformity in documentation templates and methods is a stated goal, it is important to flex documentation expectations according to the level of training. Although it is reasonable to expect a medical student to document their neurological examination and history in great detail, the same is not true for an advanced fellow or experienced attending neurologist. While longer notes are de rigeur for medical students, we expect experienced clinicians to write concise notes with few notations about normal findings. Still, we should encourage medical students to focus on succinct formulations of the neurological examination and history. Academic institutions can take advantage of current E/M guideline changes to encourage trainees to document concisely, to prioritize MDM, and to avoid adding uninformative “bullet points” (35, 36). Documentation metrics can guide trainees and their mentors to adopt the best documentation strategies.
Although the primary purpose of physician notes in the EHR is to document care rendered, to support the billing for services provided, and to serve as a medical-legal record; electronic health records and free text physician notes have shown great potential for clinical research (37–39). For example, EHRs are being used to track disease severity, and progression in cohorts of patients with amyotrophic lateral sclerosis and multiple sclerosis (40–42). Natural language processing and other artificial intelligence algorithms are unlocking latent value in EHRs. Unlike skimpy information-poor notes or bloated information-poor notes, concise information-rich clinical notes can be of great value for clinical research.
For over two decades, our clinical notes have grown too long. They are a significant burden and contribute to physician burnout. This Perspective describes recommendations to simplify documentation that can be implemented because of changes in CMS guidelines for evaluation and management coding and billing. We argue that it is time to rethink our documentation to enhance communication, improve patient care, and reduce physician burnout. Although more work is needed to find optimal strategies to reduce the documentation burden, it is not too early to start creating notes that are easy to write and read yet are still information-rich. Bulky notes waste the time of the writer and the reader alike. Evidence is growing that when concerted efforts are made to simplify documentation, physician satisfaction with the EHR improves, and burnout is reduced (43–45).
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author/s.
Initial concept by JMRF and DBH. Concept elaboration by DBH, JAL, and JMRF. Initial draft by JMRF. Revisions and rewriting by JMRF, JAL, and DBH. All authors contributed to the article and approved the submitted version.
JAL was supported in part by the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health, through Grant Award Number UL1TR002003 (JAL). The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Shanafelt TD, Dyrbye LN, Sinsky C, Hasan O, Satele D, Sloan J, et al. Relationship between clerical burden, characteristics of the electronic environment with physician burnout, professional satisfaction. Mayo Clin Proc. (2016) 91:836–48. doi: 10.1016/j.mayocp.2016.05.007
2. Busis NA, Shanafelt TD, Keran CM, Levin KH, Schwarz HB, Molano JR, et al. Burnout, career satisfaction, and well-being among us neurologists in 2016. Neurology. (2017) 88:797–808. doi: 10.1212/WNL.0000000000003640
3. Levin KH, Shanafelt TD, Keran CM, Busis NA, Foster LA, Molano JRV, et al. Burnout, career satisfaction, and well-being among us neurology residents and fellows in 2016. Neurology. (2017) 89:492–501. doi: 10.1212/WNL.0000000000004135
4. Peccoralo LA, Kaplan CA, Pietrzak RH, Charney DS, Ripp JA. The impact of time spent on the electronic health record after work and of clerical work on burnout among clinical faculty. J Am Med Inform Assoc. (2021) 28:938–47. doi: 10.1093/jamia/ocaa349
5. Tajirian T, Stergiopoulos V, Strudwick G, Sequeira L, Sanches M, Kemp J, et al. The influence of electronic health record use on physician burnout: cross-sectional survey. J Med Internet Res. (2020) 22:e19274. doi: 10.2196/19274
6. Sinsky C, Colligan L, Li L, Prgomet M, Reynolds S, Goeders L, et al. Allocation of physician time in ambulatory practice: a time and motion study in 4 specialties. Ann Intern Med. (2016) 165:753–60. doi: 10.7326/M16-0961
7. Kuhn T, Basch P, Barr M, Yackel T, Medical Informatics Committee of the American College of Physicians. Clinical documentation in the 21st century: executive summary of a policy position paper from the American College of Physicians. Ann Intern Med. (2015) 162:301–3. doi: 10.7326/M14-2128
8. American Medical Association and others. CPT® evaluation and management (E/M) office or other outpatient (99202–99215) and prolonged services (99354: 99355, 99356, 99417) code and guideline changes (2021).
9. Centers for Medicare and Medicaid Services. Calendar year (CY) 2023 medicare physician fee schedule proposed rule (2022). Available at https://www.ama–assn.org/practice–management/sustainability/joy–medicine–health–system–recognition–program.
10. Apathy NC, Hare AJ, Fendrich S, Cross DA. Early changes in billing and notes after evaluation and management guideline change. Ann Intern Med. (2022) 175:499–504. doi: 10.7326/M21-4402
11. Francis DL, Cruddas BM. 2021 E/M code changes: forecasted impacts to gastroenterology practices. Clin Gastroenterol Hepatol. (2021) 19:2002–5. doi: 10.1016/j.cgh.2021.07.008
12. Downing NL, Bates DW, Longhurst CA. Physician burnout in the electronic health record era: are we ignoring the real cause? Ann Intern Med. (2018) 169:50–1. doi: 10.7326/M18-0139
13. Wang MD, Khanna R, Najafi N. Characterizing the source of text in electronic health record progress notes. JAMA Intern Med. (2017) 177:1212–3. doi: 10.1001/jamainternmed.2017.1548
14. Turchin A, Goldberg SI, Breydo E, Shubina M, Einbinder JS. Copy/paste documentation of lifestyle counseling and glycemic control in patients with diabetes: true to form? Arch Intern Med. (2011) 171:1393–400. doi: 10.1001/archinternmed.2011.219
15. Berg S. 3 ways to begin to reduce clinical documentation by 75% by 2025. Available at https://www.ama–assn.org/practice–management/sustainability/3–ways–begin–reduce–clinical–documentation–75–2025 (Accessed September 21, 2022).
16. Postal E. The impertinence of pertinent negatives. Available at https://www.diagnosticimaging.com/view/impertinence–pertinent–negatives (Accessed September 21, 2022).
17. Barry MJ, Tseng CW. Moving to more evidence-based primary care encounters: a farewell to the review of systems. JAMA (2022) 328:1495–6. doi: 10.1001/jama.2022.18346
18. Tsou AY, Lehmann CU, Michel J, Solomon R, Possanza L, Gandhi T. Safe practices for copy, paste in the EHR. Appl Clin Inform. (2017) 26:12–34. doi: 10.4338/ACI-2016-09-R-0150
19. Melnick ER, Ong SY, Fong A, Socrates V, Ratwani RM, Nath B, et al. Characterizing physician EHR use with vendor derived data: a feasibility study and cross-sectional analysis. J Am Med Inform Assoc. (2021) 28:1383–92. doi: 10.1093/jamia/ocab011
20. The Joint Commission. Stroke. Available at https://www.jointcommission.org/measurement/measures/stroke/ (Accessed September 21, 2022).
21. Office of the National Coordinator for Health Information Technology. The ONC Cures act final rule (2020). Available at https://www.healthit.gov/sites/default/files/page2/2020–03/TheONCCuresActFinalRule.pdf.
22. Arvisais-Anhalt S, Lau M, Lehmann CU, Holmgren AJ, Medford RJ, Ramirez CM, et al. The 21st century cures act, multiuser electronic health record access: potential pitfalls of information release. J Med Internet Res. (2022) 24:e34085. doi: 10.2196/34085
23. Walker J, Leveille S, Bell S, Chimowitz H, Dong Z, Elmore JG, et al. Opennotes after 7 years: patient experiences with ongoing access to their clinicians’ outpatient visit notes. J Med Internet Res. (2019) 21:e13876. doi: 10.2196/13876
24. DesRoches CM, Leveille S, Bell SK, Dong ZJ, Elmore JG, Fernandez L, et al. The views and experiences of clinicians sharing medical record notes with patients. JAMA Netw Open. (2020) 3:e201753. doi: 10.1001/jamanetworkopen.2020.1753
25. Blease C, Torous J, Hägglund M. Does patient access to clinical notes change documentation? Front Public Health. (2020) 8:577896. doi: 10.3389/fpubh.2020.577896
26. Klein JW, Jackson SL, Bell SK, Anselmo MK, Walker J, Delbanco T, et al. Your patient is now reading your note: opportunities, problems, and prospects. Am J Med. (2016) 129:1018–21. doi: 10.1016/j.amjmed.2016.05.015
27. Delbanco T, Walker J, Bell SK, Darer JD, Elmore JG, Farag N, et al. Inviting patients to read their doctors’ notes: a quasi-experimental study and a look ahead. Ann Intern Med. (2012) 157:461–70. doi: 10.7326/0003-4819-157-7-201210020-00002
28. DesRoches CM, Bell SK, Dong Z, Elmore J, Fernandez L, Fitzgerald P, et al. Patients managing medications and reading their visit notes: a survey of opennotes participants. Ann Intern Med. (2019) 171:69–71. doi: 10.7326/M18-3197
29. Keatley E, Molton I. A shift in approach: assessment and treatment of adults with functional neurological disorder. J Health Serv Psychol. (2022) 48:79–87. doi: 10.1007/s42843-022-00061-w
30. Stone J, Burton C, Carson A. Recognising and explaining functional neurological disorder. BMJ. (2020) 371:m3745. doi: 10.1136/bmj.m3745
31. Gale SA, Heidebrink J, Grill J, Graff-Radford J, Jicha GA, Menard W, et al. Preclinical alzheimer disease and the electronic health record: balancing confidentiality and care. Neurology (2022). doi: 10.1212/WNL.0000000000201347. https://n.neurology.org/content/neurology/early/2022/09/30/WNL.0000000000201347.full.pdf36180237
32. Lin S. The present and future of team documentation: the role of patients, families, and artificial intelligence. Mayo Clin Proc. (2020) 95:852–5. doi: 10.1016/j.mayocp.2020.01.034
33. Hopkins K, Sinsky CA. Team-based care: saving time and improving efficiency. Fam Pract Manag. (2014) 21:23–9. Available at: https://pubmed.ncbi.nlm.nih.gov/25403048/25403048
34. Wei M, Salgado E, Girard CE, Santoro JD, Lepore N. Your note, your way: how to write an inpatient progress note accurately and efficiently as an intern. Postgrad Med J. (2022). Available at: https://pmj.bmj.com/content/early/2022/07/07/postgradmedj-2022-141834.info
35. Oxentenko AS, West CP, Popkave C, Weinberger SE, Kolars JC. Time spent on clinical documentation: a survey of internal medicine residents and program directors. Arch Intern Med. (2010) 170:377–80. doi: 10.1001/archinternmed.2009.534
36. Varacallo MA, Wolf M, Herman MJ. Improving orthopedic resident knowledge of documentation, coding, and medicare fraud. J Surg Educ. (2017) 74:794–8. doi: 10.1016/j.jsurg.2017.02.003
37. Alzoubi H, Alzubi R, Ramzan N, West D, Al-Hadhrami T, Alazab M. A review of automatic phenotyping approaches using electronic health records. Electronics. (2019) 8:1235. doi: 10.3390/electronics8111235
38. Fu S, Chen D, He H, Liu S, Moon S, Peterson KJ, et al. Clinical concept extraction: a methodology review. J Biomed Inform. (2020) 109:103526. doi: 10.1016/j.jbi.2020.103526
39. Shickel B, Tighe PJ, Bihorac A, Rashidi P. Deep EHR: a survey of recent advances in deep learning techniques for electronic health record (EHR) analysis. IEEE J Biomed Health Inform. (2017) 22:1589–604. doi: 10.1109/JBHI.2017.2767063
40. Yang Z, Pou-Prom C, Jones A, Banning M, Dai D, Mamdani M, et al. Assessment of natural language processing methods for ascertaining the expanded disability status scale score from the electronic health records of patients with multiple sclerosis: algorithm development and validation study. JMIR Med Inform. (2022) 10:e25157. doi: 10.2196/25157
41. Xia Z, Secor E, Chibnik LB, Bove RM, Cheng S, Chitnis T, et al. Modeling disease severity in multiple sclerosis using electronic health records. PLoS ONE. (2013) 8:e78927. doi: 10.1371/journal.pone.0078927
42. Karanevich AG, Weisbrod LJ, Jawdat O, Barohn RJ, Gajewski BJ, He J, et al. Using automated electronic medical record data extraction to model ALS survival and progression. BMC Neurol. (2018) 18:1–7. doi: 10.1186/s12883-018-1208-z
43. Sieja A, Markley K, Pell J, Gonzalez C, Redig B, Kneeland P, et al. Optimization sprints: improving clinician satisfaction and teamwork by rapidly reducing electronic health record burden. Mayo Clin Proc. (2019) 94:793–802. doi: 10.1016/j.mayocp.2018.08.036
44. Nguyen OT, Jenkins NJ, Khanna N, Shah S, Gartland AJ, Turner K, et al. A systematic review of contributing factors of and solutions to electronic health record–related impacts on physician well-being. J Am Med Inform Assoc. (2021) 28:974–84. doi: 10.1093/jamia/ocaa339
Keywords: electronic health records, documentation burden, clinician well-being, evaluation and management coding, medical decision-making
Citation: Rodríguez-Fernández JM, Loeb JA and Hier DB (2022) It’s time to change our documentation philosophy: writing better neurology notes without the burnout. Front. Digit. Health 4:1063141. doi: 10.3389/fdgth.2022.1063141
Received: 6 October 2022; Accepted: 10 November 2022;
Published: 28 November 2022.
Edited by:
Qingyu Chen, National Center for Biotechnology Information, National Library of Medicine (NIH), United StatesReviewed by:
Tian Kang, Tempus Labs, United States© 2022 Rodríguez-Fernández, Loeb and Hier. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jorge M. Rodríguez-Fernández am9ybXJvZHJAdXRtYi5lZHU=
Specialty Section: This article was submitted to Health Informatics, a section of the journal Frontiers in Digital Health
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.