 Alexis Gaudin
Alexis Gaudin Reza Arbab-Chirani2
Reza Arbab-Chirani2 Fabienne Pérez
Fabienne Pérez- 1Department of Endodontics and Restorative Dentistry (RMeS U1229), Faculty of Dental Surgery, University of Nantes (CHU Nantes), Nantes, France
- 2Department of Endodontics and Restorative Dentistry (LATIM U1101 Inserm), Faculty of Dental Surgery, University of Brest (CHU de Brest), Brest, France
The coronavirus disease 2019 (COVID-19) is an acute infectious disease leading to a global pandemic. Dental professionals (dental staff, academics) and students are one part of the healthcare workers that face the greatest severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) risk. Consequently, several measures were imposed to limit the spread of the virus, the overload of the health system, and to protect the dental professionals and students. This brief communication focuses on chronology of COVID-19 related events, the temporary modifications, and the potential impacts on dental education in France.
Introduction
Specialty Education
There are currently 16 public dental schools in France, all are government-owned. In France, dental surgery studies last 6–9 years after the bachelor's degree and take place in a training and research unit (UFR) in odontology of the French university. To date, only three recognized specialties in dentistry (Orthodontics, Oral Surgery, Oral Dentistry) may be acquired through internship or by a commission of the French dental board. Therefore, in the same way as periodontology or pediatric dentistry, endodontics is not yet an officially recognized specialty in France.
However, University Diplomas which are training courses in endodontics are delivered by some universities. The program is directed by the host dental faculty and the content varies from 1 year of training to 3 years full time. Although specific endodontic training is not compulsory, its acquisition is strongly recommended to have a limited exercise to endodontics.
Standards of Clinical Practice and Dental Education
In France, the scope of undergraduate dental (including endodontics) education is defined by French ministry of higher education, research and innovation in accordance with frame of the 2005 European directive (1). This directive concerns both the duration of studies (5,000 h of theoretical and practical training) or the compulsory subjects (basic, medico-biological, general medical, oral disciplines) in order to harmonize training between different member countries. However, this directive leads to many disparities since it does not define a specific educational program.
Organizations and Associations That Influence the Practice of Dentistry
The CNEOC (Collège National des Enseignants en Odontologie Conservatrice) is a board of academic teachers of the 16 schools of dentistry in France aiming to generate available educational resources, guidelines and recommendations (2). The HAS (Higher Health Authority) is an independent public authority that provides recommendations for professionals of both the health and social care sectors. HAS published guidelines to develop endodontic pedagogic document for French students, endodontic staff, and dental practitioners (3).
The SFE (French Society of endodontics) (4) is a scientific society member of the ESE and the IFEA (International Federation of Endodontic Association). The SFE has a long-standing implication in endodontic continuing education, in supporting endodontic limited exercise and taking part of the different French dental institutional organizations.
Chronology of COVID-19 Related Events/Circumstances Leading To The Interruption of Education and/or Dental Practice
The COVID-19 pandemic was confirmed to have reached France on January 24, 2020, when the first COVID-19 case in both Europe and France was identified in Bordeaux. The first five confirmed cases were all individuals who had recently arrived from China. A Chinese tourist who was admitted to hospital in Paris on January 28, died on February 14, making him the first Covid-19 death case in France. On May 4, retroactive testing of samples in one French hospital showed a patient had been infected with the virus on December 27, almost a month before the first officially confirmed case. Main events leading to the interruption of education and/or dental practice are summarized in (Figure 1).
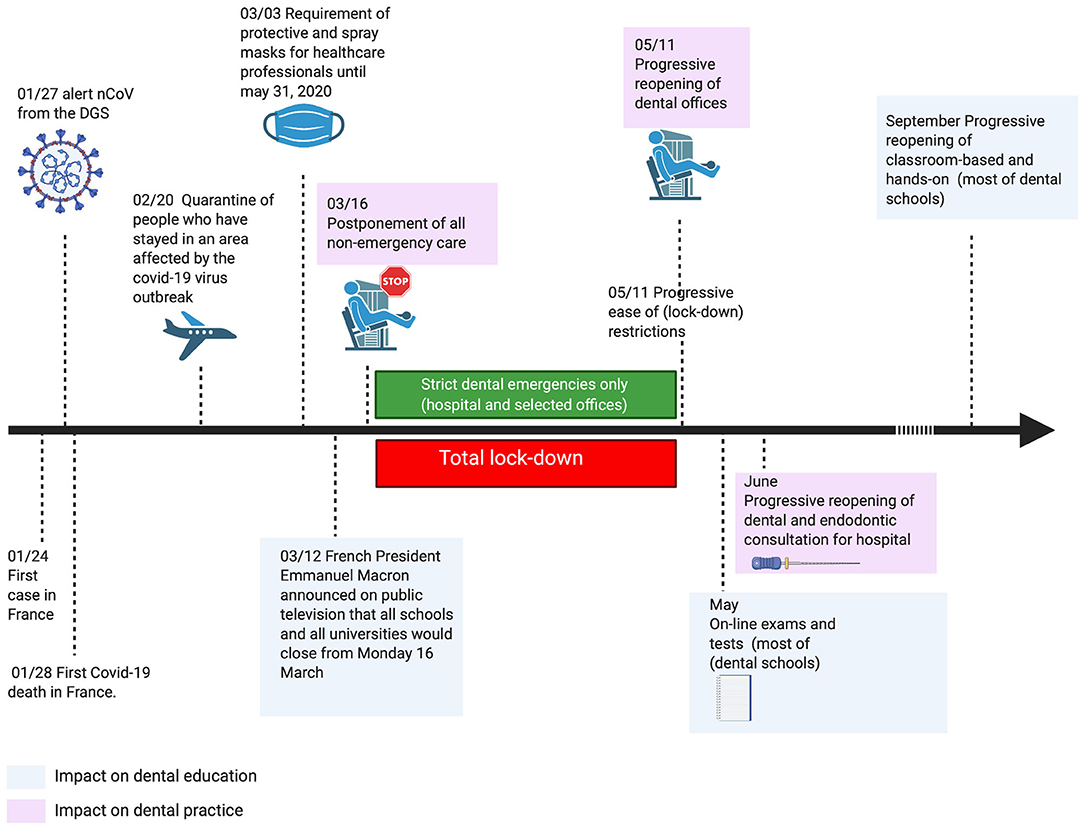
Figure 1. A chronology of COVID-19 related events leading to interruption of education and dental practice in France. nCoV, novel coronavirus; DGS, Directorate-General for Health.
Temporary Modifications
Clinical Care (Academic and Private Practice)
The total lock down in France lasted from March 1, 2020, to May 11, 2020. During this period, only strict emergency clinical care was allowed either in hospital or in selected dental offices. Strict emergencies referred to (i) severe acute dental pain, (ii) dental infection, (iii) dental traumatology, or (iv) oral hemorrhagia. During lockdown, French Society of endodontics and CNEOC took part in recommendations published by the French dental board. These information are based on international recommendations (5) and are accessible through website: http://www.ordre-chirurgiens-dentistes.fr. Other dental procedures were not allowed. Teledentistry was encouraged to avoid patients to come to dental offices. Specific schedules for strict emergencies were organized. Preprocedural mouth rinse with 0.2% povidone-iodine or 0.5–1% hydrogen peroxide mouth rinse were recommended. Personal Protective Equipment (PPE) were mandatory (FFP2 mask, gloves, face shields, surgical gowns), and strict hygiene and barrier measures were promoted and reinforced (hand-washing, disinfection of all surfaces, 15 min of aeration between patients, etc…). Use of disposable (single-use) devices such as mouth mirror, syringes to prevent cross contamination was encouraged. All aerosols generation devices (turbines handpieces, ultrasonic scaler, air-polishers) were limited to strict minimum with high suction evacuator and with the use of rubber dam. Taken together, these measures play an important role in protecting clinicians during the COVID-19 outbreak (6).
After May 11, 2020 all the recommendations to manage oral fluids were the same, however, in addition to strict dental emergency other patients may be seen. Patients were divided in four different categories according to their own risk factor and whether they (or their entourage) encountered the virus (Table 1).
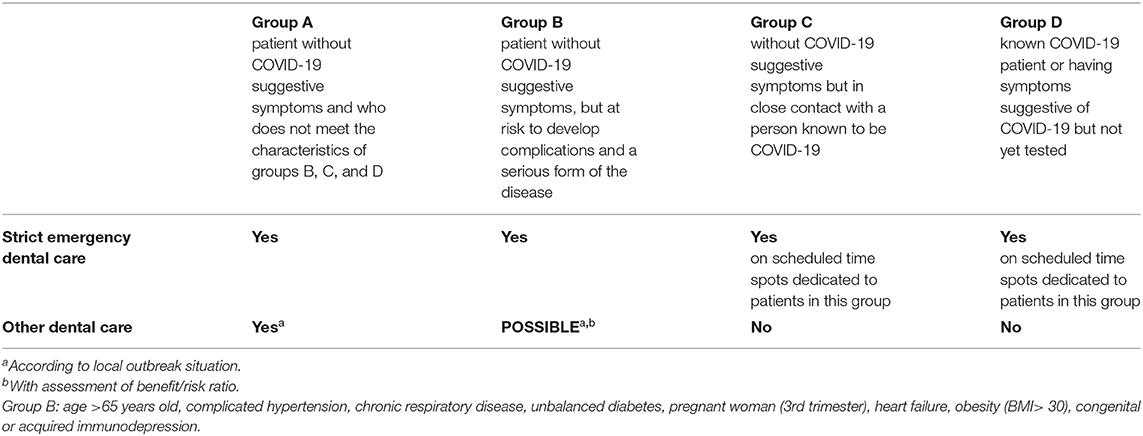
Table 1. Adapted from (guide soignant recommandations transitoires Conseil de l'ordre des chirurgiens-dentistes) (7).
Curriculum Delivery and Content
Since the closure of the Universities, all on-campus learning, hands-on and clinics were canceled. Only on-line content was accessible for dental students. All on-line contents such as e-learning, videoconferences, webinars were encouraged. Communication with students was done by email and phone calls. Moodle platforms were also used to facilitate the curriculum delivery and content.
Most of the dental schools used on-line exams through Moodle platforms with the aim of minimum disruption for students. Theses exams were customized from the “classic situation” to the “COVID-19 situation.” Overall missing content may be assessed between 10 and 15% for theoretical and practical content. Terminal hands-on assessment have been removed. Moreover, undergraduate and postgraduate students almost loose 4 months for clinical practice.
The Effects of the Temporary Modifications
A group insurance brokerage firm measured the behavior of 60,000 salaried policyholders covered by company contracts and analyzed that lockdown, with the closure of dental offices, reduced dental care consumption to almost zero (−93%) compared to the same period of the year. According to the French national health insurance fund, dental care reimbursements fell by 29.1% over the first 4 months of the year (from January to April) (8). Moreover, as other dentists, endodontists were available to perform teleconsultation and emergency dental care only.
The COVID-19 outbreak has really impacted the academic timeline. Undergraduate and postgraduate did not have the opportunity to finish their complete programs. The effects on the knowledge and skills is difficult to assess and consequences may be visible in the next year. However, less productive and less efficient students are expected.
More broadly, the loss of patient volume and therefore income may be evaluated to 20% in comparison with previous years. Most of the dental offices had to use partial unemployment for the dental staff. Some difficulty can also be expected for the retention of the dental staff after the COVID-19 outbreak.
Return To Practice
Dental surgeons have resumed their practice since May 11. The return to practice will have to face with new challenges such as respect of social distancing, management of patients that could not have been seen during the end of the academic year but also with economic issues. As consequence of the new norm of social distancing, wearing a mask by the general population is mandatory on public transportation, in schools, in hospitals, and in dental offices.
After the end of the lockdown, the dentists progressively return to pre-COVID-19 dental cares. However, the new hygiene and asepsis measures leads to a loss of activity in dental practices of about 40%, going from 15 to 20 patients per day to only 7 or 10 on average according to dental surgeon union (9). According to an online survey made by the French Union for Oral and Dental Health, on 3,396 dental practice professionals (1,725 dentists and 1,671 assistants) conducted between May 25 and 30, only 2% of dental practice professionals were unable to return to work (10). Since May 11, 44% of dentists and dental assistants have returned to work with the same working hours as before the health crisis, 29% with more working hours and 25% with fewer hours (10).
Since June 25, dentists can benefit from tests to detect the SARS-CoV-2 genome and/or tests to search for antibodies against this virus at their request and without a doctor's prescription. To help dental professionals, the French government has considered various means of action: compensation for childcare needs, tax-free financial aid of 4,500 euros from the dentist pension fund, financial compensation from the social security system, deferral of pension, banking, and insurance costs.
During the lockdown, all patients coming to teaching hospitals were treated by practitioners and residents. At this time, from the end of lockdown, patients are also treated by the last year-undergraduate students−(6th year's dental students in France). Dental university hospitals have to deal with the same challenges as private practice and some reorganization is necessary. In some of them, the treatment rooms need to be fitted out to protect against contamination (separation of chairs, etc.). Therefore, the return to full practice for every student (4th, 5th, and 6th years-students) is planned for early September. In dental schools, some hands-on and specific content and classrooms will be planned to overcome the delays encountered at the end of the 2019–2020 academic year. Each school has the freedom to organize its proper plans related to the COVID-19 situation such as duplicating Hand-on sessions to respect social distancing.
Conclusion
As healthcare professionals and academic educators, we have to be prepared to face with this outbreak since there is currently no specific treatment, with demonstrated efficacy, against Covid-19. Our aim during the acute phase of the outbreak was to maintain a basic service providing phone advices, triaging, and writing prescriptions for analgesia and appropriate medication in order to reduce pressure on the system wherever possible. Moreover, it was crucial not to risk compromising the safety of dental staff, academics, and students. Following the acute phase of the outbreak, the government, the different associations and the university will have to work together both to support dental practices preparing to re-open and to deliver the most appropriate curriculum for dental students.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author Contributions
We declare that all authors have contributed significantly and are in agreement with the manuscript.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The handling Editor declared a past co-authorship with the author AG.
Acknowledgments
Figure was created with BioRender.com.
References
1. European Union. Directive 2005/36/CE du parlement europén et du conseil. J Off l'Union Euro. (2005) 22–142.
2. CNEOC. CNEOC. Collège des Enseignats en Odontologie Conservatrice. (2020). Available online at: http://www.cneoc.eu (accessed June 4, 2020).
3. Haute Autorité de Santé. Traitement Endodontique. Texte Court Du Rapport d' Évaluation Technologique. Saint-Denis-la-Plaine (2008) 1–14.
4. Société Française d'Endodontie. SFE. Available online at: https://sfe-endo.fr
5. Ather A, Patel B, Ruparel NB, Diogenes A, and Hargreaves KM. Coronavirus disease 19 (COVID-19): implications for clinical dental care. J Endod. (2020) 46:584–95. doi: 10.1016/j.joen.2020.03.008
6. Yu J, Zhang T, Zhao D, Haapasalo M, and Shen Y. Characteristics of endodontic emergencies during coronavirus disease 2019 outbreak in Wuhan. J Endod. (2020) 46:730–5. doi: 10.1016/j.joen.2020.04.001
7. Conseil National Ordre des chirurgiens-dentistes. Guide Soignant-Recommendations Transitoires. (2020). Available online at: http://www.ordre-chirurgiens-dentistes.fr/uploads/media/Recommandations_de__confinement_01.pdf (accessed May 19, 2020).
9. Information-Dentaire. Covid-19 : ≪ la Convention Dentaire Sera Adaptée ≫ Assurent Les CDF. Première Réunion avec la CNAM le 12 juin. (2020). Available online at: https://www.information-dentaire.fr/actualites/covid-19-la-convention-dentaire-sera-adaptee-assurent-les-cdf-premiere-reunion-avec-la-cnam-le-12-juin/ (accessed June 15, 2020).
10. Information-Dentaire. Covid-19 : seuls 2 % Des Professionnels Des Cabinets Dentaires N'ont Pas Repris Leur Activité. (2020). Available online at: https://www.information-dentaire.fr/actualites/covid-19-seuls-2-des-professionnels-des-cabinets-dentaires-n-ont-pas-repris-leur-activite/ (accessed August 07, 2020).
Keywords: COVID-19, dental education, practice, outbreak, curriculum
Citation: Gaudin A, Arbab-Chirani R and Pérez F (2020) Effect of COVID-19 on Dental Education and Practice in France. Front. Dent. Med. 1:5. doi: 10.3389/fdmed.2020.00005
Received: 04 June 2020; Accepted: 10 July 2020;
Published: 19 August 2020.
Edited by:
Johnah Galicia, University of the Pacific, United StatesReviewed by:
Sheng Zhong, Independent Researcher, Minneapolis, United StatesObadah Austah, King Abdulaziz University, Saudi Arabia
Copyright © 2020 Gaudin, Arbab-Chirani and Pérez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Alexis Gaudin, YWxleGlzLmdhdWRpbkB1bml2LW5hbnRlcy5mcg==