
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
REVIEW article
Front. Dent. Med. , 28 February 2025
Sec. Regenerative Dentistry
Volume 6 - 2025 | https://doi.org/10.3389/fdmed.2025.1542913
 Ecaterina Burlui1,2Viorica Rarinca1,2,3*
Ecaterina Burlui1,2Viorica Rarinca1,2,3* Alin Ciobica2,4,5Vasile Burlui2,6Romeo Dobrin7Carmen Stadoleanu6
Alin Ciobica2,4,5Vasile Burlui2,6Romeo Dobrin7Carmen Stadoleanu6
Schizophrenia is a complex mental condition characterized by the deterioration of thought processes and inappropriate emotional responses. Compared to the general population, individuals diagnosed with schizophrenia have an increased risk of developing various dental diseases, including dental caries, periodontal disease, oral mucosal diseases, and conditions associated with oral resonance. In this context, we propose to establish links between schizophrenia and dental illness, emphasizing the importance of oxidative stress (OS) markers in schizophrenia, and also the role of dental treatments, particularly dental implants. This highlights the urgent need for an intervention program to improve oral health in patients with schizophrenia, including aspects such as prevention and prosthetic treatment. Dental implants can be a favorable option, offering good aesthetic and functional results for treated patients with schizophrenia. Additionally, a carefully developed surgical plan is essential, requiring collaboration between psychiatry, oral and maxillofacial surgery, anesthesiology, and prosthodontics departments.
Schizophrenia is a chronic psychiatric illness with complex symptoms (1). According to Schultz et al., schizophrenia affects about 1% of the population worldwide (2). Patients with Schizophrenia are characterized by positive and negative symptoms. Although the notion as well as the limits of the diagnosis itself have expanded but some of these symptoms in literature remain the same including hallucination, delusion, social withdrawal and cognitive deficits (3).
Oral health is essential for daily activities, such as eating, smiling, and speaking (4). On the other hand, poor oral health can negatively impact overall health, self esteem, and quality of life (5). Individuals with psychotic disorders tend to have worse oral health outcomes compared to the general population, including higher rates of tooth decay and tooth loss (6, 7).
Oral care in patients with schizophrenia is a challenge for these patients. In most cases, patients do not take care of their health, do not brush their teeth, which is why they are prone to the appearance of tartar and gingival plaque. This unconsciousness about oral health later leads to the appearance of various dental diseases, such as caries, gingivitis and periodontitis (3).
The poor state of oral health in individuals with schizophrenia has been attributed to a range of factors, including poverty, lack of motivation, limited resources, imbalanced mental status, the side effects of antipsychotic medications, and the impact of coexisting systemic diseases such as diabetes, hypertension, and osteoporosis, which collectively diminish patients' ability to engage in effective selfcare (8). First-generation antipsychotics, including haloperidol, chlorpromazine, thioridazine, and trifluoperazine, are known to induce hyposalivation by inhibiting parasympathetic stimulation of the salivary glands. This reduction in saliva increases the risk of dental caries, especially root caries (9). Reduced salivation can lead to several side effects, including difficulty speaking, chewing disorders, inflammation of the mucous membranes (mucositis), oral Candida infections, and mucosal atrophy. Additionally, decreased saliva flow can lead to increased plaque buildup (10).
Fear and anxiety in patients with schizophrenia can manifest as premature tooth wear. Many individuals with schizophrenia exhibit parafunctional habits such as nail biting and lip biting. Additionally, bizarre behaviors leading to self mutilation, including autoextractions, glossectomy, and excoriation of gingival tissues with sharp fingernails, have been reported (11, 12). Studies indicate that oral health tends to deteriorate with increasing age and length of hospitalization, and it is generally worse among inpatients compared to outpatients (13, 14). Studies show that 88% of people diagnosed with schizophrenia have proven to be heavy tobacco abusers (15). The reasons for such a high frequency of heavy smoking prevalent in patients with schizophrenia are thought to be partly related to its enhanced stimulant effect. Smoking induces the release of dopamine in the brain, stimulating its activity and inhibiting its degradation (16). According to several authors, patients with schizophrenia do not always receive the best oral health treatment (17–20).
The liaison between psychiatrists and dentists is crucial, and developing consultation liaison models is essential for effectively treating patients with mental health issues. These models ensure integrated care, addressing both mental and oral health needs comprehensively.
Extreme empathy, patience, and tact are essential qualities for psychiatrists and dentists working together, especially when addressing the complex needs of patients with mental health conditions. Additionally, they must possess a thorough understanding of potential adverse reactions to commonly prescribed medications and be aware of any legislative issues that may impact treatment. This knowledge helps in managing patient care effectively and navigating potential challenges in a collaborative manner.
Hence, the proposed framework of Psychiatric Dental Consultation Liaison (PDCL) services is gaining success and popularity, offering a confident and structured approach to integrating mental health and oral care. This framework enhances collaboration between psychiatrists and dentists, leading to more comprehensive and effective patient care (21, 22).
The services, in addition to classic invasive and noninvasive procedures, include relaxation techniques and psychotherapy. The consultations carried out in the morning and of short duration, the quiet atmosphere and the direct communication and the calm explanations give the patients courage and the desire to return.
Oxidative stress is defined as a pathophysiological mechanism which appears at the moment of disturbance in the balance between the production of reactive oxygen species (ROS) and antioxidant defenses (23). The theory of oxidative stress, sometimes referred to as the “oxygen paradox”, that while oxygen is essential for aerobic life, excessive amounts of free radical metabolic byproducts are toxic (24, 25).
There are theories that oxidative stress mechanisms have been implicated in the pathogenesis of psychiatric disorders. The brain is considered particularly vulnerable to oxidative damage for several reasons (26). These include comparatively high oxygen utilization and hence generation of free radical byproducts, modest antioxidant defenses, lipid rich constitution that provides ready substrates for oxidation and the reducing potential of certain neurotransmitters. Additionally, the brain is also susceptible to secondary and self-perpetuating damage from oxidative cellular injury or necrosis, via? the neurotoxic effects of released excitatory amines (mainly glutamate) and iron, and the activated inflammatory response (27). Although the exact mechanism of schizophrenia is not known, it is assumed that at the basis of these pathologies is primarily the genetic factor, but also the nongenetic factors such as drug and alcohol abuse, stressful lifestyle, medications, prenatal and neonatal infections, complications during birth, etc. By inducing metabolic stress cellular, these factors appear to increase the possibility of oxidative stress and damage (28, 29).
There is ample evidence that a variety of environmental factors contribute to the dysregulation of gene expression caused by abnormal regulation of redox sensitive transcriptional factors, noncoding ribonucleic acids (RNAs), and epigenetic mechanisms (30).
Figure 1 illustrates the relationship between oxidative stress and various factors such as reactive oxygen species, DNA damage, inflammatory responses, schizophrenia, dental care, comorbidities, environmental factors, and habits. It's a representation of how oxidative stress can be central to general and oral health, especially in patients with schizophrenia.
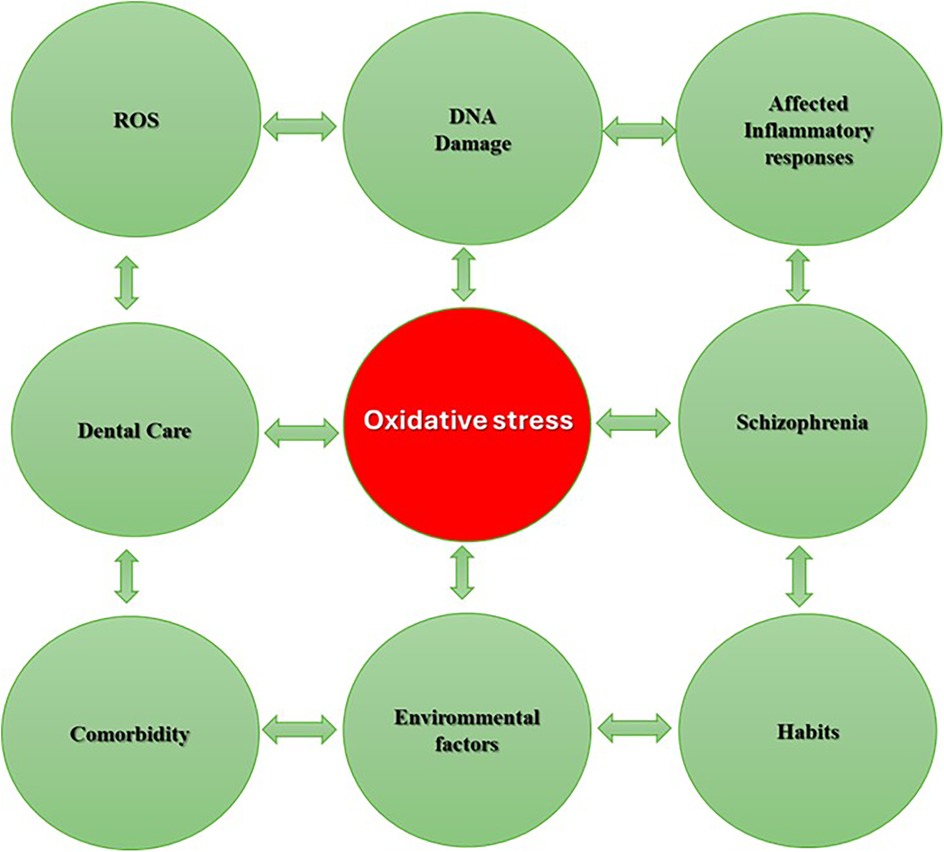
Figure 1. The connection between oxidative stress, dental care and schizophrenia.
The current review was conducted following the Preferred Reporting Items for Systematic Review and MetaAnalysis (PRISMA) guidelines, employing several electronic databases (Science Direct, PubMed, and Google Scholar) to conduct a comprehensive and systematic search using the following search terms: ((schizophrenia[Title/Abstract]) AND (dental care[Title/Abstract])) AND ((schizophrenia[Title/Abstract]) AND (oxidative stress[Title/Abstract])) AND ((oxidative stress[Title/Abstract]) AND (dental care[Title/Abstract])) AND ((schizophrenia[Title/Abstract]) AND (dental implant[Title/Abstract])). The inclusion criteria focused on studies published up until inception of November 2024 in English, proposes to establish the connection between schizophrenia and dental disease, emphasizing the importance of oxidative stress markers in schizophrenia, and the implementation of dental treatments in patients diagnosed with schizophrenia, with a particular focus on dental implant.
We applied the following exclusion criteria: (1) letters, summaries, expert opinions, and comments; (2) conference abstracts, books, book chapters, and unpublished results; (3) non-English papers.
Out of the initial 1,327 reports collected through electronic search, 826 were omitted due to duplication, 156 were excluded based on article type, and an additional 209 were excluded as they comprised conference abstracts, books, book chapters, and unpublished results. Furthermore, 8 were excluded because they were not in English.
Finally, 81 articles were included in this review demonstrated in a diagram of the literature search and selection process (Figure 2). Due to the heterogeneity of the studies, a narrative synthesis was deemed the most suitable approach. The results are summarized in one chapter about dental implants and dental treatment in schizophrenic patients and in Table 1 that compresses the study's parameters and the results that have been reported in these cases. Then, the discussion chapter continues with 5 subsections, 4 of them present information found in literature about dental implants, dental implants and oxidative stress, oxidative stress and dental health, one about schizophrenia and oxidative stress and a final one with limitations.
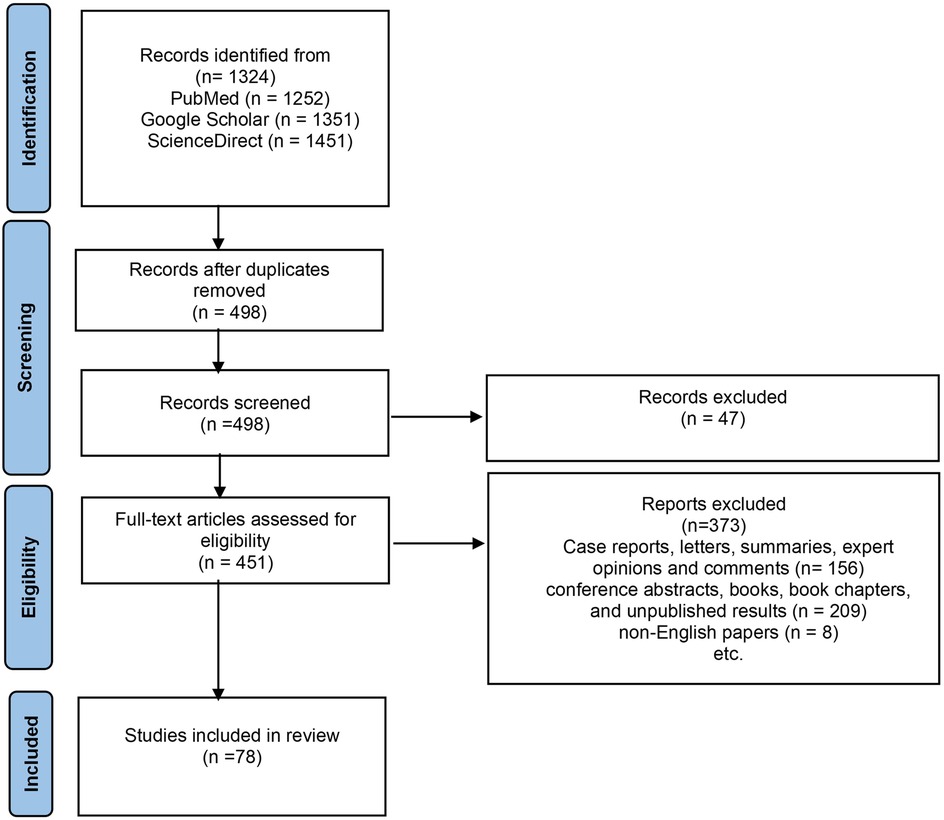
Figure 2. A flow diagram of the search strategy conducted (PRISMA flow of study selection process).
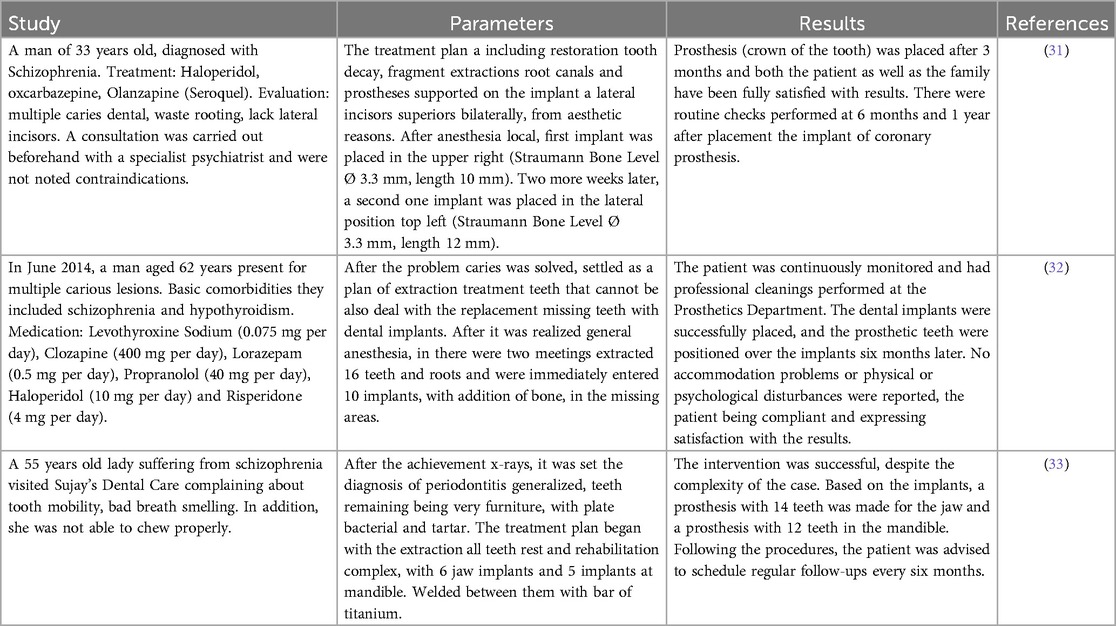
Table 1. Analysis of studies on dental implants in schizophrenic patients.
Table 1 contains information about the cases we found in the literature about dental implants in patients with schizophrenia. In all cases patients are presented with multiple caries, required extractions, or generalized tooth damage. Therefore, dental implant treatment was chosen to ensure the necessary stability, functionality, and aesthetics.
In the fist case, after completing the treatment plan, including the placement of two implants for the missing lateral incisors, the results were highly positive, with good osteointegration. At the 6-month follow-up, the implants were fully osseointegrated, as confirmed by radiographic evaluation. The patient reported significant improvement in chewing efficiency and self-confidence due to the restored aesthetics. Castellanos-Cosano et al., report no signs of peri-implant inflammation or complications were observed during the monitoring period (31). The same good results were obtained in the second case, even though it was a more complex rehabilitation and as additional comorbidities the 62-year-old patient also had hypothyroidism, requiring extra caution in managing systemic risks.
Mild gingival inflammation was detected during early follow-ups but was resolved through professional scaling and enhanced oral hygiene practices. The patient reported better dietary habits and an improved sense of well-being, with no adverse reactions to the procedures or medications used (32).
In the third case, where it was necessary to extract all the remaining, but periodontal teeth, the treatment was a complete oral rehabilitation with 6 maxillary and 5 mandibular implants resulted in stable and functional prostheses (33). The patient expressed satisfaction with the restored ability to chew and improved aesthetics. However, she required regular motivation and guidance to maintain proper oral hygiene. Minor adjustments to the prostheses were necessary to address food impaction issues, but overall, the results were successful.
These studies highlight the significant advancements in dental treatments for individuals with schizophrenia. They demonstrate that promising outcomes can be achieved, particularly through the successful healing of dental implants. Such treatments not only improve oral health but also contribute positively to the mental and psychological well-being of patients, helping to address the stigma often associated with their condition.
The individuals with schizophrenia are generally prone to orofacial adverse effects such as xerostomia, sialorrhea and oral dyskinesia caused by psychotropic drugs (17). Healing after dental implant placement heavily depends on maintaining excellent oral hygiene. For individuals with schizophrenia, adhering to a rigorous oral hygiene routine may be particularly challenging due to factors such as cognitive impairments, side effects of medication, or lack of motivation (31).
Patients with schizophrenia may already have a higher degree of oral inflammation, either due to poor hygiene or due to systemic factors associated with the disease (34).
General inflammation and oxidative stress already present in the body can compress bone regeneration and tissue healing (35).
As important as medication is during treatment and surgery, so is antibacterial medication for afterwards. Also, the balance of the oral microbiota and the immune system play an important role in oral health. Any associated comorbidity, autoimmune diseases, a compromised immune system or an organ transplant (36). All of these aspects discussed have an interdisciplinary relationship and can influence the state of oral health. That being said, dentists are generally unwilling to invest in complex conservative or rehabilitative treatments because of the difficulty of treating patients with psychiatric illnesses (37).
Dental implants are increasingly chosen as a preferred method for replacing missing natural teeth due to their notable success rates and numerous benefits.
Dental implant materials are typically composed of titanium (Ti) or Ti alloys. Upon exposure to oxygen, a titanium oxide (TiO2) layer forms on the surface of the implant. The integrity of this oxide layer is crucial to ensure proper osseointegration and prevent corrosion, thereby maintaining the stability of the bone implant interface (38).
After a dental implant is placed, an inflammatory healing response occurs, characterized by processes such as angiogenesis. Angiogenesis, the formation of new blood vessels, plays a crucial role in delivering cells and oxygen necessary for the successful integration of the implant with the surrounding bone (osseointegration) (35).
Tsarik et al., studied the effects of cathodic corrosion of titanium (Ti) on endothelial cells and found that it led to cytotoxicity and inhibition of cell proliferation. They identified ROS and hydrogen peroxide (H2O2) as byproducts of the corrosion process (39).
Typically, a baseline level of ROS exists before a dental implant is placed (40). The process of dental implantation itself inevitably generates additional ROS. While ROS play essential roles in cell signaling and normal metabolism, excessive oxidative stress can potentially cause damage to DNA, RNA, and proteins (41).
Thus, maintaining a balance in ROS levels during and after implant placement is crucial for minimizing oxidative damage and promoting successful integration of the implant with the surrounding tissues.
The sources of ROS in addition to dental materials are also relatively wide, mainly including food, cigarettes, alcohol, and drugs (42). As people increasingly prioritize dental health, various dental treatment procedures are gaining popularity. Consequently, the sources of ROS are more diverse and widespread than anticipated. Schizophrenia has the potential to worsen oral health by impairing the subject's ability to maintain oral hygiene. There is limited literature on how oral diseases manifest in individuals with schizophrenia (19).
Currently, the use of the implant in patients generally has a high, long term success rate of 90%–95% (43). However, implant treatment in disabled patients has a limited application due to the lack of compliance and oral care (44).
Oxidative stress underpins conditions such as diabetes, rheumatoid arthritis, nonalcoholic fatty liver disease, chronic inflammation, stroke, aging, various neurodegenerative diseases, and cancer (45–48). During recent years, there has been increasing research interest in the relationship between oxidative stress and oral health.
Free radicals, highly reactive molecules with unpaired electrons, can cause oxidative stress by damaging cellular components like deoxyribonucleic (DNA), proteins, and lipids. In the mouth, oxidative stress can contribute to conditions such as periodontal disease, oral cancers, lichen planus and dental caries (49).
Periodontitis is a serious gum infection that damages the soft tissue and destroys the bone that supports teeth. The fundamental causative factor is bacteria and the engagement in the destroying of the periodontium. Polymorphonuclear neutrophils (PMNs), often simply called neutrophils, are indeed crucial components of the innate immune response against bacterial pathogens. PMNs migrate to sites of inflammation in response to proinflammatory cytokines secreted as part of the immune response. Upon arrival, they utilize Nicotinamide adenine dinucleotide phosphate (NADPH), mononitrogen oxides (NOx), reactive oxygen species (ROS) and proteolytic enzymes, which are essential for combating bacterial pathogens and contributing to the inflammatory process (50).
Baltacioglu et al., investigated the serum and the saliva from patients with chronic (CP) and generalized aggressive periodontitis (GAgP). Salivary malondialdehyde (MDA) levels, as well as serum and salivary total oxidant status (TOS) and oxidative stress index (OSI) values, were found to be significantly higher in the periodontitis groups compared to the control group (51). Another study that includes patients with chronic periodontitis, detected that a overproduction of ROS by activated polymorphonuclear leukocytes in chronic inflammation may lead to premature oxidative damage of the mitochondrial DNA (mtDNA) (52). Numerous studies have explored the association between oxidative stress and oral cancer, which involves mechanistic pathways contributing to cancer initiation and progression. Overexpression of enzymes such as NOx, Cyclooxygenase (COX), Lipoxygenase (LOX), and nitric oxide synthase (NOS) serves as significant sources of ROS/reactive nitrogen species (RNS) in oral cancer (53–58). Oral cancer refers to cancers that develop in the mouth, including the lips, tongue, cheeks, gums, floor of the mouth, and roof of the mouth. ROS/RNS modulate the activity of a variety of transcription factors, including Apurinic/apyrimidinic endonuclease 1/redox effector factor 1 (APE1/Ref1), Hypoxia-Inducible Factor (HIF1α), Activator protein 1 (AP1), nuclear factor erythroid 2–related factor 2 (Nrf2), Nuclear factor-kappa B (NFκB), p53 gene, forkhead box transcription factors (FOXO), and βcatenin (57). These factors are pivotal in regulating genes associated with cell proliferation, survival, and apoptosis, thereby exerting significant influence on cancer progression (57). Oral lichen planus (OLP) is a chronic inflammatory disease that affects the mucous membranes inside the mouth. It's characterized by white, lacy patches, redness, and sometimes painful sores. OLP is known for its relatively high prevalence, ranging from 0.5% to 2% of the population, depending on the region and demographic studied. Its chronic and recurrent nature makes it a significant concern for those affected. Additionally, there is a small but established potential risk of malignant transformation, particularly to oral squamous cell carcinoma (58–60).
In patients with Oral Lichen Planus (OLP), the study found that total antioxidant defense (TAA) was significantly lower in serum samples compared to healthy subjects (61). This suggests a decreased ability to combat oxidative stress systemically in OLP. Another study points to the possible function of oxidative stress in the etiopathogenesis of OLP. The mean levels of salivary MDA were significantly higher in the OLP group (62).
These findings highlight the presence of oxidative stress and impaired antioxidant defense mechanisms in OLP, potentially influencing its pathogenesis and suggesting avenues for therapeutic intervention aimed at restoring antioxidant balance.
Saliva indeed plays a crucial role in protecting the oral cavity and controlling dental caries. Its buffering effect helps maintain a stable pH level, which is essential for preventing acidic conditions that can lead to tooth decay. Additionally, saliva possesses antioxidant capacity, which helps neutralize free radicals. This equilibrium between antioxidants and free radicals is vital for overall oral health and contributes to the body's defense mechanisms (63, 64). Saliva acts as the primary defense against free radicals, utilizing various antioxidant mechanisms such as glutamate, ascorbic acid, uric acid, and melatonin. Additionally, it contains antioxidant enzymes like superoxide dismutase, catalase, and glutathione peroxidase. These components work together to counteract the detrimental effects of excessive reactive oxygen and nitrogen species in the oral cavity, maintaining a balance necessary for physiological function (65). Researchers observed a distinct pattern of salivary antioxidant responses to oxidative stress in children with caries, noting higher total antioxidant capacity (TAC) and superoxide dismutase levels in caries-free children, alongside lower levels of MDA (66, 67).
Dental caries is considered the most widespread chronic oral disease and is recognized as a significant oral health problem worldwide. It is an irreversible microbial disease affecting the hard tissues of the teeth, characterized by damage to both the inorganic and organic components of the tooth, leading to tooth decay and potential tooth loss (68).
Currently, there are a large number of facts that indicate the development of pronounced oxidative stress in various diseases of the central nervous system. It is due to a combination of many important factors and characteristics of nervous tissue. The most significant of these is the high intensity of oxidative metabolism since 90% of the brain's energy needs are provided by aerobic processes (69).
In schizophrenia, there is a disruption of synaptic transmission and plasticity (70), including the disruption of N-methyl-D-aspartate receptor (NMDAR) activity, which is modulated by calcium ions (Ca2+). Additionally, Ca2+ ions activate neuronal nitric oxide synthase (nNOS), leading to the formation of nitric oxide (NO), carbonate (CO₃), and nitrite (NO₂) anions. These anions trigger neurodegeneration processes through the activation of heat shock protein 90 (Hsp90) and the induction of apoptosis (71).
Neurons have extremely weak antioxidant protection. Specifically, they contain 50 times less catalase compared to hepatocytes, making them more vulnerable to oxidative damage. The content of reduced glutathione (GSH) is approximately 50% lower in neurons compared to other cells. For instance, neurons have about 5 μM of GSH, whereas hepatocytes contain around 1,011 μM (72).
Numerous studies indicate a decreased concentration of reduced glutathione and an increased concentration of oxidized glutathione in various biological samples of schizophrenia patients. One of the studies conducted by Dariusz Juchnowicz revealed changes of catalase and glutathione peroxidase, which can be determining factors of schizophrenia (73). These findings have been observed in plasma (74), erythrocytes, neutrophils, platelets (73), cerebrospinal fluid (75), and in different postmortem brain regions (75–77). Although in patients with schizophrenia compared to controls, significant changes were observed in nitric oxide (NO) levels, but not in catalase (CAT) levels. However, alterations were noted in other antioxidant enzymes such as plasma glutathione peroxidase (GSHPx) and superoxide dismutase (SOD) (78).
In studies comparing neuroleptic-treated and untreated schizophrenic patients, both groups exhibited similar activities of SOD, which were approximately 60% higher than those found in normal, healthy individuals (30). This suggests that elevated SOD activity is a consistent feature in schizophrenia, regardless of neuroleptic treatment status.
The limitations of the presented cases can be categorized in biological and physiological, reflecting the challenges and constraints associated with dental treatment for patients with schizophrenia.
The use of antipsychotics and other drugs (e.g., Haloperidol, Clozapine, or Risperidone) can cause xerostomia, which affects post-operative healing (79, 80). Also, they are known that hyposalivation can induce high risk of caries, periodontitis, which are a predisposing factor for a poor oral health (9).
There is also a limitation regarding the long-term verification of the patient. Even if the primary integration has been seen, we cannot know if the patient will comply with all the indications for a long period of time. The limitations of these cases reflect the complexity of managing patients with schizophrenia, emphasizing the need for rigorous planning, effective communication among specialists, and long-term monitoring to ensure treatment success.
In recent years, research interest in the relationship between oxidative stress, inflammation, and oral health has grown significantly. However, there is still limited literature on how oral diseases and inflammation manifest in individuals with schizophrenia (19). Meanwhile, dental implants have shown high long-term success rates in most patients (39). Recently there are studies that show how choosing implant materials that reduce the risk of oxidative stress, such as implants specially treated to prevent the accumulation of ROS (10).
These clinical cases are important for both scientists and people with neuropsychiatric conditions, as they provide practical and relevant examples for the management of patients with complex medical conditions, such as schizophrenia, and demonstrate how dental treatments can be tailored to the patient's overall health status.
The essence of these clinical cases encompasses both the multidisciplinary approach and the fact that complex dental procedures can be performed with good management of systemic complications. They can serve as a foundation for the development of new protocols to balance risks, inflammation, and medical education among patients with neuropsychiatric diseases such as schizophrenia.
While it is well accepted that OS contributes significantly to the pathogenesis of schizophrenia, there is no consensus on whether OS is the primary cause of the disease or if it occurs as a secondary effect influenced by environmental factors or long-term treatments. Individuals with schizophrenia face a heightened risk of oral health issues, including dental caries, periodontal disease, and oral mucosal conditions, compared to the general population. Although we are in the stage of literature, in light of these findings, therapeutic interventions aimed at restoring oxidative balance, such as antioxidant therapies, hold promise for preventing and managing oxidative stress related oral diseases. A better understanding of the mechanisms linking oxidative stress to oral health can guide the development of targeted strategies to improve patient outcomes and overall oral health. Patients with schizophrenia face unique challenges in implant therapy due to impaired oral hygiene, limited compliance, and the added risk of oxidative stress. Despite the increasing use of dental implants, there is a significant lack of research on their outcomes in individuals with neuropsychiatric disorders, particularly schizophrenia. This gap underscores the need for tailored approaches, multidisciplinary care, and targeted research to address the specific needs of this population.
Fostering collaboration between dental professionals, psychiatrists, and caregivers, while incorporating strategies to mitigate oxidative stress, is essential for improving oral health outcomes and expanding access to implant therapy for patients with schizophrenia and other neuropsychiatric conditions.
EB: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. VR: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Software, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AC: Conceptualization, Writing – original draft, Writing – review & editing. VB: Conceptualization, Formal Analysis, Methodology, Writing – original draft, Writing – review & editing. RD: Conceptualization, Formal Analysis, Investigation, Visualization, Writing – original draft, Writing – review & editing. CS: Conceptualization, Formal Analysis, Methodology, Resources, Validation, Visualization, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Bitanihirwe BKY, Woo TUW. Oxidative stress in schizophrenia: an integrated approach. Neurosci Biobehav Rev. (2011) 35:878–93. doi: 10.1016/j.neubiorev.2010.10.008
2. Schultz SH, North SW, Shields CG. Schizophrenia: a review. Am Fam Physician. (2007) 75:1821–9.17619525
3. Yang M, Chen P, He MX, Lu M, Wang HM, Soares JC, et al. Poor oral health in patients with schizophrenia: a systematic review and meta-analysis. Schizophr Res. (2018) 201:3–9. doi: 10.1016/j.schres.2018.04.031
4. Slade GD. Communify dentistiy and oral epidemiology derivation and validation of a short-form oral health impact profile. Community Detit Oral Epidemiol. (1997) 25:284–90. doi: 10.1111/j.1600-0528.1997.tb00941.x
5. Kisely S. No mental health without oral health. Can J Psychiatry. (2016) 61:277–82. doi: 10.1177/0706743716632523
6. Kang J, Wu J, Aggarwal V, Shiers D, Doran T, Palmier-Claus J. Oral Health Inequality in People with Severe Mental Illness: A Cross-Sectional Study Using National Health and Nutrition Examination Survey 1999–2016. medRxiv. (2021).
7. Mehrabanian M, Ahari UZ, Fathi A, Parizi MM. Comparison of dental health Status in schizophrenic patients with healthy individuals. Clin Schizophr Relat Psychoses. (2021) 15:1–5. doi: 10.3371/CSRP.MMUA.102821
8. Chu KY, Yang NP, Chou P, Chiu HJ, Chi LY. Factors associated with dental caries among institutionalized residents with schizophrenia in Taiwan: a cross-sectional study. BMC Public Health. (2010) 10:482. doi: 10.1186/1471-2458-10-482
9. McGorry P. Royal Australian and New Zealand college of psychiatrists clinical practice guidelines for the treatment of schizophrenia and related disorders. Aust N Z J Psychiatry. (2005) 39:410–72. doi: 10.1177/0004867416641195
11. Tenzer JA, Orozco H. Traumatic glossectomy. Report of a case. Oral Surg Oral Med Oral Pathol. (1970) 30:182–4. doi: 10.1016/0030-4220(70)90358-0
12. Mester R. The psychodynamics of the dental pathology of chronic schizophrenic patients. Isr J Psychiatry Relat Sci. (1982) 19:255–61.7184896
13. Kenkre AM, Spadigam AE. Oral health and treatment needs in institutionalized psychiatric patients in India. Indian J Dent Res. (2000) 11:5–11.11307250
14. Friedlander AH, Marder SR. The psychopathology, medical management and dental implications of schizophrenia. J Am Dent Assoc. (2002) 133:603–10. doi: 10.14219/jada.archive.2002.0236
15. Hughes JR, Hatsukami DK, Mitchell JE, Dahlgren LA. Prevalence of smoking among psychiatric outpatients. Am J Psychiatry. (1986) 143:993–7. doi: 10.1176/ajp.143.8.993
16. Malhotra R, Kapoor A, Grover V, Kaushal S. Nicotine and periodontal tissues. J Indian Soc Periodontol. (2010) 14:72–9. doi: 10.4103/0972-124X.65442
17. Kilbourne AM, Horvitz-Lennon M, Post EP, McCarthy JF, Cruz M, Welsh D, et al. Oral health in veterans affairs patients diagnosed with serious mental illness. J Public Health Dent. (2007) 67:42–8. doi: 10.1111/j.1752-7325.2007.00007.x
18. Kiyak HA, Reichmuth M. Barriers to and enablers of older Adults’ use of dental services. J Dent Educ. (2005) 69:975–86. doi: 10.1002/j.0022-0337.2005.69.9.tb03994.x
19. Gupta S, P PK, Gupta R. Necessity of oral health intervention in schizophrenic patients—a review. Nepal J Epidemiol. (2017) 6:605–12. doi: 10.3126/nje.v6i4.17254
20. Dickerson FB, McNary SW, Brown CH, Kreyenbuhl J, Goldberg RW, Dixon LB. Somatic healthcare utilization among adults with serious mental illness who are receiving community psychiatric services. Med Care. (2003) 41:560–70. doi: 10.1097/00005650-200304000-00011
21. Saraiva S, Bachmann M, Andrade M, Liria A. Bridging the mental health treatment gap: effects of a collaborative care intervention (matrix support) in the detection and treatment of mental disorders in a Brazilian city. Fam Med Community Health. (2020) 8. doi: 10.1136/fmch-2019-000263
22. Šarac Z, Zovko R, Curlin M, Filakovi P. Dental medicine and psychiatry: the need for collaboration and bridging the professional gap. Psychiatr Danub. (2020) 32:151–8. doi: 10.24869/psyd.2020.151
23. Chaudhary P, Janmeda P, Docea AO, Yeskaliyeva B, Abdull Razis AF, Modu B, et al. Oxidative stress, free radicals and antioxidants: potential crosstalk in the pathophysiology of human diseases. Front Chem. (2023) 11:1158198. doi: 10.3389/fchem.2023.1158198
24. Davies KJ. Oxidative stress: the paradox of aerobic life. Biochem Soc Symp. (1995) 61:1–31. doi: 10.1042/bss0610001
25. Betteridge DJ. What is oxidative stress? Proceedings of the Metabolism: Clinical and Experimental. Vol. 49 (2000).
26. Ng F, Berk M, Dean O, Bush AI. Oxidative stress in psychiatric disorders: evidence base and therapeutic implications. Int J Neuropsychopharmacol. (2008) 11:851–76. doi: 10.1017/S1461145707008401
27. Halliwell B. Oxidative stress and neurodegeneration: where are we now? J Neurochem. (2006) 97:1634–58. doi: 10.1111/j.1471-4159.2006.03907.x
28. Mahadik SP, Pillai A, Joshi S, Foster A. Prevention of oxidative stress-mediated neuropathology and improved clinical outcome by adjunctive use of a combination of antioxidants and Omega-3 fatty acids in schizophrenia. Int Rev Psychiatry. (2006) 18:119–31. doi: 10.1080/09540260600581993
29. Ranjekar PK, Hinge A, Hegde MV, Ghate M, Kale A, Sitasawad S, et al. Decreased antioxidant enzymes and membrane essential polyunsaturated fatty acids in schizophrenic and bipolar mood disorder patients. Psychiatry Res. (2003) 121:109–22. doi: 10.1016/S0165-1781(03)00220-8
30. Ermakov EA, Dmitrieva EM, Parshukova DA, Kazantseva DV, Vasilieva AR, Smirnova LP. Oxidative stress-related mechanisms in schizophrenia pathogenesis and new treatment perspectives. Oxid Med Cell Longev. (2021) 2021:8881770. doi: 10.1155/2021/8881770
31. Castellanos-Cosano L, Corcuera-Flores JR, Mesa-Cabrera M, Cabrera-Domínguez J, Torres-Lagares D, Machuca-Portillo G. Dental implants placement in paranoid squizofrenic patient with obsessive-compulsive disorder: a case report. J Clin Exp Dent. (2017) 9:e1371–4. doi: 10.4317/jced.54356
32. Choi Y, Kim H, Rhee S-H, Ryoo S-H, Karm M-H, Seo K-S, et al. Multiple implant therapy with multiple inductions of general anesthesia in non-compliant patients with schizophrenia: a case report. J Dent Anesth Pain Med. (2019) 19:239–44. doi: 10.17245/jdapm.2019.19.4.239
33. Implant supported overdenture. Sujay\’s Dental Care. Available online at: https://www.sujaysdentalcare.com/smile-story-of-the-week/dental-implants-case-smile-story- (accessed August 15, 2024)
34. Santhosh Kumar S, Cantillo R, Ye D. The relationship between oral health and schizophrenia in advanced age—a narrative review in the context of the current literature. J Clin Med. (2023) 12:6496. doi: 10.3390/jcm12206496
35. Esquivel-Chirino C, Gómez-Landeros JC, Carabantes-Campos EP, Carmona-Ruiz D, Valero-Princet Y, Márquez-Correa C, et al. The impact of oxidative stress on dental implants. Eur J Dent Oral Heal. (2021) 2:1–8. doi: 10.24018/ejdent.2021.2.1.37
36. Weinberg MA, Segelnick SL, Kay LB, Nair V. Medical and dental standardization for solid organ transplant recipients. N Y State Dent J. (2013) 79:35–40.24600763
37. Zusman SP, Ponizovsky AM, Dekel D, Masarwa AES, Ramon T, Natapov L, et al. An assessment of the dental health of chronic institutionalized patients with psychiatric disease in Israel. Spec Care Dent. (2010) 30:35–40. doi: 10.1111/j.1754-4505.2009.00118.x
38. Suárez-López del Amo F, Garaicoa-Pazmiño C, Fretwurst T, Castilho RM, Squarize CH. Dental implants-associated release of Titanium particles: a systematic review. Clin Oral Implants Res. (2018) 29:1085–100. doi: 10.1111/clr.13372
39. Tsaryk R, Kalbacova M, Hempel U, Scharnweber D, Unger RE, Dieter P, et al. Response of human endothelial cells to oxidative stress on Ti6Al4V alloy. Biomaterials. (2007) 28:806–13. doi: 10.1016/j.biomaterials.2006.09.033
40. Mouthuy PA, Snelling SJB, Dakin SG, Milković L, Gašparović AČ, Carr AJ, et al. Biocompatibility of implantable materials: an oxidative stress viewpoint. Biomaterials. (2016) 109:10789–1698. doi: 10.1016/j.biomaterials.2016.09.010
41. Yanez M, Blanchette J, Jabbarzadeh E. Modulation of inflammatory response to implanted biomaterials using natural compounds. Curr Pharm Des. (2017) 23:6347–57. doi: 10.2174/1381612823666170510124348
42. Ahmadi-Motamayel F, Goodarzi MT, Hendi SS, Kasraei S, Moghimbeigi A. Total antioxidant capacity of saliva and dental caries. Med Oral Patol Oral Cir Bucal. (2013) 18:e553–6. doi: 10.4317/medoral.18762
43. Arvidson K, Bystedt H, Frykholm A, von Konow L, Lothigius E. A 3-year clinical study of astra dental implants in the treatment of edentulous mandibles. Int J Oral Maxillofac Implants. (1992) 7:321–9.1289257
44. Gabre P, Martinsson T, Gahnberg L. Longitudinal study of dental caries, tooth mortality and interproximal bone loss in adults with intellectual disability. Eur J Oral Sci. (2001) 109:20–6. doi: 10.1034/j.1600-0722.2001.00965.x
45. Fridovich I. Fundamental aspects of reactive oxygen species, or what’s the matter with oxygen? Proceedings of the Annals of the New York Academy of Sciences. Vol. 893 (1999).
46. Fang YZ, Yang S, Wu G. Free radicals, antioxidants, and nutrition. Nutrition. (2002) 18:872–9. doi: 10.1016/S0899-9007(02)00916-4
47. Gentric G, Maillet V, Paradis V, Couton D, L’Hermitte A, Panasyuk G, et al. Oxidative stress promotes pathologic polyploidization in nonalcoholic fatty liver disease. J Clin Invest. (2015) 125:981–92. doi: 10.1172/JCI73957
48. Pisoschi AM, Pop A. The role of antioxidants in the chemistry of oxidative stress: a review. Eur J Med Chem. (2015) 97:55–74. doi: 10.1016/j.ejmech.2015.04.040
49. Jin LJ, Lamster IB, Greenspan JS, Pitts NB, Scully C, Warnakulasuriya S. Global burden of oral diseases: emerging concepts, management and interplay with systemic health. Oral Dis. (2016) 22:609–19. doi: 10.1111/odi.12428
50. Waddington RJ, Moseley R, Embery G. Reactive oxygen Species: a potential role in the pathogenesis of periodontal diseases. Oral Dis. (2000) 6(3):138–51. doi: 10.1111/j.1601-0825.2000.tb00325.x
51. Baltacıoğlu E, Yuva P, Aydın G, Alver A, Kahraman C, Karabulut E, et al. Lipid peroxidation levels and total oxidant/antioxidant status in serum and saliva from patients with chronic and aggressive periodontitis. Oxidative stress index: a new biomarker for periodontal disease? J Periodontol. (2014) 85:1432–41. doi: 10.1902/jop.2014.130654
52. Çanakçı CF, Tatar A, Çanakçı V, Cicek Y, Oztas S, Orbak R. New evidence of premature oxidative DNA damage: mitochondrial DNA deletion in gingival tissue of patients with periodontitis. J Periodontol. (2006) 77:1894–900. doi: 10.1902/jop.2006.060108
53. Hezel MP, Weitzberg E. The oral microbiome and nitric oxide homoeostasis. Oral Dis. (2015) 21:7–16. doi: 10.1111/odi.12157
54. Connelly ST, Macabeo-Ong M, Dekker N, Jordan RCK, Schmidt BL. Increased nitric oxide levels and INOS over-expression in oral squamous cell carcinoma. Oral Oncol. (2005) 41:261–7. doi: 10.1016/j.oraloncology.2004.09.007
55. Peymanfar Y, Mahjour F, Shrestha N, de la Cueva A, Chen Y, Huang S, et al. The lysyl oxidase G473A polymorphism exacerbates oral cancer development in humans and mice. Int J Mol Sci. (2023) 24:9407. doi: 10.3390/ijms24119407
56. McCormick DL, Phillips JM, Horn TL, Johnson WD, Steele VE, Lubet RA. Overexpression of cyclooxygenase-2 in rat oral cancers and prevention of oral carcinogenesis in rats by selective and nonselective COX inhibitors. Cancer Prev Res. (2010) 3:73–81. doi: 10.1158/1940-6207.CAPR-09-0151
57. Gào X, Schöttker B. Reduction-oxidation pathways involved in cancer development: a systematic review of literature reviews. Oncotarget. (2017) 8:51888–906. doi: 10.18632/oncotarget.17128
58. Roopashree MR, Gondhalekar RV, Shashikanth MC, George J, Thippeswamy SH, Shukla A. Pathogenesis of oral lichen planus—a review. J Oral Pathol Med. (2010) 39:729–34. doi: 10.1111/j.1600-0714.2010.00946.x
59. Lodi G, Carrozzo M, Furness S, Thongprasom K. Interventions for treating oral lichen planus: a systematic review. Br J Dermatol. (2012) 166:938–47. doi: 10.1111/j.1365-2133.2012.10821.x
60. van der Meij EH, Mast H, van der Waal I. The possible premalignant character of oral lichen planus and oral lichenoid lesions: a prospective five-year follow-up study of 192 patients. Oral Oncol. (2007) 43:742–8. 17112770
61. Ergun S, Troşala ŞC, Warnakulasuriya S, Özel S, Önal AE, Ofluoǧlu D, et al. Evaluation of oxidative stress and antioxidant profile in patients with oral lichen planus. J Oral Pathol Med. (2011) 40:286–93. doi: 10.1111/j.1600-0714.2010.00955.x
62. Lopez-Jornet P, Martinez-Canovas A, Pons-Fuster A. Salivary biomarkers of oxidative stress and quality of life in patients with oral lichen planus. Geriatr Gerontol Int. (2014) 14:654–9. doi: 10.1111/ggi.12153
63. Buzalaf MAR, Hannas AR, Kato MT. Saliva and dental erosion. J Appl Oral Sci. (2012) 20:493–502. doi: 10.1590/s1678-77572012000500001
64. Lee YH, Wong DT. Saliva: an emerging biofluid for early detection of diseases. Am J Dent. (2009) 22:241–8.19824562
65. Tóthová L, Kamodyová N, Červenka T, Celec P. Salivary markers of oxidative stress in oral diseases. Front Cell Infect Microbiol. (2015) 5:73. doi: 10.3389/fcimb.2015.00073
66. Araujo HC, Nakamune ACMS, Garcia WG, Pessan JP, Antoniali C. Carious lesion severity induces higher antioxidant system activity and consequently reduces oxidative damage in children’s saliva. Oxid Med Cell Longev. (2020) 2020:3695683. doi: 10.1155/2020/3695683
67. Da Silva PV, Troiano JA, Nakamune ACMS, Pessan JP, Antoniali C. Increased activity of the antioxidants systems modulate the oxidative stress in saliva of toddlers with early childhood caries. Arch Oral Biol. (2016) 70:62–6. doi: 10.1016/j.archoralbio.2016.06.003
68. Li G, Shofer JB, Rhew IC, Kukull WA, Peskind ER, McCormick W, et al. Age-varying association between statin use and incident Alzheimer’s disease. J Am Geriatr Soc. (2010) 58:1311–7. doi: 10.1111/j.1532-5415.2010.02906.x
69. Lohr JB, Browning JA. Free radical involvement in neuropsychiatric illnesses. Proceedings of the Psychopharmacology Bulletin. Vol. 31 (1995).
70. Pocklington AJ, O’Donovan M, Owen MJ. The synapse in schizophrenia. Eur J Neurosci. (2014) 39:1059–67. doi: 10.1111/ejn.12489
71. Franco MC, Ye Y, Refakis CA, Feldman JL, Stokes AL, Basso M, et al. Nitration of Hsp90 induces cell death. Proc Natl Acad Sci U S A. (2013) 110:E1102–11. doi: 10.1073/pnas.1215177110
72. Dwivedi D, Megha K, Mishra R, Mandal PK. Glutathione in brain: overview of its conformations, functions, biochemical characteristics, quantitation and potential therapeutic role in brain disorders. Neurochem Res. (2020) 45:1461–80. doi: 10.1007/s11064-020-03030-1
73. Flatow J, Buckley P, Miller BJ. Meta-analysis of oxidative stress in schizophrenia. Biol Psychiatry. (2013) 74:400–9. doi: 10.1016/j.biopsych.2013.03.018
74. Raffa M, Atig F, Mhalla A, Kerkeni A, Mechri A. Decreased glutathione levels and impaired antioxidant enzyme activities in drug-naive first-episode schizophrenic patients. BMC Psychiatry. (2011) 11:124. doi: 10.1186/1471-244X-11-124
75. Do KQ, Trabesinger AH, Kirsten-Krüger M, Lauer CJ, Dydak U, Hell D, et al. Schizophrenia: glutathione deficit in cerebrospinal fluid and prefrontal cortex in vivo. Eur J Neurosci. (2000) 12:3721–8. doi: 10.1046/j.1460-9568.2000.00229.x
76. Yao JK, Leonard S, Reddy R. Altered glutathione redox state in schizophrenia. Dis Markers. (2006) 22:83–93. doi: 10.1155/2006/248387
77. Kumar J, Liddle EB, Fernandes CC, Palaniyappan L, Hall EL, Robson SE, et al. Glutathione and glutamate in schizophrenia: a 7T MRS study. Mol Psychiatry. (2020) 25:1703. doi: 10.1038/s41380-018-0104-7
78. Zhang M, Zhao ZM, He L, Wan CL. A meta-analysis of oxidative stress markers in schizophrenia. Sci China Life Sci. (2010) 53:112–24. doi: 10.1007/s11427-010-0013-8
79. Tang WK, Sun FCS, Ungvari GS, O’Donnell D. Oral health of psychiatric in-patients in Hong Kong. Int J Soc Psychiatry. (2004) 50:186–91. doi: 10.1177/0020764004043134
80. Kilian R, Becker T, Krüger K, Schmid S, Frasch K. Health behavior in psychiatric in-patients compared with a German general population sample. Acta Psychiatr Scand. (2006) 114:242–8. doi: 10.1111/j.1600-0447.2006.00850.x
Keywords: schizophrenia, dental care, oxidative stress, dental treatment, dental implants
Citation: Burlui E, Rarinca V, Ciobica A, Burlui V, Dobrin R and Stadoleanu C (2025) Insights into the schizophrenia and dental care: focusing on interaction between implant treatments and oxidative stress. Front. Dent. Med. 6:1542913. doi: 10.3389/fdmed.2025.1542913
Received: 10 December 2024; Accepted: 14 February 2025;
Published: 28 February 2025.
Edited by:
Roberta Gasparro, University of Naples Federico II, ItalyReviewed by:
Pradeep Kumar Yadalam, Saveetha Dental College and Hospitals, IndiaCopyright: © 2025 Burlui, Rarinca, Ciobica, Burlui, Dobrin and Stadoleanu. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Viorica Rarinca, cmFyaW5jYV92aW9yaWNhQHlhaG9vLmNvbQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.