 Aline dos Santos Letieri1
Aline dos Santos Letieri1 Liana Bastos Freitas-Fernandes1Lourenço Luís Albarello1Gabriela Pereira Fontes1Ivete Pomarico Ribeiro de Souza1
Liana Bastos Freitas-Fernandes1Lourenço Luís Albarello1Gabriela Pereira Fontes1Ivete Pomarico Ribeiro de Souza1 Ana Paula Valente2
Ana Paula Valente2 Tatiana Kelly da Silva Fidalgo3*
Tatiana Kelly da Silva Fidalgo3*- 1Department of Pediatric Dentistry and Orthodontics, School of Dentistry, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil
- 2National Center for Nuclear Magnetic Resonance, Medical Biochemistry, Universidade Federal do Rio de Janeiro, Rio de Janeiro, Brazil
- 3Department of Preventive and Community Dentistry, Universidade do Estado do Rio de Janeiro, Rio de Janeiro, Brazil
The aim of the present study was to verify if a protocol for cleaning the oral cavity of infants in the pre-dental period can reduce extrinsic salivary metabolites observed through Nuclear Magnetic Resonance (NMR). A cross-sectional clinical study with a convenience sample was conducted, and infants were recruited at the UFRJ Pediatric Dentistry Clinic. Participants who had used antibiotics and/or antifungals up to 3 months before and whose legal guardians did not consent or sign the Informed Consent Form were excluded. An anamnesis was performed with the guardians and the participants' intraoral clinical examination. Initial collection of unstimulated total saliva was performed using an automatic pipette with sterile plastic tips in the buccal floor region, at least 1 h after the last feeding. Subsequently, the infants' oral mucosa was cleaned with gauze moistened with filtered water, and after 5 min, a new collection was performed, using the same methodology. The obtained samples were immediately transferred on ice to the laboratory, centrifuged (10,000 g), and stored at −80°C. The NMR analyses were performed using a 500-MHz spectrometer Bruker, Germany); evaluations were done via the 1H and 1H-1H TOCSY spectra for metabolite signaling. Eleven pre-dental infants were evaluated, with a mean age of 3.8 months, including six girls (55%). Of these, nine participants (82%) were exclusively breastfed. The higher presence of components such as lactose, glucose, sugars, acetate, alanine, and lactate were observed in the samples before oral mucosa cleaning. Regarding the type of diet, more lactose was observed in the saliva of patients who were exclusively breastfed than those that received mixed feeding. We conclude that the oral mucosa cleaning of infants in the pre-dental period tends to reduce the concentration of extrinsic components from the diet, such as lactose, in the salivary metabolomic profile analyzed by NMR.
Introduction
Saliva is a highly complex biofluid, produced by the secretion of the major and minor salivary glands, the gingival crevicular fluid, residual food, and microorganisms and their metabolic products, presenting a wide spectrum of biological compounds with informative capacity. Its composition and functions, such as the regulatory mechanisms of the oral microbiota, are extremely important for the maintenance of oral homeostasis (1).
Therefore, salivary studies have been expanding over the years, mainly due to the use of new approaches, as well as studies highlighting new technologies for biomolecule identification (2). Among them, the metabolomics approach consists of the quantitative and qualitative evaluation of the metabolites that are the low-molecular-weight compounds in biofluids. The metabolites are classified as intrinsic when they are produced by the cellular metabolism of body itself or extrinsic, which are substances foreign to biological samples, such as drugs or products resulting from the microorganisms' metabolism (3). Regarding the biofluids, researches on the evaluation of salivary samples are of fundamental relevance, since saliva is an important and promising vehicle for early diagnosis, preventive use, and even for the identification of biomarkers for local and systemic diseases, mainly due the advantages of presenting simple and non-invasive forms of collection and because of sufficient precision when compared to traditional methods (4, 5).
In addition, the salivary metabolomic analysis proves to be extremely important not only in dentistry, but also in general medicine (6, 7). Based on its evaluation, it is possible to detect alterations caused by different systemic diseases, such as Sjögren's syndrome (8) and diabetes mellitus (9), as well as local alterations such as different types of oral cancer (10, 11), dental caries (12), and periodontal disease (13–15).
During the first years of life, significant physiological changes occur, which can influence the salivary composition. For this reason, saliva profile studies in this this period are important to determine the salivary fingerprint during these physiological modifications. Eighteen of the main salivary metabolites present in samples of participants in the pre-dental period have already been identified, including 3-Hydroxybutyric acid, Valeric acid, D-Glucose, D-Lactose, D-Maltose (16). The pre-dental period consists of the moment when there is still no eruption of any primary teeth and goes from birth to approximately 6 months of age. Over time, a significant change in the salivary metabolic profile is observed. These modifications that occur throughout childhood seems to be related to the eruption of primary teeth, salivary glands maturation, food transition and oral microbial changes. The increase with time of succinic, malic, and pyruvic acids may reflect an increase in the metabolism of the oral microbiota since these compounds are products of cellular metabolism (16).
Teeth eruption and diet changes substantially modify the salivary proteome profiles of infants between 3 and 6 months of age (17). On the other hand, no significant differences in the profile of salivary metabolites were observed according to the feeding history during the first months of life (16). In both studies, infant saliva was collected using the same commercial device (Salivette®, Sarstedt, Nümbrecht, Germany). However, in only one of them, saliva was collected at least 1.5 h after the last meal (16). This could have affected the results of the other study (17) since saliva collection should be performed only 1 or 2 h after the last meal (5, 9). Even after waiting for this period, large amounts of milk peaks are still present in the saliva samples of infants up to 6 months of age, which interferes with the reliability of the results (18). Thus, the idea of cleaning the infants' mucosa is relevant to reduce the concentration of extrinsic components from feeding and to obtain the intrinsic compounds from infant saliva.
In this context, we compared the profiles of salivary metabolites of infants in the pre-dental period before and after using oral mucosa hygiene procedures, with the aim to define a protocol to be used prior to saliva collection for metabolomic evaluation by NMR. These findings will allow verifying the feasibility of implementing this methodology in future studies, in an attempt to reduce bias inherent of extrinsic salivary metabolites, especially provided from dietary habits such as breastfeeding milk and from microbial metabolism. Thus, there will be an increase in the reliability of the results regarding the intrinsic metabolites. This will allow a more accurate assessment of the salivary metabolomic profile of infants in the pre-dental period and, consequently, to improve the identification of changes in physiologic conditions and also related to local or systemic diseases.
Materials and Methods
Study Design and Ethical Aspects
Prior to this study, the project was submitted and approved by the Local Research Ethics Committee under the number 3.551.037. A cross-sectional clinical study with a convenience sample was conducted, in which were selected participants from the patients from a Pediatric Dentistry Clinic of a Brazilian public Federal University. Inclusion criteria were infants between 2 and 6 months of age and who had no erupted deciduous teeth. Exclusion criteria were the use of antibiotics or antifungals in the 3 months prior to collection and the non-agreement by parents or legal guardians to participate in the study. All guardians of the recruited infants were informed about the purpose of the study and its possible risks and benefits. They voluntarily agreed to participate and signed a “Free and Informed Consent Form.”
Clinical and General Evaluation
Participants underwent an initial clinical evaluation, carried out by one trained professional, in which all intraoral structures were examined. In addition, parents answered questions about hygiene, diet habits, and health of the infants; these data were recorded in an anamnesis questionnaire.
Salivary Collection and Oral Hygiene Procedures
The initial collection of total unstimulated saliva was performed using an automatic pipette with sterile plastic tips, directed at the oral floor region of the infants, using a previously described methodology (12). Subsequently, their oral mucosa was cleaned, using a gauze moistened with filtered water. After 5 min, a new salivary collection was made, following the same methodology employed initially. All samples were obtained in the morning, between 9:00 and 11:00 am, and at least 1 h after the last feeding. They were stored directly in sterile plastic microtubes, which were kept on ice throughout the collection. At the end, the tubes were immediately transferred to the laboratory and spiked with 6 μL of sodium azide. Subsequently, they were centrifuged at 10,000 g at 4°C for 60 min (Cientec, CT-15000R, Brazil); the supernatant was transferred to labeled sterile microtubes and stored in a freezer at −80°C, as previously described (12).
Metabolomic Assessment Through Nuclear Magnetic Resonance (NMR)
Metabolomic evaluation was performed according to a standardized protocol (12), using a 500-MHz NMR spectrometer (Bruker Biospin, Rheinstetten, Germany), shown in Figure 1. We used a mixture of 153 μl of saliva supernatant with 17 μl of 20 mM phosphate buffer pH 7.0, composed of deuterated water (D2O; Cambridge Isotope Laboratories Inc., USA) and 4,4-dimethyl-4-silapentane-1-sulfonic acid (DSS; Sigma-Aldrich, Milwaukee, USA). The 1H NMR spectrum was acquired at 298 K using the Carl-Purcell-Meiboom-Gill (CPMG) pulse sequence to suppress signals from proteins and other macromolecules through a T2 filter. The 1H spectra were determined using 1,024 scans. Two-dimensional spectra of 1H-1H TOCSY were acquired at 298 K, with acquisition parameters of 256 × 2,048 points, a spectral width of 12,019 Hz in each dimension, and a spin lock time of 70 ms. A spectral width of 12,019 Hz was used to identify the metabolites found in the one-dimensional analysis and to elucidate possible ambiguities. Subsequently, each representative peak of the spectra was identified with the aid of the TOCSY experiment, using the Human Metabolome Database (http://www.hmdb.ca/) and specific literature (6, 12).

Figure 1. Photograph of the 500-MHz NMR spectrometer (Bruker Biospin, Rheinstetten, Germany) in which the metabolomic analyzes of the saliva of infants in the pre-dental period before and after oral mucosa hygiene procedures were performed.
To increases the transparence and replicability purposes, the spectra obtained and data extraction are available in Open Science Framework repository (Identifier: 10.17605/OSF.IO/YF82Q).
Statistical Analysis
A descriptive analysis of the clinical and general data from anamnesis was performed using the SPSS Statistics 21.0 program (SPSS Inc., Chicago, IL, USA). All 1H spectra were imported to Topspin program (Bruker Biospin, Rheinstetten, Germany) to perform baseline and phase correction. The spectra were aligned using the internal reference DSS with a peak at the 0.00-ppm region. Each spectrum was transformed by the software into an intensity table by displacement and divided into regions of 0.3 ppm, called “buckets,” which corresponded to the peaks of the spectrum, using the AMIX statistical program (Bruker Biospin, Rheinstetten, Germany). The water region was excluded (4.45 to 5.18 ppm). Subsequently, the matrix obtained was analyzed using the software Metaboanalyst 4.0 (http://www.metaboanalyst.ca). The data were normalized according to the sum of intensities; Pareto scaling and multivariate analysis were applied according to a previously described strategy (19).
Results
Table 1 shows the descriptive analysis of the sample. Eleven infants were evaluated, presenting a mean age of 3.81 (± 1.40) months. Six (55%) of them were female. Regarding the type of birth, six were born through vaginal birth and five via a cesarean. In relation to the diet, 9 (82%) infants were exclusively breastfed and 3 (18%) received breast and artificial milk. Regarding the oral hygiene habits, eight (73%) parents reported a routine at least once a day and three (27%) did not adopt any hygiene practices for their children. Concerning health data, 91% of the participants did not show any oral or systemic alterations. However, one infant had been infected with cytomegalovirus (CMV) during the intrauterine period, presenting thrombocytopenic purpura. In addition, the presence of mucocele in the lower lip was verified in this same patient.
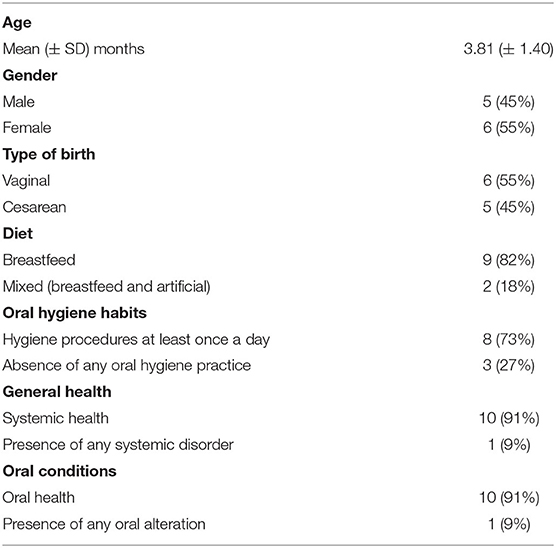
Table 1. Characterization of the participants.
The levels of lactose, glucose, sugar regions, acetate, alanine, and lactate were higher in the initial samples than after the oral hygiene procedures. In addition, a distinction in the profile of salivary metabolites between the samples collected before and after cleaning the mouth of infants in the pre-dental period was observed, which was verified through multivariate statistical analyses of PLS-DA (Figure 2A) and O-PLS-DA (Figure 2B).
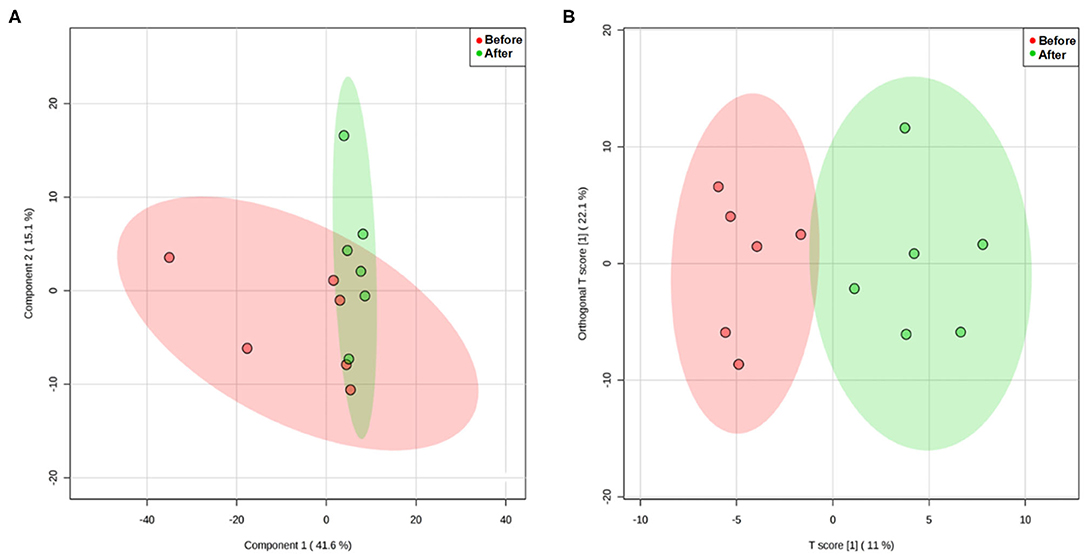
Figure 2. Analysis of PLS-DA (A) and O-PLS-DA (B) showing the distinction between the profile of total salivary metabolites before and after cleaning the oral mucosa of infants in the pre-dental period.
Regarding the main type of nutrition, we observed a decrease in sugar levels in the saliva of infants in the pre-dental period when they were exclusively breastfed after oral hygiene. Figure 3 illustrate these findings, showing a representative spectrum of saliva from infants exclusively breastfed before (Figure 3A) and after cleaning their oral mucosa (Figure 3B). Likewise, cleaning the oral cavity of participants who received mixed feeding also reduced the sugar levels, which can be seen in Figure 4, showing the representative 1H NMR spectra of these samples before (Figure 4A) and after the oral hygiene procedures (Figure 4B). We also observed that the concentration of the sugar region components was higher in the samples before oral hygiene in infants who were exclusively breastfed (Figure 3A) than in those who received mixed feeding (Figure 4A).
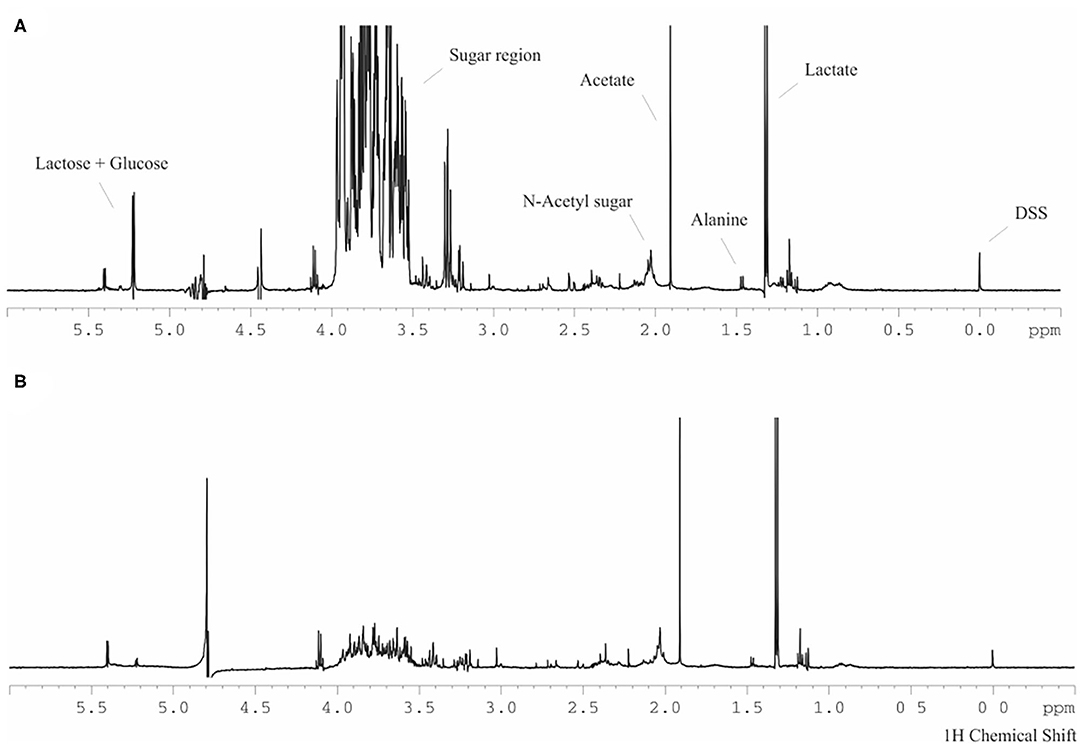
Figure 3. Representative 1H NMR spectrum of whole saliva from infants in the pre-dental period with exclusive breastfeeding before (A) and after cleaning their oral cavity (B).
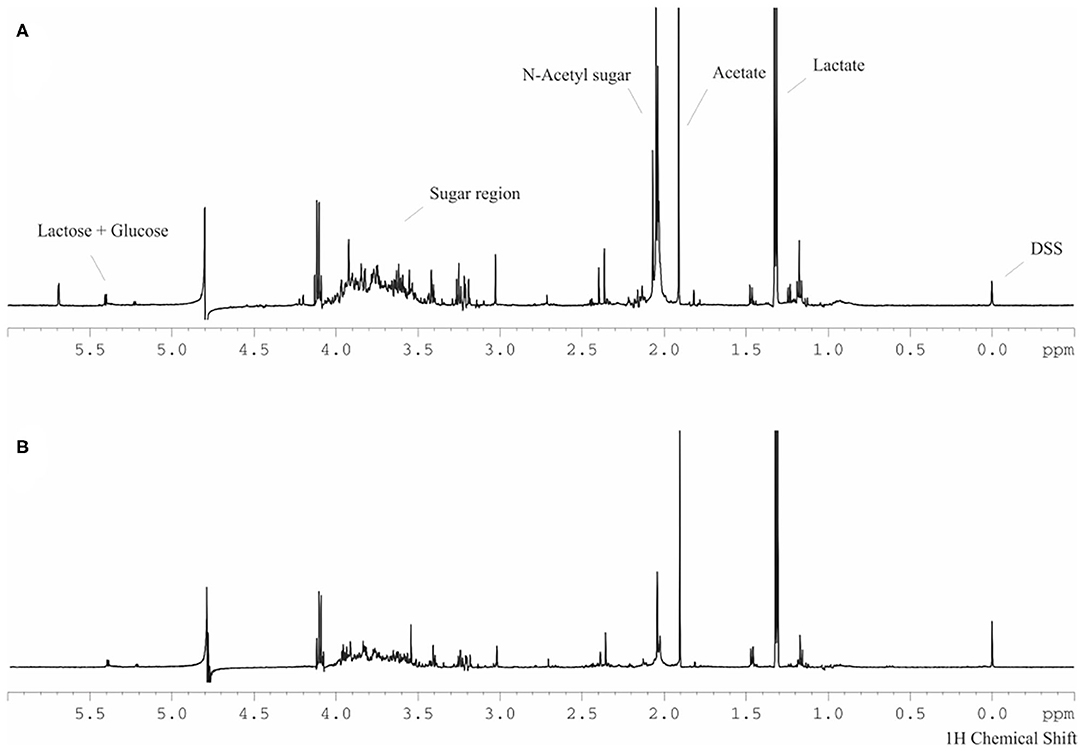
Figure 4. Representative spectrum of 1H NMR of whole saliva from infants in the pre-dental period with mixed feeding (consumption of breast and artificial milk) before (A) and after performing oral hygiene procedures (B).
A decrease in the concentrations of sucrose (5.38 ppm) and lactose (5.22 ppm) was verified after performing the oral mucosa hygiene procedures. When assessed regarding the type of diet, both sucrose and lactose components were initially higher in participants who were exclusively breastfed than in those who received mixed feeding.
Discussion
The present data demonstrate that cleaning the oral cavity of infants in the pre-dental period prior to salivary collection allowed a more precise identification and quantification of intrinsic salivary metabolites, since it decreased the levels of extrinsic compounds in the samples. These findings are extremely important for the determination of an efficient, reproducible, and accurate salivary collection protocol for infants to avoid interference of milk peaks and other extrinsic components from the diet directly interfere with the NMR analysis of the salivary metabolites. It has previously been shown that performing saliva collections in infants without previous cleaning of their mouths directly interfered with the metabolomics analysis through NMR, especially because it presents extremely intense peaks in the sugar region, acting as a confounding factor and making it difficult to obtain accurate and reliable results for the other salivary metabolites (18). In the same way, compounds such as acetate, alanine, and lactate, which were identified in infants with both feeding types, became less evident after cleaning the oral cavity of all participants. As previously suggested in a clinical evaluation of the saliva of children with and without dental caries, these compounds seem to be extrinsic and could be related to microbial metabolic activity (5).
In the present study, only infants who did not have any erupted primary teeth were included. This is because the dental eruption process alters the flow rate and the composition of saliva due to the presence of inflammatory cells in the oral cavity, related to this physiological stage (20). Besides, the development of salivary glands occurs during this phase since they only reach their full maturation at approximately 4 years of age (21). There are also differences in the salivary composition during the tooth eruption period, with an increase in the amount of total proteins with the aging of the patients (22), including in infants between 3 and 6 months of age (17). In addition, during the first years of life, there is a significant change and increase in the diversity of microbial species that colonize the oral cavity (23), which can also alter the salivary composition.
For these reasons, it is believed that the dental eruption is responsible for changes in the salivary metabolomic profile, besides being a period characterized by significant changes in physiology and development. Although preview findings indicate that age and diet are modulators of salivary peptidome in infants (24), neither any differences were found between the salivary metabolome inherent to each dentition period (5) nor relations to the eruption periods of primary teeth (16). Regarding the salivary metabolomic profile in the pre-dental period, there are still knowledge gaps. We decided to recruit only infants older than 2 months of age due to the post-natal maturation process of the salivary glands (21) and up to 6 months since normally, the eruptive processes of the first deciduous teeth start at that age (25).
Studies on the metabolome of biofluids can be performed using Nuclear Magnetic Resonance (NMR), which is a technique that allows to predict and monitor the clinical status of a patient (5). In addition, it has the advantage of being a non-invasive method, allowing the simultaneous monitoring of various components of the biofluid, and can identify foreign molecules in biological samples. It can be applied in the evaluation of urine, blood, and saliva (26). Several endogenous and exogenous salivary biomolecules can be analyzed, including those from glandular metabolism, gingival fluid, diet, as well as pharmaceutical products (5).
The present study aimed to elucidate the importance of cleaning the mouth of infants before collecting saliva samples. We opted for the elaboration of a simple and low-cost oral cleaning protocol which is also reproducible. Thus, it was decided to clean the oral mucosa of the infants in the pre-dental period with gauze wrapped in the finger soaked in filtered water. It is important to point out that one limitation of the present study was the use of only one technique, since the investigation of more methodologies would allow validate the best protocol. However, one of the advantages of using the employed technique is that it was already the form that caregivers reported using at home for oral hygiene after feeding their children. Therefore, most participants were already familiar with this type of manipulation of oral tissue, favoring its acceptance during the research. In addition, this technique had already proved to be favorable for the oral hygiene of infants when compared to the use of distilled water or 0.75% hydrogen peroxide for microorganisms reduction (27).
Among some other limitations, there is the small sample size, which should be expanded to corroborate the results found here with greater statistical power. Also, most of the evaluated children were exclusively breastfed, and one of the participants had a systemic disease and a local alteration, a mucocele. However, as the main objective of the study was to assess whether cleaning the oral mucosa of infants in the pre-dental period regardless their oral or systemic condition would interfere with the assessment of salivary metabolites, the differences between samples before and after oral hygiene were compared in a paired manner for each patient, allowing this individual to be included in the sample without causing significant repercussions or confusion to the obtained results. Then, the authors believe that the inclusion of this patient in the study represents a low risk of bias for the present overall result.
During saliva collection, some standardized protocols are important. The fidelity of the NMR metabolomic data depends on the sample integrity. In the case of salivary samples, some metabolites are altered according to differences in the conditions of salivary collection, storage, and laboratory preparation of the samples (28). Therefore, in order to minimize these possible intercurrences, a previous employed methodology (12) was adopted, since it was capable of maintaining the integrity of saliva samples for NMR analysis. All samples of this study were collected under the same conditions and immediately stored on ice to avoid any changes in the compounds. Likewise, the samples were all collected in the morning to avoid differences related to the circadian cycle of the patients, in which a decrease in salivary flow is observed after this period of the day (29). In addition, saliva collection was performed at least 1 h after the last feeding or breastfeeding, according to the protocol adopted by a previous research with participants within the same age range (18).
Besides the observation of the milk remnants in saliva, the present findings revealed a higher presence of sugar and lactose in samples from patients who were exclusively breastfed when compared to mixed feeding. This finding is controversial, because a previous study also found differences between the saliva metabolomic profile of infants who were exclusively breastfed and those who were on a mixed diet (18), while another study found no effect on salivary metabolites related to milk feeding history during the first months of life of their participants (16). In this sense, due to the limited knowledge in this field, the suggestion that the salivary pattern is related to the type of feeding should be taken with caution.
Conclusion
The oral hygiene procedures performed in infants in the pre-dental period seems to reduce some of the extrinsic metabolites present in the samples, especially lactose, sugar region compounds, acetate, and lactate, thereby changing the salivary metabolomic profile in the present sample. Therefore, it was shown to be promising as a future protocol to be instituted prior to salivary collection in future studies with this population.
Data Availability Statement
The datasets presented in this study can be found in online repositories. The names of the repository/repositories and accession numbers can be found below: Open Science Framework repository, identifier YF82Q, available at: 10.17605/OSF.IO/YF82Q.
Ethics Statement
The studies involving human participants were reviewed and approved by Universidade Salgado de Oliveira - Niterói - Approval Number 3.551.037 (CAAE: 02912418.8.0000.5289). Written informed consent to participate in this study was provided by the participants' legal guardian/next of kin.
Author Contributions
AL: conceptualization, methodology, valiadation, formal analysis, investigation, data curation, writing—original draft, writing—review & editing, and visualization. LF-F: conceptualization, methodology, valiadation, formal analysis, investigation, data curation, writing—review & editing, visualization, supervision, and project administration. GF and LA: investigation, data curation, writing—original draft, writing—review & editing, and visualization. IS and AV conceptualization, methodology, valiadation, formal analysis, resources, data curation, writing—review & editing, visualization, supervision, and project administration. TF: conceptualization, methodology, valiadation, formal analysis, investigation, resources, data curation, writing—review & editing, visualization, supervision, and project administration. All authors contributed to the article and approved the submitted version.
Funding
This study was funded by FAPERJ, CNPq, CAPES (Finance Code 001), and the National Institute of Science and Technology of Structural Biology and Bioimaging (INCT-INBEB).
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
The authors would like to thank for the financial support received from FAPERJ, CNPq, CAPES (Finance Code 001) and the National Institute of Science and Technology of Structural Biology and Bioimaging (INCT-INBEB). We are also grateful for the technical support provided by the National Center for Nuclear Magnetic Resonance Jiri Jonas and the Multidisciplinary Research Laboratory in Dentistry at the Universidade Federal do Rio de Janeiro (UFRJ).
References
1. Dodds MW, Johnson DA, Yeh CK. Health benefits of saliva: a review. J Den. (2005) 33:223–33. doi: 10.1016/j.jdent.2004.10.009
2. Sung J, Wang Y, Chandrasekaran S, Witten DM, Price ND. Molecular signatures from omics data: from chaos to consensus. Biotechnol J. (2012) 7:946–57. doi: 10.1002/biot.201100305
3. Tyagi S, Raghvendra SU, Kalra T, Munjal K. Applications of metabolomics-a systematic study of the unique chemical fingerprints: an overview. Int J Pharm Sci Rev Res. (2010) 3:83–86.
4. Gebregiworgis T, Powers R. Application of NMR metabolomics to search for human disease biomarkers. Comb Chem High Throughput Screen. (2012) 15:595–610. doi: 10.2174/138620712802650522
5. Fidalgo TK, Freitas-Fernandes LB, Angeli R, Muniz AM, Gonsalves E, Santos R, et al. Salivary metabolite signatures of children with and without dental caries lesions. Metabolomics. (2013) 9:657–66. doi: 10.1007/s11306-012-0484-7
6. Silwood CJL, Lynch E, Claxson AWD, Grootveld MC. 1H and 13C NMR spectroscopic analysis of human saliva. J Den Res. (2002) 81:422–7. doi: 10.1177/154405910208100613
7. Vinayavekhin N, Homan EA, Saghatelian A. Exploring disease through metabolomics. ACS Chem Biol. (2010) 5:91–103. doi: 10.1021/cb900271r
8. Kageyama G, Saegusa J, Irino Y, Tanaka S, Tsuda K, Takahashi S, et al. Metabolomics analysis of saliva from patients with primary Sjögren's syndrome. Clin Exp Immunol. (2015) 182:149–53. doi: 10.1111/cei.12683
9. De Oliveira LRP, Martins C, Fidalgo TKS, Freitas-Fernandes LB, de Oliveira Torres R, Soares AL, et al. Salivary metabolite fingerprint of type 1 diabetes in young children. J Prot Res. (2016) 15:2491–9. doi: 10.1021/acs.jproteome.6b00007
10. Wei J, Xie G, Zhou Z, Shi P, Qiu Y, Zheng X, et al. Salivary metabolite signatures of oral cancer and leukoplakia. Int J Can. (2011) 129:2207–17. doi: 10.1002/ijc.25881
11. Ishikawa S, Sugimoto M, Kitabatake K, Sugano A, Nakamura M, Kaneko M, et al. Identification of salivary metabolomic biomarkers for oral cancer screening. Sci Rep. (2016) 6:1–7. doi: 10.1038/srep31520
12. Fidalgo TK, Freitas-Fernandes LB, Almeida FC, Valente AP, Souza IP. Longitudinal evaluation of salivary profile from children with dental caries before and after treatment. Metabolomics. (2015) 11:583–93. doi: 10.1007/s11306-014-0717-z
13. Kuboniwa M, Sakanaka A, Hashino E, Bamba T, Fukusaki E, Amano A. Prediction of periodontal inflammation via metabolic profiling of saliva. J Den Res. (2016) 95:1381–6. doi: 10.1177/0022034516661142
14. Romano F, Meoni G, Manavella V, Baima G, Tenori L, Cacciatore S, et al. Analysis of salivary phenotypes of generalized aggressive and chronic periodontitis through nuclear magnetic resonance-based metabolomics. J Periodontol. (2018) 89:1452–60. doi: 10.1002/JPER.18-0097
15. Aimetti M, Cacciatore S, Graziano A, Tenori L. Metabonomic analysis of saliva reveals generalized chronic periodontitis signature. Metabolomics. (2012) 8:465–74. doi: 10.1007/s11306-011-0331-2
16. Neyraud E, Schwartz C, Brignot H, Jouanin I, Tremblay-Franco M, Canlet C, et al. Longitudinal analysis of the salivary metabolome of breast-fed and formula-fed infants over the first year of life. Metabolomics. (2020) 16:1. doi: 10.1007/s11306-020-01661-7
17. Morzel M, Palicki O, Chabanet C, Lucchi G, Ducoroy P, Cham bom C, et al. Saliva electrophoretic protein profles in infants: changes with age and impact of teeth eruption and diet transition. Arch Oral Biol. (2011) 56:634–42. doi: 10.1016/j.archoralbio.2010.12.015
18. Silva LP, Bastos VAS, Fidalgo TKS, Oliveira CM, Pomarico L, Valente AP, et al. Oral health of babies and mothers during the breastfeeding period. J Clin Diag Res. (2019) 13:9–13. doi: 10.7860/JCDR/2019/40860.13132
19. Almeida PA, Fidalgo TKS, Freitas-Fernandes LB, Almeida FC, Souza IPR, Valente AP. Salivary metabolic profile of children and adolescents after hemodialysis. Metabolomics. (2017) 13:1–10. doi: 10.1007/s11306-017-1283-y
20. Rabea AA. Recent advances in understanding theories of eruption (evidence based review article). Fut Den J. (2018) 4:189–96. doi: 10.1016/j.fdj.2018.05.001
21. Teshima TH, Ianez RF, Coutinho-Camillo CM, Buim ME, Soares FA, Lourenço SV. Development of human minor salivary glands: expression of mucins according to stage of morphogenesis. J Anat. (2011) 219:410–7. doi: 10.1111/j.1469-7580.2011.01405.x
22. Deshpande RR, Panvalkar PS, Kulkarni AA, Gadkri TV. Age-related changes of the human salivary secretory total protein complex and trace elements in children between the age group of 3-16 years. J Biomed Sci Res. (2011) 3:362–7.
23. Holgerson PL, Öhman C, Rönnlund A, Johansson I. Maturation of oral microbiota in children with or without dental caries. PLoS ONE. (2015) 10:e0128534. doi: 10.1371/journal.pone.0128534
24. Morzel M, Jeannin A, Lucchi G, Truntzer C, Pecqueur D, Nicklaus S, et al. Human infant saliva peptidome is modifed with age and diet transition. J Prot. (2012) 75:3665–73. doi: 10.1016/j.jprot.2012.04.028
25. Brecher EA, Lewis CW. Infant oral health. Pediatr Clin North Am. (2018) 65:909–21. doi: 10.1016/j.pcl.2018.05.016
26. Gardner A, Carpenter G, So PW. Salivary metabolomics: from diagnostic biomarker discovery to investigating biological function. Metabolites. (2020) 10:47. doi: 10.3390/metabo10020047
27. Sales AB, Palud L, Schwartz JP, Pinto MHB, dos SANTOS EB. Comparison between two oral hygiene methods in babies in the control of streptococcus spp and Candida (in portuguese). Rev Gestão Saúde. (2014) 11:18–21.
28. Duarte D, Castro B, Pereira JL, Marques JF, Costa AL, Gil AM. Evaluation of saliva stability for NMR metabolomics: collection and handling protocols. Metabolites. (2020) 10:515. doi: 10.3390/metabo10120515
Keywords: saliva, magnetic resonance spectroscopy, infant, oral hygiene, breast feeding, metabolomics
Citation: Letieri AS, Freitas-Fernandes LB, Albarello LL, Fontes GP, de Souza IPR, Valente AP and Fidalgo TKS (2021) Analysis of Salivary Metabolites by Nuclear Magnetic Resonance Before and After Oral Mucosa Cleaning of Infants in the Pre-dental Period. Front. Dent. Med. 2:667365. doi: 10.3389/fdmed.2021.667365
Received: 12 February 2021; Accepted: 11 May 2021;
Published: 04 June 2021.
Edited by:
Apoena de Aguiar Ribeiro, University of North Carolina at Chapel Hill, United StatesReviewed by:
Maristela Barbosa Portela, Fluminense Federal University, BrazilDeepti Shrivastava, Al Jouf University, Saudi Arabia
Copyright © 2021 Letieri, Freitas-Fernandes, Albarello, Fontes, de Souza, Valente and Fidalgo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Tatiana Kelly da Silva Fidalgo, dGF0aWFuYWtzZmlkYWxnb0BnbWFpbC5jb20=