 Margaret Noyes Essex1
Margaret Noyes Essex1 Caroline E. Dietrich
Caroline E. Dietrich Lisen Arnheim-Dahlström
Lisen Arnheim-Dahlström- 1Pfizer Inc., New York, NY, United States
- 2Pfizer AB, Stockholm, Sweden
- 3War on Cancer, Stockholm, Sweden
- 4Division of Clinical Epidemiology, Department of Medicine, Solna, Karolinska Institutet, Stockholm, Sweden
Introduction: Effective communication is essential for building a successful patient–healthcare professional (HCP) relationship. Understanding a patient’s emotional context is key to building this relationship. However, communication barriers often hinder the development of these relationships. Strategies to communicate emotions in healthcare settings may address this issue. Emojis are small images that together form a universal language well-suited to describe emotions.
Methods: This three-phase feasibility study used quantitative and qualitative approaches to explore current opinions around the utility of emojis in expressing emotions during patient–HCP communications. In phase 1, members of the War on Cancer digital community participated in an online survey to determine their use of emojis in personal and healthcare communications. In phase 2, selected patient volunteers were interviewed to further understand the responses from the survey. In phase 3, invited HCPs were interviewed to evaluate their use of digital communications and emojis with patients, and insights on the findings from phases 1 and 2.
Results: In phase 1, 290 community members responded to the survey (16–84 years old; twenty-two countries). Of these, 70% (n = 197/280) reported common use of emojis in personal conversations, and 62% (n = 158/256) were optimistic about their use in HCP communications. All eight patients interviewed in phase 2 (30–70 years old; three countries) used emojis in personal communications but rarely in healthcare settings. They identified four situations where emojis could be useful in HCP communication: emotional preparation before a visit, follow-up after a visit, situations with a language barrier, and to replace numeric scales when expressing strength of emotion. All five of the HCPs interviewed in phase 3 (30–45 years old; two countries) communicated digitally with patients through electronic medical records or other platforms, but none had used emojis with patients. HCPs agreed with the four scenarios identified by patients in phase 2, further suggesting that emojis may be helpful for patients with poor literacy or difficulty expressing emotions.
Conclusion: In this study, patients and HCPs agreed that emojis could potentially enhance patient–HCP communication by facilitating emotional expression. Further research is required to evaluate the practicalities and benefits of integrating emojis into healthcare communications.
1 Introduction
Effective communication is essential in achieving patient-centered care, which could positively impact clinical outcomes and patient satisfaction (King and Hoppe, 2013; Robinson et al., 2008). Understanding a patient’s emotional context is vital for building a successful patient–healthcare professional (HCP) relationship (Hashim, 2017; Yedidia, 2007). However, communication barriers often impede the development of these relationships and hinder the ability of HCPs to provide optimal care. Utilization of alternative strategies to communicate emotion in clinical settings may address this issue.
Emojis are small images that together form a universal language well-suited to describe emotions and have the potential to overcome patient–HCP communication barriers (Bai et al., 2019; Lu et al., 2016). Emojis evolved from emoticons (“emotional icons”), which consist of alphanumeric characters used to represent various expressions (e.g., a smile [:-)]) and gestures (e.g., a “wink” [;)]) (Li and Yang, 2018; Ptaszynski et al., 2012). Emojis are now considered their own visual language, with >3,600 emojis in the Unicode Standard version 15.0 depicting various emotions and topics (e.g., food, culture, activities, objects, and health) (Unicode, 1991-2022; The Unicode Consortium, 1999-2022). These emojis are relatively consistent across different geographic regions and digital platforms, offering accessibility and familiarity to users in both personal and professional settings (Lai et al., 2021).
Previous research has explored the potential utility of emojis in patient–HCP communications and investigated the value of emojis in the assessment of mood and emotion, pain, mental health, health awareness, and adherence to treatment (Davies et al., 2022; Franco and Fugate, 2020; He et al., 2022; Langdon et al., 2021; Lotfinejad et al., 2020; Marengo et al., 2019; Pourmand et al., 2020; Setty et al., 2019; Szeto et al., 2022; Van Dam et al., 2019; Bai et al., 2019; Nante, 2018). However, only a few studies have evaluated the current use of emojis in healthcare settings more generally and explored the willingness of patients and HCPs to integrate emojis into their healthcare communications. This three-phase feasibility study assessed community (phase 1), patient (phase 2), and HCP (phase 3) opinions around the utility of emojis in facilitating patient–HCP communication using both quantitative and qualitative approaches.
2 Materials and methods
2.1 Phase 1: community opinion survey
A cross-sectional survey was distributed once through the “War on Cancer” (WOC) mobile phone app and remained open for 1 month. WOC is a digital community that supports and connects people affected by cancer. Members of the community are ≥16 years old, and included patients with cancer who were undergoing treatment, cancer survivors, friends and family of people with cancer, and those who registered as “here to learn.” The survey respondents consisted of registered members of the app. Members received an invitation to participate in the study through push and in-app notifications on their mobile phones (Supplementary Figure 1). In the app, potential respondents were able to read a description of the study and provide informed consent. Access to the 26-question survey (Supplementary Table 1) was granted once informed consent had been provided. Participation in the survey was voluntary and consent could be withdrawn at any time, even after survey completion. The questions were developed to address the following key topics: emojis used by patients to describe and express emotions, emojis patients thought were missing that could be used to effectively express their emotions, and the similarities or differences between emojis used by patients in personal conversations (e.g., with friends or family) and in healthcare settings.
The personal data of survey respondents were de-identified. Statistical analyses were done using Stata version 17 (Stata Corp, College Station, Texas, United States). Descriptive analyses were presented on an aggregated level using frequency tables and bar charts.
2.2 Phase 2: qualitative interviews with patients
Qualitative patient interviews were conducted to gain a deeper understanding of the survey findings. Interview patients were recruited through the WOC app and had to be aged ≥16 years, a patient with any diagnosis, and in contact with HCPs. They were selected through convenience sampling and received an email to which they could respond by accepting informed consent. Interviews were conducted individually through the Zoom videoconferencing platform for 30–60 min and were recorded for transcription purposes, after which the files were deleted. Patients were asked six open and three closed questions to determine their current use of emojis in text-based communications, situations where emojis might and might not help them express themselves to HCPs, and emotions represented by different emojis (Supplementary Table 2). The personal data of patients were pseudonymized.
2.3 Phase 3: qualitative interviews with HCPs
Qualitative HCP interviews were conducted to determine their willingness to use emojis when communicating with patients. HCPs in the WOC community were selected by convenience sampling and invited to participate in the study. Informed consent was requested through email. HCPs were interviewed individually for 30–45 min through Zoom or face-to-face, and interviews were recorded for transcription purposes, after which the files were deleted. HCPs were asked six open-ended questions to assess their current use of digital communications and emojis with patients, insights on the findings from phase 2, and overall thoughts on using emojis in patient communications (Supplementary Table 3). The personal data of HCPs were pseudonymized.
3 Results
3.1 Phase 1: community opinion survey
Altogether, 290 of 11,750 registered members (2%) of the WOC app from 22 different countries participated in the survey between September 29 and October 29, 2021. The respondents were aged between 16 and 84 years at the time of the survey (74% aged 35–64 years), and most were patients diagnosed with cancer (81%), female (73%), and from the United Kingdom (38%), Sweden (26%), or the United States (18%) (Table 1; Supplementary Table 4).
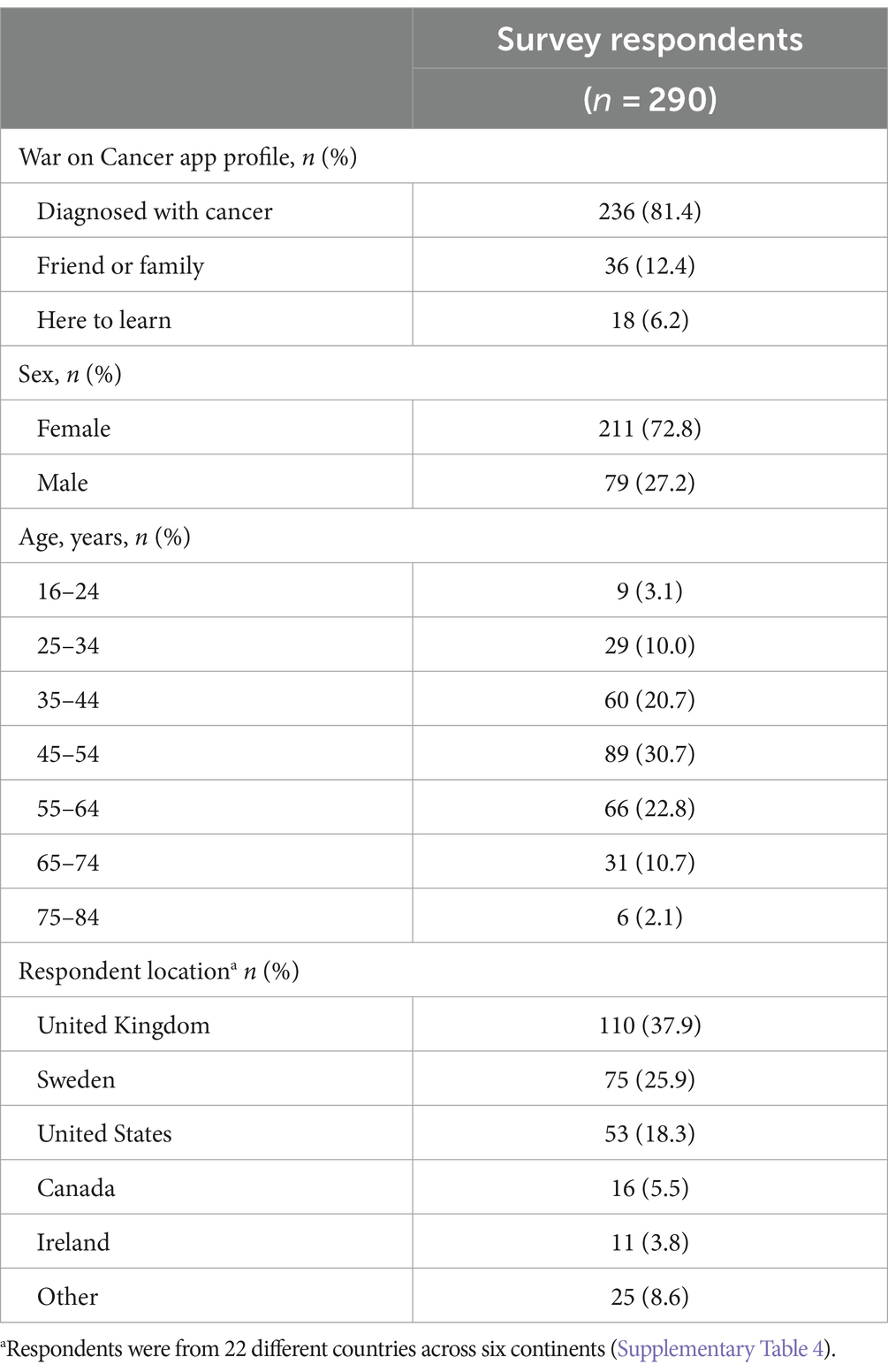
Table 1. Demographics of survey respondents in phase 1.
In personal communications (conversations with friends or family), most respondents (197/280; 70%) always or often used emojis to express emotions. When expressing emotions in text, 37% (101/271) of respondents had no preference between the use of emojis or words (Figure 1). Respondents (106/266; 40%) also considered emojis to be very or extremely useful in expressing emotions related to their mental health, and 43% (119/275) often or always used them to describe their mental health to friends and family.
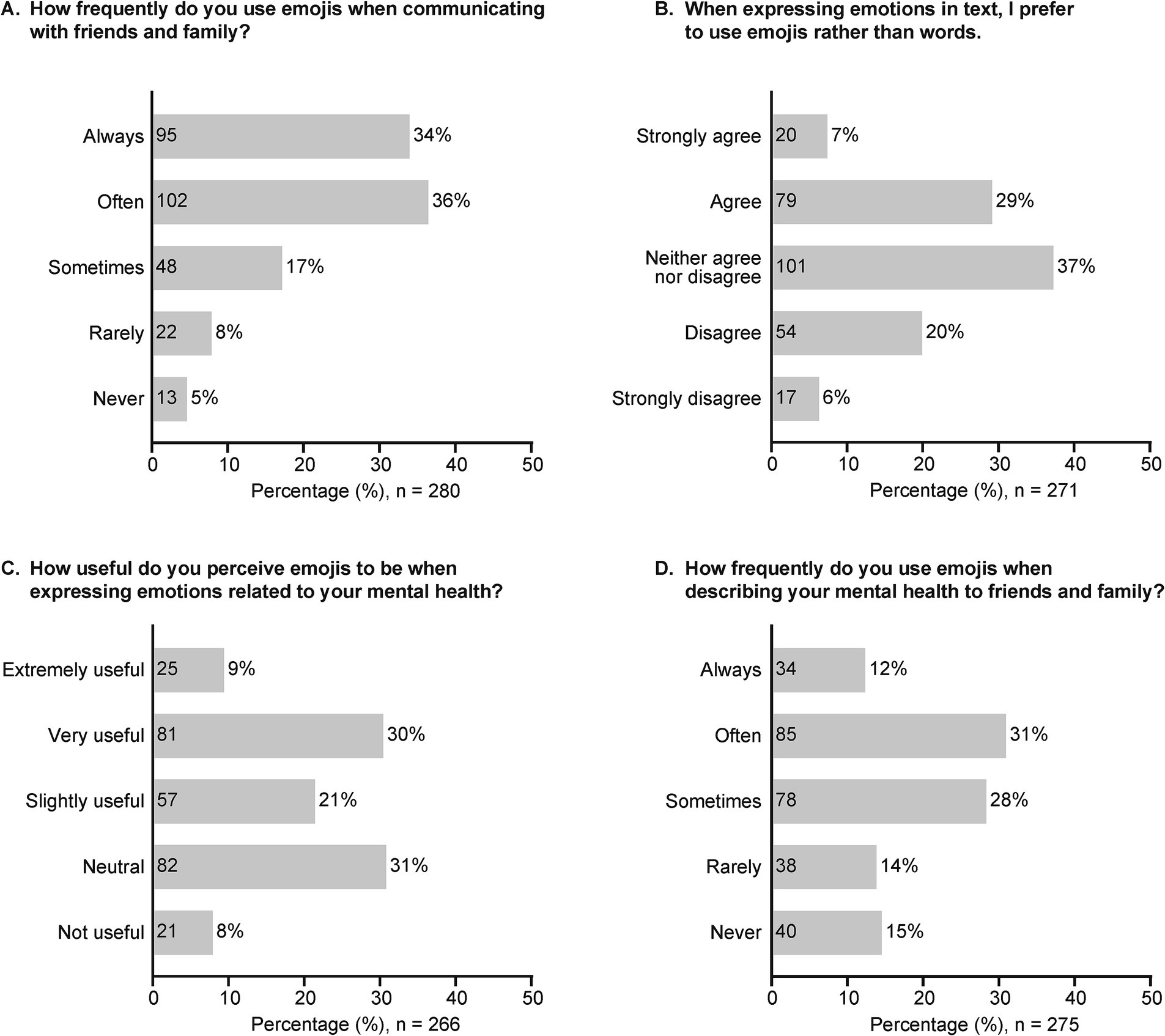
Figure 1. Survey responses to questions related to the use of emojis in text-based personal communications. (A) How frequently do you use emojis when communicating with friends and family? (B) When expressing emotions in text, I prefer to use emojis rather than words. (C) How useful you do you perceive emojis to be when expressing emotions related to your mental health? (D) How frequently do you use emojis when describing your mental health to friends and family? The value within each bar indicates the number of responses.
In healthcare settings, 76% (197/258) of respondents rarely or never used text-based communications with HCPs, but 62% (158/256) thought emojis could be or have been useful to express their feelings (Figure 2). Many respondents (97/262; 37%) thought that emojis could help improve their communication with HCPs, whereas 28% (73/262) disagreed and 35% (92/262) were undecided. When asked to choose emojis on their mobile phones to represent specific emotions (e.g., happiness, anger, and pain), most respondents chose similar emojis to depict each emotion (Figure 3; Supplementary Figures 2, 3).
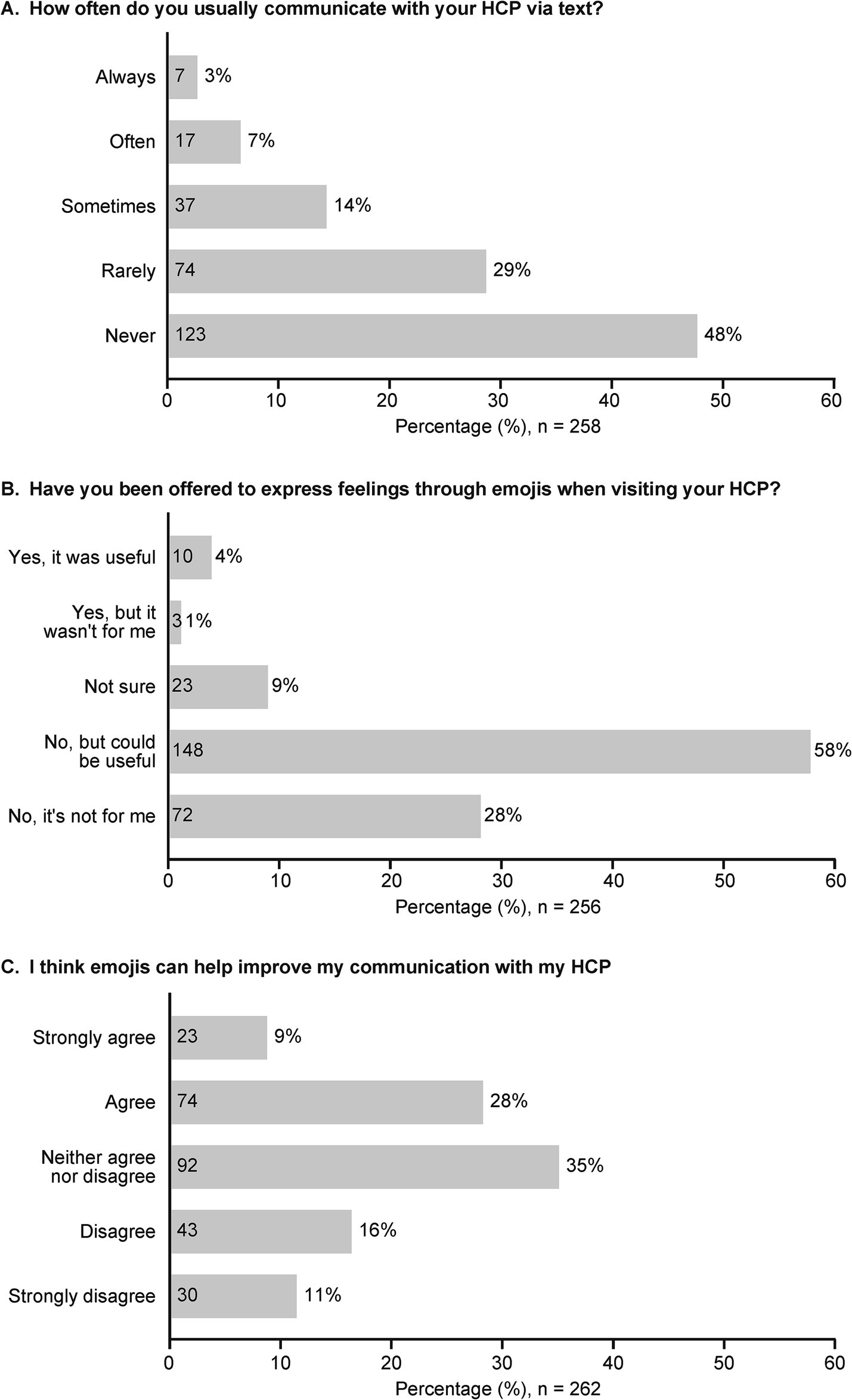
Figure 2. Survey responses to questions related to the use of emojis in text-based communication with HCPs. (A) How often do you usually communicate with your HCP via text? (B) Have you been offered to express feelings through emojis when visiting your HCP? (C) I think emojis can help improve my communication with my HCP. The value within each bar indicates the number of responses. HCP, healthcare professional.
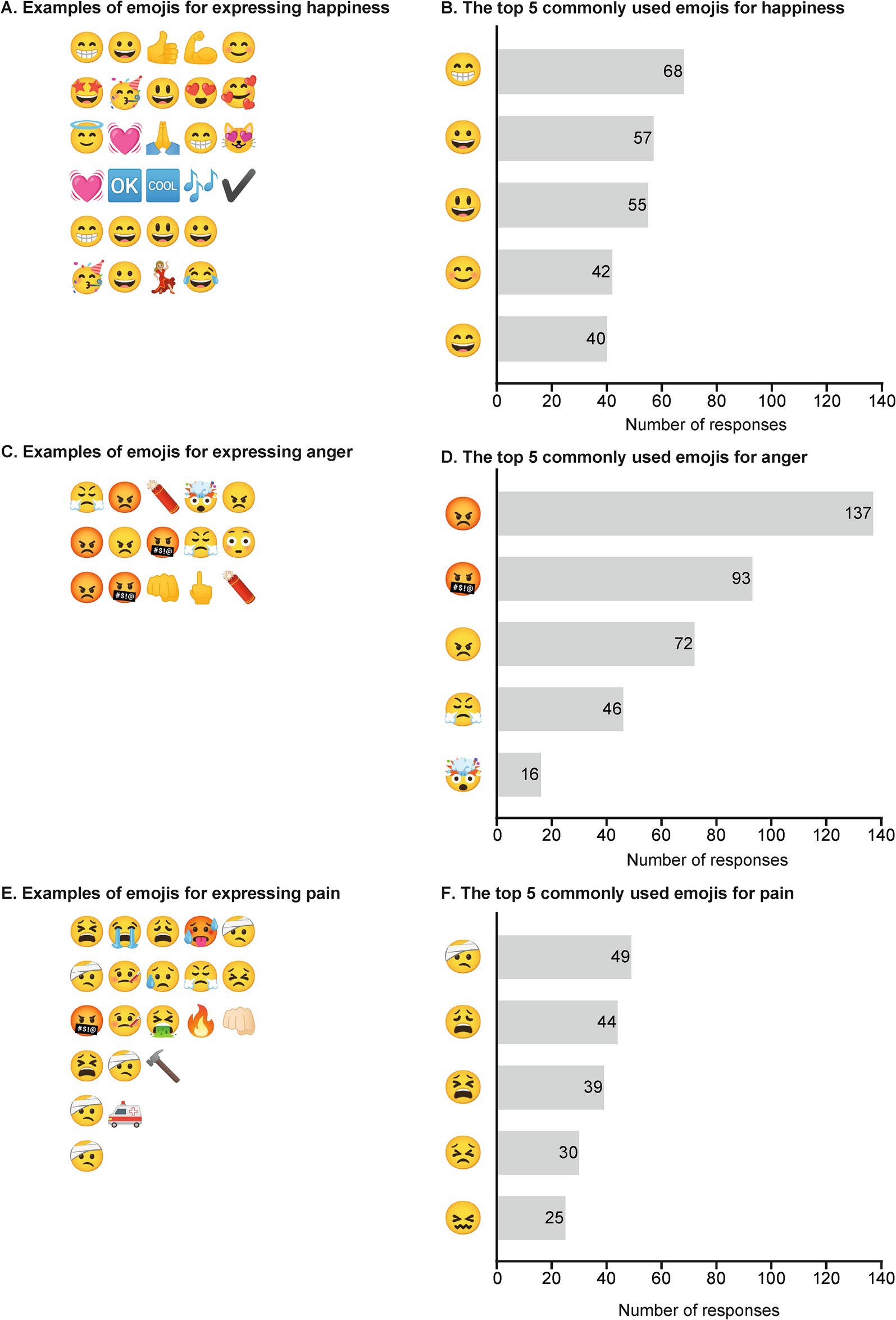
Figure 3. Examples of emojis and commonly used emojis to express (A,B) happiness, (C,D) anger, and (E,F) pain. Respondents who disagreed with the use of emojis in communicating with their HCPs did not answer the emotion-specific emoji questions. The value within each bar indicates the number of responses. Respondents could choose ≤5 emojis; hence the number of responses can be more than the number of respondents (N = 290). HCP, healthcare professional.
3.2 Phase 2: qualitative interviews with patients
Eight patients (5 female, 3 male) were interviewed by Lisen Arnheim-Dahlström, PhD (Head of Research and Development, War on Cancer) or Caroline E. Dietrich, PhD (Lead Scientist, War on Cancer) between February and March 2022. Patients were aged 30–70 years and from Sweden (n = 5), the United States (n = 2), or the United Kingdom (n = 1). Patients used emojis in text-based communications but rarely used emojis to communicate with their HCPs. Patients had different views on when and how emojis should be used with HCPs but generally identified four situations where emojis could be most useful: (1) emotional preparation before a visit, (2) follow-up after a visit, (3) in situations with a language barrier, and (4) to replace numeric scales indicating the strength of emotion (Figure 4). However, they considered emojis less useful when expressing emotions in serious situations, as a substitute for face-to-face meetings, in interactions with HCPs that they know very well, and in conversations with HCPs that they barely know.
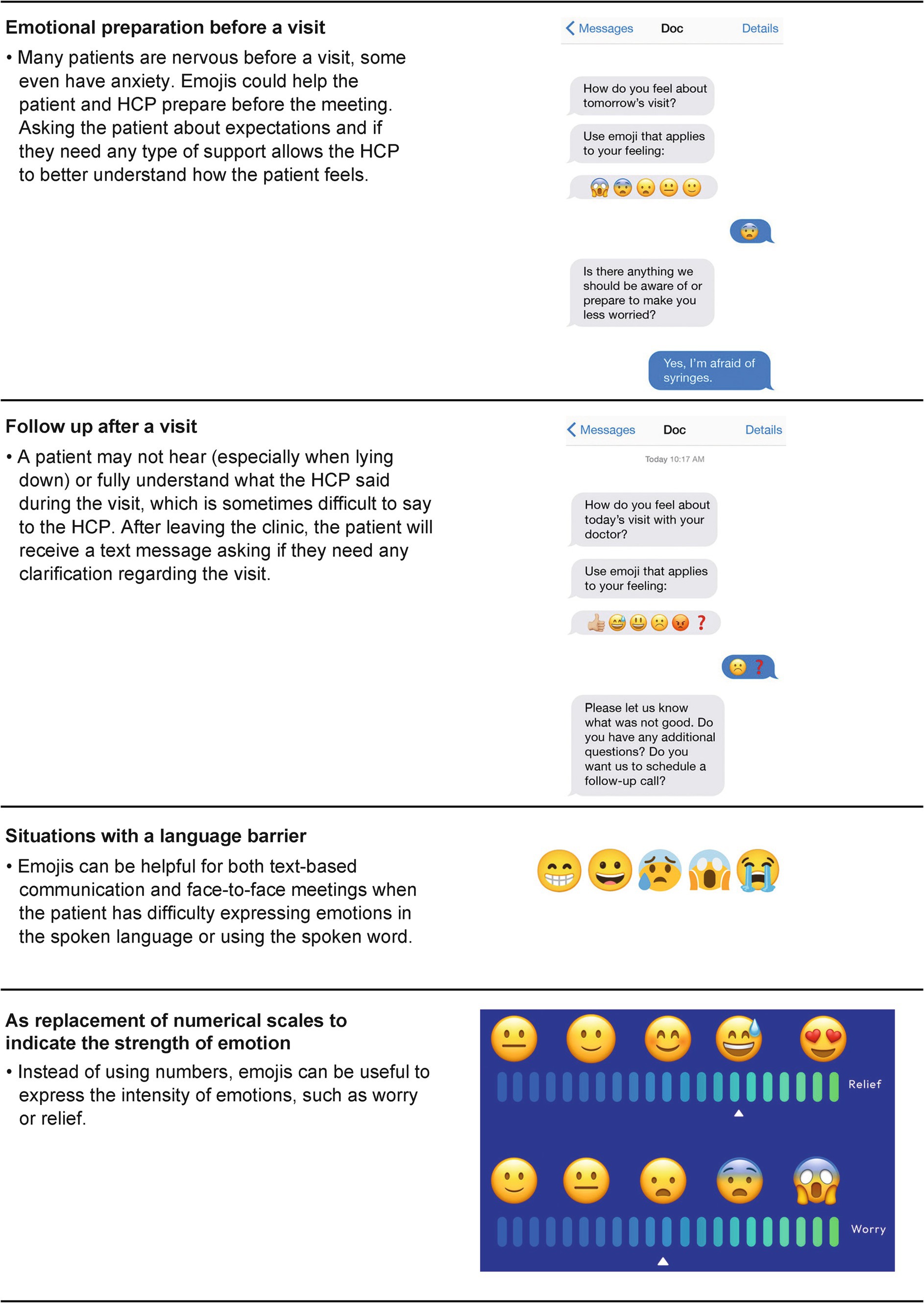
Figure 4. Four situations where emojis can be useful in patient–HCP communication. HCP, healthcare professional.
While patients interpreted emojis similarly, they had varying opinions on which emojis are suitable for use in a healthcare setting. When communicating with HCPs, most patients would primarily use the heart ( ) and “yellow” face (
) and “yellow” face ( ) emojis, but not the “devil” (
) emojis, but not the “devil” ( ) or “alcohol” (
) or “alcohol” ( ) emojis. Some of the patients thought there were no healthcare-adapted emojis and patients also noted that when using emojis for a specific emotion, the context needs to be clear.
) emojis. Some of the patients thought there were no healthcare-adapted emojis and patients also noted that when using emojis for a specific emotion, the context needs to be clear.
3.3 Phase 3: qualitative interviews with HCPs
Five HCPs were interviewed either through Zoom or face-to-face for 30–45 min by Lisen Arnheim-Dahlström between April and June 2022. HCPs were aged between 30 and 45 years (3 female, 2 male; 2 clinicians, 3 nurses) and were from the United States (n = 3) or Sweden (n = 2). All had communicated digitally with patients through electronic medical records (EMRs) or other digital platforms. Some EMR systems allow two-way communication (HCP and the patient can send and receive messages between each other), which is mostly used for filling in medical records and lab results and occasionally to check in with patients, but not to provide psychosocial support. Other EMR systems only allow one-way communication (HCP can only send messages to patients when filling in medical records) to preserve confidentiality. HCPs had also used other digital platforms (e.g., Zoom) to deliver care without text-based communication. They noticed that young people preferred text-based conversations and felt uncomfortable with digital meetings, but their parents were more open to it.
Although none of the HCPs had used emojis with patients directly, they were optimistic about incorporating emojis in patient–HCP communication. They thought that using emojis could benefit the patient in expressing themselves and would be an excellent way to enhance inclusivity. They noted that, as emotions are not routinely conveyed in written communication, incorporating emojis could be helpful when discussing sensitive topics (e.g., oncology). HCPs thought that emojis would also be helpful when it is difficult to read patients’ emotions or when patients find it hard to express their emotions (e.g., communicating with children or patients who might not be able to verbalize emotions, especially when scared or nervous).
The HCPs agreed with the four scenarios identified during patient interviews. They further suggested that: (1) as emotional preparation before a visit, the concept of using emojis is a good first means of contact between a patient and an HCP. Despite this, they expressed some concerns that emojis might be difficult to interpret, and that this type of communication may be more beneficial following a visit, as the HCP may not have been able to read messages sent before the meeting; (2) as a follow-up after the visit, as it gives the patient time to think about the meeting and ask any questions; (3) in situations with a language barrier or when a patient has poor literacy (e.g., emojis have been used at immigrant health checks on arrival in Sweden); and (4) as replacement for numerical scales, emojis may provide the HCP with a more complete sense of how a patient feels. It could also give the patient a bit of flexibility to more holistically express specific emotions.
4 Discussion
In this three-phase quantitative and qualitative feasibility study, participants (including current patients and HCPs) reported common use of a wide range of emojis in personal text-based communications. Participants demonstrated consistent understanding of the emojis used to represent specific emotions. Participants and HCPs were willing to use text-based communication in healthcare settings, but existing platforms and systems were often too restrictive. The possible advantages of using emojis in patient–HCP communications were agreed upon by both groups, and four scenarios were identified as having specific potential: emotional preparation before a visit; follow-up after a visit; in situations where there is a language barrier; and as replacement for numerical scales to indicate the strength of emotion.
Emojis represent a universal language of pictures that can be used to express emotions and provide an emotional context in a way that is globally accessible and consistently recognizable. Our findings demonstrate the ubiquity of emoji use among our diverse international survey population, where 70% reported always or often using emojis to express emotions in personal communications (43% when describing mental health). The number of emojis depicting emotions and topics is continuously increasing, but results from this study support the universality of emojis. Survey participants chose similar emojis to represent specific emotions, and patients also had similar interpretations of the emojis shown during the interviews. However, findings from interviews with patients and HCPs demonstrate concerns around possible ambiguity in meaning when using emojis. The variability of emojis across different platforms (e.g., presentation styles in Android, iOS, and Microsoft systems) and meaning across cultures, racial background, or age groups may lead to inconsistent perception and misinterpretation of emojis (Bai et al., 2019; Lotfinejad et al., 2020). Thus, in a healthcare setting, there may still be a need to clarify the meaning of an emoji with text or a reference guide to provide the appropriate context for the emotion being conveyed. However, the impact of an accompanying text or guide on the ease of using emojis in healthcare communication needs to be evaluated.
Barriers to emoji use were also explored in this study. Although 62% of survey respondents thought emojis could be, or have been, useful to express their feelings, 76% had rarely or never done so in healthcare communications. Qualitative interviews with HCPs also found a willingness to use emojis when communicating with patients, but doing so is often prevented in current practices due to confidentiality concerns or system limitations. Patients and HCPs agreed on the four potential situations where emoji use might be most valuable, and this may help to direct future efforts to include emojis in patient–HCP communications.
The ubiquitous nature of mobile phone use across geographic regions and socioeconomic groups means that emojis are almost universally available as potential tools to help overcome barriers to patient–HCP communication (Kahn et al., 2010; Kaplan, 2006; Rashid and Elder, 2009). The perceived willingness and benefits of using emojis in healthcare settings described in this study align with findings from previous research that investigated the applications of emojis in pediatric or adult health care. A few studies have demonstrated the potential utility of emojis in overcoming illiteracy and language barriers when monitoring patients’ mood and emotion, to express the intensity of pain, in evaluating psychosocial aspects (e.g., mental health, wellbeing, resilience, and community connection), in health awareness, and to improve medication adherence (Davies et al., 2022; Franco and Fugate, 2020; He et al., 2022; Langdon et al., 2021; Lotfinejad et al., 2020; Pourmand et al., 2020; Szeto et al., 2022; Van Dam et al., 2019). In support of the proposal from patients and HCPs in our study, He et al have previously demonstrated that findings from an emoji-based visual analog pain scale were highly consistent with those from a numeric rating scale in a survey of 109 patients admitted to the emergency or surgical department (He et al., 2022). Furthermore, Setty et al showed that an animated emoji scale could be an effective and child-friendly tool to assess anxiety during dental visits (Setty et al., 2019). Results from our study also indicated that most survey respondents found emojis helpful in expressing emotions related to mental health; this aligns with previous publications that have investigated the possible utility of emojis as a screening tool for depression and in monitoring mental health through app-based self-reporting (Marengo et al., 2019; Van Dam et al., 2019). However, these earlier studies were limited by the lack of diversity in the study population. Many studies were mainly conducted in one country or medical facility, and some included people from specific age groups. Our feasibility study was both quantitative and qualitative and included a range of respondents of different ages and residing in different countries (including patients, friends or family of patients with cancer, people interested in learning about the study, and HCPs) to provide broad insights into the acceptability and potential benefits of integrating emojis into healthcare settings.
This study has several limitations. As this was a feasibility study, convenience sampling and descriptive statistics were used for the survey and interviews to determine current opinions on the utility of emojis in patient–HCP communication and generate hypotheses toward integrating emojis in healthcare communication. Members of the WOC community who did not participate in the survey may have different opinions to the respondents, and our results could possibly include volunteer bias. All survey respondents were English speakers, mostly from developed countries, aged 35–64 years (74%), and patients diagnosed with cancer or friends/family of a patient with cancer. Demographic and clinical characteristics of the participants may have affected their access and overall willingness to participate in text-based communication with their HCPs and their use and interpretation of emojis. Therefore, it is recommended to further evaluate the findings of this study in larger studies with various patients or HCP groups and including those from other regions and non-English speaking areas. Other relevant factors (e.g., personal communication preferences, age, sex, racial/cultural, or language differences) identified in previous research that could potentially impact the acceptability and benefits of using emojis in healthcare communication also need to be assessed in future studies (Brants et al., 2019; Herring and Dainas, 2020; Waughtal et al., 2021).
In summary, this three-phase feasibility study found that emojis could potentially improve patient–HCP communication by facilitating emotional expression, which is a core component of patient-centered care. Participants, including patients and HCPs, agreed that there were potential advantages of using emojis in healthcare settings. In the future, an interventional study in at least one of the four situations where emojis were identified as having the most potential benefit could be conducted to determine the added value of emojis in patient–HCP communication. Further research is also required to determine the practicalities of integrating emojis into healthcare communication and evaluate the impact on clinical outcomes.
Data availability statement
Data are available upon reasonable request. All data relevant to this study are included in the article or uploaded as supplemental information.
Ethics statement
This study was considered exempt from ethical review according to the Swedish Parliamentary Act 2003:460, because it is non-interventional, and it does not involve any sensitive personal data as referred to Article 9.1 of the EU Data Protection Regulation or any method aimed to affect the research subject physically or psychologically (Department of Education, Sveriges Riksdag, 2003). This study was also considered exempt from institutional research board review according to the US Department of Health and Human Services, Office for Human Research Protections, 45 CFR 46.104, (d)(2) because it involved survey and interview procedures, and the information obtained could not be linked to the research subjects or place them at risk (U.S. Department of Health and Human Services, 2018). The studies were conducted in accordance with the local legislation. The participants provided their written informed consent to participate in this study.
Author contributions
ME: Conceptualization, Writing – review & editing. KB: Conceptualization, Writing – review & editing. CD: Data curation, Formal analysis, Investigation, Methodology, Validation, Writing – review & editing. LA-D: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Validation, Visualization, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was sponsored by Pfizer.
Acknowledgments
Medical writing support was provided by April Cabang, PhD, of Engage Scientific Solutions (Fairfield, CT) and Jennifer Bodkin, PhD, of Engage Scientific Solutions (Horsham, UK) and was funded by Pfizer.
Conflict of interest
ME and KB are employees of Pfizer and hold stock/stock options. CD and LA-D were employees at War on Cancer, which was a paid contractor to Pfizer in connection with this study and the development of this manuscript.
The authors declare that this study was supported by Pfizer. Pfizer contributed to the study design. In their role as authors, employees of Pfizer were involved in the design of the study, interpretation of data, preparation, review, and approval of the manuscript and the decision to submit for publication, along with their co-authors. The study sponsor approved the manuscript from an intellectual property perspective but had no right to veto the publication.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcomm.2024.1402788/full#supplementary-material
References
Bai, Q., Dan, Q., Mu, Z., and Yang, M. (2019). A systematic review of emoji: current research and future perspectives. Front. Psychol. 10:2221. doi: 10.3389/fpsyg.2019.02221
Brants, W., Sharif, B., and Serebrenik, A. (2019). “Assessing the meaning of emojis for emotional awareness-a pilot study,” in Companion Proceedings of the 2019 World Wide Web Conference, 419–423.
Davies, J., Mckenna, M., Denner, K., Bayley, J., and Morgan, M. (2022). The emoji current mood and experience scale: the development and initial validation of an ultra-brief, literacy independent measure of psychological health. J. Ment. Health 33, 218–226. doi: 10.1080/09638237.2022.2069694
Department of Education, Sveriges Riksdag . (2003). Act (2003:460) on ethical review of research involving humans. Available at: https://www.riksdagen.se/sv/dokument-och-lagar/dokument/svensk-forfattningssamling/lag-2003460-om-etikprovning-av-forskning-som_sfs-2003-460/ (Accessed January 2, 2024).
Franco, C. L., and Fugate, J. M. B. (2020). Emoji face renderings: exploring the role emoji platform differences have on emotional interpretation. J. Nonverbal Behav. 44, 301–328. doi: 10.1007/s10919-019-00330-1
He, S., Renne, A., Argandykov, D., Convissar, D., and Lee, J. (2022). Comparison of an emoji-based visual analog scale with a numeric rating scale for pain assessment. JAMA 328, 208–209. doi: 10.1001/jama.2022.7489
Herring, S. C., and Dainas, A. R. (2020). Gender and age influences on interpretation of emoji functions. ACM. T. Soc. Comput. 3, 1–26. doi: 10.1145/3375629
Kahn, J. G., Yang, J. S., and Kahn, J. S. (2010). 'Mobile' health needs and opportunities in developing countries. Health. Aff. 29, 252–258. doi: 10.1377/hlthaff.2009.0965
Kaplan, W. (2006). Can the ubiquitous power of mobile phones be used to improve health outcomes in developing countries? Glob. Health 2:9. doi: 10.1186/1744-8603-2-9
King, A., and Hoppe, R. B. (2013). "Best practice" for patient-centered communication: a narrative review. J. Grad. Med. Educ. 5, 385–393. doi: 10.4300/JGME-D-13-00072.1
Lai, D., Lee, J., and He, S. (2021). Emoji for the medical community-challenges and opportunities. JAMA 326, 795–796. doi: 10.1001/jama.2021.8409
Langdon, K. J., Scherzer, C., Ramsey, S., Carey, K., Rich, J., and Ranney, M. L. (2021). Feasibility and acceptability of a digital health intervention to promote engagement in and adherence to medication for opioid use disorder. J. Subst. Abus. Treat. 131:108538. doi: 10.1016/j.jsat.2021.108538
Li, L., and Yang, Y. (2018). Pragmatic functions of emoji in internet-based communication—a corpus-based study. Asian-Pac. J. Sec. Foreign Lang. Educ. 3:16. doi: 10.1186/s40862-018-0057-z
Lotfinejad, N., Assadi, R., Aelami, M. H., and Pittet, D. (2020). Emojis in public health and how they might be used for hand hygiene and infection prevention and control. Antimicrob. Resist. Infect. Control 9:27. doi: 10.1186/s13756-020-0692-2
Lu, X., Ai, W., Liu, X., Li, Q., Wang, N., and Huang, G. (2016). “Learning from the ubiquitous language: an empirical analysis of emoji usage of smartphone users,” in UBICOMP '16, September 12–16, 2016. Heidelberg: Association for Computing Machinery, 770–780.
Marengo, D., Settanni, M., and Giannotta, F. (2019). Development and preliminary validation of an image-based instrument to assess depressive symptoms. Psychiatry Res. 279, 180–185. doi: 10.1016/j.psychres.2019.02.059
Nante, G. T. N. (2018). Emoji: what does the scientific literature say about them? A new way to communicate in the 21th century. J. Hum. Behav. Soc. Environ. 28, 528–533. doi: 10.1080/10911359.2018.1437103
Pourmand, A., Quan, T., Amini, S. B., and Sikka, N. (2020). Can emojis assess patients' mood and emotion in the emergency department? An emoji based study. Am. J. Emerg. Med. 38, 842–843. doi: 10.1016/j.ajem.2019.09.008
Ptaszynski, M., Maciejewski, J., Dybala, P., Rzepka, R., Araki, K., and Momouchi, Y. (2012). Science of emoticons. In: Siddiqui, Tanveer J. (eds.) Speech, image, and language processing for human computer interaction: Multi-modal advancements. Hershey, PA: IGI Global.
Rashid, A. T., and Elder, L. (2009). Mobile phones and development: an analysis of IDRC-supported projects. Electron. J. Inf. Sys. Dev. Countr 36, 1–16. doi: 10.1002/j.1681-4835.2009.tb00249.x
Robinson, J. H., Callister, L. C., Berry, J. A., and Dearing, K. A. (2008). Patient-centered care and adherence: definitions and applications to improve outcomes. J. Am. Acad. Nurse Pract. 20, 600–607. doi: 10.1111/j.1745-7599.2008.00360.x
Setty, J. V., Srinivasan, I., Radhakrishna, S., Melwani, A. M., and Dr, M. K. (2019). Use of an animated emoji scale as a novel tool for anxiety assessment in children. J. Dent. Anesth. Pain Med. 19, 227–233. doi: 10.17245/jdapm.2019.19.4.227
Szeto, M. D., Barber, C., Ranpariya, V. K., Anderson, J., Hatch, J., Ward, J., et al. (2022). Emojis and emoticons in health care and dermatology communication: narrative review. JMIR. Dermatol. 5:e33851. doi: 10.2196/33851
The Unicode Consortium . (1999-2022). About Emoji. Available at: https://home.unicode.org/emoji/about-emoji/ (Accessed November 17, 2022).
Unicode, I. (1991-2022). Emoji counts, v15.0. Available at: https://unicode.org/emoji/charts/emoji-counts.html (Accessed November 17, 2022).
U.S. Department of Health and Human Services . (2018). Exemptions (2018 Requirements). Subpart A. Basic HHS policy for protection of human research. Available at: https://www.hhs.gov/ohrp/regulations-and-policy/regulations/45-cfr-46/common-rule-subpart-a-46104/index.html (Accessed January 2 2024).
Van Dam, L., Rietstra, S., Van Der Drift, E., Stams, G., Van Der Mei, R., Mahfoud, M., et al. (2019). Can an emoji a day keep the doctor away? An explorative mixed-methods feasibility study to develop a self-help app for youth with mental health problems. Front. Psych. 10:593. doi: 10.3389/fpsyt.2019.00593
Waughtal, J., Luong, P., Sandy, L., Chavez, C., Ho, P. M., and Bull, S. (2021). Nudge me: tailoring text messages for prescription adherence through N-of-1 interviews. Transl. Behav. Med. 11, 1832–1838. doi: 10.1093/tbm/ibab056
Keywords: emojis, patient–healthcare professional communication, patient-centered care, healthcare communication, survey
Citation: Essex MN, Blakeman KH, Dietrich CE and Arnheim-Dahlström L (2024) The potential for emojis to facilitate communication between patients and healthcare professionals: results from a digital survey and qualitative interviews. Front. Commun. 9:1402788. doi: 10.3389/fcomm.2024.1402788
Edited by:
Parul Jain, Ohio University, United StatesReviewed by:
Jennifer K. Ptacek, University of Dayton, United StatesMohammed Habes, Yarmouk University, Jordan
Copyright © 2024 Essex, Blakeman, Dietrich and Arnheim-Dahlström. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lisen Arnheim-Dahlström, bGlzZW4uYXJuaGVpbS5kYWhsc3Ryb21AZ21haWwuY29t
†Worked at War on Cancer at the time of the study