
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Dent. Med. , 28 April 2021
Sec. Pediatric Dentistry
Volume 2 - 2021 | https://doi.org/10.3389/fdmed.2021.670948
This article is part of the Research Topic Women in Pediatric Dentistry: 2021 View all 6 articles
 Alexandre Rezende Vieira1,2*
Alexandre Rezende Vieira1,2* Paulo Germano Cavalcanti Furtado3Valdécio Vasconcelos Lacerda Filho3Jéssica Amorim Teotônio Pereira3Isabelle Silvério Tenório3André Macedo Luna3Vitor Marques Filgueiras3
Paulo Germano Cavalcanti Furtado3Valdécio Vasconcelos Lacerda Filho3Jéssica Amorim Teotônio Pereira3Isabelle Silvério Tenório3André Macedo Luna3Vitor Marques Filgueiras3 Rosa Helena Wanderley Lacerda2,3
Rosa Helena Wanderley Lacerda2,3Objective: Cleft lip and/or palate is the most common congenital anomaly in a human face, with a multifactorial and complex etiology. Although many studies have been developed, the role of the environment is still unclear. This study aims to test the hypothesis that differences in lifestyle and environment change the reproductive risks of orofacial clefts.
Methods: A total of 2,422 medical records of individuals born with cleft lip and/or palate in a reference center in the northeast of Brazil over a period of 30 years were analyzed. Data on the cleft type, geographic origin of the patient (coast or inland), presence of associated congenital anomalies or syndromes, maternal age, and maternal parity were recorded. Differences in frequencies between the cleft types were compared based on geographic origin, maternal age, and parity. Chi-square, Student's t, Kruskal–Wallis, and logistic regression were used to analyze the interference of covariables on the cleft type.
Results: The distribution of cleft types was significantly different between the coastal and inland areas (chi-square test, p < 0.0001). A higher frequency of cleft lip with or without palate was observed the inland area (chi-square test, p = 0.0006), while cleft palate only (chi-square test, p = 0.003) and rare facial clefts (chi-square test, p = 0.004) were more frequent in the coastal area. No difference was found in the distribution of maternal age (t-test, p > 0.05) between the two geographic areas, but parity was higher inland (t-test, p = 0.04). Logistic regression suggested that parity explained just a small portion of the differences in frequency between cleft types of the coast vs. inland.
Conclusion: Frequency of orofacial cleft types differs by geographic area in this region of the South American continent.
Cleft lip and/or palate is the most common congenital anomaly affecting a human face. The etiology is multifactorial with a polygenic genetic model with influence of environmental factors (1).
The role of the environment is still unclear, even though maternal smoking (1) and antiepileptic drugs are associated with increased cleft lip and palate risk (2). Stress and nutritional deficiency related to hunger are variables we hypothesize that may also contribute to orofacial cleft formation.
Oral clefts are historically subdivided into cleft lip with or without cleft palate and cleft palate only based on genetic and biological grounds (2–4). Few studies analyzed the impact of the environment on gene function in different cleft types (5).
The opportunity to study the impact of the environment on gene function that modifies the risk for orofacial clefts exists in the northeast of Brazil, where water shortage is frequent. A cleft treatment reference center serving the area is the perfect opportunity to test the hypothesis that living inland changes the reproductive risks of orofacial clefts in comparison with the coast, where access to water and food is uninterrupted. Individuals living inland are of lower family income and frequently experience drought and food shortages. Individuals living in the capital by the sea where there is a higher demographic density can be assumed to be under non-specific stress conditions (6). These two areas have differences in access to medical care and lifestyle, and we hypothesize that these differences may impact the frequency of orofacial clefts. Here, we report differences in frequency of types of clefts depending on being born inland vs. at the coast.
This study was conducted with 2,422 medical records of patients treated at Lauro Wanderley University Hospital Cleft Lip and Palate Center, a reference center at the northeast of Brazil. Medical records comprised all cases treated from January 1991 to July 2020. Data on cleft type, geographic origin of the patient (coast or inland), presence of associated congenital anomalies or syndromes, maternal age, maternal parity, consanguinity, and maternal smoking during pregnancy were recorded.
This study was reviewed and approved by the local Institutional Ethics Board (Lauro Wanderley Hospital Ethics Committee approval #1.335.087).
Data were compiled into the Jamovi 1.2 computer software (7). Cleft type was defined as cleft lip with or without palate, cleft palate only, and rare forms of cleft, based on embryologic grounds and clinical presentations. Syndromic cases were recorded and analyzed separately. The geographic origin was divided into two main ones: coast and inland.
Differences in frequencies between the cleft types were compared based on geographic origin, maternal age, and parity; and chi-square, Student's t, Kruskal–Wallis, and logistic regression were used to analyze the interference of covariables on the cleft type. Information on consanguinity and maternal smoking was missing in 50% of the records, and these variables were not studied here.
From the 2,422 cases, 2,335 were isolated and 87 syndromic. As expected, more males were found with cleft lip and palate (female:male ratio of 1:1.45) and more females with cleft palate only (female:male ratio of 1.34:1) and rare types of clefts (ratio of 16:1) (Table 1).

Table 1. Distribution of orofacial clefts according to type and sex.
Figure 1 describes the distribution of orofacial clefts according to type and geographic origin. Cleft palate only and rare forms of cleft were found more often at the coastline, and cleft lip with or without cleft palate was more frequent inland.
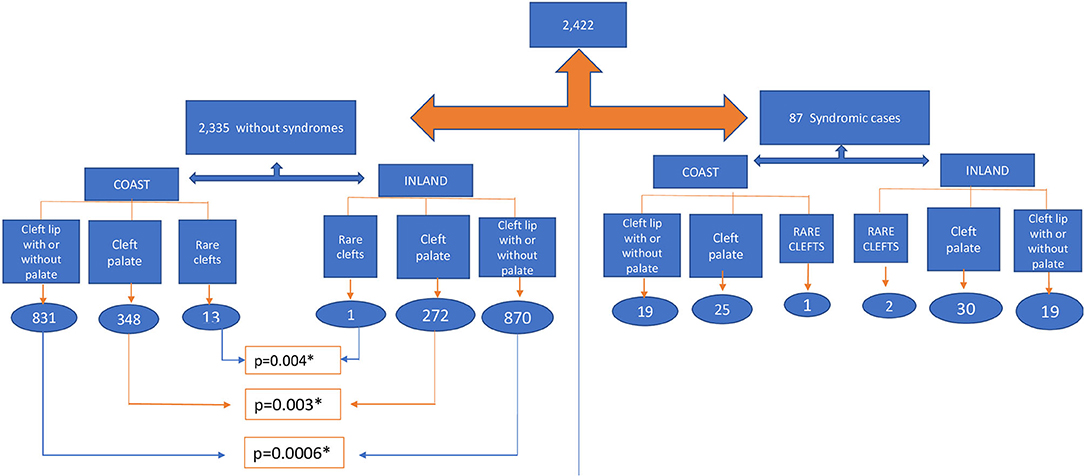
Figure 1. Distribution of orofacial clefts according to type and geogaphic origin. *indicate statistically significant difference.
No difference was found in the distribution of maternal age between the two geographic origins, but parity was higher inland (Table 2). Figure 2 shows more children with higher parity inland. Logistic regression suggested that parity explained just a small portion of the differences in frequency between cleft types in the coast vs. inland (Figure 3).
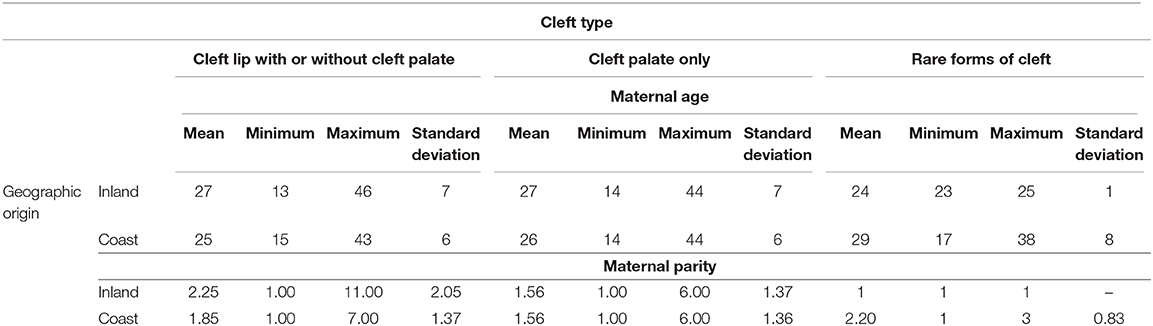
Table 2. Distribution of maternal age, maternal parity, according to geographic origin, and cleft type.
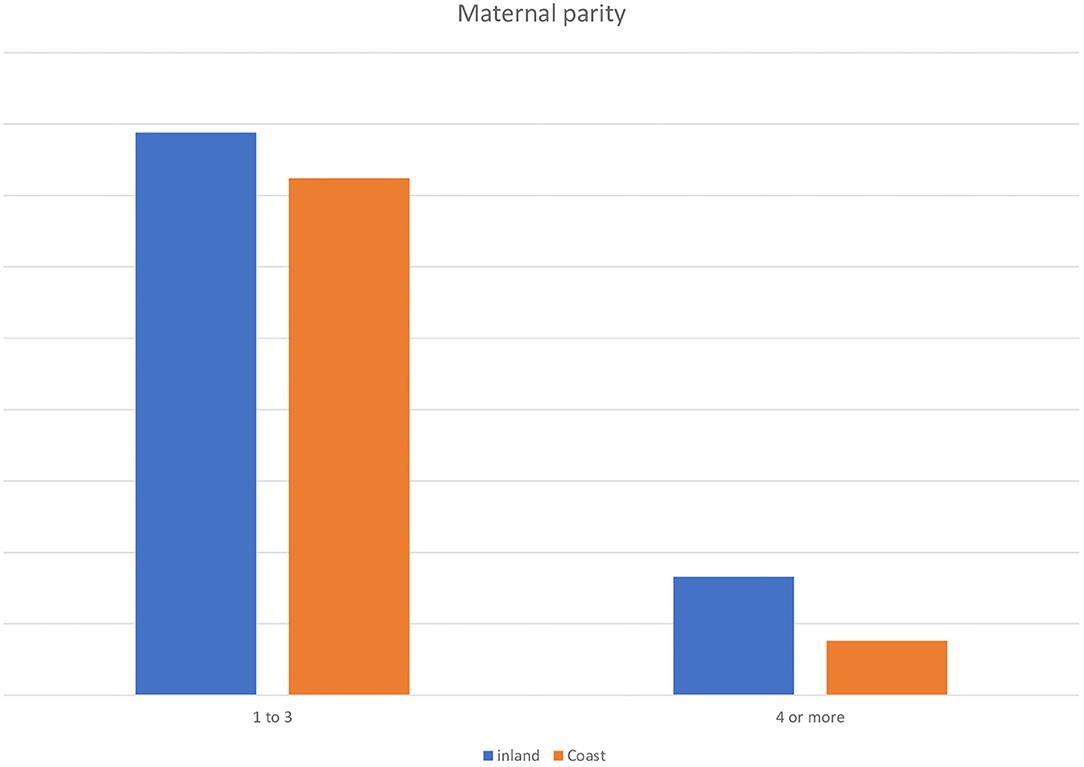
Figure 2. Parity 4 or higher was more frequent inland in comparison with the coast in children born with orofacial clefts.
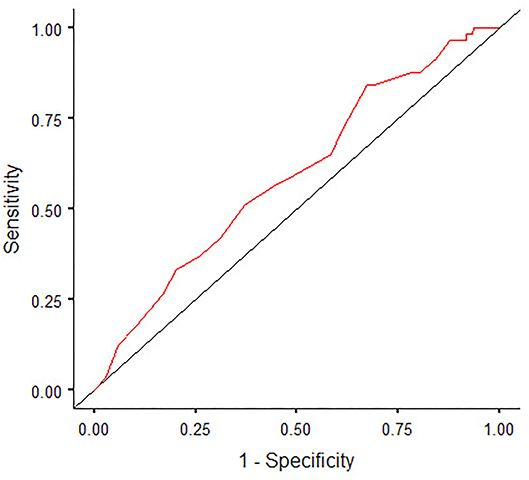
Figure 3. Receiver operating characteristic (ROC) curve logistic regression model for cleft type considering, maternal parity, sex, and geographic origin.
The complex etiology of orofacial clefts has been studied for decades. There is a consensus that it has a multifactorial mode of inheritance with contributions from more than one gene and environmental factors (1, 2).
The overall breakdown of cleft types found in the present study was what was expected: 71% of the sample had cleft lip with or without palate, and 28% had cleft palate only (8–10). The distribution by sex was also within the expected proportions (10, 11). Rare clefts showed a much higher frequency in females (16 out of 17). For those instances, it appears that the development of the male sex protects against disturbances that lead to rare facial cleft forms. The expression of the testis-determining factor (TDF), beginning at around the sixth week of gestation, may be this protective factor. A molecular cascade of events follow, with the activation of the sex region of the Y chromosome (SRY) right after the expression of steroidogenic factor 1 (SF1). SRY raises SF-1 and SOX9 gene activity, leading to male differentiation and activation of the anti-Müllerian hormone (AMH) gene (12). These events are occurring at the same time that the face is developing.
The evidence of remarkable differences in lifestyle and environment between the coastal and inland regions (Figure 4) motivated to stratify frequencies of cleft types by geographic region, which are known to affect the etiology of the cleft (1, 2, 13). The distribution of cleft types was significantly different between the regions (chi-square test, p < 0.0001). Inland, there was a higher frequency of cleft lip with or without palate (chi-square test, p = 0.0006), while cleft palate only (chi-square test, p = 0.003) and rare facial clefts (chi-square test, p = 0.004) were more frequent in the coastal area (Figure 1). Previously, we have shown that older maternal age did not associate with oral clefts, but higher parity did (14, 15). In the present data, it was more likely for the child to have higher parity if she or he was born inland; however, parity appeared to explain very little of the difference between frequencies of inland vs. coastal areas. We hypothesize that the distinct frequencies of cleft types by geographic area in this region might be due to genetic differences, including differences in the control of gene expression that may be influenced by the environment. These differences in cleft type incidence depending on geographic region may exist in other parts of the world. In Egypt, Luxor appeared to have more cases of cleft lip only and no cleft palate only than Cairo (16). In Iran, the incidence of cleft lip and palate, but not the other cleft types, was increased between 2002 and 2011, in comparison with 1982 and 2001 (17). These data are from the northeast of Iran, where the city of Mashhad is. Mashhad has had an accelerated growth since the early 2000s, a factor that widened social gap and made the city particularly prone to slum proliferation; and the population in marginal neighborhoods has limited access to hospital care, pharmacy, and stable jobs and is required to have long commute times (18).
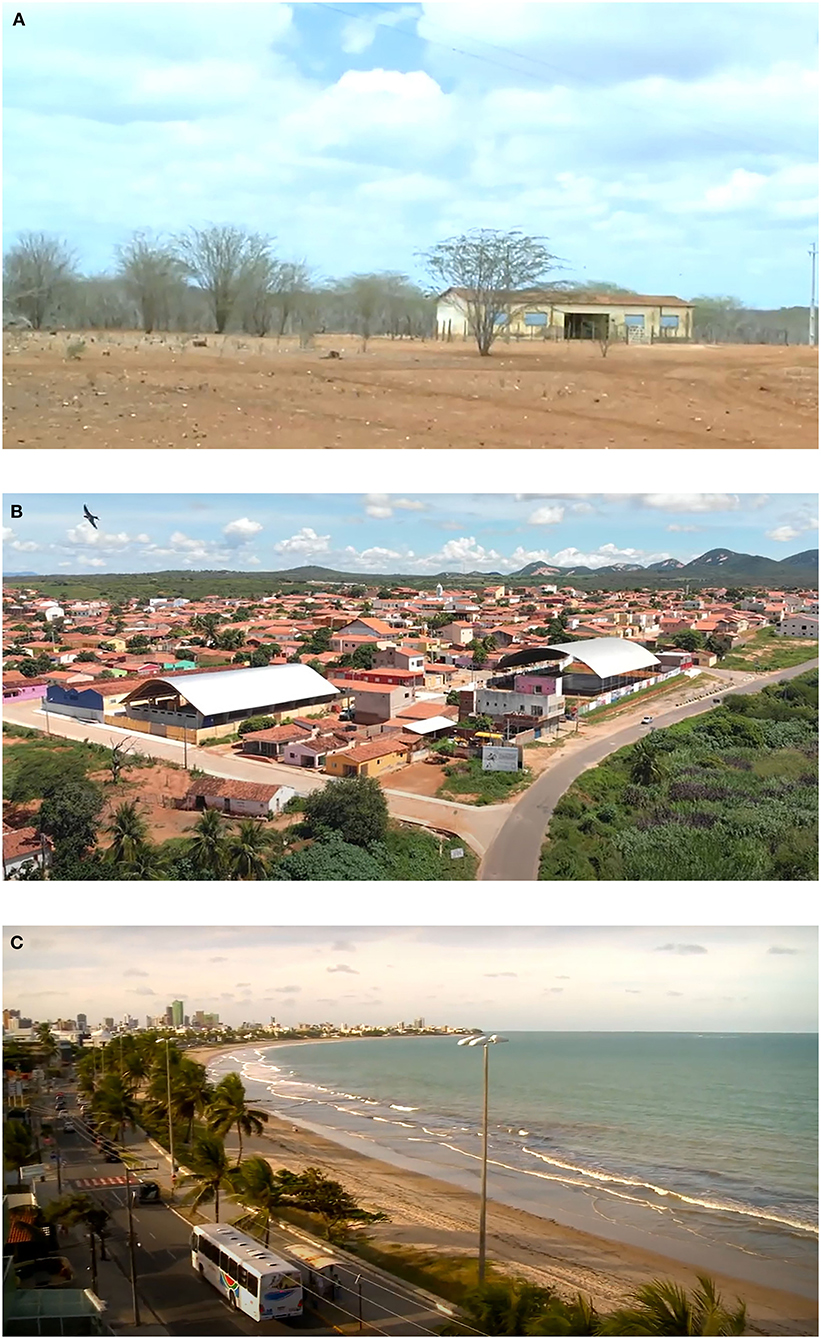
Figure 4. Examples of living conditions of families included in the study. Inland areas vary from (A) isolated households in the drylands to (B) small size cities. (C) The coastal city, which is larger and more afluent.
The study was done in a specific geographic area that corresponds to one state of a country, and this can be perceived as a limitation, since the results may not be generalizable to other parts of the continent or other continents. However, the evaluation presented here corresponds to data collected over a period of 30 years and represents the population of a specific geographic area. In that sense, these population-based results are the true representation of the state in question. In conclusion, there were differences in the expected frequencies of types of cleft lip and palate when coastal and inland areas were compared. Future studies will focus on possible gene–environmental mechanisms that might explain these differences.
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by Lauro Wanderley Hospital Ethics Committee approval # 1.335.087. Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
RL, VLF, VF, JP, IT, and AL obtained the data. PF and RL critically revised the manuscript. AV proposed the concept and design, interpreted and analyzed data, and wrote the first draft of the manuscript. All authors contributed to the article and approved the submitted version.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors are indebted to the participants of the study and to Smile Train, which supports cleft care.
1. Vieira AR. Genetic and environmental factors in human cleft lip and palate. Front Oral Biol. (2012) 16:19–31. doi: 10.1159/000337521
2. Dixon MJ, Marazita ML, Beaty TH, and Murray JC. Cleft lip and palate: synthesizing genetic and environmental influences. Nat Rev Genet. (2011) 12:167–78. doi: 10.1038/nrg2933
3. Fogh-Andersen P. Inheritance of Harelip and Cleft Palate: contribution to the elucidation of the etiology of the congenital clefts of the face (dissertation/master's thesis). Københavns universitet, Copenhagen, Denmark (1942).
4. Vieira-Machado CD, de Carvalho FM, Santana da Silva LC, Dos Santos SE, Martins C, Poletta FA, et al. Analysis of the genetic ancestry of patients with oral clefts from South American admixed populations. Eur J Oral Sci. (2016) 124:406–11. doi: 10.1111/eos.12275
5. Sharp GC, Ho K, Davies A, Stergiakouli E, Humpries K, McArdle W, et al. Distinct DNA methylation profiles in subtypes of orofacial cleft. Clin Epigenetics. (2017) 9:63. doi: 10.1186/s13148-017-0362-2
6. IBGE, Diretoria de Pesquisas C de P e IS. Estimativas da população residente com data de referência 1o de julho de. Paraíba (2019).
7. Anon N. The Jamovi Project. jamovi. (Version 1.2) [Computer Software] (2020). Available online at: https://www.jamovi.org.o Title.
8. Lofredo LCM, Freitas JAS, and Grigolli AAG. Prevalence of oral clefts from 1975 to 1994, Brazil. Rev Saúde Pública. (2001) 35:571–5. doi: 10.1590/S0034-89102001000600011
9. Moreira HSB, Machado RA, Aquino SN, Carrinho AL, Rangel A, Martelli-Junior H, et al. Epidemiological features of patients with nonsyndromic cleft lip and/or palate in Western Paraná. Braz J Oral Sci. (2016) 15:39–44. doi: 10.20396/bjos.v15i1.8647121
10. Freitas JAS, Dalben GS, Santamaria Júnior M, and Freitas PZ. Current data on the characterization of oral clefts in Brazil. Braz Oral Res. (2004) 18:128–33. doi: 10.1590/S1806-83242004000200007
11. Rodrigues K, Sena MF, Roncalli AG, and Ferreira MAF. Prevalence of orofacial clefts and social factors in Brazil. Braz Oral Res. (2009) 23:38–42. doi: 10.1590/S1806-83242009000100007
12. Karkanaki A, Praras N, Katsikis I, Kita M, and Panidis D. Is the Y chromosome all that is required for sex determination? Hippokratia. (2007) 11:120–3.
13. Leite ICG, and Koifman S. Oral clefts, consanguinity, parental tobacco and alcohol use: a case-control study in Rio de Janeiro, Brazil. Braz Oral Res. (2009) 23:31–7. doi: 10.1590/S1806-83242009000100006
14. Vieira AR, Orioli IM, and Murray JC. Maternal age and oral clefts: a reappraisal. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. (2002) 94:530–5. doi: 10.1067/moe.2002.128875
15. Vieira AR, and Orioli IM. Birth order and oral clefts: a meta analysis. Teratology. (2002) 66:209–16. doi: 10.1002/tera.10088
16. Alswairki HJR, El-Sayed FAA, Fouda MY, Fahim FH, Haque S, and Alam MK. Incidence of Egyptian live births of cleft lip and/or palate in Cairo, Luxor, Aswan and New Valley governorates: a survey study in 237,783 children. Pesqui Bras Odontopediatria Clín Integr. (2019) 19:e4695. doi: 10.4034/PBOCI.2019.191.100
17. Kianifar H, Hasanzadeh N, Jahanbin A, Ezzati A, and Kianifar H. Cleft lip nd palate: a 30-year epidemiologic study in north-east of Iran. Iran J Otorhinolaryngol. (2015) 27:35–41.
18. Hoad P. Mashhad in the spotlight: inequality plagues Iran's holy city. The Guardian. (2018). Available online at: https://www.theguardian.com/cities/2018/jan/22/mashhad-spotlight-rising-inequality-iran-holy-city-imam-reza-shrine~
Keywords: cleft lip and palate, orofacial clefts, etiology, lifestyle, environment
Citation: Vieira AR, Furtado PGC, Filho VVL, Pereira JAT, Tenório IS, Luna AM, Filgueiras VM and Lacerda RHW (2021) Orofacial Cleft Frequency Differences Depending on Geographic Origin: Coast vs. Inland. Front. Dent. Med. 2:670948. doi: 10.3389/fdmed.2021.670948
Received: 22 February 2021; Accepted: 17 March 2021;
Published: 28 April 2021.
Edited by:
Sreekanth Kumar Mallineni, Majmaah University, Saudi ArabiaReviewed by:
Sivakumar Nuvvula, Narayana Dental College and Hospital, IndiaCopyright © 2021 Vieira, Furtado, Filho, Pereira, Tenório, Luna, Filgueiras and Lacerda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexandre Rezende Vieira, YXJ2MTFAcGl0dC5lZHU=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.