 Sarah P. Kruse
Sarah P. Kruse Levita D’Souza
Levita D’Souza Jeanine Young
Jeanine Young Hannah G. G. Tuncer
Hannah G. G. Tuncer
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Commun., 10 March 2025
Sec. Health Communication
Volume 10 - 2025 | https://doi.org/10.3389/fcomm.2025.1527164
This article is part of the Research TopicCommunicating Breastfeeding Benefits and Supporting New Mothers’ Wellbeing: Cross-Cultural PerspectivesView all 4 articles
To reduce the occurrence of sudden infant death, organisations have created recommendations about infant safer sleep and shared sleep. With the considerable volume of documents, consistency in messaging is paramount to reduce caregiver confusion and to reduce engagement in practices deemed to be unsafe for their infant. This review aimed to systematically compare documents that contain recommendations on infant safer sleep, including shared sleep, in Australia. Documents were identified by researchers with subject matter expertise, and through a systematic webpage search. A total of n = 32 eligible documents were included from n = 26 organisations. If an organisation had a separate document for shared sleeping, both documents were included and reviewed together. Consistency of recommendations were evaluated against the recommendations within the International Society for the Study and Prevention of Perinatal and Infant Death’s (ISPID)‘s guidelines, while the approach taken to discuss shared sleep from via Risk Minimisation vs. Risk Elimination was also evaluated using a coding framework. No organisation’s document/s contradicted ISPID’s guidelines, although there was variation in the quantity included. The approaches taken towards shared sleep by organisations were diverse between Risk Elimination and Risk Minimisation. Strategies to engage in safer shared sleep were provided by less than half of the organisations, as was the acknowledgement of familial, cultural, or logistical preferences for shared sleep, or that shared sleep may also occur unintentionally. Most organisations recommended that infants be breastfed but did not discuss the bi-directional link between breastfeeding and shared sleeping. Organisations need to provide consistent messaging on infant safer sleep to avoid public confusion. The adoption of a Risk Minimisation approach with clearer messaging provides considerations for informed choice, and strategies for safer shared sleeping; intentional or unintentional.
Sudden unexpected death in infancy (SUDI) is the sudden and unexpected death of an infant (aged <1 year) with no apparent cause of death (Fleming et al., 2000; Krous et al., 2004). SUDI can be further classified into explained SUDI (deaths for which a cause is later identified post-mortem, for example sleep accidents, illness and non-accidental injury), and unexplained SUDI (deaths for which no cause could be determined, e.g., Sudden Infant Death Syndrome [SIDS]; Queensland Family and Child Commission (QFCC), 2022). In 2020, 79 infants under 1 year died from SIDS and undetermined causes in Australia, a rate of 0.3 per 1,000 live births (noting this data does not include statistics from Tasmania, Northern Territory or the Australian Capital Territory; Queensland Family and Child Commission (QFCC), 2023). Although Australia’s SUDI rates have decreased since the 1990s (Australian Institute of Health and Welfare, 2022), they have since plateaued and continue to be ‘mid-range’ compared to other countries (Freemantle and Ellis, 2018). There is also a disparity in SUDI rates with Aboriginal and Torres Strait Islander infants experiencing higher rates of SUDI compared to non-Indigenous infants (Shipstone et al., 2020).
In 1991, the ‘Reduce the Risk’ campaign in Australia was created to inform the public about infant safer sleep (Freemantle and Ellis, 2018; Raven, 2018). Today, organisations continue to provide recommendations focused on modifying elements of the sleep environment (e.g., clear sleep space free of toys and loose cords), positioning (e.g., laying baby in the supine position, face and head uncovered), and parental factors (e.g., maternal smoking) to reduce the influence of these found in research to be linked to SUDIs (Blair et al., 2014; Raven, 2018; Red Nose Australia, 2024; Vennemann et al., 2012).
The International Society for the Study and Prevention of Perinatal and Infant Death (ISPID) is a leading organisation working towards advancing and disseminating evidence-based knowledge and measures to reduce the prevalence of SUDI and stillbirth worldwide (International Society for the Study and Prevention of Perinatal and Infant Death (ISPID), 2024; Raven, 2018). In August 2023, ISPID updated their evidence-based safer infant sleep recommendations, noting there is consensus between countries on some recommendations (e.g., placing infants on their back to sleep), and not others (e.g., practice of shared sleeping; International Society for the Study and Prevention of Perinatal and Infant Death (ISPID), 2023).
Shared sleeping is when an adult sleeps on the same sleep surface as an infant, where falling asleep may be intended or not (International Society for the Study and Prevention of Perinatal and Infant Death (ISPID), 2023; Mileva-Seitz et al., 2017). This is sometimes referred to as ‘bed-sharing’ or ‘co-sleeping’, although definitions can vary in the literature (Kruse et al., 2024). This review uses the term ‘shared sleeping’ to refer to an adult sharing an adult bed with an infant. In some countries and cultures, shared sleep is common (Mileva-Seitz et al., 2017; Owens, 2004), and it can be beneficial in promoting parent–child bonding, and secure attachment (Barry, 2019).
Further to this, shared sleep has been well documented to aid with breastfeeding (Bailey, 2016; D’Souza et al., 2024; Goldberg and Keller, 2007; McKenna et al., 2007; Salm Ward, 2015), aiding in the frequency and total duration of night-time breastfeeding (McKenna et al., 2007; Goldberg and Keller, 2007; Baddock et al., 2019; Huang et al., 2013; Vieira et al., 2021), while shared sleep during breastfeeding also assists in preserving maternal sleep due to more rapid infant settling as they do not progress to full arousal crying, and the reduced frequency of getting out of bed (Salm Ward, 2015). The health benefits of breastfeeding to both mother and child are well documented (Mohamed Ahmed et al., 2023; Couto et al., 2020; Dieterich et al., 2013).
However, in other countries and cultures, particularly in Western countries such as Australia, shared sleeping is often not perceived as the norm. A recent review of infant sleep safety guidelines found that most industrialised countries indicated that sharing any sleeping surface was unsafe and/or that a separate cot was the safest sleeping environment for an infant (Doering et al., 2019).
International Society for the Study and Prevention of Perinatal and Infant Death (ISPID) (2023) noted that with regard to shared sleeping, some countries take a risk elimination (RE) approach while others choose to adopt a risk minimisation (RM) approach. RE recommends against all engagement in shared sleeping (Moon et al., 2022; Queensland Health, Queensland Clinical Guidelines, 2022) while RM recommends against shared sleep in circumstances where the risk is known to be increased (Carpenter et al., 2013; Mileva-Seitz et al., 2017; Young and Shipstone, 2018). RM also considers the family’s personal circumstances, and supports the idea of providing information on risks, benefits and how to increase infant sleep safety in all sleep environments in parent education resources to allow for informed decision making (Australian College of Midwives (ACM), 2014; Queensland Health, Queensland Clinical Guidelines, 2022).
Over time concerns have been raised over the feasibility and efficacy of RE in relation to shared sleep to further reduce SUDI. In Australia, less than 15% of families routinely adopted all six current safer sleep recommendations advocated by Red Nose Australia (Cole et al., 2020), and less than half of surveyed families could list four or more of the recommendations or accurate infant safer sleep strategies (Cole et al., 2021a). Furthermore, shared sleeping in Australia does still occur, with rates reported as high as 76% of families having shared sleep in the first 3 months of life (Cole et al., 2021a) and other studies showing that shared sleeping can be both intentional and unintentional (Cole et al., 2020; D’Souza et al., 2024; Cunningham et al., 2018). RE often fails to acknowledge or respond to cultural and circumstantial reasons for shared sleep (Dodd, 2012; Pease et al., 2017; Young and Shipstone, 2018), and the lack of cultural consideration and person-centred approach may lead to avoidance of discussions with healthcare providers for risk of judgement or fear of repercussions (Bailey, 2016), thereby missing opportunities to receive education about engaging in shared sleeping safely. RE also fails to acknowledge or respond to other reasons for shared sleep including aiding with breastfeeding, sleep and familial bonding (Barry and McKenna, 2022; D’Souza et al., 2024), contributing to parents receiving an imbalanced presentation of bed-sharing, and reducing the opportunity to make an informed choice for their family (Cunningham et al., 2018; Marinelli et al., 2019). Recent research has continued to support the need for safer sleep strategies to adopt open dialogue between parents and educators around motivations for shared sleep in a safe, culturally sensitive, non-judgmental environment, particularly with vulnerable populations (Barrett et al., 2024; Dodd, 2012; Pease et al., 2017; Shiells et al., 2024).
In 2021 a set of infant safe sleep priorities for Australian families was created through a content expert consensus research activity involving field experts and stakeholders (Cole et al., 2021b). Emerging from this process was the need to drive consistent messaging across all channels to reduce public confusion (Cole et al., 2021b). As mentioned previously, messaging on shared sleep internationally is inconsistent (Doering et al., 2019; International Society for the Study and Prevention of Perinatal and Infant Death (ISPID), 2023) but there are also inconsistencies within countries themselves. A recent review of local governments in the UK found significant discrepancies between such authorities in whether and how they carried out SUDI awareness education to families (Ball et al., 2023). Such discrepancies can cause confusion for caregivers who want to engage in infant safer sleep practices. Similar inconsistencies in messaging around bed-sharing were reported in Australia (Australian Association for Infant Mental Health (AAIMH), 2022), although these inconsistencies have not been formally reviewed. To date, there has been no review of the current policies, position statements, or guidance documents available in Australia containing recommendations about infant safer sleep.
The aim of this review was to examine the current, publicly available guidance documents on infant safer sleep in Australia and evaluate the level of consistency within these documents. A secondary focus of the review was on evaluating messaging towards shared sleep. This review did not aim to evaluate the quality of these documents.
Given the potential variety of information sources, the review was split into two parts to maximise the number of included documents.
Part 1 aimed to evaluate documents from Australian state or territory governments, organisations endorsed by government, or professional bodies operating (e.g., nursing, midwifery). Such documents typically are used to inform practice guidelines, particularly for healthcare and education professionals, or to provide evidence-based support to caregivers.
Based on expert knowledge of the field the authors constructed a preliminary list of organisations (n = 20, seen in Table 1 denoted by *). The documents were sourced via public web searching and then checked by co-authors to ensure they were the most appropriate and recently published version of the source’s document for inclusion. During this stage n = 3 sources were excluded due to absence of relevant, accessible documentation regarding infant safer sleep. Only the main documents outlining infant safe sleep recommendations and any accompanying documents that included shared sleep were included. From this search n = 20 eligible documents were identified from n = 17 sources.
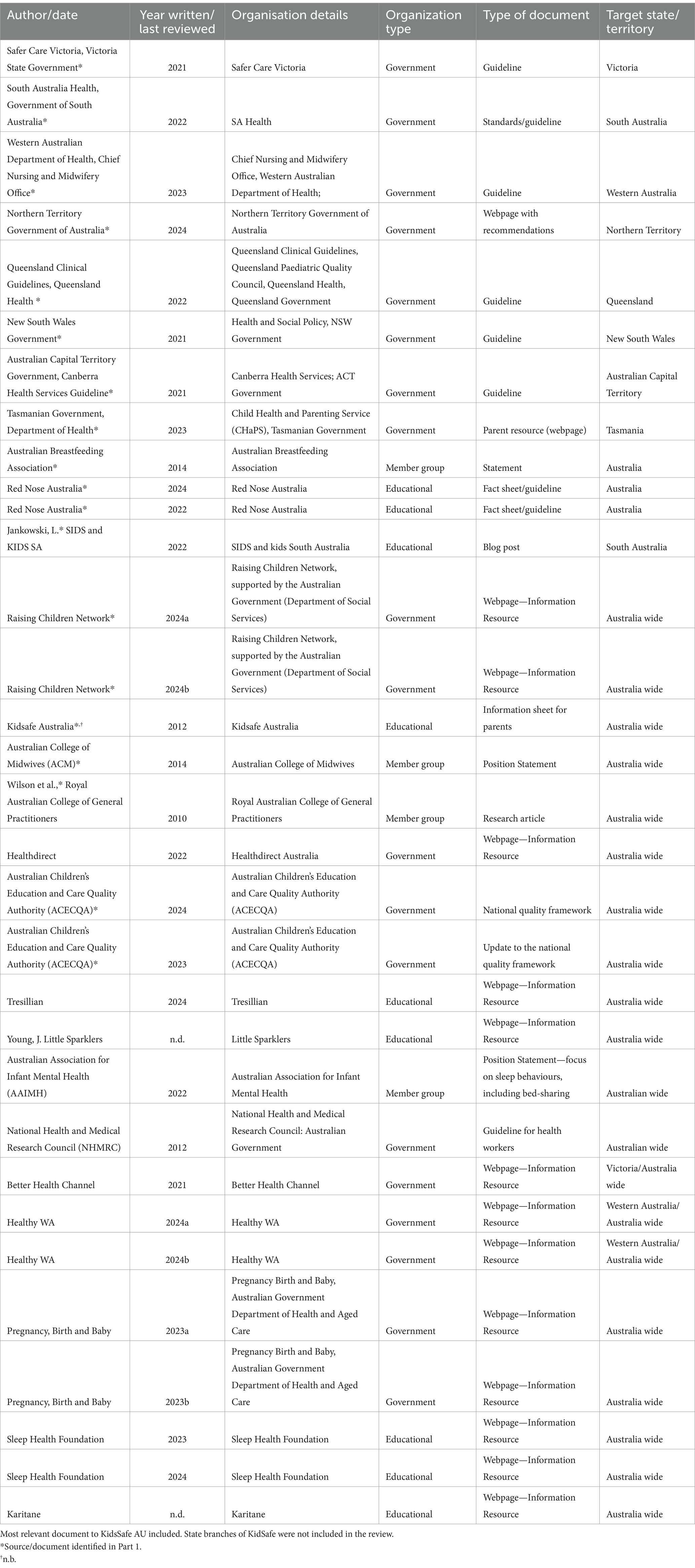
Table 1. Characteristics of documents included.
A second search to find other relevant documents for inclusion involved.
a grey literature search conducted systematically by two authors. Each author ran multiple web-searches through a search engine,1 using the search strategy (infant OR baby OR newborn) safe* sleep OR sleep (environment OR position OR location) AND (Guidelines OR policy OR recommendations OR practices OR operational directive OR position statement) AND (location). Each reviewer ran the search nine times, changing the ‘location’ each time to cover each of Australia’s eight states and territories, and one for ‘Australia’ itself. From each search, the first 100 webpages were screened. A total of n = 1,800 webpages were screened. The search strategy and terms used were discussed in consultation with a librarian of Monash University.
Documents were excluded if they did not discuss infant safer sleep, were not aimed to be consumed by people living in Australia, were focused towards a subset of the population (e.g., families in child protection services, Indigenous Australians), or came from a source in which the organisation was not a charity/non-profit or government affiliate, with recommendations being produced by an individual (as opposed to a Board or formal working party). Documents were also excluded if the source was already included in part 1. A total of n = 1,800 webpages/documents were reviewed, equating to n = 509 unique web-pages when duplicate URLs were removed. These 509 webpages were further reviewed and grouped together by their overarching source (e.g., Queensland Government, Red Nose) or duplicate pages (e.g., same book identified across different webpages). A further n = 211 webpages were removed as duplicates, leaving n = 298. A further n = 28 sources were removed as they were already included in part 1. From this n = 13 documents from n = 10 sources met inclusion criteria (see Figure 1 for screening processes and exclusion reasons). Prior to data extraction, all documents were searched again to check for any document updates or changes (August 2024). From this search, one organisation was found to have dissolved; this document was removed from review (Reflux Infant Support Association). Any ambiguity around inclusion was discussed with the wider research team.
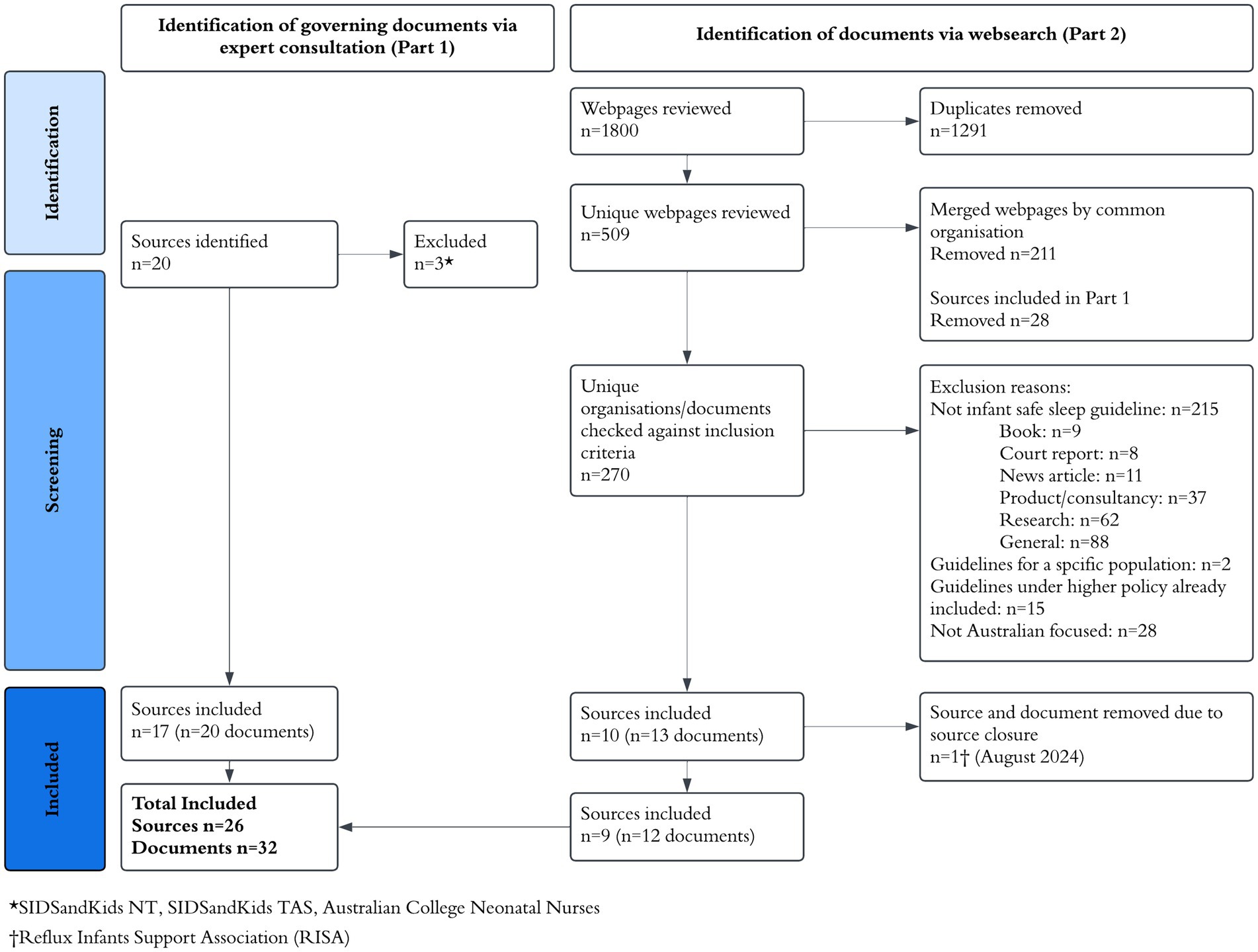
Figure 1. Flowchart. Submitted in separate file due (.exe).
While this review does not strictly meet all PRISMA guidelines (Page et al., 2021), the authors took care to closely follow recommendations to ensure that this review was conducted in a systematic and rigorous manner to ensure validity where possible. This included the double reviewing of documents for inclusion, documentation of exclusion reasons throughout the review, and continuous review and consolidation with the wider review team when discrepancies arose. The flow chart in Figure 1 provides further information on screening processes and exclusion reasons.
A final total of n = 32 documents from n = 26 organisations were included in the review. For the purposes of data extraction and analysis, if an organisation had multiple documents these were reviewed in conjunction as one.
To evaluate consistency of guidelines, each document was checked against the ISPID’s safe infant sleep recommendations (International Society for the Study and Prevention of Perinatal and Infant Death (ISPID), 2023), both in which consensus (n = 13) and non-consensus had been achieved (n = 6).
To examine how shared sleep was referred to within current guidelines (and the level of consistency across these documents), an examination of whether guidelines took an RM or RE approach was conducted.
In this review, a RM approach referred to balanced information dissemination to enable parents to make an informed decision about their family’s sleep arrangements, whilst allowing them to consider their own circumstances, values, and preferences within this context (Australian College of Midwives (ACM), 2014; Queensland Health, Queensland Clinical Guidelines, 2022; Salm Ward and Doering, 2014). Contrastingly, a RE approach aims to remove all potential and perceived risks and is prescriptive in recommendations around what families should and should not be engaging in. Each document was reviewed for approach and consistency to shared sleeping.
The authors compiled a set of seven criteria to evaluate whether a RE or an RM approach was taken (see Supplementary Figure 1). The seven criteria were (a) wording about engagement in shared sleep, specifically bed-sharing, (b) provision of strategies for engaging in shared sleep, (c) benefits of shared sleep, (d) risks of shared sleep, (plus an additional criteria to acknowledge if the risks and benefits have been equally discussed), (e) acknowledgement of reasons and circumstances for shared sleep, including likelihood of unintentional shared sleeping (i.e., cultural, or personal circumstances), (f) acknowledgement of shared sleep’s association with breastfeeding, and (g) overall framing of messaging. Criteria were developed based on elements to allow for informed choice to be obtained (i.e., risks, benefits and strategies outlined), consideration around the use of language that preferences one behaviour over another, and the acknowledgement of the positive association between breastfeeding and bed-sharing. The level of RE vs. RM approach for each document was evaluated by scoring each criterion based on the extracted data, with higher scores indicating more of an RM approach. The coding framework used to score the level of RM vs. RE can be found in the Supplementary material. The seven criteria were weighted in their scoring, in that criteria that were more critical and reflective of a RM approach (e.g., criteria b and g), had a higher scoring scale (0–4), allowing for these criteria to be appropriately acknowledged. The weighting of each criterion was determined by the authors based on the importance of this information in creating a safer shared sleep environment in the likely event shared sleeping will occur, intended or not. Furthermore, there is acknowledgement of the ethical principle of autonomy and the rights of the parents to balanced information that include both risks and benefits to allow them to engage in informed decision-making, together with best practice principles in conveying health promotions messages (i.e., non-judgment, strength-based, solution-focussed), were also key when considering the weighting of each criterion.
Each document was double-scored against the coding framework (SK scored 100% of the documents, while authors HT, LD and JY scored a third each). Interrater reliability of scoring was calculated using Krippendorff’s Alpha (Hayes and Krippendorff, 2007) using a web-based statistical package K-Alpha Calculator (Marzi et al., 2024). Krippendorff’s Alpha coefficient was 0.875, indicating a high and satisfactory interrater reliability. When differences occurred, ratings were discussed by the wider group until consensus was achieved.
Six organisations (Australian Children’s Education and Care Quality Authority (ACECQA), Healthy WA, Pregnancy, Birth and Baby, Raising Children Network, Red Nose and Sleep Health Foundation) had two relevant documents which were reviewed in conjunction. The total number of documents reviewed is reported as n = 26 henceforward. An overview of the specifications for each document can be found in Table 1 including where documents came from and their purpose.
Tables 2 and 3 displays the inclusion of ISPID recommendations within each document.
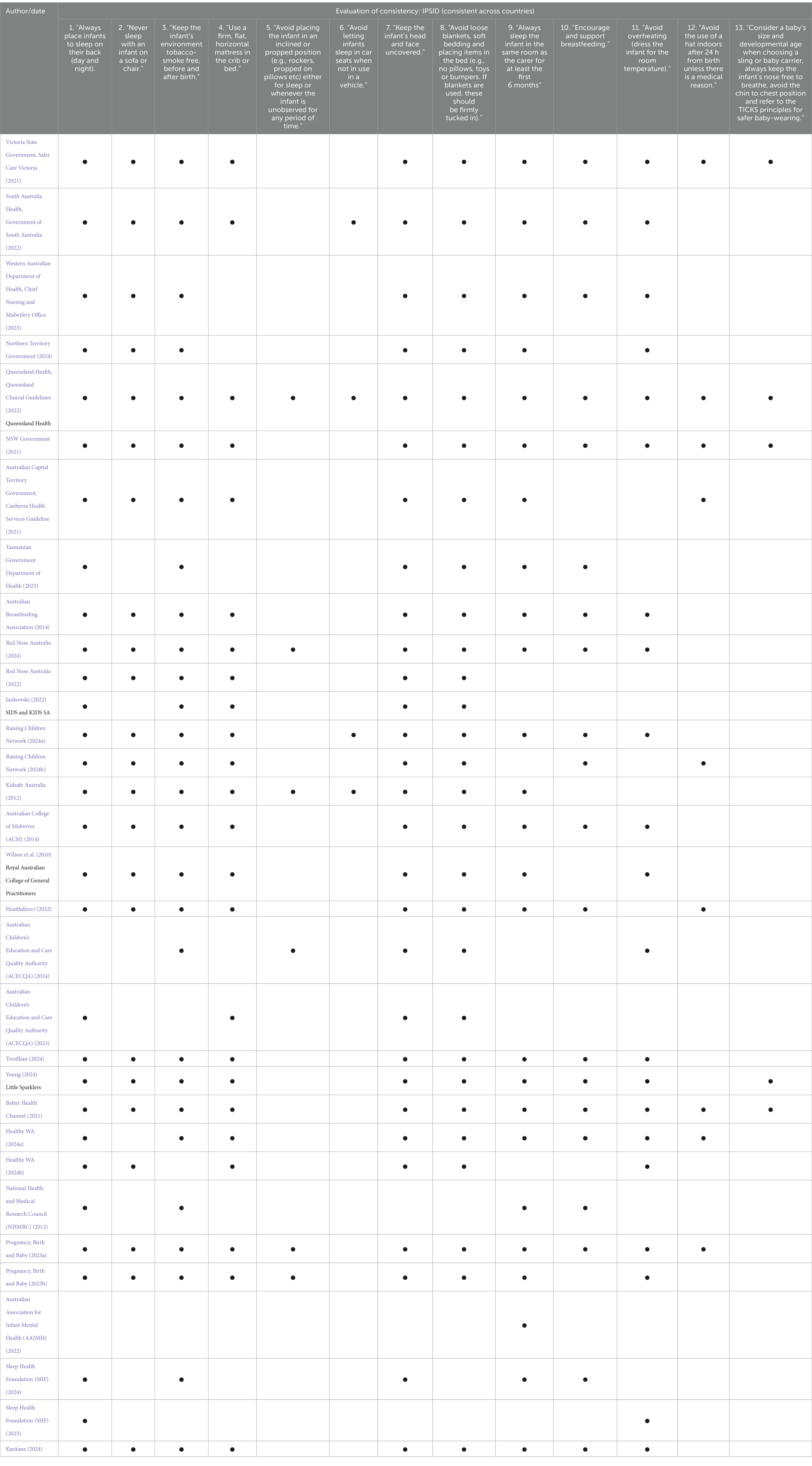
Table 2. Inclusion of IPSID guidelines (consensus).
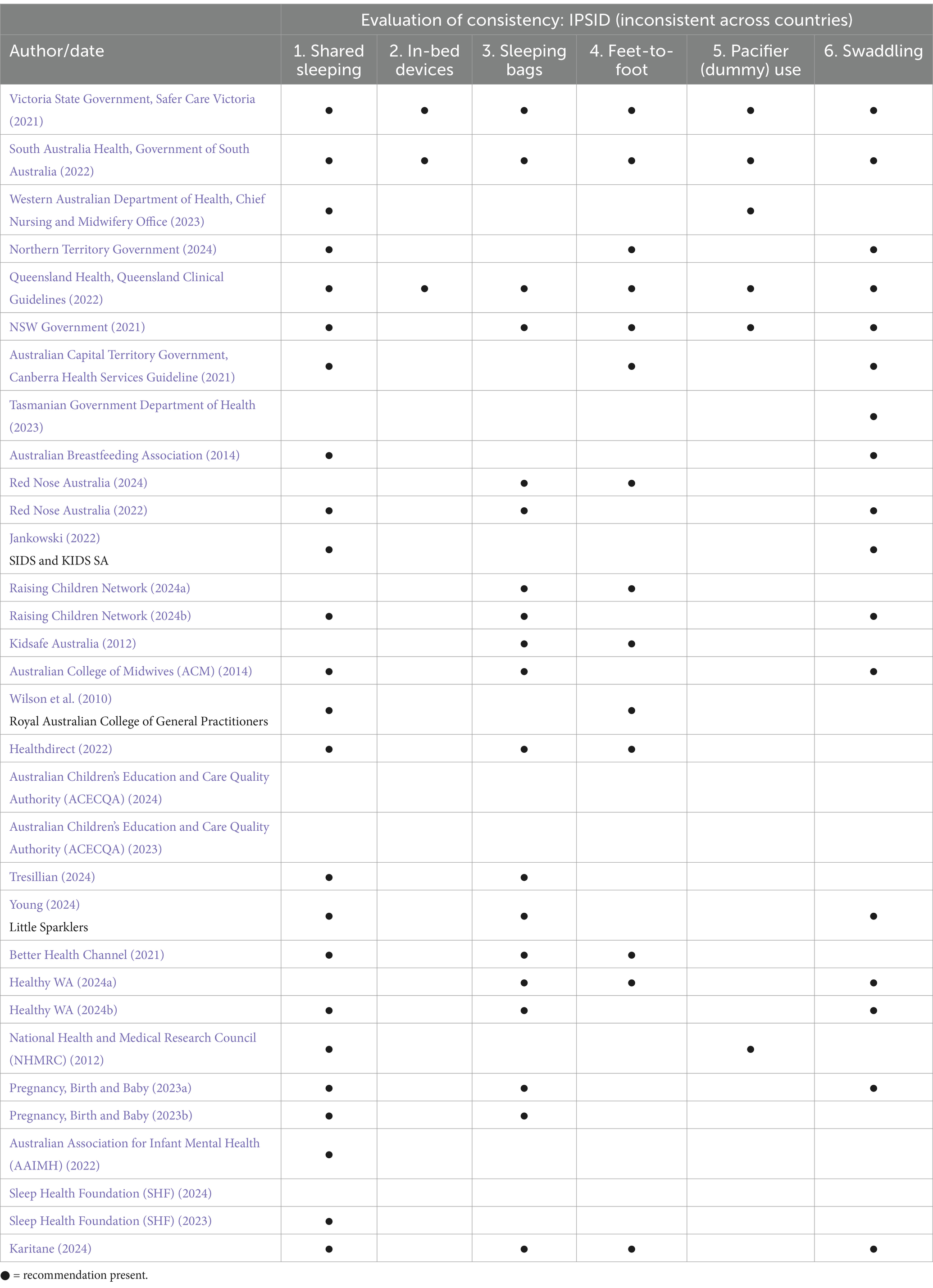
Table 3. Inclusion of IPSID guidelines (non-consensus).
All but one document (Australian Association for Infant Mental Health (AAIMH), 2022) stated infants should be placed on their back to sleep. Most documents (n = 20) did not explicitly state or indicate with pictures that infants should avoid being in an inclined position or on a device that inclines them. No documents said that infants should be placed on an incline.
All but n = 2 documents (Australian Association for Infant Mental Health (AAIMH), 2022; National Health and Medical Research Council (NHMRC), 2012) indicated that infants should not have their face and/or head covered while sleeping, while most advised parents to avoid overheating their baby for sleep, in relation to clothes and bedding (n = 20).
Most documents stated in some form that infants should be breastfed where possible (n = 19). This was sometimes described simply as ‘breastfeed baby’ (Tasmanian Government Department of Health, 2023; Young, 2024) while others stated that breastfeeding can help protect against SIDS and SUDI (Healthdirect, 2022; Tresillian, 2024).
Most documents reported that the mattress the baby sleeps on should be firm and flat (n = 19). One document (Northern Territory Government, 2024) noted the mattress should be ‘safe’ but did not specify what this meant, while another, reported that the mattress should be firm but did not specify it should also be flat (Tresillian, 2024). All but n = 3 documents (Australian Association for Infant Mental Health (AAIMH), 2022; National Health and Medical Research Council (NHMRC), 2012; Sleep Health Foundation (SHF), 2023, 2024), specified to avoid the use of soft bedding, and/or having items around the infant or in their sleeping space.
Most documents stated that sleeping on a sofa or chair with an infant was unsafe and/or should be avoided (n = 20). Of these South Australia Health, Government of South Australia (2022) discussed couch sleeping both as part of bed-sharing and then later as a separate arrangement, while Healthy WA (2024b) defined co-sleeping as including bed-sharing and couch sharing, stating that co-sleeping was not recommended. All but one document (Jankowski, 2022) stated that infants should sleep in the same room as a caregiver for the first 6 months of life. Three documents stated the cot should be in the parents’ room but no timeframe was given (Tasmanian Government Department of Health, 2023; Western Australian Department of Health, Chief Nursing and Midwifery Office, 2023; Wilson et al., 2010). All but one document (Australian Association for Infant Mental Health (AAIMH), 2022) discussed the importance of keeping the infant’s environment smoke free.
Only five documents included recommendations about using a sling or baby carrier (Better Health Channel, 2021; NSW Government, 2021; Queensland Health, Queensland Clinical Guidelines, 2022; Victoria State Government, Safer Care Victoria, 2021; Young, 2024). All referred to considerations around breathing, positioning or T.I.C.K.S. (Tight, In view at all times, Close enough to kiss, Keep chin off chest, Supported back), but only one document (Queensland Health, Queensland Clinical Guidelines, 2022) specifically noted that infant developmental assessment was relevant to all care practices (including therefore carrier use).
Four documents described in-bed, portable sleep spaces to provide infants their own space in a shared sleep environment while bed-sharing (Queensland Health, Queensland Clinical Guidelines, 2022; Raising Children Network, 2024a; South Australia Health, Government of South Australia, 2022; Victoria State Government, Safer Care Victoria, 2021), and the use of sleeping bags was in n = 16 documents. No documents specifically stated sleeping bags should be used instead of bedding or blankets.
Placing the infant in the lower third of the cot (feet-to-foot position) was stated in n = 13 documents. Only n = 6 documents referred to dummy/pacifier use, five of those noting that dummy use may be a protective factor against SUDI (NSW Government, 2021; Queensland Health, Queensland Clinical Guidelines, 2022; South Australia Health, Government of South Australia, 2022; Victoria State Government, Safer Care Victoria, 2021; Western Australian Department of Health, Chief Nursing and Midwifery Office, 2023).
Many documents (n = 16) included swaddling/infant wrapping, while the context and use of swaddling/infant wrapping was diverse. Some documents discussed its help with settling and how to keep infants safe when wrapping, such as using light wrapping and to stop swaddling when the infant begins to roll, but only eight documents specifically stated that infants who bed-share with an adult should not be wrapped.
As shown in Table 4, documents included in this analysis ranged from adopting strong RM approaches to strong RE approaches with a mean score of 8.62 (SD = ±5.95). This does not reflect that most documents were ‘balanced’, rather that some features of RM and RE were included; wide variability in scores highlights the considerable lack of consistency between documents on the approach taken to discussing safer infant shared sleep.
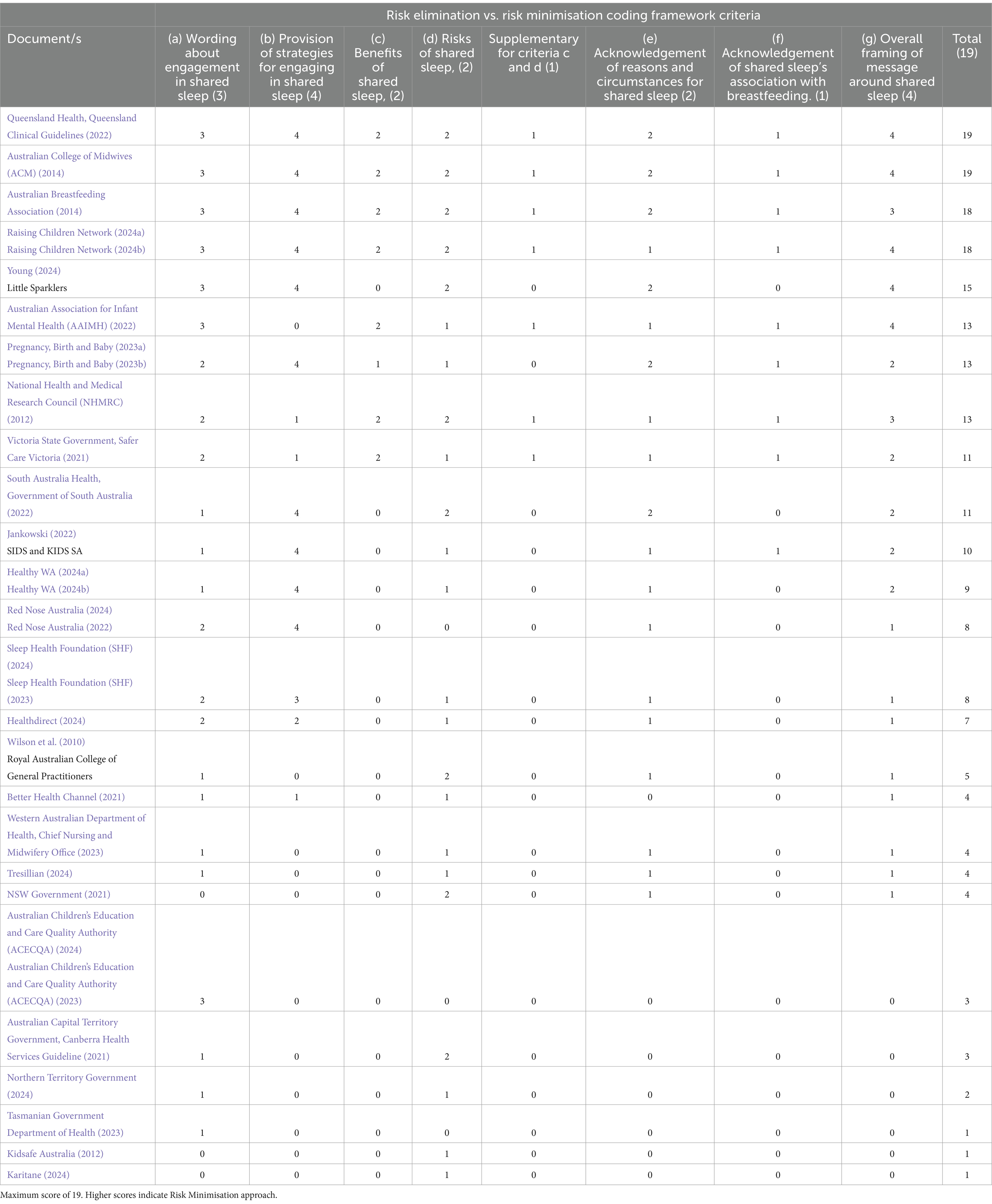
Table 4. Risk elimination vs. risk minimisation coding framework criteria.
Wording around engagement in shared infant sleep varied considerably, with half of the documents (n = 13) taking a neutral position regarding where infants should sleep, or preferenced cot sleeping but did not deem shared sleeping as unsafe, while the other half stated that parents should not engage in shared sleep in any capacity or referred to cot sleeping as the safest location and/or the adult bed as unsafe.
Most of the documents that provided a neutral position (n = 13), had higher RM scores, and their messaging aimed to engage families in informed decision making regarding shared-sleep, including consideration of circumstances, preferences and intentionality using non-judgement, practical and solution-focused language. Three documents, that preferenced cot sleeping but did not deem shared sleeping as unsafe, and that had lower scores of 8 and 7 overall (indicating some RE and some RM features), were found to have highly prescriptive messaging, minimal acknowledgement of individual family circumstances and minimal encouragement for parents to consider different sleep strategies and options to meet their circumstances (Healthdirect, 2022; Red Nose Australia, 2022, 2024; Sleep Health Foundation (SHF), 2023, 2024).
Most documents (n = 23) provided potential risks of infant shared sleep, while fewer included potential benefits (n = 8). For most therefore there was an imbalance between the provision of risks against benefits (n = 19).
Almost two-thirds of documents (n = 15) provided no strategies for how to safely engage in shared sleep or most of their strategies focused on when to avoid shared sleep (e.g., shared sleep if you or your partner smokes). Documents that did include strategies for shared infant sleep typically also included suggestions for the bed/bedroom set up (e.g., moving the mattress or bed away from the wall, so your baby cannot get trapped) or the infant’s positioning (e.g., laying them on their back beside one parent, not in-between two people).
Fewer than half of the documents (n = 6) provided acknowledgement that shared sleep may be a familial or culture preference, may occur due to environmental limitations, or that it can occur intentionally or unintentionally. In half of the cases there was some acknowledgement of potential reasons or circumstances for shared sleeping although these were minimal or only focused on one consideration (e.g., culture). In n = 9 documents there was acknowledgment of shared sleep’s association with breastfeeding outcomes, which was also often stated as a benefit to shared sleep as well. Seven documents made no acknowledgement of reasons or circumstances for shared sleep.
Nineteen documents referred or acknowledged that infant safer sleeping information could be sought from sources external to their organisation or that their own guidelines were taken from, or developed in collaboration with, such sources.
The most commonly referred to or acknowledged external source was Red Nose, referred to by n = 12 other documents/organisations. Additionally, n = 3 other documents referred to SIDS and KIDS, prior to Red Nose’s rebranding and one document referred to Red Nose specifically in relation to their room sharing recommendation.
Raising Children Network was also referred to by a few documents/organisations, in relation to both infant safer sleep information generally, and shared sleeping.
This review evaluated documents publicly available to people living in Australia that contain information regarding infant safer sleep, whether these are designed for caregivers or the information is disseminated through third parties (i.e., healthcare professionals). Evaluation was focussed on the consistency of infant safer sleep information (including surface sharing messaging), and whether messaging on surface sharing took a RE or RM approach.
The consistency of information between documents generally aligned with infant safer sleep messaging recommended by ISPID, with no documents contradicting recommendations that ISPID deemed to be internationally consistent. This was positive and suggests that organisations are including appropriate and evidence-based recommendations for infant safer sleep. However, there were significant inconsistencies in the number of recommendations included and only one document included all 13 ISPID recommendations (Queensland Health, Queensland Clinical Guidelines, 2022). Recommendations coined as the ‘Safe Six’ by Red Nose Australia (Red Nose Australia, 2024) were the most frequently included recommendations. Higher consistency across these recommendations is likely due to Red Nose Australia being a member of ISPID and regarded by some as one of Australia’s most renowned sources of infant safer sleep messaging (Australian Children’s Education and Care Quality Authority (ACECQA), 2024; Healthdirect, 2024; Young, 2018). Indeed, this review found that 15 documents acknowledged the existence of, referred the reader to, or that their information had come from, Red Nose Australia (or as previously known as SIDSandKIDS).
Contrastingly, many recommendations not included in most documents may be seen as ‘extensions’ of others. For example, while most documents stated that infants should be placed on their backs to sleep, fewer explicitly stated that infants should not sleep on an incline. It is acknowledged that this recommendation could also have been covered in the wording of guideline 1 (baby on back) or 4 (use a firm, flat mattress), however, as ISPID has stated this as a separate recommendation, this review evaluated it as such.
Finally, most documents also clearly stated that sleeping on a sofa or a chair with an infant was unsafe and/or should be avoided. The risk of SUDI from sofa sharing has been found to be high (Blair et al., 2014) due to the risk of entrapment. This message is important to relay to caregivers, but there are documents which group messaging around bed-sharing with sofa sharing (South Australia Health, Government of South Australia, 2022; Western Australian Department of Health, Chief Nursing and Midwifery Office, 2023). As per ISPID recommendations, the two practices are distinct from one another, acknowledging the significant difference in risk each holds. Messaging that merges the two practices can result in confusion while failure to specifically discuss sofa sharing as different from bed-sharing may result in parents misinterpreting that the risks and strategies apply across contexts; misinformed risk mitigation by parents has unintentionally increased SUDI risk (Cole et al., 2021c).
A secondary aim of this review was to evaluate the information regarding shared sleep. Results highlight that while most documents did discuss shared sleep, there was considerable variation in messaging towards RM or RE approaches, with multiple documents sitting at both extremes, and a few documents scattered throughout the middle of the rating scores (typically indicating the presence of some RM features in an otherwise RE focused document). Other documents scored low, not necessarily because they actively advised against shared sleep but because they were missing information about shared sleep generally.
Furthermore, there was also a notable difference in consistency across the different government documents, both regarding whether RM or RE approaches were taken and in the breadth of the inclusion of ISPID recommendations. For example, Queensland’s guidelines (Queensland Health, Queensland Clinical Guidelines, 2022) scored 19, the highest scores of the review, showing a strong RM position being taken with detailed discussions in their document regarding strategies, risks, benefits, and informed decision making, keeping language neutral/balanced and non-alarmist. This contrasts with webpages from the Northern Territory and Tasmanian governments (Northern Territory Government, 2024; Tasmanian Government Department of Health, 2023) who explicitly advise against shared sleep, provide no strategies for safe shared sleep and their reporting of ISPID recommendations were also minimal. Unlike Queensland and other state and territory documents reviewed, comprehensive guideline documents and operational statements could not be found for the Northern Territory and Tasmania. While more detailed documentation may be available, it does not appear to be publicly available or easily accessible and thus not likely to be encountered by parents looking for safety guidance. Additionally, such government documents may also act as overarching guidelines or policies for other organisations, (e.g., the New South Wales’ guidelines (NSW Government, 2021) would be adopted by each regional healthcare or council service within the state). While it was out of the scope of this review to examine the consistency within organisations, contradictory stances within the same document were seen. For example, in the resource of National Health and Medical Research Council (NHMRC)’s (2012) the document itself mentions co-sleeping briefly, although an insert in the appendix from the Royal Australasian College of Physicians Breastfeeding Position Statement moved the document’s approach from RE to RM. Likewise a strong RE stance by NSW Government (2021) referred to Raising Children Network (2024a, 2024b) which presented a more neutral approach within the co-sleeping statement.
Discrepancies in the inclusion of ISPID guidelines and the shift of messages from RE to RM or vice versa between documents assumed to be internally consistent, can confuse parents, making them adopt practices with the potential to increase, rather than reduce risk for babies (Cole et al., 2021c).
The language used in documents that were strongly RE focused was typically prescriptive, directly instructing parents (or healthcare workers) what they should or should not do, with minimal to no consideration of the circumstances or preferences of the family, or the likely possibility of unintentional bed-sharing. Health promotion messaging and programs that rely on didactic styles of communication in which it is perceived that an authority, rather than the target person/s, is in control, can negatively result in resistance to change (Laverack, 2017). Furthermore, it disregards the person’s circumstances and perceptions, leading to experiencing the sources of the recommendations are paternalistic, thereby risking further disengagement (Laverack, 2017). That is not to say that RE approaches constantly fail to adopt family-centered communication as part of their education strategies. Rather, this review highlights that the scope of such communication does not extend to shared sleep.
Families that experience social vulnerability also tend to reject ‘do-and-do-not’ advice finding it condescending and unhelpful (Pease et al., 2017). Many documents that were RE focused used strong language targeted towards highlighting the severity of potential risk. The identification of fear as a potential influencer of change may also produce unintended consequences including avoidance, stigmatization, anxiety, and increased risk behaviour (Cole et al., 2021c; Earl and Albarracín, 2007; Kok et al., 2018; Ruiter et al., 2014). Other documents, perhaps in an effort to ‘soften’ their language but remain clear on their messaging to discourage shared sleep, included messaging around how the safest place for an infant to sleep was in a cot (Healthdirect, 2022; Karitane, 2024), and discuss co-sleeping as a choice [i.e., ‘if you choose to co-sleep’ (Red Nose Australia, 2022); ‘if you do choose to start sharing a sleeping surface’ (Healthy WA, 2024b)]. Rather than making co-sleeping parents feel empowered and informed about their sleep environment, such examples push the onus of any possible risk onto parents, designating them as the enablers of an unsafe safe environment.
Breastfeeding was included in both parts of this review. Recommendation 10 from ISPID stated that breastfeeding should be encouraged and supported, with the review finding that most organisations mentioned breastfeeding (73%). In regards to shared sleeping, as previous research has shown the strong bi-directional link between breastfeeding and shared sleep (Bailey, 2016; D’Souza et al., 2024; Goldberg and Keller, 2007; McKenna et al., 2007; Salm Ward, 2015), the acknowledgement of shared sleep’s association with breastfeeding was considered to be an important inclusion in determining whether organisations were taking an RE or RM approach to shared sleep. This review found that approximately only one-third of the documents reviewed specifically acknowledged this link (35%). These results highlight that the positive association that shared sleep can have on supporting breastfeeding mothers is not being commonly acknowledged in guidelines or spoken about in Australia. The World Health Organisation (WHO) recommends that infants are exclusively breastfed for the first 6 months of life, and that breastfeeding alongside complementary foods should continue for at least the first 2 years of life, (World Health Organisation, 2021). In 2022, the Australian Government released the Australian National Breastfeeding Strategy (Australian Government, Australian Government Department of Health and Aged Care, 2022), aiming to increase the number of breastfed babies and improve and increase the education and support available to parents. This, as well as support from groups such as the Australian College of Midwives (ACM) (2021) and Australian Breastfeeding Association (2021), has backed the encouragement and promotion of breastfeeding by healthcare professionals when women choose or are able to breastfeed, respecting the choice of the mother. With infant sleep and feeding going hand-in-hand and many of these documents being used or referred to by healthcare professionals in their communication with parents, it appears that documents that take a RE approach miss the opportunity to provide parents with education and validation around the use of shared sleep to help support their breastfeeding journey. Documents continue to fail to acknowledge this association, further contributing to the structural and societal barriers that hinder mothers continuing to breastfeed (Rollins et al., 2016).
Within RM focused public messaging, there are concerns that the provision of information may permit people to engage in undesired behaviours, and that potential risks are downplayed. However, the absence of balanced information on shared sleep can be just, if not more dangerous. While efforts continue to educate parents not to bed-share, the prevalence of shared sleep remains high with parents’ bed-sharing intentionally and unintentionally (Cole et al., 2020; Cunningham et al., 2018; D’Souza et al., 2024). As this review showed, documents that take a more RE approach often fail to provide information on how to minimize risk when engaging in shared sleep. Further to this, the language in such approaches can be seen as judgmental, preferencing one sleep arrangement over another, potentially causing distress and confusion for parents when they are unable to settle infants in a separate sleep space (Cole et al., 2020; Cole et al., 2021c). Perceived negative attitudes towards co-sleeping by healthcare professionals, or restrictive policies can result in parents avoiding or concealing information from healthcare professionals (Bailey, 2016; Cole et al., 2021c; Kruse et al., 2024). Such gatekeeping of information may inadvertently result in lost opportunities to discuss infant safer sleep (including surface sharing) using a RM approach.
The lack of acknowledgement about alternative sleep arrangements in more RE focused documents also inhibits the opportunity to make informed choices based on parental preferences, circumstances and needs. Our review found that only seven documents ‘balanced’ their reporting of the potential benefits and risk of shared sleeping, and that 11 documents did not provide strategies on how to surface share safely. RM approaches are not designed to encourage people to engage in risky behaviours or view such behaviours as risk-free, but rather provide information to allow for informed decision making, in a judgement-free way, recognizing practical realities. A recent analysis of the literature by Shiells et al. (2024) further highlighted this, finding that discussions about motivations for safer sleep are often not discussed in safer sleep interventions, thus missing an opportunity for education and collaborative decision-making. RM approaches have been used successfully in public health initiative including safer sex (Yzer et al., 2000), substance use (Australian Department of Health, 2017), and liquor harm campaigns (Queensland Government, 2024). Providing parents with access to a range of sources, with both risk, benefits and strategies, encourages informed decision making.
The diversity in approaches currently taken in Australia, as found in this review, means that parents are likely to encounter contrasting information about shared sleep depending on where they live, and who and where they receive their information from. Further to this, some sources had placed their online information on infant safer sleep in locations difficult to access or required parents to navigate multiple pages, and/or click additional links to information across various websites, reducing accessibility.
In 2018 the Queensland Social Survey found that 65% of participants had used the internet to search for health information, the most common sources being health organisations and government websites (Nikoloudakis et al., 2018). Given the accessibility and the increased use of webpages/social media by people to gather health information governments, health organisations, and health platforms should ensure that online health information is accurate and clear, as well as accessible efficiently (Jia et al., 2021).
While evidently there are inconsistencies in the approach to discussing shared sleep, there is also evidence of movement towards the adoption of strategies that recognize and encourage RM characteristics. For example, Queensland government’s most recent co-designed update of the infant safer sleep guidelines (Queensland Health, Queensland Clinical Guidelines, 2022) which guide health professional practices and parent education in government facilities, included changes to the content and framing of messaging, adopting an explicit RM approach, and keeping families’ unique circumstances, concerns, and needs at the forefront alongside risk reduction strategies.
Similarly, with the creation of specific co-sleeping documents (Red Nose Australia, 2022; Raising Children Network, 2024b; Healthy WA, 2024b; Pregnancy, Birth and Baby, 2023b), organisations are acknowledging that the provision of bed-sharing strategies reduces potential harm through education, although as previously mentioned in some of these cases the language is still prescriptive, potentially perceived as judgmental (e.g., if you choose to bedshare) and may not always be easily accessible.
One consideration that was overlooked in most documents was regarding the culture of the family, and bed-sharing. In Australia, the prevalence of SUDI is higher in Indigenous Aboriginal and Torres Strait Islander infants than in non-Indigenous infants (Australian Institute of Health and Welfare, 2024), and Indigenous SUDI has not decreased at the same rate as non-Indigenous SUDI (Shipstone et al., 2020). Therefore, there are calls for targeted strategies in priority populations to reduce deaths (Dodd, 2012; Shipstone et al., 2020). Recently there have been campaigns aimed towards this (Red Nose Australia, 2022; Deadly Kids SA, 2019), however, messaging continues to state that they discourage shared sleep. As shared sleep is an important cultural and normal practice for many Indigenous families (Desmosthesous and Desmosthesous, 2011), it is imperative that strategies are culturally responsive and appropriate as to not further alienate the community (Dodd, 2012). The inclusion and discussion of in-bed devices (such as the Pēpi-Pod® portable sleep space or Coolamon Crib) is another initiative that plays a role in minimizing the risk of SUDI in ‘at-risk’ populations or when there are other factors present that may increase the risk of SUDI (McEniery et al., 2022), and where shared sleep is likely to occur, intended or not. However, only four documents in this review mentioned the use of such devices, highlighting a significant gap that needs to be filled in Australian infant safer sleep education and practice.
There were several limitations within the current review that should be considered. Firstly, it is acknowledged that not all Australian based organisations with infant safer sleep recommendations that would have otherwise met criteria for inclusion are present. While not all documents from all organisations have been included, the review does still include accessible government guidelines from each Australian state and territory, as well as recommendations that are likely to be most accessible by the public. Additionally, this review compared documents between sources, rather than within sources. Some organisations were found to have multiple documents for multiple features of infant safer sleep (e.g., separate, detailed documents for overheating, dummy use, use of slings), but to examine this level of consistency was outside the scope of the review, and some relevant information may have been missed. However, as discussed previously, it is also possible that further inconsistencies within organisations may also be present and it is encouraged that consistency within organisational messaging is continuously reviewed, as is effort to streamline information over multiple pages to increase accessibility.
It is also noted that the intended purpose and audience of the documents in this review varied (e.g., Red Nose (2022, 2024) is worded for parent/caregiver consumption while Victorian guidelines (Victoria State Government, Safer Care Victoria, 2021) are to be presented to parents; Australian Breastfeeding Association (2014) is a position statement of infant sleep, Australian Association for Infant Mental Health (AAIMH) (2022) is a position statement on sleep behaviours while SidsandKidsSA (Jankowski, 2022) appears as a blog post). Given this, the language, focus, and level of detail in the documents varied. However, it is highlighted that each of these documents are publicly available to be consumed by Australian parents and thus the depth, content, and consistency of their messaging is still relevant, particularly as accessing these documents and finding inconsistencies can result in confusion for parents.
Finally, the purpose of this review was to evaluate the consistency between documents and the approaches taken, not the quality of their content. Further research may explore this aspect of each document specifically, and it is encouraged that organisations that write such documents containing guidelines to use an internal quality measure before dissemination.
Accessible, evidence-based infant safer sleep information for parents and health professionals is critical to minimise the risk of SUDI. This review systematically examined the level of consistency, including in current approaches to shared sleep—a common infant care practice—in current, publicly available guidance documents.
Recommendations included in documents regarding infant safer sleep strongly reflected those recommended by IPSID, although the quantity of these recommendations varied. Shared sleep messaging varied, with considerable inconsistency in the provision of strategies to engage in safer shared sleep, the discussion of risks vs. benefits, and the consideration for culture and family circumstances and choices, as well as unintentional bed-sharing. The overall approach taken in the documents varied significantly between RM and RE approaches. This variation in messaging and the differing approaches taken regarding shared sleep likely contributes to parents and caregivers ‘filling the gaps’ themselves about what safer shared sleep may look like, thereby potentially engaging in risky behaviours due to confusion and poor access to quality resources. Further to this, while RE provides education on safer sleep generally, the scope of this education in relation to shared sleep is narrow, thus it restricts parents from engaging in informed decision making due to the lack of balanced information being presented, and feelings of being negatively judged by health professionals who are in turn bound by restrictive gatekeeping RE policies. There is a clear need for organisations that distribute infant safer sleep information, including information on shared sleep, to ensure their messaging is consistent, evidence-based and is considerate of the practical realities of infant sleep. The use of neutral and non-alarmist language may leave parents feeling more informed and empowered about strategies they can implement to create safer environments for their infant in a range or circumstances.
The datasets presented in this article are not readily available because the format of the data (Systematic Review) has no quantitative data analysis. Requests to access the datasets should be directed to c2FyYWgua3J1c2VAbW9uYXNoLmVkdQ==.
SK: Conceptualization, Data curation, Formal analysis, Methodology, Project administration, Validation, Writing – original draft, Writing – review & editing. LD'S: Conceptualization, Methodology, Supervision, Writing – review & editing. JY: Conceptualization, Methodology, Supervision, Writing – review & editing. HT: Formal analysis, Methodology, Writing – review & editing, Data curation, Validation.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. Sarah Kruse is a recipient of a Research Training Program (RTP) Scholarship provided by the Australian Government to support both domestic and international students undertaking Research Doctorate and Research Masters degrees.
The authors would like to thank Monash University Liaison Librarian Tracey Woods for her guidance regarding the search strategy and terms used.
JY is a volunteer member of the parent consumer charity Little Sparkler and was a founding member of the Red Nose (formerly SIDS and Kids) National Scientific Advisory Group (2004-June 2021). JY also provided content expertise and was co-lead in the development of the Queensland Health Safer Infant Sleep guidelines and has consulted, on request, to a range of organizations providing safe sleep information for health professionals and families including the Raising Children’s Network (RCN), Red Nose, Australian Breastfeeding Association, and the Australian College of Midwives.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Gen AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcomm.2025.1527164/full#supplementary-material
Australian Association for Infant Mental Health (AAIMH) (2022). Infant sleep. AAIMH, Norwood (AU). AAIMH, Available at: https://www.aaimh.org.au/media/website_pages/resources/position-statements-and-guidelines/sleep-position-statement-AAIMH_final-March-2022.pdf (Accessed August 22, 2024).
Australian Breastfeeding Association (2014). Position statement on safe infant sleeping, Available at: https://www.breastfeeding.asn.au/sites/default/files/2021-10/POL-Statement%20Safe%20Infant%20Sleeping-V2.1-201403.pdf (Accessed August 22, 2024).
Australian Breastfeeding Association (2021). Position statement on breastfeeding. Available at: https://www.breastfeeding.asn.au/sites/default/files/2021-11/POL-Statement%20on%20Breastfeeding-V2.2-201311_1%20%282%29.pdf (Accessed November 01, 2024).
Australian Capital Territory Government, Canberra Health Services Guideline (2021). Safe sleeping guideline: Neonates and infants up to 12 months of age. ACT Government, Canberra (AU). Available at: https://www.canberrahealthservices.act.gov.au/about-us/policies-and-guidelines?result_1981007_result_page=22 (Accessed August 22, 2024).
Australian Children’s Education and Care Quality Authority (ACECQA). (2023). Sleep and rest legislative requirements. ACECQA. Available at: https://www.acecqa.gov.au/resources/supporting-materials/infosheet/safe-sleep-and-rest-practices#NewLeg (Accessed August 22, 2024).
Australian Children’s Education and Care Quality Authority (ACECQA). (2024). Sleep and rest for children: policy guidelines. ACECQA. Available at: https://www.acecqa.gov.au/sites/default/files/2024-08/PolicyGuidelines_SleepRestForChildren_August2024.pdf (Accessed August 22, 2024).
Australian College of Midwives (ACM). (2014). Position statement for bed sharing and co-sleeping. Available at: https://www.midwives.org.au/common/Uploaded%20files/_ADMIN-ACM/Co-sleeping-and-Bed-sharing-(ACM)-Position-Statement-2014.pdf (Accessed August 22, 2024).
Australian College of Midwives (ACM). (2021). Position statement for infant feeding. Available at: https://www.midwives.org.au/common/Uploaded%20files/_ADMIN-ACM/Infant%20Feeding%20Position%20Statement%202021.pdf (Accessed November 01, 2024).
Australian Department of Health. (2017). National drug strategy 2017–2026. Commonwealth of Australia, Canberra (AU), 2024. Available at: https://www.health.gov.au/sites/default/files/national-drug-strategy-2017-2026.pdf (Accessed August 22, 2024).
Australian Government Department of Health and Aged Care. (2022). Australian National Breastfeeding Strategy, Australian Government Department of Health and Aged Care, Canbeera (AU). Available at: https://www.health.gov.au/sites/default/files/documents/2022/03/australian-national-breastfeeding-strategy-2019-and-beyond.pdf (Accessed November 01, 2024).
Australian Institute of Health and Welfare. (2022). Infant and child deaths: Australian Government, Canberra (AU). Available at: https://www.aihw.gov.au/reports/children-youth/australias-children/contents/health/infant-child-deaths (Accessed August 22, 2024).
Australian Institute of Health and Welfare. (2024). Aboriginal and Torres Strait islander health performance Framework.1.20 infant and child mortality, Available at: https://www.indigenoushpf.gov.au/measures/1-20-infant-and-child-mortality (Accessed August 22, 2024).
Baddock, S. A., Purnell, M. T., Blair, P. S., Pease, A. S., Elder, D. E., and Galland, B. C. (2019). The influence of bed-sharing on infant physiology, breastfeeding and behaviour: A systematic review. Sleep Med. Rev. 43, 106–117. doi: 10.1016/j.smrv.2018.10.007
Bailey, C. (2016). Breastfeeding mothers' experiences of bedsharing: a qualitative study. Breastfeed. Rev. 24, 33–40. doi: 10.3316/informit.268164166573611
Ball, H., Keegan, A. A., Whitehouse, D. R., Cooper, L. S., Lovell-Kennedy, S. R., Murray, L. M., et al. (2023). Multiagency approaches to preventing sudden unexpected death in infancy (SUDI): a review and analysis of UK policies. BMJ. Public Health 1. doi: 10.1136/bmjph-2023-000017
Barrett, S., Barlow, J., Cann, H., Pease, A., Shiells, K., Woodman, J., et al. (2024). Parental decision making about safer sleep practices: a qualitative study of the perspectives of families with additional health and social care needs. PLoS One 19:e0298383. doi: 10.1371/journal.pone.0298383
Barry, E. S. (2019). Co-sleeping as a proximal context for infant development: the importance of physical touch. Infant Behav. Dev. 57:101385. doi: 10.1016/j.infbeh.2019.101385
Barry, E. S., and McKenna, J. J. (2022). Reasons mothers bedshare: a review of its effects on infant behavior and development. Infant Behav. Dev. 66:101684. doi: 10.1016/j.infbeh.2021.101684
Better Health Channel. (2021). Sudden unexpected death in infants (SUDI and SIDS). Victoria State Government Department of Health. Available at: https://www.betterhealth.vic.gov.au/health/healthyliving/sudden-unexpected-death-in-infants-sudi-and-sids (Accessed August 22, 2024).
Blair, P. S., Sidebotham, P., Pease, A., Fleming, P. J., and van Wouwe, J. (2014). Bed-sharing in the absence of hazardous circumstances: is there a risk of sudden infant death syndrome? An analysis from two case-control studies conducted in the UK. PLoS One 9:e107799. doi: 10.1371/journal.pone.0107799
Carpenter, R., McGarvey, C., Mitchell, E. A., Tappin, D. M., Vennemann, M. M., Smuk, M., et al. (2013). Bed sharing when parents do not smoke: is there a risk of SIDS? An individual level analysis of five major case–control studies. BMJ Open 3:e002299. doi: 10.1136/bmjopen-2012-002299
Cole, R., Young, J., Kearney, L., and Thompson, J. M. (2021b). Priority setting: consensus for Australia’s infant safe sleeping public health promotion programme. J. Paediatr. Child Health 57, 219–226. doi: 10.1111/jpc.15178
Cole, R., Young, J., Kearney, L., and Thompson, J. M. D. (2020). Infant care practices and parent uptake of safe sleep messages: a cross-sectional survey in Queensland, Australia. BMC Pediatr. 20:27. doi: 10.1186/s12887-020-1917-5
Cole, R., Young, J., Kearney, L., and Thompson, J. M. D. (2021a). Awareness of infant safe sleep messages and associated care practices: findings from an Australian cohort of families with young infants. BMJ Paediatrics Open 5, –e000972. doi: 10.1136/bmjpo-2020-000972
Cole, R., Young, J., Kearney, L., and Thompson, J. M. D. (2021c). Challenges parents encounter when implementing infant safe sleep advice. Acta Paediatr. 110, 3083–3093. doi: 10.1111/apa.16040
Couto, G. R., Dias, V., and Oliveira I de, J. (2020). Benefits of exclusive breastfeeding: an integrative review. Nurs. Pract. Today 7. doi: 10.18502/npt.v7i4.4034
Cunningham, H. M., Vally, H., and Bugeja, L. (2018). Bed-sharing in the first 8 weeks of life: an Australian study. Matern. Child Health J. 22, 556–564. doi: 10.1007/s10995-017-2424-7
D’Souza, L., Morris, Z. A., Borgkvist, A., and Blunden, S. (2024). Understanding motivations and satisfaction with sleep location among co-sleeping (including bed-sharing) parents. Fam. Relat. 73, 661–682. doi: 10.1111/fare.12955
Deadly Kids SA. (2019). Safe sleeping. SA Health Government of South Australia. Available at: https://www.sahealth.sa.gov.au/wps/wcm/connect/4c273d06-e63a-476f-bc5b-b4f10cd9d1ec/Safe+Sleeping.pdf?MOD=AJPERES&CACHEID=ROOTWORKSPACE-4c273d06-e63a-476f-bc5b-b4f10cd9d1ec-nwKRUiF (Accessed August 22, 2024).
Desmosthesous, C., and Desmosthesous, T. (2011). The indigenous safe sleep project: Closing the gap on knowledge, resources and access in Queensland. Brisbane (AU): Sids and Kids Queensland.
Dieterich, C. M., Felice, J. P., O’Sullivan, E., and Rasmussen, K. M. (2013). Breastfeeding and health outcomes for the mother-infant dyad. Pediatr. Clin. North Am. 60, 31–48. doi: 10.1016/j.pcl.2012.09.010
Dodd, J. (2012). Evaluation of the Department of Health Western Australia operational directive statewide co-sleeping/bed-sharing policy for WA Health hospitals and health services. Department of Health, State of Western Australia, Western Australia (AU). Available at: https://www.health.wa.gov.au/~/media/Files/Corporate/general%20documents/Health%20Networks/Womens%20and%20Newborns/Evaluation-of-Statewide-cosleeping-bed-sharing-policy-for-WA-Health-Hospitals.pdf (Accessed August 22, 2024).
Doering, J. J., Salm Ward, T. C., Strook, S., and Campbell, J. K. (2019). A comparison of infant sleep safety guidelines in nine industrialized countries. J. Community Health 44, 81–87. doi: 10.1007/s10900-018-0556-3
Earl, A., and Albarracín, D. (2007). Nature, decay, and spiraling of the effects of fear-inducing arguments and HIV counseling and testing: a meta-analysis of the short- and long-term outcomes of HIV-prevention interventions. Health Psychol. 26, 496–506. doi: 10.1037/0278-6133.26.4.496
Fleming, P. J., Blair, P. S. P., Bacon, C., and Berry, P. J. (2000). “Sudden unexpected death in infancy” in The CESDI SUDI studies 1993–1996 (London: The Stationary Office).
Freemantle, J., and Ellis, L. (2018). “An Australian perspective” in SIDS sudden infant and early childhood death: The past, the present and the future. eds. J. R. Duncan and R. W. Byard (Adelaide (AU): University of Adelaide Press).
Goldberg, W. A., and Keller, M. A. (2007). Co-sleeping during infancy and early childhood: key findings and future directions. Infant Child Dev. 16, 457–469. doi: 10.1002/icd.522
Hayes, A. F., and Krippendorff, K. (2007). Answering the call for a standard reliability measure for coding data. Commun. Methods Meas. 1, 77–89. doi: 10.1080/19312450709336664
Healthdirect. (2022). Sudden infant death syndrome (SIDS). Australian Government Department of Health and Aged Care. Available at: https://www.healthdirect.gov.au/sudden-infant-death-syndrome-sids (Accessed August 22, 2024).
Healthdirect. (2024). Red nose. Australian Government Department of Health and Aged Care. Available at: https://www.healthdirect.gov.au/partners/red-nose (Accessed August 22, 2024).
Healthy WA. (2024a). Safe infant sleeping. Government of Western Australia Department of Health. Available at:https://www.healthywa.wa.gov.au/Articles/S_T/Safe-infant-sleeping#:~:text=Keep%20baby's%20head%20and%20face,safe%20cot%20in%20your%20room (Accessed August 22, 2024).
Healthy WA. (2024b). Co-sleeping and the risks to your baby’s health. Government of Western Australia Department of Health. Available at: https://www.healthywa.wa.gov.au/Articles/A_E/Co-sleeping-and-the-risks-to-your-babys-health#:~:text=Co%2Dsleeping%20is%20not%20recommended%20%E2%80%93%20it%20increases%20the%20risk%20of,that%20will%20make%20you%20sleepy (Accessed August 22, 2024).
Huang, Y., Hauck, F. R., Signore, C., Yu, A., Raju, T. N. K., Huang, T. T.-K., et al. (2013). Influence of bedsharing activity on breastfeeding duration among US mothers. JAMA Pediatr. 167, 1038–1044. doi: 10.1001/jamapediatrics.2013.2632
International Society for the Study and Prevention of Perinatal and Infant Death (ISPID). (2023). Safe infant sleep recommendations for the ISPID website evidence-based guidelines. Available at: https://www.ispid.org/fileadmin/user_upload/textfiles/ISPID_Safe_Sleep_Recommendations_23_Aug_2023__final_120623.pdf (Accessed August 22, 2024).
International Society for the Study and Prevention of Perinatal and Infant Death (ISPID). (2024). International Society for the Study and Prevention of Perinatal and Infant Death. Available at: https://www.ispid.org/index (Accessed August 22, 2024).
Jankowski, L. (2022). The co-sleeping debate - what you need to know. SIDS and Kids South Australia, Hindmarsh (AU). Available at: https://sidssa.org.au/2022/08/22/why-do-parents-choose-to-share-a-sleep-surface-co-sleep-and-what-things-should-they-consider-before-making-this-decision/ (Accessed August 22, 2024).
Jia, X., Pang, Y., and Liu, L. S. (2021). Online health information seeking behavior: a systematic review. Healthcare (Basel) 9:1740. doi: 10.3390/healthcare9121740
Karitane,. (2024). Safe sleep environments. Available at: https://karitane.com.au/safe-sleep-environments (Accessed August 22, 2024).
Kidsafe Australia. (2012). Safe sleep for infants: Information for parents and caregivers. Kidsafe Australia. Available at:https://www.kidsafevic.com.au/wp-content/uploads/2019/09/Safe-Sleeping-2012-national.pdf (Accessed August 22, 2024).
Kok, G., Peters, G.-J. Y., Kessels, L. T. E., ten Hoor, G. A., and Ruiter, R. A. C. (2018). Ignoring theory and misinterpreting evidence: the false belief in fear appeals. Health Psychol. Rev. 12, 111–125. doi: 10.1080/17437199.2017.1415767
Krous, H. F., Beckwith, J. B., Byard, R. W., Rognum TOBajanowski, T., Corey, T., et al. (2004). Sudden infant death syndrome and unclassified sudden infant deaths: a definitional and diagnostic approach. Pediatrics 114, 234–238. doi: 10.1542/peds.114.1.234
Kruse, S. P., D’Souza, L., Tuncer, H. G. G., and Stewart, S. E. (2024). Sources of attitudes towards parent-child co-sleeping and their effects: a systematic scoping review. Fam. Process 63, 2484–2504. doi: 10.1111/famp.13022
Laverack, G. (2017). The challenge of behaviour change and health promotion. Challenges (Basel) 8. doi: 10.3390/challe8020025
Marinelli, K. A., Ball, H. L., McKenna, J. J., and Blair, P. S. (2019). An integrated analysis of maternal-infant sleep, breastfeeding, and sudden infant death syndrome research supporting a balanced discourse. J. Hum. Lact. 35, 510–520. doi: 10.1177/0890334419851797
Marzi, G., Balzano, M., and Marchiori, D. (2024). K-alpha calculator–Krippendorff’s alpha calculator: a user-friendly tool for computing Krippendorff’s alpha inter-rater reliability coefficient. MethodsX 12:102545. doi: 10.1016/j.mex.2023.102545
McEniery, JA., Young, J., Cruice, DC., Archer, J., and Thompson, JMD. (2022). Measuring the effectiveness of the Pēpi-pod® program in reducing infant mortality in Queensland. Queensland Health State of Queensland, South Brisbane (AU).Available at: https://www.childrens.health.qld.gov.au/__data/assets/pdf_file/0017/176120/d8ea8e6a94ab355470c435a2363fbc6cfc129023.pdf (Accessed August 22, 2024).
McKenna, J. J., Ball, H. L., and Gettler, L. T. (2007). Mother-infant cosleeping, breastfeeding and sudden infant death syndrome: what biological anthropology has discovered about normal infant sleep and pediatric sleep medicine. Am. J. Phys. Anthropol. 134, 133–161. doi: 10.1002/ajpa.20736
Mileva-Seitz, V. R., Bakermans-Kranenburg, M. J., Battaini, C., and Luijk, M. P. C. M. (2017). Parent-child bed-sharing: the good, the bad, and the burden of evidence. Sleep Med. Rev. 32, 4–27. doi: 10.1016/j.smrv.2016.03.003
Mohamed Ahmed, S. O., Ashgar, R. I., Mohammed Abdelgader, A. A., Abdalla Hamid, H. I., Mathkor, D. M., Abdelsadig Ali, M. A., et al. (2023). Exclusive breastfeeding: impact on infant health. Clin. Nutr. Open Sci. 51, 44–51. doi: 10.1016/j.nutos.2023.08.003
Moon, R. Y., Carlin, R. F., and Hand, I. (2022). Sleep-related infant deaths: updated 2022 recommendations for reducing infant deaths in the sleep environment. Pediatrics (Evanston) 150. doi: 10.1542/peds.2022-057990
National Health and Medical Research Council (NHMRC). (2012). Literature review: infant feeding guidelines. Australian government National Health and Medical Research Council, Canberra (AU), Available at: https://www.nhmrc.gov.au/file/3346/download?token=-n_zgsh1 (Accessed August 22, 2024).
Nikoloudakis, I. A., Vandelanotte, C., Rebar, A. L., Schoeppe, S., Alley, S., Duncan, M. J., et al. (2018). Examining the correlates of online health information–seeking behavior among men compared with women. Am. J. Mens Health 12, 1358–1367. doi: 10.1177/1557988316650625
Northern Territory Government. (2024) Sleep and your child: zero to six years. Available at: https://nt.gov.au/community/parents-and-families/sleep-and-your-child-zero-to-six-years/safe-sleeping (Accessed August 22, 2024).
NSW Government. (2021). Recommended safe sleep practices for babies. NSW Government, New South Wales (AU). Available at: https://www1.health.nsw.gov.au/pds/ActivePDSDocuments/GL2021_013.pdf (Accessed August 22, 2024).
Owens, J. A. (2004). Sleep in children: cross-cultural perspectives. Sleep Biol. Rhythms 2, 165–173. doi: 10.1111/j.1479-8425.2004.00147.x
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Syst. Rev. 10:89. doi: 10.1186/s13643-021-01626-4
Pease, A., Ingram, J., Blair, P. S., and Fleming, P. J. (2017). Factors influencing maternal decision-making for the infant sleep environment in families at higher risk of SIDS: a qualitative study. BMJ Paediatrics Open 1:e000133. doi: 10.1136/bmjpo-2017-000133
Pregnancy, Birth and Baby. (2023a). Safe sleep for babies. Australian Government Department of Health and Aged Care. Available at: https://www.pregnancybirthbaby.org.au/safe-sleep-for-babies, (Accessed August 22, 2024).
Pregnancy, Birth and Baby. (2023b). Co-sleeping with your baby. Australian Government Department of Health and Aged Care. Available at: https://www.pregnancybirthbaby.org.au/co-sleeping-with-your-baby (Accessed August 22, 2024).
Queensland Family and Child Commission (QFCC). (2022). Deaths of children and young people Queensland 2021–2022. Queensland Government, Queensland (AU). Available at: https://www.qfcc.qld.gov.au/sites/default/files/2022-11/QFCC%20Annual%20Report%20Deaths%20children%20young%20people%20Queensland%202021%E2%80%9322.pdf (Accessed August 22, 2024).
Queensland Family and Child Commission (QFCC). (2023). Australian child death statistics 2020. Queensland Government, Queensland (AU). Available at: https://www.qfcc.qld.gov.au/sites/default/files/2023-03/QFCC%20Australian%20Child%20Death%20Statistics%202020.pdf (Accessed September 06, 2024).
Queensland Government. (2024). Liquor harm minimisation campaigns. Queensland Government, Queensland (AU), Available at: https://www.business.qld.gov.au/industries/hospitality-tourism-sport/liquor-gaming/liquor/harm-minimisation (Accessed August 22, 2024).
Queensland Health, Queensland Clinical Guidelines. (2022). Safer infant sleep. Queensland Health, Queensland (AU). Available at: https://www.health.qld.gov.au/__data/assets/pdf_file/0025/1166353/g-safer-sleep.pdf (Accessed August 22, 2024).
Raising Children Network. (2024a). Safe sleep environments for babies. Australian Government Department of Social Services. Available at: https://raisingchildren.net.au/babies/sleep/sleep-safety/safe-sleep-environments-for-babies (Accessed August 22, 2024).
Raising Children Network. (2024b). Co-sleeping with your baby. Australian Government Department of Social Services. Available at: https://raisingchildren.net.au/newborns/sleep/where-your-baby-sleeps/co-sleeping (Accessed August 22, 2024).
Raven, L. (2018). “Sudden infant death syndrome: history” in SIDS sudden infant and early childhood death: The past, the present and the future. eds. J. R. Duncan and R. W. Byard (Adelaide (AU): University of Adelaide Press).
Red Nose Australia. (2022). Co-sleeping, Available at: https://rednose.org.au/downloads/RN0493_23_Co-Sleeping.pdf (Accessed August 22, 2024).
Red Nose Australia. (2024). Safe Sleeping. Available at: https://rednose.org.au/downloads/Safe_Sleeping_Guide_for_Parents.pdf (Accessed August 22, 2024).
Rollins, N. C., Bhandari, N., Hajeebhoy, N., Horton, S., Lutter, C. K., Martines, J. C., et al. (2016). Why invest, and what it will take to improve breastfeeding practices? Lancet 387, 491–504. doi: 10.1016/S0140-6736(15)01044-2
Ruiter, R. A. C., Kessels, L. T. E., Peters, G.-J. Y., and Kok, G. (2014). Sixty years of fear appeal research: current state of the evidence. Int. J. Psychol. 49, 63–70. doi: 10.1002/ijop.12042
Salm Ward, T. C. (2015). Reasons for mother–infant bed-sharing: a systematic narrative synthesis of the literature and implications for future research. Matern. Child Health J. 19, 675–690. doi: 10.1007/s10995-014-1557-1
Salm Ward, T. C., and Doering, J. J. (2014). Application of a socio-ecological model to mother-infant bed-sharing. Health Educ. Behav. 41, 577–589. doi: 10.1177/1090198114543010
Shiells, K., Cann, H., Pease, A., McGovern, R., Woodman, J., Barrett, S., et al. (2024). A behaviour change analysis of safer sleep intervenions for infants at risk of sudden and unexpected death. Child Abuse Rev. 33:e2860. doi: 10.1002/car.2860
Shipstone, R. A., Young, J., Kearney, L., and Thompson, J. M. D. (2020). Prevalence of risk factors for sudden infant death among indigenous and non-indigenous people in Australia. Acta Paediatr. 109, 2614–2626. doi: 10.1111/apa.15274
Sleep Health Foundation (SHF). (2023). Safe sleeping and babies. Available at: https://www.sleephealthfoundation.org.au/sleep-topics/tips-to-help-baby-sleep-better (Accessed August 22, 2024).
Sleep Health Foundation (SHF). (2024). Tips to help baby sleep better. Available at: https://www.sleephealthfoundation.org.au/sleep-topics/safe-sleeping-and-babies (Accessed August 22, 2024).
South Australia Health, Government of South Australia. (2022). South Australian safe infant sleeping standards. Government of South Australia, South Australia (AU). https://www.sahealth.sa.gov.au/wps/wcm/connect/public+content/sa+health+internet/resources/south+australian+safe+infant+sleeping+standard (Accessed August 22, 2024).
Tasmanian Government Department of Health. (2023). Sleep and settling including safe sleep information, https://www.health.tas.gov.au/health-topics/child-and-youth-health/child-health-and-parenting-service-chaps/sleep-and-settling-including-safe-sleep-information (Accessed August 22, 2024).
Tresillian. (2024). Safe sleeping. Availble at: https://www.tresillian.org.au/baby/sleep/safe-sleeping/ (Accessed August 22, 2024).
Vennemann, M. M., Hence, H.-W., Bajanowski, T., Blair, P. S., Complojer, C., Moon, R. Y., et al. (2012). Bed sharing and the risk of sudden infant death syndrome: can we resolve the debate? J. Pediatr. 160, 44–48.e2. doi: 10.1016/j.jpeds.2011.06.052
Victoria State Government, Safer Care Victoria. (2021). Infant safe sleeping: Clinical guidance. Victoria State Government, Melbourne (AU). Available at: https://www.safercare.vic.gov.au/best-practice-improvement/clinical-guidance/neonatal/infant-safe-sleeping (Accessed August 22, 2024).
Vieira, G. O., de Oliveira Vieira, T., da Cruz Martins, C., de Santana Xavier Ramos, M., and Giugliani, E. R. J. (2021). Risk factors for and protective factors against breastfeeding interruption before 2 years: a birth cohort study. BMC Pediatr. 21, 310–10. doi: 10.1186/s12887-021-02777-y
Western Australian Department of Health, Chief Nursing and Midwifery Office. (2023). Safe Infant: safe infant sleeping guideline. Western Australian Department of Health; Western Australia (AU). Available at: https://www.health.wa.gov.au/~/media/Corp/Policy-Frameworks/Clinical-Services-Planning-and-Programs/Safe-Infant-Sleeping-Policy/Supporting/Safe-Infant-Sleeping-Guideline.pdf (Accessed August 22, 2024).
Wilson, L., Quine, S., and Lewis, M. (2010). Sleeping infants safely: considerations for GPs. Aust. Fam. Physician 39, 66–68
World Health Organisation. (2021). Breastfeeding. Available at: https://www.who.int/health-topics/breastfeeding#tab=tab_1 (Accessed November 01, 2024).
Young, J. (2024). Safer sleep. Little Sparklers. Available at: https://littlesparklers.org/infant-and-toddler-sleep/safer-sleep (Accessed August 22, 2024).
Young, J. (2018). “Promoting evidence-based public health recommendations to support reductions in infant and child mortality: the role of National Scientific Advisory Groups” in SIDS sudden infant and early childhood death: The past, the present and the future. eds. J. R. Duncan and R. W. Byard (Adelaide (AU): University of Adelaide Press).
Young, J., and Shipstone, R. (2018). “Shared sleeping surfaces and dangerous sleeping environments” in SIDS sudden infant and early childhood death: The past, the present and the future. eds. J. R. Duncan and R. W. Byard (Adelaide (AU): University of Adelaide Press).
Keywords: infant safer sleep, co-sleeping, bed-sharing, shared sleep, sudden infant death syndrome (SIDS), sudden unexpected death in infancy (SUDI)
Citation: Kruse SP, D’Souza L, Young J and Tuncer HGG (2025) A systematic evaluation and comparison of the consistency of infant safer sleep messaging in Australia. Front. Commun. 10:1527164. doi: 10.3389/fcomm.2025.1527164
Edited by:
Rukhsana Ahmed, University at Albany, United StatesReviewed by:
Bryanne Colvin, Washington University in St. Louis, United StatesCopyright © 2025 Kruse, D’Souza, Young and Tuncer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sarah P. Kruse, c2FyYWgua3J1c2VAbW9uYXNoLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.