 Claudio Pizzolato1,2
Claudio Pizzolato1,2 David G. Lloyd1,2*
David G. Lloyd1,2* Rod S. Barrett1,2
Rod S. Barrett1,2 Jill L. Cook3
Jill L. Cook3 Ming H. Zheng4
Ming H. Zheng4 Thor F. Besier5
Thor F. Besier5 David J. Saxby1,2
David J. Saxby1,2- 1School of Allied Health Sciences, Griffith University, Gold Coast, QLD, Australia
- 2Gold Coast Orthopaedic Research and Education Alliance, Menzies Health Institute Queensland, Griffith University, Gold Coast, QLD, Australia
- 3La Trobe Sport and Exercise Medicine Research Centre, La Trobe University, Melbourne, VIC, Australia
- 4Centre for Orthopaedic Translational Research, School of Surgery, University of Western Australia, Nedlands, WA, Australia
- 5Auckland Bioengineering Institute and Department of Engineering Science, University of Auckland, Auckland, New Zealand
Musculoskeletal tissues respond to optimal mechanical signals (e.g., strains) through anabolic adaptations, while mechanical signals above and below optimal levels cause tissue catabolism. If an individual's physical behavior could be altered to generate optimal mechanical signaling to musculoskeletal tissues, then targeted strengthening and/or repair would be possible. We propose new bioinspired technologies to provide real-time biofeedback of relevant mechanical signals to guide training and rehabilitation. In this review we provide a description of how wearable devices may be used in conjunction with computational rigid-body and continuum models of musculoskeletal tissues to produce real-time estimates of localized tissue stresses and strains. It is proposed that these bioinspired technologies will facilitate a new approach to physical training that promotes tissue strengthening and/or repair through optimal tissue loading.
Introduction
Musculoskeletal diseases, such as osteoarthritis and tendinopathy, impose substantial burden on individuals and health care systems. As a community of scientists and clinicians, we have been largely ineffective in managing musculoskeletal diseases, as current prevalence, incidence, and socioeconomic burden are at alarming levels and projected to increase sharply in coming decades (Hunter et al., 2014). In particular, we have a limited understanding of how physical behavior, i.e., whole-body mechanics, influences tissue state (Forwood and Burr, 1993), and this could underpin our failure to cure, or curb, these prevalent, harmful, and costly diseases. A case in point is the study of the effects of physical activity on cartilage morphology. Studies of animals (Kiviranta et al., 1987, 1988, 1992; Newton et al., 1997) and humans (Jones et al., 2000, 2003; Roos and Dahlberg, 2005) have reported increased physical activity to be associated with positive structural and biochemical adaptations in weight-bearing joints, while other studies have reported no effects of physical activity on bulk measures of cartilage morphology (Eckstein et al., 2002, 2006).
The failure to effectively treat musculoskeletal disease is frustrating for scientists and clinicians alike. We possess a wealth epidemiologic data detailing risk factors for many musculoskeletal diseases, e.g., increased age, female sex, body mass, prior joint trauma, obesity, abnormal physical activity levels, and joint structural deformity (Felson et al., 1997, 2000, 2013; Cooper et al., 2000; Coggon et al., 2001; Lohmander et al., 2004, 2007; Roemer et al., 2009; Andriacchi et al., 2015). At tissue- and sub-tissue levels, studies have explored the effect of loading on structure and biology (Radin and Paul, 1971; Simon et al., 1972; Radin et al., 1973, 1984; Rubin and Lanyon, 1985; Forwood and Turner, 1995; Wang et al., 2013, 2015; Joo Kim et al., 2016). However, integrating experimental results with whole-body-, tissue-, and cell-level computational models, and using these models to modulate physical behavior to affect musculoskeletal tissue health remains challenging (Erdemir et al., 2015). In a recent narrative review, Ng et al. (2017) proposed physical therapy to enhance and promote tissue regeneration, linking external mechanical stimuli to tissue mechanobiology. In line with Ng et al. (2017), we describe an approach to deterministically quantify the link between physical behavior and tissue mechanobiology, inspired by integration of biomedical technologies (i.e., wearable devices, contemporary motion capture, and medical imaging) coupled to computational models of joints and musculoskeletal tissues.
Wearable body sensors and systems for “Quantified-Self” are set to transform how people interact with their environment and may facilitate personalized training and rehabilitation programs in the future. Biofeedback is a psychophysical process to augment awareness of afferent signals from sensory receptors in the human body. In the case of musculoskeletal tissues, biofeedback can be used to increase awareness and modify physical behavior (Sigrist et al., 2013). However, current rehabilitation and training protocols which incorporate biofeedback to modulate physical behavior target external biomechanics, such as the knee adduction moments (Barrios et al., 2010; Shull et al., 2011, 2013a,b; Wheeler et al., 2011) or gait spatiotemporal parameters (Wrigley et al., 2009; Erhart-Hledik et al., 2017). Eternal biomechanics are readily measured or calculated, and thus viable for use in biofeedback paradigms. Unfortunately, external biomechanics have tenuous relationships with internal biomechanics, such as articular contact loads (Walter et al., 2010; Winby et al., 2013; Saxby et al., 2016b).
Musculoskeletal tissue stresses and strains are potentially superior to external biomechanics for use in biofeedback paradigms because they are physically coupled to the processes of mechanotransduction, whereby mechanical signals are registered as biologic stimuli, and result in cell- and tissue-level adaptations controlled by biologic regulatory mechanisms. However, musculoskeletal tissue stresses and strains have not been used in biofeedback technologies, because their computation is non-trivial, and depends on a complex interplay of multiple factors, including external biomechanics, neural control, tissue morphology and micro-architecture, and material properties (Figure 1). Importantly, recent advances in neuromusculoskeletal modeling have enabled real-time prediction of whole-body kinematics and external loading (Pizzolato et al., 2017a), as well as musculoskeletal tissue loading, such as muscle-tendon unit and articular contact forces during walking gait (Pizzolato et al., 2017b). Real-time musculoskeletal modeling can now be coupled to models of internal tissue mechanics and mechanobiology, and used to provide feedback to target training for tissue strengthening and repair.
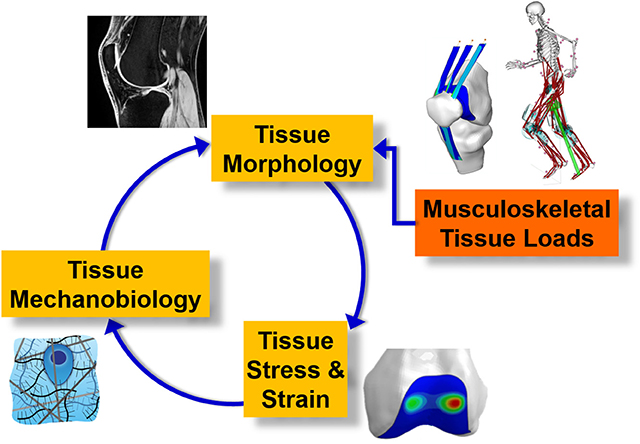
Figure 1. Schematic of complex dynamic interplay between external rigid body biomechanics, internal tissue biomechanics, tissue mechanobiology, and tissue state.
In this narrative review we present an overview of (1) the known mechanical stimuli for promoting positive tissue adaptation in musculoskeletal tissues, (2) how local tissue stresses and strains can be estimated using computational methods, (3) an approach to estimating musculoskeletal tissue stresses/strains in real-time, and (4) challenges and future directions for research in this area.
Mechanobiology and the Optimal Mechanical Environment for Musculoskeletal Tissues
Mechanobiology is the study of the effect of mechanical stimuli on tissue biology. It is well-established that mechanical loading plays an essential role in (1) musculoskeletal tissue development throughout human maturation (Carter, 1987; Carter and Wong, 1988a,b, 1990; Wong and Carter, 1990; Carter et al., 1998, 2004; Beaupre et al., 2000), (2) maintenance of mature structures (Frost, 1988, 1990a,b,c,d), and (3) healing following injury, e.g., bone fracture (Pivonka and Dunstan, 2012). In particular, musculoskeletal tissues, such as articular cartilage, tendon, and bone, respond to strains by modulating tissue composition and organization. Generally, strains depend on the nature of applied loading, i.e., magnitude, location, orientation, duration, and frequency, as well as structural state of the object, i.e., morphology and material properties (Figure 1). Important to our study of musculoskeletal tissues, identical loads applied to different tissues (e.g., cartilage vs. bone vs. tendon), or same tissues but of different structural features (e.g., healthy vs. compromised, developing vs. mature), will produce different strains and eventually different biologic responses. Thus, to develop therapies targeting positive musculoskeletal tissue adaptations we must quantify relevant states. Equally important, if we wish evaluate therapeutic effectiveness we must also quantify changes to tissue states in response to those interventions.
Estimating the State of Musculoskeletal Tissue
Musculoskeletal tissue state encompasses tissue morphology and function, both of which may be non-invasively assessed using medical imaging. Morphology, which encompasses all spatial descriptions of an object, can be measured using different medical imaging modalities, such as computed tomography (CT), magnetic resonance (MR), and ultrasound (US).
Computed tomography is well-suited to the study of bone and provides high-resolution images that can be automatically- or semi-automatically segmented to render volumetric representations (Dufresne, 1998). Peripheral quantitative CT can be used to image cortical and trabecular bone microstructure (Lespessailles et al., 2017), which are important structural features to include in analysis of bone remodeling (Hambli, 2011). However, CT exposes tissues to ionizing radiation and may not be suitable for certain clinical or developing populations.
Magnetic resonance imaging is a powerful modality that does not produce ionizing radiation, and can be used to image a wide range of musculoskeletal tissues (Hunter et al., 2015). However, individuals with implanted medical devices (e.g., cardiac stimulators) or ferrous prosthetics cannot safely undergo MR imaging. Unlike CT, MR images require manual segmentation to produce three-dimensional reconstructions of musculoskeletal tissues. Currently, manual segmentation is time consuming, but advances in image auto-segmentation (Mimics, Materialize NV, Leuven, Belgium) will hopefully reduce labor demands. Once MR images can be rapidly segmented, this will make MR imaging a routine process to assess musculoskeletal tissue morphology.
Ultrasound is an inexpensive, non-invasive, and non-radiating modality to image musculoskeletal tissues. Importantly, US can accurately measure muscle morphology (Barber et al., 2009), track muscle fascicles during contractions (Cronin et al., 2011; Gillett et al., 2013), and measure in vivo tendon morphology at rest and under load in healthy (Obst et al., 2014a,b) and pathologic tendon (Nuri et al., 2017). In addition to muscle-tendon applications, US has been used to measure bone landmark coordinates (Peters et al., 2010; Passmore and Sangeux, 2016) and make in vivo clinical measurements of bone alignment (Passmore et al., 2016). However, limited signal penetration into the body means that many deep anatomic structures cannot be imaged using US. Furthermore, deformation of soft tissues out of the imaging plane impairs measurement fidelity. To summarize, CT, MR, and US are imaging modalities capable of measuring musculoskeletal tissue morphology, however, morphology is only one component of tissue state, and alone is an insufficient indicator of tissue function and integrity.
Tissue function is related to tissue mechanical properties, such as stiffness and strength. As many pathologic tissue changes are accompanied by changes in tissue elasticity (Ophir et al., 1991), measures of tissue mechanical properties may serve as surrogate measures of tissue health and integrity. Henceforth, we will refer to medical imaging modalities used to assess musculoskeletal tissue mechanical properties as “functional imaging.” Elastography is a class of functional imaging, and is the study of elastic properties of materials. Elastography uses principles from the physics of wave propagation to quantify tissue mechanical properties (Ophir et al., 1991). In general, an internally- or externally- generated stimulus causes tissue deformation, which is measured and related to tissue elastic modulus (Yamakoshi et al., 1990). Relaxography is another class of functional imaging, whereby MR is used to indirectly assess tissue integrity by measuring time constants, e.g., T2, , and T1ρ, associated with the slow motion of water molecules. Relaxography has emerged as a potent method to study and detect early signs of articular cartilage degeneration (Baum et al., 2013). As cartilage degenerates, its extracellular matrix is disrupted and proteoglycan content is reduced, which results in increased water content and motility. Relaxographic imaging is sensitive to early degenerative changes, as T2 relaxation times associated with healthy cartilages (~25–45 ms) are lower than those associated with degenerated cartilages (Dunn et al., 2004). Overall, there are several imaging modalities capable of assessing musculoskeletal tissue state, thus enabling creation of personalized musculoskeletal tissue models as well as quantifying intervention outcomes. However, it is first necessary to identify the optimal mechanical environments of each musculoskeletal tissue, which will serve as targets for bioinspired rehabilitation and training.
Just as hyper-physiologic loading can cause musculoskeletal tissue damage (Bonnevie et al., 2015; Christiansen et al., 2015), load deprivation due to low-gravity (Lang et al., 2006), or spinal-cord injury (Vanwanseele et al., 2002, 2003) causes tissue atrophy and weakening. More subtle changes in tissue loading can also affect tissue properties. For example a lower than normal knee contact force following orthopedic surgery has been associated with future onset of knee osteoarthritis (Wellsandt et al., 2016). Specifically, reductions of 10–20% of a body weight in the medial contact forces 6-months after anterior cruciate ligament reconstruction were associated with onset of medial knee osteoarthritis 5-years post-operation (Wellsandt et al., 2016). Similarly, animal experiments of unloading the weight-bearing limbs following knee ligament transection found subsequent muscle atrophy and loss of trabeculae (Anderson et al., 2016). Likewise, the human proximal tibia experiences substantial bone mineral density loss over the first year following anterior cruciate ligament reconstruction (Mundermann et al., 2015), which may be related to lower magnitude ambulatory tibiofemoral contact forces (Saxby et al., 2016a; Wellsandt et al., 2016). Overall, these results re-inforce the concept that inappropriate loading, due to over- and/or under-loading, precede articular tissue degeneration. It therefore follows that each tissue must have an optimal mechanical stimulus or “sweet spot” which maximizes anabolic tissue adaptation, where loads are neither too high to cause tissue damage, or too low to result in tissue degeneration (Figure 2).
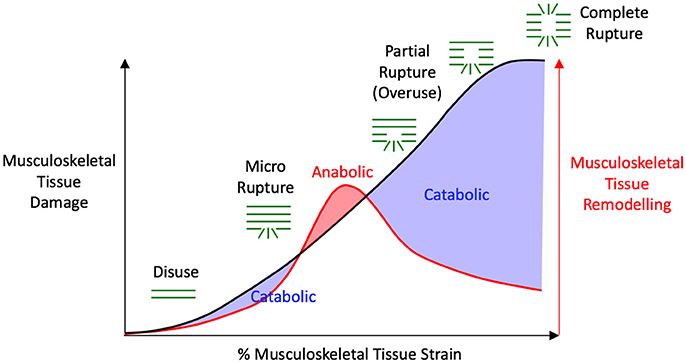
Figure 2. Schematic of mechanobiologic interplay between tissue strains that induce damage and remodeling. Within the anabolic “sweet spot” (i.e., red shaded area), tissues experience hypertrophy and improved mechanical properties. Within catabolic regions (i.e., two blue shaded areas), which are brought about due to over- or under-loading, tissues atrophy or degenerate, and this results in increased compliance and loss of strength. Adapted from Wang et al. (2013).
Tendon Optimal Mechanical Environment
An illustrative example of a “sweet spot” in tissue regulation is drawn from in vitro studies of Achilles tendon. The Achilles tendon is a viscoelastic structure that links calf muscles, i.e., gastrocnemii and soleus, with the calcaneus bone of the foot, thus spanning the ankle joint. The Achilles tendon is crucial to common ambulatory tasks, such as walking, running, and jumping, through its role in biomechanical power generation and movement efficiency. When conditioned in a bioreactor, excised sections of Achilles tendons have shown optimal biomechanical response when subjected to ~6% cyclic tensile strains (Wang et al., 2013, 2015). Cyclic 6% tensile strains, 0.25 Hz loading cycle, 8 h per day, maintained tendon homeostasis (Wang et al., 2013) and, importantly, regenerated injured tendon (Wang et al., 2015). Consistent with the idea of over- and under-loading as mechanisms for tissue degeneration, tendon tensile strains below 3% or above 9% disrupted extracellular matrix (Wang et al., 2013), while tenocytes optimally responded to 4–6% strains (Joo Kim et al., 2016). These results reinforce the need to target specific strain ranges to maintain and repair tissue.
Cartilage Optimal Mechanical Environment
Articular cartilage caps the terminal regions of long bones involved in synovial joints, and provides a smooth ultra-low friction bearing surface for articulation. Articular cartilage is considered biphasic, consisting of a solid phase composed primarily of organized collagenous extracellular matrix interposed with chondrocytes, highly charged macromolecules, and immersed in an ionized interstitial fluid phase. Interaction between solid and fluid phases causes the mechanical behavior of cartilage, i.e., anisotropy, strength, and viscoelasticity (Mow et al., 1980; Armstrong and Mow, 1982). Indeed, the network of collagens and macromolecules of the extracellular matrix provide enormous resistance to internal fluid motility, primarily through friction. Consequently, during rapid loading of cartilage, as occurs during sport and activities of daily living, cartilage behaves as a nearly incompressible isotropic material. Internal resistance to fluid flow is an essential mechanism by which cartilage resists externally applied compression. However, as cartilage is avascular (Buckwalter, 2002; Buckwalter and Brown, 2004), large resistance to internal fluid flow prevents effective transport of materials and cells to injury sites. When cartilage deteriorates due to age, injury, or disease, it becomes more compliant (Setton et al., 1999). Consequently, collagen networks in the extracellular matrix experience larger, and potentially injurious, strains.
Limited interstitial motility combined with the avascular nature of cartilage, results in minimal regenerative capabilities (Newman, 1998; Buckwalter, 2002; Buckwalter and Brown, 2004). Understandably, research has focused on engineering cartilage implants and effective scaffolding to promote seamless uptake of implanted constructs into native cartilage. A recent review of literature found in vitro compressive strains of >20% applied at 0.5–1 Hz, were optimal for promoting cartilage cultivation (Natenstedt et al., 2015). A 20% strain is in the middle of the physiologic range experienced by cartilage (Grodzinsky et al., 2000), and 0.5–1 Hz loading rates are similar to the natural knee loading frequency during human gait. Thus, ~20% and 0.5–1 Hz cartilage strain and loading rate, respectively, provide logical targets to condition cartilage to prevent future degeneration, and may be effective to attenuate, stop, and even reverse degeneration in cases of established disease.
Bone Optimal Mechanical Environment
In vitro studies provide a rich source of direct measurements of strains that stimulate bone remodeling, as well as strains that injury or fracture bone. As many strain measures in the literature were acquired from experiments that did not incorporate bone dynamics, they should be considered time-independent mechanical targets, that may stimulate bone remodeling (Lanyon et al., 1975; O'connor et al., 1982; Rubin and Lanyon, 1985; Ehrlich and Lanyon, 2002). Different bone components, i.e., cancellous and cortical bone, may have different optimal strain ranges required to elicit adaptive remodeling. However, a range of ~200–1,000 με (1 με = 1 microstrain; 1 με = 0.0001% strain) represents everyday strains. During vigorous physical activities, such as sprinting, bone strains may reach peak values of ~2,000–3,000 με (Burr et al., 1996) and strain rates of ~10,000–50,000 μεs−1 (Lanyon et al., 1975). Even during vigorous physical activities, bone strains and strain rates do not necessarily damage tissue, as injurious strains are ~25,000 με in tension or compression directed longitudinally (Reilly and Burstein, 1974). Bone durability is first due to its innate capacity to withstand large stresses at low strain rates, i.e., ~80–170, ~100–300, and ~150–240 MPa in tensile, compressive, and bending modes, respectively (Reilly and Burstein, 1974). Second, bone is a viscoelastic material and its stiffness increases when subject to high strain rates, for example during running and jumping. Bone strains during strenuous physical activities have been reported to be ~10% of ultimate failure, well below bone fracture threshold and therefore considered safe healthy for individuals (Burr et al., 1996). Low impact and activities such as walking do not appear to be oesteogenic.
Estimating the Mechanical Environment of Musculoskeletal Tissues
Musculoskeletal tissue state varies between individuals, and is affected by disease processes. To personalize therapy, we must account for subject-specificity, such that training programs can be tailored to the individual. A further technical challenge is that we need to estimate musculoskeletal tissue mechanics in real-time, providing an appropriate form of biofeedback to enable individuals to volitionally modulate tissue mechanics during rehabilitation, recreation, or daily activities. To achieve this goal we must merge whole-body representations of human physical behavior with models of musculoskeletal tissue mechanics and mechanobiology within efficient computational frameworks.
Currently, there is no feasible method to directly measure in vivo loading applied to, and stresses/strains within, musculoskeletal tissues in native human joints. Articular contact forces can be measured in cadavers through a combination of robotic control and mathematical modeling (Wang et al., 2014) or by inserting pressure sensitive film between articulating surfaces (Ihn et al., 1993). However, a valid method of applying physiologic muscle, body, and inertial loads to cadavers has not been reported, thus casting doubt whether these measurements are representative of in vivo loading. Contact forces can also be measured by instrumenting prostheses used in arthroplasty, as has been done at knee (D'lima et al., 2005, 2006; Heinlein et al., 2007, 2009; Fregly et al., 2012), hip (Rydell, 1966; English and Kilvington, 1979; Bergmann et al., 2010), and shoulder (Bergmann et al., 2007) joints. Contact loads measured by instrumented prostheses provide critical information to implant designers regarding the nature of the mechanical demands placed upon these devices. Unfortunately, instrumented prosthetic implants are only appropriate for measuring contact loads in arthroplasty patients, who are typically elderly individuals with substantially degenerated joints and peri-articular muscle atrophy. Furthermore, arthroplasty, by definition, does not preserve the native joint and restricts the activity types that could be studied in these patients, e.g., it is unethical to ask an elderly knee arthroplasty patient to perform vigorous athletic movements. Consequently, contact loads sustained by implants are unlikely to be representative of contact loads in native joints of young physically active populations.
In addition to articular contact forces, muscle-tendon unit forces have also been directly measured in both animals (Walmsley et al., 1978; Hodgson, 1983; Herzog et al., 1992) and humans (Gregor et al., 1987; Komi et al., 1987; Fukashiro et al., 1995) by surgically implanting mechanical gauges. Proficient surgical implantation results in minimal inflammatory response, and instruments may left in situ in animals for days or even weeks. However, extrapolating in vivo animal muscle-tendon force measurements to humans is questionable and certainly of limited clinical relevance. In humans, surgical implantation of strain gauges into tendon may affect an individual's physical behavior, thus limiting ecologic validity of the measurements. Furthermore, muscle-tendon forces are subject-, task-, and state-specific, thus limiting applicability of measurements from an individual performing a specific task to another individual, movement or control task, or the same individual at a later date, i.e., following an intervention, suffering an injury, or onset of disease. Given the serious limitations of direct measurement of musculoskeletal tissue loads, researchers have used computational neuromusculoskeletal to predict musculoskeletal tissue loading.
Neuromusculoskeletal Models to Estimate Musculoskeletal Tissue Loading
Neuromusculoskeletal models are bioinspired mathematical representations of specific neurologic, physiologic, and anatomic characteristics of an individual (Hatze, 1977; Buchanan et al., 2004, 2005; Lloyd et al., 2005). Neuromusculoskeletal models may be used to estimate muscle (Lloyd and Besier, 2003; Erdemir et al., 2007), ligament (Shelburne and Pandy, 1997; Pandy and Sasaki, 1998; Lloyd et al., 2005; Shelburne et al., 2005), and articular contact forces (Shelburne et al., 2005; Winby et al., 2009; Gerus et al., 2013; Manal and Buchanan, 2013; Erdemir et al., 2015; Walter et al., 2015; Saxby et al., 2016b; Smith et al., 2016; Konrath et al., 2017), and have been deployed across a wide range of scientific, industrial, and clinical applications, such as investigating fundamental properties of human motor control (Haeufle et al., 2014; Sartori et al., 2015), evaluating ergonomic demands of automotive operation (Rasmussen et al., 2009), and informing medical device designs by predicting in vivo loading conditions (Marra et al., 2015). Typically, structural characteristics used in a model are based on measurements from a small number of cadavers, and subsequently used as a generic template for each analysis. Bone dimensions and mass-inertia properties in a generic template are linearly scaled to match subject's dimensions (Delp et al., 1990), thus providing a basic level of model personalization. Using generic templates facilitates rapid and routine use of neuromusculoskeletal models, but scaled generic models are often poor representations of an individual's musculoskeletal anatomy, which may lead to inaccurate results, spurious conclusions, and potentially detrimental clinical decisions. For example, linear scaling of a generic model template may result in incorrect representation of muscle moment arms (Arnold et al., 2000; Scheys et al., 2008) and consequently erroneous joint contact force estimates (Lenaerts et al., 2009; Gerus et al., 2013; Wesseling et al., 2016).
Several aspects of neuromusculoskeletal models can be personalized to the individual to improve simulation results. Bone morphology and joint mechanics have been shown to influence kinematics and kinetics estimates (Brito da Luz et al., 2016; Kainz et al., 2016), and knee contact forces have been shown to be sensitive to tibiofemoral alignment (Lerner et al., 2015). Skeletal geometry also affects muscle-tendon paths and insertion points, which in turn define muscle-tendon lines of action, influencing both muscle-tendon lengths and moment arms. Overall, better representation of an individual's musculoskeletal anatomy has been shown to produce more realistic results, e.g., improved representation of muscle-tendon moment arms, improved knee (Gerus et al., 2013) and hip (Modenese et al., 2013) contact forces estimates.
Muscle activation patterns are known to vary between individuals and controls tasks (Tax et al., 1990; Buchanan and Lloyd, 1995), and are affected by training (Menegaldo and Oliveira, 2011) and pathology (Besier et al., 2009). Incorporating experimental measures of muscle activation patterns into neuromusculoskeletal models adds an important dimension of personalization. Electromyography (EMG)-informed neuromusculoskeletal models (Manal et al., 2002; Lloyd and Besier, 2003; Manal and Buchanan, 2013; Sartori et al., 2014; Pizzolato et al., 2015) are a class of neuromusculoskeletal models sensitive to variations in motor control. Specifically, EMG-informed neuromusculoskeletal models use experimentally measured muscle excitations and movement patterns to account for complex interplay between external biomechanics and muscle recruitment to estimate musculoskeletal tissue loadings, i.e., joint, muscular, ligamentous, and articular contact loads, that may serve as boundary conditions for continuum mechanics analysis.
Finite Element Method to Estimate Musculoskeletal Tissues Mechanical Environment
The finite element method (FEM) is a well-established computational method used in many branches of engineering. In a FEM model, the real system is discretized into a field of elements of known geometries and material properties, from which constitutive equations may be developed. The model system dynamics are then equilibrated by imposing a set of boundary conditions, e.g., musculoskeletal tissue loads informed by a neuromusculoskeletal model. Halloran et al. (2010) applied this combined neuromusculoskeletal and FEM modeling to foot and ankle strains, while Besier et al. (2009) verified predicted patellofemoral stresses/strains using measurements of cartilage deformation acquired in a vertical bore MR unit. Recently, others have explored tibiofemoral cartilage stresses/strains during gait (Shim et al., 2016; Smith et al., 2016) and acetabulum stress distributions in relation to bone remodeling (Fernandez et al., 2014). These studies have shown the potential of the FEM models, but the models employed were not fully personalized.
Generating personalized FEM models of tissue requires both morphology and material properties. As previously described, different imaging modalities can be used to directly acquire tissue-specific morphology, but non-invasive methods to estimate material properties are scarce. Musculoskeletal tissues have a heterogeneous multiphasic structure, resulting in anisotropies and non-linear time-varying behavior (Freutel et al., 2014), thus making the estimation of material properties challenging. Relaxography (Labadie et al., 1994) is a powerful tool to assess tissue function, but it only provides measures which correlate with, but do not quantify, tissue material properties (Lammentausta et al., 2006). Elastography (Ophir et al., 1991) can provide direct measurement of musculoskeletal tissue stiffness by analyzing the response of tissue to external stimuli. In MR elastography, low frequency vibrations are externally introduced to the body by means of electromechanical devices, while multiple images are recorded to analyse tissue response at different time points and directions (Glaser et al., 2012). Ultrasound elastography works by the same principle as MR elastography, but the external stimuli can be provided by the US transducer itself. Ultrasound-based shear-wave elastography has recently been applied to musculoskeletal tissues (Eby et al., 2013) to quantify stiffness, but is limited to superficial tissues and subject to errors due to probe positioning (Brandenburg et al., 2014). Reverse FEM could also be used to estimate tissue material properties, whereby tissue is subject to multiple and explicitly known applied loading conditions that alter morphology. A numerical optimization then estimates a set of material properties best fitting the measured morphology change (Hansen et al., 2017).
Informing tissue material properties in FEM models through non-invasive imaging would provide a level of personalization well beyond current standard approaches, which typically apply literature values established through experiments performed on cadavers. Indeed, tissue material properties are specific to individuals and are affected by aging, training, injury, and disease (Arokoski et al., 2000; Buckwalter, 2002; Buckwalter and Brown, 2004). Different tissue stress and strain patterns will arise from FEM simulations that use different tissue material properties, even when composed of identical tissue morphology and subjected to identical boundary conditions. Finally, simulations of musculoskeletal tissue mechanics may use physiologic and personalized boundary conditions informed by neuromusculoskeletal models (Besier et al., 2005, 2009; Fernandez et al., 2014). Overall, when FEM models of musculoskeletal tissues are informed by measurements of subject-specific morphology, material properties, and boundary conditions, they are powerful tools to understand musculoskeletal tissue mechanics.
Finite Element Method to Estimate Musculoskeletal Tissue Remodeling
Considerable research focus has been applied to studying relationships between applied tissue loading and morphology, with a fundamental assumption that tissue health may be assessed through structural analysis (e.g., thicker cartilage is indicative of healthy cartilage; Koo and Andriacchi, 2007). Rigid-body computational models have been used to determine external joint or articular loads, which in turn have been compared to measures of articular tissue structure using linear statistics (Koo and Andriacchi, 2007; Koo et al., 2011; Scanlan et al., 2013; Van Rossom et al., 2017). However, primary focus on applied loading may not be appropriate, as other biomechanical signals, such as extracellular fluid motion in bone (Zadpoor, 2013; Villette and Phillips, 2016) or bone strain energy (Kerner et al., 1999), are physically closer to cellular mechanisms of remodeling and have been shown to influence tissue adaptation. Simulations of trabecular remodeling have been performed whereby structural modifications were driven by local mechanical criteria, e.g., minimizing density of material anisotropy with respect to principle stresses (Fyhrie and Carter, 1986) or non-uniformity in local stresses (Adachi et al., 1997; Tsubota et al., 2002). Such simulations were able predict trabecular distributions consistent with experimental observations (Fyhrie and Carter, 1990), and results were highly sensitive to loading condition complexity. When complex loading patterns were applied to FEM models with embedded bone remodeling algorithms, predicted bone material property distributions were consistent with ex vivo imaging (Geraldes et al., 2016). Similarly, features such as bone cortical thickness and regional femoral trabecular density were better predicted when complex physiologic loads were applied compared to simple axially oriented compressive loads (Geraldes et al., 2016). When complex muscle loading patterns were included in FEM simulations of femoral bone remodeling in the context of prosthetic hip implants, simulations predicted bone retention patterns in regions of muscle attachment, which is not predicted by FEM models using simple idealized boundary conditions (Bitsakos et al., 2005). These results suggest incorporation of complex biomechanical loads into FEM models is required to predict correct spatial distribution and peculiar features of musculoskeletal tissue structure.
The complex biomechanical loads sustained by the human body are generated by non-linear muscle dynamics and their interaction with convoluted three-dimensional musculoskeletal architecture. Including muscle dynamics into FEM models directly affects spatial distribution of musculoskeletal tissue strains, and hence influences predictions of tissue remodeling (Duda et al., 1998). When pairing together computational rigid-body neuromusculoskeletal and FEM models, the degrees of freedom associated with the respective models must be consistent (Phillips et al., 2015). For example, the popular musculoskeletal modeling software OpenSim (Delp et al., 2007) enables users to define complex joint motions that are both arbitrarily bounded and computationally efficient (Seth et al., 2010). The OpenSim model may then be used to solve external joint and muscle loads, which can, in principle, be applied to FEM models. However, the FEM model must be constrained in an analogous manner to the OpenSim model to ensure model degree of freedom consistency. This is not a peculiar consideration of OpenSim models, rather, all hierarchical modeling frameworks which combine boundary conditions from a rigid-body simulation to a FEM model should respect this demand for consistency. In the context of bone remodeling simulations, Phillips et al. (2015) presented a method to ensure model degree of freedom consistency, but noted that the constraints of model displacement may limit scope of the analysis.
Optimal mechanical environments for musculoskeletal tissue adaptation have been provided from ex vivo, in vitro, and in silico studies. This knowledge, combined with an appreciation for modeling complexity required to estimate musculoskeletal tissue stresses and strains, leaves us well posited to move forward and apply these models in clinical contexts such as training or rehabilitation. If we can gain control of an individual's physical behavior through biofeedback paradigms, and target the optimal in vivo mechanical environment of their musculoskeletal tissues, we may be able to prevent tissue deterioration or restore health. We represent our vision in Figure 3, and its realization would be a breakthrough for rehabilitation science and medicine. However, to realize this aim, current computation processes that are performed offline must be performed in real-time.
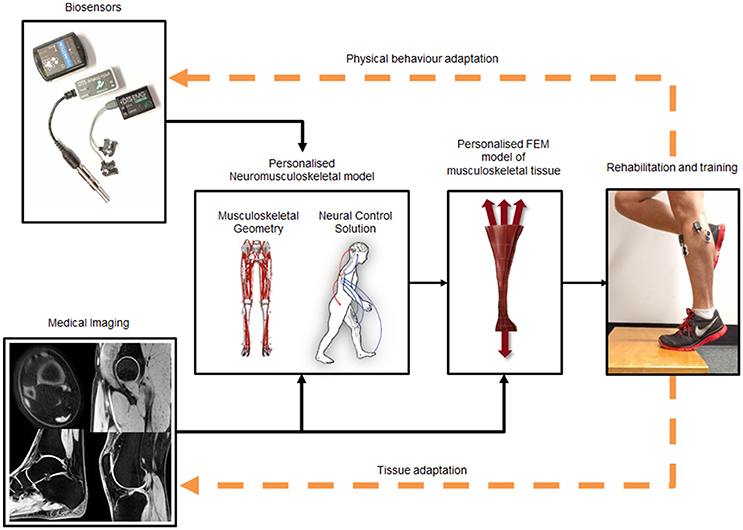
Figure 3. Framework to estimate in vivo musculoskeletal tissue stresses and strains. Medical imaging is used to create personalized musculoskeletal geometry and FEM models of the tissue of interest. Biosensors (e.g., EMG, inertial measurement units, and/or motion capture) are used to drive a neuromusculoskeletal model, which provides boundary conditions necessary for the FEM model to estimate musculoskeletal tissue stresses and strains. Tissue stresses and strains can be fed-back, in real-time, to enable the person to modify their behavior to affect tissue mechanical environment. Finally, tissue and physical behavior adaptations update the computational system indicated by orange dashed feedback arrows.
Real-time Estimation and Biofeedback of Musculoskeletal Tissue Stress and Strain
Behavioral movement changes, in the form of modulation of body kinematics and kinetics, have been used in rehabilitation to assist motor learning and improve function following injury or disease (Sigrist et al., 2013). Much research has focused on biofeedback technologies to improve movement and function in knee osteoarthritis patients (Barrios et al., 2010; Shull et al., 2013a,b; Van Den Noort et al., 2015). In these patients, larger magnitude walking knee adduction moments have been associated with structural progression of knee osteoarthritis (i.e., joint space narrowing; Miyazaki et al., 2002) and knee pain (Amin et al., 2004), making reduction of the magnitude of the knee adduction moment a logical target for physical therapy.
Numerous studies have combined biofeedback technologies with gait modification strategies to modify joint kinematics or external loads with the aim of improving health outcomes or reducing movement variability. For example, real-time visual biofeedback of upper-body posture (Hunt et al., 2011) and dynamic knee alignment (Barrios et al., 2010) have been used to reduce walking knee adduction moments in healthy individuals and knee osteoarthritis patients, respectively. Knee braces instrumented with auditory feedback have been used to reduce knee loading rates during walking (Riskowski et al., 2009), while instrumented footwear has been used to reduce lateral foot pressures through vibrotactile feedback (Dowling et al., 2010). Notably, Shull et al. (2013b) provided haptic feedback, delivered through body worn vibrating motors, to inform participants of their changes in foot progression and trunk sway during treadmill walking. This resulted in patients with knee osteoarthritis reducing their peak knee adduction moment magnitudes. However, the main limitation of modifying external kinematics and kinetics is their tenuous relationships with internal loads (Walter et al., 2010, 2015; Winby et al., 2013; Saxby et al., 2016b), which implies weaker still relationships to articular tissue stresses and strains. The reason for these poor relationships is external biomechanics cannot account for the direct effect of muscles on musculoskeletal tissue loading (Walter et al., 2010; Winby et al., 2013; Saxby et al., 2016b).
As previously discussed, neuromusculoskeletal models can provide FEM with appropriate boundary conditions to estimate musculoskeletal tissue stresses and strains (Besier et al., 2005, 2009; Fernandez et al., 2014). This may be done in an offline analysis, but real-time estimation of musculoskeletal tissue stresses and strains requires interfacing with, and enabling data flow from, external devices to modeling software to complete necessary computations within given time constraints. For neuromusculoskeletal models, this means solving kinematics, kinetics, and muscletendon forces in real-time. Muscle forces have been calculated in real-time using a static optimization method (van den Bogert et al., 2013), where an algorithm determined the minimized weighted sum of muscle forces that matched external joint moments (Van Der Helm, 1994). However, the real-time approach presented by (van den Bogert et al., 2013) was based on a generic anatomic model that could not be personalized. Model personalization, noted earlier in this review, is essential when coupling neuromusculoskeletal and FEM models of musculoskeletal tissue mechanics. Furthermore, many neuromusculoskeletal models rely on mechanical optimization to solve the muscle redundancy problem (Crowninshield, 1979; Crowninshield and Brand, 1981), however, mechanical optimization methods struggle to predict many empirical features of muscle coordination, such as patterns of muscle activation (Herzog and Binding, 1992), co-contraction (Herzog and Binding, 1993), and force sharing (Binding et al., 2000). To our knowledge, the first use of a real-time EMG-informed neuromusculoskeletal model was by Manal et al. (2002), and first applied to musculoskeletal tissue loading in Achilles tendon rehabilitation by Manal et al. (2012). These papers advanced the field and should be acknowledged as pioneering, but were limited in application to quasi-static movements and a single joint with few degrees of freedom. Recently, Pizzolato et al. (2017b) developed software, based on OpenSim (Delp et al., 2007), to calculate full-body kinematics and kinetics (Pizzolato et al., 2017a), as well as musculoskeletal tissue loading (Pizzolato et al., 2015, 2017b), in real-time. Their method is fully extensible to other joints and musculoskeletal tissues, but is currently limited to expensive and immobile laboratory-based stereophotogrammetry systems (Pizzolato et al., 2017b).
Wearable sensors that accurately estimate human kinematics are a promising alternative to laboratory-based measurement systems. Linear accelerometers have been used for many years to quantify movement patterns relative to the gravitational field and ambulatory temporal-spatial parameters (Kavanagh and Menz, 2008), but their estimates of joint kinematics are limited by signal drift caused by integration errors (Djuric-Jovicic et al., 2011). Improvements in microelectromechanical systems have enabled embedding tri-axial accelerometer, gyroscope, and magnetometer into a single sensor. These integrated sensors are known as inertial measurement units and are able to estimate spatial orientation (Sabatini, 2006; Madgwick et al., 2011) and, when used in combination with anatomic models, joint angles. Strain sensors are another class of promising wearable sensors that can be used to estimate joint angles (Nakamoto et al., 2016). Strain sensors are low profile, flexible, and can be easily embedded into garments or mounted on the skin (Amjadi et al., 2016). To date, strain sensors have been used in biomechanics primarily to classify movement (Mattmann et al., 2007) or estimate single joints angles (Nakamoto et al., 2016). However, continuous technologic improvements in smart textiles (Honarvar and Latifi, 2017) may soon lead to advanced garments capable of estimating full-body kinematics.
Measuring or estimating reaction forces between body and ground is required to correctly estimate load applied to specific musculoskeletal structures, such as joints and ligaments. In laboratory conditions, ground reaction forces are acquired via ground mounted force plates, but alternative solutions are required for applications in the real-world. Pressure-sensitive insoles can be used to estimate the normal component of the ground reaction force, but they neglect shear components (Chesnin et al., 2000). Conversely, shoes instrumented with tri-axial force sensors have shown agreement with force plates for all components of the ground reaction force vector (Liedtke et al., 2007). Alternative to measurements, deep learning algorithms have been shown to correctly estimate ground reaction forces during walking (Oh et al., 2013). However, these data-driven models require big data as training sets. Mechanical approaches can be used to solve dynamics of motion and estimate ground reaction forces without body-worn force sensors. For example, the zero-point moment is an algorithm developed for humanoid robots (Xiang et al., 2009) that has also been successfully applied human biomechanics (Fluit et al., 2014; Dijkstra and Gutierrez-Farewik, 2015). However, to correctly estimate ground reaction forces, full-body kinematics and subject-specific musculoskeletal models are required (Fluit et al., 2014).
Overall, advances in wearable sensors, i.e., smaller, lighter, low-power, and integrated sensor systems, will enable novel real-world applications (Brodie et al., 2008). Currently, intrinsic limitations and measurement inaccuracies associated with these devices prevent their use in advanced biomechanical analysis. Combining wearable sensors with sophisticated biomechanical models may help to minimize the limitations associated with wearable sensors. Realistic musculoskeletal models, such as those offered by OpenSim (Delp et al., 2007), associated with probabilistic frameworks that adequately model wearable sensor inaccuracies (Latella et al., 2016) and computationally efficient real-time software architectures (Pizzolato et al., 2017a,b), have the potential to accurately estimate human motion in real-world setting free from the laboratory.
As previously stated, boundary conditions for subsequent FEM model simulations may be computed in real-time using neuromusculoskeletal models. However, even if appropriate boundary conditions are provided, real-time solutions to continuum mechanics problems is an ongoing computational challenge. When implementing entire musculoskeletal structures in FEM models (e.g., complete bones), computational demand may be substantially reduced by spatially averaging many microstructural features, such as trabecular and cortical bone architecture. However, spatial averaging neglects analysis of tissue anisotropy and micro-architecture, which are known to influence tissue function (Stein et al., 2010). Generally, FEM models are computationally demanding and not solvable in real-time. Thus, FEM models must be reduced to surrogates by a process known as “Kriging” (Matheron, 1963), whereby the continuum model is first solved offline for all possible, or physiologic, configurations (Wu et al., 2014; Eskinazi and Fregly, 2016), and simulation results are then be stored for future real-time use. However, it is computationally expensive to establish robust surrogates of musculoskeletal tissue continuum models, given the large data throughput imposed by performing many multi-scale simulations (Erdemir et al., 2015). One potential strategy we are pursuing is use of high-performance computing, whereby a large number of simulations are managed and solved by a remote computing cluster.
Challenges and Future Directions
Our proposed framework to modify an individual's physical behavior to optimize musculoskeletal tissue mechanobiology (Figure 3) is feasible and currently being developed. In Table 1 we have summarized several challenges and possible future directions discussed in the text. To move these bioinspired technologies to clinical settings we need to direct our efforts toward: (1) rapid generation and seamless integration of personalized neuromusculoskeletal and FEM models, (2) use of wearable sensors, and (3) improvement of biofeedback modalities for stress and strain modulation.
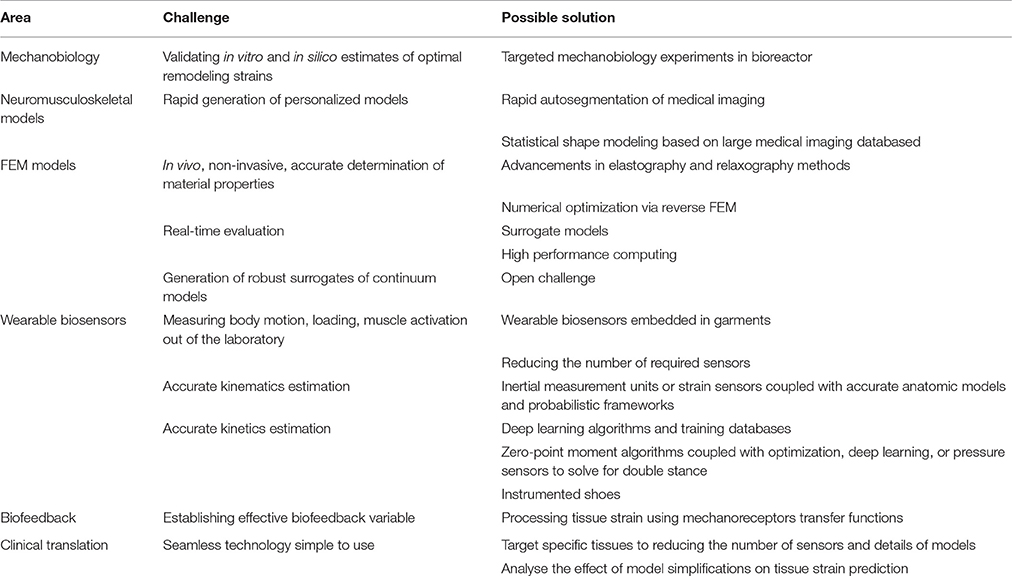
Table 1. Summary of the various challenges faced in modeling tissue mechanobiology and using biofeedback to modulate in vivo tissue strains in real-time.
Currently, creating personalized anatomic models from medical imaging is expensive (i.e., involves costly image acquisition and numerous man-hours to process raw medical imaging into high-fidelity computational models). However, improvements in image processing software, such as automatic segmentation and statistical shape modeling (Zhang et al., 2014; Zhang and Besier, 2017) may greatly accelerate model generation. Statistical shape modeling is promising as it may limit the need to acquire expensive medical imaging, relying instead upon a musculoskeletal atlas database to characterize an individual's anatomy from sparse or meta-data (Zhang and Besier, 2017). However, it is unclear whether current publically available medical imaging databases are sufficient to represent the variability in musculoskeletal anatomy in clinical populations, or those with traumas or implants. This is a limitation that will eventually be addressed by data sharing amongst research teams, which is an effort we thoroughly support.
Another limitation is that motion capture systems typically used in research gait laboratories are seldom used into clinical settings, because of their complexity, space requirements, and high purchase and operational costs. For bioinspired technologies to be broadly adopted, we need to free ourselves of traditional motion capture systems and look to wearable sensors to measure movement, external loads, and muscle excitation. A promising and relatively inexpensive example of wearable sensors that could help us on this mission are inertial measurement units, which provide a wealth of data that may be used to determine whole-body motion. Currently, inertial measurement units are limited by issues such as insufficient shielding from electromagnetic interference (i.e., while walking on treadmills or near informatics cabling) and registration of body-worn sensor positions to anatomic models. Wireless EMG systems have been used effectively in research and clinical settings for many years, and are now being integrated with inertial measurement units and other sensors as standalone devices or embedded into garments. Future research should aim to first establish if these wearable sensor systems can match the performance of traditional motion capture systems, and then minimize the number of sensors required to drive neuromusculoskeletal models.
Very little is currently known about the ability of individuals to volitionally modulate musculoskeletal tissue stresses and strains in response to real-time feedback. To our knowledge, musculoskeletal tissue stresses and strains have never been estimated in real-time, let alone used to modify physical behavior. To date, only two research groups (Manal et al., 2012; Pizzolato et al., 2017b) have provided real-time biofeedback of musculoskeletal tissue loads, but their work has been limited to muscle-tendon and rigid articular contact forces, and did not model tissue stresses and strains.
We know from previous studies people can use visual biofeedback to manipulate external biomechanical variables, muscle excitations, and tibiofemoral contact forces (Manal et al., 2012; Pizzolato et al., 2017b). Future research should strive to identify the biofeedback modality optimal for modulating musculoskeletal tissue stresses and strains through changes in human movement and muscle activation. Further, it may be possible to draw inspiration from a variety of native mechanoreceptors in the human body to provide enhanced visual biofeedback of stresses and strains. We imagine a technology whereby estimates of musculoskeletal tissue loading (i.e., forces or stresses and strains) could be transformed according to golgi organelle and muscle spindle transfer functions to provide more intuitive biofeedback.
By optimizing the mechanical environment it may be possible to regulate musculoskeletal tissue mechanobiology, potentially preventing disease, or restoring degraded tissue to health. Consequently, modeling and controlling physical behavior of individuals has enormous implications for development and management of chronic musculoskeletal diseases such as osteoarthritis or tendinopathies. We have presented a framework to move from in vitro and ex vivo studies of tissue mechanobiology to personalized in silico real-time models of musculoskeletal tissue loading. Integrating and translating these bioinspired technologies to clinical settings will prove challenging and resource intensive. Skepticism from clinicians accustomed to generic recommendations based on linear statistics is anticipated and will need to be overcome by demonstrating the efficacy and clinical utility of the proposed new approach. However, there awaits a wide spectrum of important clinical conditions to which these bioinspired technologies could be applied with the goal of reducing the socio-economic burden of musculoskeletal diseases.
Author Contributions
CP, DL, and DS contributed to conceptualize, draft, critically revise, and approve the final version of the article. RB, JC, MZ, and TB contributed to conceptualize, critically revise, and approve the final version of the article.
Conflict of Interest Statement
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Acknowledgments
This work was supported by the Australian Research Council Linkage Project scheme (LP150100905).
References
Adachi, T., Tomita, Y., Sakaue, H., and Tanaka, M. (1997). Simulation of trabecular surface remodeling based on local stress nonuniformity. JSME Int. J. Ser. C, 40, 782–792. doi: 10.1299/jsmec.40.782
Amin, S., Luepongsak, N., McGibbon, C. A., Lavalley, M. P., Krebs, D. E., and Felson, D. T. (2004). Knee adduction moment and development of chronic knee pain in elders. Arthritis Rheum. 51, 371–376. doi: 10.1002/art.20396
Amjadi, M., Kyung, K. U., Park, I., and Sitti, M. (2016). Stretchable, skin-mountable, and wearable strain sensors and their potential applications: a review. Adv. Funct. Mater. 26, 1678–1698. doi: 10.1002/adfm.201504755
Anderson, M. J., Diko, S., Baehr, L. M., Baar, K., Bodine, S. C., and Christiansen, B. A. (2016). Contribution of mechanical unloading to trabecular bone loss following non-invasive knee injury in mice. J. Orthop. Res. 34, 1680–1687. doi: 10.1002/jor.23178
Andriacchi, T. P., Favre, J., Erhart-Hledik, J. C., and Chu, C. R. (2015). A systems view of risk factors for knee osteoarthritis reveals insights into the pathogenesis of the disease. Ann. Biomed. Eng. 43, 376–387. doi: 10.1007/s10439-014-1117-2
Armstrong, C. G., and Mow, V. C. (1982). Variations in the intrinsic mechanical properties of human articular cartilage with age, degeneration, and water content. J. Bone Joint Surg. Am. 64, 88–94. doi: 10.2106/00004623-198264010-00013
Arnold, A. S., Salinas, S., Asakawa, D. J., and Delp, S. L. (2000). Accuracy of muscle moment arms estimated from MRI-based musculoskeletal models of the lower extremity. Comput. Aided Surg. 5, 108–119. doi: 10.3109/10929080009148877
Arokoski, J. P., Jurvelin, J. S., Vaatainen, U., and Helminen, H. J. (2000). Normal and pathological adaptations of articular cartilage to joint loading. Scand. J. Med. Sci. Sports 10, 186–198. doi: 10.1034/j.1600-0838.2000.010004186.x
Barber, L., Barrett, R., and Lichtwark, G. (2009). Validation of a freehand 3D ultrasound system for morphological measures of the medial gastrocnemius muscle. J. Biomech. 42, 1313–1319. doi: 10.1016/j.jbiomech.2009.03.005
Barrios, J. A., Crossley, K. M., and Davis, I. S. (2010). Gait retraining to reduce the knee adduction moment through real-time visual feedback of dynamic knee alignment. J. Biomech. 43, 2208–2213. doi: 10.1016/j.jbiomech.2010.03.040
Baum, T., Joseph, G. B., Karampinos, D. C., Jungmann, P. M., Link, T. M., and Bauer, J. S. (2013). Cartilage and meniscal T2 relaxation time as non-invasive biomarker for knee osteoarthritis and cartilage repair procedures. Osteoarthr. Cartil. 21, 1474–1484. doi: 10.1016/j.joca.2013.07.012
Beaupre, G. S., Stevens, S. S., and Carter, D. R. (2000). Mechanobiology in the development, maintenance, and degeneration of articular cartilage. J. Rehabil. Res. Dev. 37, 145–151.
Bergmann, G., Graichen, F., Bender, A., Kaab, M., Rohlmann, A., and Westerhoff, P. (2007). In vivo glenohumeral contact forces–measurements in the first patient 7 months postoperatively. J. Biomech. 40, 2139–2149. doi: 10.1016/j.jbiomech.2006.10.037
Bergmann, G., Graichen, F., Rohlmann, A., Bender, A., Heinlein, B., Duda, G. N., et al. (2010). Realistic loads for testing hip implants. Biomed. Mater. Eng. 20, 65–75. doi: 10.3233/BME-2010-0616
Besier, T. F., Fredericson, M., Gold, G. E., Beaupre, G. S., and Delp, S. L. (2009). Knee muscle forces during walking and running in patellofemoral pain patients and pain-free controls. J. Biomech. 42, 898–905. doi: 10.1016/j.jbiomech.2009.01.032
Besier, T. F., Gold, G. E., Beaupre, G. S., and Delp, S. L. (2005). A modeling framework to estimate patellofemoral joint cartilage stress in vivo. Med. Sci. Sports Exerc. 37, 1924–1930. doi: 10.1249/01.mss.0000176686.18683.64
Binding, P., Jinha, A., and Herzog, W. (2000). Analytic analysis of the force sharing among synergistic muscles in one- and two-degree-of-freedom models. J. Biomech. 33, 1423–1432. doi: 10.1016/S0021-9290(00)00108-1
Bitsakos, C., Kerner, J., Fisher, I., and Amis, A. A. (2005). The effect of muscle loading on the simulation of bone remodelling in the proximal femur. J. Biomech. 38, 133–139. doi: 10.1016/j.jbiomech.2004.03.005
Bonnevie, E. D., Delco, M. L., Fortier, L. A., Alexander, P. G., Tuan, R. S., and Bonassar, L. J. (2015). Characterization of tissue response to impact loads delivered using a hand-held instrument for studying articular cartilage injury. Cartilage 6, 226–232. doi: 10.1177/1947603515595071
Brandenburg, J. E., Eby, S. F., Song, P. F., Zhao, H., Brault, J. S., Chen, S. G., et al. (2014). Ultrasound elastography: the new frontier in direct measurement of muscle stiffness. Arch. Phys. Med. Rehabil. 95, 2207–2219. doi: 10.1016/j.apmr.2014.07.007
Brito da Luz, S., Modenese, L., Sancisi, N., Mills, P. M., Kennedy, B., Beck, B. R., et al. (2016). Feasibility of using MRIs to create subject-specific parallel-mechanism joint models. J. Biomech. 53, 45–55. doi: 10.1016/j.jbiomech.2016.12.018
Brodie, M., Walmsley, A., and Page, W. (2008). Fusion motion capture: a prototype system using inertial measurement units and GPS for the biomechanical analysis of ski racing. Sports Technol. 1, 17–28. doi: 10.1080/19346182.2008.9648447
Buchanan, T. S., and Lloyd, D. G. (1995). Muscle-activity is different for humans performing static tasks which require force control and position control. Neurosci. Lett. 194, 61–64. doi: 10.1016/0304-3940(95)11727-E
Buchanan, T. S., Lloyd, D. G., Manal, K., and Besier, T. F. (2004). Neuromusculoskeletal modeling: estimation of muscle forces and joint moments and movements from measurements of neural command. J. Appl. Biomech. 20, 367–395. doi: 10.1123/jab.20.4.367
Buchanan, T. S., Lloyd, D. G., Manal, K., and Besier, T. F. (2005). Estimation of muscle forces and joint moments using a forward-inverse dynamics model. Med. Sci. Sports Exerc. 37, 1911–1916. doi: 10.1249/01.mss.0000176684.24008.6f
Buckwalter, J. A. (2002). Articular cartilage injuries. Clin. Orthop. Relat. Res. 21–37. doi: 10.1097/00003086-200209000-00004
Buckwalter, J. A., and Brown, T. D. (2004). Joint injury, repair, and remodeling: roles in post-traumatic osteoarthritis. Clin. Orthop. Relat. Res. 7–16. doi: 10.1097/01.blo.0000131638.81519.de
Burr, D. B., Milgrom, C., Fyhrie, D., Forwood, M., Nyska, M., Finestone, A., et al. (1996). In vivo measurement of human tibial strains during vigorous activity. Bone 18, 405–410. doi: 10.1016/8756-3282(96)00028-2
Carter, D. R. (1987). Mechanical loading history and skeletal biology. J. Biomech. 20, 1095–1109. doi: 10.1016/0021-9290(87)90027-3
Carter, D. R., and Wong, M. (1988a). Mechanical stresses and endochondral ossification in the chondroepiphysis. J. Orthop. Res. 6, 148–154. doi: 10.1002/jor.1100060120
Carter, D. R., and Wong, M. (1988b). The role of mechanical loading histories in the development of diarthrodial joints. J. Orthop. Res. 6, 804–816. doi: 10.1002/jor.1100060604
Carter, D. R., and Wong, M. (1990). “Mechanical stresses in joint morphogenesis and maintenance,” in Biomechanics of Diarthrodial Joints, eds V. C. Mow, A. Ratcliffe, and S. Woo (New York, NY: Springer-Verlag), 155–174.
Carter, D. R., Beaupre, G. S., Giori, N. J., and Helms, J. A. (1998). Mechanobiology of skeletal regeneration. Clin. Orthop. Relat. Res. S41–S55. doi: 10.1097/00003086-199810001-00006
Carter, D. R., Beaupre, G. S., Wong, M., Smith, R. L., Andriacchi, T. P., and Schurman, D. J. (2004). The mechanobiology of articular cartilage development and degeneration. Clin. Orthop. Relat. Res. S69–S77. doi: 10.1097/01.blo.0000144970.05107.7e
Chesnin, K. J., Selby-Silverstein, L., and Besser, M. P. (2000). Comparison of an in-shoe pressure measurement device to a force plate: concurrent validity of center of pressure measurements. Gait Posture 12, 128–133. doi: 10.1016/S0966-6362(00)00071-0
Christiansen, B. A., Guilak, F., Lockwood, K. A., Olson, S. A., Pitsillides, A. A., Sandell, L. J., et al. (2015). Non-invasive mouse models of post-traumatic osteoarthritis. Osteoarthr. Cartil. 23, 1627–1638. doi: 10.1016/j.joca.2015.05.009
Coggon, D., Reading, I., Croft, P., McLaren, M., Barrett, D., and Cooper, C. (2001). Knee osteoarthritis and obesity. Int. J. Obes. Relat. Metab. Disord. 25, 622–627. doi: 10.1038/sj.ijo.0801585
Cooper, C., Snow, S., McAlindon, T. E., Kellingray, S., Stuart, B., Coggon, D., et al. (2000). Risk factors for the incidence and progression of radiographic knee osteoarthritis. Arthritis Rheum. 43, 995–1000. doi: 10.1002/1529-0131(200005)43:5<995::AID-ANR6>3.0.CO;2-1
Cronin, N. J., Carty, C. P., Barrett, R. S., and Lichtwark, G. (2011). Automatic tracking of medial gastrocnemius fascicle length during human locomotion. J. Appl. Physiol. 111, 1491–1496. doi: 10.1152/japplphysiol.00530.2011
Crowninshield, R. D. (1979). Use of optimization techniques to predict muscle forces. J. Biomech. 12:627. doi: 10.1016/0021-9290(79)90098-8
Crowninshield, R. D., and Brand, R. A. (1981). The prediction of forces in joint structures; distribution of intersegmental resultants. Exerc. Sport Sci. Rev. 9, 159–181. doi: 10.1249/00003677-198101000-00004
Delp, S. L., Anderson, F. C., Arnold, A. S., Loan, P., Habib, A., John, C. T., et al. (2007). OpenSim: open-source software to create and analyze dynamic simulations of movement. IEEE Trans. Biomed. Eng. 54, 1940–1950. doi: 10.1109/TBME.2007.901024
Delp, S. L., Loan, J. P., Hoy, M. G., Zajac, F. E., Topp, E. L., and Rosen, J. M. (1990). An interactive graphics-based model of the lower extremity to study orthopaedic surgical procedures. IEEE Trans. Biomed. Eng. 37, 757–767. doi: 10.1109/10.102791
Dijkstra, E. J., and Gutierrez-Farewik, E. M. (2015). Computation of ground reaction force using zero moment point. J. Biomech. 48, 3776–3781. doi: 10.1016/j.jbiomech.2015.08.027
Djuric-Jovicic, M. D., Jovicic, N. S., and Popovic, D. B. (2011). Kinematics of gait: new method for angle estimation based on accelerometers. Sensors 11, 10571–10585. doi: 10.3390/s111110571
D'lima, D. D., Patil, S., Steklov, N., Slamin, J. E., and Colwell, C. W. Jr. (2006). Tibial forces measured in vivo after total knee arthroplasty. J. Arthroplasty 21, 255–262. doi: 10.1016/j.arth.2005.07.011
D'lima, D. D., Townsend, C. P., Arms, S. W., Morris, B. A., and Colwell, C. W. Jr. (2005). An implantable telemetry device to measure intra-articular tibial forces. J. Biomech. 38, 299–304. doi: 10.1016/j.jbiomech.2004.02.011
Dowling, A. V., Corazza, S., Chaudhari, A. M., and Andriacchi, T. P. (2010). Shoe-surface friction influences movement strategies during a sidestep cutting task: implications for anterior cruciate ligament injury risk. Am. J. Sports Med. 38, 478–485. doi: 10.1177/0363546509348374
Duda, G. N., Heller, M., Albinger, J., Schulz, O., Schneider, E., and Claes, L. (1998). Influence of muscle forces on femoral strain distribution. J. Biomech. 31, 841–846. doi: 10.1016/S0021-9290(98)00080-3
Dufresne, T. (1998). Segmentation techniques for analysis of bone by three-dimensional computed tomographic imaging. Technol. Health Care 6, 351–359.
Dunn, T. C., Lu, Y., Jin, H., Ries, M. D., and Majumdar, S. (2004). T2 relaxation time of cartilage at MR imaging: comparison with severity of knee osteoarthritis. Radiology 232, 592–598. doi: 10.1148/radiol.2322030976
Eby, S. F., Song, P. F., Chen, S. G., Chen, Q. S., Greenleaf, J. F., and An, K. N. (2013). Validation of shear wave elastography in skeletal muscle. J. Biomech. 46, 2381–2387. doi: 10.1016/j.jbiomech.2013.07.033
Eckstein, F., Faber, S., Muhlbauer, R., Hohe, J., Englmeier, K. H., Reiser, M., et al. (2002). Functional adaptation of human joints to mechanical stimuli. Osteoarthr. Cartil. 10, 44–50. doi: 10.1053/joca.2001.0480
Eckstein, F., Hudelmaier, M., and Putz, R. (2006). The effects of exercise on human articular cartilage. J. Anat. 208, 491–512. doi: 10.1111/j.1469-7580.2006.00546.x
Ehrlich, P. J., and Lanyon, L. E. (2002). Mechanical strain and bone cell function: a review. Osteoporos. Int. 13, 688–700. doi: 10.1007/s001980200095
English, T. A., and Kilvington, M. (1979). In vivo records of hip loads using a femoral implant with telemetric output (a preliminary report). J. Biomed. Eng. 1, 111–115. doi: 10.1016/0141-5425(79)90066-9
Erdemir, A., Bennetts, C., Davis, S., Reddy, A., and Sibole, S. (2015). Multiscale cartilage biomechanics: technical challenges in realizing a high-throughput modelling and simulation workflow. Interface Focus 5:20140081. doi: 10.1098/rsfs.2014.0081
Erdemir, A., McLean, S., Herzog, W., and Van Den Bogert, A. J. (2007). Model-based estimation of muscle forces exerted during movements. Clin. Biomech. 22, 131–154. doi: 10.1016/j.clinbiomech.2006.09.005
Erhart-Hledik, J. C., Asay, J. L., Clancy, C., Chu, C. R., and Andriacchi, T. P. (2017). Effects of active feedback gait retraining to produce a medial weight transfer at the foot in subjects with symptomatic medial knee osteoarthritis. J. Orthop. Res. 35, 2251–2259. doi: 10.1002/jor.23527
Eskinazi, I., and Fregly, B. J. (2016). An open-source toolbox for surrogate modeling of joint contact mechanics. IEEE Trans. Biomed. Eng. 63, 269–277. doi: 10.1109/TBME.2015.2455510
Felson, D. T., Lawrence, R. C., Dieppe, P. A., Hirsch, R., Helmick, C. G., Jordan, J. M., et al. (2000). Osteoarthritis: new insights. Part 1: the disease and its risk factors. Ann. Intern. Med. 133, 635–646. doi: 10.7326/0003-4819-133-8-200010170-00016
Felson, D. T., Niu, J., Gross, K. D., Englund, M., Sharma, L., Cooke, T. D., et al. (2013). Valgus malalignment is a risk factor for lateral knee osteoarthritis incidence and progression: findings from the Multicenter Osteoarthritis Study and the Osteoarthritis Initiative. Arthritis Rheum. 65, 355–362. doi: 10.1002/art.37726
Felson, D. T., Zhang, Y., Hannan, M. T., Naimark, A., Weissman, B., Aliabadi, P., et al. (1997). Risk factors for incident radiographic knee osteoarthritis in the elderly: the Framingham Study. Arthritis Rheum. 40, 728–733. doi: 10.1002/art.1780400420
Fernandez, J., Sartori, M., Lloyd, D., Munro, J., and Shim, V. (2014). Bone remodelling in the natural acetabulum is influenced by muscle force-induced bone stress. Int. J. Numer. Method. Biomed. Eng. 30, 28–41. doi: 10.1002/cnm.2586
Fluit, R., Andersen, M. S., Kolk, S., Verdonschot, N., and Koopman, H. F. J. M. (2014). Prediction of ground reaction forces and moments during various activities of daily living. J. Biomech. 47, 2321–2329. doi: 10.1016/j.jbiomech.2014.04.030
Forwood, M. R., and Burr, D. B. (1993). Physical activity and bone mass: exercises in futility? Bone Miner. 21, 89–112. doi: 10.1016/S0169-6009(08)80012-8
Forwood, M. R., and Turner, C. H. (1995). Skeletal adaptations to mechanical usage: results from tibial loading studies in rats. Bone 17, 197S–205S. doi: 10.1016/8756-3282(95)00292-L
Fregly, B. J., Besier, T. F., Lloyd, D. G., Delp, S. L., Banks, S. A., Pandy, M. G., et al. (2012). Grand challenge competition to predict in vivo knee loads. J. Orthop. Res. 30, 503–513. doi: 10.1002/jor.22023
Freutel, M., Schmidt, H., Durselen, L., Ignatius, A., and Galbusera, F. (2014). Finite element modeling of soft tissues: material models, tissue interaction and challenges. Clin. Biomech. 29, 363–372. doi: 10.1016/j.clinbiomech.2014.01.006
Frost, H. M. (1988). Vital biomechanics: proposed general concepts for skeletal adaptations to mechanical usage. Calcif. Tissue Int. 42, 145–156. doi: 10.1007/BF02556327
Frost, H. M. (1990a). Skeletal structural adaptations to mechanical usage (SATMU): 1. Redefining Wolff's law: the bone modeling problem. Anat. Rec. 226, 403–413. doi: 10.1002/ar.1092260402
Frost, H. M. (1990b). Skeletal structural adaptations to mechanical usage (SATMU): 2. Redefining Wolff's law: the remodeling problem. Anat. Rec. 226, 414–422. doi: 10.1002/ar.1092260403
Frost, H. M. (1990c). Skeletal structural adaptations to mechanical usage (SATMU): 3. The hyaline cartilage modeling problem. Anat. Rec. 226, 423–432. doi: 10.1002/ar.1092260404
Frost, H. M. (1990d). Skeletal structural adaptations to mechanical usage (SATMU): 4. Mechanical influences on intact fibrous tissues. Anat. Rec. 226, 433–439. doi: 10.1002/ar.1092260405
Fukashiro, S., Komi, P. V., Jarvinen, M., and Miyashita, M. (1995). In vivo Achilles tendon loading during jumping in humans. Eur. J. Appl. Physiol. Occup. Physiol. 71, 453–458. doi: 10.1007/BF00635880
Fyhrie, D. P., and Carter, D. R. (1986). A unifying principle relating stress to trabecular bone morphology. J. Orthop. Res. 4, 304–317. doi: 10.1002/jor.1100040307
Fyhrie, D. P., and Carter, D. R. (1990). Femoral head apparent density distribution predicted from bone stresses. J. Biomech. 23, 1–10. doi: 10.1016/0021-9290(90)90363-8
Geraldes, D. M., Modenese, L., and Phillips, A. T. (2016). Consideration of multiple load cases is critical in modelling orthotropic bone adaptation in the femur. Biomech. Model. Mechanobiol. 15, 1029–1042. doi: 10.1007/s10237-015-0740-7
Gerus, P., Sartori, M., Besier, T. F., Fregly, B. J., Delp, S. L., Banks, S. A., et al. (2013). Subject-specific knee joint geometry improves predictions of medial tibiofemoral contact forces. J. Biomech. 46, 2778–2786. doi: 10.1016/j.jbiomech.2013.09.005
Gillett, J. G., Barrett, R. S., and Lichtwark, G. A. (2013). Reliability and accuracy of an automated tracking algorithm to measure controlled passive and active muscle fascicle length changes from ultrasound. Comput. Methods Biomech. Biomed. Eng. 16, 678–687. doi: 10.1080/10255842.2011.633516
Glaser, K. J., Manduca, A., and Ehman, R. L. (2012). Review of MR elastography applications and recent developments. J. Magn. Reson. Imaging 36, 757–774. doi: 10.1002/jmri.23597
Gregor, R. J., Komi, P. V., and Jarvinen, M. (1987). Achilles tendon forces during cycling. Int. J. Sports Med. 8(Suppl. 1), 9–14. doi: 10.1055/s-2008-1025698
Grodzinsky, A. J., Levenston, M. E., Jin, M., and Frank, E. H. (2000). Cartilage tissue remodeling in response to mechanical forces. Annu. Rev. Biomed. Eng. 2, 691–713. doi: 10.1146/annurev.bioeng.2.1.691
Haeufle, D. F., Gunther, M., Wunner, G., and Schmitt, S. (2014). Quantifying control effort of biological and technical movements: an information-entropy-based approach. Phys. Rev. E Stat. Nonlin. Soft Matter Phys. 89:012716. doi: 10.1103/PhysRevE.89.012716
Halloran, J. P., Ackermann, M., Erdemir, A., and Van Den Bogert, A. J. (2010). Concurrent musculoskeletal dynamics and finite element analysis predicts altered gait patterns to reduce foot tissue loading. J. Biomech. 43, 2810–2815. doi: 10.1016/j.jbiomech.2010.05.036
Hambli, R. (2011). Numerical procedure for multiscale bone adaptation prediction based on neural networks and finite element simulation. Finite Elem. Anal. Des. 47, 835–842. doi: 10.1016/j.finel.2011.02.014
Hansen, W., Shim, V., Obst, S., Lloyd, D. G., Newsham-West, R., and Barrett, R. (2017). Achilles tendon stress is more sensitive to subject-specific geometry than subject-specific material properties: a finite element analysis. J. Biomech. 56, 26–31. doi: 10.1016/j.jbiomech.2017.02.031
Hatze, H. (1977). A myocybernetic control model of skeletal muscle. Biol. Cybern. 25, 103–119. doi: 10.1007/BF00337268
Heinlein, B., Graichen, F., Bender, A., Rohlmann, A., and Bergmann, G. (2007). Design, calibration and pre-clinical testing of an instrumented tibial tray. J. Biomech. 40(Suppl. 1), S4–S10. doi: 10.1016/j.jbiomech.2007.02.014
Heinlein, B., Kutzner, I., Graichen, F., Bender, A., Rohlmann, A., Halder, A. M., et al. (2009). ESB Clinical Biomechanics Award 2008: complete data of total knee replacement loading for level walking and stair climbing measured in vivo with a follow-up of 6-10 months. Clin. Biomech. 24, 315–326. doi: 10.1016/j.clinbiomech.2009.01.011
Herzog, W., and Binding, P. (1992). Predictions of antagonistic muscular activity using nonlinear optimization. Math. Biosci. 111, 217–229. doi: 10.1016/0025-5564(92)90071-4
Herzog, W., and Binding, P. (1993). Cocontraction of pairs of antagonistic muscles: analytical solution for planar static nonlinear optimization approaches. Math. Biosci. 118, 83–95. doi: 10.1016/0025-5564(93)90034-8
Herzog, W., Leonard, T. R., Renaud, J. M., Wallace, J., Chaki, G., and Bornemisza, S. (1992). Force-length properties and functional demands of cat gastrocnemius, soleus and plantaris muscles. J. Biomech. 25, 1329–1335. doi: 10.1016/0021-9290(92)90288-C
Hodgson, J. A. (1983). The relationship between soleus and gastrocnemius muscle activity in conscious cats–a model for motor unit recruitment? J. Physiol. 337, 553–562. doi: 10.1113/jphysiol.1983.sp014641
Honarvar, M. G., and Latifi, M. (2017). Overview of wearable electronics and smart textiles. J. Text. Instit. 108, 631–652. doi: 10.1080/00405000.2016.1177870
Hunt, M. A., Simic, M., Hinman, R. S., Bennell, K. L., and Wrigley, T. V. (2011). Feasibility of a gait retraining strategy for reducing knee joint loading: increased trunk lean guided by real-time biofeedback. J. Biomech. 44, 943–947. doi: 10.1016/j.jbiomech.2010.11.027
Hunter, D. J., Altman, R. D., Cicuttini, F., Crema, M. D., Duryea, J., Eckstein, F., et al. (2015). OARSI Clinical Trials Recommendations: knee imaging in clinical trials in osteoarthritis. Osteoarthr. Cartil. 23, 698–715. doi: 10.1016/j.joca.2015.03.012
Hunter, D. J., Schofield, D., and Callander, E. (2014). The individual and socioeconomic impact of osteoarthritis. Nat. Rev. Rheumatol. 10, 437–441. doi: 10.1038/nrrheum.2014.44
Ihn, J. C., Kim, S. J., and Park, I. H. (1993). In vitro study of contact area and pressure distribution in the human knee after partial and total meniscectomy. Int. Orthop. 17, 214–218. doi: 10.1007/BF00194181
Jones, G., Ding, C., Glisson, M., Hynes, K., Ma, D., and Cicuttini, F. (2003). Knee articular cartilage development in children: a longitudinal study of the effect of sex, growth, body composition, and physical activity. Pediatr. Res. 54, 230–236. doi: 10.1203/01.PDR.0000072781.93856.E6
Jones, G., Glisson, M., Hynes, K., and Cicuttini, F. (2000). Sex and site differences in cartilage development: a possible explanation for variations in knee osteoarthritis in later life. Arthritis Rheum. 43, 2543–2549. doi: 10.1002/1529-0131(200011)43:11<2543::AID-ANR23>3.0.CO;2-K
Joo Kim, J., Musson, D. S., Matthews, B. G., Cornish, J., Anderson, I. A., and Shim, V. B. (2016). Applying physiologically relevant strains to tenocytes in an in vitro cell device induces in vivo like behaviors. J. Biomech. Eng. 138:121003. doi: 10.1115/1.4034031
Kainz, H., Modenese, L., Lloyd, D. G., Maine, S., Walsh, H. P., and Carty, C. P. (2016). Joint kinematic calculation based on clinical direct kinematic versus inverse kinematic gait models. J. Biomech. 49, 1658–1669. doi: 10.1016/j.jbiomech.2016.03.052
Kavanagh, J. J., and Menz, H. B. (2008). Accelerometry: a technique for quantifying movement patterns during walking. Gait Posture 28, 1–15. doi: 10.1016/j.gaitpost.2007.10.010
Kerner, J., Huiskes, R., Van Lenthe, G. H., Weinans, H., Van Rietbergen, B., Engh, C. A., et al. (1999). Correlation between pre-operative periprosthetic bone density and post-operative bone loss in THA can be explained by strain-adaptive remodelling. J. Biomech. 32, 695–703. doi: 10.1016/S0021-9290(99)00041-X
Kiviranta, I., Jurvelin, J., Tammi, M., Saamanen, A. M., and Helminen, H. J. (1987). Weight bearing controls glycosaminoglycan concentration and articular cartilage thickness in the knee joints of young beagle dogs. Arthritis Rheum. 30, 801–809. doi: 10.1002/art.1780300710
Kiviranta, I., Tammi, M., Jurvelin, J., Arokoski, J., Saamanen, A. M., and Helminen, H. J. (1992). Articular cartilage thickness and glycosaminoglycan distribution in the canine knee joint after strenuous running exercise. Clin. Orthop. Relat. Res. 302–308. doi: 10.1097/00003086-199210000-00046
Kiviranta, I., Tammi, M., Jurvelin, J., Saamanen, A. M., and Helminen, H. J. (1988). Moderate running exercise augments glycosaminoglycans and thickness of articular cartilage in the knee joint of young beagle dogs. J. Orthop. Res. 6, 188–195. doi: 10.1002/jor.1100060205
Komi, P. V., Salonen, M., Jarvinen, M., and Kokko, O. (1987). In vivo registration of Achilles tendon forces in man. I. Methodological development. Int. J. Sports Med. 8(Suppl. 1), 3–8. doi: 10.1055/s-2008-1025697
Konrath, J. M., Saxby, D. J., Killen, B. A., Pizzolato, C., Vertullo, C. J., Barrett, R. S., et al. (2017). Muscle contributions to medial tibiofemoral compartment contact loading following ACL reconstruction using semitendinosus and gracilis tendon grafts. PLoS ONE 12:e0176016. doi: 10.1371/journal.pone.0176016
Koo, S., and Andriacchi, T. P. (2007). A comparison of the influence of global functional loads vs. local contact anatomy on articular cartilage thickness at the knee. J. Biomech. 40, 2961–2966. doi: 10.1016/j.jbiomech.2007.02.005
Koo, S., Rylander, J. H., and Andriacchi, T. P. (2011). Knee joint kinematics during walking influences the spatial cartilage thickness distribution in the knee. J. Biomech. 44, 1405–1409. doi: 10.1016/j.jbiomech.2010.11.020
Labadie, C., Lee, J. H., Vetek, G., and Springer, C. S. Jr. (1994). Relaxographic imaging. J. Magn. Reson. B 105, 99–112. doi: 10.1006/jmrb.1994.1109
Lammentausta, E., Kiviranta, P., Nissi, M. J., Laasanen, M. S., Kiviranta, I., Nieminen, M. T., et al. (2006). T-2 relaxation time and delayed gadolinium-enhanced MRI of cartilage (dGEMRIC) of human patellar cartilage at 1.5 T and 9.4 T: relationships with tissue mechanical properties. J. Orthop. Res. 24, 366–374. doi: 10.1002/jor.20041
Lang, T. F., Leblanc, A. D., Evans, H. J., and Lu, Y. (2006). Adaptation of the proximal femur to skeletal reloading after long-duration spaceflight. J. Bone Miner. Res. 21, 1224–1230. doi: 10.1359/jbmr.060509
Lanyon, L. E., Hampson, W. G., Goodship, A. E., and Shah, J. S. (1975). Bone deformation recorded in vivo from strain gauges attached to the human tibial shaft. Acta Orthop. Scand. 46, 256–268. doi: 10.3109/17453677508989216
Latella, C., Kuppuswamy, N., Romano, F., Traversaro, S., and Nori, F. (2016). Whole-body human inverse dynamics with distributed micro-accelerometers, gyros and force sensing. Sensors 16:E727. doi: 10.3390/s16050727
Lenaerts, G., Bartels, W., Gelaude, F., Mulier, M., Spaepen, A., Van Der Perre, G., et al. (2009). Subject-specific hip geometry and hip joint centre location affects calculated contact forces at the hip during gait. J. Biomech. 42, 1246–1251. doi: 10.1016/j.jbiomech.2009.03.037
Lerner, Z. F., Demers, M. S., Delp, S. L., and Browning, R. C. (2015). How tibiofemoral alignment and contact locations affect predictions of medial and lateral tibiofemoral contact forces. J. Biomech. 48, 644–650. doi: 10.1016/j.jbiomech.2014.12.049
Lespessailles, E., Ibrahim-Nasser, N., Toumi, H., and Chapurlat, R. (2017). Contribution of high resolution peripheral quantitative CT to the management of bone and joint diseases. Joint Bone Spine. doi: 10.1016/j.jbspin.2017.04.012. [Epub ahead of print].
Liedtke, C., Fokkenrood, S. A. W., Menger, J. T., Van Der Kooij, H., and Veltink, P. H. (2007). Evaluation of instrumented shoes for ambulatory assessment of ground reaction forces. Gait Posture 26, 39–47. doi: 10.1016/j.gaitpost.2006.07.017
Lloyd, D. G., and Besier, T. F. (2003). An EMG-driven musculoskeletal model to estimate muscle forces and knee joint moments in vivo. J. Biomech. 36, 765–776. doi: 10.1016/S0021-9290(03)00010-1
Lloyd, D. G., Buchanan, T. S., and Besier, T. F. (2005). Neuromuscular biomechanical modeling to understand knee ligament loading. Med. Sci. Sports Exerc. 37, 1939–1947. doi: 10.1249/01.mss.0000176676.49584.ba
Lohmander, L. S., Englund, P. M., Dahl, L. L., and Roos, E. M. (2007). The long-term consequence of anterior cruciate ligament and meniscus injuries: osteoarthritis. Am. J. Sports Med. 35, 1756–1769. doi: 10.1177/0363546507307396
Lohmander, L. S., Ostenberg, A., Englund, M., and Roos, H. (2004). High prevalence of knee osteoarthritis, pain, and functional limitations in female soccer players twelve years after anterior cruciate ligament injury. Arthritis Rheum. 50, 3145–3152. doi: 10.1002/art.20589
Madgwick, S. O., Harrison, A. J., and Vaidyanathan, A. (2011). Estimation of IMU and MARG orientation using a gradient descent algorithm. IEEE Int. Conf. Rehabil. Robot. 2011:5975346. doi: 10.1109/ICORR.2011.5975346
Manal, K., and Buchanan, T. S. (2013). An electromyogram-driven musculoskeletal model of the knee to predict in vivo joint contact forces during normal and novel gait patterns. J. Biomech. Eng. 135:021014. doi: 10.1115/1.4023457
Manal, K., Gonzalez, R. V., Lloyd, D. G., and Buchanan, T. S. (2002). A real-time EMG-driven virtual arm. Comput. Biol. Med. 32, 25–36. doi: 10.1016/S0010-4825(01)00024-5
Manal, K., Gravare-Silbernagel, K., and Buchanan, T. S. (2012). A real-time EMG-driven musculoskeletal model of the ankle. Multibody Syst. Dyn. 28, 169–180. doi: 10.1007/s11044-011-9285-4
Marra, M. A., Vanheule, V., Fluit, R., Koopman, B. H., Rasmussen, J., Verdonschot, N., et al. (2015). A subject-specific musculoskeletal modeling framework to predict in vivo mechanics of total knee arthroplasty. J. Biomech. Eng. 137:020904. doi: 10.1115/1.4029258
Matheron, G. (1963). Principles of geostatistics. Econ. Geol. 58, 1246–1266. doi: 10.2113/gsecongeo.58.8.1246
Mattmann, C., Amft, O., Harms, H., Troster, G., and Clemens, F. (2007). “Recognizing upper body postures using textile strain sensors,” in Eleventh IEEE International Symposium on Wearable Computers (Boston, MA).
Menegaldo, L. L., and Oliveira, L. F. (2011). An EMG-driven model to evaluate quadriceps strengthening after an isokinetic training. Proc. IUTAM 2, 131–141. doi: 10.1016/j.piutam.2011.04.014
Miyazaki, T., Wada, M., Kawahara, H., Sato, M., Baba, H., and Shimada, S. (2002). Dynamic load at baseline can predict radiographic disease progression in medial compartment knee osteoarthritis. Ann. Rheum. Dis. 61, 617–622. doi: 10.1136/ard.61.7.617
Modenese, L., Gopalakrishnan, A., and Phillips, A. T. (2013). Application of a falsification strategy to a musculoskeletal model of the lower limb and accuracy of the predicted hip contact force vector. J. Biomech. 46, 1193–1200. doi: 10.1016/j.jbiomech.2012.11.045
Mow, V. C., Kuei, S. C., Lai, W. M., and Armstrong, C. G. (1980). Biphasic creep and stress relaxation of articular cartilage in compression? Theory and experiments. J. Biomech. Eng. 102, 73–84. doi: 10.1115/1.3138202
Mundermann, A., Payer, N., Felmet, G., and Riehle, H. (2015). Comparison of volumetric bone mineral density in the operated and contralateral knee after anterior cruciate ligament and reconstruction: a 1-year follow-up study using peripheral quantitative computed tomography. J. Orthop. Res. 33, 1804–1810. doi: 10.1002/jor.22962
Nakamoto, H., Ootaka, H., Tada, M., Hirata, I., Kobayashi, F., and Kojima, F. (2016). Stretchable strain sensor with anisotropy and application for joint angle measurement. IEEE Sens. J. 16, 3572–3579. doi: 10.1109/JSEN.2016.2535489
Natenstedt, J., Kok, A. C., Dankelman, J., and Tuijthof, G. J. (2015). What quantitative mechanical loading stimulates in vitro cultivation best? J. Exp. Orthop. 2:15. doi: 10.1186/s40634-015-0029-x
Newman, A. P. (1998). Articular cartilage repair. Am. J. Sports Med. 26, 309–324. doi: 10.1177/03635465980260022701
Newton, P. M., Mow, V. C., Gardner, T. R., Buckwalter, J. A., and Albright, J. P. (1997). Winner of the 1996 Cabaud Award. The effect of lifelong exercise on canine articular cartilage. Am. J. Sports Med. 25, 282–287. doi: 10.1177/036354659702500302
Ng, J. L., Kersh, M. E., Kilbreath, S., and Knothe Tate, M. (2017). Establishing the basis for mechanobiology-based physical therapy protocols to potentiate cellular healing and tissue regeneration. Front. Physiol. 8:303. doi: 10.3389/fphys.2017.00303
Nuri, L., Obst, S. J., Newsham-West, R., and Barrett, R. S. (2017). The tendinopathic Achilles tendon does not remain iso-volumetric upon repeated loading: insights from 3D ultrasound. J. Exp. Biol. 220, 3053–3061. doi: 10.1242/jeb.159764
Obst, S. J., Newsham-West, R., and Barrett, R. S. (2014a). In vivo measurement of human achilles tendon morphology using freehand 3-D ultrasound. Ultrasound Med. Biol. 40, 62–70. doi: 10.1016/j.ultrasmedbio.2013.08.009
Obst, S. J., Renault, J. B., Newsham-West, R., and Barrett, R. S. (2014b). Three-dimensional deformation and transverse rotation of the human free Achilles tendon in vivo during isometric plantarflexion contraction. J. Appl. Physiol. 116, 376–384. doi: 10.1152/japplphysiol.01249.2013
O'connor, J. A., Lanyon, L. E., and Macfie, H. (1982). The influence of strain rate on adaptive bone remodelling. J. Biomech. 15, 767–781. doi: 10.1016/0021-9290(82)90092-6
Oh, S. E., Choi, A., and Mun, J. H. (2013). Prediction of ground reaction forces during gait based on kinematics and a neural network model. J. Biomech. 46, 2372–2380. doi: 10.1016/j.jbiomech.2013.07.036
Ophir, J., Cespedes, I., Ponnekanti, H., Yazdi, Y., and Li, X. (1991). Elastography: a quantitative method for imaging the elasticity of biological tissues. Ultrason. Imaging 13, 111–134. doi: 10.1177/016173469101300201
Pandy, M. G., and Sasaki, K. (1998). A three-dimensional musculoskeletal model of the human knee joint. part 2: analysis of ligament function. Comput. Methods Biomech. Biomed. Eng. 1, 265–283. doi: 10.1080/01495739808936707
Passmore, E., and Sangeux, M. (2016). Defining the medial-lateral axis of an anatomical femur coordinate system using freehand 3D ultrasound imaging. Gait Posture 45, 211–216. doi: 10.1016/j.gaitpost.2016.02.006
Passmore, E., Pandy, M. G., Graham, H. K., and Sangeux, M. (2016). Measuring femoral torsion in vivo using freehand 3-d ultrasound imaging. Ultrasound Med. Biol. 42, 619–623. doi: 10.1016/j.ultrasmedbio.2015.10.014
Peters, A., Baker, R., and Sangeux, M. (2010). Validation of 3-D freehand ultrasound for the determination of the hip joint centre. Gait Posture 31, 530–532. doi: 10.1016/j.gaitpost.2010.01.014
Phillips, A. T. M., Villetteab, C. C., and Modenese, L. (2015). Femoral bone mesoscale structural architecture prediction using musculoskeletal and finite element modelling. Int. Biomech. 2, 43–61. doi: 10.1080/23335432.2015.1017609
Pivonka, P., and Dunstan, C. R. (2012). Role of mathematical modeling in bone fracture healing. Bonekey Rep. 1:221. doi: 10.1038/bonekey.2012.221
Pizzolato, C., Lloyd, D. G., Sartori, M., Ceseracciu, E., Besier, T. F., Fregly, B. J., et al. (2015). CEINMS: a toolbox to investigate the influence of different neural control solutions on the prediction of muscle excitation and joint moments during dynamic motor tasks. J. Biomech. 48, 3929–3936. doi: 10.1016/j.jbiomech.2015.09.021
Pizzolato, C., Reggiani, M., Modenese, L., and Lloyd, D. G. (2017a). Real-time inverse kinematics and inverse dynamics for lower limb applications using OpenSim. Comput. Methods Biomech. Biomed. Eng. 20, 436–445. doi: 10.1080/10255842.2016.1240789
Pizzolato, C., Reggiani, M., Saxby, D. J., Ceseracciu, E., Modenese, L., and Lloyd, D. G. (2017b). Biofeedback for gait retraining based on real-time estimation of tibiofemoral joint contact forces. IEEE Trans. Neural Syst. Rehabil. Eng. 25, 1612–1621. doi: 10.1109/TNSRE.2017.2683488
Radin, E. L., and Paul, I. L. (1971). Response of joints to impact loading. I. In vitro wear. Arthritis Rheum. 14, 356–362. doi: 10.1002/art.1780140306
Radin, E. L., Martin, R. B., Burr, D. B., Caterson, B., Boyd, R. D., and Goodwin, C. (1984). Effects of mechanical loading on the tissues of the rabbit knee. J. Orthop. Res. 2, 221–234. doi: 10.1002/jor.1100020303
Radin, E. L., Parker, H. G., Pugh, J. W., Steinberg, R. S., Paul, I. L., and Rose, R. M. (1973). Response of joints to impact loading. 3. Relationship between trabecular microfractures and cartilage degeneration. J. Biomech. 6, 51–57. doi: 10.1016/0021-9290(73)90037-7
Rasmussen, J., Torholm, S., and De Zee, M. (2009). Computational analysis of the influence of seat pan inclination and friction on muscle activity and spinal joint forces. Int. J. Ind. Ergon. 39, 52–57. doi: 10.1016/j.ergon.2008.07.008
Reilly, D. T., and Burstein, A. H. (1974). Review article. The mechanical properties of cortical bone. J. Bone Joint Surg. Am. 56, 1001–1022. doi: 10.2106/00004623-197456050-00012
Riskowski, J. L., Mikesky, A. E., Bahamonde, R. E., and Burr, D. B. (2009). Design and validation of a knee brace with feedback to reduce the rate of loading. J. Biomech. Eng. 131:084503. doi: 10.1115/1.3148858
Roemer, F. W., Zhang, Y., Niu, J., Lynch, J. A., Crema, M. D., Marra, M. D., et al. (2009). Tibiofemoral joint osteoarthritis: risk factors for MR-depicted fast cartilage loss over a 30-month period in the multicenter osteoarthritis study. Radiology 252, 772–780. doi: 10.1148/radiol.2523082197
Roos, E. M., and Dahlberg, L. (2005). Positive effects of moderate exercise on glycosaminoglycan content in knee cartilage: a four-month, randomized, controlled trial in patients at risk of osteoarthritis. Arthritis Rheum. 52, 3507–3514. doi: 10.1002/art.21415
Rubin, C. T., and Lanyon, L. E. (1985). Regulation of bone mass by mechanical strain magnitude. Calcif. Tissue Int. 37, 411–417. doi: 10.1007/BF02553711
Rydell, N. W. (1966). Forces acting on the femoral head-prosthesis. A study on strain gauge supplied prostheses in living persons. Acta Orthop. Scand. 37(Suppl. 88), 1–132. doi: 10.3109/ort.1966.37.suppl-88.01
Sabatini, A. M. (2006). Quaternion-based extended Kalman filter for determining orientation by inertial and magnetic sensing. IEEE Trans. Biomed. Eng. 53, 1346–1356. doi: 10.1109/TBME.2006.875664
Sartori, M., Farina, D., and Lloyd, D. G. (2014). Hybrid neuromusculoskeletal modeling to best track joint moments using a balance between muscle excitations derived from electromyograms and optimization. J. Biomech. 47, 3613–3621. doi: 10.1016/j.jbiomech.2014.10.009
Sartori, M., Maculan, M., Pizzolato, C., Reggiani, M., and Farina, D. (2015). Modeling and simulating the neuromuscular mechanisms regulating ankle and knee joint stiffness during human locomotion. J. Neurophysiol. 114, 2509–2527. doi: 10.1152/jn.00989.2014
Saxby, D. J., Bryant, A. L., Modenese, L., Gerus, P., Killen, B. A., Konrath, J., et al. (2016a). Tibiofemoral contact forces in the anterior cruciate ligament-reconstructed knee. Med. Sci. Sports Exerc. 48, 2195–2206. doi: 10.1249/MSS.0000000000001021
Saxby, D. J., Modenese, L., Bryant, A. L., Gerus, P., Killen, B., Fortin, K., et al. (2016b). Tibiofemoral contact forces during walking, running and sidestepping. Gait Posture 49, 78–85. doi: 10.1016/j.gaitpost.2016.06.014
Scanlan, S. F., Favre, J., and Andriacchi, T. P. (2013). The relationship between peak knee extension at heel-strike of walking and the location of thickest femoral cartilage in ACL reconstructed and healthy contralateral knees. J. Biomech. 46, 849–854. doi: 10.1016/j.jbiomech.2012.12.026
Scheys, L., Spaepen, A., Suetens, P., and Jonkers, I. (2008). Calculated moment-arm and muscle-tendon lengths during gait differ substantially using MR based versus rescaled generic lower-limb musculoskeletal models. Gait Posture 28, 640–648. doi: 10.1016/j.gaitpost.2008.04.010
Seth, A., Sherman, M., Eastman, P., and Delp, S. (2010). Minimal formulation of joint motion for biomechanisms. Nonlinear Dyn. 62, 291–303. doi: 10.1007/s11071-010-9717-3
Setton, L. A., Elliott, D. M., and Mow, V. C. (1999). Altered mechanics of cartilage with osteoarthritis: human osteoarthritis and an experimental model of joint degeneration. Osteoarthr. Cartil. 7, 2–14. doi: 10.1053/joca.1998.0170
Shelburne, K. B., and Pandy, M. G. (1997). A musculoskeletal model of the knee for evaluating ligament forces during isometric contractions. J. Biomech. 30, 163–176. doi: 10.1016/S0021-9290(96)00119-4
Shelburne, K. B., Torry, M. R., and Pandy, M. G. (2005). Muscle, ligament, and joint-contact forces at the knee during walking. Med. Sci. Sports Exerc. 37, 1948–1956. doi: 10.1249/01.mss.0000180404.86078.ff
Shim, V. B., Besier, T. F., Lloyd, D. G., Mithraratne, K., and Fernandez, J. F. (2016). The influence and biomechanical role of cartilage split line pattern on tibiofemoral cartilage stress distribution during the stance phase of gait. Biomech. Model. Mechanobiol. 15, 195–204. doi: 10.1007/s10237-015-0668-y
Shull, P. B., Lurie, K. L., Cutkosky, M. R., and Besier, T. F. (2011). Training multi-parameter gaits to reduce the knee adduction moment with data-driven models and haptic feedback. J. Biomech. 44, 1605–1609. doi: 10.1016/j.jbiomech.2011.03.016
Shull, P. B., Shultz, R., Silder, A., Dragoo, J. L., Besier, T. F., Cutkosky, M. R., et al. (2013a). Toe-in gait reduces the first peak knee adduction moment in patients with medial compartment knee osteoarthritis. J. Biomech. 46, 122–128. doi: 10.1016/j.jbiomech.2012.10.019
Shull, P. B., Silder, A., Shultz, R., Dragoo, J. L., Besier, T. F., Delp, S. L., et al. (2013b). Six-week gait retraining program reduces knee adduction moment, reduces pain, and improves function for individuals with medial compartment knee osteoarthritis. J. Orthop. Res. 31, 1020–1025. doi: 10.1002/jor.22340
Sigrist, R., Rauter, G., Riener, R., and Wolf, P. (2013). Augmented visual, auditory, haptic, and multimodal feedback in motor learning: a review. Psychon. Bull. Rev. 20, 21–53. doi: 10.3758/s13423-012-0333-8
Simon, S. R., Radin, E. L., Paul, I. L., and Rose, R. M. (1972). The response of joints to impact loading. II. In vivo behavior of subchondral bone. J. Biomech. 5, 267–272. doi: 10.1016/0021-9290(72)90042-5
Smith, C. R., Won Choi, K., Negrut, D., and Thelen, D. G. (2016). Efficient computation of cartilage contact pressures within dynamic simulations of movement. Comput. Methods Biomech. Biomed. Eng. Imaging Vis. 1–8. doi: 10.1080/21681163.2016.1172346
Stein, E. M., Liu, X. S., Nickolas, T. L., Cohen, A., Thomas, V., McMahon, D. J., et al. (2010). Abnormal microarchitecture and reduced stiffness at the radius and tibia in postmenopausal women with fractures. J. Bone Miner. Res. 25, 2572–2581. doi: 10.1002/jbmr.152
Tax, A. A., Denier Van Der Gon, J. J., and Erkelens, C. J. (1990). Differences in coordination of elbow flexor muscles in force tasks and in movement tasks. Exp. Brain Res. 81, 567–572. doi: 10.1007/BF02423505
Tsubota, K., Adachi, T., and Tomita, Y. (2002). Functional adaptation of cancellous bone in human proximal femur predicted by trabecular surface remodeling simulation toward uniform stress state. J. Biomech. 35, 1541–1551. doi: 10.1016/S0021-9290(02)00173-2
van den Bogert, A. J., Geijtenbeek, T., Even-Zohar, O., Steenbrink, F., and Hardin, E. C. (2013). A real-time system for biomechanical analysis of human movement and muscle function. Med. Biol. Eng. Comput. 51, 1069–1077. doi: 10.1007/s11517-013-1076-z
Van Den Noort, J. C., Steenbrink, F., Roeles, S., and Harlaar, J. (2015). Real-time visual feedback for gait retraining: toward application in knee osteoarthritis. Med. Biol. Eng. Comput. 53, 275–286. doi: 10.1007/s11517-014-1233-z
Van Der Helm, F. C. (1994). A finite element musculoskeletal model of the shoulder mechanism. J. Biomech. 27, 551–569. doi: 10.1016/0021-9290(94)90065-5
Van Rossom, S., Smith, C. R., Zevenbergen, L., Thelen, D. G., Vanwanseele, B., Van Assche, D., et al. (2017). Knee cartilage thickness, T1rho and T2 relaxation time are related to articular cartilage loading in healthy adults. PLoS ONE 12:e0170002. doi: 10.1371/journal.pone.0170002
Vanwanseele, B., Eckstein, F., Knecht, H., Spaepen, A., and Stussi, E. (2003). Longitudinal analysis of cartilage atrophy in the knees of patients with spinal cord injury. Arthritis Rheum. 48, 3377–3381. doi: 10.1002/art.11367
Vanwanseele, B., Eckstein, F., Knecht, H., Stussi, E., and Spaepen, A. (2002). Knee cartilage of spinal cord-injured patients displays progressive thinning in the absence of normal joint loading and movement. Arthritis Rheum. 46, 2073–2078. doi: 10.1002/art.10462
Villette, C. C., and Phillips, A. T. (2016). Informing phenomenological structural bone remodelling with a mechanistic poroelastic model. Biomech. Model. Mechanobiol. 15, 69–82. doi: 10.1007/s10237-015-0735-4
Walmsley, B., Hodgson, J. A., and Burke, R. E. (1978). Forces produced by medial gastrocnemius and soleus muscles during locomotion in freely moving cats. J. Neurophysiol. 41, 1203–1216.
Walter, J. P., D'lima, D. D., Colwell, C. W. Jr., and Fregly, B. J. (2010). Decreased knee adduction moment does not guarantee decreased medial contact force during gait. J. Orthop. Res. 28, 1348–1354. doi: 10.1002/jor.21142
Walter, J. P., Korkmaz, N., Fregly, B. J., and Pandy, M. G. (2015). Contribution of tibiofemoral joint contact to net loads at the knee in gait. J. Orthop. Res. 33, 1054–1060. doi: 10.1002/jor.22845
Wang, T., Lin, Z., Day, R. E., Gardiner, B., Landao-Bassonga, E., Rubenson, J., et al. (2013). Programmable mechanical stimulation influences tendon homeostasis in a bioreactor system. Biotechnol. Bioeng. 110, 1495–1507. doi: 10.1002/bit.24809
Wang, T., Lin, Z., Ni, M., Thien, C., Day, R. E., Gardiner, B., et al. (2015). Cyclic mechanical stimulation rescues achilles tendon from degeneration in a bioreactor system. J. Orthop. Res. 33, 1888–1896. doi: 10.1002/jor.22960
Wang, X., Malik, A., Bartel, D. L., Wickiewicz, T. L., and Wright, T. (2014). Asymmetric varus and valgus stability of the anatomic cadaver knee and the load sharing between collateral ligaments and bearing surfaces. J. Biomech. Eng. 136:081005. doi: 10.1115/1.4027662
Wellsandt, E., Gardinier, E. S., Manal, K., Axe, M. J., Buchanan, T. S., and Snyder-Mackler, L. (2016). Decreased knee joint loading associated with early knee osteoarthritis after anterior cruciate ligament injury. Am. J. Sports Med. 44, 143–151. doi: 10.1177/0363546515608475
Wesseling, M., De Groote, F., Bosmans, L., Bartels, W., Meyer, C., Desloovere, K., et al. (2016). Subject-specific geometrical detail rather than cost function formulation affects hip loading calculation. Comput. Methods Biomech. Biomed. Engin. 19, 1475–1488. doi: 10.1080/10255842.2016.1154547
Wheeler, J. W., Shull, P. B., and Besier, T. F. (2011). Real-time knee adduction moment feedback for gait retraining through visual and tactile displays. J. Biomech. Eng. 133:041007. doi: 10.1115/1.4003621
Winby, C. R., Gerus, P., Kirk, T. B., and Lloyd, D. G. (2013). Correlation between EMG-based co-activation measures and medial and lateral compartment loads of the knee during gait. Clin. Biomech. 28, 1014–1019. doi: 10.1016/j.clinbiomech.2013.09.006
Winby, C. R., Lloyd, D. G., Besier, T. F., and Kirk, T. B. (2009). Muscle and external load contribution to knee joint contact loads during normal gait. J. Biomech. 42, 2294–2300. doi: 10.1016/j.jbiomech.2009.06.019
Wong, M., and Carter, D. R. (1990). A theoretical model of endochondral ossification and bone architectural construction in long bone ontogeny. Anat. Embryol. 181, 523–532. doi: 10.1007/BF00174625
Wrigley, T. V., Simic, M., Hunt, M. A., Hinman, R. S., and Bennell, K. L. (2009). “Real-time movement biofeedback for walking gait modification in knee osteoarthritis,” in 2009 Virtual Rehabilitation International Conference (Haifa), 132–135. doi: 10.1109/ICVR.2009.5174219
Wu, T., Martens, H., Hunter, P., and Mithraratne, K. (2014). Emulating facial biomechanics using multivariate partial least squares surrogate models. Int. J. Numer. Method Biomed. Eng. 30, 1103–1120. doi: 10.1002/cnm.2646
Xiang, Y. J., Arora, J. S., Rahmatalla, S., and Abdel-Malek, K. (2009). Optimization-based dynamic human walking prediction: one step formulation. Int. J. Numer. Methods Eng. 79, 667–695. doi: 10.1002/nme.2575
Yamakoshi, Y., Sato, J., and Sato, T. (1990). Ultrasonic imaging of internal vibration of soft tissue under forced vibration. IEEE Trans. Ultrason. Ferroelectr. Freq. Control 37, 45–53. doi: 10.1109/58.46969
Zadpoor, A. A. (2013). Open forward and inverse problems in theoretical modeling of bone tissue adaptation. J. Mech. Behav. Biomed. Mater. 27, 249–261. doi: 10.1016/j.jmbbm.2013.05.017
Zhang, J., and Besier, T. F. (2017). Accuracy of femur reconstruction from sparse geometric data using a statistical shape model. Comput. Methods Biomech. Biomed. Engin. 20, 566–576. doi: 10.1080/10255842.2016.1263301
Keywords: biomechanics, mechanobiology, wearable devices, tissue strain, biofeedback, modeling
Citation: Pizzolato C, Lloyd DG, Barrett RS, Cook JL, Zheng MH, Besier TF and Saxby DJ (2017) Bioinspired Technologies to Connect Musculoskeletal Mechanobiology to the Person for Training and Rehabilitation. Front. Comput. Neurosci. 11:96. doi: 10.3389/fncom.2017.00096
Received: 03 March 2017; Accepted: 04 October 2017;
Published: 18 October 2017.
Edited by:
Massimo Sartori, University of Göttingen, GermanyReviewed by:
Sara Checa, Charité Universitätsmedizin Berlin, GermanySergiy Yakovenko, West Virginia University, United States
Andrew Phillips, Imperial College London, United Kingdom
Copyright © 2017 Pizzolato, Lloyd, Barrett, Cook, Zheng, Besier and Saxby. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) or licensor are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: David G. Lloyd, ZGF2aWQubGxveWRAZ3JpZmZpdGguZWR1LmF1