 Nele A. J. De Witte
Nele A. J. De Witte Steven Joris
Steven Joris Eva Van Assche
Eva Van Assche Tom Van Daele
Tom Van Daele- Expertise Unit Psychology, Technology & Society, Thomas More University of Applied Sciences, Antwerp, Belgium
Background: Research increasingly shows how selective and targeted use of technology within care and welfare can have several advantages including improved quality of care and active user involvement.
Purpose: The current overview of reviews aims to summarize the research on the effectiveness of technology for mental health and wellbeing. The goal is to highlight and structure the diverse combinations of technologies and interventions used so far, rather than to summarize the effectiveness of singular approaches.
Methods: The current overview includes reviews published in the past five years with a focus on effectiveness of digital and technological interventions targeting mental health and wellbeing.
Results: A total of 246 reviews could be included. All reviews examined the effectiveness of digital and technological interventions in the context of care and welfare. A combination of two taxonomies was created through qualitative analysis, based on the retrieved interventions and technologies in the reviews. Review classification shows a predominance of reviews on psychotherapeutic interventions using computers and smartphones. It is furthermore shown that when smartphone applications as stand-alone technology are researched, the primary focus is on self-help, and that extended reality is the most researched emerging technology to date.
Conclusion: This overview of reviews shows that a wide range of interventions and technologies, with varying focus and target populations, have been studied in the field of care and wellbeing. The current overview of reviews is a first step to add structure to this rapidly changing field and may guide both researchers and clinicians in further exploring the evidence-base of particular approaches.
Introduction
Within the broad field of healthcare and welfare a wide range of services are offered which are aimed at promoting the wellbeing and mental health of individuals. While the context and target populations can vary substantially, professionals in this field share many interventions which often rely on face-to-face interactions. However, digital technologies can also support these services, either stand-alone or in combination with an existing service offer. New technologies can allow for more flexibility, can offer interventions in the natural context, can reach a larger population without risk of stigma, and can be more cost-effective as compared to existing services (1, 2). Research increasingly shows how selective and targeted use of technology can have a meaningful impact on the quality of care and the role users can take in the organization and delivery of services (3). For example, users may be able to have more control over their care, especially in the context of chronic illness (4).
Nevertheless, there is a sharp contrast between what is technically possible and the amount of research that has actually been done so far. As a result, there are an overwhelming number of options, which hampers overview. To address this, attempts have already been made to structure parts of the field, for example for specific technologies, e.g., internet-supported mental health interventions (5, 6), smartphone apps (7) or for particular domains, e.g., for emotion regulation in clinical psychology (8). The current overview of reviews aims to extend those previous endeavors by expanding the scope to all technologies applied to the broad domain of mental health and wellbeing. The goal is to structure existing technologies and interventions which have been the focus of reviews, rather than to summarize the effectiveness of singular approaches. By summarizing the large body of research to date and by highlighting both similarities and differences across approaches and settings, we hope to further structure this domain and to inform about gaps in research that currently still exists.
Materials and Methods
This review was preregistered in the Open Science Framework as part of a larger study (https://osf.io/hdxky).
Search Strategy
The databases Scopus and Web of Sciences were searched on 4 January 2021 for reviews written in English and published in the past five years with a focus on effectiveness of digital and technological interventions in the field of care and welfare. A combination of two sets of search terms was used, one with a focus on technological interventions and the other on wellbeing. The search string was as follows: (websites OR “smartphone app*” OR wearable OR “virtual reality” OR “augmented reality” OR “immersive technology” OR platform OR mhealth OR “mobile health” OR ehealth OR “e-mental health” OR e-health OR internet OR mail OR chat) AND (“mental health*” OR “mental wellbeing” OR “social support” OR “psychological support” OR psycholog* OR psychiatr* OR “mental illness” OR “mental disorder” OR “quality of life”).
Inclusion and Exclusion Criteria
Articles were included if they were systematic reviews, meta-analyses, scoping reviews, or overviews of reviews with an exclusive focus on the efficacy of technological tools or interventions in the context of mental health, wellbeing, or quality of life. No limitations were placed on the setting, control condition, or population, which could consist of participants of all ages of the general population, at-risk groups or individuals with underlying conditions. Studies were excluded if the focus was on strictly medical applications, lab research, assistive technology for disability, mere feasibility of technology, and if research took place among low- and middle-income countries.
Literature Screening and Data Extraction
The online review platform Covidence (https://www.covidence.org) was used, which aims to facilitate screening and data extraction with multiple reviewers. Titles, abstracts and full texts were screened by two independent reviewers in each phase. Conflicts were resolved through discussion. A data extraction template was designed to extract the characteristics of each included study. Reviews were categorized regarding:
(1) Focus: prevention, treatment, or relapse prevention.
(2) Target population, or the intended audience of the reviewed interventions: general population, at-risk population, somatic disorders, pain or neurological disorders, substance use, mental illness, or other.
(3) Age: children and young adults, adults, or elderly.
(4) Setting: home, outpatient, or residential.
(5) Integration with conventional care: online, blended.
The included reviews were also labeled according to the intervention(s) and implemented technology(/ies) through inductive qualitative analysis with the goal of creating a taxonomy. Three authors independently developed an intervention and technology taxonomy based on 50 included reviews. These categorizations were subsequently compared, and the final matrix combining interventions and technologies was developed through discussion. All reviews were subsequently labeled according to these taxonomies. A review could load on multiple interventions and technologies simultaneously. After data extraction was complete, each entry was checked for errors in extraction by the first author.
For a number of combinations of interventions and technologies a review was selected and its focus described, to briefly illustrate what each combination might. Three criteria for selection were put forward: (1) the review is the most recent available, (2) the review is of high-quality, as determined by the JBI Critical Appraisal Checklist for Systematic Reviews and Research Syntheses [a maximum of four negative evaluations; (9)], and (3) the review focuses on the combination of a single methodology and technology.
Results
Study Identification
The systematic search strategy yielded 6,113 results. The selection process is visually summarized in a PRISMA flowchart (10) in Figure 1. A total of 246 reviews could be included. All reviews examined the effectiveness of digital and technological interventions in the context of care and welfare. The reviews were diverse in scope and the quality of the studies they retrieved varied greatly (cfr. supra, review illustrations). Each review included an average of 16 studies, with outliers ranging from 1 to 111 studies.
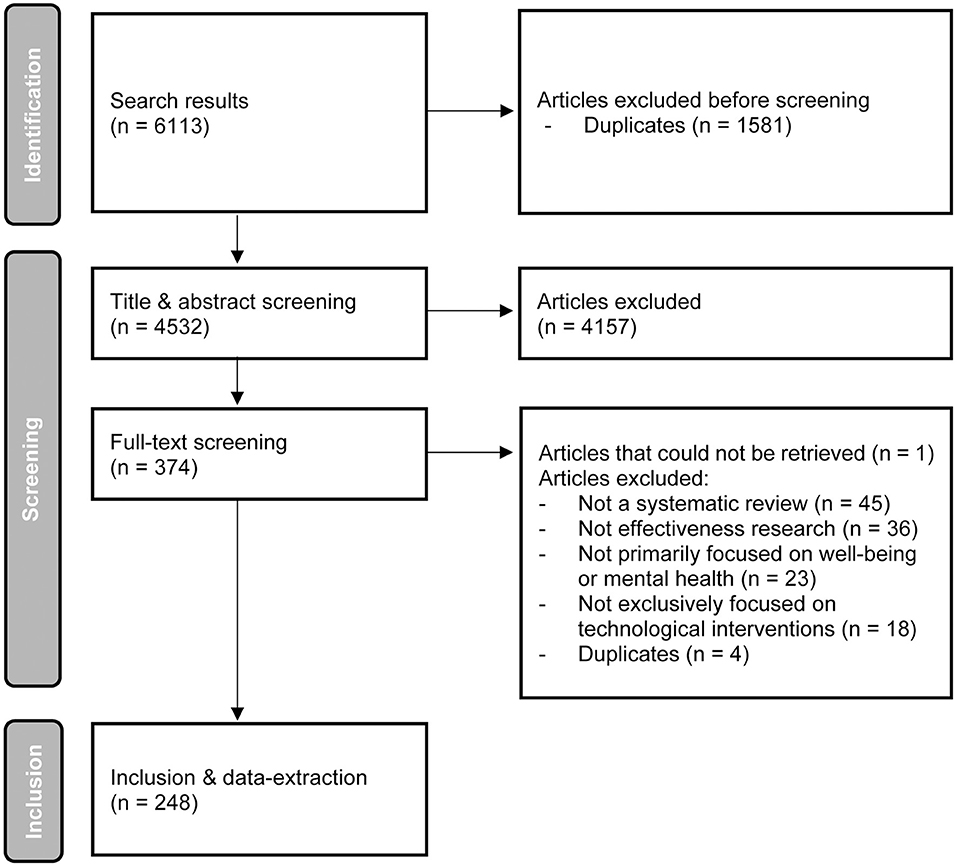
Figure 1. PRISMA flowchart.
Characteristics of Reviews
A detailed overview of the characteristics of each review can be found in Supplementary Table 1. Results show that most reviews focused on treatment (N = 196). Prevention was also fairly common (N = 107), but only a limited number of reviews examined applications for relapse prevention or maintenance of treatment effects (N = 20). In line with the focus on treatment or, in this context, psychotherapy, the largest subset of reviews had an (exclusive) focus on individuals with mental illness (N = 142; Figure 2). This was followed by the general population (N = 58) and somatic conditions (N = 56). The “other” category of Figure 2 consisted of informal caregivers (N = 22) and perinatal women (N = 9). A third of the studies focused on more than one target group in their review (e.g., both general population and at risk populations). In terms of age group, most studies focus primarily on adults (N = 203). However, there are also several studies that focus on children to young adults (N = 81). The age group that is currently understudied in systematic reviews is the older population (N = 23). Since most reviews do not clearly indicate the setting in which the studies took place (e.g., outpatient or residential), it was not possible to formally categorize reviews on this behalf. In general, however, many interventions were offered in the home setting. Additionally, interventions also took place in outpatient care, residential care, school/university setting, and the work context. Finally, there were only three reviews that clearly and explicitly examined blended care (a combination of online and face-to-face contact). Most reviews examined interventions that were entirely digital or did not clearly report whether complementary face-to-face contact was provided.
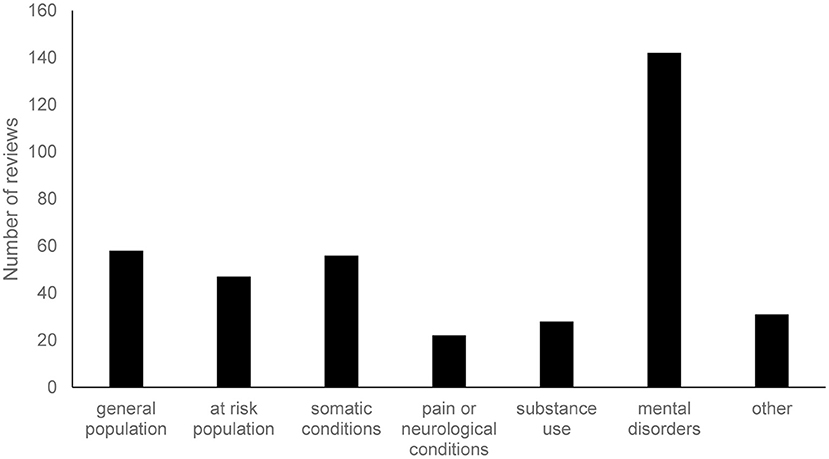
Figure 2. Target groups of the included reviews. Each review could be assigned multiple categories.
Taxonomies
The taxonomy concerning interventions consists of 9 types, which are described in Table 1 and can be considered as an operationalization of the mental health intervention spectrum of mental disorders, developed by Mrazek and Haggerty (23).
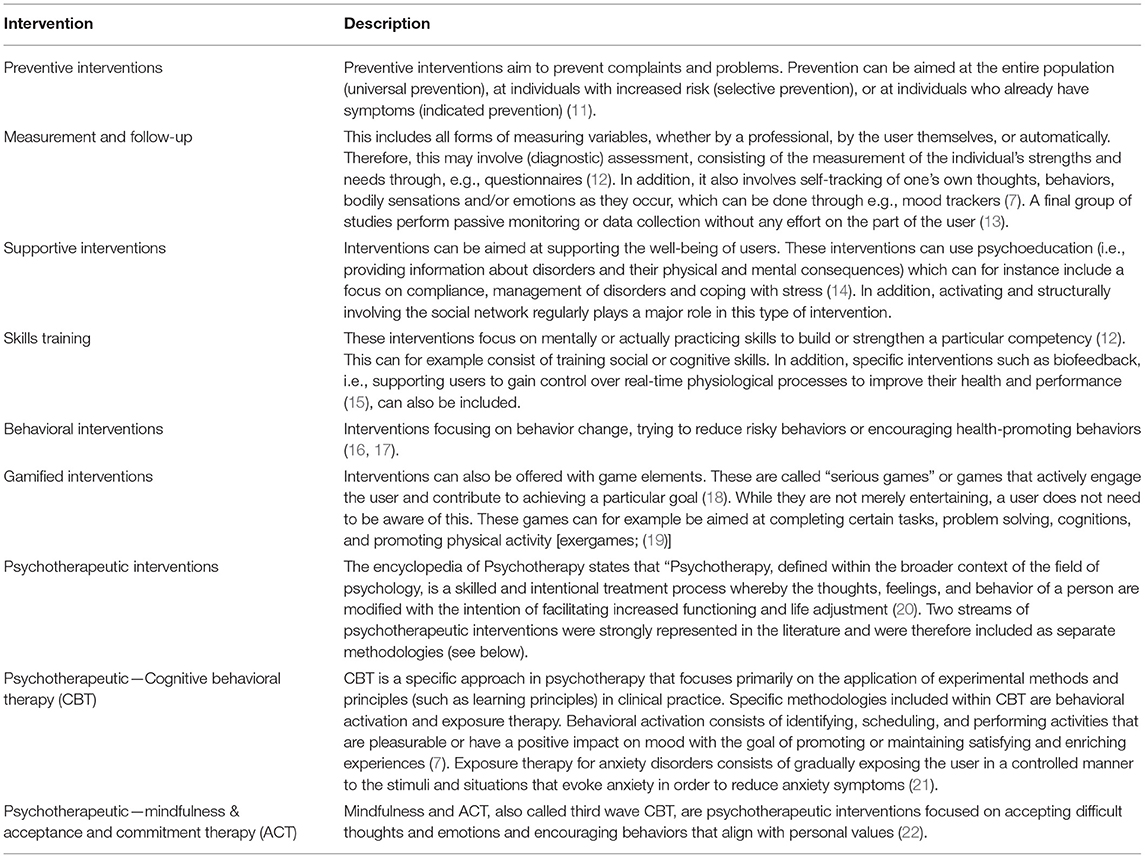
Table 1. Taxonomy of interventions determined through inductive qualitative analysis, and their description.
Three broad clusters of technologies can be distinguished: a first is technologies taking conventional care online. A second is technology to be used as (stand-alone) interventions. Finally, there are emerging technologies, on which there may already be substantial research evidence, but which have not necessarily been (frequently) implemented in clinical practice up to now. Table 2 provides an overview of the taxonomy of technologies.
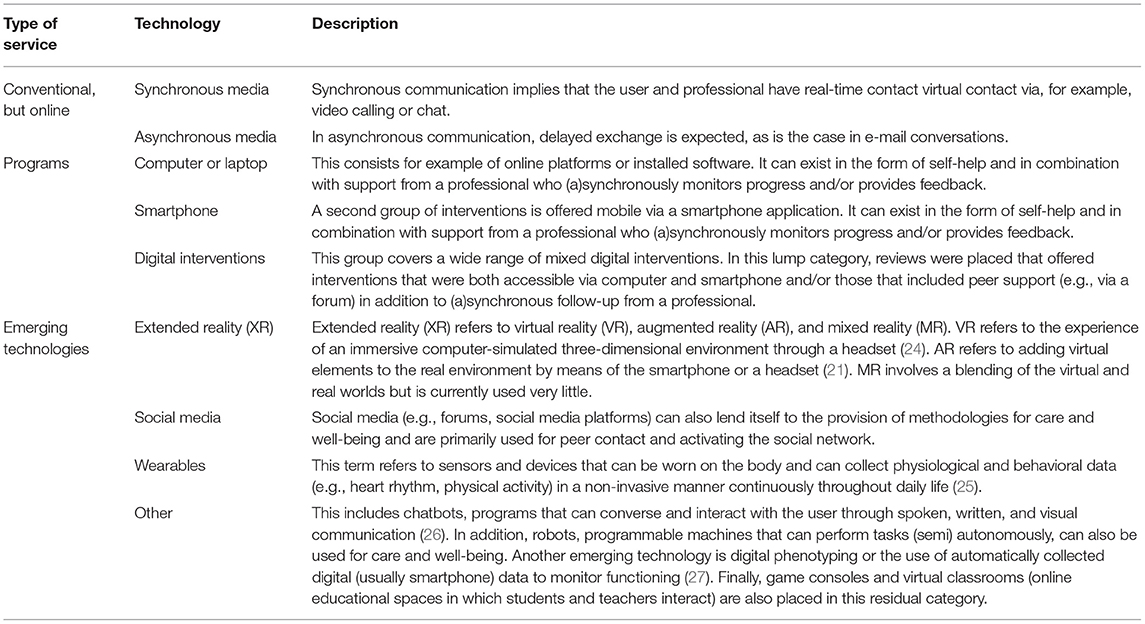
Table 2. Taxonomy of implemented technologies, determined through inductive qualitative analysis, and their description.
Technological and digital interventions rely on the combination of a technical component and an intervention. The retrieved reviews can thereby be categorized under several interventions and/or technology forms. The matrix in Table 3 should therefore not be viewed as an exhaustive overview of possible combinations of interventions and technologies. What can be derived from it are common and less common combinations of technologies and interventions and the relative difference in weight of the various possible combinations.
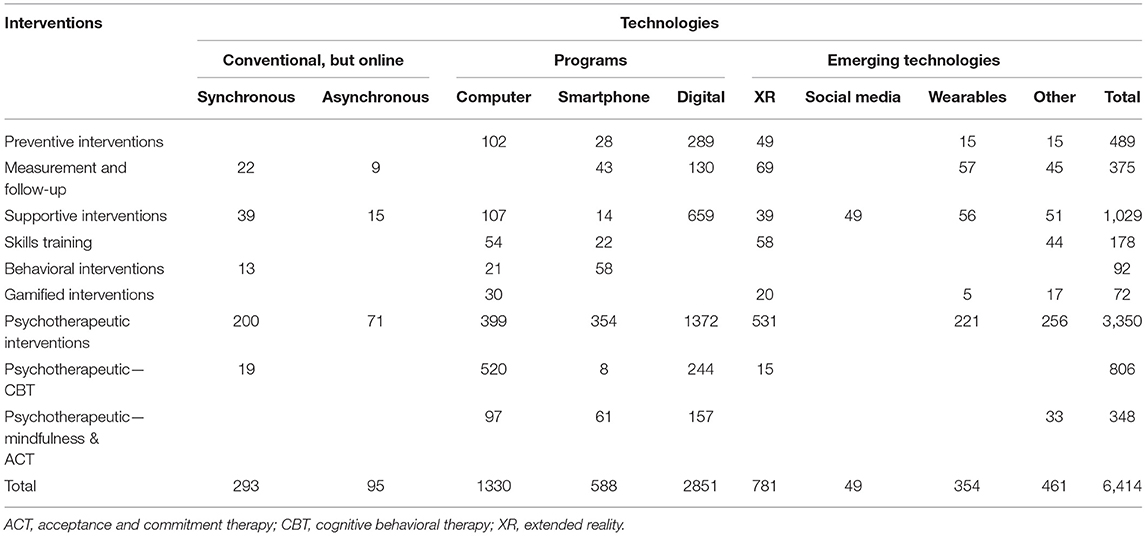
Table 3. Overview of the number of studies retrieved in the reviews for combinations of interventions and technologies.
The overview in Table 3 shows that the focal point of research into technological and digital interventions for mental health and wellbeing is on interventions offered through computer, smartphone, or a combination of both.
Programs can be offered in the form of mere self-help or can include some form of (mainly digital) support from a professional. Table 4 provides an overview of the number of studies included in the reviews that discuss pure self-help in relation to studies that (also) include interventions that are supported by a professional. While the majority of studies on smartphone applications are limited to self-help, studies exploring computerized programs do more commonly include professional support. Conventional services delivered online are less represented. In terms of emerging technologies, studies using VR and wearables are most common. When inspecting the interventions, and in line with the predominance of samples with mental disorders, psychotherapeutic interventions are strongly represented in the literature. Supportive interventions are also common and mostly target informal caregivers and individuals with somatic conditions.
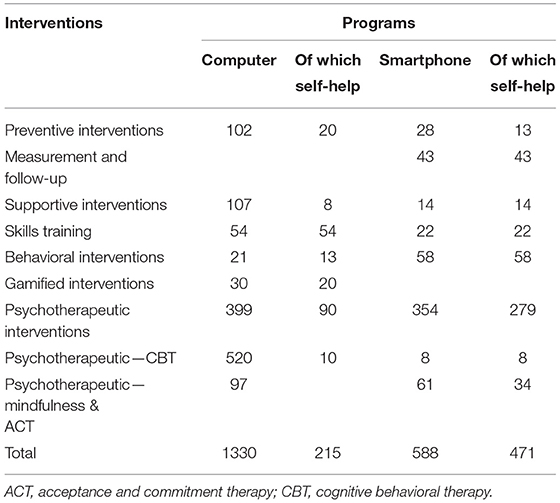
Table 4. Overview of the number of studies retrieved in the reviews for combinations focusing on interventions and self-help.
Illustrations of Reviews Within the Combination of Both Taxonomies
Discussing each of the 246 studies would lead us to far. To nevertheless offer some insight into both taxonomies, we briefly describe the most common combinations of technologies and interventions. For that purpose, we choose the most frequent combinations within the three technological clusters defined earlier and selected the review meeting all three criteria defined earlier. The JBI quality assessments of all retrieved studies can be found in Supplementary Table 2.
Conventional Approach Using (a)Synchronous Technologies
Corry et al. (28) focused on synchronous technology and supportive interventions. They conducted a systematic review on telephone interventions delivered by healthcare professionals, for providing education and psychosocial support to informal caregivers of adults with diagnosed illnesses. The combination of asynchronous technology and psychotherapeutic interventions was reviewed by Senanayake et al. (29). In text messaging interventions for the management of depression, texts were being used for various purposes: therapeutic, motivational and supportive.
Programs Supported by Technology
Digital programs were explored in combination with a wide variety of interventions, for example with preventive interventions in the context of technology-enhanced youth suicide prevention and interventions (30). Others were combined with measurement and follow-up, using digital interventions for routine outcome monitoring (ROM) and measurement-based care (MBC), the routine use of outcome measurement to guide treatment decisions of patients receiving face-to-face psychotherapy (31). Leng et al. (32) furthermore focused on the potential of combing digital programs and supportive interventions, more specifically the use of digital interventions to support informal caregivers of people with dementia. Victorson et al. (33), finally, explored the combination with psychotherapeutic interventions—ACT and mindfulness when looking into technology-enabled mindfulness-based programs.
Self-help smartphone programs were either most commonly combined with behavioral interventions or with psychotherapeutic interventions. On the one hand, a systematic review by Milne-Ives et al. (34) focused for example on the effectiveness of smartphone apps for health behavior change, in physical activity, diet, drug and alcohol use, and mental health. On the other hand, Ilagan et al. (35) looked into psychotherapeutic interventions targeting borderline personality disorder (BDP) symptoms like anger, suicidality and self-harm, using smartphone apps. These apps were used to set up safety plans, to help patients track their mood, or to facilitate emotion regulation exercises.
Computer programs often looked into psychotherapeutic interventions, both general or CBT, but were also used in the context of skills training. Dugdale et al. (36) summarized current evidence on the potential of computer-based treatment programs to reduce symptoms of substance misuse and mental health difficulties in adults with a dual diagnosis. Following an initial screening, users could for example access an interactive coping strategy training, which helped them to address the lifestyle factors which are maintaining their harmful alcohol consumption. Eilert et al. (37) conducted a systematic review and meta-analysis on the effectiveness of computer-based treatment for generalized anxiety disorder. All but one of the online interventions included some form of human support alongside the intervention and most were primarily based on CBT. To be more specific, interventions relied on (a combination of) psychoeducation, case examples, mindfulness and/or relaxation exercises, notification and/or reminder emails, homework, summaries, and relapse prevention and maintenance. Finally, a scoping review by Zhang et al. (38) assessed the potential of computer-based cognitive bias modification interventions. These interventions, for which evidence initially emerged from experimental psychology, aim to retrain automatic attention to stimuli that are either harmful (e.g., in the context of substance abuse) or threatening (e.g., in the context of social anxiety disorder). In order to do so, participants for example completed online series of modified Stroop tasks. In these tasks, the computer presented them with series of threatening and neutral words, in varying colors. Every time, participants were asked to name the color of these words, while ignoring their semantic content.
Emerging Technologies
XR was most commonly used in combination with psychotherapeutic interventions—CBT. Kothgassner and Felnhofer (39) examined the effectiveness of virtual reality exposure therapy (VRET) for the treatment of anxiety disorders in children and adolescents. Social media, in turn was most frequently combined with supportive interventions. Ridout and Campbell (40) conducted a systematic review on the current evidence base for using social networking sites as a means to deliver mental health interventions for young people up to the age of 25, particularly for sharing knowledge and providing peer-to-peer support. Wearables were often used for measurement and follow-up and were for example used to unobtrusively measure and monitor depressive symptoms in children and adolescents (41). Chatbots were applied in the context of pychotherapeutic interventions, for example in the review by Abd-Alrazaq et al. (26) who explored to what extent chatbots might meet the needs of people with mental health conditions, in particular people with symptoms of depression, anxiety and stress and acrophobia. Emerging technologies which are less frequent in current literature are digital phenotyping and robots. Cornet and Holden (13) looked into the potential of digital phenotyping for health and wellbeing and found that smartphones were most commonly used to capture accelerometery, location, audio, and usage data, for example with patients with bipolar disorder or schizophrenia. The obtained data were primarily used for unobtrusive monitoring. Finally, Scoglio et al. (42) was the only review with an exclusive focus on robots, but found only a very limited number of studies to date.
Discussion
The current overview of reviews on technological and digital interventions in the field of care and welfare shows that there is a large diversity, both in terms of interventions and technologies used. Although the focus is mainly on treatment, a relevant portion of the reviews also consider a preventive approach. Furthermore, both in the case of young people and adults, the reviews focus on a wide variety of target groups. No clear-cut differences regarding these target groups were found amongst the diversity of retrieved reviews, aside from the fact that supportive interventions mostly targeted informal caregivers and individuals with somatic conditions. Technologies most frequently researched are programs, both on computers, smartphones, or cross-platform digital environments (74% of all study categorizations). Not only emerging technologies (e.g., XR), but also technologies that allow conventional therapy to take place online (e.g., video calling) have been the focus of research far less often. Remarkably, an explicit focus on blended interventions is largely absent from the reviews. Combining online and face-to-face offerings is often cited as the most promising avenue for technological and digital interventions in care and welfare (43). However, only three of the 246 reviews appear to explicitly focus on this.
A classification matrix focusing on the type of technology and the content of the activity or intervention was created through qualitative analysis. This proved challenging as many reviews included a wide range of interventions. While the current solution can help to understand the variety of possible interventions and gaps in research and practice, other ways of classification are also possible and have been proposed. The list of treatment elements and definitions for the classification of smartphone apps by Wasil et al. (7) for example demonstrated that psychoeducation, relaxation and medication were the three most common elements in smartphone apps. Since our study goes beyond smartphone apps and focuses on reviews that each include a broad range of treatment elements, a categorization at a higher level was warranted. Fernandez-Álvarez et al. (8) recently made a similar attempt to structure current research on digital technologies for the intervention of emotion regulation, in which a distinction was made between three distinct categories: digital technologies (1) to understand process and outcome (e.g., (bio)sensors, (2) to create new interventions (e.g., bio- and neurofeedback and XR) and (3) to disseminate psychological treatments [e.g., (un)guided interventions and videoconferencing psychotherapy]. Although their categorization is solely focused on emotion regulation, the structuring does show similarities to the current overview of review. However, as our study took a more systematic approach and looked at combinations of technologies and interventions in a broader field, it might offer better insights in current gaps and potential opportunities. The potential of XR is for example not limited to creating new interventions, but might very well also be used to understand process and outcome. A structuring of the field using the combination of two taxonomies therefore seems to better allow for a flexible categorization of (future) studies.
The focus of future research can be twofold. Firstly, it can further explore novel combinations of interventions and technologies, as combining both taxonomies resulted in a 9 x 9 matrix. This implies that, theoretically, 81 combinations could be made of different technologies and interventions. However, no studies were retrieved for 31 of those combinations (38%). This might lead one to conclude that the different forms of technology have only been used rather one-sided so far. However, not every technology is necessarily suitable for every intervention. Nevertheless, there are various technologies included in the matrix that are still recent: research on these paradigms has therefore only recently started developing. Those emerging technologies have currently been relatively understudied, except for XR, where virtual reality already has an extensive and long-standing research tradition, but is only now gradually making its way into practice. Secondly, even more established combinations need further strengthening, especially those who already see strong uptake in clinical practice. To be more specific, this overview for example shows that (self-help) smartphone apps and programs, which are currently already frequently disseminated in practice, have not been the focus of as much research as often might be thought.
There are also limitations to the current study. Given the broad scope of our overview and the large number of reviews retrieved, we opted to rely on the count of studies within reviews as an indication for the amount of research that has been conducted to date. This obviously does not provide a proper indication of the actual evidence-base for particular combinations of technologies and interventions. We are therefore cautious in our interpretations and see the current overview primarily as a way to provide a structuring of a very broad field, which is currently still in the midst of expanding. Also important to note is that this overview was set up in the context of a broader study on the potential of technological and digital interventions for Flanders, a region and community in Belgium. To assure sufficient local relevance of the literature overview, it was therefore limited to only include reviews with a focus on high-income countries. In the initial abstract screening process several articles were excluded focusing on low to middle income countries. Digital interventions seem (also) most prevalent there as well, although the number of studies specifically taking these contexts into account are still limited (44).
Taken together, the current overview shows that technological and digital interventions in the field of care and welfare can vary substantially in terms of the aims for which they are used, their focus, and target population. Overall, reviews focusing on effectiveness of such applications do appear to have mostly concentrated on psychotherapeutic interventions for mental illness offered through computers and smartphones. Regardless of the underlying rationale, however, adding structure to this diverse and rapidly expanding field helps to offer some insights in current (lack) of evidence-base of certain technologies and interventions that rely on them.
Author Contributions
EV, SJ, and ND created the taxonomy. All authors contributed to the screening process and participated in the data extraction and the writing of the manuscript.
Funding
The funding for this overview was provided by the Policy Research Centre Welfare, Public Health and Family of the Flemish Government (Project EF73).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
We would like to thank the reviewers, as well as the members of the project's advisory board and particularly the chair of the board, Loes Houthuys, for their reflections and constructive input.
Supplementary Material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fdgth.2021.754337/full#supplementary-material
References
1. Ebert DD, Van Daele T, Nordgreen T, Karekla M, Compare A, Zarbo C, et al. Internet- and mobile-based psychological interventions: applications, efficacy, and potential for improving mental health: a report of the EFPA E-Health Taskforce. Eur. Psychol. (2018) 23:167–87. doi: 10.1027/1016-9040/a000318
2. Musiat P, Goldstone P, Tarrier N. Understanding the acceptability of e-mental health - attitudes and expectations towards computerised self-help treatments for mental health problems. BMC Psychiatry. (2014) 14:1–8. doi: 10.1186/1471-244X-14-109
3. Van Daele T, Karekla M, Kassianos AP, Compare A, Haddouk L, Salgado J, et al. Recommendations for policy and practice of telepsychotherapy and e-mental health in Europe and beyond. J Psychother Integr. (2020) 30:160–173. doi: 10.1037/int0000218
4. Karekla M, Kasinopoulos O, Neto D, Ebert DD, Van Daele T, Nordgreen T, et al. Best practices and recommendations for digital interventions to improve engagement and adherence in chronic illness sufferers. Eur Psychol. (2019) 24:49–67. doi: 10.1027/1016-9040/a000349
5. Barak A, Klein B, Proudfoot JG. Defining internet-supported therapeutic interventions. Ann Behav Med. (2009) 38:4–17. doi: 10.1007/s12160-009-9130-7
6. Barak A, Grohol JM. Current and future trends in Internet-supported mental health interventions. J Technol Hum Serv. (2011) 29:155–96. doi: 10.1080/15228835.2011.616939
7. Wasil AR, Gillespie S, Patel R, Petre A, Venturo-Conerly KE, Shingleton RM, et al. Reassessing evidence-based content in popular smartphone apps for depression and anxiety: developing and applying user-adjusted analyses. J Consult Clin Psychol. (2020) 88:983–93. doi: 10.1037/ccp0000604
8. Fernandez-Álvarez J, Díaz-García A, Colombo D, Botella C, Cipresso P, Riva G. Digital Technologies for the Intervention of Emotion Regulation. In: Reference Module in Neuroscience and Biobehavioral Psychology. Edinburgh: Elsevier (2020). doi: 10.1016/B978-0-12-818697-8.00033-9
9. Joanna Briggs Institute. Checklist for Systematic Reviews Research Syntheses. Adelaide, SA: Jonna Briggs Institute (2017). Available online at: https://joannabriggs.org/sites/default/files/2019-05/JBI_Critical_Appraisal-Checklist_for_Systematic_Reviews2017_0.pdf
10. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
11. Deady M, Choi I, Calvo RA, Glozier N, Christensen H, Harvey SB. eHealth interventions for the prevention of depression and anxiety in the general population: a systematic review and meta-analysis. BMC Psychiatry. (2017) 17:310. doi: 10.1186/s12888-017-1473-1
12. Lindsey MA, Brandt NE, Becker KD, Lee BR, Barth RP, Daleiden EL, et al. Identifying the common elements of treatment engagement interventions in children's mental health services. Clin Child Fam Psychol Rev. (2014) 17:283–98. doi: 10.1007/s10567-013-0163-x
13. Cornet VP, Holden RJ. Systematic review of smartphone-based passive sensing for health and wellbeing. J Biomed Inform. (2018) 77:120–32. doi: 10.1016/j.jbi.2017.12.008
14. Bártolo A, Pacheco E, Rodrigues F, Pereira A, Monteiro S, Santos IM. Effectiveness of psycho-educational interventions with telecommunication technologies on emotional distress and quality of life of adult cancer patients: a systematic review. Disabil Rehabil. (2019) 41:870–8. doi: 10.1080/09638288.2017.1411534
15. De Witte NAJ, Buyck I, Van Daele T. Combining biofeedback with stress management interventions: a systematic review of physiological and psychological effects. Appl Psychophysiol Biofeedback. (2019) 44:71–82. doi: 10.1007/s10484-018-09427-7
16. Hutton, A., Prichard, I., Whitehead, D., Thomas, S., Rubin, M., Sloand, E., et al. mHealth interventions to reduce alcohol use in young people: a systematic review of the literature. Compr Child Adolesc Nurs. (2020) 43:171–202 doi: 10.1080/24694193.2019.1616008
17. Young CL, Trapani K, Dawson S, O'Neil A, Kay-Lambkin F, Berk M, et al. Efficacy of online lifestyle interventions targeting lifestyle behaviour change in depressed populations: a systematic review. Aust N Z J Psychiatry. (2018) 52:834–46. doi: 10.1177/0004867418788659
18. Susi T, Johannesson M, Backlund P. Serious Games: An Overview. Skövde: School of Humanities and Informatics, University of Skövde (2007).
19. Lau HM, Smit JH, Fleming TM, Riper H. Serious games for mental health: are they accessible, feasible, and effective? a systematic review and meta-analysis. Front Psychiatry. (2017) 7:209. doi: 10.3389/fpsyt.2016.00209
20. Lambert MJ, Vermeersch DA. Effectiveness of psychotherapy. In: Lambert MJ, Bergin AE, and Garfield LS, editors. Encyclopedia of Psychotherapy. Amsterdam: Elsevier Science (1994). p. 709–14. doi: 10.1016/B0-12-343010-0/00084-2
21. De Witte NAJ, Scheveneels S, Sels R, Debard G, Hermans D, Van Daele T. Augmenting exposure therapy: mobile augmented reality for specific phobia. Front Virtual Real. (2020) 1:8. doi: 10.3389/frvir.2020.00008
22. Brown M, Glendenning A, Hoon AE, John A. Effectiveness of web-delivered acceptance and commitment therapy in relation to mental health and well-being: a systematic review and meta-analysis. J Med Internet Res. (2016) 18:e221. doi: 10.2196/jmir.6200
23. Mrazek, P. J., and Haggerty, R. J., (eds.). Reducing risks for mental disorders: Frontiers for preventive intervention research. Washington, DC: National Academy Press (1994).
24. Bisso E, Signorelli MS, Milazzo M, Maglia M, Polosa R, Aguglia E, et al. Immersive virtual reality applications in schizophrenia spectrum therapy: a systematic review. Int J Environ Res Public Health. (2020) 17:6111. doi: 10.3390/ijerph17176111
25. Debard G, De Witte N, Sels R, Mertens M, Van Daele T, Bonroy B. Making wearable technology available in mental healthcare through an online platform with stress detection algorithms: the Carewear project. J Sensors. (2020) 2020:8846077. doi: 10.1155/2020/8846077
26. Abd-Alrazaq AA, Rababeh A, Alajlani M, Bewick BM, Househ M. Effectiveness and Safety of using chatbots to improve mental health: systematic review and meta-analysis. J Med Internet Res. (2020) 22:e16021. doi: 10.2196/16021
27. Buneviciene I, Mekary RA, Smith TR, Onnela J, Bunevicius A. Can mHealth interventions improve quality of life of cancer patients? A systematic review and meta-analysis. Critic Rev Oncol Hematol. (2021) 157:103123. doi: 10.1016/j.critrevonc.2020.103123
28. Corry M, Neenan K, Brabyn S, Sheaf G, Smith V. Telephone interventions, delivered by healthcare professionals, for providing education and psychosocial support for informal caregivers of adults with diagnosed illnesses. Cochrane Database Syst Rev. (2019) 5:CD012533. doi: 10.1002/14651858.CD012533.pub2
29. Senanayake B, Wickramasinghe SI, Chatfield MD, Hansen J, Edirippulige S, Smith AC. Effectiveness of text messaging interventions for the management of depression: A systematic review and meta-analysis. J Telemed Telecare. (2019) 25:513–23. doi: 10.1177/1357633X19875852
30. Szlyk H, Tan J. The role of technology and the continuum of care for youth suicidality: systematic review. J Med Internet Res. (2020) 22:e18672. doi: 10.2196/18672
31. Gual-Montolio P, Martínez-Borba V, Bretón-López JM, Osma J, Suso-Ribera C. How are information and communication technologies supporting routine outcome monitoring and measurement-based care in psychotherapy? A systematic review. Int J Environ Res Public Health. (2020) 17:3170. doi: 10.3390/ijerph17093170
32. Leng M, Zhao Y, Xiao H, Li C, Wang Z. Internet-based supportive interventions for family caregivers of people with dementia: systematic review and meta-analysis. J Med Internet Res. (2020) 22:e19468. doi: 10.2196/19468
33. Victorson DE, Sauer CM, Wolters L, Maletich C, Lukoff K, Sufrin N. Meta-analysis of technology-enabled mindfulness-based programs for negative affect and mindful awareness. Mindfulness. (2020) 11:1884–99. doi: 10.1007/s12671-020-01373-y
34. Milne-Ives M, Lam C, De Cock C, Van Velthoven MH, Meinert E. Mobile apps for health behavior change in physical activity, diet, drug and alcohol use, and mental health: Systematic review. JMIR mHealth uHealth. (2020) 8:e17046. doi: 10.2196/17046
35. Ilagan GS, Iliakis EA, Wilks CR, Vahia IV, Choi-Kain LW. Smartphone applications targeting borderline personality disorder symptoms: a systematic review and meta-analysis. Borderline Personal Disord Emot Dysregul. (2020) 7:1–15. doi: 10.1186/s40479-020-00127-5
36. Dugdale S, Elison-Davies S, Semper H, Ward J, Davies G. Are computer-based treatment programs effective at reducing symptoms of substance misuse and mental health difficulties within adults? A systematic review. J Dual Diagn. (2019) 15:291–311. doi: 10.1080/15504263.2019.1652381
37. Eilert N, Enrique A, Wogan R, Mooney O, Timulak L, Richards D. The effectiveness of Internet-delivered treatment for generalized anxiety disorder: an updated systematic review and meta-analysis. Depress Anxiety. (2021) 38:196–219. doi: 10.1002/da.23115
38. Zhang M, Ying J, Song G, Fung DS, Smith H. Attention and cognitive bias modification apps: review of the literature and of commercially available apps. JMIR mHealth uHealth. (2018) 6:e10034. doi: 10.2196/10034
39. Kothgassner OD, Felnhofer A. Lack of research on efficacy of virtual reality exposure therapy (VRET) for anxiety disorders in children and adolescents. Neuropsychiatr. (2021) 35:68–75. doi: 10.1007/s40211-020-00349-7
40. Ridout B, Campbell A. The use of social networking sites in mental health interventions for young people: systematic review. J Med Internet Res. (2018) 20:e12244. doi: 10.2196/12244
41. Sequeira L, Perrotta S, LaGrassa J, Merikangas K, Kreindler D, Kundur D, et al. Mobile and wearable technology for monitoring depressive symptoms in children and adolescents: a scoping review. J Affect Disord. (2020) 265:314–24. doi: 10.1016/j.jad.2019.11.156
42. Scoglio AA, Reilly ED, Gorman JA, Drebing CE. Use of social robots in mental health and well-being research: systematic review. J Med Internet Res. (2019) 21:e13322. doi: 10.2196/13322
43. Ruwaard J, Kok R. Wild west eHealth: time to hold our horses? Eur Health Psychol. (2015) 17:45–9.
44. Carter H, Araya R, Anjur K, Deng D, Naslund JA. The emergence of digital mental health in low-income and middle-income countries: a review of recent advances and implications for the treatment and prevention of mental disorders. J Psychiatr Res. (2020) 133:223–46. doi: 10.1016/j.jpsychires.2020.12.016
Keywords: digital applications (apps), digital mental health, wellbeing, technologies, interventions
Citation: De Witte NAJ, Joris S, Van Assche E and Van Daele T (2021) Technological and Digital Interventions for Mental Health and Wellbeing: An Overview of Systematic Reviews. Front. Digit. Health 3:754337. doi: 10.3389/fdgth.2021.754337
Received: 06 August 2021; Accepted: 07 December 2021;
Published: 23 December 2021.
Edited by:
Marcela Tiburcio, National Institute of Psychiatry Ramon de la Fuente Muñiz (INPRFM), MexicoReviewed by:
Simon D'Alfonso, The University of Melbourne, AustraliaClaire R. van Genugten, VU Amsterdam, Netherlands
Copyright © 2021 De Witte, Joris, Van Assche and Van Daele. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tom Van Daele, dG9tLnZhbmRhZWxlQHRob21hc21vcmUuYmU=