 Ma. Cristina Aurea Garcia
Ma. Cristina Aurea Garcia Ma. Therese Blanche Sta. Maria
Ma. Therese Blanche Sta. Maria Filipina Ng
Filipina Ng
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
OPINION article
Front. Dent. Med. , 10 November 2020
Sec. Endodontics
Volume 1 - 2020 | https://doi.org/10.3389/fdmed.2020.573103
This article is part of the Research Topic The Global Response to the SARS-CoV-2 Pandemic from Endodontists and Researchers View all 9 articles
Dental practice in the Philippines began in the 1900's when barbers used to double as dentists, using crude and queer methods in treating toothaches and extracting teeth. It was only in the 1800's that real dental practice began in the country when Jose Arevalo opened a dental clinic in Quiapo, Manila (1).
Formal education in the field of dentistry started when the Americans came to the Philippines in 1903. In the same year, the first Dental Law Act No. 593 was approved by the Philippine Civil Commission, which provided for the organization of the Board of Dental Examiners. The Philippines' first formal education was influenced by the Americans, in which the curriculum was the same as that in the United States of America (2).
A Dentariae Medicinae Doctor (DMD) degree is awarded to graduates of Philippine dental schools after 6 years of education. Private dental schools are regulated by the Commission on Higher Education (CHED), the government agency that implements and monitors the standards and guidelines for all higher education institutions (HEIs). The DMD program implements a standard curriculum consisting of general education, basic medical and dental sciences, pre-clinical subjects in the first 4 years, and clinical training in the last 2 years (3). During their clinical training, students are required to demonstrate clinical competencies obtained after encountering varied clinical experiences in restorative dentistry, periodontics, pedodontics, oral surgery, endodontics, and prosthodontics (i.e., fixed partial, removable partial, and complete denture).
The Professional Regulatory Commission (PRC) and the Philippine Dental Association (PDA) are two groups that oversee the dental practice in the country. The PRC is the government agency that regulates and supervises the practice of professionals. PDA, being the mother national association of dental professionals, promotes and protects the interest of its members through updates on policies and guidelines and continuing education. After graduating with a degree in Doctor of Dental Medicine, students must pass the two-part Dentist Licensure Exam conducted twice a year by the PRC. Dentists may either continue a post-graduate degree or pursue their career in private practice, teaching, public health, research, and hospital dentistry.
The Philippine Board of Endodontics (PBE), an implementing arm of the PRC, sets the standards and practice of endodontics in the Philippines. A dentist who wishes to be qualified as an endodontic specialist must meet the requirements set by the PBE. The requirements involve residency or advanced graduate education in a university- or hospital-based program in endodontics1. Endodontic specialty education requires engagement to both clinical and experimental research as well as in deep practice limited to endodontics.
An endodontic specialist may be elevated to become a fellow or a diplomate when the requirements set by the PBE are met. Such requirements include active participation in endodontic and interdisciplinary seminars and conferences, active participation in literature and textbook reviews, serving as a resource speaker in seminars or scientific forum in endodontics, continued professional advancement, teaching skills in endodontology in a university or institution accredited by CHED, and a minimum of 10 years of teaching experience in endodontics (4).
In December 2019, a new strain of coronavirus was detected and confirmed in Wuhan, China. In just a few months after the detection, the number of people infected with COVID-19 cases increased radically, which prompted the World Health Organization (WHO) to declare the COVID-19 disease as a pandemic by March 2020 (5).
On the 30th of January 2020, the first case of COVID-19 in the Philippines was reported by its Department of Health (DOH) when a 38-year-old female Chinese national, despite being asymptomatic, tested positive of the virus (6). CHED released its first advisory on February 12 on the guidelines for the prevention, control, and mitigation of the spread of COVID-19 in HEIs in the Philippines (7).
On March 7, 2020, DOH confirmed the first case of local transmission in the country after verification with the Bureau of Immigration showed that the patient had no recent travel history (8). Four days after, the CHED and the PDA had recommended the suspension of all classes and elective procedures, respectively, following the issuance of their guidelines in preventing the spread of the said virus.
With these reported developments, CHED enjoined all HEIs to draft emergency plans based on the WHO guidelines and in line with the Inter-Agency Task Force on Emerging Infectious Disease (IAFT) for screening and response to COVID-19. As physical classes continued to be suspended, CHED invoked the exercise of academic freedom through distance learning, E-learning, and a flexible academic calendar to help the students finish their requirements and training. HEIs were given the freedom to exercise their judgment in the deployment of available flexible learning and other alternative modes of delivery in lieu of in-campus learning if they have the resources to do so as long as discretion is reasonable, transparent, and outcomes-based.
On its latest advisory, CHED further prescribed the following: (a) skeleton workforce on HEI operations, (b) physical classes, on-the job training (OJT) and internship programs remain suspended until the government says otherwise, and (c) no residential or face-to-face mode of instruction until August 31, 2020 (7).
Based on the recommendations of the DOH, WHO, and Center for Disease Control and Prevention (CDC), the PDA issued a series of guidelines to avoid the spread of COVID-19, urging a no-contact screening procedure. The recommended guidelines are as follows:
1. Dentists and all staff must wear the prescribed personal protective equipment (PPE) including protective eyewear, surgical mask, disposable caps, and disposable gloves.
2. Dentists should screen patients by phone before confirming an appointment to avoid close physical contact with persons infected with COVID-19.
3. Elective procedures are not allowed.
4. Only immediate concerns such as pain, infection, oromaxillofacial conditions, or trauma can be addressed by dentists. Patients for these urgent dental concerns are required to fill up a screening form, including their companion.
5. Patients with temperature higher than 37.3°C or 99.14°F and with respiratory disease will be referred to a hospital immediately (9) (Figure 1B).
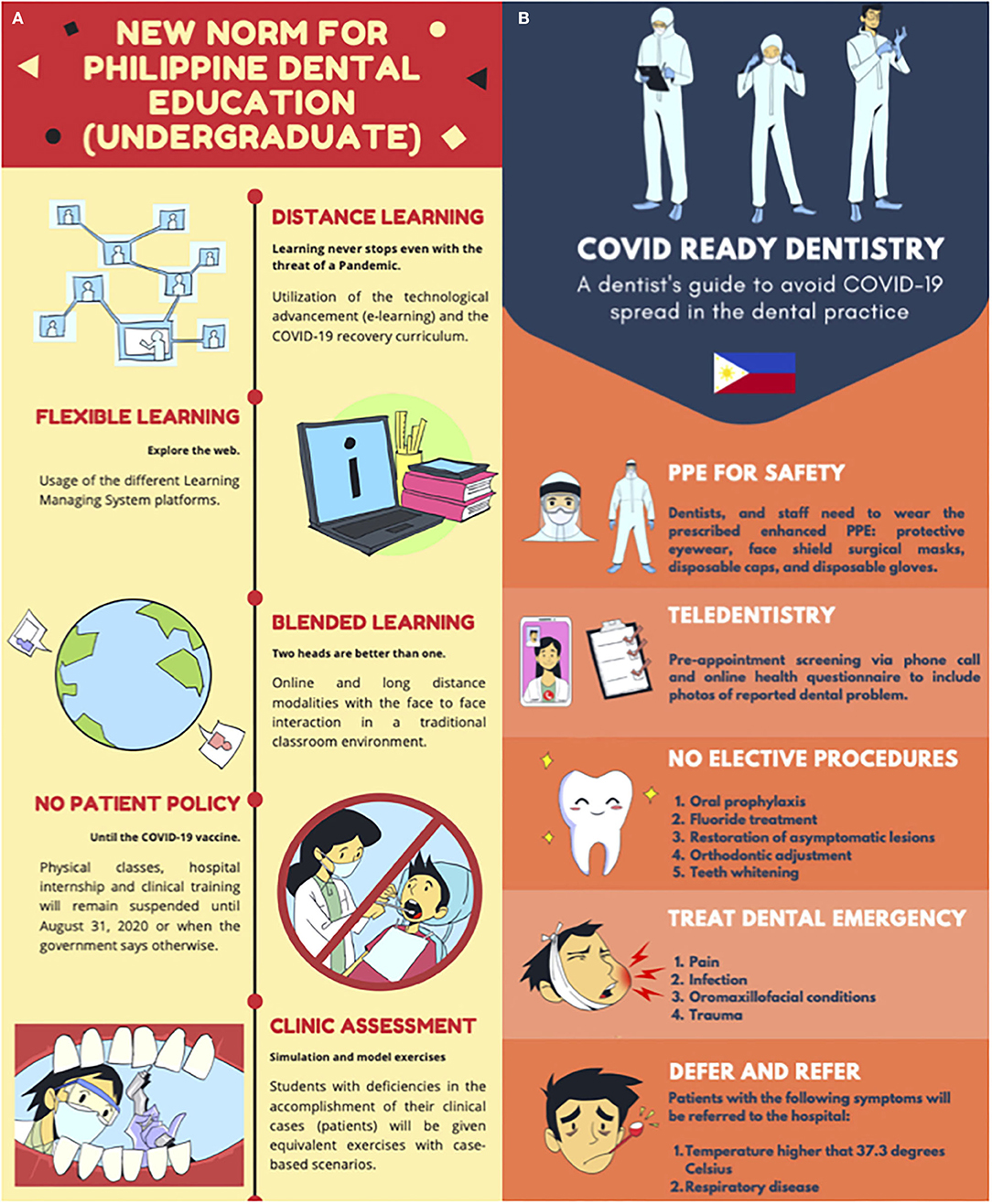
Figure 1. (A) Modification on Dental Education based on CHED guidelines (7); (B) PDA interim guidelines for dental practice (9).
Guidelines on the Standard Infection Control Precaution to consider air exchange, ease of cleaning, and minimizing exposure to a patient were also disseminated. On its latest update as of May 31, 2020, the PDA stressed that alongside the use of PPE, other measures including air engineering, universal infection control protocols, and meticulous disinfection must be included (9).
When and how to reopen schools and clinics are among the toughest and most sensitive decisions on political agendas today in the country. There are contentions between different government departments and agencies about safety when schools and dental clinics should reopen. It has been nearly 6 months since clinic operations were restricted and schools were closed, affecting nearly 28.5 M students, 3.5 M students of which belong to tertiary or higher education (10). As dental medicine requires pre-clinical and clinical training, this posts a great challenge in dental education.
While physical class is the best policy tool to raise skills, dental schools in the country have no choice but to yield to remote learning solutions to adapt to the “new norm” in dental education. HEIs are given the liberty to innovate on how they will carry out the dental curriculum without compromising the expected outcome from students. As shown on Figure 1A, activities that may not require the physical presence of both teacher and students will be done online using different learning management system platforms. These include, but are not limited to, lectures, group discussions, and case presentations. Blended learning techniques with a limited traditional place-based classroom method will be adapted to facilitate activities that require the use of the laboratory and/or a simulator.
In the Philippines, remote learning is not the preferred and conditioned choice of teaching–learning method. A lot of teachers are not technically, mentally, and educationally prepared for online classes. Therefore, series of trainings for the faculty on flexible learning and distance learning are now being conducted to ensure that curriculum content and the set learning outcomes are achieved at the correct timeline.
At the time of writing, based on the recommendations of the Philippine Association of Dental Colleges, a “no patient policy” will be implemented in the clinical training (Figure 1A). While study guides and manuals are in the offing, laboratory and clinical experiences will instead be simulated using models, typodonts, and mechanical articulators during the first semester of academic year 2020–2021 or until the threat of COVID-19 is eradicated. Students will not be able to experience treating actual patients, which may compromise the acquisition and the assessment of the affective domain. The same could be said for critical thinking. The effects of these modifications in the delivery of clinical dentistry are yet to be evaluated by CHED when school reopens. PRC, for the part of the board licensure examination for dentists, has issued its guidelines on the use of mechanical articulators in lieu of live patients in the complete denture exercise.
The IATF continues to place the Philippines under community quarantine, and face-to-face learning is still not allowed. The CHED Commissioner said in his recent interview that courses which require face-to-face learning, such as OJTs and clinic internship, will be deferred to the next school term. This automatically would mean that graduation and board examinations are deferred until the quarantine is lifted.
While some clinics are starting to reopen, dentists are strictly following the guidelines set forth by WHO, ADA, AAE, IFEA, PDA, and other dental organizations. The Endodontic Society of the Philippines has shared the PBE-penned practice guidelines in the time of COVID, strictly adhering to emergency, emergent, and non-aerosol-generating procedure cases with limited aerosol-generating procedure cases and following the infection control protocols. Engineering and administrative controls are aptly put in place with the use of PPE. Dentists are continually on their toes to keep abreast with new and emerging information by attending webinars.
With these modifications to comply with administrative and engineering controls and with the number of patients being reduced, it is expected to create a great impact on the finances of both schools and clinics. More clinics are expected to reopen soon, and schools are expected to reopen in October 2020 as local governments decide to transition Metro Manila from enhanced community quarantine to general community quarantine (11). Some educational institutions have announced their plan to reduce tuition, considering that a great portion of the delivery mode will be online. This could unfortunately mean retrenchment in the number of their staff.
On the other hand, the opposite happened to many dental private clinics. Additional staff were hired to manage work such as infection control and installation of equipment such as air filters, high vacuum evacuators, and aerosol suctions among others. In addition, the expected use of an extra layer of PPE will surely cause a price hike in dental procedures.
As dental clinics and universities prepare for the new normal in the profession of dentistry, school administrators and dental practitioners are making sure that their guidelines and protocols are in accordance with the recommendations issued by all reputable organizations in the field of health and dentistry—CHED, PDA, DOH, and CDC among others.
All educational institutions and clinics are expected to monitor new advisories from the health department to keep their protocols up to date.
Despite the challenges they are about to face, dental schools are hopeful that teaching and learning situations will eventually adjust to the new normal as the country—and the whole world—awaits the existence of a vaccine against COVID-19.
FN carried out the manuscript. MG and FN disseminated and collated questionnaires to the Deans of Dental Schools. FN and MSM conceptualized the infographics. MG supervised the findings of this work. All authors discussed the results and contributed to the final manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The authors wish to express their gratitude to the Deans of the Philippine Association of Dental Colleges, especially to Dr. Vicente Medina III, and Hon. Melinda Garcia for taking time to review and comment on the manuscript.
1. History of Philippine Dentistry. (2012). Available online at: http://www.philippinedentalassociation.info/pda/history/ (accessed September 5, 2020).
2. Dalanon J, and Matsuka Y. The evolution of dental education in the Philippines. Health Prof Educ. (2019) 5:172–6. doi: 10.1016/j.hpe.2018.07.001
3. CMO No. 3 s. 2018. (2018). Available online at: https://ched.gov.ph/cmo-no-3-series-of-2018-policies-and-standards-and-guidelines-for-the-doctor-of-dental-medicine-dmd-program/ (accessed May 25, 2020).
4. Annex F. Level Alignment Matrix Between Specialized Dentistry Fellowship and Diplomate Qualification Outcomes to the PQF Levels 7 and 8 Descriptors (Specialized Dentistry-Endodontics). PRC-SB Resolution. As distributed by Philippine Regulatory Board of Dentistry (2020).
5. Coronavirus, Disease (COVID-19)–Events as They Happen (n,.d.). Available online at: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/events-as-they-happen (accessed May 18, 2020).
6. DOH Confirms First 2019-NCOV Case in the Country; Assures Public of Intensified Containment Measures: Department of Health website (n.d.). Available online at: https://www.doh.gov.ph/doh-press-release/doh-confirms-first-2019-nCoV-case-in-the-country (accessed May 25, 2020).
7. COVID-19 Updates (2020). Available online at: https://ched.gov.ph/covid-19-updates/ (accessed June 10, 2020).
8. DOH Confirms Local Transmission of COVID-19 in PH; Reports 6th Case: Department of Health website (n.d.). Available online at: https://www.doh.gov.ph/doh-press-release/doh-confirms-local-transmission-of-covid-19-in-ph (accessed May 25, 2020).
9. PDA, Covid Interim Guidelines on Infection Prevention for CoVid-19 Pandemic (n,.d.). Available online at: https://www.fdiworlddental.org/sites/default/files/media/documents/interim_guidelines_on_infection_prevention_during_covid-19_pandemic.pdf (accessed August 19, 2020).
10. COVID-19 Educational Disruption and Response. (2020). Available online at: https://en.unesco.org/covid19/educationresponse (accessed May 30, 2020).
11. WSAS_RR. Home (n.d.). Available online at: http://www.pnp.gov.ph/index.php/news-and-information/3700-differences-between-enhanced-community-quarantine-and-general-community-quarantine (accessed September 2, 2020).
Keywords: COVID-19 guidelines, dental education, dental practice, distance learning, flexible learning
Citation: Garcia MCA, Sta. Maria MTB and Ng F (2020) Effects of COVID-19 to Dental Education and Practice in the Philippines. Front. Dent. Med. 1:573103. doi: 10.3389/fdmed.2020.573103
Received: 16 June 2020; Accepted: 09 September 2020;
Published: 10 November 2020.
Edited by:
Johnah Galicia, University of the Pacific, United StatesReviewed by:
Sheng Zhong, Independent Researcher, Minneapolis, MN, United StatesCopyright © 2020 Garcia, Sta. Maria and Ng. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Filipina Ng, ZmlsaXBpbmEubmdAZ21haWwuY29t
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.