 Heidi Gazelle
Heidi Gazelle Jessie K. Shafer Lundin
Jessie K. Shafer Lundin Haochen Lei
Haochen Lei Hongyuan Cao
Hongyuan Cao Meghan Litchfield
Meghan Litchfield- 1Social Development Lab, Department of Human Development and Family Science, Florida State University, Tallahassee, FL, United States
- 2Department of Psychology, Northern Arizona University–Yuma, Yuma, AZ, United States
- 3Department of Statistics, Florida State University, Tallahassee, FL, United States
This systematic review and set of five meta-analyses synthesized the results of prospective longitudinal publications on childhood and/or adolescent social withdrawal as a predictor of adult psychosocial adjustment. Meta-analyses were conducted with results for five adult outcomes from 31 publications derived from 14 longitudinal samples and a combined sample size of 19,806 adults (50% women, M = 38.88 years, 83% White) with childhood and/or adolescent ( ≤ 16 years) histories of social withdrawal and their offspring (N = 175). Dependency among publications derived from the same longitudinal samples was explicitly modeled in meta-analyses with clustering. Meta-analytic results support childhood and/or adolescent social withdrawal as a medium-sized risk factor for adult social anxiety and intergenerational difficulties in mothers and their offspring (both p < 0.0001); a small-size risk factor for delayed adult developmental milestones (p < 0.05), adult social withdrawal (p < 0.0001), other anxiety (p < 0.05), and depression (p < 0.01); and a small-size protective factor against adult substance use (p < 0.01). However, meta-analytic results did not support childhood and/or adolescent social withdrawal as a predictor of physical health, likely due to the heterogeneous nature of the investigated health outcomes. Consistent with a Developmental Science Model, results are interpreted as supporting interpersonal mechanisms (missing out, interpersonal stress, and poor relationship quality) and developmental cascades (cross domain-influences) in socially withdrawn children's life-course development. Because evidence for intergenerational difficulties was based on a single longitudinal sample, confidence in intergenerational effects would be increased by replication in other samples. Heterogeneity among effect sizes included in most meta-analyses suggests that the relation between childhood and/or adolescent social withdrawal and adult outcomes is likely to be moderated by other factors. Future directions in this area of research are discussed.
1 Introduction
Are children and adolescents who demonstrate social withdrawal in social contexts with familiar peers (e.g., play alone at school recess, sit alone at school lunch) at risk for psychosocial maladjustment in adulthood? In this systematic review and set of meta-analyses of long-term prospective longitudinal studies of psychosocial adjustment in adults with childhood and adolescent histories of social withdrawal, we test whether existing evidence supports childhood and adolescent social withdrawal as a predictor of five forms of adult psychosocial maladjustment: delays in adult developmental milestones for participation in families (e.g., marriage, procreation) and society (e.g., education, occupation), adult social withdrawal and internalizing difficulties (social anxiety, other anxiety, depression), substance use, physical health, and intergenerational difficulties. Because of the long-term nature of the longitudinal studies required to address this query, the number of eligible publications across relevant adult outcomes (n = 33, 31 publications with sufficient information to calculate effect sizes) and the longitudinal samples (n = 14) on which they are based is moderate, but based on a substantial combined sample size (19,806 adults). Importantly, the available publications are sufficient for meta-analysis using modern techniques which explicitly model shared samples (i.e., with clustering) and accurately test relatively small samples (i.e., with bootstrapping, Joshi et al., 2022). Thus, this is an opportune time for a first set of meta-analyses of available evidence to assess the current state of knowledge in this area and identify directions for future research.
In this systematic review and meta-analysis, we first describe common ground in how child and adolescent social withdrawal and related constructs were defined in the reviewed publications, despite variation in their usage of withdrawal-related terms. Next, to provide an organized framework for interpreting meta-analytic results, we propose an overarching Developmental Science framework and three interpersonal mechanisms and a cascade mechanism that help to explain links between childhood social withdrawal and adult psychosocial adjustment. We then describe our methodological approach to this review. Next, we present results of meta-analyses evaluating evidence for childhood social withdrawal as a predictor of five forms of adult psychosocial adjustment.
1.1 Social withdrawal among peers in childhood and adolescence
This review focuses on psychosocial adjustment in adults with histories of social withdrawal in childhood and/or adolescence (hereafter “childhood social withdrawal”). Social withdrawal is a behavioral pattern in which children remain alone more often than age-mates in contexts which present the opportunity for peer interaction, such as freeplay at childcare or recess at school (Gazelle and Rubin, 2010; Rubin and Chronis-Tuscano, 2021; Rubin et al., 2009; Spangler and Gazelle, 2009). Social withdrawal is an “umbrella term” for solitary behavior in social contexts, although children demonstrate this behavior for multiple reasons (Asendorpf, 1990a; Rubin et al., 2009; Spangler and Gazelle, 2009). We reviewed publications with a common focus on children who exhibited socially withdrawn behavior regardless of underlying affect, motivation, or social cognition, because most reviewed publications identified children as socially withdrawn without identifying the reason or motivation for withdrawal.
The most common reason for childhood social withdrawal is social anxiety (Coplan et al., 2013). Social anxiety is conceptualized as children's anticipatory worry about how they will be received by peers and whether they will interact competently (social evaluative concerns). Children who display social withdrawal due to social anxiety are conceptualized as experiencing social approach-avoidance conflict (Asendorpf, 1990a), sometimes referred to as “conflicted shyness,” in which they want to interact with peers (normative social approach motivation) but are impeded from engaging in normative rates of interaction by their social anxiety and social evaluative concerns (high social avoidance motivation). Two reviewed publications identified children as anxious withdrawn (Goodwin et al., 2004; Jakobsen et al., 2012), but most reviewed publications identified children as socially withdrawn without identifying the reason or motivation for withdrawal. Although a minority of children included in these publications may have demonstrated social withdrawal due to social disinterest (a.k.a. unsociability, low social approach motivation, Asendorpf, 1990a), most children in these publications should have demonstrated social withdrawal due to social anxiety. Another potential reason for social withdrawal is “avoidance” (having high social avoidance motivation paired with low social approach motivation). However, none of the reviewed publications examined adult outcomes of childhood avoidant withdrawal, with the exception of one study of both conflicted and avoidant shyness (Tang et al., 2022). For this study we review results for “conflicted shyness” for the sake of consistency with the most probable reason for withdrawal in other reviewed publications.
This article reviews long-term longitudinal studies in which children were identified as socially withdrawn among peers in general, including with familiar peers such as classmates (Coplan et al., 1994; Gazelle and Ladd, 2003; Gazelle and Rubin, 2010), rather than only with strangers or in novel situations. Although some children who demonstrate social withdrawal among familiar peers also display similar behavior when meeting unfamiliar peers (Gazelle et al., 2005), other children withdraw from unfamiliar peers but not familiar peers (Gazelle and Faldowski, 2014). Therefore, our focus on studies of children identified as withdrawing from peers in general should capture those who withdraw from familiar peers (and may also withdraw from unfamiliar peers), while minimizing inclusion of studies of those who only withdraw from unfamiliar peers. This is important because we conceptualize withdrawal from familiar peers as a manifestation of social evaluative concerns linked with social learning processes (Coplan et al., 1994; Gazelle and Faldowski, 2014; Gazelle and Rubin, 2010), whereas withdrawal from unfamiliar peers only is conceptualized as a temperamentally-based manifestation of wariness in the face of novelty (Kagan et al., 2007). It was necessary to use a broad definition of social withdrawal to ensure inclusion of relevant available research, while nonetheless distinguishing between studies of social withdrawal vs. behavioral inhibition (but allowing inclusion of studies which identify children who demonstrate both).
Reviewing studies of social withdrawal from peers in general was both practically necessary given the state of the literature, and unique relative to previous meta-analyses. Because most reviewed studies identified children who withdrew from peers in general without distinguishing between familiar and unfamiliar peers, it was not possible to examine withdrawal from familiar vs. unfamiliar peers as a factor in meta-analyses. Furthermore, meta-analyses of social anxiety and other anxiety outcomes (including in adulthood) in children who are wary of the unfamiliar (behaviorally inhibited children) have already been conducted (Clauss and Blackford, 2012; Sandstrom et al., 2020), whereas a meta-analysis of anxiety and other psychosocial outcomes in adults with childhood social withdrawal had not been conducted prior to the current investigation.
We reviewed 31 studies which shared a common focus on children who exhibited social withdrawn behavior among peers in general, despite the variety of withdrawal-related terms used. This included studies that identified children not only as socially withdrawn (16 studies) or anxious withdrawn (two studies, Goodwin et al., 2004; Jakobsen et al., 2012), but also with other constructs related to social withdrawal (solitary/solitude, shy, socially inhibited, and socially anxious/phobic) if they referred to children's social behavior in general, rather than only with strangers. Two studies assessed youths' solitude in relation to peers in general (Jaffee et al., 2002; Monk et al., 2023). Seven studies assessed youth shyness as self-consciousness in situations of perceived social evaluation, rather than exclusively in situations of social novelty (Caspi et al., 1989, 1988; Crum et al., 2006; Ensminger et al., 2002; Fothergill and Ensminger, 2006; Kerr et al., 1996; Tang et al., 2022). Another two studies met this definition of shyness and are described in the text, although it was not possible to include them in meta-analyses of variable-oriented analyses because they reported person-oriented analyses (Schmidt et al., 2017; Tang et al., 2017). Four studies assessed social inhibition as uneasy reactions (hesitant approach, fearful, anxious, reserved, and reticent) in social-evaluative or unfamiliar situations (Asendorpf et al., 2008), including with familiar classmates (Asendorpf et al., 2008; Bohlin and Hagekull, 2009; Kagan et al., 1962). Similarly, one study assessed child and adolescent social anxiety disorder (SAD or social phobia) in relation to peers in general (Fichter et al., 2009), rather than exclusively in relation to novel social partners or situations. SAD identifies children who avoid or endure with distress at least some social situations with peers because they are afraid of embarrassing themselves, when this avoidance or distress is sufficiently intense to interfere with their lives (APA., 2022; Gazelle and Rubin, 2010; WHO, 1982). We use the term “social withdrawal” or “social withdrawal and related constructs” to refer to all these terms in studies which share these common criteria.
1.2 Potential mechanisms linking childhood social withdrawal to adult psychosocial adjustment
According to a Developmental Science perspective (Bergman et al., 2000; Lerner et al., 2015; Magnusson and Stattin, 2006), individual development is influenced by the interplay of multi-level systems over time, ranging from those within the individual (e.g., their biological sex), to those in their proximal social context (e.g., interactions and relationships with parents and peers), to broader ecological contexts (e.g., cultural context), and generational time (generation). In this set of meta-analyses, we expect childhood and adolescent social withdrawal to predict adult psychosocial outcomes due to several proximal interpersonal processes. Therefore, to provide a framework for interpreting results, we propose that three interpersonal process mechanisms link childhood vulnerability to adult psychosocial adjustment. Additionally, drawing from “cascade” models, we propose that difficulties in one domain of development (e.g., interpersonal) can cascade or spill over to influence other domains over time (e.g., educational, Masten and Cicchetti, 2010). Additionally, we make the secondary assumption that the extent to which childhood and adolescent social withdrawal predicts adult psychosocial outcomes and the nature of those adult outcomes, may be influenced by systems at both more proximal (within-person) and more distal levels ranging from biological sex to broader context (generation, culture).
1.2.1 Interpersonal processes
Interpersonal models of social withdrawal development propose that transactions between young people and their social partners (parents, peers, friends) and social contexts (family, school, workplace) contribute to continuity and change in social withdrawal over time and the development of psychosocial difficulties (Boivin et al., 2001; Boivin and Vitaro, 1995; Gazelle, 2022; Gazelle and Cui, 2020, 2021; Rubin and Chronis-Tuscano, 2021; Rubin et al., 2009). These interpersonal transactions may both exacerbate temperamental vulnerability to social withdrawal in some young people, and contribute to the emergence of social withdrawal in others (Gazelle and Faldowski, 2019). Long-term prospective longitudinal studies of psychosocial adjustment in adults with childhood social withdrawal adopt compatible transactional frameworks but are attuned to adult development. We will evaluate meta-analytic findings for compatibility with three potential interpersonal mechanisms derived from interpersonal models of social withdrawal (Gazelle, 2022; Rubin and Chronis-Tuscano, 2021; Rubin et al., 2009): (1) missing out on interpersonal interaction, (2) stressful interpersonal interaction, and (3) poor relationship quality.
1.2.1.1 Missing out on interpersonal interaction
Adults with childhood social withdrawal may be at risk for psychosocial difficulties in part because they miss(ed) out on interpersonal interaction in childhood, adolescence, and adulthood. This may occur for internal and/or external reasons, because: they choose not to participate in social environments (environmental selection), and/or others exclude them from social groups or environments. Both mechanisms limit opportunities for interpersonal interaction that are critical to building interpersonal and professional skills and maturity appropriate for adults.
Adults with childhood social withdrawal may choose not to participate in social groups and environments (environmental selection). Whereas young peoples' school attendance is mandatory, and their parents may encourage them to participate in additional social groups (e.g., religious youth groups, organized sports), adults exercise greater choice about participation in social groups. Some adults with childhood histories of social withdrawal may not finish high school, attend college, or work. Avoiding participation in social environments may be motivated by the desire to avoid stressful interpersonal interaction. Avoidance further reduces social interaction.
Others may exclude adults with childhood social withdrawal from social groups. Exclusion may occur because group members perceive these adults to be low in interpersonal skill or maturity in situations required to gain entry to or maintain involvement in social groups. This may occur when adults negotiate interpersonal challenges in interviews for admission to educational institutions, employment, or other social groups. Additionally, exclusion may occur when interpersonally challenging situations undermine educational or work performance or group harmony, thus diminishing chances for continuing inclusion or promotion in social groups. Exclusion not only limits opportunities for interpersonal learning, but also is hurtful. For instance, excluded vs. non-excluded anxious solitary children demonstrate more stable anxious solitude and depression over time (Gazelle and Ladd, 2003).
1.2.1.2 Stressful interpersonal interaction
Adults with childhood social withdrawal may be at risk for psychosocial difficulties in part because they experience stressful interpersonal interaction. Specifically, they may be vulnerable to victimization by peers, coworkers, and others. Their vulnerability may stem from social awkwardness, difficulty responding to victimization in interpersonally effective ways, and lack of alliances with others who might provide protection (Gazelle and Faldowski, 2019; Kochenderfer and Ladd, 1997). Evidence suggests that transactions occur between children's social withdrawal and stressful interaction with social partners (Gazelle and Cui, 2020, 2021). Similar transactions are likely in adulthood. Importantly, victimization contributes to risk for anxiety and depression (McDougall and Vaillancourt, 2015).
1.2.1.3 Poor relationship quality
Adults with childhood social withdrawal may experience poor-quality relationships with multiple close relationship partners including parents, friends, and romantic partners. Similar relationship quality among multiple close relationships is consistent with Attachment Theory (Bowlby, 1969). According to Attachment Theory, children construct a working model of close relationships based on parent-child relationships which is comprised in part of expectations about the availability and trustworthiness of close social partners, as well as expectations of themselves as relationship partners worthy of care and able to provide care. This working model then guides individuals in co-constructing other close relationships (Bretherton and Munholland, 2008). Individuals with insecure attachments to their parents are likely to have suboptimal expectations for themselves and/or their relationship partners, experience challenges in forming and maintaining close relationships with well-adjusted relationship partners, and have suboptimal interactions in relationships. Consequently, they may not derive optimal support from their close relationships, nor provide optimal support to their partners.
Poor relationship quality in adults with childhood social withdrawal may stem from imbalance in reciprocity, restricted companionship, and dependence (e.g., overreliance on one friend). Because interactions with friends are typically more rich and complex than interactions with other peers (Gottman and Graziano, 1983), infrequent and poor quality interaction with friends may limit the growth of perspective taking, social skill, and maturity in adulthood. Additionally, poor relationship quality may contribute to delays in achieving relationship-focused adult developmental milestones (e.g., cohabitation, marriage, procreation) and relationship dissolution (e.g., friendship instability, divorce).
1.2.2 Developmental cascades
Childhood social withdrawal may interfere with achieving adult developmental milestones on a normative time schedule because interpersonal interaction is inherent in many adult developmental tasks (e.g., initiating and maintaining relationships with a romantic partner, friends, coworkers; seeking advice from teachers and supervisors). Furthermore, consistent with a cascade model (Masten and Cicchetti, 2010), lack of interpersonal maturity and skill may influence development in other domains. For example, children who experience peer mistreatment at school are at risk for disliking school (Ladd and Coleman, 1997), underachieving, and dropping out of school in adolescence (Serbin et al., 1998). Graduating from high school and engaging in higher education are pivotal adult developmental milestones which subsequently impact socioeconomic status (SES), access to housing and healthcare, and ability to support oneself and one's family.
1.3 Research questions and hypotheses
This set of meta-analyses address the following research questions: Does childhood social withdrawal predict (1) delayed achievement of adult developmental milestones for participation in families and society, risk for (2) internalizing patterns, including: (2a) adult social withdrawal, (2b) social anxiety sx/dx, (2c) other anxiety sx/dx, (2d) depressive sx/dx, (3) substance use, (4) physical ill-health, and (5) intergenerational difficulties?
We expected childhood social withdrawal to predict delays in adult developmental milestones for participation in families and society, internalizing problems and particularly social anxiety, and intergenerational difficulties in mothers and their offspring. We expected these adult outcomes to stem from the proposed interpersonal processes and developmental cascades. However, we did not expect childhood social withdrawal to predict adult substance abuse because substance abuse is not consistent with the overall over-controlled pattern exhibited by these individuals, nor the reduced likelihood that they would be introduced to substance abuse in social contexts. Additionally, we did not advance a specific hypothesis about adult physical health outcomes because the connection between interpersonal processes and health outcomes was less clear, especially given that the health outcomes investigated to date are diverse.
We expected social withdrawal across a broad range of childhood and adolescence to predict adult psychosocial maladjustment (Fichter et al., 2009). Therefore, we did not advance hypotheses about whether social withdrawal earlier vs. later in development (e.g., in childhood vs. adolescence) would differentially predict adult outcomes. Moreover, most publications included in the meta-analyses were not designed to address this question. Likewise, adult adjustment outcomes were intended to capture patterns of adaptation relevant across development in early to middle adulthood. As such, we also did not advance hypotheses about differential outcomes at different points of adult development.
We also test the secondary research question of whether the relation between childhood social withdrawal and each form of adult psychosocial adjustment was heterogenous, and therefore likely to be moderated (strengthened or weakened) by other (unspecified) factors. If results suggest moderation, although the extent of evidence available was insufficient for meta-analyses of moderated effects, we will review available evidence from individual studies for moderation by factors such as biological sex. Although this review of moderation would not have a meta-analytic basis, it would result from a systematic review of the literature and be intended to provide researchers with guideposts for moderators which have received some support in extant literature.
2 Method
We conducted meta-analyses with results from 31 prospective longitudinal publications on childhood and adolescent social withdrawal as a predictor of adult psychosocial adjustment and health. These publications were derived from 14 longitudinal samples, 5 of which generated multiple publications, and yielded a combined sample size of 19,806 participants (50% women: n = 9,827) and an additional 175 of their offspring.
2.1 Publication search, selection, and data extraction procedures
We followed PRISMA guidelines (Page et al., 2021) for search, selection, and data extraction procedures. Peer-reviewed empirical journal articles and a book published before April 11th, 2023 were located with searches of a university library catalog, PsychINFO, PubMed, Web of Science, and Google Scholar databases. Keywords for the initial literature search were “social withdrawal,” “anxious withdrawal,” “anxious solitude,” “longitudinal,” “childhood,” and “adult outcomes.” The references of these publications then served as sources of additional articles. Theses, dissertations, non-empirical publications, and retrospective longitudinal studies were not reviewed. Also, studies using person-oriented trajectories as predictors (n = 2 studies) were not included in meta-analyses (but are described in the text) because person-and variable-oriented results could not be combined in weighted means. Articles were selected by analyzing definitions of social withdrawal and related constructs (shyness, solitude, inhibition, wariness, SAD/social phobia) to ensure that they were not operationalized only in reference to “new” or “novel” social partners or situations. Table 1 lists complete inclusion and exclusion criteria.
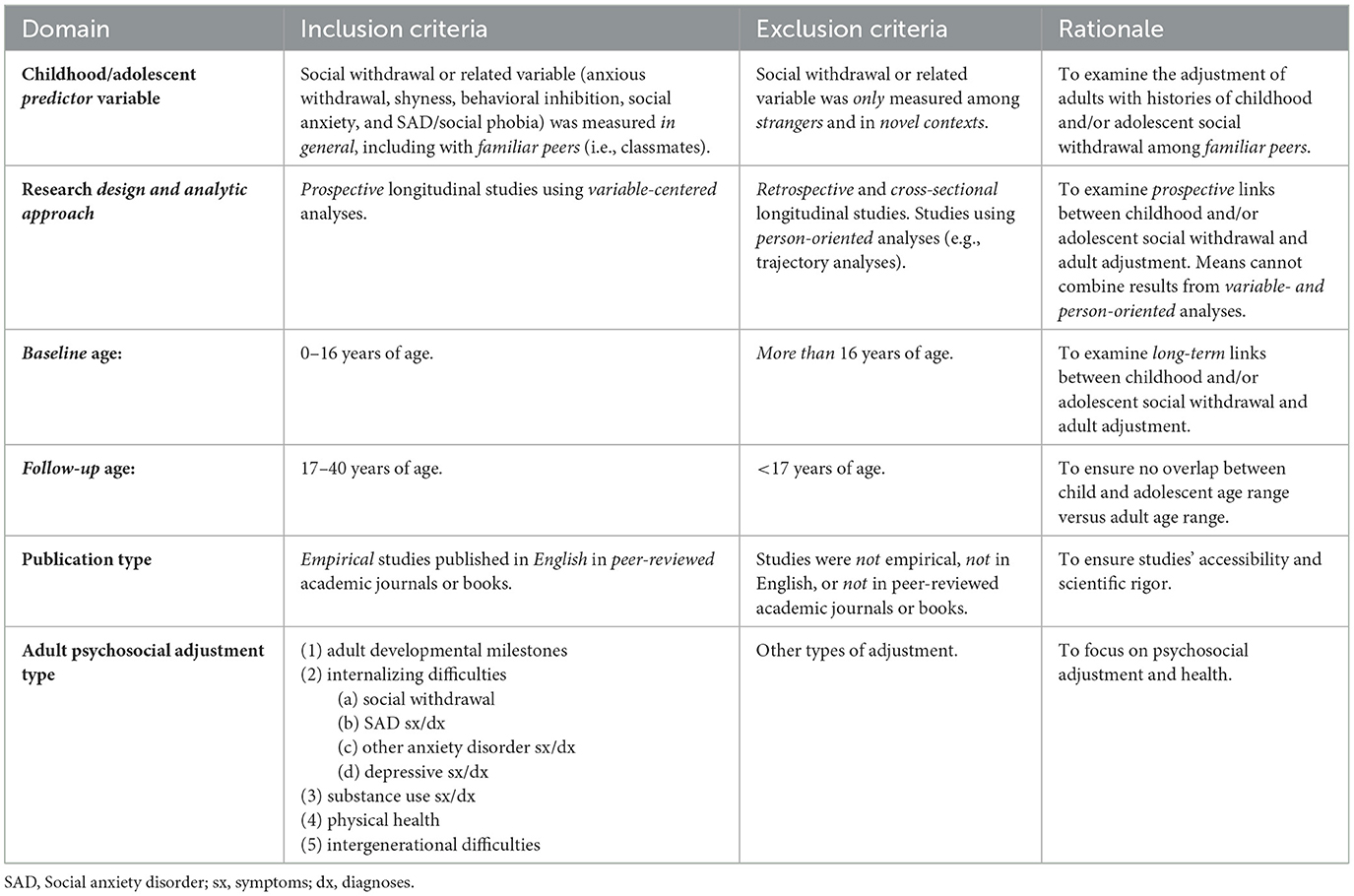
Table 1. Criteria for inclusion or exclusion of publications in meta-analyses.
Of the 18 articles initially selected for review, 16 assessed childhood “social withdrawal,” and two “anxious withdrawal.” To enlarge the evidence base, a second search added the keywords “shyness,” “solitary/solitude,” “inhibition,” “wariness,” “social anxiety,” “social phobia,” “adolescence,” and “peer.” This search yielded 15 additional articles featuring the constructs “shyness” (seven articles), “inhibition” or “inhibition/overcontrol” (four articles), solitude/solitary (two articles), or “SAD” or “social phobia” (two articles). Studies were selected if the withdrawal-related construct definition referred to familiar peers (i.e., classmates) or peers in general (i.e., not only strangers and novel situations). We reviewed only studies that reported specified forms of psychosocial adjustment (Table 1) for adults with childhood social withdrawal.
Guided by inclusion and exclusion criteria (Table 1), the second author (in consultation with first author) screened publications for eligibility based on (1) titles and abstracts, and then (2) the full text of publications. The second author extracted data onto a pre-defined form, including: study information (authors, publication year, social withdrawal construct name, and definition); sample characteristics (size, age at childhood and adult assessments, biological sex proportions, country, and generation/year at first assessment); social withdrawal or related construct assessment (assessment name, informant); and relevant results for adults with childhood social withdrawal (but not aggressive-withdrawal) with notes on control variables and moderated and mediated effects. When publications lacked data, the second author attempted to contact corresponding authors via email. Four authors responded with the necessary information, one author was unreachable, and one author had passed away and his co-authors were not able to provide data. Therefore, it was not possible to include two eligible studies in meta-analysis for insufficient data (Copeland et al., 2014; Schwartzman et al., 2009), but they are nonetheless listed in tables. Thus 33 eligible publications were identified, and we were able to obtain sufficient information to calculate effect sizes for 31 of these publications. Figure 1 summarizes the PRISMA-guided literature search process.
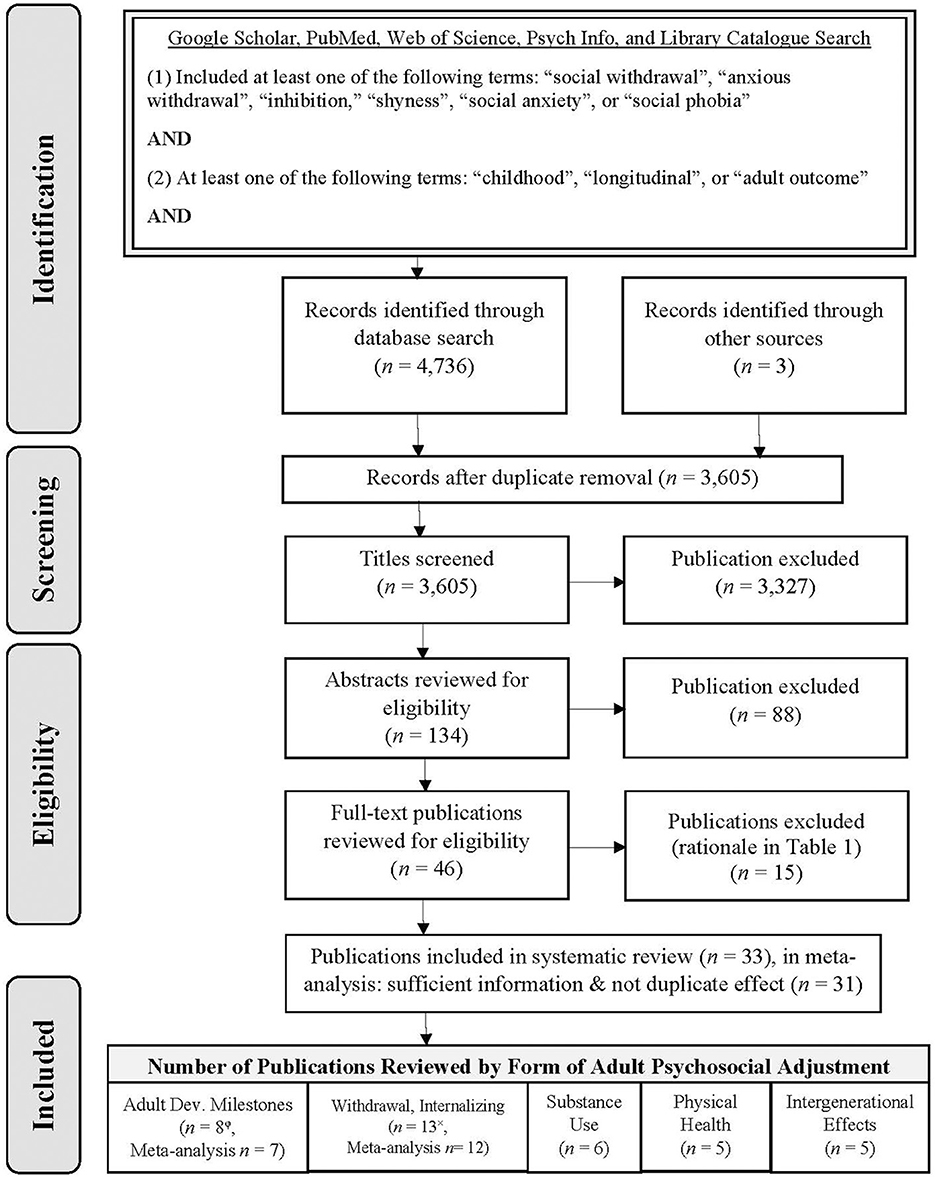
Figure 1. Flow chart of publication selection process. Publications are listed in multiple “included” categories if they report multiple forms of adult psychosocial adjustment. The number of publications included in meta-analysis is specified separately when eligible publications were excluded from meta-analysis due to φinsufficient data for calculating effect sizes or ×reporting duplication (the same effect in the same sample across multiple publications).
2.2 Converting effect sizes to Fisher's z and Pearson's r for each relevant result in individual studies
To obtain a uniform effect size statistic for each meta-analysis, each relevant result (summary statistic) from each study was converted to a Fisher's z statistic (see statistical supplement). Fisher's z was chosen because: (1) Pearson's r was the effect size most frequently reported in studies, and its transformation into Fisher's z ensures a normal distribution; (2) Pearson's r and Fisher's z can both capture the link between childhood social withdrawal and adult psychosocial adjustment. Therefore, other effect size statistics were first converted into Pearson's r (Borenstein et al., 2021; Cumming, 2013) and then Fisher's z. Finally, other statistics were first converted to Cohen's d (Thalheimer and Cook, 2002), then Pearson's r (Borenstein et al., 2021; Cumming, 2013), and then Fisher's z. Then after meta-analyses were performed with Fisher's z values, results were converted back to Pearson's r for interpretability (Borenstein et al., 2021). Pearson's r values were interpreted as small (≥0.1), medium (≥0.3), or large (≥0.5) effects (Cohen, 1988). When a study reported multiple effects in the same domain of adult psychosocial adjustment, their mean effect size was entered into meta-analysis.
2.3 Calculating a clustered weighted mean effect size across studies for each form of adult adjustment
To generate a weighted mean effect size for each form of adult psychosocial adjustment, clustered effects meta-analyses with bootstrapping were performed in the software platform R (R Core Team, 2019) with the “metafor” (Viechtbauer, 2010) and “boot” (Canty and Ripley, 2024) packages. To account for dependency among multiple publications based on the same longitudinal sample, these correlated hierarchical effect structures (Hedges et al., 2010) were explicitly modeled as clusters (see statistical supplement) in “metafor.” Additionally, to account for the relatively small number of studies available for each meta-analysis, we used bootstrapping (see statistical supplement) (Davison and Hinkley, 1997), which has been shown to control Type 1 error rates while preserving power under these conditions (Davison and Hinkley, 1997; Joshi et al., 2022). Separate meta-analyses were computed for each form of adult psychosocial adjustment: (1) adult developmental milestones; (2) internalizing difficulties (including 2a-d): (2a) social withdrawal; (2b) SAD symptoms (sx)/diagnoses (dx); (2c) other anxiety disorder sx/dx; (2d) depressive sx/dx; (3) substance use sx/dx; (4) physical health; and (5) intergenerational difficulties.
Before computing a weighted mean effect for each outcome, the valence (+ or – sign) of some individual study effects were reversed for consistency with one another when needed. Specifically, effects were recoded to have the same valence (e.g., higher values suggest greater maladjustment).
All eligible studies are listed in Tables 2–6. Those eligible studies entered into meta-analyses are marked with an *in the reference section. A few eligible studies could not be entered into meta-analyses either because multiple publications reported effects for the same adult outcome for the same sample (a duplicate effect not entered into meta-analyses is marked with an × in Table 2), or because insufficient information was available to calculate an effect size [marked with an φ in Table 3 (other anxiety, depression)].
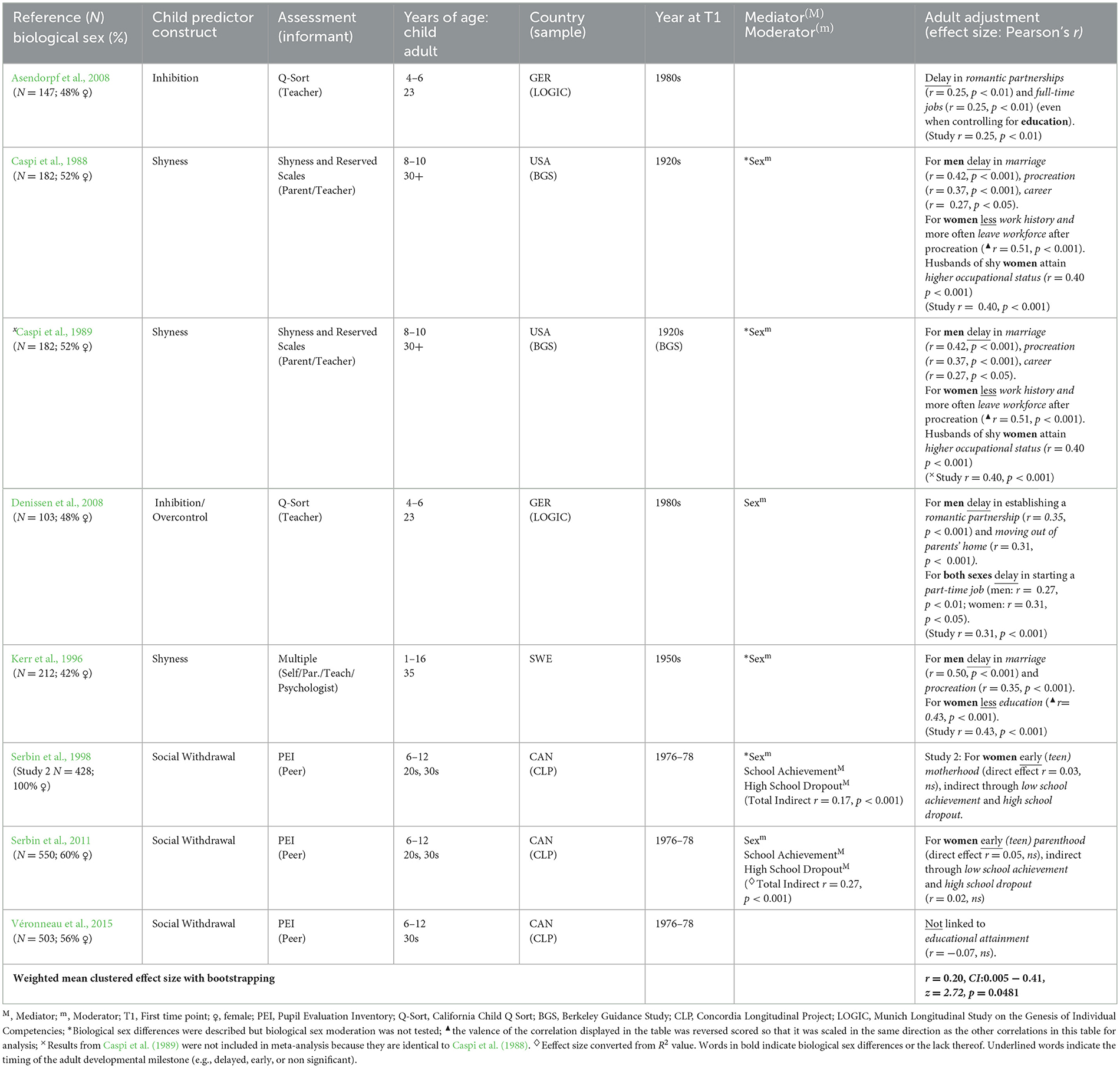
Table 2. Adult developmental milestones (N = 7× studies, N = 4 samples, N = 1,091 adult participants).
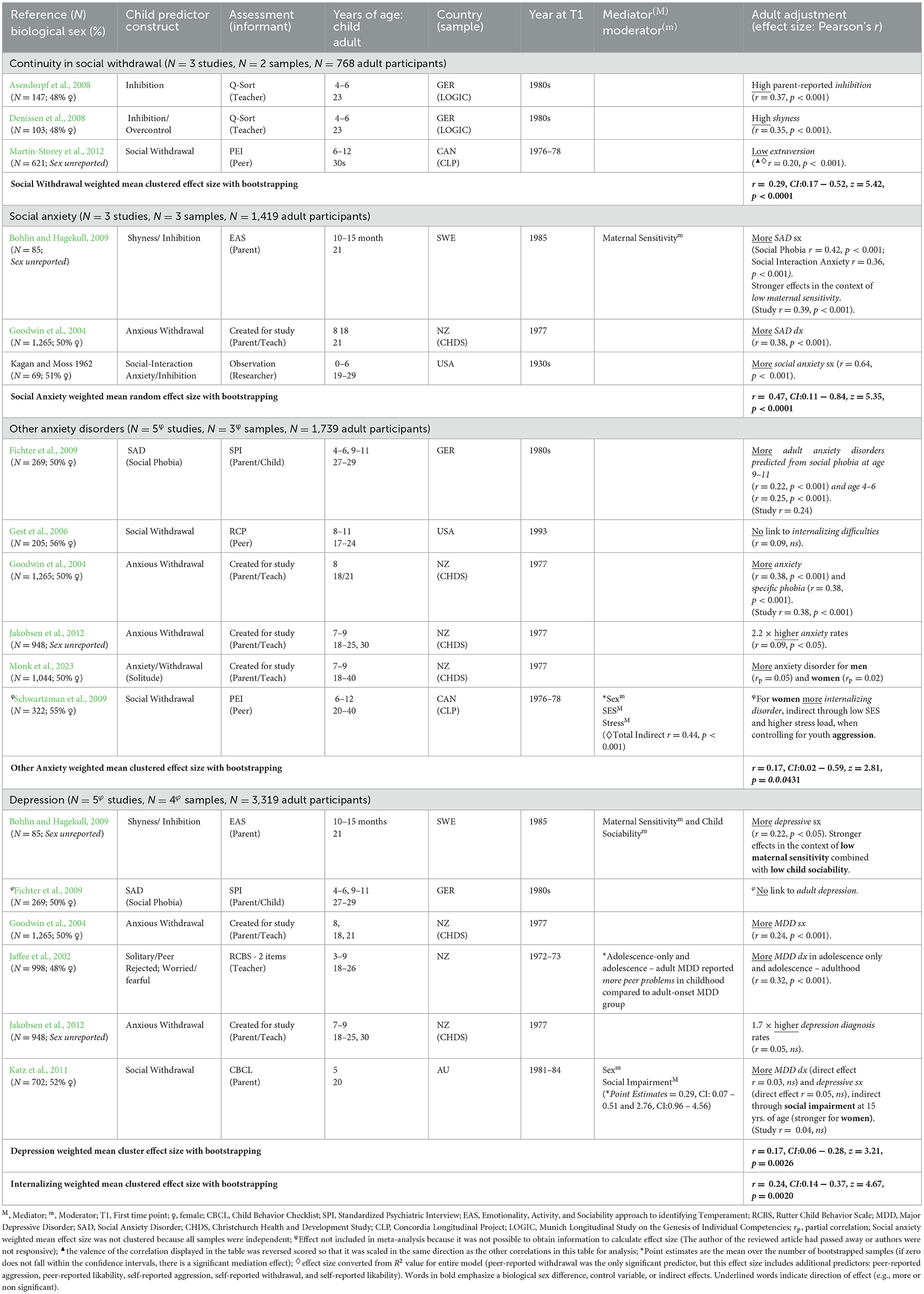
Table 3. Adult social withdrawal and internalizing difficulties (N = 12φ studies, N = 9 samples, N = 4,361 adult participants).
2.4 Preliminary analyses: Checking for publication bias and moderation of meta-analyses
Each meta-analysis was assessed for publication bias statistically via Egger's regression and Begg's rank correlation tests (see statistical supplement) of asymmetry in funnel plots computed in Excel with the Meta-Essentials workbook. Egger's regression (t) and Begg's rank correlation (z) tests were not significant, indicating no significant deviation from symmetry in funnel plots (i.e., no significant bias; p > 0.05 for t tests; p > 0.10 for z tests). Specifically, funnel plots were not significantly asymmetric for adult (1) developmental milestones (t = 2.22, p = 0.08; z = 1.05, p = 0.29), (2a) social withdrawal (t = 2.27, p = 0.26; z = 0.52, p = 0.60), (2b) SAD sx/dx (t = 0.94, p = 0.52; z = 1.57, p = 0.12), (2c) other anxiety disorder sx/dx (t = −0.20, p = 0.86; z = 0.00, p = 1.00), (2d) depressive sx/dx (t = 0.20, p = 0.86; z = −0.49, p = 0.96), (3) substance use (t = 0.30, p = 0.78; z = −0.75, p = 0.45), (4) physical health (t = 1.10, p = 0.35; z = 0.49, p = 0.62), and (5) intergenerational difficulties (t = 0.78, p = 0.49; z = 0.73, p = 0.46). Therefore, findings indicate no significant deviation from symmetry in statistical tests, supporting the absence of significant publication bias (Lin and Chu, 2018) and other threats to reliability (such as unreliable results from small studies, data irregularities, and chance results, Sterne and Harbord, 2004). These results support the validity of meta-analytic results.
To examine the potential for moderation of effect sizes included in meta-analyses, we analyzed heterogeneity among effect sizes for each outcome. Analyses suggest significant heterogeneity among effect sizes for adult (1) developmental milestones (Q = 66.71, p < 0.001), (2a) social withdrawal (Q = 5.42, p < 0.01), (2b) SAD sx/dx (Q = 8.04, p < 0.001), (2c) other anxiety sx/dx (Q = 92.93, p < 0.001), (2d) depressive sx/dx (Q = 58.08, p < 0.001), (3) substance use (Q = 157.95, p < 0.001), and (4) physical health (Q = 257.07, p < 0.001). No significant heterogeneity was found for intergenerational difficulties (Q = 3.59, p = 0.46), perhaps because all publications on intergenerational difficulties were derived from a single longitudinal sample. Heterogeneity for most forms of adult adjustment suggests that moderated meta-analyses might be fruitful in the future. At present, moderated meta-analyses were not possible because of the limited number of studies available for review (i.e., < 4 effect sizes per level of moderator, Pearcey et al., 2021). Given this support for moderation in most adult outcomes, in addition to reporting meta-analytic results, we review evidence for moderation from individual studies when available.
3 Results
3.1 Sample characteristics
We identified 33 eligible empirical publications reporting on prospective longitudinal studies of psychosocial adjustment in adults with childhood social withdrawal published over the past 61 years from 1962 to 2023. Of these studies, it was possible to obtain sufficient information to calculate effect sizes for 31 studies (listed in Tables 2–6, references marked with *in reference section) which were based on 14 long-term longitudinal samples.
3.1.1 Demographics
The combined sample size across these 31 studies was 19,806 adults (50% women1: n = 9,827) with childhood/adolescent histories of social withdrawal, and 175 of their offspring (56% girls: n = 98). Combined sample sizes throughout this report were calculated such that each sample was counted only once even when it resulted in multiple publications.
Childhood social withdrawal was assessed at the outset of these studies at 6 years of age or less for 59% of the combined sample (n = 11,619 adults, n = 7 studies), and at 6 to 15 years of age for the remaining 41% of the combined sample (n = 8,187 adults, n = 24 studies; Tables 2–6). Only 3 of these studies reported a mean age at which children were assessed (weighted m = 11.83 years of age). Repeated measurements of childhood social withdrawal at 6 years of age and younger were employed as predictors in several studies (Asendorpf et al., 2008; Denissen et al., 2008; Tang et al., 2022), and repeated measurements of social withdrawal across both childhood and adolescence served as predictors in other studies (Jaffee et al., 2002; Kerr et al., 1996).
Adult adjustment was assessed in the 20s only for 57% (n = 11,409 adults, n = 3 studies) of the combined sample of 19,806 adults, 30s only for 2% of the combined sample (n = 394 adults, n = 3 studies), or from the late teenage years (17–19 years) to adulthood (21–42 years of age) for 38% of the combined sample (n = 7,502 participants, n = 21 studies). Mean age at adult assessment (weighted m = 28.46 years of age) was reported for only 3% of the combined sample (n = 501 adults; n = 4 studies). The offspring of adults with childhood social withdrawal were assessed in middle childhood (weighted m = 7.76 years, n = 5 studies).
Race/ethnicity was reported for 61% of the combined sample (n = 12,033 adults, n = 7 studies): 83% (n = 9,941 participants) were White, 10% (n = 1,157 participants) were Black, < 1% (n = 26 participants) were Native American, < 1% (n = 67 participants) were Latinx, < 1% (n = 6 participants) were Asian, and 7% (n = 836 participants) were “Other.” Additionally, majority White participants (without frequency or percentage, sample n = 1,289 participants, n = 4 studies) were reported for 6% of the combined sample. Race/ethnicity was not reported for the remaining 33% of the combined sample (n = 6,484 participants, n = 20 studies).
The combined sample was of diverse SES. Half of the sample was of varied SES (50%, n = 9,815 adults, n = 7 studies) and about another third of the sample was mostly low SES (32%, n = 6,385 adults, n = 16 studies). One study focused on a mostly middle SES sample (< 1%, n = 69 adults). SES was not reported (or reported in an uninterpretable manner) for the remaining 18% of the sample (n = 3,537 adults, n = 7 studies).
3.1.2 Generation and nationality
Children born in the 1990s comprised just under half the combined sample (49%, n = 9,696 participants; n = 2 studies), although they were drawn from only two studies. Children born in the 1970s and 1980s comprised forty percent of the combined sample (40%; n = 8,595 participants; n = 22 studies), and children born in or before the 1960s comprised the remaining seven percent of the combined sample (7%; n = 1,515 participants; n = 7 studies).
All studies were conducted in Western countries: Europe, North America, or Australia/New Zealand. The largest contribution to the combined sample was from the UK (48%, n = 9,491 participants, 1 study), whereas other European countries made modest contributions: Germany (2%; n = 416 participants, 3 studies) and Sweden (1%, n = 297 participants, 2 studies). The next largest contribution to the combined sample came from North America: the U.S. (14% of combined sample, n = 2,724 participants, 8 studies) and Canada (20% of combined sample, n = 3,913 participants, 12 studies), followed by Australia/New Zealand: New Zealand (11%, n = 2,263 participants, 4 studies) and Australia (4%, n = 702 participants, 1 study, Tables 2–6). All of the Canadian studies were from the Concordia Longitudinal Project (CLP).
3.2 Meta-analytic results overview: Childhood social withdrawal predicts adult adjustment
Meta-analytic results (Tables 2–6) revealed that child social withdrawal significantly predicted: (1) delayed adult developmental milestones (r = 0.20, p < 0.05); more adult (2) internalizing tendencies (r = 0.24, p < 0.01), including: (2a) social withdrawal (r = 0.29, p < 0.0001); (2b) SAD sx/dx (r = 0.47 p < 0.0001); (2c) other anxiety sx/dx (r = 0.17, p < 0.05); and (2d) depressive sx/dx (r = 0.17, p < 0.01); and (3) intergenerational difficulties (r = 0.32, p < 0.0001). However, adults with childhood social withdrawal were less likely than others to abuse substances (r = −0.16, p < 0.01). Effects were of medium size (≥0.3) for adult SAD sx/dx and intergenerational difficulties, whereas effects were of small size (≥0.1) for adult developmental milestones, internalizing tendencies, social withdrawal, other anxiety sx/dx, depressive sx/dx, and substance abuse (Tables 2–6, Cohen, 1988).
Meta-analytic results also suggest that childhood social withdrawal was not significantly related to physical health (r = 0.13, ns; Table 5). However, this result may be influenced by biological sex and heterogeneity of physical health outcomes.
Tables 2–6 each list the following for the adult outcome identified at the top of the table: number of publications reporting on the outcome, number of unique samples on which those publications were based, and combined sample size across those unique samples (at the top of the table), and weighted mean clustered effect size (r) across all publications for the specified form of adult adjustment, 95% confidence interval, test statistic, and significance level (at the bottom of the table), and for each study reporting results for a particular adult outcome (in each row within the table): reference (first author and year only), sample size and biological sex percentage, child predictor construct, assessment name and informant for child predictor, young person's age in years at childhood and adult assessments, country from which sample was drawn, name of the longitudinal sample (for shared samples); calendar year at first assessment, mediator and/or moderator effects (if reported), form of adult adjustment, effect size (Pearson's r between childhood social withdrawal and adult outcome) for each relevant adult adjustment result from each publication.
3.3 Detailed review of meta-analytic results and their evidence-base
In this section we provide a detailed account of each meta-analysis, including characterizing the evidence-base for each meta-analysis: the number of publications, number of unique longitudinal samples, and combined sample size on which each meta-analysis was based. We also describe specific types of adult psychosocial adjustment included in each meta-analysis.
When available, we highlight odds ratios and statistical controls for individual studies, and describe developmental trajectories that could not be included in meta-analyses. Given support for moderated effects for all adult outcomes (except intergenerational effects) in preliminary analyses, we also review patterns that suggest moderation by biological sex (and generation for adult developmental milestones) in individual study results.
3.3.1 Adult developmental milestones, biological sex, and generation
Childhood social withdrawal was evaluated as a predictor of the timing of adult developmental milestones for participation in families (e.g., age at commencing dating, marriage, parenthood) and society (e.g., age at commencing higher education, work) in seven2 studies based on 4 longitudinal samples and a combined sample size of 1,091 adults (Table 2). Meta-analysis supported childhood social withdrawal as a small-size predictor of delayed adult developmental milestones (r = 0.20, [CI: 0.005 − 0.41], z = 2.72, p < 0.05). The pattern of individual study results suggests that findings varied by biological sex and generation. Some cultural variation was also observed among Western cultures.
For men in earlier generations (boys in the 1920s−50s), childhood shyness predicted delayed marriage (3–4 years), parenthood (3–4 years) and, in the US but not Sweden (Kerr et al., 1996), entry to a stable career (3 years) which, in turn, predicted less work achievement and occupational stability (Caspi et al., 1989, 1988). Effects remained after controlling for SES origins; educational attainment; age at educational completion, first job, military service; physical attractiveness; and childhood ill-temperedness (Caspi et al., 1989).
For women in earlier generations, childhood shyness predicted abbreviated participation in society but not families in both the US and Sweden. For women in earlier generations, childhood shyness predicted less education in Sweden (Kerr et al., 1996), and having no work history or leaving the workforce after childbirth in the US (Caspi et al., 1989, 1988) after controlling for SES origins, educational attainment, and adolescent IQ (Caspi et al., 1989). Thus, shy women compared to their non-shy counterparts focused more on family than societal participation.
For recent generations (children in the 80s/90s), the pattern of individual study findings suggests that men with childhood histories of social withdrawal continued to demonstrate delayed romantic partnerships. However, findings were mixed for whether women in recent generations demonstrated delayed romantic relationships, and whether men were delayed (about 1 year) in leaving their parents' home (women wer not delayed, Asendorpf et al., 2008; Denissen et al., 2008).
Nonetheless, studies of recent generations have often found delayed adult occupational and financial milestones for both women and men with childhood social withdrawal. For example, both German women and men with childhood social inhibition were delayed in joining the workforce by 10 months (Asendorpf et al., 2008) to over a year (Denissen et al., 2008).
3.3.2 Internalizing difficulties: Adult social withdrawal, social anxiety, other anxiety, and depression
Meta-analysis of 12 (see footnote 2) articles based on 9 longitudinal samples and a combined sample size of 4,361 adults (Table 3) support childhood social withdrawal as a small-size predictor of adult internalizing problems {including social withdrawal, SAD sx/dx, other anxiety sx/dx, and depression sx/dx r = 0.24, [CI: 0.14 − 0.37], z = 4.67, p < 0.01}. Additional meta-analyses of specific internalizing problems reveal consistent, but more nuanced results. Meta-analyses support childhood social withdrawal as a medium-size predictor of adult SAD sx/dx (r = 0.47, p < 0.0001), and small-size predictor of social withdrawal (r = 0.29, p < 0.0001), other anxiety sx/dx (r = 0.17, p < 0.05), and depressive sx/dx (r = 0.17, p < 0.01). Most individual study results were not specific to biological sex. In one study, effects for adult SAD, other anxiety, and depression remained significant when controlling for childhood conduct and attentional problems, child abuse, maternal education, parental separation, stressful family life events, and parental internalizing disorders (Goodwin et al., 2004).
3.3.2.1 Social withdrawal
Meta-analysis of 3 publications based on 2 longitudinal samples and a combined sample size of 768 adults supported childhood social withdrawal as a small-sized predictor of adult social withdrawal (r = 0.29, CI: 0.17 − 0.52, z = 5.42, p < 0.0001). All three (see footnote 2) studies support continuity from peer-reported social withdrawal in childhood and adolescence to adult shyness (Denissen et al., 2008), parent-reported inhibition (Asendorpf et al., 2008), and low extraversion (Martin-Storey et al., 2012).
3.3.2.2 Social anxiety
Meta-analysis of results from 3 publications based on 3 longitudinal samples and a combined sample size of 1,419 adults supported childhood social withdrawal as a medium-sized predictor of adult social anxiety sx/dx (r = 0.47, CI: 0.11 − 0.84, z = 5.35, p < 0.0001). We report the weighted mean effect (rather than the clustered effect) for social anxiety because there were no shared samples among the publications that reported on this outcome. All three (see footnote 2) investigations found that childhood social withdrawal predicted adult SAD dx (Goodwin et al., 2004) or sx (Bohlin and Hagekull, 2009; Kagan et al., 1962). In one study, these effects remained significant after controlling for adult depressive sx (Bohlin and Hagekull, 2009).
3.3.2.3 Other anxiety
Meta-analysis of results from 5 publications based on 3 longitudinal samples and a combined sample size of 1,739 adults (Fichter et al., 2009; Goodwin et al., 2004; Jakobsen et al., 2012; Monk et al., 2023) indicated that childhood social withdrawal was a small-sized predictor of other anxiety disorders in adulthood (r = 0.17, CI: 0.02 − 0.59, z = 2.81, p < 0.05). Specifically, other anxiety disorders predicted included generalized anxiety disorder (GAD), obsessive-compulsive disorder (OCD), specific phobias, panic disorder, agoraphobia, and internalizing composites including anxiety (Fichter et al., 2009; Goodwin et al., 2004). In one study, children who scored highest vs. lowest on anxious withdrawal demonstrated 2.2 times higher rates of adult anxiety disorder (Jakobsen et al., 2012). The only study (Gest et al., 2006) that found no relation between child social withdrawal and adult internalizing had a relatively small sample.
In regard to developmental range, child SAD assessed at both preschool/early middle childhood (4–6 years) and preadolescence (9–11 years) predicted adult anxiety disorders (Fichter et al., 2009). This is consistent with our expectation that social withdrawal across a broad age range in childhood and adolescence would predict adult adjustment.
3.3.2.4 Depression
Meta-analysis of results from 5 publications based on 4 longitudinal samples, and a combined sample size of 3,319 adults support childhood social withdrawal as a small-sized predictor of adult depressive sx/dx (r = 0.17, CI: 0.06 − 0.28, z = 3.21, p < 0.01). In four of five studies childhood social withdrawal (Bohlin and Hagekull, 2009; Goodwin et al., 2004; Jaffee et al., 2002; Jakobsen et al., 2012) directly predicted adult major depressive disorder (MDD) sx/dx. In one study, children who scored highest vs. lowest on anxious withdrawal demonstrated 1.7 times higher rates of adult MDD (Jakobsen et al., 2012). However, in another study (Bohlin and Hagekull, 2009) the link between childhood shyness/inhibition and adult depression was no longer significant after controlling for social anxiety. Additionally, two studies (Fichter et al., 2009; Katz et al., 2011) found no direct prediction of depression. Nonetheless, one of these studies (Katz et al., 2011) found that childhood social withdrawal indirectly predicted MDD sx/dx for women.
Taken together, social withdrawal demonstrated substantial continuity from childhood to adulthood and predicted adult internalizing sx/dx, especially SAD.
3.3.3 Substance use and biological sex
Meta-analysis of 6 publications based on 3 longitudinal samples and a combined sample size of 2,944 adults support childhood social withdrawal (controlling for childhood aggression) as a small-size protective factor for adult substance use (r = −0.16, CI: −0.39–−0.08, z = −3.78, p < 0.01; Table 4). Consistent with this result, all six studies suggest that childhood social withdrawal (controlling for aggression) reduced risk for adult alcohol and/or substance use (Table 4).
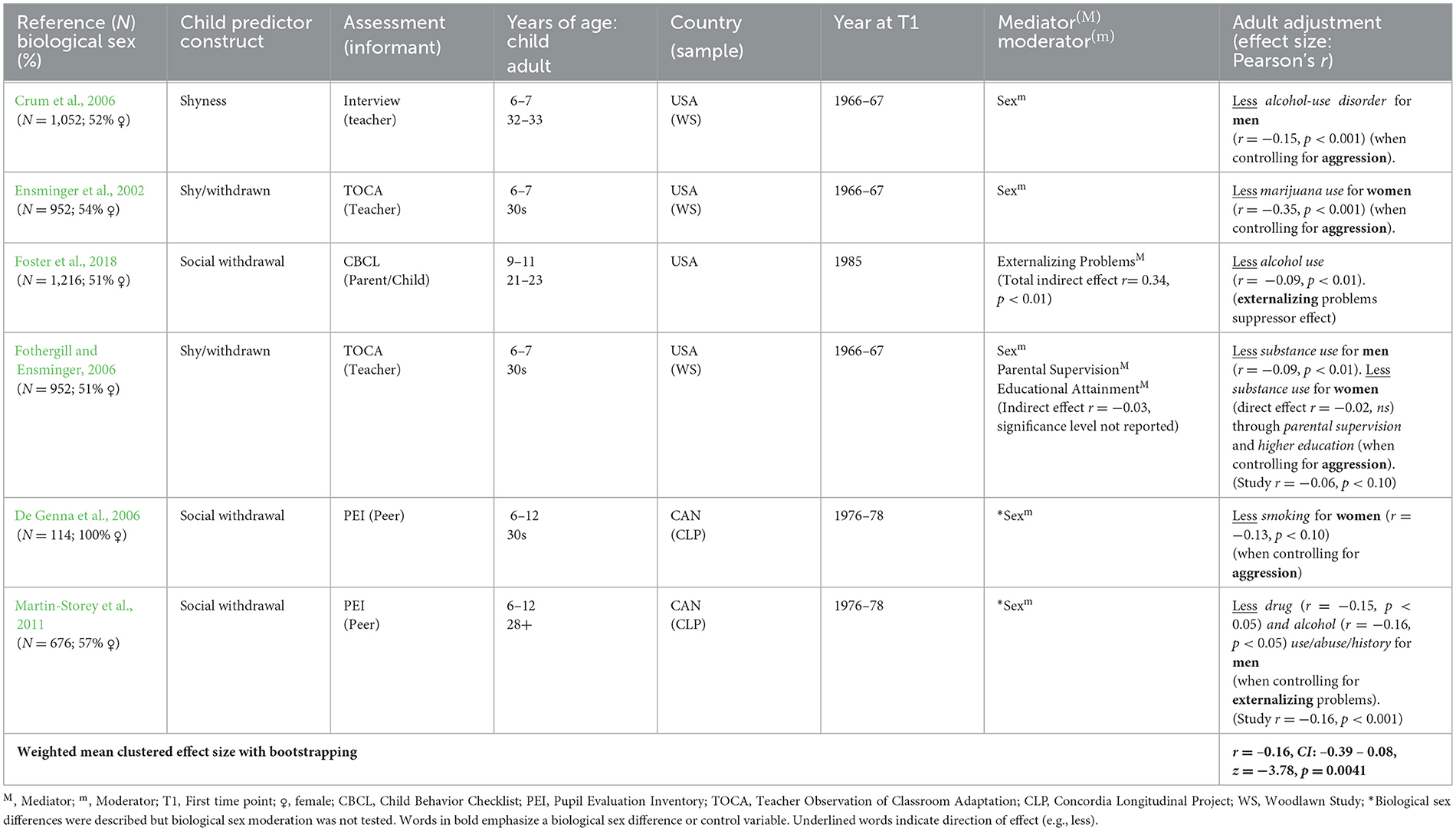
Table 4. Adult substance use (N = 6 studies, N =3 samples, N = 2,944 adult participants).
The pattern of results across studies indicates childhood social withdrawal reduced risk for adult alcohol and/or substance use in both sexes, even though most individual study results were specific to biological sex. Childhood social withdrawal reduced risk for: alcohol abuse in men in two studies (Crum et al., 2006; Martin-Storey et al., 2011); drug use in women in another study (Ensminger et al., 2002); and adult alcohol or substance use in both men and women in another two studies (Foster et al., 2018; Fothergill and Ensminger, 2006). In one of the studies that found effects for both sexes (Fothergill and Ensminger, 2006), the effect was direct for men, but indirect for women. Similarly, after controlling for aggression, women with vs. without childhood social withdrawal were less likely to engage in additional health risk behaviors such as smoking (De Genna et al., 2006). Taken together, meta-analysis indicates that childhood social withdrawal protected against adult substance use.
3.3.4 Physical health and biological sex
Meta-analysis of results of 5 publications based on 2 longitudinal samples and a combined sample of 13,404 adults did not support childhood social withdrawal as a predictor of physical health (r = 0.13, CI: −0.71 − 0.91, z = 2.04, ns; Table 5). Although individual studies suggest effects for specific health indicators, the non-significance of meta-analytic results may reflect the heterogeneity of these health indicators and that some were specific to biological sex. In regard to heterogenous health indicators, childhood conflicted-shyness (compared to avoidant-shyness) directly predicted higher adult body mass index (BMI), but lower C-reactive protein (CRP) levels (Tang et al., 2022). Additionally, childhood social withdrawal predicted more adult dentist visits (Temcheff et al., 2011a).
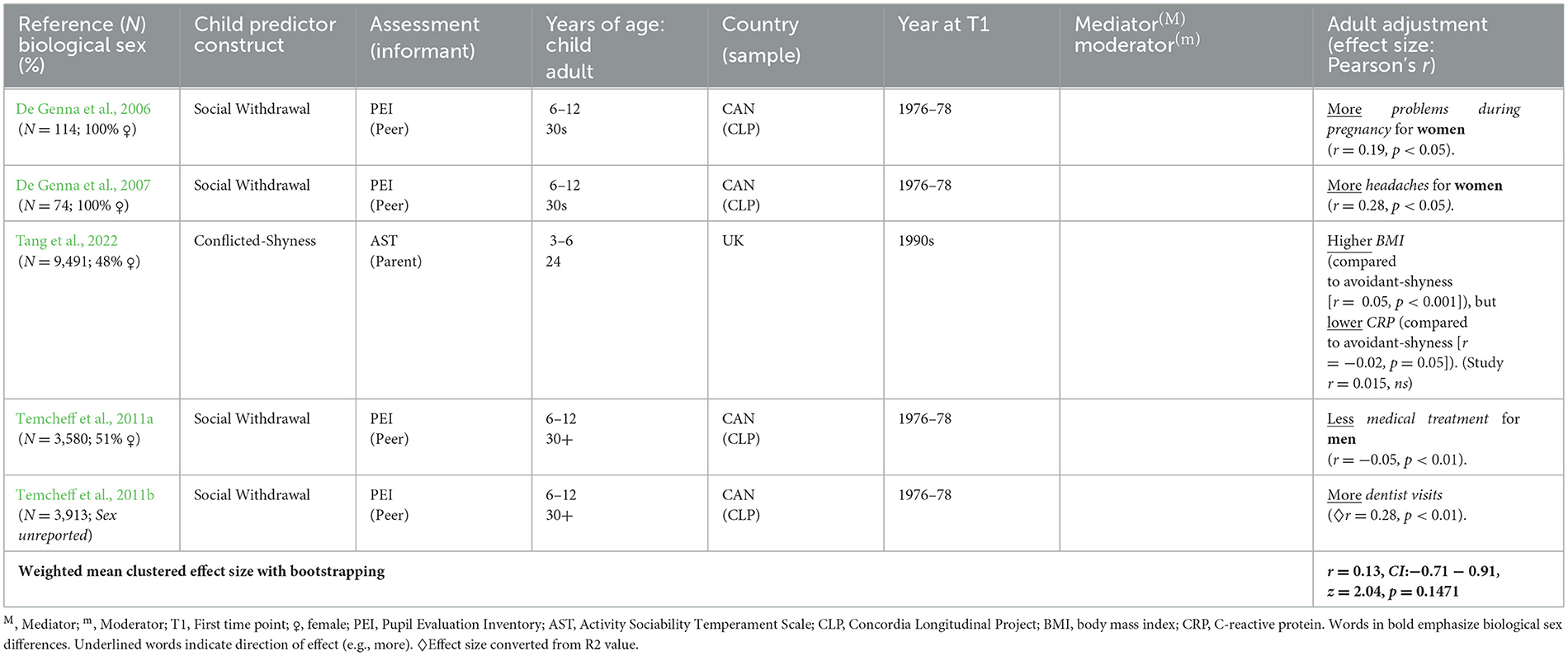
Table 5. Adult physical health (N = 5 studies, N = 2 samples, N = 13,404 adult participants).
In regard to health patterns in individual studies that were specific to biological sex (or examined only in one sex), as well as heterogeneous, mothers with vs. without childhood social withdrawal reported more somatization sx, such as frequent headaches (De Genna et al., 2007) and pregnancy problems (De Genna et al., 2006). Conversely, men but not women with childhood social withdrawal had fewer injuries (Temcheff et al., 2011b). Thus, certain health patterns may be specific to women or men with childhood social withdrawal.
3.3.5 Intergenerational difficulties for mothers and their offspring
Meta-analytic results from 5 publications on the CLP sample and a combined sample of 109 mothers and 175 of their offspring support childhood social withdrawal as a medium-size predictor of intergenerational patterns of mothering and offspring adjustment (r = 0.32, CI: 0.24 – 0.40, z = 6.32, p < 0.0001; Table 6). Results from individual studies suggest that childhood social withdrawal predicted both suboptimal mothering and offspring maladjustment.
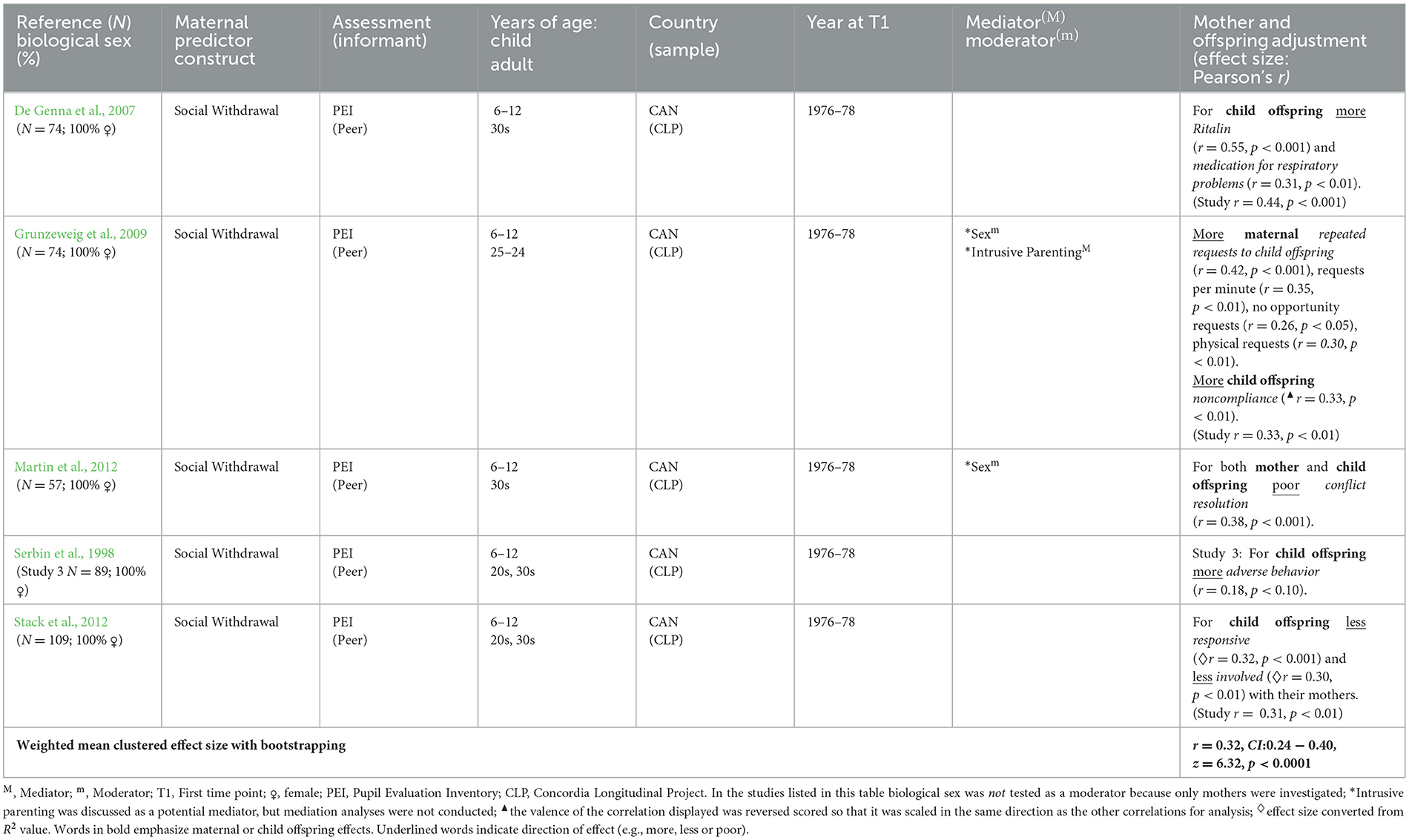
Table 6. Intergenerational difficulties for mothers and their offspring (N = 5 studies, N = 1 sample, N = 109 mothers, N = 175 offspring).
3.3.5.1 Mothering
Mothers' childhood social withdrawal (controlling for their childhood aggression) predicted their parenting when mother-child dyads engaged in interactive and confrontational tasks in two related studies (Grunzeweig et al., 2009; Serbin et al., 1998). Mothers with childhood social withdrawal were observed to be less responsive and supportive (Serbin et al., 1998), and more rapidly repeat requests and physically intervene (Grunzeweig et al., 2009) with their offspring. Nonetheless, these parenting behaviors may have been evoked by offspring behavior.
3.3.5.2 Offspring behavior and health
Mothers' childhood social withdrawal was evaluated as a predictor of their offspring's interactions with their mothers or offspring health in five studies. Mothers' childhood social withdrawal (controlling for their childhood aggression) directly predicted greater offspring unresponsiveness and fewer efforts to elicit maternal involvement (Stack et al., 2012), offspring aggression toward mothers (Serbin et al., 1998), and indirectly predicted more offspring noncompliance through repeated maternal requests, and offspring defiance though maternal physical intervention (Grunzeweig et al., 2009).
Also, mothers' childhood social withdrawal predicted their offspring's atypical social problem-solving: offspring provided more solutions for resolving a conflict, but more autonomous solutions (i.e., solitary solutions without help from others, Martin et al., 2012). However, it is unclear whether offspring demonstrated this tendency only with their mothers, or also with peers.
Additionally, mothers' childhood social withdrawal predicted more offspring headaches/migraines and medication for attention-deficit disorder (ADD: Ritalin) and respiratory problems, despite no higher incidence of these conditions in mothers (De Genna et al., 2007).
Taken together, findings support links between mothers' childhood social withdrawal and subsequent suboptimal mothering and offspring behavioral maladjustment and ill-health. Because all publications were based on the same sample, results may be influenced by its sociocultural context (i.e., low SES French-Canadian population in Montreal). Therefore, replication of results in other samples will be needed to increase confidence in the generalizability of findings.
4 Discussion
This is the first systematic review and set of meta-analyses of psychosocial adjustment in adults with childhood and/or adolescent histories of social withdrawal. Meta-analyses of available prospective longitudinal studies indicate that childhood social withdrawal was a risk factor for adult psychosocial maladjustment across multiple domains—the strongest effects were for SAD sx/dx and intergenerational difficulties in mothers with childhood social withdrawal and their offspring, and more modest effects occurred for delayed adult developmental milestones, adult social withdrawal, and risk for other adult internalizing problems (other anxiety, depression sx/dx).
Conversely, meta-analysis indicated that childhood social withdrawal was a modest protective factor for adult substance abuse. This result is contrary to the idea that adults with childhood social withdrawal use substances to self-medicate (Turner et al., 2018).
Analyses revealed that the effect sizes entered into meta-analyses were heterogeneous, suggesting that the relation between childhood social withdrawal and adult outcomes is likely to be moderated by other factors, such as biological sex. In individual publications, women and men with childhood social withdrawal often demonstrated differences in adult psychosocial adjustment (except for internalizing problems), as described below. Nonetheless, the overarching pattern of findings from individual publications indicates that childhood social withdrawal was a risk factor for adult psychosocial maladjustment in both women and men.
4.1 Meta-analytic results
Meta-analytic results support childhood social withdrawal as a medium-sized risk factor for adult SAD sx/dx and intergenerational difficulties in mothers with childhood histories of social withdrawal and their offspring; as well as a small-size risk factor for delayed adult developmental milestones, social withdrawal, other anxiety disorders, and depression. Meta-analytic results also support childhood social withdrawal as a small-size protective factor for substance abuse. Each of these forms of adjustment in adults with childhood social withdrawal is discussed in turn in the following sections.
Analyses of heterogeneity of effect sizes among individual studies contributing to each form of adult adjustment (except for intergenerational effects) suggests that the relation between childhood social withdrawal and adult outcomes was likely to be moderated by other factors, but available information was insufficient for moderated meta-analyses. Therefore, we also review available evidence from individual studies for moderation by biological sex (and generation for adult developmental milestones).
4.2 Adult developmental milestones, biological sex, and generation
Consistent with the proposed missing out mechanism, meta-analytic results support childhood social withdrawal as a small-size risk factor for delayed adult developmental milestones for participation in families and society. The modest size of meta-analytic effects for adult developmental milestones may be due to their heterogeneity (e.g., employment, romantic relationships), and potential biological sex and generational moderation. Many individual studies indicated that childhood social withdrawal predicted delays in adult developmental milestones specific to biological sex, and the pattern of findings across studies with samples from different generations suggests that generational shifts may have occurred in some of these patterns over time.
In earlier generations, the pattern of individual study findings suggests that American women and men with childhood histories of social withdrawal, compared to their non-withdrawn same-sex counterparts, demonstrated different occupational delays (for women abbreviated or no work history, for men delayed entry into a stable career), and men demonstrated delayed romantic partnerships and procreation. In recent generations, both women and men with childhood histories of social withdrawal demonstrated similar delays in entering the work force and adult financial milestones, and men continued to demonstrate delayed romantic partnerships. Therefore, individual study patterns suggest potential moderation by biological sex and generation in which women as well as men now experience similarly delayed adult occupational and financial milestones. This potential generational shift suggests that childhood social withdrawal was detrimental for women in recent generations who were expected to take initiative in occupational and financial domains based on changed cultural norms. This pattern is also consistent with the possibility that more change in women's roles may have occurred in Western countries at a societal level than in heterosexual romantic and familial relationships. Nonetheless, because recent studies were conducted abroad, study of contemporary American adults with childhood social withdrawal is needed.
The pattern of results across investigations also suggests that the link between childhood social withdrawal and certain adult developmental milestones demonstrated some cultural specificity within Western countries. In particular, men with childhood social withdrawal demonstrated less occupational stability and achievement in the US (Caspi et al., 1989, 1988), but not Sweden (Kerr et al., 1996). This pattern may reflect greater demands for men's self-assertion in American vs. Swedish workplaces (Kerr et al., 1996). These patterns suggest that adults with childhood social withdrawal may find American workplaces inaccessible or that their competitive culture is incompatible with their interaction style. Although recent research supports delayed workforce entry for adults of both sexes with childhood withdrawal in Germany and Canada (Asendorpf et al., 2008; Denissen et al., 2008; Schmidt et al., 2017), further research is needed to examine whether such occupational delays occur for contemporary American adults.
Despite these occupational patterns, women with vs. without childhood social withdrawal did not demonstrate lower educational attainment in the US, but attained less education in Sweden (Kerr et al., 1996) and Canada (Serbin et al., 1998, 2011), and demonstrated poor educational achievement in Canada (Serbin et al., 1998, 2011). Therefore, despite the competitiveness of American work culture, the range of educational opportunities available in the US may support educational parity for adults with childhood histories of social withdrawal. As more studies become available from diverse cultures in the future, more nuanced meta-analytic results may be obtained by separate moderated meta-analysis of specific types of adult developmental milestones.
4.3 Social withdrawal and internalizing difficulties
Consistent with expectations, childhood social withdrawal was a medium-size predictor of adult SAD sx/dx, and small-sized predictor of adult social withdrawal, other anxiety (e.g., GAD, OCD, specific phobias, panic disorder, and agoraphobia), depressive sx/dx, and all of these internalizing difficulties combined. These long-term longitudinal linkages between childhood social withdrawal and subsequent adult internalizing psychopathology reflect more than homotypic continuity. For childhood social withdrawal, which is not a diagnosis of psychopathology, to predict adult psychopathology it must translate into significant distress and impairment in functioning (i.e., life interference, Gazelle and Rubin, 2010). Socially withdrawn children and adolescents may experience distress when they experience significant interpersonal stress (e.g., peer exclusion and victimization) and/or lack of support (e.g., low maternal sensitivity). These patterns are compatible with diathesis (vulnerability)-stress processes in which individuals with childhood social withdrawal may develop psychopathology in the context of interpersonal stress, or experience mental health in the context of interpersonal support and low interpersonal stress (Gazelle and Rubin, 2019). Importantly diathesis-stress models of the development of psychopathology should nonetheless be informed by a broader Developmental Science perspective to provide insight on developmentally-relevant stressors (e.g., peer difficulties) and vulnerable periods of development (e.g., school transitions, puberty). Much is left to be understood about the circumstances under which individuals demonstrate continuity vs. change in social withdrawal from childhood and adolescence to adulthood and develop internalizing psychopathology or relative mental health by adulthood.
Parenting moderated the link between child social withdrawal and adult internalizing psychopathology in one reviewed publication. Low maternal sensitivity at age 4 strengthened (moderated) the relation between childhood shyness/inhibition and adult social anxiety and depression (Table 3, Bohlin and Hagekull, 2009). In the future, other interpersonal influences (e.g., peer relations) on the development of internalizing psychopathology should be investigated in adults with childhood social withdrawal.
With few exceptions, internalizing problems occurred in both women and men with childhood social withdrawal. Although extant research indicates that women compared to men experience higher rates of internalizing problems overall (Albano and Krain, 2005), results of individual studies included in our meta-analysis indicated that adults of both sexes who experienced childhood social withdrawal were at risk for adult internalizing psychopathology. This lack of biological sex differences suggests that childhood patterns of social withdrawal identify individuals who, perhaps regardless of their biological sex, have a long-term tendency to respond to stress in ways that render them vulnerable to internalizing difficulties (e.g., rumination).
Nonetheless, women and men with childhood social withdrawal may develop internalizing problems through somewhat different mechanisms. The only two instances of gender moderation of risk for adult internalizing psychopathology in individual reviewed publications involved moderation of indirect or mediated effects. This may have occurred because girls and women may weight their relationships more strongly in their self-appraisals and, therefore, are more likely to develop internalizing problems when they experience interpersonal difficulties (Albano and Krain, 2005), whereas boys and men may weight their achievement at school and work more strongly in their self-appraisals.
4.4 Intergenerational difficulties
Consistent with the proposed interpersonal stress and relationship quality mechanisms, meta-analysis revealed that childhood social withdrawal was a medium-size predictor of intergenerational difficulties in mothers and their offspring. Women with childhood social withdrawal demonstrated unresponsive or intrusive parenting of their offspring, and their offspring responded to them with non-compliance, defiance, and aggression (Table 6). This parenting pattern may reflect a general tendency to enact ineffective strategies for pursuing social goals. Offspring's responses may suggest both withdrawn and externalizing behavior, but it is not clear whether these behaviors generalize beyond interactions with their mother. These patterns suggest that relationship difficulties are central to adult maladjustment and intergenerational transmission of risk in women with childhood histories of social withdrawal. However, as these intergenerational investigations were exclusively conducted with the urban, low-income, French Canadian CLP sample, it will be important to investigate whether they generalize to other contexts and samples.
4.5 Substance use
Meta-analytic results support childhood social withdrawal (controlling for childhood aggression) as a small-size protective factor against adult substance use. All studies included in the meta-analysis reported that childhood social withdrawal predicted less adult substance use.
Meta-analytic evidence that childhood social withdrawal protects against adult substance use is important because it contradicts suggestions that anxious individuals might use substances to self-medicate (Turner et al., 2018). Rather, childhood social withdrawal may protect adults from substance use by reducing the likelihood that they are introduced to such behavior via social situations (e.g., parties) and friends (Foster et al., 2018; Martin-Storey et al., 2011), consistent with the missing out mechanism. Additionally, adults with childhood social withdrawal likely tend to have over-controlled tendencies, and may dislike the prospect of losing control via substance use.
One study not included in the meta-analysis (due to person-oriented results that could not be combined with variable-oriented results from other studies in a weighted mean) found that childhood shyness was related to increased risk for substance use (Tang et al., 2017). However, this finding was likely due to no control for childhood aggression. Therefore, aggressive-withdrawn children (Gazelle and Ladd, 2003; Ladd and Burgess, 1999) may be at risk for substance use. This pattern resembles that in Foster et al. (2018), in which the non-shared variance between childhood social withdrawal and externalizing problems reduced risk for adult alcohol problems, whereas their shared variance (perhaps negative affect) increased risk for adult alcohol problems.
4.6 Physical health
Meta-analytic results did not suggest that childhood social withdrawal predicts adult physical health. However, the health conditions investigated in available publications were heterogeneous. The pattern of individual study results suggest that childhood social withdrawal predicted higher BMI and more dental visits in adults, headaches and pregnancy difficulties in women, but fewer adult injuries in men (Table 5). Social withdrawal may have reduced men's inclination to engage in risky behavior, resulting in fewer injuries. Therefore, adults with childhood social withdrawal may be less likely to engage in adult health risk behaviors (i.e., physical injury for men and substance use for both sexes). In the future, as more studies become available, moderated (biological sex) meta-analyses conducted separately by type of health condition will be warranted.
4.7 Contributions, limitations, and future directions
This is the first systematic review and meta-analysis of psychosocial adjustment in adults with childhood social withdrawal. This set of meta-analyses of prospective longitudinal studies contributes to current knowledge by supporting childhood social withdrawal as a risk factor for multiple forms of adult psychosocial maladjustment, but a protective factor against adult substance abuse.
The focus of this set of meta-analyses of childhood social withdrawal among peers is unique, as previous meta-analyses on the most closely related topics have focused on behavioral inhibition to unfamiliar people, objects, and situations as a risk for subsequent anxiety (Clauss and Blackford, 2012; Sandstrom et al., 2020). We reviewed longitudinal studies of adjustment in adults with childhood social withdrawal and related constructs in relation to peers in general, rather than exclusively in relation to unfamiliar social partners. We imposed as much clarity as possible on the operationalization of social withdrawal by the theoretically-motivated selection of studies which had assessed social withdrawal in relation to peers in general, including familiar peers such as classmates (not only unfamiliar social partners), to emphasize functioning among familiar peers. We encourage future investigators to assess children's withdrawal in relation to familiar peers because this is most likely to impact psychosocial development (Asendorpf, 1990b; Gazelle and Faldowski, 2014). We also encourage assessment of anxious and solitary behaviors, in addition to socially anxious affect and self-conscious thoughts. These methods may yield stronger, more consistent future findings.
The number of publications and longitudinal samples upon which they were based, and combined sample size across those publications was greater for some adult outcomes than others (Tables 2–6). Therefore, to ensure the accuracy of results, we conducted statistical tests with methods that are well-suited to small samples (i.e., bootstrapping, Joshi et al., 2022). Importantly, effect sizes and the significance of effects appear to correspond to the nature of each outcome rather than the number of publications, number of longitudinal samples, or combined sample size for each outcome. For instance, meta-analysis revealed a highly significant medium size effect for adult social anxiety based on 3 publications derived from 3 longitudinal samples and a combined sample size of 1,419 adults, and this was reinforced by a highly significant small size effect for the umbrella construct of internalizing difficulties (which included social anxiety) which was based on 12 publications derived from 9 longitudinal samples and a combined sample size of 4,361 adults. In contrast, meta-analysis yielded a non-significant effect for adult physical health despite being based on 5 publications derived from 2 longitudinal samples and a combined sample size of 13,404 adults. Importantly, this pattern of results was also in line with our hypotheses.
Likewise, although meta-analysis of intergenerational outcomes was based on 5 studies and a combined sample of 109 mothers and 175 offspring, it yielded a highly significant medium sized effect. Nonetheless, because the data for this intergenerational effect is based on a single longitudinal sample, future replication of results in other samples would increase confidence in intergenerational effects.
The studies included in the meta-analyses assessed social withdrawal across a broad range of ages in childhood and adolescence through 16 years of age. Because the focus of this paper is on long term longitudinal studies, some studies used childhood and adolescent social withdrawal predictors that were based on repeated measurements across childhood and adolescence (Jaffee et al., 2002; Kerr et al., 1996). Also, other studies used social withdrawal predictors that were composites of repeated assessments at ages 6 and younger (Asendorpf et al., 2008; Denissen et al., 2008; Tang et al., 2022), whereas other studies assessed children at one time point at ages ranging from 6 to older (CLP studies, Crum et al., 2006; Ensminger et al., 2002; Fothergill and Ensminger, 2006), so that there was overlap at 6 years of age even between studies that assessed children at mostly younger or older ages. Therefore, it was not possible to enter the age at which social withdrawal was assessed in childhood or adolescence in the analyses.
Moreover, we did not advance hypotheses about the relation between age of social withdrawal assessment in childhood or adolescence and prediction of adult outcomes. We did not advance such hypotheses because previous research had shown that social withdrawal assessed in different developmental periods (both middle childhood and early adolescence) are both predictive of psychosocial adjustment difficulties in early adolescence (Gazelle and Faldowski, 2019). This is partially due to continuity in social withdrawal from middle childhood through early adolescence, but also when social withdrawal emerged in early adolescence it was predictive of concurrent adjustment difficulties (Gazelle and Faldowski, 2019). Similar comparisons of childhood and adolescent developmental periods have not been tested for prediction of adult outcomes (for an exception see Fichter et al., 2009), but based on these findings earlier in development, as well as one study of adult outcomes (Fichter et al., 2009), we would expect that social withdrawal across a broad range of ages in childhood and adolescence would predict adult psychosocial difficulties. Many investigations support this assumption, as many of the investigations included in our meta-analyses successfully utilized assessments across childhood and adolescence as predictors of adult adjustment (Jaffee et al., 2002; Kerr et al., 1996).
The studies included in our meta-analyses also predicted outcomes across a broad range of ages in adulthood (and late adolescence from 17 to 40 years of age). Because the focus of this paper is on long term longitudinal studies, an overarching pattern (e.g., delay in adult developmental milestones) is often assessed across a broad span of adulthood (and late adolescence), but the manifestation of that pattern was assessed in a developmentally appropriate manner (e.g., delay in starting first job in late adolescence and early adulthood vs. delay in achieving a stable career in middle adulthood). Thus, the reviewed studies were able to capture an overarching pattern of psychosocial adjustment despite variation in specific manifestations at different points of adult development. Other outcomes (e.g., internalizing problems) have stable assessments across adulthood, but these assessments flexibly allow for different manifestations across adult development (e.g., life interference at earlier vs. later ages may be manifested at school vs. work or in dating vs. marital relationships). Thus, although the extent of the research available at this point does not allow for a comparison of adult outcomes during different periods of adult development, it does an excellent job of capturing adaptational patterns relevant across adult development.
All studies which met our review criteria were conducted in Western countries. No studies were excluded due to non-English language. In the future prospective long-term longitudinal studies of socially withdrawn children should be conducted in diverse global contexts to achieve a fuller understanding of contextual influences on life-course development. This is important because the implications of childhood social withdrawal for children's peer relationships are culturally specific (Chen and French, 2008) and this may also translate into culturally-specific life-course outcomes. Social withdrawal also has culturally-specific manifestations, such as “hikikomori” in Japan, in which young people physically isolate themselves in their room at home and do not go out into society (Furlong, 2008). Such culturally-specific manifestations of social withdrawal may be especially likely to translate into culturally-specific life-course outcomes.
Most studies of psychosocial adjustment in adults with childhood social withdrawal used designs which compare adults with vs. without childhood social withdrawal. However, designs are needed that compare adults with childhood social withdrawal who demonstrate psychosocial maladjustment to their counterparts who demonstrate adaptive development. This requires testing mediators and moderators of adjustment over time.
This review revealed that few studies have tested interpersonal mediators of the relation between childhood withdrawal and adult psychosocial adjustment (Tables 2–6). Such research is needed to support efforts to interrupt interpersonal processes that lead to psychosocial maladjustment in adults with childhood social withdrawal.
Contemporary research is increasingly investigating biological mechanisms of anxiety development. Although no reviewed studies examined biological mechanisms in anxiety development (despite recent coverage of biological criterions such as BMI), individuals with increasing shyness trajectories demonstrated adult hypervigilance to angry faces (Tang et al., 2017). Such findings are typically interpreted as evidence for a temperamentally based attentional “bias” toward threat which is thought to be a mechanism involved in the development of anxiety disorders. However, attentional patterns can be learned in threatening environments (Shackman et al., 2007) and may be adaptive in such environments, but maladaptive when they transfer to other environments. Therefore, future studies should investigate both environmental and biological origins of sensitivity toward threat and integrate biological assessment (including genetic vulnerability, Hoekstra et al., 2008) into investigations of the life course development of socially withdrawn children.
5 Conclusion
Meta-analytic evidence indicates that childhood social withdrawal forecasts adult psychosocial maladjustment in multiple domains. However, future research on life-course development in contemporary American samples of socially withdrawn children is needed for several reasons. First, little relevant research has been conducted in the US recently, so adjustment patterns in contemporary American adults with childhood social withdrawal are uncertain. Second, updated evidence for American samples is needed because anxiety rates in American youth have been at historic highs since the 90s (Twenge, 2011). Third, contemporary patterns may differ from historic and cross-cultural patterns for women given their changed gender roles and increased participation in education and the workplace. Finally, key interpersonal, self , and educational processes that link child social withdrawal to adult psychosocial adjustment are poorly understood. Processes consistent with the missing out, interpersonal stress, relationship quality, and developmental cascade mechanisms (Masten and Cicchetti, 2010) need to be tested. Empirical tests of interpersonal, self, educational, and biological processes that may mediate the relation between childhood social withdrawal and adult psychosocial adjustment are needed to yield sufficient evidence for mediated meta-analyses and guide prevention and therapeutic efforts. Such efforts aim to assist adults with childhood social withdrawal in reaching their full potential and becoming healthy and fully participating members of their families and society (Véronneau et al., 2015).
Data availability statement
The original contributions presented in the study are included in the article/Supplementary material, further inquiries can be directed to the corresponding author.
Author contributions
HG: Conceptualization, Funding acquisition, Methodology, Resources, Supervision, Writing – original draft, Writing – review & editing. JS: Data curation, Formal analysis, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. HL: Conceptualization, Formal analysis, Writing – original draft, Writing – review & editing. HC: Conceptualization, Formal analysis, Supervision, Writing – original draft, Writing – review & editing. ML: Formal analysis, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. The publication of this article was partially supported by Florida State University Libraries' Open Access Fund.
Acknowledgments
Thanks to support from the Department of Human Development and Family Science at Florida State University.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fdpys.2024.1408166/full#supplementary-material
Footnotes
1. ^This proportion and n of adult participants by biological sex does not include the sample from one publication (n = 85, Bohlin and Hagekull, 2009) in which biological sex was not reported.
2. ^The number of studies with unique effects for each outcome that were included in each meta-analysis is specified in each section (not counting studies with duplicate effects marked with an × in Tables 2–6).
3. ^References included in meta-analyses.
References
Albano, A. M., and Krain, A. (2005). “Anxiety and anxiety disorders in girls,” in Handbook of behavioral and emotional problems in girls, eds. D. J. Bell, S. L. Foster, and E. J. Mash (Netherlands: Kluwer), 79–116. doi: 10.1007/0-306-48674-1_3
APA. (2022). Diagnostic and Statistical Manual of Mental Disorders (5th ed., text rev. ed.). London: Routledge.
Asendorpf, J. B. (1990a). Beyond social withdrawal: shyness, unsociability, and peer avoidance. Hum. Dev. 33, 250–259. doi: 10.1159/000276522
Asendorpf, J. B. (1990b). Development of inhibition during childhood: evidence for situational specificity and a two-factor model. Dev. Psychol. 26, 721–730. doi: 10.1037//0012-1649.26.5.721
*Asendorpf, J. B., Denissen, J. J. A., and van Aken, M. A. G. (2008). Inhibited and aggressive preschool children at 23 years of age: Personality and social transitions into adulthood. Dev. Psychol. 44, 997–1011. doi: 10.1037/0012-1649.44.4.997
Bergman, L. R., Cairns, R. B., Nilsson, L.-G., and Nystedt, L. (2000). Developmental Science and the Holistic Approach. New York: Psychology Press. doi: 10.4324/9781410605405
*Bohlin, G., and Hagekull, B. (2009). Socio-emotional development: from infancy to young adulthood. Scand. J. Psychol. 50, 592–601. doi: 10.1111/j.1467-9450.2009.00787.x
Boivin, M., Hymel, S., and Hodges, E. V. (2001). “Toward a process view of peer rejection and harassment,” in Peer harassment in school: The plight of the vulnerable and victimized, 265–289.
Boivin, M., and Vitaro, F. (1995). “The impact of peer relationships on aggression in childhood: Inhibition through coercion or promotion through peer support,” in Coercion and punishment in long-term perspectives, ed. J. McCord (Cambridge: Cambridge University Press), 183–197. doi: 10.1017/CBO9780511527906.011
Borenstein, M., Hedges, L. V., Higgins, J. P., and Rothstein, H. R. (2021). “Converting among effect sizes,” in Introduction to meta-analysis (Wiley), 43–47. doi: 10.1002/9781119558378.ch7
Bretherton, I., and Munholland, K. A. (2008). “Internal working models in attachment relationships: elaborating a central construct in attachment theory,” in Handbook of attachment: Theory, research, and clinical applications, 2nd ed. (The Guilford Press), 102–127.
Canty, A., and Ripley, B. D. (2024). “Boot: Bootstrap r (s-plus) functions,” in R package version 1.3–30.
*Caspi, A., Bem, D. J., and Elder, G. H. (1989). Continuities and consequences of interactional styles across the life course. J. Pers. 57, 375–406. doi: 10.1111/j.1467-6494.1989.tb00487.x
*Caspi, A., Elder, G. H., and Bem, D. J. (1988). Moving away from the world: life-course patterns of shy children. Dev. Psychol. 24, 824–831. doi: 10.1037/0012-1649.24.6.824
Chen, X., and French, D. C. (2008). Children's social competence in cultural context. Annu. Rev. Psychol. 59, 591–616. doi: 10.1146/annurev.psych.59.103006.093606
Clauss, J. A., and Blackford, J. U. (2012). Behavioral inhibition and risk for developing social anxiety disorder: a meta-analytic study. J. Am. Acad. Child Adol. Psychiat. 51, 1066–1075.e1061. doi: 10.1016/j.jaac.2012.08.002
Cohen, 1988 Cohen, J. (1988). Statistical Power Analysis for the Behavioral Sciences (2nd ed.). London: Routledge.
Copeland, W. E., Angold, A., Shanahan, L., and Costello, E. J. (2014). Longitudinal patterns of anxiety from childhood to adulthood: the great smoky mountains study. J. Am. Acad. Child Adolesc. Psychiatry 53, 21–33. doi: 10.1016/j.jaac.2013.09.017
Coplan, R. J., Rose-Krasnor, L., Weeks, M., Kingsbury, A., Kingsbury, M., and Bullock, A. (2013). Alone is a crowd: Social motivations, social withdrawal, and socioemotional functioning in later childhood. Dev. Psychol. 49:861. doi: 10.1037/a0028861
Coplan, R. J., Rubin, K. H., Fox, N. A., Calkins, S. D., and Stewart, S. L. (1994). Being alone, playing alone, and acting alone: distinguishing among reticence and passive and active solitude in young children. Child Dev. 65, 129–137. doi: 10.2307/1131370
*Crum, R. M., Juon, H.-S., Green, K. M., Robertson, J., Fothergill, K., and Ensminger, M. (2006). Educational achievement and early school behavior as predictors of alcohol-use disorders: 35-year follow-up of the woodlawn study. J. Stud. Alcohol 67, 75–85. doi: 10.15288/jsa.2006.67.75
Cumming, G. (2013). Understanding the New Statistics: Effect Sizes, Confidence Intrervals, and Meta-Analysis. London: Routledge. doi: 10.4324/9780203807002
Davison, A. C., and Hinkley, D. V. (1997). Bootstrap Methods and Their Application (Vol. No. 1). Cambridge: Cambridge University Press. doi: 10.1017/CBO9780511802843
*De Genna, N. M., Stack, D. M., Serbin, L. A., Ledingham, J., and Schwartzman, A. E. (2007). Maternal and child health problems: the inter-generational consequences of early maternal aggression and withdrawal. Soc. Sci. Med. 64, 2417–2426. doi: 10.1016/j.socscimed.2007.03.001
*De Genna, N. M., Stack, D. M., Serbin, L. A., Ledingham, J. E., and Schwartzman, A. E. (2006). From risky behavior to health risk: continuity across two generations. J. Dev. Behav. Pediatr. 27, 297–309. doi: 10.1097/00004703-200608000-00004
*Denissen, J. J. A., Asendorpf, J. B., and Van Aken, M. A. G. (2008). Childhood personality predicts long-term trajectories of shyness and aggressiveness in the context of demographic transitions in emerging adulthood. J. Pers. 76, 67–100. doi: 10.1111/j.1467-6494.2007.00480.x
*Ensminger, M. E., Juon, H. S., and Fothergill, K. E. (2002). Childhood and adolescent antecedents of substance use in adulthood. Addiction 97, 833–844. doi: 10.1046/j.1360-0443.2002.00138.x
*Fichter, M. M., Kohlboeck, G., Quadflieg, N., Wyschkon, A., and Esser, G. (2009). From childhood to adult age: 18-year longitudinal results and prediction of the course of mental disorders in the community. Soc. Psychiat. Psychiatr. Epidemiol. 44, 792–803. doi: 10.1007/s00127-009-0501-y
*Foster, K. T., Hicks, B. M., and Zucker, R. A. (2018). Positive and negative effects of internalizing on alcohol use problems from childhood to young adulthood: the mediating and suppressing role of externalizing. J. Abnorm. Psychol. 127, 394–403. doi: 10.1037/abn0000337
*Fothergill, K. E., and Ensminger, M. E. (2006). Childhood and adolescent antecedents of drug and alcohol problems: a longitudinal study. Drug. Alcohol. Depend. 82, 61–76. doi: 10.1016/j.drugalcdep.2005.08.009
Furlong, A. (2008). The japanese hikikomori phenomenon: acute social withdrawal among young people. Sociol. Rev. 56, 309–325. doi: 10.1111/j.1467-954X.2008.00790.x
Gazelle, H. (2022). Two models of the development of social withdrawal and social anxiety in childhood and adolescence: progress and blind spots. Children 9:734. doi: 10.3390/children9050734
Gazelle, H., and Cui, M. (2020). Relations among anxious solitude, peer exclusion, and maternal overcontrol from 3rd through 7th grade: peer effects on youth, youth evocative effects on mothering, and the indirect effect of peers on mothering via youth. J. Abnorm. Child Psychol. 48, 1485–1498. doi: 10.1007/s10802-020-00685-w
Gazelle, H., and Cui, M. (2021). Anxious solitude, reciprocated friendships with peers, and maternal overcontrol from third through seventh grade: a transactional model. Children 8:379. doi: 10.3390/children8050379
Gazelle, H., and Faldowski, R. A. (2014). Peer exclusion is linked to inhibition with familiar but not unfamiliar peers at two years of age. Infant Child Dev. 23, 220–228. doi: 10.1002/icd.1853
Gazelle, H., and Faldowski, R. A. (2019). Multiple trajectories in anxious solitary youths: the middle school transition as a turning point in development. J. Abnorm. Child Psychol. 47, 1135–1152. doi: 10.1007/s10802-019-00523-8
Gazelle, H., and Ladd, G. W. (2003). Anxious solitude and peer exclusion: a diathesis-stress model of internalizing trajectories in childhood. Child Dev. 74, 257–278. doi: 10.1111/1467-8624.00534
Gazelle, H., Putallaz, M., Li, Y., Grimes, C. L., Kupersmidt, J. B., and Coie, J. D. (2005). Anxious solitude across contexts: Girls' interactions with familiar and unfamiliar peers. Child Dev. 76, 227–246. doi: 10.1111/j.1467-8624.2005.00841.x
Gazelle, H., and Rubin, K. H. (2010). “Social anxiety in childhood: Bridging developmental and clinical perspectives,” in Social anxiety in childhood: Bridging developmental and clinical perspectives: New directions in child and adolescent development, eds. H. Gazelle and K. H. Rubin (New York: Jossey-Bass), 1–16. doi: 10.1002/cd.259
Gazelle, H., and Rubin, K. H. (2019). Social withdrawal and anxiety in childhood and adolescence: Interaction between individual tendencies and interpersonal learning mechanisms in development: Introduction to the special issue. J. Abnorm. Child Psychol. 47, 1101–1106. doi: 10.1007/s10802-019-00557-y
*Gest, S. D., Sesma, A., Masten, A. S., and Tellegen, A. (2006). Childhood peer reputation as a predictor of competence and symptoms 10 years later. J. Abnorm. Child Psychol. 34:507. doi: 10.1007/s10802-006-9029-8
*Goodwin, R. D., Fergusson, D. M., and Horwood, L. J. (2004). Early anxious/withdrawn behaviours predict later internalising disorders. J. Child Psychol. Psychiatry 45, 874–883. doi: 10.1111/j.1469-7610.2004.00279.x
Gottman, J. M., and Graziano, W. G. (1983). How children become friends. Monogr. Soc. Res. Child Dev. 48, 1–86. doi: 10.2307/1165860
*Grunzeweig, N., Stack, D. M., Serbin, L. A., Ledingham, J., and Schwartzman, A. E. (2009). Effects of maternal childhood aggression and social withdrawal on maternal request strategies and child compliance and noncompliance. J. Appl. Dev. Psychol. 30, 724–737. doi: 10.1016/j.appdev.2009.02.001
Hedges, L. V., Tipton, E., and Johnson, M. C. (2010). Robust variance estimation in meta-regression with dependent effect size estimates. Res. Synth. Methods 1, 39–65. doi: 10.1002/jrsm.5
Hoekstra, R. A., Bartels, M., Hudziak, J. J., Van Beijsterveldt, T. C. E. M., and Boomsma, D. I. (2008). Genetic and environmental influences on the stability of withdrawn behavior in children: a longitudinal, multi-informant twin study. Behav. Genet. 38, 447–461. doi: 10.1007/s10519-008-9213-4
*Jaffee, S. R., Moffitt, T. E., Caspi, A., Fombonne, E., Poulton, R., and Martin, J. (2002). Differences in early childhood risk factors for juvenile-onset and adult-onset depression. Arch. Gen. Psychiatry 59, 215–222. doi: 10.1001/archpsyc.59.3.215
*Jakobsen, I. S., Horwood, L. J., and Fergusson, D. M. (2012). Childhood anxiety/withdrawal, adolescent parent–child attachment and later risk of depression and anxiety disorder. J. Child Fam. Stud. 21, 303–310. doi: 10.1007/s10826-011-9476-x
Joshi, M., Pustejovsky, J. E., and Beretvas, S. N. (2022). Cluster wild bootstrapping to handle dependent effect sizes in meta-analysis with a small number of studies. Res. Synth. Methods 13, 457–477. doi: 10.1002/jrsm.1554
*Kagan, J., Moss, H. A., and Kagan, S. (1962). Birth to Maturity: A Study in Psychological Development. New Haven: Yale University Press. doi: 10.1037/13129-000
Kagan, J., Snidman, N., Kahn, V., and Towsley, S. (2007). “The preservation of two infant temperaments into adolescence,” in Monographs of the Society for Research in Child Development, 8–18.
*Katz, S. J., Conway, C., Hammen, C., Brennan, P., and Najman, J. (2011). Childhood social withdrawal, interpersonal impairment, and young adult depression: a mediational model. J. Abnorm. Child Psychol. 39, 1227–1238. doi: 10.1007/s10802-011-9537-z
*Kerr, M., Lambert, W. W., and Bem, D. J. (1996). Life course sequelae of childhood shyness in sweden: comparison with the united states. Dev. Psychol. 32, 1100–1105. doi: 10.1037/0012-1649.32.6.1100
Kochenderfer, B. J., and Ladd, G. W. (1997). Victimized children's responses to peers' aggression: behaviors associated with reduced versus continued victimization. Dev. Psychopathol. 9, 59–73. doi: 10.1017/S0954579497001065
Ladd, G. W., and Burgess, K. B. (1999). Charting the relationship trajectories of aggressive, withdrawn, and aggressive/withdrawn children during early grade school. Child Dev. 70, 910–929. doi: 10.1111/1467-8624.00066
Ladd, G. W., and Coleman, C. C. (1997). Children's classroom peer relationships and early school attitudes: Concurrent and longitudinal associations. Early Educ. Dev. 8, 51–66. doi: 10.1207/s15566935eed0801_5
Lerner, R., Hershberg, R., Hilliard, L., and Johnson, S. (2015). “Concepts and theories of human development,” in Developmental science: An advanced textbook, eds. M. H. Bornstein and M. E. Lamb (New York: Taylor and Francis), 3–42.
Lin, L., and Chu, H. (2018). Quantifying publication bias in meta-analysis. Biometrics 74, 785–794. doi: 10.1111/biom.12817
Magnusson, D., and Stattin, H. (2006). “The person in context: a holistic-interactionistic approach,” in Handbook of child psychology: Vol 3. Social, emotional, and personality development, eds. W. Damon and R. M. Lerner (New York: Wiley), 400–464. doi: 10.1002/9780470147658.chpsy0108
*Martin, J. P., Stack, D. M., Serbin, L. A., Schwartzman, A. E., and Ledingham, J. (2012). Social problem solving in high-risk mother—child dyads: an intergenerational study. Soc. Dev. 21, 47–67. doi: 10.1111/j.1467-9507.2011.00600.x
*Martin-Storey, A., Serbin, L. A., Stack, D. M., Ledingham, J. E., and Schwartzman, A. E. (2011). Self and peer perceptions of childhood aggression, social withdrawal and likeability predict adult substance abuse and dependence in men and women: a 30-year prospective longitudinal study. Addict. Behav. 36, 1267–1274. doi: 10.1016/j.addbeh.2011.07.043
*Martin-Storey, A., Serbin, L. A., Stack, D. M., Ledingham, J. E., and Schwartzman, A. E. (2012). Self and peer perceptions of childhood aggression, social withdrawal and likeability predict adult personality factors: a prospective longitudinal study. Pers. Individ. Dif. 53, 843–848. doi: 10.1016/j.paid.2012.06.018
Masten, A. S., and Cicchetti, D. (2010). Developmental cascades. Dev. Psychopathol. 22, 491–495. doi: 10.1017/S0954579410000222
McDougall, P., and Vaillancourt, T. (2015). Long-term adult outcomes of peer victimization in childhood and adolescence: Pathways to adjustment and maladjustment. Am. Psychol. 70, 300–310. doi: 10.1037/a0039174
*Monk, N. J., McLeod, G. F. H., Mulder, R. T., Spittlehouse, J. K., and Boden, J. M. (2023). Childhood anxious/withdrawn behaviour and later anxiety disorder: a network outcome analysis of a population cohort. Psychol. Med. 53, 1343–1354. doi: 10.1017/S0033291721002889
Page, M. J., Moher, D., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). Prisma 2020 explanation and elaboration: updated guidance and exemplars for reporting systematic reviews. BMJ 372:n160. doi: 10.1136/bmj.n160
Pearcey, S., Gordon, K., Chakrabarti, B., Dodd, H., Halldorsson, B., and Creswell, C. (2021). Research review: the relationship between social anxiety and social cognition in children and adolescents: a systematic review and meta-analysis. J. Child Psychol. Psychiat. 62, 805–821. doi: 10.1111/jcpp.13310
R Core Team (2019). “R: A language and environment for statistical computing,” in Vienna R Foundation for Statistical Computing. Available at: https://www.R-project.org (accessed September 4, 2024).
Rubin, K. H., and Chronis-Tuscano, A. (2021). Perspectives on social withdrawal in childhood: past, present, and prospects. Child Dev. Perspect. 15, 160–167. doi: 10.1111/cdep.12417
Rubin, K. H., Coplan, R. J., and Bowker, J. C. (2009). Social withdrawal in childhood. Annu. Rev. Psychol. 60, 141–171. doi: 10.1146/annurev.psych.60.110707.163642
Sandstrom, A., Uher, R., and Pavlova, B. (2020). Prospective association between childhood behavioral inhibition and anxiety: a meta-analysis. Res. Child Adoles. Psychopathol. 48, 57–66. doi: 10.1007/s10802-019-00588-5
Schmidt, L. A., Tang, A., Day, K. L., Lahat, A., Boyle, M. H., Saigal, S., et al. (2017). Personality development within a generational context: life course outcomes of shy children. Child Psychiatry Hum. Dev. 48, 632–641. doi: 10.1007/s10578-016-0691-y
Schwartzman, A. E., Serbin, L. A., Stack, D. M., Hodgins, S., and Ledingham, J. E. (2009). Likeability, aggression, and social withdrawal in childhood, psychiatric status in maturity: a prospective study. Eur. J. Dev. Sci. 3, 51–63. doi: 10.3233/DEV-2009-3107
*Serbin, L. A., Cooperman, J. M., Peters, P. L., Lehoux, P. M., Stack, D. M., and Schwartzman, A. E. (1998). Intergenerational transfer of psychosocial risk in women with childhood histories of aggression, withdrawal, or aggression and withdrawal. Dev. Psychol. 34, 1246–1262. doi: 10.1037/0012-1649.34.6.1246
*Serbin, L. A., Temcheff, C. E., Cooperman, J. M., Stack, D. M., Ledingham, J., and Schwartzman, A. E. (2011). Predicting family poverty and other disadvantaged conditions for child rearing from childhood aggression and social withdrawal: a 30-year longitudinal study. Int. J. Behav. Dev. 35, 97–106. doi: 10.1177/0165025410372008
Shackman, J. E., Shackman, A. J., and Pollak, S. D. (2007). Physical abuse amplifies attention to threat and increases anxiety in children. Emotion 7, 838–852. doi: 10.1037/1528-3542.7.4.838
Spangler, T., and Gazelle, H. (2009). Anxious solitude, unsociability, and peer exclusion in middle childhood: a multitrait–multimethod matrix. Soc. Dev. 18, 833–856. doi: 10.1111/j.1467-9507.2008.00517.x
*Stack, D. M., Serbin, L. A., Girouard, N., Enns, L. N., Bentley, V. M. N., Ledingham, J. E., et al. (2012). The quality of the mother–child relationship in high-risk dyads: application of the emotional availability scales in an intergenerational, longitudinal study. Dev. Psychopathol. 24, 93–105. doi: 10.1017/S095457941100068X
Sterne, J. A. C., and Harbord, R. M. (2004). Funnel plots in meta-analysis. Stata J. 4, 127–141. doi: 10.1177/1536867X0400400204
Tang, A., Fox, N. A., and Slopen, N. (2022). Examination of early childhood temperament of shyness and social avoidance and associations with cardiometabolic health in young adulthood. JAMA Netw. Open 5:e2144727. doi: 10.1001/jamanetworkopen.2021.44727
Tang, A., Van Lieshout, R. J., Lahat, A., Duku, E., Boyle, M. H., Saigal, S., et al. (2017). Shyness trajectories across the first four decades predict mental health outcomes. J. Abnorm. Child Psychol. 45, 1621–1633. doi: 10.1007/s10802-017-0265-x
Temcheff, C. E., Serbin, L. A., Martin-Storey, A., Stack, D. M., Hastings, P., Ledingham, J., et al. (2011a). Childhood aggression, withdrawal and likeability, and the use of health care later: a longitudinal study. Can. Med. Assoc. J. 183, 2095–2101. doi: 10.1503/cmaj.091830
*Temcheff, C. E., Serbin, L. A., Martin-Storey, A., Stack, D. M., Ledingham, J., and Schwartzman, A. E. (2011b). Predicting adult physical health outcomes from childhood aggression, social withdrawal and likeability: a 30-year prospective, longitudinal study. Int. J. Behav. Med. 18, 5–12. doi: 10.1007/s12529-010-9082-0
Thalheimer, W., and Cook, S. (2002). How to calculate effect sizes from published research: a simplified methodology. Work-Learn. Res. 1, 1–9. Available at: www.work-learning.com/effect_sizes.htm
Turner, S., Mota, N., Bolton, J., and Sareen, J. (2018). Self-medication with alcohol or drugs for mood and anxiety disorders: a narrative review of the epidemiological literature. Depress. Anxiety 35, 851–860. doi: 10.1002/da.22771
Twenge, J. M. (2011). Generational differences in mental health: are children and adolescents suffering more, or less? Am. J. Orthopsychiatry 81, 469–472. doi: 10.1111/j.1939-0025.2011.01115.x
*Véronneau, M.-H., Serbin, L. A., Stack, D. M., Ledingham, J., and Schwartzman, A. E. (2015). Emerging psychopathology moderates upward social mobility: the intergenerational (dis)continuity of socioeconomic status. Dev. Psychopathol. 27, 1217–1236. doi: 10.1017/S0954579415000784
Viechtbauer, W. (2010). Conducting meta-analyses in r with the metafor package. J. Stat. Softw. 36, 1–48. doi: 10.18637/jss.v036.i03
Keywords: child and adolescent social withdrawal/shyness/social anxiety, prospective longitudinal study, meta-analysis, adult psychosocial adjustment, interpersonal processes, child and adolescent development, depression, substance use
Citation: Gazelle H, Shafer Lundin JK, Lei H, Cao H and Litchfield M (2024) Child and adolescent social withdrawal predict adult psychosocial adjustment: A meta-analysis. Front. Dev. Psychol. 2:1408166. doi: 10.3389/fdpys.2024.1408166
Received: 27 March 2024; Accepted: 11 September 2024;
Published: 11 October 2024.
Edited by:
Laura Hanish, Arizona State University, United StatesReviewed by:
Yayouk Eva Willems, Max Planck Institute for Human Development, GermanySilke Schauder, University of Picardie Jules Verne, France
Copyright © 2024 Gazelle, Shafer Lundin, Lei, Cao and Litchfield. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Heidi Gazelle, aGdhemVsbGVAZnN1LmVkdQ==