 Suruchi Sood1*
Suruchi Sood1* Onika Beckles2Jennifer Orkis1Sean Wilson2Gabrielle Hunter1TrishAnn Davis1Mona Hussain1Kashana James3
Onika Beckles2Jennifer Orkis1Sean Wilson2Gabrielle Hunter1TrishAnn Davis1Mona Hussain1Kashana James3- 1Department of Health Behavior and Society, Center for Communication Programs, Bloomberg School of Public Health, Johns Hopkins University, Baltimore, MD, United States
- 2Breakthrough ACTION Guyana, Georgetown, Guyana
- 3National Malaria Program, Ministry of Health, Georgetown, Guyana
Between 2000 and 2019, malaria cases witnessed a global decline. Recent WHO data indicates a reversal of these gains, threatening the goal to eliminate malaria by 2030. In Guyana, malaria is concentrated in remote regions and among itinerant gold miners who have limited access to malaria health services and will thus often self-medicate or delay care. The government implemented a volunteer malaria tester (VMT) program to increase access to malaria testing and treatment in mining communities. Social and behavior change (SBC) interventions targeting psychosocial determinants of malaria-related behaviors complement this program. The “Lil Mosquito, Big Problem” (LMBP) campaign promotes malaria prevention, testing, and treatment behaviors among miners. This campaign, designed and implemented through a participatory human-centered design process, used the ideation model as its conceptual framework to address knowledge, attitudes, beliefs, and social norms to influence malaria-related behaviors. Surveys conducted in 2019 and 2022 among gold miners in regions 7 and 8 showed increased knowledge and improved psychosocial determinants associated with malaria prevention and treatment. Exposure to the combined VMT and LMBP interventions was associated with significantly higher levels of prompt care-seeking. Interventions should consider attitudes and perceptions and address descriptive norms and the benefits of prompt care-seeking and treatment adherence. Changes in the mining population and economic hardships impact these results. Theory-driven programs systematically designed and implemented through stakeholder involvement and engagement are practical and applicable to similar settings and SBC interventions on other global health issues.
Introduction
Past gains in malaria prevention and control efforts are evident from global data showing malaria cases falling from 243 million to 233 million and malaria deaths declining steadily from 864,000 in 2000 to 576,000 in 2019. However, the latest data from the WHO’s World Malaria Report (WHO, 2023) show that these gains have stagnated or even reversed, with a reported 249 million global malaria cases in 2022.
Guyana, like other countries in the Guiana Shield– Suriname, French Guiana, and parts of Venezuela, Colombia, and Brazil –has been reporting between 20,000 and 30,000 malaria cases since 2000 (PAHO). However, a 164% increase in the region between 2015 and 2019, threatens the region’s ability to eliminate malaria by 2030 (Malaria Elimination Initiative, 2023). Among several reasons, one of the main reasons for the resurgence of malaria cases is increased extractive industry and migration due to climate change in both known and new areas (De Salazar et al., 2021; Earle, 2011). The key drivers of malaria in Guyana and other countries in the Guiana Shield are mining and logging, tropical rainforest temperatures, rainfall, and agricultural activities (Abdallah et al., 2022).
In Guyana, malaria is prevalent in well-defined geographic areas with specific population groups (Vreden, n.d.). This includes the remote regions (Regions 1, 7, 8, 9, and some parts of 10), which account for 95% of reported cases in the country (USAID, 2014). Malaria is particularly high among itinerant gold miners, who typically have limited access to malaria services and higher malaria-related risk behaviors such as self-medication and delayed or no care-seeking for fever.
The World Health Organization (WHO) Global Technical Strategy for Malaria recommends universal long-lasting insecticidal net (LLIN) coverage with suitable preventive and curative interventions (WHO, 2015). Recent studies have shown that using LLINs in combination with indoor residual spraying may only be sufficient to reduce malaria cases if the broader influence of indirect factors, including economic activities, population demographics, and private demand for interventions, are considered (Smith et al., 2020). Combining social and behavior change (SBC) interventions focusing on psychosocial determinants of malaria-related behaviors with health systems strengthening and structural interventions is essential to achieving malaria elimination goals (Casella et al., 2024).
According to the literature, one important and often overlooked factor is how individuals, families, and communities act and adopt habits to protect themselves from malaria, highlighting the value of behavior change theory to inform evidence-based social and behavior change interventions (Roll Back Malaria Partnership, 2015; WHO, 2017a, 2017b). A recent systematic review of peer-reviewed literature and a supplemental manual search of gray literature attempted to determine the relationship between the measured psychosocial factors and malaria behaviors in low transmission settings. The results showed little variation in malaria-related knowledge in both high and low-transmission settings. Therefore, programs and research should work to understand better the psychosocial factors that are positively associated with care-seeking behaviors, such as norms, perceived response efficacy, perceived self-efficacy, and communication about malaria with others (Casella et al., 2024).
In Guyana, like elsewhere, malaria prevention efforts depend heavily on behaviors occurring at multiple levels, including individual, household, community, and societal. Households must obtain LLINs, a primary malaria control intervention through available distribution channels. Furthermore, individuals must use the LLINs consistently and care for them appropriately. Indoor residual spraying, another core malaria intervention, depends on the deployment of well-trained spray teams and individuals’ acceptance of residual spraying in their homes, agreeing to remove their possessions from the house before spraying, and refraining from major post-spray modifications of walls such as painting or hanging decorations, which can reduce spray efficacy. Supplementary vector control tools can help fill gaps in protection that LLINs and spraying cannot fill, such as outdoor exposure to malaria mosquitoes. However, no matter how efficacious an approach is, it will only be effective if people engage with it and use it appropriately (WHO, 2017a, 2017b). In the 2015 Malaria Treatment Guideline for Health Facilities in Guyana, the Ministry of Health of Guyana, the National Malaria Program, and the Pan-American Health Organization recommended antimalarials that are known to be efficacious and safe and that are unlikely to be affected by resistance once correctly applied at all levels of the health care system in Guyana. To provide the best-standardized treatment of malaria for the public and private sectors in Guyana, the Ministry of Health studied the epidemiological situation of malaria in Guyana to create an antimalarial treatment policy, guidelines for timely diagnosis and adequate doses of treatment for complicated and uncomplicated malaria and, in unstable and specific populations (Ministry of Public Health of Guyana, 2015).
While prevention is critical, the high burden of malaria morbidity and mortality requires people to seek care promptly if they suspect malaria. Prompt care-seeking is necessary for adequate case management, including testing, medication provision, and follow-up to ensure treatment adherence. Previous research has identified several barriers to malaria treatment adherence in Guyana among gold miners who often work in remote areas where established health facilities are scarce, making it difficult to access timely malaria diagnosis and treatment services. The mobile nature of their work and low literacy rates further compounds this issue. Many miners also need more specific information about malaria transmission, prevention, and treatment. In one survey, conducted in Guyana, 48% of respondents were only partially knowledgeable and 14% had inadequate knowledge. It is possible that miners may not fully understand the importance of completing prescribed treatments (Olapeju et al., 2020).
Moreover, a substantial number of miners resort to self-medication, using over-the-counter drugs, painkillers, or traditional herbal medicines instead of seeking proper medical treatment. These practices, driven by mistrust of formal health services and beliefs in the efficacy of self-treatment methods, significantly hinder treatment adherence. Studies reveal that treatment adherence is not a norm, and interpersonal communication regarding malaria prevention needs to be enhanced. Economic pressures also contribute to this issue. The high cost of losing work time for treatment and the expense associated with traveling to health facilities discourage miners from seeking appropriate malaria treatment. Consequently, the economic necessity to continue working often outweighs the perceived benefits of adhering to the complete treatment regimen (WHO, 2022; Casella et al., 2024).
Malaria elimination program in Guyana
Effectively managing uncomplicated malaria cases is a vital component of Guyana’s malaria control and elimination strategies. This includes early recognition of symptoms and prompt care-seeking, which is defined as care-seeking within 24 hours from the onset of fever at a health facility, facility provider, or community provider (WHO, 2015). Since 2017, the Vector Control Services National Malaria Program (VCS-NMP) in Guyana has implemented a community-based case management (CCM) program to improve timely access to malaria testing and treatment for gold mining communities. The program involves training members of mining communities, such as camp managers, cooks, and shopkeepers, as volunteer malaria testers (VMTs) to use rapid diagnostic tests to diagnose suspected uncomplicated malaria and provide treatment for positive malaria cases (Olapeju et al., 2020). In 2020, the supply-side structural case management intervention was complemented with a demand-generating SBC intervention, Lil Mosquito, Big Problem (LMBP), a multi-channel campaign to address psychosocial barriers and promote key malaria prevention, testing, and treatment behaviors among miners.
This paper aims to describe the process involved in the design, implementation, and evaluation of results from this multi-component intervention aimed at improving prompt care-seeking among gold miners who bear a high burden of malaria in Regions 7 and 8. This manuscript seeks explicitly to:
1. Assess pre- and post-intervention levels of prompt care-seeking among gold miners in Guyana, and;
2. Explore the direct and indirect influence of combined SBC interventions on prompt care-seeking post-intervention.
Conceptual framework
The LMBP effort is grounded within the ideational conceptual model for strategic communication and behavior change. The ideation model focuses on the multiple, interrelated psychosocial variables that commonly influence individual behavior, often in a cumulative way. The model has three components, each of which comprises several elements: (i) cognitive elements, which include variables such as attitudes, beliefs, values, and perceived threat (susceptibility and severity); (ii) emotional elements, which include emotional response to a health issue, empathy for others, and self-efficacy variables; and (iii) social elements including social support and influence, communication about malaria with others, and personal advocacy variables. These variables function like risk factors for disease, but positively: the more these ideational variables apply to a person, the more likely that individual is to adopt a behavior. The advantage of the ideational analysis approach is that, while it allows inspection of the individual variables that go into a cumulative ideation score, it also simultaneously emphasizes and analyzes all these factors, recognizing the potential for interactions among them while controlling for various demographic and contextual variables (Kincaid, 2000; Babalola and Kincaid, 2009; Storey et al., 2018).
A Guyana-specific ideation model was developed based on formative research and in consultation with the National Malaria Program. This model hypothesized that SBC interventions could address knowledge, skills, and ideational factors and help facilitate an enabling environmental context to promote LLIN acquisition, use, and care, as well as prompt care-seeking followed by testing and adherence to treatment. Specifically, the model addressed myths and misperceptions and improved prevention, testing, diagnosis, and treatment knowledge. Skills included using and caring for LLINs, monitoring symptoms, seeking information and care, and treatment adherence. Ideational factors highlighted the role of attitudes, perceived social norms, fear of side effects, interpersonal communication, self and response efficacy, and trust in health workers and government services (Figure 1).
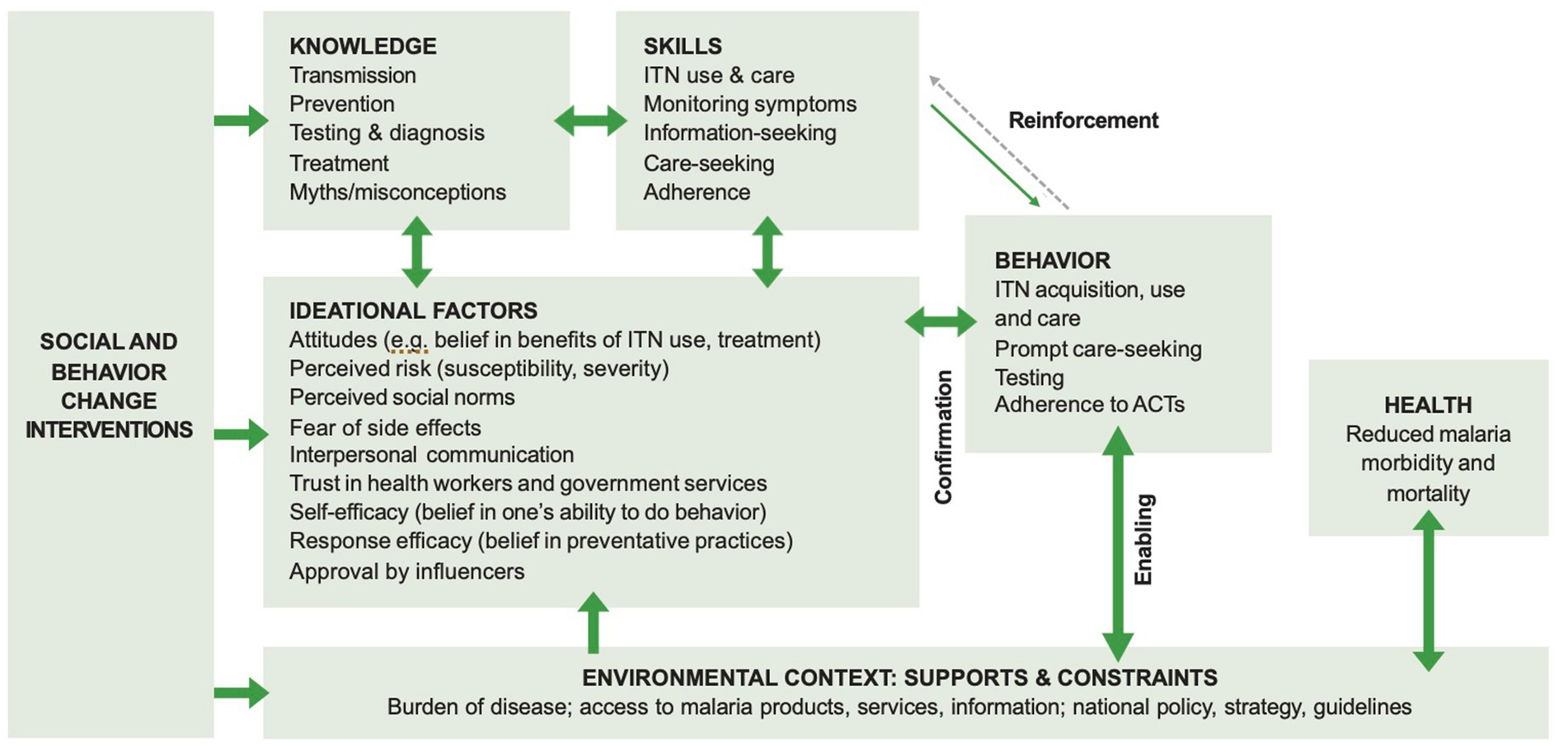
Figure 1. Ideation model for the Guyana LMBP campaign. Source: Guyana National Malaria Social and Behaviour Change Strategy 2021–2025.
Literature on using ideation for malaria
Studies suggest that malaria behaviors are often influenced by multiple psychosocial determinants simultaneously. The importance of different factors can vary across contexts and specific behaviors, highlighting the importance of locally available evidence to inform SBC programs.
There is significant literature on the usefulness of ideation as a framework to describe psychosocial determinants of malaria-related behaviors across settings (Monroe et al., 2021). SBC interventions employing the ideation model have been shown to significantly improve several malaria prevention and treatment behaviors, including household coverage of insecticide-treated nets (Ricotta et al., 2015; Storey et al., 2018), administration of artemisinin-based combination therapies (Babalola et al., 2018; Awantang G. et al., 2018; Awantang G. N. et al., 2018) and receiving preventive treatment with sulfadoxine-pyrimethamine during pregnancy (Awantang G. et al., 2018; Awantang G. N. et al., 2018). The impact of ideational variables on prompt care-seeking for fevers is also well-established in the literature (Do et al., 2018).
Previous research in Guyana has explored the relationship between gold miners’ malaria-related ideation and the adoption of behaviors, including prompt care-seeking. This research found that miners’ care-seeking/treatment ideation varied across subgroups, and ideation scores were associated with higher care-seeking for fever, getting tested for malaria, and lower odds of self-medication. The NMP has used these study findings to scale up their VMT model complemented by LMBP, a multi-channel mass media campaign to improve miners’ ideation (Olapeju et al., 2022).
Description of the LMBP campaign
The LMBP campaign is designed and implemented by the Breakthrough ACTION Guyana project, a multi-year USAID-funded activity led by Johns Hopkins Center for Communication Programs in collaboration with the VCS/NMP and Public Relations Health Promotion Unit (PR/HPU) of the MOH, and umbrella mining organizations including the Guyana Gold and Diamond Miners Association (GGDMA), Guyana Women’s Miners Organization (GWMO), Guyana Forestry Commission (GFC), and Guyana Geology and Mines Commission (GGMC). The LMBP campaign is innovative in that it is informed by a human-centered design (HCD) approach to understand and address miners’ ideation related to care-seeking and treatment and increase demand for malaria-related services (Yan et al., 2021). HCD is a qualitative method that helps groups solve problems and seek solutions by involving the human perspective in all steps of the problem-solving process. The HCD process generally involves three phases of sequential work: define, design and test, and apply, with measurement critical at every step for feedback, scale-up, and sustainability. HCD recognizes that people and their needs are changing, so solutions must adapt (Bazzano et al., 2017; Design for Health, n.d.).
Qualitative research with over 100 miners, camp managers, trained malaria testers, community health workers, pharmacists, regional administrative officers, and other vital stakeholders on the nature of current malaria services, behaviors around malaria testing, use of recommended and alternative treatments, and the broader malaria context that miners work in was used to create 11 insights, audience segments, personas, and journey maps. In HCD, insight is a deep understanding of users’ underlying needs, behaviors, motivations, and experiences. Insights are derived from research and are critical for guiding the design process and can be translated into specific design actions. Independent reflection and collaborative workshops were utilized to identify one or more “design opportunities” for each insight. These design opportunities involved converting the challenges present in each insight in the form of a question (i.e., “How might we?”), thus translating the insights into ideas, concepts, and solutions or prototypes. Personas are archetypal users representing larger groups’ needs, goals, values, and behaviors. The qualitative research generated personas to help understand and empathize with the target audiences realistically and humanistically. Multiple personas were identified for each of the stakeholder groups. The most evocative personas for each stakeholder group were further developed along with individual journey maps to illustrate the experience pathway or “journey” of a persona from their perspective, including a timeline, opportunities for intervention, and elements of the persona such as pain points, thoughts, and feelings (Richardson, 2010; Breakthrough ACTION Guyana, 2019; Yan et al., 2021).
The resulting LMBP campaign spans various channels, including radio, television, print materials, and social media. Initially, the campaign used a fictional miner’s experience to increase risk perception, self-efficacy, malaria knowledge, prompt care-seeking, and treatment adherence. This fictional character has subsequently been replaced with real-life stories and experiences of actual miners. The campaign also includes other influential persons in the mining community speaking out on the need for prompt and proper care-seeking for malaria. LMBP complements the VMTs’ efforts by branding malaria testing and treatment locations with flags to increase the visibility of the free program. Volunteer testers are trained and given certificates to promote their buy-in and validate them within their communities. The volunteer testers are also given job aids such as rapid counseling cards and a treatment pocket guide to improve the quality and accuracy of the service provided. Treatment adherence handouts and envelopes are given to malaria-positive clients that illustrate how the treatment regimen works to encourage treatment adherence (Breakthrough ACTION, n.d.; Breakthrough ACTION, n.d.).
Evaluation
A cross-sectional quantitative study, including a baseline and endline survey of gold miners, was completed to assess the impact of the combined VMT and LMBP interventions on miners’ behaviors and malaria outcomes in Regions 7 and 8. The baseline data was drawn from a 2019 baseline survey of 1,685 adult miners in regions 1, 7, and 8 (1,295 miners only in regions 7 and 8). Endline data were collected in 2022 from a cross-section of 1,251 miners in regions 7 and 8. Region 1 was excluded from the endline because, contrary to original plans, the LMBP and VMT programs were not fully implemented in Region 1 due to the lack of resources. This manuscript uses baseline and endline data only from regions 7 and 8. Full details of the research methodology applied in both surveys have been published elsewhere (Olapeju et al., 2020).
Due to the transitory nature of gold mining, a verification exercise was conducted before both surveys to confirm mining camp locations and numbers. This information was used to compile the final sample listing of mining camps. The survey cluster unit was the mining camp and the sample size calculation accounted for the lack of data on the size and distribution of the hard-to-reach mining population. Upon arrival at the selected mining camps, a gold miner was identified, and a trained data collector approached him/her to provide information regarding the purpose of the study. This was done using a standardized recruitment and consent script.
The study received institutional review board approval from the Johns Hopkins Bloomberg School of Public Health (IRB # 9884) and the Guyana Ethical Review Committee (#636/2019 and #135/2021). The data collector documented all enrolled miners’ written consent to participate.
After informed consent was obtained, the interviewer asked questions using a structured questionnaire. Interviews were administered face to face in a quiet location in the mining camp, with particular attention to privacy so that the interviewee’s responses could not be overheard. On average, the interviews lasted about 20 minutes. The questionnaire included the following sections: (i) Mining camp identification; (ii) Personal information; (iii) Psychosocial factors related to malaria; (iv) Malaria prevention, testing, and treatment behavior; (v) Exposure to malaria interventions. For both baseline and endline, 95% of gold miners consented to participate.
Key variables
The total sample of 2,546 miners in regions 7 and 8 were included in the baseline and endline analytical sample. This manuscript describes key demographics (residence, age, gender, education, marital status, ethnicity, religion) by comparing baseline and endline data.
Psychological factors identified from the ideation model include knowledge of malaria care-seeking and testing, beliefs about care-seeking, perceived susceptibility to and risk of malaria, perceived self-efficacy to seek and adhere to treatment, and response efficacy of care-seeking and treatment. Sociological factors include perceived norms related to care-seeking grouped as descriptive and subjective norms; communication about malaria with others/personal advocacy with family or friends related to care-seeking; and social influence (whether key people in miner’s life from within the mining community approve of care-seeking). Table 1 includes the specific questions asked to measure each ideation element, information on the number of questions used to measure each element, and explains how individual ideation variables were operationalized.
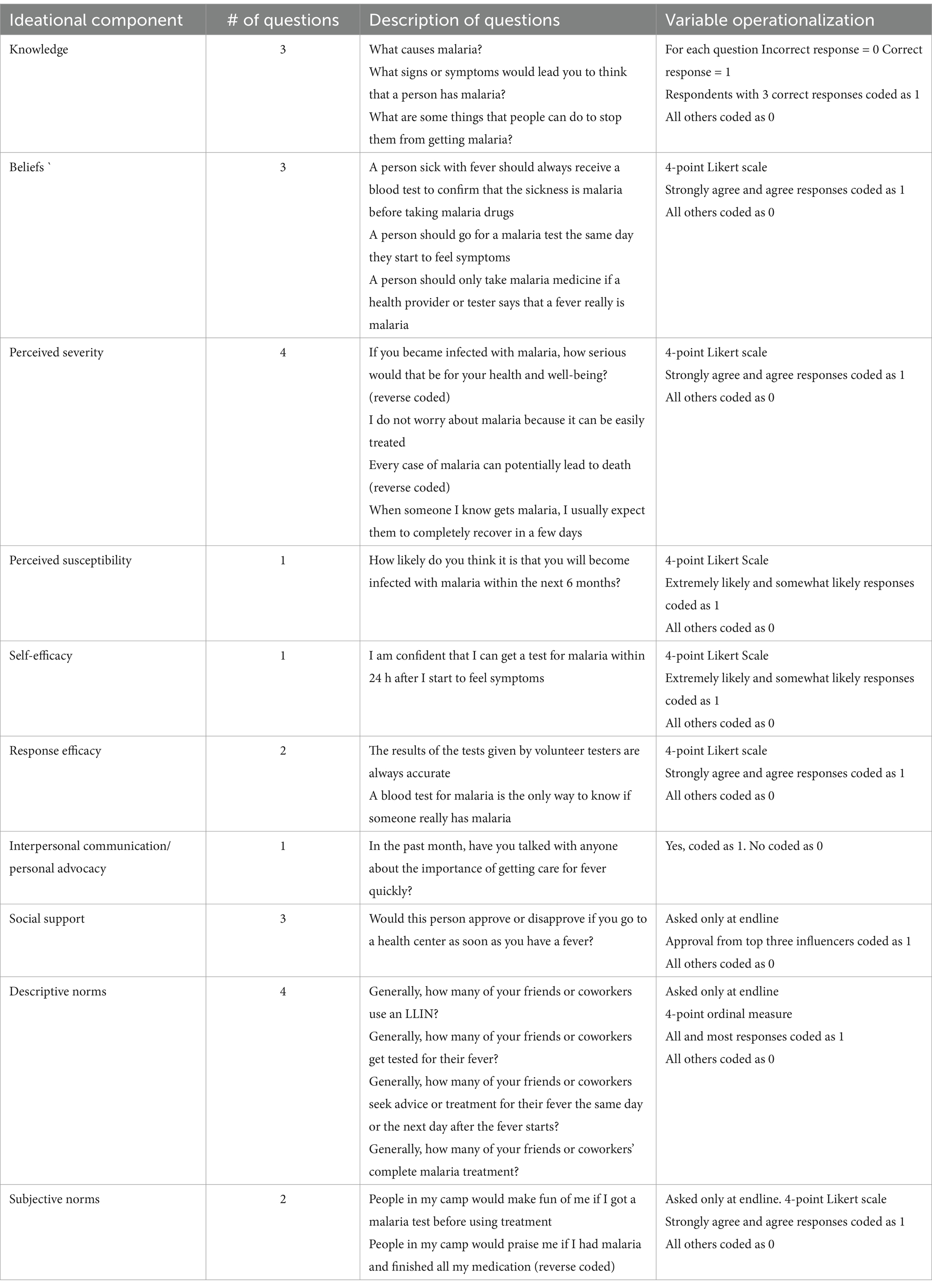
Table 1. Operationalization of the ideation variables.
All individual ideation elements were coded as categorical yes = 1 and no = 0. Three of the ideation questions, descriptive norms, subjective norms, and social support, were only asked at the endline. Therefore, these questions were dropped from the ideation score when comparing baseline with endline data. The ideation score for comparing baseline and endline ranged from 0 to 7, with the higher score representing positive ideation. Endline responses were added to create an additive index with scores ranging from 0 to 10, with the higher scores representing positive ideation. Endline ideation scores were used to examine the effect of exposure to the combined VMT and LMBP interventions.
Exposure to the complementary interventions was measured by creating an additive index of questions related to exposure to the different messages and materials in the LMBP campaign and reported knowledge of the VMT program. Combining these variables yielded a three-level variable. Miners who did not know anything about the LMBP or the VMT program were coded as having “no exposure”; exposure only to LMBP or exposure only to VMT was combined to measure “Exposure to either LMBP or VMT,” while exposure to both VMT and LMBP were combined to measure “Exposure to both LMBP and VMT.”
The key outcome of this study is prompt care-seeking, which is defined as “seeking advice or treatment the same or the next day after the onset of fever symptoms (WHO, 2015).” Prompt care-seeking was measured as responding to the following question: “How long after the fever started did you seek advice or treatment?” The reason for selecting prompt care-seeking as the primary outcome variable was that it could be considered a gateway behavior, with testing, treatment, and adherence contingent upon prompt care-seeking. A gateway behavior in public health refers to an initial behavior or practice that leads to or facilitates further behaviors. Gateway behaviors are crucial because they can initiate a cascade of positive health practices, leading to more comprehensive and effective malaria control and elimination efforts. According to the WHO (2015), initial preventive actions for malaria control include using insecticide-treated bed nets (ITNs) and early diagnosis and treatment, which can act as gateway behaviors leading to broader and more comprehensive malaria control efforts.
Statistical methods
Analytical methods used in this manuscript include tests of association (Chi-square for exploratory analysis) and crude and adjusted logistic regressions to measure the impact of background variables, ideation, and exposure on prompt care-seeking.
Results
The demographic characteristics of the sample populations were similar between baseline and endline, with a few exceptions. Table 2 compares the demographic background of miners at baseline with the endline, noting statistically significant differences.
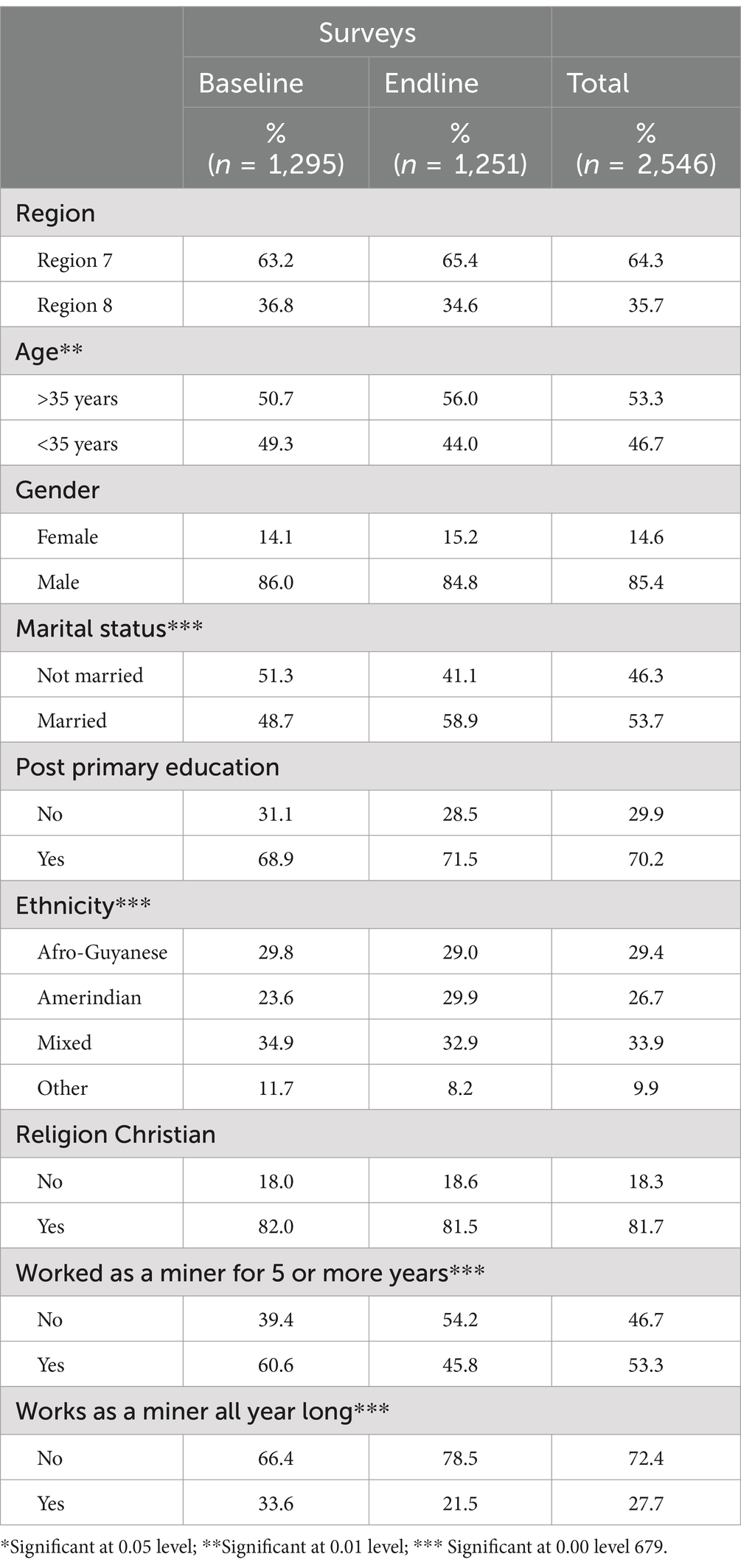
Table 2. Characteristics of the sample baseline versus endline.
The results shown in Table 2 show that miners were male (86%) and Christian (81%) with a primary level of education (70%). These results indicate some similarities in the demographic profiles of the miners as well as several significant differences between baseline and endline data collection. At baseline, the sample included significantly higher numbers of unmarried, mixed race, and more experienced individuals who worked as miners all year round in comparison to the endline where the miners were older, worked part-time as miners, and had been miners for less than 5 years. Bivariate results comparing baseline and endline data for individual ideation variables are presented in Table 3.
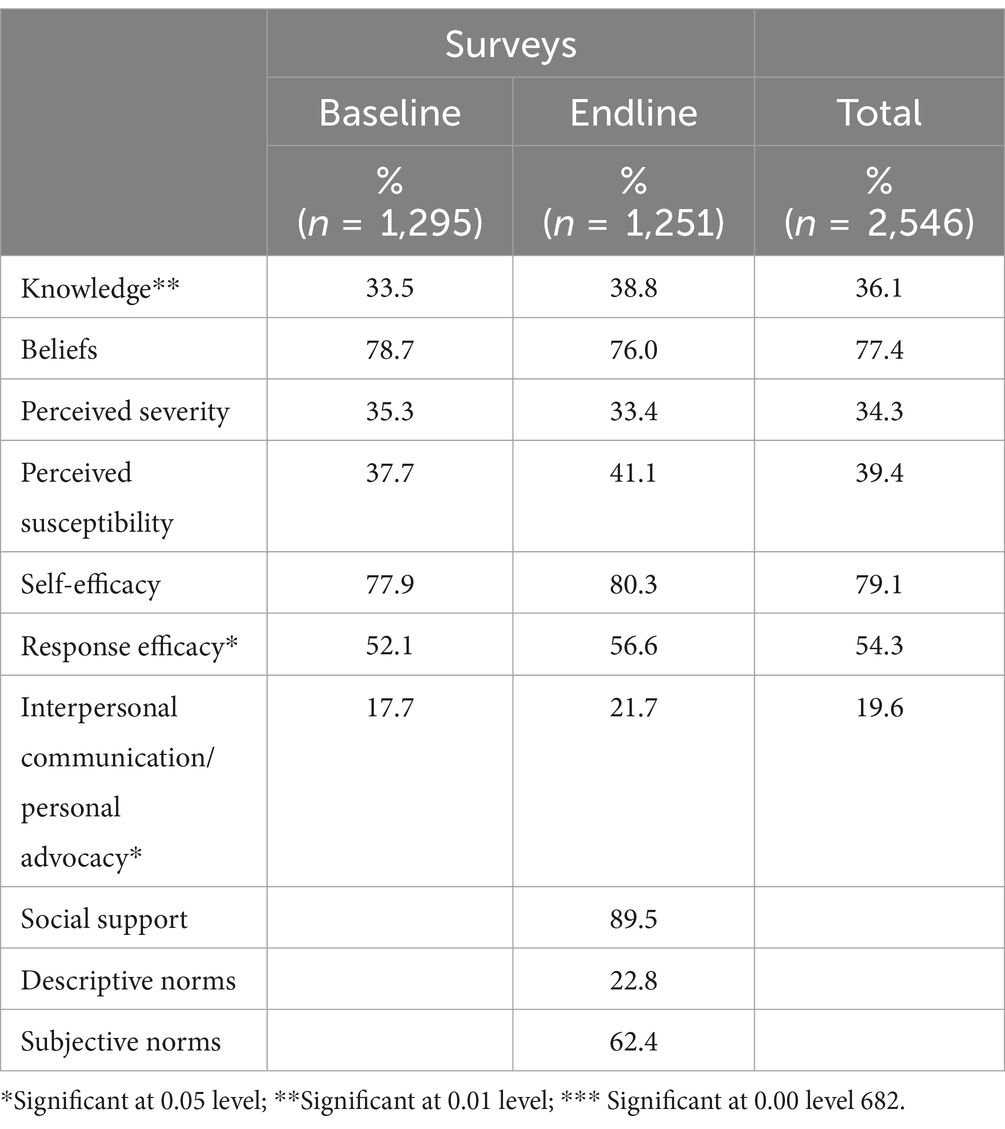
Table 3. Bivariate comparisons of ideation between baseline and endline.
A comparison of baseline and endline data reported in Table 3 shows that significantly more miners reported knowledge, response efficacy, and communication about malaria with others/personal advocacy at the endline compared to the baseline. For the ideation questions asked only at the endline, the results show that social support was remarkably high; some six out of 10 respondents reported positive subjective norms, but less than a quarter reported positive descriptive norms. The mean ideation score for the 10 variables asked in the endline survey was 4.7, whereas the mean ideation score for the seven variables included in the baseline and endline were 4.2 and 3.4, respectively. Knowledge about the VMT program and exposure to the LMBP campaign of the overall SBC intervention was measured by computing a four-level variable. The LMBP campaign included several messages and materials; at the endline, 77% of miners recalled at least one LMBP campaign component, and a third of the miners knew about the VMT program. Overall endline results show that slightly more than a quarter of the respondents knew about both the VMT program and LMBP campaign, 6% reported knowledge about the VMT program but not the LMBP campaign and 50% were exposed to the LMBP campaign but did not know about VMTs. Figure 2 provides information on the endline scores for this measure of exposure.
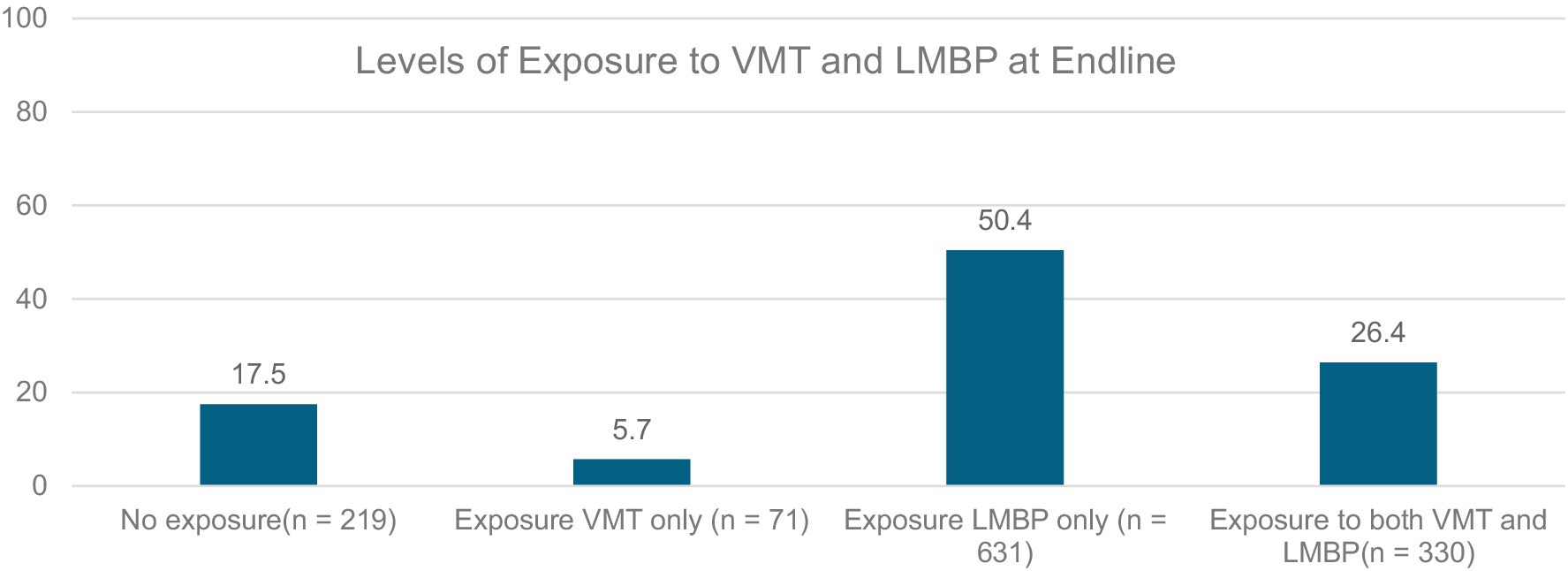
Figure 2. Levels of exposure to the VMT and LMBP at endline.
For the analysis, the miners who reported exposure to the VMT only (n = 71) or exposure to the LMBP campaign only (n = 631) were combined to include miners who were exposed to either the VMT or the LMBP campaign (n = 702). The key outcome behavior, prompt care-seeking, was only asked of respondents who reported fever in the past 12 months. Overall, 1,028 respondents reported having a fever 12 months before the survey. Approximately half of the 1,028 respondents who had fever sought treatment promptly. Baseline respondents were less likely, at 47.3%, to seek prompt care for fever than the endline (56.1%), and this difference was statistically significant at the 0.05 level. Bivariate analysis on practicing prompt care seeking by exposure found that levels of exposure were significantly correlated with prompt care seeking. Miners who had a fever in the past 12 months but had not been exposed to the VMT or LMBP components of the intervention reported lower levels of prompt care seeking (31.8%) in comparison to miners who reported being to either one of the two components (45.1%) and this difference was statistically significant at the 0.05 level. The highest levels of prompt care seeking (52.9%) were reported by miners exposed to both the VMT and LMBP components (Figure 3).
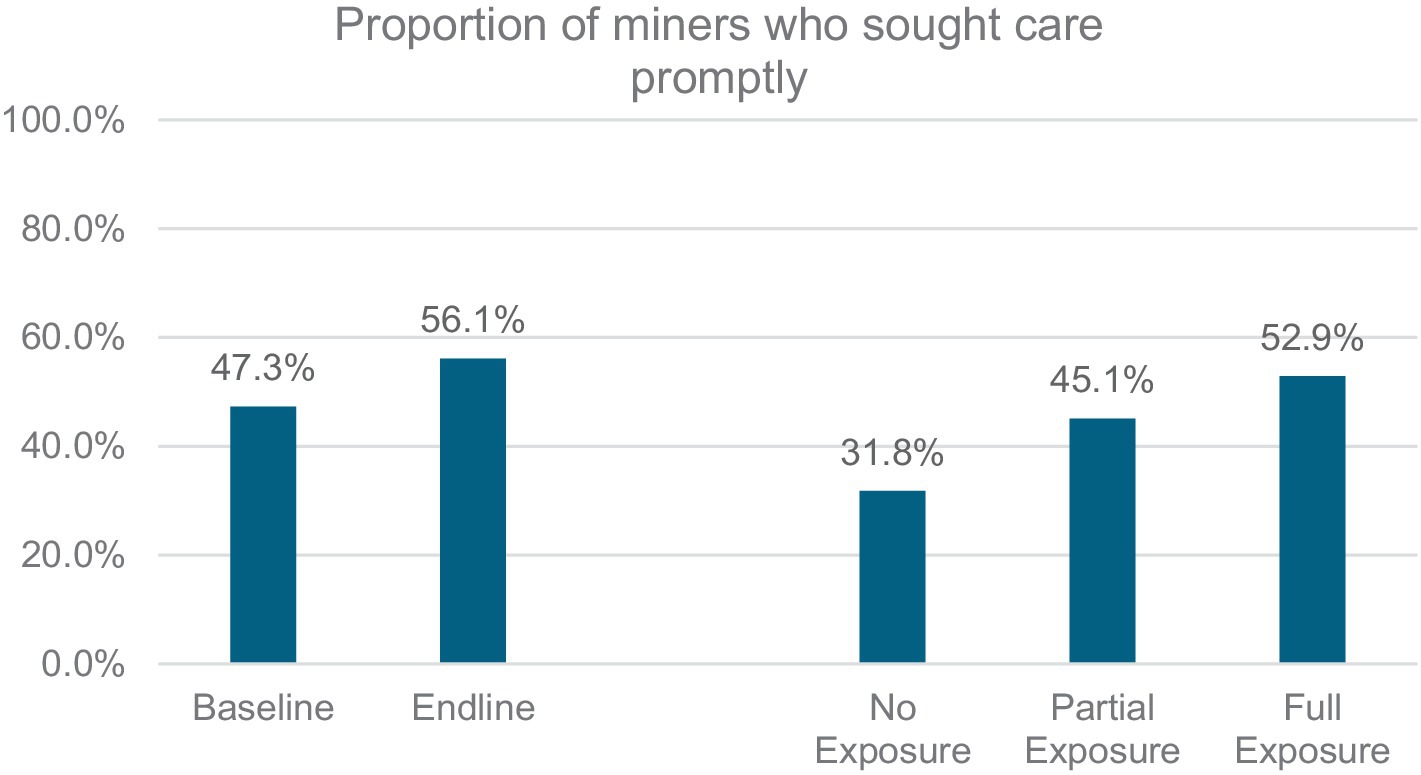
Figure 3. Prompt care seeking among miners over time and by exposure at endline.
The final set of bivariate analyses focused on the relationship between exposure and individual ideation elements (Table 4).
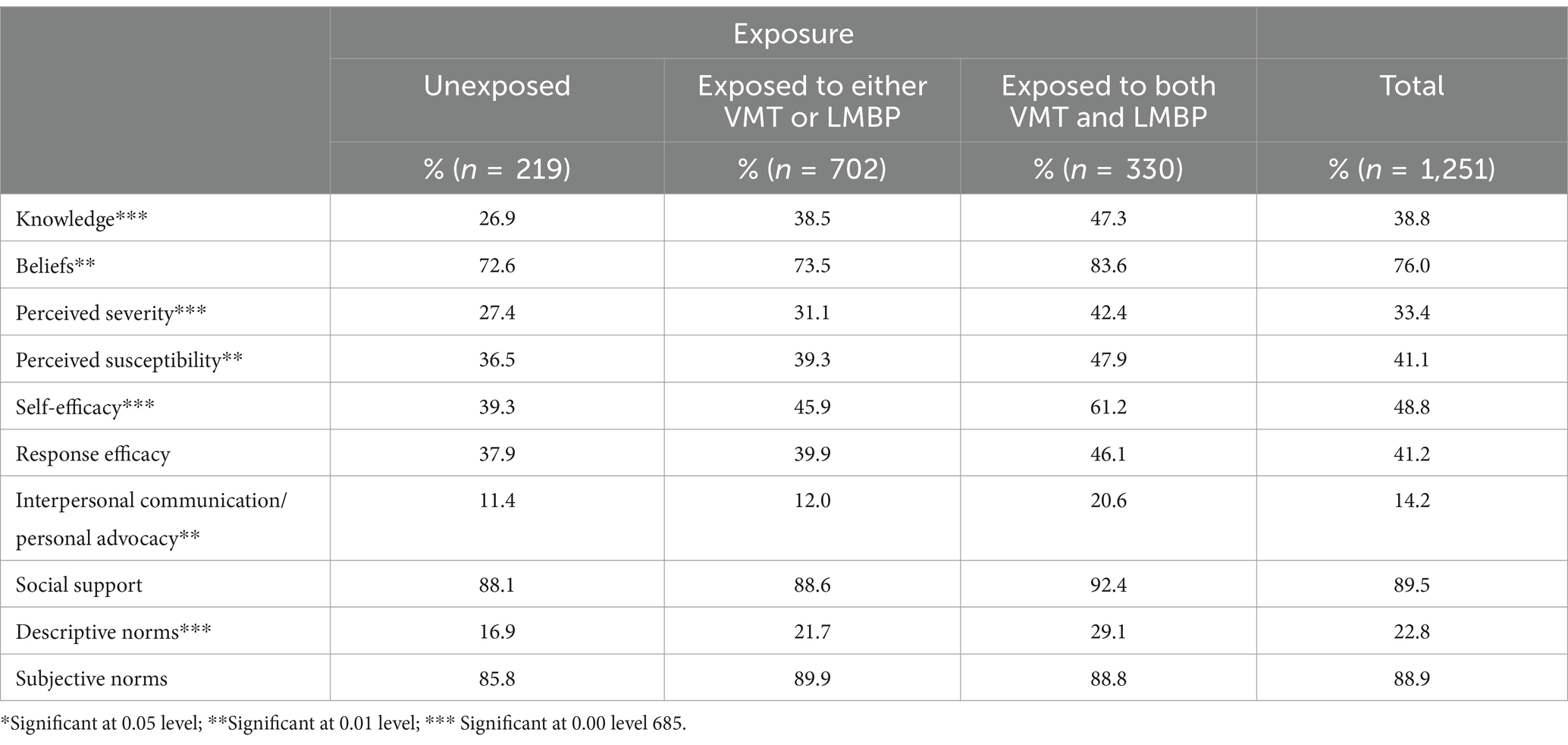
Table 4. Bivariate analysis of ideation factors based on levels of exposure at endline.
Bivariate analysis of individual ideation elements by exposure the endline shows significant relationships between the level of exposure and individual ideation elements: knowledge, beliefs, perceived severity, perceived susceptibility, interpersonal communication about malaria with others/personal advocacy, and descriptive norms. The lack of significant associations with social support and subjective norms could be a function of ceiling effects since 9 out of 10 miners indicated high social support and positive subjective norms.
Multivariate analysis
The multivariate analysis included logistic regressions for the binary variables and ordinal logistic regression for the three-level exposure variable. The tables below provide both unadjusted and adjusted odds ratios. The adjusted odds ratios control for all the background variables: region, age, gender, marital status, education, ethnicity, religion, how long the respondent has worked as a miner and if the respondent worked as a miner year-round.
Table 5 examines exposure as the independent variable. It measures the impact of exposure on the outcome of prompt care seeking, followed by the odds of higher and more positive ideation among miners exposed to the combined VMT and LMBP intervention.
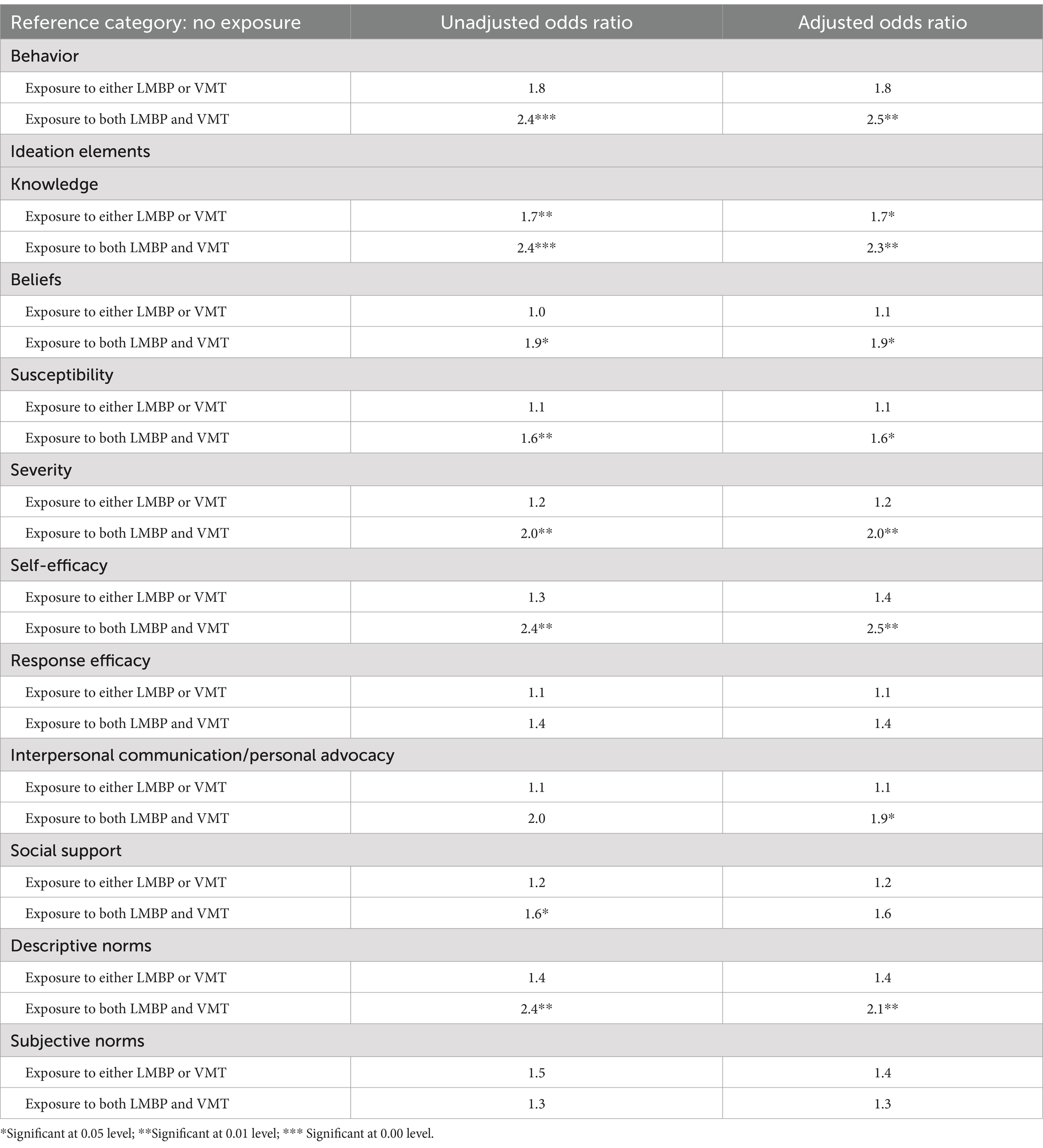
Table 5. Impact of exposure on behavior and ideation elements.
Miners exposed to either LMBP or VMT had higher but not significant odds of seeking care promptly compared to miners who were not exposed. However, comparing non-exposed miners with miners who reported exposure to LMBP and VMT, they were 2.5 times more likely to report prompt care seeking after adjusting for all background variables. Miners with any level of exposure displayed significantly high levels of knowledge about the causes and ways to protect themselves from malaria. Miners with exposure to either LMBP or VMT were 1.7 times more likely to display correct knowledge, while those with full exposure to both LMBP and VMT were 2.5 times more likely to report correct knowledge about what causes malaria, its signs and symptoms, and ways of preventing malaria. Exposure to both LMBP and VMT was associated with significantly higher odds of several ideation components, including attitudes (AOR; 1.9); susceptibility (AOR: 1.6); severity (AOR: 2.0); self-efficacy (AOR: 2.5) and descriptive norms (AOR: 2.1). Respondents reporting the highest level of exposure were also likely to have significantly higher odds of engaging in communication about malaria with others or personal advocacy (AOR: 1.9). The only ideation factors that were not significantly associated with exposure were response efficacy and subjective norms.
Table 6 below examines the odds of prompt care seeking based on high or positive ideational elements and presents ideation data associated with both the baseline and endline results.
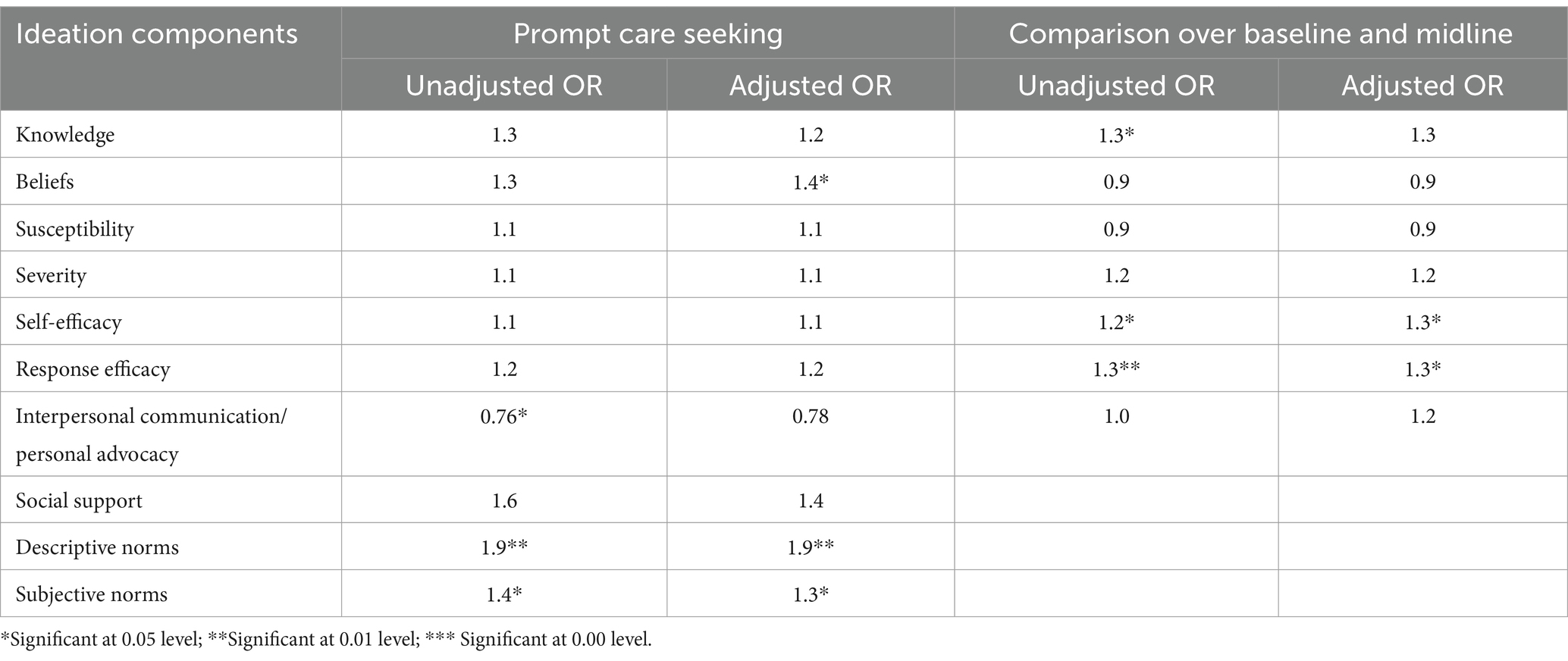
Table 6. Impact of ideation on prompt care seeking and changes in ideation over time.
Specific ideational elements impacted prompt care seeking. Both descriptive norms (what respondents believe others do) and subjective norms, i.e., respondents’ beliefs that they will not be made fun of if they test before treatment, were significantly associated with higher odds of prompt care seeking. These results remain significant after adjusting for background variables. Beliefs were a significant predictor of prompt care-seeking in the adjusted model. Interestingly, communication about malaria with others and personal advocacy is inversely related to prompt care seeking, indicating that miners who reported having talked with their friends and family members about malaria had significantly lower odds of prompt care seeking. However, this association was not significant in the adjusted model.
The simple logistic regression model comparing baseline and endline results shows that miners had significantly higher levels of knowledge, self-efficacy (confidence that they could get tested), and response efficacy (perceptions about the reliability and accuracy of the blood test). After adjusting for background variables, knowledge was no longer significant, but the self-efficacy and response-efficacy of miners at the endline continued to show higher odds (AORs 1.3) for both measures of efficacy.
Discussion
This manuscript has two aims. First, it attempts to assess pre- and post-intervention levels of prompt care seeking among gold miners in Regions 7 and 8 in Guyana. Second, exploring the direct and indirect influence of an integrated SBC intervention that combined community-based malaria case management through VMTs with a multi-channel SBC campaign to facilitate and promote prompt care-seeking. Combining SBC efforts with the VCS-NMP’s effort to establish an accessible service delivery system is especially vital for remote mining locations in Guyana where malaria is endemic. A carefully designed and executed SBC campaign filled gaps in both the supply and demand for malaria case detection and prompt treatment. Implementing public health interventions with complementary components has a much greater chance of success than interventions that only address one aspect (Panter-Brick et al., 2006; Pell et al., 2011). The SBC program was developed using an innovative participatory process based on human-centered design principles. While it is not possible to causally link the use of the HCD process with SBC, there is literature from Guyana that shows that engaging and involving multiple stakeholders in program design is a best practice in the field of SBC (Holliman et al., 2022). The results presented above highlight the transient nature of mining, as evidenced by the difference in background characteristics of miners between baseline and endline. Creating and promoting accessible health systems is vital to meet these populations’ needs (IOM, 2017; Tam et al., 2021).
The use of stable residents from these locations as VMTs to the extent possible aimed to improve continuity in service availability. However, simply creating a VMT system is not enough to promote the uptake of protective behaviors on the part of the miners. Implementing a multi-channel intervention designed to elevate the availability of free malaria testing and treatment at specific locations helped popularize the use of VMT services. The campaign did not just serve to promote the availability of VMTs, it also involved the creation of specific mass media, social media, print, and interpersonal communication and counseling materials to directly and indirectly influence miner behavior based on the ideation framework. The use of a proven conceptual framework, the ideation model, for the design and implementation ensured that the campaign specifically targeted key ideational elements that specifically addressed audience needs. For example, formative research found that malaria was considered commonplace. Therefore, many of the LMBP materials focused on risk perceptions. The name of the campaign (Lil Mosquito, Big Problem) was specifically meant to address risk perceptions.
A review of the individual ideation variables yields low levels of knowledge and descriptive norms. The reason for this could be the stringent measures used to create these variables. Overall, respondents displayed high levels of knowledge. However, several respondents simultaneously believed malaria could be caused by other sources than mosquitos. It is possible to hypothesize that high levels of correct knowledge are attenuated by myths and misperceptions around malaria transmission. The questions around descriptive norms required respondents to report that others in their community were likely to perform all four behaviors: LLIN use, prompt care seeking, testing, and adherence. While many respondents reported that some of these behaviors were normative in their community, the proportion who perceived all these behaviors as normative was low. For example, while more than half of the respondents reported their positive perception of bed net use, less than 30% of respondents felt that others in their community adhered to treatment.
Evaluation plays a key role in documenting program effectiveness; baseline, and endline surveys allowed for measuring assess pre- and post-intervention levels of prompt care seeking among gold miners in Guyana. The results clearly show positive trends in care-seeking, with endline respondents reporting higher levels of prompt care seeking compared to the baseline. Logistic regressions were used to explore the direct and indirect influence of the combined VMT and LMBP intervention. These results highlight several important points. The value of combined interventions is evident from the positive ideation and behaviors among miners exposed to both the VMT and LMBP interventions. Exposure to both the VMT program and the LMBP campaign was directly significantly associated with prompt care-seeking. The indirect influence of the intervention on behaviors through the ideation model is also important to consider. The logistic regressions examining the relation between the level of exposure and ideation found that higher levels of exposure were significantly associated with higher levels of several ideation variables. The only ideational factors that did not have significantly higher odds of positive ideation associated with exposure were response efficacy and subjective norms. The proportion of respondents exposed to the VMT and LMBP also showed higher response efficacy levels. Similarly, there was a significant association in the proportion of miners reporting higher levels of response efficacy between baseline and endline. The lack of a significant relationship between prompt care seeing and response efficacy could be a function of the fact that LMBP messages were not specific to the two measures of response efficacy: “The results of the tests given by volunteer testers are always accurate” and “A blood test for malaria is the only way to know if someone really has malaria.” The messages focused on the accuracy of the test but did not necessarily link it with testing by VMTs, and the messaging around the importance of blood tests was tied to learning about what type of malaria a person has but not for the diagnosis of malaria. As far as subjective norms are concerned, the lack of a statistically significant association between exposure and subjective norms could be attributed to the fact that the measure of subjective norms asked respondents if they felt that people in the camp would make fun of them for getting tested before treatment. Most of the respondents felt that this statement was not the norm. The more accurate statement, as asked in the global Malaria Behavior Survey (MBS), a research tool used to gather data on behaviors, attitudes, and practices related to malaria prevention, diagnosis, and treatment, asks if respondents will be criticized for getting tested (Malaria Behavior Survey, n.d.). Further, the LMBP campaign did not include specific messages regarding subjective norms.
The influence of specific ideation elements on prompt care-seeking, including personal beliefs, descriptive norms, and subjective norms, is important to remember as it shows the relationship between audience attitudes and perceptions about what others are doing or how others would react to prompt care-seeking efforts. These results indicate the key role of perceptions in prompt care-seeking. The programmatic implication is for interventions to consider addressing attitudes and perceptions rather than simply attempting to increase knowledge. These results also support recent theorizing among SBC practitioners and researchers, who have proposed the importance of addressing norms around harmful practices. The reasons for not practicing a behavior are not driven by individual concerns of susceptibility and severity or a lack of confidence in one’s ability to seek care promptly but more directly associated with the desire to fit in is based on perceptions of what their peer networks are doing. Messaging designed to influence descriptive norms, specifically that others are promptly seeking care for a fever, getting tested, and adhering to the treatment regimen are likely to resonate with audiences.
One puzzling finding reported in the results associated with communication about malaria with others and personal advocacy is that individuals engaging in higher levels of communication about malaria with others or personal advocacy are significantly less likely to get tested promptly. Intuitively, one would assume that communication about malaria with others on a topic would be associated with higher levels of practice. One possible explanation could be that the content of the communication matters. In this case, we know that these respondents discussed prompt care-seeking with their friends and family. However, we do not know what specifically was discussed. We can hypothesize that the discussion convinced miners not to seek testing rather than encouraging them to get tested. The programmatic implications of this finding are that the role of secondary and tertiary audiences is important in promoting prompt care-seeking. Messages encouraging individuals to discuss and advise people in their social networks to practice prompt care-seeking could be a win-win as these discussions could also help shape positive norms. From a research perspective, this finding reminds us to probe for the content of interpersonal communication about malaria with others; the question around discussion needs to be contextualized within a conceptual framework that examines the discussion and focuses on the content of the discussion.
Limitations
As is the case with any research, this study has several limitations. For example, this study was conducted in specific regions in Guyana, which may limit the generalizability of the findings to other populations or geographic areas. The population surveyed changed considerably from endline to baseline. The primary reason for this shift is economic hardships, further fueled by the global COVID-19 pandemic, which could confound the interpretations of the intervention’s effectiveness. Gold miners in Guyana tend to be mobile, moving in and out of specific mining locations in large numbers. The shifting demographics of the mining population impact their perceptions of health and experiences with malaria. This limitation may be one reason for relatively small shifts in specific ideational factors between baseline and endline. As those exposed to the SBC program leave the area and new miners unexposed to the SBC program take their place, it is hard to expect ideation to change over time.
This study also has methodological limitations. This baseline and endline design help measure change over time. However, the cross-sectional nature of the sampling and the fact that the background characteristics of the baseline and endline respondents were different is a significant limitation. Future research could consider including a control or comparison group in the study design. While reliance on a tried and tested model—ideation—is a strength, the limitation is that the study relied on self-reported data to measure ideational variables, which introduces the risk of social desirability and recall bias. The research did not include questions about some ideational variables. For example, there was no measure of emotional response. Other elements, such as communication about malaria with others and personal advocacy, need to be measured more comprehensively. Additionally, the ideation model focuses on psychosocial determinants, but it does not account for political or economic factors that may impact malaria prevention or reduction efforts.
A third limitation is that the primary outcome variable was care-seeking behavior, which does not allow for insights into individual actions such as wearing protective clothing, using insecticide-treated bed nets, applying mosquito repellent, ensuring proper ventilation and screening and avoiding peak malaria activity time nor does it emphasize evidence of environmental management to reduce or eliminate mosquito breeding habitats, such as draining or filling in areas where water accumulates, ensuring proper drainage, proper disposal of waste. The focus on care-seeking needs to address the issue of treatment adherence, which is crucial to the success of malaria elimination efforts.
A fourth limitation may be the use of logistic regression analysis, which was selected to improve understandability and dissemination of results among a broad spectrum of readers. Additional analysis using robust structural equation modeling to examine direct and indirect effects of exposure and ideation on prompt care seeking while controlling for the baseline results could be beneficial. A fifth study limitation is that not all questions relevant to examining the impact of ideation on prompt care-seeking behaviors were included in the baseline, curtailing our ability to compare all relevant ideation elements between baseline and endline. A final limitation is the need for more information on the long-term sustainability of the intervention.
Conclusion
Despite the limitations noted above, this study proves that theory-driven programs systematically designed and implemented through stakeholder involvement and engagement set the stage for future success. Finally, including evaluation as part of the design process and including a baseline allows for recommendations that are relevant not just for prompt care-seeking for malaria in Guyana but also applicable to similar settings, for example, other mining communities in Latin America and the Caribbean (LAC) region and beyond that to other global health issues being tackled by social and behavior change interventions.
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
The studies involving humans were approved by Johns Hopkins University Bloomberg School of Public Health. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
Author contributions
SS: Formal analysis, Writing – original draft, Writing – review & editing. OB: Writing – original draft. JO: Conceptualization, Project administration, Resources, Writing – review & editing. SW: Conceptualization, Project administration, Supervision, Writing – review & editing. GH: Writing – review & editing. TD: Writing – review & editing. MH: Writing – review & editing. KJ: Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This work is made possible by the support of the American people through the United States Agency for International Development under the Breakthrough ACTION Cooperative Agreement #AID-OAA-A-17-00017.
Acknowledgments
The authors would like to thank Dr. Reza Niles-Robin and Dr. Olivia Valz at the Guyana Ministry of Health Vector Control Services for their close collaboration with the Breakthrough ACTION Guyana project, as well as Erika Venegas and Andrew Tompsett at the United States Agency for International Development for their technical support and comments on earlier drafts of this manuscript.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Abdallah, R., Louzada, J., Carlson, C., Ljolje, D., Udhayakumar, V., Oliveira-Ferreira, J., et al. (2022). Cross-border malaria in the triple border region between Brazil, Venezuela, and Guyana. Sci. Rep. 12:1200. doi: 10.1038/s41598-022-05205-y
Awantang, G. N., Babalola, S. O., Koenker, H., Fox, K. A., Toso, M., and Lewicky, N. (2018). Malaria-related ideational factors, and other correlates associated with intermittent preventive treatment among pregnant women in Madagascar. Malar. J. 17:176. doi: 10.1186/s12936-018-2308-3
Awantang, G., Babalola, S., Koenker, H., Fox, K., Toso, M., Lewicky, N., et al. (2018). Correlates of social behavior change communication on care-seeking behaviors for children with fever: an analysis of malaria household survey data from Liberia. Malar. J. 17:105. doi: 10.1186/s12936-018-2249-x
Babalola, S., Adedokun, S. T., McCartney-Melstad, A., Okoh, M., Asa, S., Tweedie, I., et al. (2018). Factors associated with caregivers’ consistency of use of bed nets in Nigeria: a multilevel multinomial analysis of survey data. Malar. J. 17:280. doi: 10.1186/s12936-018-2427-x
Babalola, S., and Kincaid, D. L. (2009). New methods for estimating the impact of health communication programs. Commun. Methods Meas. 3, 61–83. doi: 10.1080/19312450902809706
Bazzano, A. N., Martin, J., Hicks, E., Faughnan, M., and Murphy, L. (2017). Human-centred design in global health: a scoping review of applications and contexts. PLoS One 12:e0186744. doi: 10.1371/journal.pone.0186744
Breakthrough ACTION (n.d.). There is gold in social and behavior change. Human-centered design research around malaria care-seeking behaviors in gold mining communities of Guyana. Available at: https://express.adobe.com/page/hQqC9bmmsQ0lr/
Breakthrough ACTION (n.d.). Mining for Social and Behavior change. Human-centered design research around malaria care-seeking behaviors in gold mining communities of Guyana. Available at: https://express.adobe.com/page/Tz8iFCbSYiyFu/
Breakthrough ACTION Guyana (2019). Insights Report Using human-centered design to strengthen Guyana’s malaria testing and treatment adherence program. Available at: https://thecompassforsbc.org/wp-content/uploads/BA-Guyana-Insights-Report-2019MAY3-2.pdf
Casella, A., Monroe, A., Toso, M., Hunter, G., Underwood, C., Pillai, R., et al. (2024). Understanding psychosocial determinants of malaria behaviors in low-transmission settings: a scoping review. Malar. J. 23:15. doi: 10.1186/s12936-023-04831-9
De Salazar, P. M., Cox, H., Imhoff, H., Alexandre, J. S. F., and Buckee, C. O. (2021). The association between gold mining and malaria in Guyana: a statistical inference and time-series analysis. Lancet. Planet. Health 5, e731–e738. doi: 10.1016/S2542-5196(21)00203-5
Design for Health. Advancing the appropriate use of Design in Global Health contexts [Internet]. (n.d.). Available at: https://www.designforhealth.org/ (Accessed February 8, 2019).
do, M., Babalola, S., Awantang, G., Toso, M., Lewicky, N., and Tompsett, A. (2018). Associations between malaria-related ideational factors and care-seeking behavior for fever among children under five in Mali, Nigeria, and Madagascar. PLoS One 13:e0191079. doi: 10.1371/journal.pone.0191079
Earle, J. (2011). Warming Guyana coast risks malaria resurgence. Thomson Reuters Foundation. Available at: https://news.trust.org/item/20110907101200-1o7sp
Holliman, R., Marino, A., Grand, A., Berardi, A., Mistry, J., Jafferally, D., et al. (2022). A case study from Guyana of adapting engaged research design to promote ‘fairness in knowing’. Res. All 6, 1–17. doi: 10.14324/RFA.06.1.12
IOM (2017). ‘Migration and migrants: A global overview’, in IOM (2017) world migration report 2018. Geneva: IOM.
Kincaid, D. L. (2000). Mass media, ideation, and behavior: a longitudinal analysis of contraceptive change in the Philippines. Commun. Res. 27, 723–763. doi: 10.1177/009365000027006003
Malaria Behavior Survey. (n.d.). Toolkit. Survey Questionnaire. Available at: https://malariabehaviorsurvey.org/toolkit/
Malaria Elimination Initiative. (2023). Accelerating malaria elimination in the Guyana shield. Shrinking the Malaria Map. Available at: https://shrinkingthemalariamap.org/accelerating-malaria-elimination-in-the-guyana-shield
Ministry of Public Health of Guyana (2015). Malaria treatment guideline for health facilities in Guyana. National Malaria National Malaria Program and Pan-American health organization. Available at: https://fi-admin.bvsalud.org
Monroe, A., Olapeju, B., Moore, S., Hunter, G., Merritt, A. P., Okumu, F., et al. (2021). Improving malaria control by understanding human behavior. Bull. World Health Organ. 99, 837–839. doi: 10.2471/BLT.20.285369
Olapeju, B., Adams, C., Hunter, G., Wilson, S., Simpson, J., Mitchum, L., et al. (2020). Malaria prevention and care seeking among gold miners in Guyana. PLoS One 15:e0244454. doi: 10.1371/journal.pone.0244454
Olapeju, B., Adams, C., Wilson, S., Simpson, J., Hunter, G. C., Davis, T., et al. (2022). Malaria care-seeking and treatment ideation among gold miners in Guyana. Malar. J. 21:29. doi: 10.1186/s12936-022-04045-5
Panter-Brick, C., Clarke, S. E., Lomas, H., Pinder, M., and Lindsay, S. W. (2006). Culturally compelling strategies for behavior change: a social ecology model and case study in malaria prevention. Soc. Sci. Med. 62, 2810–2825. doi: 10.1016/j.socscimed.2005.10.009
Pell, C., Straus, L., Andrew, E. V., Meñaca, A., and Pool, R. (2011). Social and cultural factors affecting uptake of interventions for malaria in pregnancy in Africa: a systematic review of the qualitative research. PLoS One 6:e22452. doi: 10.1371/journal.pone.0022452
Richardson, A. (2010). Using customer journey maps to improve customer experience. Harv. Bus. Rev. 15, 2–5.
Ricotta, E. E., Boulay, M., Ainslie, R., Babalola, S., Fotheringham, M., Koenker, H., et al. (2015). The use of mediation analysis to assess the effects of a behavior change communication strategy on bed net ideation and household universal coverage in Tanzania. Malar. J. 14:15. doi: 10.1186/s12936-014-0531-0
Roll Back Malaria Partnership. (2015). Action and investment to defeat malaria 2016–2030 (AIM) –for a malaria-free world. World Health Organization. Available at: https://www.rollbackmalaria.org/wp-content/uploads/2017/09/AIM-2016-2030-Executive-Summary.pdf
Smith, R. D., Keogh-Brown, M. R., Chico, R. M., Bretscher, M. T., Drakeley, C., and Jensen, H. T. (2020). Will more of the same achieve malaria elimination? Results from an integrated macroeconomic epidemiological demographic model. Am. J. Trop. Med. Hyg. 103, 1871–1882. doi: 10.4269/ajtmh.19-0472
Storey, J. D., Babalola, S. O., Ricotta, E. E., Fox, K. A., Toso, M., Lewicky, N., et al. (2018). Associations between ideational variables and bed net use in Madagascar, Mali, and Nigeria. BMC Public Health 18:484. doi: 10.1186/s12889-018-5372-2
Tam, G., Cowling, B. J., and Maude, R. J. (2021). Analyzing human population movement data for malaria control and elimination. Malar. J. 20, 1–9. doi: 10.1186/s12936-021-03828-6
USAID (2014). Communication Strategy for Malaria Control Co-operative Republic of Guyana 2014–2016. Available at: https://fi-admin.bvsalud.org
Vreden, S. (n.d.). Focus on malaria in the Guyana shield. National Malaria Board/RAVREDA Suriname. Available at: https://www3.paho.org/hq/dmdocuments/2011/13-Towards-malaria-control-Guyana-shield1.pdf
WHO (2017a). A framework for malaria elimination : World Health Organization. Available at: https://apps.who.int/iris/bitstream/handle/10665/254761/9789241511988-eng.pdf
WHO (2017b). Vector control for malaria prevention and control: A guide for malaria-endemic countries. Geneva: World Health Organization. Available at: https://www.who.int/publications/i/item/9789241512041
WHO. (2023). World Malaria Report. Available at. https://www.who.int/teams/global-malaria-programme/reports/world-malaria-report-2023
WHO. (2022). Tackling malaria in remote mining communities in Guyana. Available at: https://www.who.int/news-room/feature-stories/detail/tackling-malaria-in-remote-mining-communities-in-guyana.
Keywords: Guyana, malaria, prevention, treatment, social and behavior change, communication, human-centered design
Citation: Sood S, Beckles O, Orkis J, Wilson S, Hunter G, Davis T, Hussain M and James K (2024) Impact of a social and behavior change campaign and volunteer malaria tester program on malaria care seeking among gold miners in Guyana. Front. Commun. 9:1462943. doi: 10.3389/fcomm.2024.1462943
Edited by:
Sean J. Upshaw, The University of Texas at Austin, United StatesReviewed by:
Sílvio Manuel da Rocha Brito, Polytechnic Institute of Tomar (IPT), PortugalVenugopal Rao Miyyapuram, Thermo Fisher Scientific, United States
Copyright © 2024 Sood, Beckles, Orkis, Wilson, Hunter, Davis, Hussain and James. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Suruchi Sood, c3Nvb2QzQGpoLmVkdQ==