
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
CASE REPORT article
Front. Dent. Med. , 09 August 2021
Sec. Pediatric Dentistry
Volume 2 - 2021 | https://doi.org/10.3389/fdmed.2021.704423
This article is part of the Research Topic Amelogenesis Imperfecta View all 4 articles
 Blanca Urzúa1†
Blanca Urzúa1† Susanne Krämer2,3†Irene Morales-Bozo1Claudia Camacho4María Joao Yubero3Francis Palisson3
Susanne Krämer2,3†Irene Morales-Bozo1Claudia Camacho4María Joao Yubero3Francis Palisson3 Ignacia Fuentes3,5
Ignacia Fuentes3,5 Ana Ortega-Pinto4*
Ana Ortega-Pinto4*Background: Epidermolysis bullosa (EB) corresponds to a series of conditions characterized by extreme fragility of the skin and/or mucous membranes. Of the four main types of EB, junctional EB (JEB) is the most associated with alterations in the teeth. The purposes of this study were to determine the clinical, histopathological, and ultrastructural characteristics of teeth with amelogenesis imperfecta (AI) in a patient with JEB, and compare them with control teeth, and correlate the findings with the mutations present in the patient.
Case Report: The study was conducted on a 10-year-old patient with JEB carrier of two recessive mutations in the LAMB3 gene and absence of the laminin-332 protein (LM-332), determined by immunofluorescence on a skin biopsy. The patient presents hypoplastic AI with very thin and yellow-brown colored enamel. Extraction of two permanent molars was performed due to pain and soft tissue covering the crown, resembling pulp polyp or hyperplastic gingiva. Light and scanning electron microscopy (SEM) revealed very thin enamel varying from complete absence to 60 μm, absence of normal prismatic structure, and presence of a cross-banding with a laminated appearance. The histopathological study revealed granulation tissue causing external crown resorption.
Conclusion: Although coronary resorption has been reported in patients with syndromic and non-syndromic AI, this is the first clinicopathological report of coronary resorption in partially erupted teeth in patients with JEB with mutations in the LAMB3 gene and hypoplastic AI. In patients with this condition, the presence of partially erupted teeth with soft tissue covering part of the crown, without a periodontal pocket, and with a radiographic image of partial coronal radiolucency should lead to suspicion of external coronary resorption.
Among the genetic conditions that can affect tooth development is epidermolysis bullosa (EB), which corresponds to a series of conditions characterized by fragility of the skin and mucosa, where blisters are generated by minimal trauma. In this disease, mutations have been reported in the genes encoding proteins related to the basal lamina and epidermis, causing severe architectural alterations in tissues (1, 2).
Four types of EB are recognized: simplex (EBS), junctional (JEB), dystrophic (DEB), and Kindler epidermolysis bullosa (KEB). Patients with all four types of EB can present skin fragility and mucous membranes lesions such as oral blisters and ulcers. All patients diagnosed with JEB have alterations of the structures of the teeth. In JEB, the most frequently observed alteration of the teeth is a hypoplasia of the enamel, which can be extremely thin (2–5). EB can be caused by alterations in 1 of 16 genes encoding proteins related to the maintenance of dermo-epidermal junction proteins, which provide the skin with enormous stability (2).
Junctional EB occurs due to recessive mutations in the genes encoding the laminin-332 protein (LAMA3, LAMB3, and LAMC2), integrin α6β4 (ITGA6 and ITGB4), integrin α3 (ITGA3), and collagen type XVII (COL17A1). The three protein complexes are located in the lamina lucida, joining the basal keratinocytes with the lamina densa, thus giving stability and adhesion to the two regions (2, 3, 6).
Junctional EB is most frequently caused by recessive mutations in the LAMB3 gene, which, in addition to the skin phenotype, also produces amelogenesis imperfecta (AI) in these patients (4, 5, 7). On the other hand, dominant mutations in LAMB3 can cause non-syndromic AI (8–10). In these cases, the teeth present a thin enamel in the temporary and permanent dentition, but no skin conditions are described. Interestingly, a family has been described in which the proband presented JEB with a dominant mutation in the gene for collagen 17 (COL17A1; p.G627V) and hypoplastic tooth enamel in both dentitions. The mother carrying the same mutation had hypoplastic tooth enamel and an absence of skin fragility (11).
These findings suggest that the dental enamel would be more prone than the skin to express clinical changes due to the mutations in the genes that synthesize proteins of the lamina lucida (11). However, there has been only limited information regarding dental structural alterations associated with the different mutated genes responsible for JEB. The main objective of this research was to compare the clinical, radiographic, histopathological, and ultrastructural characteristics of teeth with AI in one patient with JEB with the unaffected teeth of the control subject and to correlate these findings with the mutations found in LAMB3.
The results of this study are of great importance for patients since they contribute to an accurate diagnosis of each of these pathologies and their clinical variants. Several findings, in this case, are unique, such as the histopathological diagnosis of coronary resorption that clinically resembled a pulp or gingival polyp and the reduction in tooth sensitivity after crowning the remaining teeth affected by AI. These findings allow us to understand the pathogenesis of these conditions and contribute to undertaking preventive measures and providing specific dental therapies to protect and/or restore altered dental structures in these patients with special needs.
A 10-year-old female patient with severe JEB presented with dental pain to the Special Care Clinic at the Faculty of Dentistry of the University of Chile. The patient has been on a preventive dental program since the age of 3 years. The care has been based on education and prevention using fluoride varnish applications. Clinically, very thin yellowish enamel was observed, both in the temporary and permanent dentition.
Her EB diagnosis was based on clinical, histopathological, and molecular findings. Immunofluorescence mapping showed the absence of the β3 chain of laminin 332 in the zone of the basement membrane, and two recessive mutations in LAMB3: c.957_958dup77 and c.3228+1G>A (NM_000228.2) were identified and previously published in Fuentes I. (12).
Despite the generalized enamel hypoplasia, the patient had remained free of decay. At the dental checkup at age 10, she reported pain in the first permanent mandibular molars: teeth 3.6 and 4.6. Clinically, soft tissue was covering the crown of both permanent mandibular molars, compatible with pulp polyp or hyperplastic gingiva. The patient refused to receive restorative treatment because her perioral granulation tissue areas caused too much pain when opening the mouth for long periods, and she was concerned about the slow healing rate of these wounds. Therefore, a surgical approach was chosen (extraction of both molars). Both sockets healed uneventfully. The remaining teeth were restored using fixed crowns. Ceramic fixed crowns were performed on all eight incisors that were already fully erupted, and provisory acrylic crowns were used to cover the canines, premolars, and molars, which were partially erupted.
Surprisingly, the greatest benefit of covering the teeth was the reduction of tooth sensitivity while eating reported by the patient. She had never complained of sensitivity before because she has always had the same discomfort since her teeth erupted.
The morphological study of the two extracted molars presented in this article was part of the REGULAR FONDECYT project number 1140905, which was approved by the Ethics Committee of the Faculty of Dentistry at the University of Chile (Act No. 2013/06). The mutations of the patient were detected under research funded by INITIATION FONDECYT project number 11140440. Informed consent was obtained from all individual participants included in the study.
To detect mutations causing the disease, DNA from peripheral blood was isolated with a DNA extraction kit (Thermo Fisher Scientific, USA). The DNA was used as a template to amplify the exons of 16 genes related to EB. The resulting library was sequenced in the Ion PGM Sequencer (Life Technologies), and massive sequencing data were analyzed with Ion Reporter (Life Technologies Thermo Fisher, USA) software. To confirm the findings with massive sequencing, bidirectional Sanger sequencing was used. Finally, the pattern of recessive inheritance of both mutations found in the patient was confirmed by analyzing the genomic sequence of the parents and a healthy sister of the patient and was previously published in Fuentes I (12).
The two extracted molars were sent to the laboratory in 10% buffered formalin. The molar with the greatest amount of soft tissue adhered to the crown was decalcified for routine histopathology in 10% ethylene diamine tetra-acetic acid (EDTA) for 4 weeks, processed by routine histopathological technique, and stained with hematoxylin and eosin. The second tooth was segmented for ground section light microscopy and scanning electron microscopy (SEM). The ground sections were made in a Buehler cutting machine IsoMet® 1000, Illinois, USA. Cuts of 0.6 mm were obtained, which were then thinned with Arkansas stone to achieve samples smaller than 0.4 mm. The samples were dehydrated in ascending alcohols and xylol and mounted for histopathological examination. The histopathological study was performed using an optical microscope (Olympus CX 21, Japan) with traditional and polarized light.
For this study, the samples were fractured, washed in 7% EDTA to remove the smear layer, and dehydrated in ascending concentrations of alcohol. The preparation of samples was conducted in the electron microscopy laboratory of the Faculty of Medicine at the University of Chile (CESAT). These samples were analyzed with a Zeiss model DMS 940, German SEM.
The results of the analysis allowed the identification of two recessive mutations in LAMB3: c.957_958dup77 and c.3228+1G>A (NM_000228.2) as previously published in Fuentes I (12). The pedigree, chromatogram, and agarose gel electrophoresis are shown in Supplementary Figure 1 (Not shown in previous reports).
During the clinical examination of the patient, it was observed that the teeth had a very thin yellowish enamel. Clinically, soft tissue covered the crown of the lower first permanent molars, compatible with pulp polyp or hyperplastic gingiva (Figures 1A,B). Figure 1C shows the restored incisor teeth. Panoramic x-ray showed very thin, almost undetectable enamel. First mandibular molars presented partial coronal radiolucencies (Figure 1D).
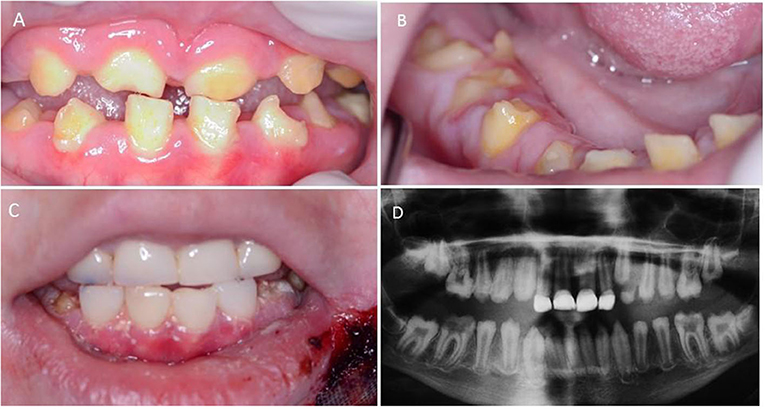
Figure 1. Clinical and radiographic images of a patient with amelogenesis imperfecta (AI) and junctional epidermolysis bullosa (JEB), with LAMB3 gene mutations. (A) Permanent incisors at 10 years of age in were thin, yellow-brown colored enamel is observed. (B) Lower right molar with soft tissue over the crown, premolars, and canine have partially erupted. (C) Incisors restored with ceramic crowns. (D) Panoramic radiograph, almost undetectable, very thin enamel throughout the dentition. Mandibular first molars with coronal radiolucencies and maxillary incisors rehabilitated with ceramic crowns.
In the ground sections of an affected molar, extremely thin enamel was observed, varying from complete absence to very thin enamel. The thicker enamel was adjacent to the root cementum zone while it was absent in some coronary cusp areas (Figures 2A,B). The enamel in the cervical area showed an absence of normal prismatic structure and the presence of a cross-banding with a laminated appearance compatible with cross-striations (Figure 3A, black arrow). Despite the marked thinness or absence of enamel, the dentin and cementum had a normal appearance (Figures 2A,B) except for the cementum at the apical level, which had an increased thickness (not shown). In contrast, control teeth presented an enamel more than 10 times thicker, with normal prisms (Figures 2C,D, 3C,D).

Figure 2. Molar ground section from a patient with AI and JEB visualized with light microscopy. (A) Photomicrograph with transmitted light of the coronary area of the permanent molar. (B) The same section was studied with polarized light. (C) Transmitted light photomicrograph of a permanent molar from a healthy control patient. (D) Healthy control molar visualized with polarized light. Original magnification ×4. E, Enamel; D, Dentin; C, Root cement.
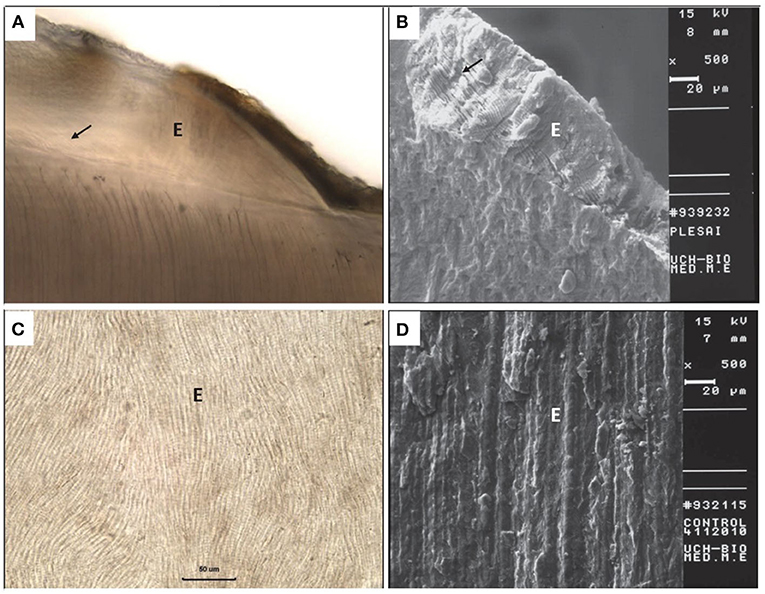
Figure 3. Optical microscopy and scanning electron microscopy (SEM) of a molar from the patient with AI and JEB and molar from a healthy control patient. (A) Ground section of a permanent molar from the patient with AI and JEB. In the cervical area, enamel bands semi-parallel to the dentin-enamel junction (black arrow) (×40) are observed. (B) SEM of a molar from the patient with AI and JEB. Cervical enamel, with transverse striations indicated by black arrows (×500). (C) Ground section of a permanent molar from a healthy control patient showing normal enamel prisms (×40). (D) SEM of a normal permanent molar (×500). E, Enamel.
In the demineralized segment treated with routine histopathological technique, crown and cervical dentin resorption were observed, with the presence of odontoclasts, apposition of cement-like material, and slight chronic inflammatory infiltrate in the resorption connective tissue (Figures 4A,B). Figures 4C,D show a normal permanent tooth.
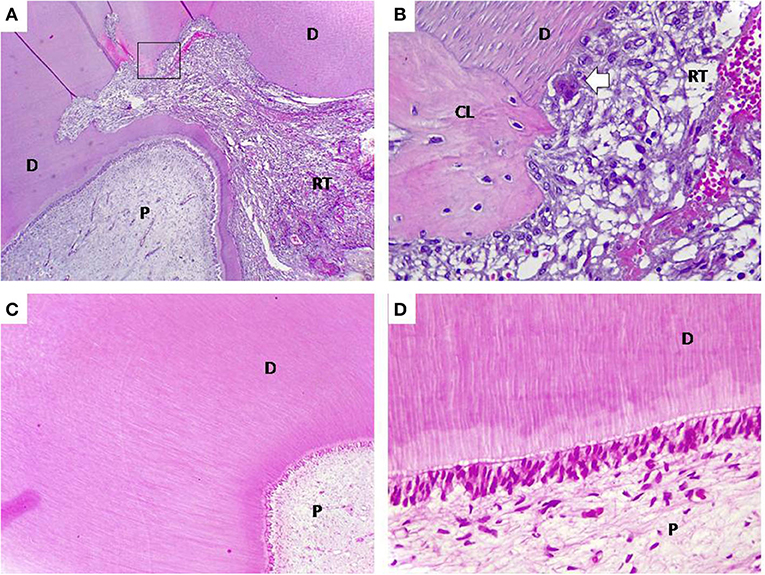
Figure 4. Routine histopathology of a demineralized molar from a patient with AI and JEB and molar from a control patient. (A) Dental crown area where pulp (P), dentin (D), and resorptive connective tissue (RT) are observed, (Original magnification 4×). (B) Magnification of the area of the rectangle in (A). Odontoclast (white arrow) and cement-like material (CL) (Original magnification ×40). (C) Control molar, note the continuity of the dentin around the pulp. (Original magnification ×4). (D) Control molar, note the presence and continuity of odontoblasts (Original magnification ×40) (Hematoxylin-eosin staining).
When analyzing the affected molars with SEM, the absence of enamel was observed in the cusp areas. In the cervical area, very thin enamel, up to 60 μm thick was measured. The cross-banding with a laminated appearance observed in the ground sections became more recognizable, with a width of 4 μm. The prisms remained undetectable (Figure 3B, black arrow). In the control teeth, the presence of normal prismatic structures was observed (Figure 3D).
Of the four types of EB recognized today, only patients with JEB presents significant alterations of the enamel structure (13). Among the defects of the dental structure, the most frequently reported are enamel hypoplasia, pits, and irregular surface (2, 13, 14). Other features described in patients with JEB are generalized failure of dental eruption and rarely resorption of unerupted teeth (15). Although dental resorption has been described in non-syndromic AI hypoplastic type associated with mutations of the AMELX, ENAM, or FAM20A genes (16–18) and syndromic types like enamel renal syndrome (19), to our knowledge, no histopathological and ultrastructural description of dental resorption has been reported in patients with JEB with LAMB3 gene recessive mutations.
Most cases of non-syndromic hypoplastic AI with coronary resorption have been described in non-erupted teeth and are asymptomatic (20). In the present case, the resorption occurred in a partially erupted molar and was associated with pain. It is most likely that the pain is due to the extreme thinness of the enamel since the dental resorptions are generally painless (21). Additionally, the anterior teeth were sensitive, which disappeared when covering them with crowns.
Although tooth resorptions have been reported in up to 41% of patients with AI (22), the reason for the occurrence of coronary resorptions in teeth with AI is unknown. It has been suggested that it can occur due to an alteration in the surface texture of the enamel (16), or poor recognition of self, causing the body to set up an autoimmune response to the teeth (20).
Wright et al. (13) studied teeth from patients with different forms of EB with SEM technique and found that teeth from patients with the severe, generalized form of JEB (formerly called the Herlitz type) had very thin enamel of ~40 μm thick. These changes were considered a direct consequence of genetic alterations in laminin-332 (13). Currently, it is known that JEB can be caused by mutations in the genes encoding laminin-332, type XVII collagen, and integrins (2). It is unclear whether mutations of these different genes involved in the structure of the lamina lucida generate ultrastructural differences in the enamel specific to each mutated gene.
In the present study, enamel was observed both in the clinical and microscopic examination as extremely thin or absent in some areas. The zone in which a greater amount of enamel was observed in ground sections was near the cementoenamel junction. Better preservation of enamel in the cementoenamel junction has been reported in other forms of AI (23, 24), and a protective role of the gingival fluid has been suggested.
When analyzing the structure of the affected enamel with SEM, absence of prisms, and the presence of laminar structure in the cervical area, semi-parallel to the surface of the dentin-enamel junction, exhibiting periodicity of ~4 μm were observed. In 2009, Antoine et al. (25) recorded a similar frequency of cross-striations in normal human teeth, so these laminar structures could correspond to these striations. To our knowledge, the presence of prominent cross-striations in the enamel has not been previously described in patients with JEB.
During odontogenesis, the three subunits of laminin-332 α3, β3, and γ2 are expressed in ameloblasts. In the presecretory and maturation stages, they are part of the basal lamina and pre-ameloblasts and disappear at the early bell stage. Therefore, it has been suggested that laminin-332 would play an important role in differentiating ameloblasts (26).
The presence of severe hypoplastic enamel abnormalities as a manifestation of AI should alert dentists, and ideally, mutation analysis of the genes encoding proteins of the lamina lucida should be carried out. Murrell et al. (27) reported a family in which two children died before the first year of life with the development of multiple bullae on the skin. When studying the parents and the older brother of these children, it was found that the parents and the living child had heterozygous mutations in the COL17A1 gene in addition to the presence of AI. Both parents presented pits on their teeth and the brother presented white spots on the teeth, none of them had skin changes. Thus, a retrospective diagnosis of JEB in the two deceased children was carried out (27). Moreover, Pasmooj et al. reported a genotype-phenotype correlation analysis performed in 12 patients with JEB who were deficient in collagen XVII. The DNA analysis showed five different deletions. These patients had phenotypes ranging from very mild to severe forms of bullae in the skin and mucous membranes, accompanied by alopecia and nail dystrophy. Despite the different expressions of lesions on the skin, mucous membranes, and nails, AI was observed in all 12 patients (28).
Although the literature has described patients with this type of enamel as having a high tendency to develop caries (7), the patient, in this case, remained without decay until the age of 13, when she passed away. The main dental problems of the patient were tooth sensitivity, aesthetic changes, attrition, and occlusal alterations due to very thin enamel and crown resorption. Almost all the features listed were successfully managed when complete crown treatment was performed at the age of 10.
It is of utmost importance that patients with this condition are looked after by a multidisciplinary medical and dental team, to manage timely each complication that can arise, thus offering them a better oral health-related quality of life. The preventive approach allowed this patient to remain free from decay throughout her life, and rehabilitation based on the crowns solved her tooth sensitivity. Suggestions for the dental management of patients with EB can be found in the Clinical Guidelines published in 2020 (5).
As this is a case report of a very rare condition, its main limitation is that it is not possible to know whether coronary resorption occurs in all patients with AI associated with JEB. We hope that new reports will provide more information and complement the guidelines for the care of these patients.
To conclude, this is the first report of coronary resorption in partially erupted teeth in patients with JEB with mutations in the LAMB3 gene and hypoplastic AI. In patients with this condition, the presence of partially erupted teeth with soft tissue covering part of the crown, without a periodontal pocket, and with a radiographic image of a partial crown radiolucency should lead to suspicion of coronary resorption. In addition to the skin and mucous membrane bullae, patients with this disorder have teeth defects, such as an extremely thin enamel and absence of prismatic structure. In this patient, conservative treatment based on education, prevention, and restorations with dental crowns reduced tooth sensitivity and improved oral health-related quality of life.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving human participants were reviewed and approved by Comite de Etica, School Dentistry, and University of Chile for the INITIATION FONDECYT project no. 11140440. The study was reviewed and approved by the Ethics Committee at Facultad de Odontologia, Universidad de Chile. Written informed consent to present this case description and clinical images was provided by the participant's legal guardian.
AO-P and BU helped with drafting and critical analysis of the general article. SK helped with clinical dental evaluation, prevention and treatment, and analyzed clinical dental data. AO-P and CC helped with histopathological and ultrastructural analysis. BU and IM-B performed the critical analysis of the article regarding amelogenesis imperfecta (AI). MY, FP, and IF performed analysis of LAMB3 gene mutations. IF performed the critical analysis of the article regarding epidermolysis bullosa (EB). All authors contributed to the article and approved the submitted version.
This study was supported by the REGULAR FONDECYT project no.1140905 for morphological study of the teeth and the INITIATION FONDECYT project no. 11140440 for genetic study of mutation of LAMB3.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
We acknowledge the support from the Dental School of the University of Chile, the DEBRA foundation, and Clinica Alemana, Santiago-Chile.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fdmed.2021.704423/full#supplementary-material
1. Atar M, Korperich E. Systemic disorders and their influence on the development of dental hard tissue: a literature review. J Dentistry. (2010) 38:296–306. doi: 10.1016/j.jdent.2009.12.001
2. Has C, Bauer JW, Bodemer C, Bolling MC, Bruckner-Tuderman L, Diem A, et al. Consensus reclassification of inherited epidermolysis bullosa and other disorders with skin fragility. Br J Dermatol. (2020) 183:614–27. doi: 10.1111/bjd.18921
3. Kiritsi D, Has C, Bruckner-Tuderman L. Laminin 332 in junctional epidermolysis bullosa. Cell Adh Migr. (2013) 7:135–41. doi: 10.4161/cam.22418
4. Yuen WY, Pasmooij AM, Stellingsma C, Jonkman MF. Enamel defects in carriers of a novel LAMA3 mutation underlying epidermolysis bullosa. Acta Derm Venereol. (2012) 92:695–6. doi: 10.2340/00015555-1341
5. Krämer S, Lucas J, Gamboa F, Peñarrocha Diago M, Peñarrocha Oltra D, Guzmán-Letelier M, et al. Clinical practice guidelines: oral health care for children and adults living with epidermolysis bullosa. Spec Care Dentist. (2020) 40(Suppl. 1):3–81. doi: 10.1111/scd.12511
6. Farooq M, Kurban M, Iguchi R, Abbas O, Fujimoto A, Fujikawa H, et al. Genetic analysis of epidermolysis bullosa: Identification of mutations in LAMB3 and COL7A1 genes in three families. J Dermatol Sci. (2013) 72:61–77. doi: 10.1016/j.jdermsci.2013.05.002
7. Sadler E, Laimer M, Diem A, Klausegger A, Pohla-Gubo G, Muss W, et al. Dental alterations in junctional epidermolysis bullosa-report of a patient with a mutation in the LAMB3-gene. J Dtsch Dermatol Ges. (2005) 3:359–63. doi: 10.1111/j.1610-0387.2005.05703.x
8. Lee K-E, Ko J, Le CGT, Shin TJ, Hyun H-K, Lee S-H, et al. Novel LAMB3 mutations cause non-syndromic amelogenesis imperfecta with variable expressivity. Clin Genet. (2015) 87:90–2. doi: 10.1111/cge.12340
9. Poulter JA, El-Sayed W, Shore RC, Kirkham J, Inglehearn CF, Mighell AJ. Whole-exome sequencing, without prior linkage, identifies a mutation in LAMB3 as a cause of dominant hypoplastic amelogenesis imperfecta. Eur J Hum Genet. (2014) 22:132–5. doi: 10.1038/ejhg.2013.76
10. Kim JW, Seymen F, Lee KE, Ko J, Yildirim M, Tuna EB, et al. LAMB3 mutations causing autosomal-dominant amelogenesis imperfecta. J Dent Res. (2013) 92:899–4. doi: 10.1177/0022034513502054
11. Almaani N, Liu L, Dopping-Hepenstal PJ, Lovell PA, Lai-Cheong JE, Graham RM, et al. Autosomal dominant junctional epidermolysis bullosa. Br J Dermatol. (2009) 160:1094–7. doi: 10.1111/j.1365-2133.2008.08977.x
12. Fuentes I, Campos M, Repetto G, Morandé P, Yubero MJ, Gonzalez S, et al. Molecular epidemiology of junctional epidermolysis bullosa: discovery of novel and frequent LAMB3 mutations in Chilean patients with diagnostic significance. Br J Dermatol. (2017) 176:1090–2. doi: 10.1111/bjd.14920
13. Wright JT, Hall KI, Deaton TG, Fine JD. Structural and compositional alteration of tooth enamel in hereditary epidermolysis bullosa. Connect Tissue Res. (1996) 34:271–9. doi: 10.3109/03008209609005271
14. Wright JT, Johnson LB, Fine JD. Developmental defects of enamel in humans with hereditary epidermolysis bullosa. Arch Oral Biol. (1993) 38:945–55. doi: 10.1016/0003-9969(93)90107-W
15. Brooks JK, Bare LC, Davidson J, Taylor LS, Wright JT. Junctional epidermolysis bullosa associated with hypoplastic enamel and pervasive failure of tooth eruption: oral rehabilitation with use of an overdenture. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. (2008) 105:e24–e8. doi: 10.1016/j.tripleo.2007.12.038
16. Lee KE, Lee SK, Jung SE, Song SJ, Cho SH, Lee ZH, et al. A novel mutation in the AMELX gene and multiple crown resorptions. Eur J Oral Sci. (2011) 119:324–8. doi: 10.1111/j.1600-0722.2011.00858.x
17. Lindemeyer RG, Gibson CW, Wright TJ. Amelogenesis imperfecta due to a mutation of the enamelin gene: clinical case with genotype-phenotype correlations. Pediatr Dent. (2010) 32:56–60.
18. Wang X, Zhao Y, Yang Y, Qin M. Novel ENAM and LAMB3 mutations in Chinese families with hypoplastic amelogenesis imperfecta. PLoS One. (2015) 10:e0116514. doi: 10.1371/journal.pone.0116514
19. Wang SK, Aref P, Hu Y, Milkovich RN, Simmer JP, El-Khateeb M, et al. FAM20A mutations can cause enamel-renal syndrome (ERS). PLoS Genet. (2013) 9:e1003302. doi: 10.1371/journal.pgen.1003302
20. Korbmacher HM, Lemke R, Kahl-Nieke B. Progressive pre-eruptive crown resorption in autosomal recessive generalized hypoplastic amelogenesis imperfecta. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. (2007) 104:540–4. doi: 10.1016/j.tripleo.2006.08.022
21. Patel S, Kanagasingam S, Ford TP. External cervical resorption: a review. J Endod. (2009) 35:616–25. doi: 10.1016/j.joen.2009.01.015
22. Collins MA1, Mauriello SM, Tyndall DA, Wright JT. Dental anomalies associated with amelogenesis imperfecta: a radiographic assessment. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. (1999) 88:358–64. doi: 10.1016/S1079-2104(99)70043-0
23. Seymen F, Lee KE, Koruyucu M, Gencay K, Bayram M, Tuna EB, et al. Novel ITGB6 mutation in autosomal recessive amelogenesis imperfecta. Oral Dis. (2015) 21:456–61. doi: 10.1111/odi.12303
24. Urzúa B, Martínez C, Ortega-Pinto A, Adorno D, Morales-Bozo I, Riadi G, et al. Novel missense mutation of the FAM83H gene causes retention of amelogenin and a mild clinical phenotype of hypocalcified enamel. Arch Oral Biol. (2015) 60:1356–67. doi: 10.1016/j.archoralbio.2015.06.016
25. Antoine D, Hillson S, Dean C. The developmental clock of dental enamel: a test for the periodicity of prism cross-striations in modern humans and an evaluation of the most likely sources of error in histological studies of this kind. J Anat. (2009) 214:45–55. doi: 10.1111/j.1469-7580.2008.01010.x
26. Yoshiba K, Yoshiba N, Aberdam D, Meneguzzi G, Perrin-Schmitt F, Stoetzel C, et al. Expression and localization of laminin-5 subunits during mouse tooth development. Dev Dyn. (1998) 211:164–76. doi: 10.1002/(SICI)1097-0177(199802)211:2<164::AID-AJA5>3.0.CO;2-F
27. Murrell DF, Pasmooij AM, Pas HH, Marr P, Klingberg S, Pfendner E, et al. Retrospective diagnosis of fatal BP180-deficient Non-Herlitz Junctional Epidermolysis Bullosa suggested by immunofluorescence (IF) antigen-mapping of parental carriers bearing enamel defects. J Invest Dermatol. (2007) 127:1772–5. doi: 10.1038/sj.jid.5700766
Keywords: amelogenesis imperfecta, junctional epidermolysis bullosa, crown resorption, laminin-332, rehabilitation of teeth, bullous genetic disease
Citation: Urzúa B, Krämer S, Morales-Bozo I, Camacho C, Yubero MJ, Palisson F, Fuentes I and Ortega-Pinto A (2021) Case Report: Crown Resorption in a Patient With Junctional Epidermolysis Bullosa and Amelogenesis Imperfecta With LAMB3 Gene Mutations. Front. Dent. Med. 2:704423. doi: 10.3389/fdmed.2021.704423
Received: 02 May 2021; Accepted: 17 June 2021;
Published: 09 August 2021.
Edited by:
Mine Koruyucu, Istanbul University, TurkeyReviewed by:
Merve Bayram, Istanbul Medipol University, TurkeyCopyright © 2021 Urzúa, Krämer, Morales-Bozo, Camacho, Yubero, Palisson, Fuentes and Ortega-Pinto. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Ortega-Pinto, YW9ydGVnYUBvZG9udG9sb2dpYS51Y2hpbGUuY2w=
†These authors share first authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.