 Natalie Hadad-Arrascue
Natalie Hadad-Arrascue María Claudia Garcés-Elías*
María Claudia Garcés-Elías*
- Facultad de Estomatología, Universidad Peruana Cayetano Heredia, Lima, Peru
Background: Leading international health organizations advise using toothpaste that contains at least 1,000 parts per million of fluoride, emphasizing that this practice should begin with the eruption of the first primary tooth.
Aim: To determine the association between access to dental services and the use of toothpaste with 1,000 ppm fluoride or more in Peruvian children under twelve years of age.
Materials and methods: A cross-sectional analysis was conducted using data from the 2021 Demographic and Family Health Survey. The main variable studied was the use of toothpaste containing a fluoride concentration of 1,000 ppm or more. Additionally, the access to dental care, the time elapsed since the last dental visit, and the type of healthcare facility were analyzed. Multilevel regression was applied to examine the relationship between variables and the dependent variable, with Peru's 24 regions serving as the analytical level.
Results: According to the bivariate analysis, the natural region, area of residence, place of residence, wealth index, and age were associated with the use of fluoride toothpaste with 1,000 ppm or more. In the multilevel analysis, the access to dental services was not associated with the use of fluoride toothpaste with 1,000 ppm or more (p = 0.454); similarly, the time elapsed since the last dental visit also showed no association (p = 0.676), as did the type of healthcare facility (p = 0.752, p = 0.896, p = 0.983).
Conclusion: Accessing dental services, the time elapsed since the last dentist visit, and the location where that care was received were not associated with the use of toothpaste containing 1,000 ppm or more of fluoride among Peruvian children during the year 2021.
Introduction
Several factors can prevent the development and progression of dental caries, with the practice of favorable behaviors like using fluoride toothpaste (FT) and regular toothbrushing standing out as key measures (1, 2). This combination is regarded as the primary preventive approach, independent of direct interventions by dentists, for maintaining good oral health. Consequently, many international organizations recommend using toothpaste with a minimum fluoride content of 1,000 parts per million (ppm). This practice should begin with the eruption of the first primary tooth, with its effectiveness maximized by applying it twice a day during toothbrushing (3, 4).
Since the World Health Organization includes FT in its model list of essential medicines, its quality and availability are crucial concerns for international public health (5). Among the critical factors associated with using FT are the financial capacity to purchase it regularly, the socio-cultural integration of its use into personal habits, product availability, and access to dental services (6, 7). In terms of the latter, timely dental care is essential for adopting a preventive approach and successfully developing beneficial oral health habits (8), such as using FT (9).
In Peru, the Clinical Practice Guidelines for the Prevention, Diagnosis, and Treatment of Dental Caries emphasizes the importance of a dental visit before the first year of life to identify a child's risk of caries and to educate parents or caregivers about oral health. This includes recommendations for home care, such as the use of FT. However, there are few nationally contextualized studies on the use of FT (7, 10) and its associated factors. Therefore, this research aimed to determine the association between access to dental services and the use of toothpaste with 1,000 ppm fluoride or more in Peruvian children under twelve years of age.
Materials and methods
Study design
A cross-sectional analysis was conducted using data from the 2021 Demographic and Family Health Survey (ENDES), managed by the National Institute of Statistics and Informatics of Peru (INEI). The ENDES survey is conducted annually by a rigorously trained team that performs in-home interviews and administers questionnaires to the selected population.
A two-stage, stratified, probabilistic, and independent sampling method was employed at the departmental level, covering both urban and rural areas. In 2021, the sample included 168,145 children under twelve years old. The final sample size, consisting of 24,057 children, was determined based on the respondents’ reports regarding the use of FT (measured in ppm). Incomplete records were excluded as part of the data management process. It is important to note that the information was provided by the individuals responsible for the children's healthcare (11). The ENDES survey sampling frame is based on the statistical and cartographic information from the 2017 National Population and Housing Censuses. The sampling units used are private households and clusters. In reference to two-stage sampling, the first stage involves selecting the primary sampling units (PSUs), which are the clusters, while the second stage involves selecting the secondary sampling units, which are the households. In two-stage household surveys, it is common to rotate clusters within the sample. Each year, a group of clusters is removed from the sample and another group is added, enabling continuous updating of the sampling process (11, 12).
Variables
In this study, the dependent variable was defined as the use of toothpaste containing a fluoride concentration of 1,000 ppm or more. Question 839 from the ENDES health questionnaire states: “Please, could you show me the toothbrush and toothpaste that (NAME) uses to brush their teeth? Verify the fluoride concentration of the toothpaste and circle the corresponding code.” The possible responses pertain to the fluoride concentration in parts per million (ppm). The independent variables included access to dental care, the time elapsed since the last dental visit (measured in years), and the place of dental care. The type of healthcare facility providing the service was categorized as the Ministry of Health of Peru (MINSA), the Social Health Insurance of Peru (ESSALUD), the Armed Forces (FF.AA), the Police Forces (PNP), and the private sector. Additionally, covariates were delineated, including the natural region classified as Metropolitan Lima, the rest of the coast, the highlands, and the jungle.
Additionally, the area of residence was categorized into urban and rural settings, while the place of residence was classified as capital, small city, town, or countryside. Altitude was measured as either less than 2,500 meters above mean sea level (MAMSL) or 2,500 MAMSL and above. A wealth index was used to indicate each household's capacity to access and enjoy goods and services. This index applied a scoring system developed by the Demographic and Health Surveys Program of the United States, allowing for the classification of households into quintiles ranging from the least advantaged to the most advantaged (13, 14). Lastly, the variables included health insurance coverage, sex, and age.
Procedures and statistics
Regarding the data acquisition process, the data were obtained from the official website of the National Institute of Statistics and Informatics (INEI) (http://iinei.inei.gob.pe/microdatos/), utilizing various modules and information sources. The data were then consolidated into a single matrix for analysis using STATA software, version 17. The statistical analysis involved calculating absolute and relative frequencies through descriptive methods. Chi-square tests were employed to investigate associations among the study variables. The “svy” command was used to ensure representative estimates aligned with the survey's design, incorporating sampling strata, primary units, and assigned weights.
Poisson logistic regression was used for multivariate analysis, determining crude (PR) and adjusted prevalence ratios (aPR) based on significant variables identified beforehand. Multilevel regression was applied to examine the relationship between variables and the dependent variable, with Peru's 24 regions serving as the analytical level. A variance component model (null model) was built using the dependent variable—use of toothpaste containing 1,000 ppm fluoride or more—without explanatory variables to assess overall variability attributed to regions, supporting subsequent analysis (P < .001).
Explanatory variables were then introduced to explore their associations with each independent variable and covariates. Four models were developed: unadjusted models 1, 2, and 3 for access to dental services, geographical characteristics, and sociodemographic factors, respectively, and adjusted model 4 for dental service access adjusted for covariates. It is important to note that the multilevel analysis performed accounted for the sampling method utilized in the study. A 95% confidence level and a significance level of P < 0.05 were applied uniformly across all analyses.
Ethics
Regarding ethical considerations, the Institutional Ethics Committee of Universidad Peruana Cayetano Heredia granted approval on August 3, 2021. These datasets are publicly available and include coded records to ensure the anonymity of survey participants.
Results
It must be stated that every frequency was analyzed independently. The use of toothpaste containing 1,000 ppm fluoride or more was reported by 81.46% (n = 4,507) of participants, while access to dental services was reported by 56.23% (n = 17,063). Only a minority, 12.64% (n = 1,985), indicated their last dental visit occurred less than two years ago, with the majority seeking care primarily from the Ministry of Health of Peru, accounting for 45.98% (n = 9,914) of visits (Table 1). In bivariate analysis, access to dental services, time since the last dental care, and the type of healthcare facility did not show significant associations with the use of toothpaste containing 1,000 ppm fluoride or more (p = 0.943, p = 0.800, and p = 0.166, respectively). Conversely, other sociodemographic factors such as natural region, area of residence, place of residence, wealth index, and age showed associations with the outcome (p < 0.001) (Table 2).
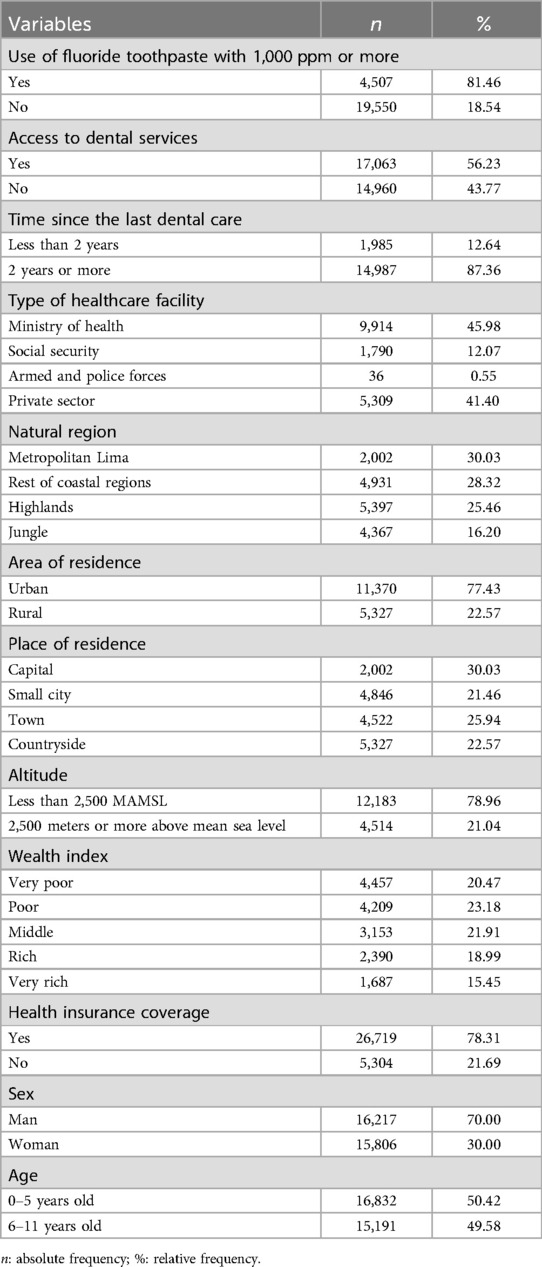
Table 1. Characteristics of children under 12 years old in Peru, 2021.

Table 2. Use of fluoride toothpaste with 1,000 ppm or more according to access to dental services and other characteristics in Peruvian children under 12 years old, 2021.
According to the multilevel regression analysis, access to dental services was not associated with the use of toothpaste with 1,000 ppm or more (p = 0.454); similarly, the time elapsed since the last dental visit also showed no association (p = 0.676), nor did the type of healthcare facility (p = 0.752, p = 0.896, p = 0.983) (Table 3).
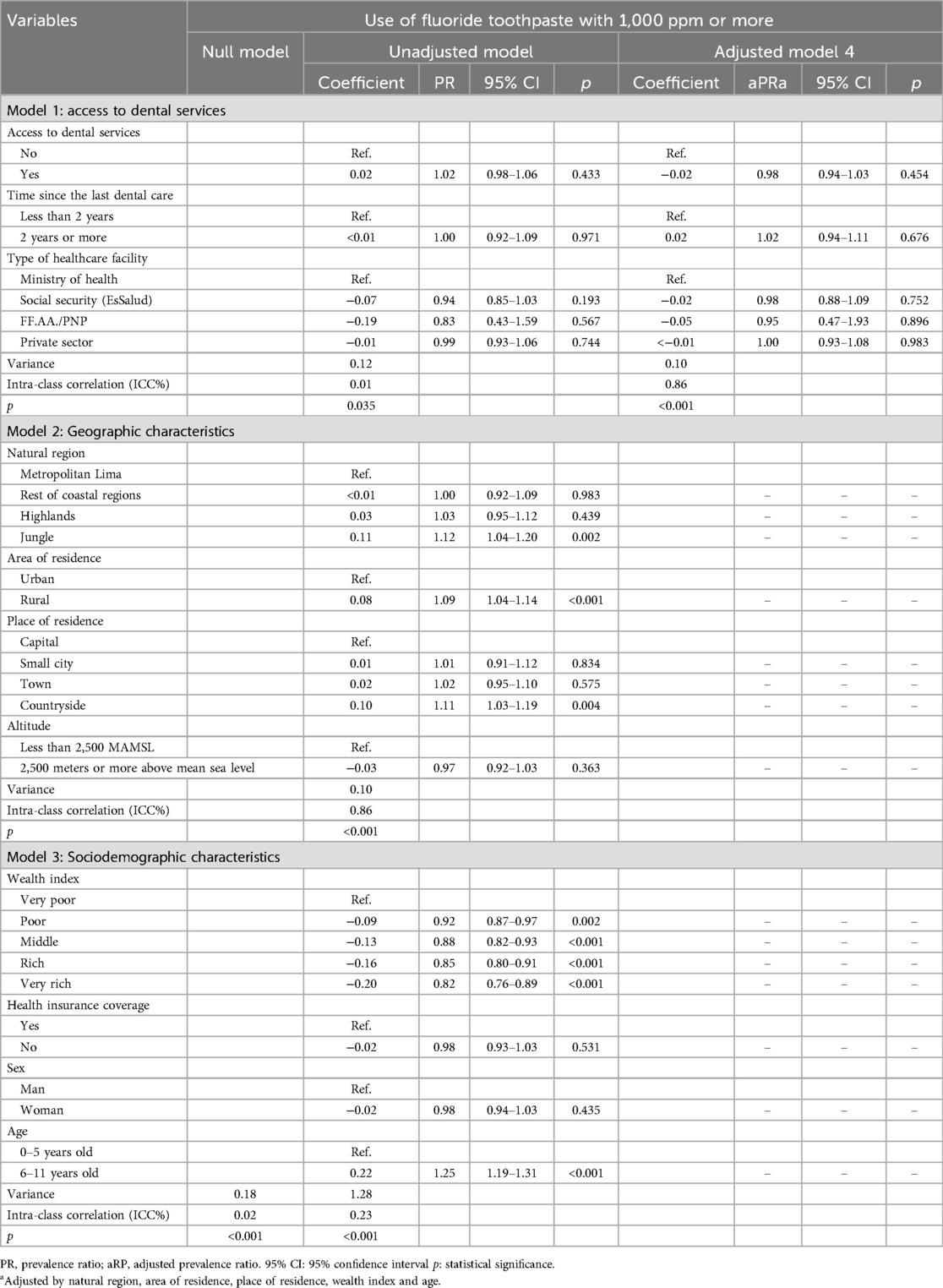
Table 3. Multilevel analysis between the use of fluoride toothpaste with 1,000 ppm or more and access to dental services.
Discussion
This research reveals that as of 2021, the use of toothpaste with a fluoride content of 1,000 ppm or more among Peruvian children is not associated with their use of dental services, the time since their last dental care, or the provider of this care. These findings provide valuable insights into the oral health practices of Peruvian children.
In contrast, in 2018, Hernández-Vásquez and Azañedo (1) analyzed the ENDES survey and found that more than a quarter of Peruvian children who had received dental care in the six months before the survey used toothpaste with an inadequate fluoride concentration (less than 1,000 ppm); moreover, these differences were statistically significant. However, those results were merely descriptive and did not include additional regression analyses to determine the strength of the association. Another study applied to Peruvian children, comparing the years 2019 and 2020, reported that the use of toothpaste with at least 1,000 ppm increased in the last year. The factors associated with this outcome were the natural region, area of residence, place of residence, wealth index, and age (2).
Two studies conducted in Asia examined oral hygiene habits and their associated factors. The first, a nationally representative study, revealed that Chinese adolescents who had previously received dental care and had a positive attitude towards regular dental check-ups were more likely to brush their teeth twice a day with fluoride toothpaste (15); however, it did not specify if the amount of fluoride in the toothpaste was adequate. Similarly, the second study, focused on Japanese university students, identified that dental services are the primary source of knowledge about oral hygiene and the implements they use (16). The findings of this research contrast with the results obtained in other studies, indicating that the factors influencing toothpaste use among Peruvian children are not linked to access to the healthcare system.
A survey conducted in 136 countries between December 2005 and March 2006 indicated that the economic ability to purchase toothpaste was one of the main barriers to its use (6). This situation persists more than 19 years later (17). In this regard, a report revealed a wide variability in the prices of fluoride toothpaste, notably high for the poorest 15% of the population in Sub-Saharan Africa, as well as in regions of South and Southeast Asia and the Pacific Islands. In these territories, the cost of an annual supply of fluoride toothpaste per person could represent a catastrophic health expense (18), which could lead to foregoing its use or purchasing lower-priced options that may not have an adequate formulation to meet preventive purposes. Research conducted in 2021 revealed that Peruvian children from higher socioeconomic levels were less likely to use fluoride toothpaste (more than 1,000 ppm) compared to those from families in extreme poverty.
Coinciding with this point, Quevedo and Carrizales (19), in their analysis of ENDES for 2019, 2020, and 2021, found that the socioeconomic level of children in Peru influenced the use of toothpaste with optimal fluoride content. Children from economically disadvantaged households showed greater use of this product than those from higher quintiles. An explanation for these findings could be that higher social strata have greater access to various options regarding oral hygiene products, allowing them to consider more factors when purchasing these products. A study classifies the fluoride content in toothpaste as the main factor in its choice, followed by previous experience and, finally, a dentist's recommendation (20).
According to the geographic characteristics that showed statistically significant differences in this study, Mlenga and Mumghamba indicate that there are inequalities in toothpaste use between rural and urban sectors (21), as demonstrated in Malawi, a country in Africa where more than three-quarters of the population live in rural areas. However, this publication does not specify whether the toothpaste contained adequate parts per million of fluoride. This study found that residing in rural areas was positively associated with using toothpaste with fluoride of 1,000 ppm or more, compared to urban areas. However, in Saudi Arabia, no statistically significant differences were identified between the two sectors (22).
In 2019, it was observed that Peruvian children aged 0–5 mainly used toothpaste with less than 1,000 ppm fluoride (7). This trend has persisted, as this research reports a similar situation in 2021. Consequently, age appears to be a characteristic indicating vulnerability in Peruvian children. Given the results of a study conducted in the capital city (10), this finding reinforces the need for the state and health authority to ensure compliance with the guidelines established in their clinical practice guidelines to prevent dental caries and the marketing of products in the country, which is also supported by their regulation on toothpaste manufacturing (23).
Among the limitations of this research is the use of a database extracted from nationwide surveys, meaning that the responses provided by the participating population could present certain inaccuracies due to self-reporting. Additionally, a slight loss of data occurred for certain variables, as not all respondents answered every question posed by the interviewers during the administration of the ENDES survey. Nevertheless, this remains Peru's primary source of monitoring oral health indicators. Additionally, the established study type only allows the results to identify levels of associated factors and not causal relationships.
Conclusion
Accessing dental services, the time elapsed since the last dentist visit, and the location where that care was received were not associated with the use of toothpaste containing 1,000 ppm or more of fluoride among Peruvian children during the year 2021.
Data availability statement
Publicly available datasets were analyzed in this study. This data can be found here: https://proyectos.inei.gob.pe/microdatos/.
Ethics statement
This study, which involved information records from human subjects, received approval from the Institutional Ethics Committee of Universidad Peruana Cayetano Heredia. Written informed consent from participants or participants' legal guardians/next of kin was not required, as the records were anonymized and coded.
Author contributions
NH-A: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing. MG-E: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Visualization, Writing – original draft, Writing – review & editing.
Funding
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. Facultad de Estomatología of Universidad Peruana Cayetano Heredia will cover the article processing charges.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
1. World Health Organization. Global oral health status report. Towards universal health coverage for oral health by 2030 (2023). Available online at: https://www.who.int/publications/i/item/9789240061484 (accessed July 25, 2023).
2. Whelton HP, Spencer AJ, Do LG, Rugg-Gunn AJ. Fluoride revolution and dental caries: evolution of policies for global use. J Dent Res. (2019) 98(8):837–46. doi: 10.1177/0022034519843495
3. Clark MB, Keels MA, Slayton RL, Section On Oral Health. Fluoride use in caries prevention in the primary care setting. Pediatrics. (2020) 146(6):e2020034637. doi: 10.1542/peds.2020-034637
4. Toumba KJ, Twetman S, Splieth C, Parnell C, van Loveren C, Lygidakis NΑ. Guidelines on the use of fluoride for caries prevention in children: an updated EAPD policy document. Eur Arch Paediatr Dent. (2019) 20(6):507–16. doi: 10.1007/s40368-019-00464-2
5. World Health Organization. Executive summary: the selection and use of essential medicines 2021: report of the 23 WHO Expert Committee on the selection and use of essential medicines (2021). Available online at: https://apps.who.int/iris/bitstream/handle/10665/345554/WHO-MHP-HPS-EML-2021.01-eng.pdf?sequence=1&isAllowed=y (accessed September 15, 2023).
6. Goldman AS, Yee R, Holmgren CJ, Benzian H. Global affordability of fluoride toothpaste. Global Health. (2008) 4:7. doi: 10.1186/1744-8603-4-7
7. Hernández-Vásquez A, Azañedo D. Cepillado dental y niveles de flúor en pastas dentales usadas por niños peruanos menores de 12 años [tooth brushing and fluoride levels in toothpaste used by Peruvian children under 12 years old]. Rev Peru Med Exp Salud Publica. (2019) 36(4):646–52. doi: 10.17843/rpmesp.2019.364.4900
8. Rosing K, Leggett H, Csikar J, Vinall-Collier K, Christensen LB, Whelton H, et al. Barriers and facilitators for prevention in Danish dental care. Acta Odontol Scand. (2019) 77(6):439–51. doi: 10.1080/00016357.2019.1587503
9. Brecher EA, Lewis CW. Infant oral health. Pediatr Clin N Am. (2018) 65(5):909–21. doi: 10.1016/j.pcl.2018.05.016
10. Chávez BA, Vergel GB, Cáceres CP, Perazzo MF, Vieira-Andrade RG, Cury JA. Fluoride content in children’s dentifrices marketed in Lima, Peru. Braz Oral Res. (2019) 33:e051. doi: 10.1590/1807-3107bor-2019.vol33.0051
11. Instituto Nacional de Estadística e Informática del Perú. Encuesta Demográfica y de Salud Familiar 2021 – Informe principal (2022). Available online at: https://proyectos.inei.gob.pe/endes/(accessed November 22, 2023).
12. Instituto Nacional de Estadística e Informática del Perú. Encuesta Demográfica y de Salud Familiar 2021- Diseño y cobertura de la muestra (2022). Available online at: https://www.inei.gob.pe/media/MenuRecursivo/publicaciones_digitales/Est/Lib1838/pdf/ApendiceA.pdf (accessed September 10, 2024).
13. United States Agency for International Development. The Demographic and Health Surveys Program. Wealth index (2016). Available online at: https://dhsprogram.com/topics/wealth-index/(accessed November 22, 2023).
14. National Institute of Statistics and Informatics, Peru. Demographic and Family Health Survey (2013). Available online at: https://www.inei.gob.pe/media/MenuRecursivo/publicaciones_digitales/Est/Lib1153/libro.pdf (accessed November 22, 2023).
15. Cui Z, Wang W, Si Y, Wang X, Feng X, Tai B, et al. Tooth brushing with fluoridated toothpaste and associated factors among Chinese adolescents: a nationwide cross-sectional study. BMC Oral Health. (2023) 23(1):765. doi: 10.1186/s12903-023-03506-w
16. Fukuhara D, Ekuni D, Kataoka K, Taniguchi-Tabata A, Uchida-Fukuhara Y, Toyama N, et al. Relationship between oral hygiene knowledge, source of oral hygiene knowledge and oral hygiene behavior in Japanese university students: a prospective cohort study. PLoS One. (2020) 15(7):e0236259. doi: 10.1371/journal.pone.0236259
17. Gkekas A, Varenne B, Stauf N, Benzian H, Listl S. Affordability of essential medicines: the case of fluoride toothpaste in 78 countries. PLoS One. (2022) 17(10):e0275111. doi: 10.1371/journal.pone.0275111
18. World Health Organization. Fluoride toothpaste (2021). Available online at: https://cdn.who.int/media/docs/default-source/essential-medicines/2021-eml-expert-committee/applications-for-addition-of-new-medicines/a.14_fluoride-toothpaste.pdf?sfvrsn=4eb40f4c_4 (accessed December 18, 2024).
19. Carrizales L, Quevedo E. Uso de pastas dentales en niños menores de 12 años en el perú durante los años 2019–2021: un análisis multivariado. Rev Estomatol Herediana. (2024) 34(2):157–65. doi: 10.20453/reh.v34i2.5533
20. Opeodu OI, Gbadebo SO. Factors influencing choice of oral hygiene products by dental patients in a Nigerian teaching hospital. Ann Ib Postgrad Med. (2017) 15(1):51–6.28970772
21. Mlenga F, Mumghamba EG. Oral hygiene practices, knowledge, and self-reported dental and gingival problems with rural-urban disparities among primary school children in Lilongwe, Malawi. Int J Dent. (2021) 2021:8866554. doi: 10.1155/2021/8866554
22. Alhudaithi AS, Alsughier Z, Alzaidan H, Aldhelai TA. Children’s oral health status among urban and rural areas of Qassim region, Saudi Arabia: a cross-sectional study. Cureus. (2023) 15(10):e47947. doi: 10.7759/cureus.47947
23. Ministerio de salud del Perú. Resolución Ministerial N° 454-2001-SA-DM. Aprueban Norma Técnica Sanitaria para la Adición de Fluoruros en Cremas Dentales, Enjuagatorios y otros productos utilizados en la Higiene Bucal (2021). Available online at: https://www.gob.pe/institucion/minsa/normas-legales/255609-454-2001-sa-dm (accessed December 18, 2024).
Keywords: dental care, toothpaste, health services accessibility, Peru, cross-sectional studies
Citation: Hadad-Arrascue N and Garcés-Elías MC (2024) Access to dental services and use of toothpaste with optimal fluoride content in Peruvian children. Front. Dent. Med 5:1467501. doi: 10.3389/fdmed.2024.1467501
Received: 20 July 2024; Accepted: 17 September 2024;
Published: 8 October 2024.
Edited by:
Oyinkan Sofola, University of Lagos, NigeriaReviewed by:
Olubukola Olamide Olatosi, University of Lagos, NigeriaOchiba Mohammed Lukandu, Moi University, Kenya
Copyright: © 2024 Hadad-Arrascue and Garcés-Elías. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: María Claudia Garcés-Elías, bWFyaWEuZ2FyY2VzQHVwY2gucGU=