 Sompop Bencharit1
Sompop Bencharit1 Barry Quinn2
Barry Quinn2 Maria F. Sittoni-Pino3
Maria F. Sittoni-Pino3 Santiago Arias-Herrera3Simona-Georgiana Schick4Sarah Rampf4
Santiago Arias-Herrera3Simona-Georgiana Schick4Sarah Rampf4 Samantha Byrne5Muhammad A. Shazib1Ulf Örtengren6
Samantha Byrne5Muhammad A. Shazib1Ulf Örtengren6 Walter Yu Hang Lam7
Walter Yu Hang Lam7 Mikko Liukkonen8
Mikko Liukkonen8 David Rice9Masako Nagasawa10Amitha Ranauta11
David Rice9Masako Nagasawa10Amitha Ranauta11 Sobia Zafar12Kinga Bágyi13Thomas J. Greany14
Sobia Zafar12Kinga Bágyi13Thomas J. Greany14 Amirul Faiz Luai15,16Marit Øilo17Gitana Rederiene18Rebecca Stolberg19Gülsün Gül19Jorge Tricio20
Amirul Faiz Luai15,16Marit Øilo17Gitana Rederiene18Rebecca Stolberg19Gülsün Gül19Jorge Tricio20 Reinhard Chun Wang Chau7
Reinhard Chun Wang Chau7 Mihaela Pantea21Murat Mutluay22
Mihaela Pantea21Murat Mutluay22 Peter Lingström6Ophir Klein23,24Sıla Nur Usta25
Peter Lingström6Ophir Klein23,24Sıla Nur Usta25 Liisa Suominen22,26
Liisa Suominen22,26 Szabolcs Felszeghy22*
Szabolcs Felszeghy22*
- 1Workman School of Dental Medicine, High Point University, High Point, NC, United States
- 2School of Dentistry, University of Liverpool, Liverpool, United Kingdom
- 3Faculty of Health Sciences, Department of Dentistry, Universidad Europea de Valencia, Valencia, Spain
- 4Clinic for Oral, Dental and Maxillofacial Diseases, Department of Conservative Dentistry, Heidelberg University, Heidelberg, Germany
- 5Melbourne Dental School, University of Melbourne, Melbourne, VIC, Australia
- 6Department of Cariology, Institute of Odontology, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden
- 7Prosthodontics, Faculty of Dentistry, The University of Hong Kong, Hong Kong, Hong Kong SAR, China
- 8Institute of Clinical Medicine, School of Medicine, University of Eastern Finland, Kuopio, Finland
- 9Department of Oral and Maxillofacial Diseases, University of Helsinki and Helsinki University Hospital, Helsinki, Finland
- 10Faculty of Dentistry & Graduate School of Medical and Dental Sciences, Division of Bio-Prosthodontics, Niigata University, Niigata, Japan
- 11Queen Mary University of London, London, United Kingdom
- 12School of Dentistry, The University of Queensland, Brisbane, QLD, Australia
- 13Faculty of Dentistry, University of Debrecen, Debrecen, Hungary
- 14School of Dental Medicine, University of Colorado Anschutz Medical Campus, Aurora, CO, United States
- 15Centre of Population Oral Health and Clinical Prevention Studies, Faculty of Dentistry, Universiti Teknologi MARA (UiTM) Sungai Buloh, Selangor, Malaysia
- 16Dental Public Health Unit, Department of Family Oral Health, Faculty of Dentistry, Universiti Kebangsaan Malaysia (UKM), Kuala Lumpur, Malaysia
- 17Department of Clinical Dentistry, University of Bergen, Bergen, Norway
- 18European Dental Hygienists Federation, Utrecht, Netherlands
- 19American Dental Education Association, Washington, DC, United States
- 20Faculty of Dentistry, Universidad de los Andes, Santiago, Chile
- 21Faculty of Dentistry, “Carol Davila” University of Medicine and Pharmacy, Bucharest, Romania
- 22Institute of Dentistry, School of Medicine, University of Eastern Finland, Kuopio, Finland
- 23Program in Craniofacial Biology, Department of Orofacial Sciences, University of California, San Fransisco, CA, United States
- 24Department of Pediatrics, Cedars-Sinai Guerin Children’s, Los Angeles, CA, United States
- 25Department of Endodontics, Gulhane Faculty of Dentistry, University of Health Sciences, Ankara, Türkiye
- 26Oral Health Teaching Unit, Kuopio University Hospital, Kuopio, Finland
Background: Haptics-enhanced virtual reality (VR-haptics), a supplementary tool for traditional oral health training, shows promise in enhancing knowledge acquisition, manual dexterity, performance, and student well-being.
Aim: The aim of this study was to understand dental educators' perceptions and needs regarding the acceptability and application of VR-haptics in dental education, as well as to gather suggestions for system improvements.
Methods: In this global cross-sectional study, the VR-Haptic Thinkers Consortium used a 28-item online questionnaire distributed to 1,023 participants by August 1, 2024. The survey included questions on general demographics, multiple choice and five-point Likert-style questions, and open-ended questions.
Results: A total of 378 responses were collected from 156 institutions. 57% of respondents had a dental doctorate degree and 59% had a PhD. VR-haptic trainers were used more often in preclinical training (94% of responses) than clinical training (46%). The three most common course types with VR-haptics incorporation were restorative, prosthodontic, and endodontic courses. Most respondents thought that the best approach to implementing VR-haptics is alongside phantom head training in the preclinical stage (58%). A third of the feedback on the challenges in VR-haptics utilization in dental training highlighted a need for further hardware and software development, while more than one-fourth cited economic issues in system acquisition and housing, and another one-fourth reported low acceptance of the technology among educators and students. The most mentioned enhancement requests for dental trainers were more diverse training scenarios (20%), improved software (19%) and hardware (19%) elements, and advancements in AI-based personalized training and monitoring (18%). Additionally, 10% of respondents suggested gamification features.
Conclusions: VR-haptic technology is constantly evolving and will likely become more and more accepted as an integral part of dental hand skill development to complement traditional preclinical training. Future research and development should emphasize transitioning from preclinical to clinical restorative, prosthodontic, endodontic, and implantology procedures as part of individualized education and patient care.
1 Introduction
Dental education has never hesitated to adapt itself to innovative technologies. Oral health educators have continuously embraced technological advances to meet evolving student needs, competencies, and professional standards to ensure high-quality education (1). Dental students' learning and hand skill development begins in the preclinical training phase, transitioning to professional roles in later phases. Preclinical training fosters a sense of belonging and skill development essential for motivation and preparation for the clinical years (2, 3).
Traditionally, practical dental education utilizes teaching strategies such as operating on manikins to enable new students to practice dental procedures and enhance the retention of knowledge. Immersive technologies, such as virtual reality (VR) and augmented reality (AR), have the potential to provide interactive, engaging, and immersive experiences that enhance education, prevention, and patient care (4, 5). Basic forms of virtual simulation have existed for many decades thanks to the military and aviation sectors' needs (6). However, a wider adaptation of VR and AR educational methodologies in engineering, medical, and other fields has only become reality in the past two decades thanks to advances in computational and display technologies (7–10). VR technologies with added force feedback methods, VR-haptics, hope to supplement some of the aspects where physical training methods have been perceived to be lacking (11). Haptics-enhanced dental trainers were introduced in the early 2010s, with global interest in VR-haptics having surged since 2020, driven by increased accessibility and acceptance post-COVID-19 (12). A previous consensus-based report elaborated on the benefits of VR-haptic methodology employed to create three-dimensional (3D) virtual replicas of operable structures combined with haptic sensory feedback (13). Studies have examined the effectiveness of VR-haptics and students' perceptions of it in both medical and anatomical education, finding that its use seems to enhance student motivation and engagement compared to traditional methodologies, while improving comprehension (14–16).
In 2024, the Virtual Reality-Haptic Thinkers Consortium (VRHTC) was established (17, 18). The consortium has experienced significant growth, doubling its membership and number of participating institutions within the first year, fueled by the renewed interest in accelerated educational pathways supported by VR-haptic technology. The global consortium includes educators and researchers from 41 dental schools that have integrated traditional dental training with VR-haptics-based simulations in their curricula.
Research indicates that this approach not only enhances motor skill acquisition in dental training but also potentially improves overall learning outcomes and mental well-being (5, 19–23). These advancements could allow students to enter their clinical training years feeling less stressed and better prepared (24–26). Incorporation of VR-haptic technology into dental curriculum enhances students' manual dexterity and knowledge acquisition, yet global acceptance among oral health professionals remains underexplored (25–31). Additionally, understanding teaching styles and traits can guide VR-haptic curriculum development, improving learning outcomes. Addressing these knowledge gaps through targeted surveys and curriculum development can drive industrial and educational advancements, shaping the future of dental training.
In our search for a comprehensive survey of educator's perspectives on VR-haptics in dental education, we were confronted with a lack of such work. Most existing studies have concentrated on the development and testing of VR-haptic applications and their implementation in dental curricula, primarily assessing single-centered participants' viewpoints and the local potential educational impact, thus potentially lacking in global applicability. There is a pressing need for more empirical research that focuses specifically on teachers, gaining an even deeper understanding of their perspectives, attitudes, abilities, and readiness to integrate innovative solutions like VR-haptics. Furthermore, understanding the applications of VR-haptics in various disciplines such as restorative dentistry, prosthodontics, endodontics, and implantology can provide a better foundation for future collaboration and broader applications of the technology. Therefore, we initiated a validated anonymous global cross-sectional online survey to explore and understand oral health educators' perceptions on VR-haptic training in preclinical and clinical dental courses. The aim of this study was to provide an overview of the current landscape of challenges and future innovation needs in VR-haptics, along with their distinctive characteristics.
2 Materials and methods
This global validated survey was classified as a non-human subject program evaluation, and it followed the guidelines of the European and Finnish National Board on Research Integrity. Ethical approval was obtained from the University of Eastern Finland Committee on Research Ethics (Approval No. 13/2023).
In early 2024, a 28-item online mixed-method questionnaire was created in English by expert educators who have experience in the use of haptic simulators in dental education. Spanish and Japanese translations were also acquired from native speaker colleagues. It included questions on general demographics, multiple choice and five-point Likert-style questions (47, 48), and open-ended questions regarding oral health educators’ perceptions on VR-haptic training.
The voluntary, anonymous online survey was broadly distributed to the members of VRHTC and through social media (X, Instagram, LinkedIn). Non-core VRHTC respondents were incentivized to join with a draw for three monetary prizes (250€ each) to aid them to participate in the 2025 VR-Haptic Thinkers Meetup in London.
The purpose of the study was to gather information on oral health educators' perceptions of VR-haptic training in various dental preclinical and clinical courses. As such, the survey included questions on such topics as the number of preclinical and clinical courses that implement VR-haptics and the challenges related to the integration and use of VR-haptics in the dental curricula. The survey questions and (where available) answer choices have been included as a Supplementary File S1.
Qualitative data obtained from the open-ended questions underwent thematic analysis. The responses were systematically coded based on the data and organized into overarching themes, which were further refined and categorized into sub-categories as necessary to provide a more detailed understanding of the data.
3 Results
3.1 Respondent demographics
A total of 378 responses were collected from 156 institutions across the world (Figure 1). The respondents had an even gender distribution, roughly half of them were aged 41 or over, and 84% had a PhD and/or DDS degree (Figure 2). Of the remaining 16%, 95% consisted of bachelor's and/or master's degree holders, as well as three other education type replies. More than half of the replies were received from universities ranked 500 or higher on the QS World University Rankings 2024.
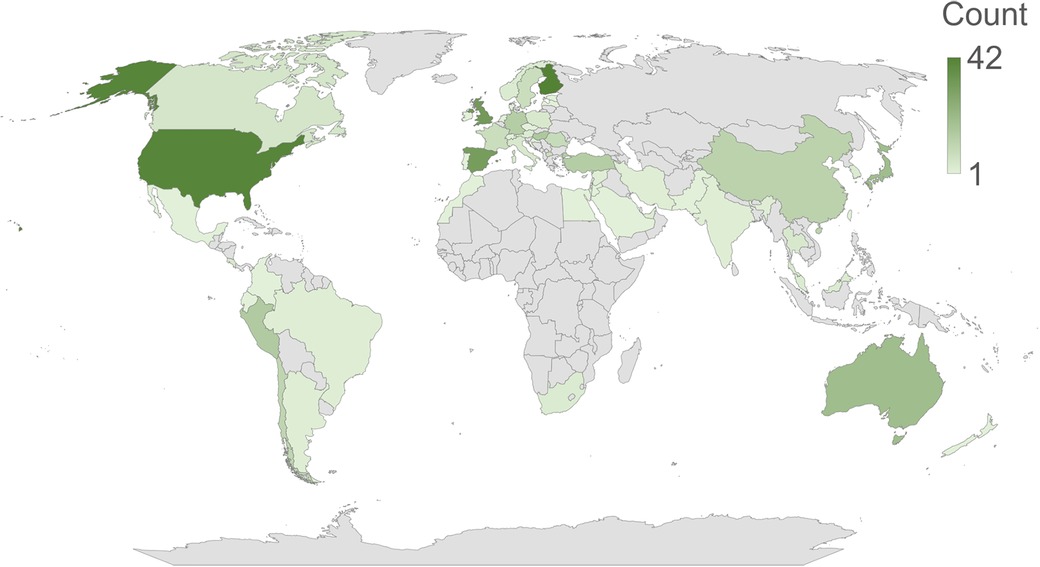
Figure 1. Distribution of the responses based on their country of origin.
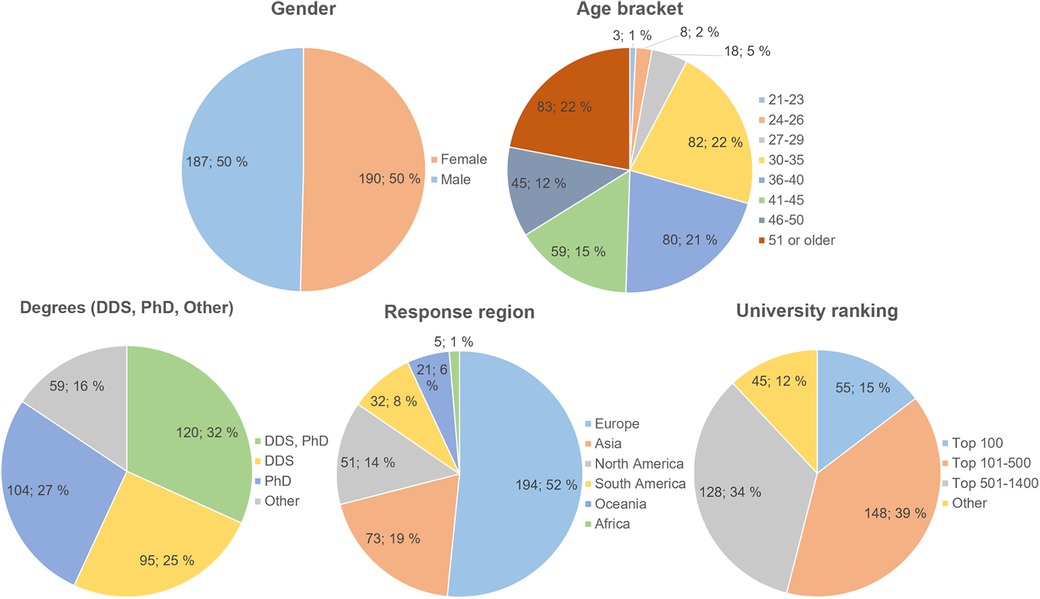
Figure 2. Survey respondent demographics. Gender data omits one “Prefer not to say” response. Scholarly degree data has been simplified to just DDS, PhD, and Other (95% bachelor's and master's) degrees, respondents may have reported other degrees as well. University rankings are based on the QS World University Rankings 2024 data. Data are shown as n; %.
3.2 Use of VR-haptics in dental education
Among the 273 respondents who indicated using VR-haptics in dental education, 37% (100) use it solely as a supportive or adjunct educational tool. Only 4% (11) use it for a specific purpose, with half of them (6) using it as a manual dexterity skills evaluation tool and half (5) as an exclusive training method. The remaining 59% (162) of respondents stated mixed utilization of these applications. 99% (161) of the mixed utilizers incorporated this technology as a supportive tool.
A total of 283 respondents stated that VR-haptic trainers are employed as a supplementary component in dental education. The majority (94%; 266) of respondents indicated their use in preclinical sessions. These tools are commonly utilized in predoctoral (46%; 131) and advanced dental education training including specialist and residency programs (36%; 102). However, their use in interprofessional education remains uncommon (3%; 9).
3.3 Integration of VR-haptics in preclinical and clinical training
Of the 373 responses to the question about the types of courses where VR-haptic dental trainers are used in preclinical education, 289 responses identified at least one course or discipline. For clinical education responses, the respective figures were 363 and 245. On average, respondents mentioned 3.2 (SD 1.6, range 1–8) different types of courses for both preclinical and clinical courses. The most cited courses using VR-haptics were restorative dentistry, prosthodontics, and endodontics (Table 1).
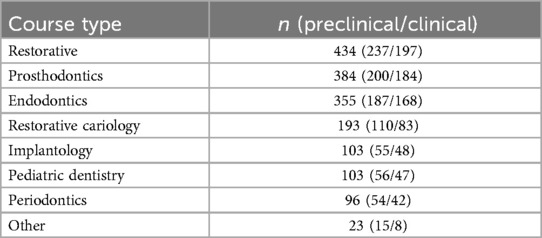
Table 1. The types of courses incorporating VR-haptics in preclinical and clinical dental education.
The timing of VR-haptics integration in preclinical dental education is a topic of interest. Of the 372 respondents, 58% (214) thought that VR-haptics should be implemented concurrently with phantom head training to maximize its benefits. Another 30% (111) preferred starting motor skill training with VR-haptics before moving to phantom head simulation. Less than a tenth (9%; 35) thought that it is best to introduce VR-haptics after phantom head training, while only 3% suggested reserving its use for the clinical training phase.
3.4 Challenges in implementing VR-haptics
When asked to identify the challenges impeding the implementation of VR-haptics in dental education, a total of 421 responses were received, covering both preclinical (222) and clinical (199) aspects. A total of 436 different challenges were mentioned by the respondents (237 for preclinical and 199 for clinical), which were categorized into 4 different themes: missing or lacking features, high overall cost, lack of acceptance and dismissive perceptions, and the amount of time required for implementation (Table 2). As the main challenge was related to hardware and software needing improvements or additions, it was further divided into 13 sub-categories. The most frequently cited missing features included a lack of clinical metrics and easily accessible performance analysis tools, insufficient realism or precision, and the absence of high and low-speed handpiece options.
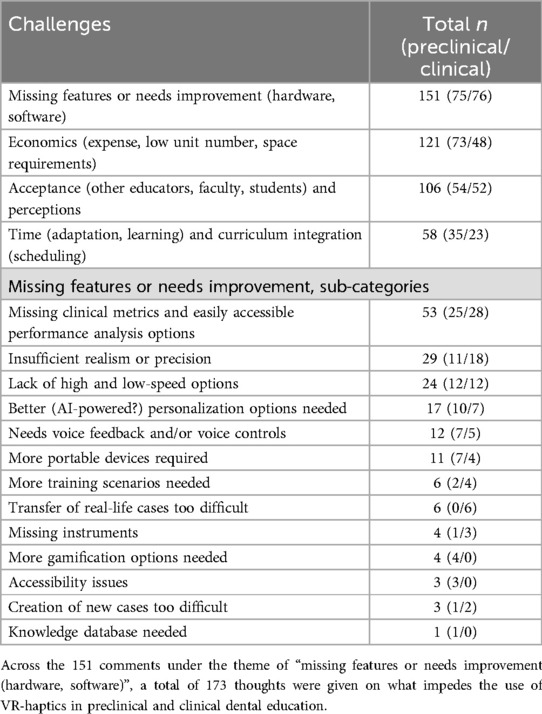
Table 2. Themes related to the perceived challenges in using VR-haptics in preclinical and clinical dental education.
3.5 Areas for improvement
When asked about functions the respondents would like to see added to VR-haptic dental trainers, 182 comments were received with a total of 217 different suggestions made. The suggestions were categorized into seven themes (Table 3). The most common suggestions were for adding in more types of training scenarios, improving the software and hardware aspects of the dental trainers, and incorporating AI-based personalization and assessment methods.
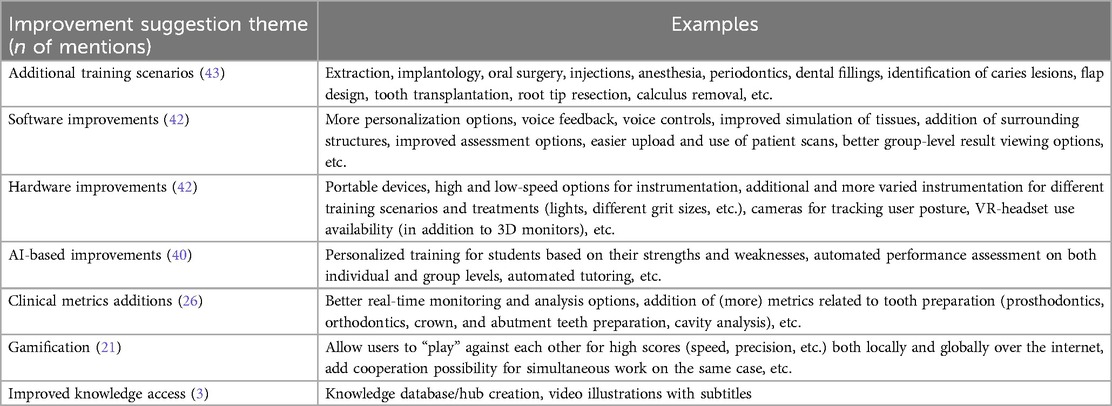
Table 3. Themes for improving the usability of VR-haptics in dental education. A total of 217 suggestions were made across 182 comments.
4 Discussion
The implementation of VR-haptic educational methods relies on suitable tools and educators' positive attitudes towards digital technologies (32). Our global survey covering 156 institutions revealed strong worldwide interest in integrating VR-haptics into dental education. This underscores the importance of identifying the potential, shortcomings, and future expectations in haptic simulators through public surveys.
4.1 Challenges in implementation
Integrating VR-haptic training in oral health education faces resistance, with the survey highlighting the key concerns and challenges associated with this modern approach. More than a third of the replies (35%) highlight the capabilities of the VR-haptic dental trainers as a hurdle in their implementation. This gap can affect the reliability of skill transfer from simulation to actual patient care. Enhancing the haptic precision and expanding procedural options could improve the acceptance and integration of VR-haptic systems into dental education.
More than a quarter of the responses (28%) highlighted economic challenges related to the acquisition, housing, and maintenance of these systems, leading to a shortage of available devices. Accordingly, many institutions struggle to invest in enough devices to meet student demand, which leads to limited hands-on time and prevents some programs from fully integrating these tools into their curricula. Addressing these financial constraints, possibly through funding support or cost-reduction innovations, could help increase access to these valuable educational resources.
Almost a quarter of the responses (24%) lamented low acceptance levels of VR-haptics among educators, faculty, and students. This hesitation can hinder the integration of VR-haptic systems in educational settings, as both faculty and students may be resistant to adopting new tools that disrupt established routines. Increasing training and demonstrating the educational benefits through research could help improve acceptance and foster a more supportive environment for VR-haptic dental training equipment.
Lastly, 13% of respondents noted that time constraints related to learning how to use the new equipment and adapting the curriculum for their addition can be prohibitive. Adapting the curriculum to include these simulators requires additional training sessions for faculty and students to become proficient with the equipment, which can be time-consuming. This adaptation process can take time away from other critical learning activities, making it difficult for programs to balance existing curriculum demands with the incorporation of new technology. Easily accessible databases, streamlined training, and phased integration strategies may help mitigate these time-related challenges, enabling smoother transition to VR-haptic learning.
These insights underscore the need for further development and refinement of VR-haptic systems to better meet educational standards and enhance the learning and assessments outcomes in dental training. They also align with findings from other, more localized studies where key obstacles included ineffective management, insufficient training, infrastructural limitations, and limited access to digital technologies (33).
4.2 Clinical phase utilization
Based on the responses, there is little resistance to adopting VR-haptic technology in preclinical settings, while its suitability for clinical phase utilization sees a 49% drop in our survey. Many factors diminish the perceived applicability of VR-haptic dental tools in a clinical context. For example, this reluctance towards its use may stem from the clinicians' resistance to moving away from traditional, patient-based educational methods. Another aspect to this may be that VR-haptic training is not seen as sufficiently relevant to the real-world aspect of practical dental education. The use of scans of patients’ oral structures could be a solution to this issue, but their use was seen as difficult by 56% of those who responded to the related question. Concerns on the effectiveness of such a format were likely a big part in this perceived difficulty, as 29% of the respondents mentioned reluctance of clinical instructors as the most challenging factor in implementing patient scans. On the other hand, lack of familiarity with modern technology was an even larger contributor to this hesitation, as 35% thought that technical proficiency is an issue. Improving this area could lead to better utilization of VR-haptics in the clinical phase of dental education. Lack of scanning equipment (19%) and concerns about patient rights and confidentiality (16%) also gained support as major factors in why patient scans are seen as difficult to use.
A lack of transferring VR-haptics applications from preclinical to clinical experiential learning is evident from the survey. The desire for discipline and subject matter-specific training scenarios for each program or institution also suggests a need for more broad and inclusive scientific interest groups and cross-discipline collaboration and training. The three most common disciplines mentioned, restorative dentistry, prosthodontics, and endodontics, would also form the most obvious multidisciplinary collaboration team that could naturally form and thus might improve future research and novel education protocols. Customized learning based on patient-specific and learner-specific VR-haptics for restorative dentistry, prosthodontics, and endodontics would be a powerful tool to train highly competent general dentists.
4.3 Gamification and VR-haptic dental training
During the analysis of the free-form comments, an intriguing suggestion emerged: 10% of respondents advocated for the integration of gamification elements and better interconnectedness in VR-haptics. This feedback highlights a growing interest among users in enhancing the training experience through gamified features. It has been shown that gamified dental education enhances interaction, communication, and collaboration while improving knowledge acquisition and comprehension (34–37). These immersive environments provide realistic experiences that boost student satisfaction and curiosity, while also enhancing experiential learning. Importantly, gamified sessions offer more personalized experiences, and they tend to provide more accessible adaptive feedback, making learning enjoyable and engaging for students. Free-time, gamified VR-haptic sessions with social media integration could also provide mechanisms for recognition, such as likes and shares. This validation has the potential for satisfying individuals' social needs for acknowledgment and appreciation, reinforcing their willingness to improve. Finally, gamified VR-haptic sessions might involve setting collective objectives that require teamwork. This action not only fosters collaboration but also cultivates a sense of unity as members work together towards common and individual goals (38–40). This could provide benefits in the students' overall mental wellbeing.
Overall, integrating gamification into dental education could enrich the learning process and create opportunities for unique teaching experiences, enabling students to learn in ways that were previously impossible. Due to its nature, gamified VR-haptics could be applied in various subjects across various educational levels, but especially during the formative preclinical phase.
4.4 Reliability of responses
Providing suggestions for improving teaching equipment is a nuanced topic, affected by several factors including individual attitudes towards technology, prior experiences with virtual learning, and the specific context of their dental research training. We learned during the analysis of the free-hand comments that of the 182 suggestion givers for device enhancements, 74% held a dental doctorate degree, with 61% also possessing a PhD. Such extensive research training may have made them more accustomed to technology, making them more receptive to adopting newer education methods, including VR-haptics and other digital platforms. Notably, more than half of the free-hand comments on potential improvements came from respondents engaged in educational research utilizing VR-haptics. Studies have shown that medical educators are increasingly integrating virtual learning due to its potential to enhance educational quality and accessibility (41–44). Those with a PhD are typically involved in research and may recognize the value of innovative digital educational tools that can enhance both teaching and learning. For instance, VR has been noted for its ability to bridge hands-on training with theoretical knowledge, which could appeal to those who prioritize evidence-based practices in education (21).
Considering this context, we believe that our data provides significant insights into critical areas for the advancement of VR-haptic technology within healthcare education. Among the suggestions for device enhancements, the top four categories identified were the need for more training scenarios, improvements at both software and hardware levels, and AI-based improvements, which each accounted for roughly a fifth of the suggestions. These reflect the factors identified as barriers to the implementation of VR-haptic technology in dental education (4, 27).
4.5 Future directions
Oral health care educators play a vital role in educating, training, and supporting students to become practice-ready professionals upon graduation (45). Dental education extends beyond merely training dentists; it aims to cultivate dedicated professionals committed to enhancing patient oral health and improving educational standards for future generations of dentists. This holistic approach is reflected in various educational frameworks that emphasize the importance of comprehensive training, including digital technology-reinforced traditional skills training, ethical considerations, and community health advocacy (46). American Dental Education Association and Association for Dental Education in Europe highlight that dental education programs are designed to produce graduates who not only possess technical skills but also demonstrate a commitment to lifelong learning and community service. This commitment is essential for addressing the evolving needs of patient populations and ensuring high standards in dental practice. The future of oral health education will be rooted in advanced digital health education systems. By integrating different digital technology-based training courses, we can significantly enhance the quality of education for oral health undergraduates, ultimately ensuring the oral health of our nations for years to come.
4.6 Strengths and weaknesses of the study
Conducting a global online survey on the utilization of VR-haptics in dental education, reaching 53 countries and 156 schools with 378 respondents, presents several strengths and weaknesses. Having such a wide outreach provided diverse perspectives and insights from experienced educators from many leading institutions. The convenience of an online survey helped lower the hurdle of participating and completing the survey, potentially helping to increase response rates. Given that a significant proportion (72%) of the survey responses were from practitioners who utilize VR-haptic training systems in their educational efforts, this study provides useful information for dental educators who wish to understand the current benefits and weaknesses of VR-haptic technologies. This study clearly shows that there is a large body of educators and researchers who are actively working towards the advancement of the effectiveness and benefits of these advanced training methods in dental education.
On the other hand, the response rate could still be higher to reach an even smaller margin of error. The response rates to this survey from outside Europe, Oceania, and North America were proportionally (population-wise) lower, likely stemming from a combination of lower VR-haptics availability and usage (economic issues) and our survey distribution channels not reaching them (social barriers). It should also be considered that participants who choose to respond to a voluntary survey may have different views from those who do not, leading to potential bias in the results. In addition, online surveys rarely manage to capture the depth of information that could be obtained through direct interviews or focus groups. These factors should be considered when interpreting the survey results to ensure a balanced understanding of the data collected.
4.7 Concluding remarks
In short, hardware and software aspects of VR-haptic dental trainers still need improvement to further push their adaptation and acceptance in dental schools. Lower costs, better dental discipline training scenario coverage, increased realism, and streamlined, student- and educator-friendly personalization and assessment options would make them more easily marketable to the portion of people who currently reject or are hesitant to embrace the technology. There is a real need for collaboration between restorative dentistry, prosthodontics, and endodontics educators and researchers. Establishment of easily accessible research-based databases on how to best implement VR-haptics in dental curricula and train the users are also needed to lighten the burden on the portion of educators who are actively trying to move forward its adaptation. Moving forward, it is also essential for future research to focus on how VR-haptics can specifically influence distinct aspects of the educational process or target variables related to student learning on the big scale. In addition, global surveys on students’ current perspectives on the use of VR-haptics in dental education could, in conjunction with educators' voices, lead towards the establishment of better guidelines for the use and incorporation of VR-haptics in dental education curricula. Cross-border studies such as this one will provide more nuanced insights and contribute to a more effective integration of technology in oral health education worldwide. By identifying the specific needs of teachers and the skills they may lack in implementing VR-haptics in their classrooms, the VR-Haptic Thinkers Consortium could potentially assist in developing targeted training programs. These programs would not only enhance the educators' skills but also increase their readiness to adopt such innovative approaches.
Data availability statement
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
Ethics statement
Written informed consent was not obtained from the individual(s) for the publication of any potentially identifiable images or data included in this article because Becasue of the study is an antonym, validated survey.
Author contributions
SB: Investigation, Supervision, Writing – review & editing. BQ: Investigation, Writing – review & editing. MS-P: Conceptualization, Investigation, Writing – review & editing. SA-H: Writing – review & editing. S-GS: Data curation, Investigation, Methodology, Writing – original draft, Writing – review & editing. SR: Investigation, Writing – original draft, Writing – review & editing. SB: Investigation, Writing – review & editing. MS: Investigation, Writing – review & editing. UÖ: Investigation, Methodology, Writing – review & editing. WL: Investigation, Writing – review & editing. ML: Data curation, Formal Analysis, Investigation, Methodology, Validation, Visualization, Writing – original draft, Writing – review & editing. DR: Investigation, Writing – original draft, Writing – review & editing. MN: Investigation, Methodology, Writing – review & editing. AR: Conceptualization, Investigation, Writing – review & editing. SZ: Writing – review & editing. KB: Investigation, Writing – review & editing. TG: Investigation, Writing – review & editing. AL: Writing – review & editing. MØ: Conceptualization, Investigation, Writing – review & editing. GR: Writing – review & editing. RS: Writing – review & editing. GG: Writing – review & editing. JT: Investigation, Writing – review & editing. RC: Data curation, Investigation, Writing – review & editing. MP: Investigation, Writing – review & editing. MM: Writing – review & editing. PL: Investigation, Writing – review & editing. OK: Writing – review & editing. SU: Data curation, Investigation, Writing – review & editing. LS: Investigation, Writing – review & editing. SF: Conceptualization, Data curation, Formal Analysis, Investigation, Methodology, Project administration, Supervision, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare that no financial support was received for the research and/or publication of this article.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
Generative AI statement
The author(s) declare that no Generative AI was used in the creation of this manuscript.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fdmed.2025.1576646/full#supplementary-material
References
1. Miyazono S, Shinozaki Y, Sato H, Isshi K, Yamashita J. Use of digital technology to improve objective and reliable assessment in dental student simulation laboratories. J Dent Educ. (2019) 83(10):1224–32. doi: 10.21815/JDE.019.114
2. Wenger E. Communities of Practice: Learning, Meaning, and Identity. Cambridge: Cambridge University Press (1998). Available at: https://www.cambridge.org/highereducation/books/communities-of-practice/724C22A03B12D11DFC345EEF0AD3F22A (Accessed November 10, 2024).
3. Roudsari MS, Namdari M, Mortazavi H, Malek-Mohammadi M, Tohidi S. Psychosocial impacts, perceived stress, and learning effects during the transition from preclinical to clinical dental education: validation and translation of a questionnaire. Dent Res J. (2022) 19:26. doi: 10.4103/1735-3327.340111
4. Luai AF, Malek AA, Hassan EH, Sabri BAM, Radzi NAM. Effectiveness of immersive technologies in oral health promotion and education: a systematic review. J Dent. (2024) 150:105324. doi: 10.1016/j.jdent.2024.105324
5. Bandiaky ON, Lopez S, Hamon L, Clouet R, Soueidan A, Le Guehennec L. Impact of haptic simulators in preclinical dental education: a systematic review. J Dent Educ. (2024) 88(3):366–79. doi: 10.1002/jdd.13426
6. Southgate E. Virtual Reality in Curriculum and Pedagogy: Evidence from Secondary Classrooms. Oxford, United Kingdom: Taylor & Francis Group (2020). Available at: http://ebookcentral.proquest.com/lib/uef-ebooks/detail.action?docID=6186748 (Accessed December 12, 2024).
7. Abdul-Hadi GA, Attridge A, Williams MA. Virtual reality in engineering education: the future of creative learning. Int J Emerg Technol Learn Online. (2011) 6(4):4–11. doi: 10.1109/EDUCON.2011.5773223
8. Birt J, Stromberga Z, Cowling M, Moro C. Mobile mixed reality for experiential learning and simulation in medical and health sciences education. Information. (2018) 9(2):31. doi: 10.3390/info9020031
9. Ntakakis G, Plomariti C, Frantzidis C, Antoniou PE, Bamidis PD, Tsoulfas G. Exploring the use of virtual reality in surgical education. World J Transplant. (2023) 13(2):36–43. doi: 10.5500/wjt.v13.i2.36
10. Zhao X, Ren Y, Cheah KSL. Leading virtual reality (VR) and augmented reality (AR) in education: bibliometric and content analysis from the web of science (2018–2022). Sage Open. (2023) 13(3):21582440231190821. doi: 10.1177/21582440231190821
11. Yang Y, Cheng G, Xing X, Li Z, Zhang W. Application of a multimedia-supported manikin system for preclinical dental training. BMC Med Educ. (2022) 22(1):693. doi: 10.1186/s12909-022-03757-1
12. de Boer IR, Bakker DR, Wesselink PR, Vervoorn JM. [The simodont in dental education]. Ned Tijdschr Tandheelkd. (2012) 119(6):294–300. doi: 10.5177/ntvt.2012.06.12105
13. Felszeghy S, Mutluay M, Liukkonen M, Flacco N, Bakr MM, Rampf S, et al. Benefits and challenges of the integration of haptics-enhanced virtual reality training within dental curricula. J Dent Educ. (2024). doi: 10.1002/jdd.13800
14. Daud A, Matoug-Elwerfelli M, Khalid A, Ali K. The impact of virtual reality haptic simulators in pre-clinical restorative dentistry: a qualitative enquiry into dental students’ perceptions. BMC Oral Health. (2024) 24:988. doi: 10.1186/s12903-024-04704-w
15. Izumi M, Hagiya H, Otsuka Y, Soejima Y, Fukushima S, Shibata M, et al. Effectiveness of sensing gloves–applied virtual reality education system on hand hygiene practice: a randomized controlled trial. Am J Infect Control. (2024) 53(1):65–9. doi: 10.1016/j.ajic.2024.08.003
16. Aboregela AM, Khired Z, Osman SET, Farag AI, Hassan NH, Abdelmohsen SR, et al. Virtual dissection applications in learning human anatomy: international medical students’ perspectives. BMC Med Educ. (2024) 24:1259. doi: 10.1186/s12909-024-06218-z
17. Felszeghy S, Liukkonen M, Flacco N, Bakr MM, Rampf S, Schick SG, et al. Establishing the VR-haptic thinkers group: insights and progress in dental training technologies. Saudi Dent J. (2024) 36(12):1655–9. doi: 10.1016/j.sdentj.2024.11.008
18. Felszeghy S. VR-Haptic Thinkers (2023). Available at: https://vr-hapticthinkers.com/ (Accessed November 12, 2024).
19. Al-Saud LM. The utility of haptic simulation in early restorative dental training: a scoping review. J Dent Educ. (2021) 85(5):704–21. doi: 10.1002/jdd.12518
20. Al-Saud LM, Mushtaq F, Allsop MJ, Culmer PC, Mirghani I, Yates E, et al. Feedback and motor skill acquisition using a haptic dental simulator. Eur J Dent Educ. (2017) 21(4):240–7. doi: 10.1111/eje.12214
21. Felszeghy S, Huhtela O, Manninen K, Mäenpää M, Banafa A, Liukkonen M, et al. VR-haptic and phantom head dental training: does the order matter? A comparative study from a preclinical fixed prostho-dontics course. Int J Comput Dent. (2023) 27(4):389. doi: 10.3290/j.ijcd.b4451364
22. Hamilton-Flack M, Orsini C. Simulation suite vs virtual reality: which simulated learning environment better prepares final year medical students for emergencies? Future Healthc J. (2023) 10(Suppl 3):38. doi: 10.7861/fhj.10-3-s38
23. Tricio JA, Kleiman SE, Eiriksson VI, Vicuña DP, Cacciuttolo FR, Jorquera GA, et al. Students’ and tutors’ perceptions of a deliberate simulated practice using patient-specific virtual and three-dimensional printed teeth models: a pilot study. J Dent Educ. (2022) 86(8):1006–14. doi: 10.1002/jdd.12909
24. Li Y, Ye H, Wu S, Zhao X, Liu Y, Lv L, et al. Mixed reality and haptic–based dental simulator for tooth preparation: research, development, and preliminary evaluation. JMIR Serious Games. (2022) 10(1):e30653. doi: 10.2196/30653
25. Azhari AA, Ashy Y, Abulhamail L, Sharshar H, Ahmed WM. Integrating virtual–reality into restorative dentistry training: a study on the acceptability and effectiveness of tooth preparation simulations. J Dent Educ. (2024) 89(3):1–16. doi: 10.1002/jdd.13723
26. Hamama H, Harrison KY, Murbay S. Benefits of using virtual reality in cariology teaching. BMC Med Educ. (2024) 24(1):1051. doi: 10.1186/s12909-024-05980-4
27. Algarni YA, Saini RS, Vaddamanu SK, Quadri SA, Gurumurthy V, Vyas R, et al. The impact of virtual reality simulation on dental education: a systematic review of learning outcomes and student engagement. J Dent Educ. (2024) 88(11):1–14. doi: 10.1002/jdd.13619
28. Alroomy R, Almimoni M, Alotaibi A, Almutairi A, Alyahya E, Unozawa M, et al. Students’ perception of remote extended reality simulation systems using patient-specific three-dimensional-printed models in endodontic education: a pilot study. Eur Endod J. (2024) 9(3):273–8.39213454
29. Suebnukarn S, Hataidechadusadee R, Suwannasri N, Suprasert N, Rhienmora P, Haddawy P. Access cavity preparation training using haptic virtual reality and microcomputed tomography tooth models. Int Endod J. (2011) 44(11):983–9. doi: 10.1111/j.1365-2591.2011.01899.x
30. Choi Y, Lee M, Kim J, Park W. Clinical observation using virtual reality for dental education on surgical tooth extraction: a comparative study. BMC Med Educ. (2024) 24:643. doi: 10.1186/s12909-024-05605-w
31. Usta SN, Doğuş E, Uğur Aydın Z. Evaluation of the effect of Mozart’s music on stress, anxiety, and dexterity levels of dental students in preclinical endodontic training using a haptic virtual reality simulator. Turk Endod J TEJ. (2024) 9(2):96–102. doi: 10.14744/TEJ.2024.97658
32. Abu Arqub S, Al-Shehri NA, Meyer S, Asefi S, Al-Moghrabi D. The effectiveness of technology-enhanced learning in prosthodontic education: a systematic review. Eur J Dent Educ. (2024) 28(4):995–1015. doi: 10.1111/eje.13035
33. Luai AF, Radzi NAM, Sabri BAM. Perceived barriers in digitalizing oral health promotion: phenomenological study among Malaysian dental public health specialists. J Int Oral Health. (2024) 16(2):128. doi: 10.4103/jioh.jioh_281_23
34. Nguyen LM, Le C, Lee VD. Game-based learning in dental education. J Dent Educ. (2023) 87(5):686–93. doi: 10.1002/jdd.13179
35. Sharmin N, Chow AK. Gamification of formative assessments in an undergraduate dentistry program. J Dent Educ. (2023) 88(Suppl 3):1–3. doi: 10.1002/jdd.13441
36. Lin CS, Yang CC. Evaluation of a digital game for teaching behavioral aspects of clinical communication in dentistry. BMC Med Educ. (2023) 23:78. doi: 10.1186/s12909-023-04040-7
37. Felszeghy S, Pasonen-Seppänen S, Koskela A, Nieminen P, Härkönen K, Paldanius KMA, et al. Using online game-based platforms to improve student performance and engagement in histology teaching. BMC Med Educ. (2019) 19:273. doi: 10.1186/s12909-019-1701-0
38. Gentry SV, Gauthier A, L’Estrade Ehrstrom B, Wortley D, Lilienthal A, Tudor Car L, et al. Serious gaming and gamification education in health professions: systematic review. J Med Internet Res. (2019) 21(3):e12994. doi: 10.2196/12994
39. Nakamoto K, Jones DB, Adra SW. Gamification of robotic simulation to train general surgery residents. Surg Endosc. (2023) 37:3136–44. doi: 10.1007/s00464-022-09520-3
40. Sardi L, Idri A, Fernández-Alemán JL. A systematic review of gamification in e-health. J Biomed Inform. (2017) 71:31–48. doi: 10.1016/j.jbi.2017.05.011
41. Felszeghy S, Pasonen-Seppänen S, Koskela A, Mahonen A. Student-focused virtual histology education: do new scenarios and digital technology matter? MedEdPublish (2016). (2017) 6:154. doi: 10.15694/mep.2017.000154
42. Kaplan T, Tarolli C, Doughty CT. Integrating virtual teaching in a new era of medical education: lessons from a neurology course. Adv Med Educ Pract. (2023) 14:1147–56. doi: 10.2147/AMEP.S413816
43. Jiang H, Vimalesvaran S, Wang JK, Lim KB, Mogali SR, Car LT. Virtual reality in medical students’ education: scoping review. JMIR Med Educ. (2022) 8(1):e34860. doi: 10.2196/34860
44. Pang M, Dong Y, Zhao X, Wan J, Jiang L, Song J, et al. Virtual and interprofessional objective structured clinical examination in dentistry and dental technology: development and user evaluations. JMIR Form Res. (2024) 8:e44653. doi: 10.2196/44653
45. Escontrías OA, Istrate EC, Flores S, Stewart DCL. Operational and financial impact of the COVID-19 pandemic on U.S. Dental school clinics. J Dent Educ. (2021) 85(12):1863–9. doi: 10.1002/jdd.12814
46. Patel US, Shapira L, Gallagher JE, Davis J, Garcia LT, Valachovic RW. ADEA-ADEE shaping the future of dental education III: engaging with global networking to enable global oral health. J Dent Educ. (2020) 84(1):117–22. doi: 10.1002/jdd.12026
47. Jebb AT, Ng V, Tay L. A review of key Likert scale development advances: 1995–2019. Front Psychol. (2021) 12:637547. doi: 10.3389/fpsyg.2021.637547
Keywords: dental education, challenges, haptic technology, implementation barriers, virtual reality
Citation: Bencharit S, Quinn B, Sittoni-Pino MF, Arias-Herrera S, Schick S-G, Rampf S, Byrne S, Shazib MA, Örtengren U, Lam WYH, Liukkonen M, Rice D, Nagasawa M, Ranauta A, Zafar S, Bágyi K, Greany TJ, Luai AF, Øilo M, Rederiene G, Stolberg R, Gül G, Tricio J, Chau RCW, Pantea M, Mutluay M, Lingström P, Klein O, Usta SN, Suominen L and Felszeghy S (2025) Insights from the global education survey on the use of VR-haptics in dental education. Front. Dent. Med. 6:1576646. doi: 10.3389/fdmed.2025.1576646
Received: 14 February 2025; Accepted: 28 March 2025;
Published: 24 April 2025.
Edited by:
Mario Lorenz, Chemnitz University of Technology, GermanyReviewed by:
Christian Diegritz, Ludwig-Maximilians-Universität München, GermanyLukasz Zadrozny, Medical University of Warsaw, Poland
MengWei Pang, Chongqing Medical University, China
Copyright: © 2025 Bencharit, Quinn, Sittoni-Pino, Arias-Herrera, Schick, Rampf, Byrne, Shazib, Örtengren, Lam, Liukkonen, Rice, Nagasawa, Ranauta, Zafar, Bágyi, Greany, Luai, Øilo, Rederiene, Stolberg, Gül, Tricio, Chau, Pantea, Mutluay, Lingström, Klein, Usta, Suominen and Felszeghy. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Szabolcs Felszeghy, c3phYm9sY3MuZmVsc3plZ2h5QHVlZi5maQ==