
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Commun. , 24 October 2023
Sec. Language Communication
Volume 8 - 2023 | https://doi.org/10.3389/fcomm.2023.1176827
This article is part of the Research Topic Digital Participation and Communication Disorders across the Lifespan View all 15 articles
 Juliane Leinweber1*
Juliane Leinweber1* Birte Alber2*
Birte Alber2* Maria Barthel1
Maria Barthel1 Alexander Sean Whillier1
Alexander Sean Whillier1 Silke Wittmar3
Silke Wittmar3 Bernhard Borgetto3
Bernhard Borgetto3 Anja Starke2
Anja Starke2Introduction: In Germany, as around the world, the use of digital media in speech and language therapy became part of the service during the COVID-19 pandemic. This resulted in a need for empirical studies on the use and acceptance of digital media technologies, to determine users' requirements and concerns regarding the newly mandated technologies, in order to support its expansion in education and training going forward. “Acceptance” has been previously identified as an important aspect behind successful technology adoption. Therefore, two online questionnaire studies were conducted to explore how technology use is accepted among speech and language therapists in Germany.
Methods: Study 1 involved a questionnaire about video therapy with 15 question groupings, examining technology acceptance and competence. From 841 initial respondents, 707 complete responses were included in the analysis. Study 2 involved a different questionnaire, examining technology acceptance and digital media in therapy. In total, 79 individuals participated in the second survey. Study 1 data were analyzed to identify unifying factors underlying respondent attitudes and was followed up with a logistical regression; Study 2 data were analyzed with multiple linear regression.
Results: In Study 1, external inhibiting and facilitating conditions were identified which had an impact on attitudes toward video therapy adoption and its intended future use. In Study 2, the modified model of the Unified Theory of Acceptance and Use of Technology (UTAUT) explained 58.8% of the variability in therapist's Behavioral Intention to Use digital media. Here, Performance Expectancy was a significant predictor.
Conclusions: Both studies investigated facilitating and inhibiting factors for the implementation of digital media including video therapy in future speech therapy services. Results demonstrated that the use is accepted in therapy. Therefore, optimal conditions—both institutional and individual—are needed to enable digital participation for therapists and patients. In future education and training, trainers should focus on the functional aspects of the technologies to be used, in order to positively influence Performance Expectancy in a targeted manner and thus increase the therapists' intention to use digital technology in therapy, which in turn promotes patients' digital participation.
Information and communication technology (ICT) is a growing area of research in health care, including in speech and language therapy (SLT), and its applications are varied—e.g. synchronous and asynchronous telerehabilitation, technology-based interventions and therapy applications, documentation and administration (Alber and Starke, 2021b; Kearns and Kelly, 2022). The use of digital media in speech and language therapy has been repeatedly called for in the past and became part of therapists' everyday life due to the mandate to transition to video therapy during the COVID-19 pandemic in Germany. Speech and language therapists around the world have access to an increasing number of technological resources to support clinical practice, such as electronic devices, software and internet resources, which have been shown to positively impact therapy (e.g. Albudoor and Pena, 2021). ICT is increasingly used in SLT as it comes to be seen as offering efficient and effective options to improve therapeutic outcomes (Jesus et al., 2019; Kearns and Kelly, 2022).
ICT should not be used in isolation—it should be viewed as a set of tools in the therapist's toolbox, as successful integration of ICT into therapy has been shown to confer many benefits. Technology integration in therapy can improve engagement from both patients and therapists (Leinweber and Barthel, 2022; Olszewski et al., 2022). Video therapy technologies make it possible for people to participate in therapy who would not otherwise be able to receive care due to illness, poor healthcare coverage in their region or other factors (Cason, 2009; Tucker, 2012; Hall et al., 2013; Fairweather et al., 2016; Lauer, 2020; Buabbas et al., 2022; Leinweber and Barthel, 2022). With increased integration of ICT in therapy, its use can extend into everyday life and thus enable both independent and supervised practice (Theodoros, 2012; Jakob et al., 2018; Böhm, 2019; Preßler, 2019; Nichol et al., 2022) or facilitate exchange with other people via apps or social media, thus further improving therapeutic outcomes (Welch et al., 2016). In particular, people with language impairments need targeted support in order to successfully participate in both the digital world and in the real world (Steiner, 2023). By including ICT in SLT, it is possible to work on concrete digital participation goals (Steiner, 2023) and to concurrently expand and reshape existing forms of therapy on the grand scale.
ICT represents a very diverse toolkit (Starke and Leinweber, 2019); for example, in the broad variety of software applications (apps). In general use, apps support communication, sometimes by supplementing it—e.g., when a group of people sitting in a café discuss a video playing on someone's phone—or sometimes completely substituting it—e.g., when the same group of people are half a world apart discussing the video while on a messaging forum. Apps can also remove communication barriers, such as social distancing; they can serve as learning aids, e.g., language apps; they can facilitate unlikely connections, e.g., job-seeker apps; they can support motivation, e.g., fitness apps.
In the context of research and therapy, apps can facilitate a similarly broad array of possibilities. In simple terms, apps can serve as a feedback aid for the speech therapist (Wahl et al., 2018). Patients can use apps to practice independently, which can be an effective supplement to their therapy (Böhm, 2019; Nichol et al., 2022). Apps have also been shown to increase the intensity and frequency of therapy (Nordness and Beukelmann, 2010; Hall et al., 2013; Lauer, 2020). The use of apps has been demonstrated to improve therapy motivation (Gačnik et al., 2018; Preßler, 2019). Edwards and Dukhovny (2017) have also noted various advantages in the research and therapy contexts in streamlining data capturing process, cost savings and, most importantly, the benefit of interactive presentation of multimodal therapy, i.e., 3D audio-visual animation. Apps provide all of these benefits and possibilities, regardless of location (Gačnik et al., 2018).
Besides apps, another example of digital media use is videoconferencing systems, such as those which were employed in SLT services in Germany for the first time during the COVID-19 pandemic. Without the possibility of video therapy services, adequate care of patients could not be ensured (Bilda et al., 2020; Schwinn et al., 2020; Bürkle et al., 2021). SLT primarily involves a patient and a therapist engaging in auditory and visual interactions; these interactions can be easily transferred to an online or technology-based environment, provided that auditory and visual cues can be adequately replicated and broadcast over a distance (Theodoros, 2012). While video therapy had already been established internationally in SLT for some years (Rangarathnam et al., 2016; Wales et al., 2017; Sutherland et al., 2018; McGill et al., 2019), it had not been nationally implemented as standard practice in Germany.
Various studies have shown that video therapy is appropriate for use in SLT (Wales et al., 2017; Jung et al., 2020; Weidner and Lowman, 2020). In their meta-analysis, Jung et al. (2020), concluded that the effectiveness of teletherapy and face-to-face therapy may vary depending on the characteristics of the client and the type of therapy, and that it is important to consider the patient's disorder and the type of therapy when choosing between teletherapy and face-to-face therapy. Telepractice does not seem to negatively impact the relationship between speech language therapists and pediatric clients compared to face-to-face therapy (Freckmann et al., 2017; Oprandi et al., 2021), and in various German studies it has been shown that it can be used with patients of different indications and age groups (Bilda et al., 2020; Schwinn et al., 2020; Beushausen and Sippel, 2021; Mörsdorf and Beushausen, 2021).
When considering a patient's digital participation in video therapy, not only the patient's experience but also the therapist's experiences matter. In cases where therapists' early experiences of video therapy were negative, the chance of immediate discontinuation of videoconferencing systems rose considerably (Hastall et al., 2017). In this context, therapists have a stakeholder role—they are concurrently users themselves and they provide patients with access to and guidance in appropriate technologies. Clinician behavior explains much of the variation in the uptake, expansion and sustainability of telemedicine services (Wade et al., 2014)—when therapists integrate ICT into therapy and make it possible for patients to associate ICT with positive experiences, a foundation can be laid for the future use of digital media on the part of patients. The digital participation of patients is therefore strongly dependent on the attitudes and skills of therapists with regard to digital media (Steiner, 2023). Thus, to improve patient usage and therapeutic outcomes, the positive and negative factors influencing therapists must be clearly understood.
To gain this understanding, the current two studies were designed to explore how technology use is accepted among speech and language therapists in Germany. In this context, acceptance refers to the positive decision to utilize and apply an innovation (Simon, 2001). Although a highly subject-specific positive attitude of an individual is usually a prerequisite for acceptance, it alone is not sufficient—acceptance also takes into account the potential or actual use of the new technology in addition to attitude formation (Kollmann, 1999). In the context of video therapy usage, Rettinger et al. (2021) identified that acceptance was one of the two key elements that define the usage of video therapy (the other being regulatory frameworks).
When it comes to the early acceptance of video therapy, the most common obstacle worldwide is technically overstretched staff (Scott Kruse et al., 2018). In order to be able to digitally act safely in the future and to support their patients' digital participation, therapists need to be digitally competent. Unfortunately, digital skills and the use of digital tools are not as yet an integral part of healthcare education in Germany and Europe more generally (European Health Parliament, 2020). The training of digital skills, alongside its underlying acceptance, represents one of the current challenges in professionalization in the field of communication disorders (Lin et al., 2021). Incorporating digital topics and skills into academic and professional development curricula has been well identified as critical to ensure that the field of communication disorders is prepared for the ever-digitizing healthcare environment (Brennan et al., 2010; Theodoros, 2012; Edwards and Dukhovny, 2017; Lin et al., 2021). Understanding the adoption and acceptance of digital media in SLT is crucial for optimizing application selections in therapy itself and educational strategies in training settings (Hastall et al., 2017; Albudoor and Pena, 2021). Thus a clear understanding of the challenges facing therapists can inform educational institutions of any systematic gaps in understanding.
Acceptance, as defined above, is a latent construct (Jockisch, 2010), which is why models are used to explain which facets make up the construct and which factors influence it; one such model is the Unified Theory of Acceptance and Use of Technology (UTAUT) (Venkatesh et al., 2003). This model was used in Study 2 of this paper. The model, and its supplements and modifications, will be introduced here.
The UTAUT is an empirically tested integrative and global model developed from the main existing technology acceptance theories. Subsequent research has combined or extended the UTAUT model with other theories to examine a variety of technologies in organizational and non-organizational contexts (Venkatesh et al., 2016). The increasing prevalence of ICT applications has led to the UTAUT being widely adopted in a variety of research areas (Williams et al., 2014; Venkatesh et al., 2016). The UTAUT has also been validated in different environments, such as education (Birch and Irvine, 2009; Khechine et al., 2014) and healthcare (El-Gayar et al., 2008; Liu et al., 2015).
In the original UTAUT model, four constructs were identified as predictors of Behavioral Intentions and Usage of ICT: performance expectancy (PE), Effort Expectancy (EE), Social Influence (SI) and Facilitating Conditions (FC). PE is defined as the degree to which a person believes that using ICT will help him or her to attain goals in job performance. EE refers to the degree of ease associated with the use of ICT. SI represents the degree to which a person perceives that other important or influential people believe he or she should use ICT. Finally, FC is defined as the degree to which an individual believes that organizational and technical infrastructure exists to support the use of ICT (Venkatesh et al., 2003). The model used in Study 2 was modified, as in other studies, to also consider Facilitating Conditions (FC) as a direct predictor of Behavioral Intentions to Use (BIU).
In addition to the predictors, there are four moderating variables which can affect the relative influence of the predictors in the original model: gender, age, experience and voluntariness of use (Venkatesh et al., 2003). In addition to the determinant factors, the model uses Behavioral Intention to Use (BIU) as a dependent variable. Behavioral Intention is defined as “the degree to which a person has formulated conscious plans to perform or not perform some specific future behavior” (Warshaw and Davis, 1985, p. 214), in this case the use of technology. Both the original authors (Venkatesh et al., 2003) and future publications (e.g., Lakhal et al., 2013) have suggested enriching the UTAUT model; in order to additionally capture and map specific influences in the field of speech and language therapy, four supplementary UTAUT concepts (impact of peers, familiarity, self-efficacy and attitude) are each presented below.
In outpatient SLT settings, many therapists are part of teams that support and influence each other in terms of content and/or organization. Peer support can enhance users understanding, by providing insight on job relevance, output quality, and result demonstrability of a system (Venkatesh and Bala, 2008). Peer support can also influence the subjective norm and image associated with using digital media. If peers have a positive attitude toward digital media, it is more likely that employees will hold a positive perception (Venkatesh and Davis, 2000; Venkatesh and Bala, 2008). Therefore, the Attitude of Colleagues (AoC) is a relevant supplemental factor.
When people begin to use new digital media in their work, they are likely to experience changes in their intrinsic work characteristics, work processes, routines, and habits (Millmann and Hartwick, 1987). Reactions to these changes are highly individualized and can be positive or negative (Orlikowski, 2000; Boudreau and Robey, 2005). If individuals feel their wellbeing is threatened by these changes, avoidance and rejection are more likely to occur (Beaudry and Pinsonneault, 2005). Comparatively, if digital media are already used in the workplace and superiors have a positive attitude toward ICT use, therapists may feel more comfortable with the next step—accurate perception of a system or a tool is very important before using new ICT (Venkatesh and Bala, 2008). Familiarity with the use of digital media in the direct work environment can have a positive influence on the acceptance of the technology. This is the factor addressed by the model supplement Digitality at Work (DaW).
A related factor is an individual's self-efficacy with a computer; that is, the degree to which an individual believes that he or she possesses the ability to perform a specific task or job using a computer (Compeau and Higgins, 1995; Venkatesh and Bala, 2008). The personal conviction of one's own abilities can influence the intention to use digital media and thus their acceptance of technology (Compeau and Higgins, 1995; Compeau et al., 1999). This construct has been termed the Self-Assessment of Digital Competencies (SAoDC).
Based on different theories of technology acceptance, attitude toward using digital media can also have an impact on acceptance. Attitude is a learned predisposition to respond in a positive or negative way to a given object in a consistent manner (Lakhal et al., 2013). The concept represents a summary of underlying basic constructs of individual theories, e.g., Theory of Reasoned Action (Fishbein and Ajzen, 1975; Davis et al., 1989), Theory of Planned Behavior (Taylor and Todd, 1995b), Combined TAM and TPB (Taylor and Todd, 1995a), Motivational Model (Davis et al., 1992), Model of PC Utilization (Thompson et al., 1991), and Social Cognitive Theory (Compeau and Higgins, 1995; Compeau et al., 1999). Venkatesh et al. (2003, p. 455) summarized the concept as follows: “Attitude toward using technology is defined as an individual's overall affective reaction to using a system”. The concept of Attitude and Affect Toward Digital Media Use (AUDM) appeared relevant for the present study. Figure 1 shows the extended model which is relevant for Study 2.
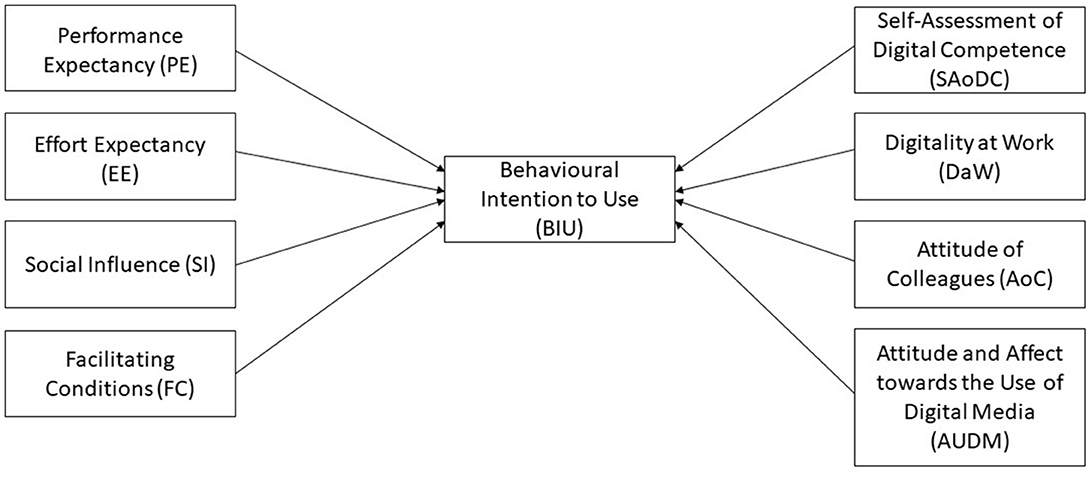
Figure 1. Basic UTAUT-model extended by four variables (Study 2).
Despite the modifications, the UTAUT follows a relatively simple premise. Venkatesh et al. (2003) assume that the intention to use technology, which is influenced by various factors, has a direct impact on actual use.
More recently, Hastall et al. (2017) criticized such technology acceptance models for ignoring the dynamic and multi-determined process of using technology; this critique is of particular relevance to Study 1. More in detail, they claimed that the attention to the developmental process of technologies, the view of human motivation on technology, the social influences on individuals and the differences between individuals using technologies were all inadequately considered. Therefore, they discussed three approaches through which technology adoption can be promoted: (1) a realistic view about decision-making processes of individuals, (2) sufficient knowledge about different stages of technology adoption, and (3) focus on social, organizational and situational determinants. This results in three dimensions—individual-related factors, environment-related factors, and technology-related factors.
More specifically, Individual-related factors encompass approach behaviors and avoidance behaviors. In the case of video therapy, both behaviors can arise simultaneously in a given situation, for example, while the therapist supports the patient verbally during the exercise, the patient needs a hands-on situation to fully engage. Environment-related factors, such as social, organizational and situational factors, can express as external supportive or inhibitive influences on video therapy. Technology-related factors encompasses the technology itself, including negative complications (e.g., costs, software incompatibility) and rewarding aspects (e.g., increased accuracy, increased efficiency). All factors have implications on the adoption and acceptance of digital media in health care.
Overall, the failure of digital media use in a given setting is underpinned by the non-acceptance and non-usage of the technology by its end users (Standing et al., 2016). In considering the factors that underpin acceptance and use, Niklas (2015) emphasizes that acceptance is a result of a complex decision-making process that is affected by social and situational influences. Thus, to achieve a successful rollout of any digital media technology, different goals must be met; these include: reducing individual barriers, increasing psychological wellbeing, facilitating healthy aging in familiar places and ensuring social participation (Hastall et al., 2017). If technology is assessed and accepted as useful and necessary for professional life, then people are also prepared to deal with future innovations and iterations, and to review and expand their own competencies to match. In this way, it becomes possible to include digital participation as a fundamental goal of SLT work. This results in a need for empirical studies on the use, acceptance and adoption of digital media in SLT in order to be able to determine needs with regard to the expansion of competencies in education and training, but also to increase acceptance.
As ICTs, such as video therapy and apps, are promising innovations in SLT, the current two studies were designed to examine the acceptance of these technologies by German speech and language therapists. Study 1 focuses on positive and negative factors which correlate with the therapist's future use of video therapy and it interprets which factors may thus influence successful implementation of video therapy. Study 2 examines factors influencing the therapists' intention to use digital media in SLT in the future and identifies factors that influence this intention. By identifying supporting and inhibiting factors based on different theoretical assumptions and models, these studies build together to inform the development of training and professional education, to ensure and expand the targeted use of digital media in the future. By inference, these studies would also improve and sustain the future digital participation of patients.
In order to investigate the factors which correlate with successful implementation of video therapy in SLT, Study 1 narrowed its focus on the constructs of acceptance and competence. The authors sought questions from past research on technical acceptance, drawing heavily on Hastall et al. (2017), as well as past key findings in the area of adoption and acceptance especially of video therapy in SLT (Molini-Avejonas et al., 2015; Pitt et al., 2018; Tyagi et al., 2018; Leinweber and Schulz, 2019).
The following research questions were investigated by Study 1:
a. What factors correlate with the prospective adoption of video therapy by speech and language therapists?
b. What constructs underlie the attitudes of users toward technology acceptance and technology competence in the context of SLT?
An initial questionnaire, made up of 52 question groupings (see Measure below), was developed at the University of Applied Sciences and Arts (German: HAWK Hildesheim/Holzminden/Göttingen) in early 2020. The survey was hosted online from June 3rd to July 1st, 2020, on the online freeware SoSciSurvey website (Leiner, 2019). The data were stored on the SoSciSurvey server until the end of the data collection period, then they were transferred to the university's own server until June 30th, 2030, and deleted from the SoSciSurvey server. Persons outside the project team and temporary staff have no access to the data.
Recruitment was conducted through the German Federal Association of Speech and Language Therapy (Deutscher Bundesverband für Logopädie e.V.), which has about 10,000 members. Respondents were asked to participate if they were providing speech and language therapy in an outpatient setting in Germany at the time of the survey. The participants were informed about the study contents and data privacy and gave their informed consent. Where consent was refused, retracted or could not be ensured, participation was excluded.
From 841 online responses, 25 were excluded due to denied informed consent (n = 22), invalid data (n = 2) and a profession outside of SLT (n = 1). Subsequently, an inconsistency check was made to proof data validity (Schrepp, 2016). In this context, a time-related test and a content test were made, but no irregularities were found. However, an additional 109 participants submitted substantially incomplete responses, meaning more than 80% missing data, and were therefore excluded from the analysis. Thus, in the end, 707 participant responses were included and analyzed in this study.
From the 707 complete respondents, 671 were female and 36 male (94.9% female). Participants ranged in age from 21 to 68 years (M = 43.32 years, SD 11.38 years), with one respondent not reporting their age. Work experience ranged from zero to 44 years (M = 16.81 years, SD = 9.85 years). Most of the participating therapists were self-employed in their own practice (62.4%), nearly one-third were employed in an outpatient practice (33.1%), a few were working on a fee basis (freelancer) (2.5%) and a few did not respond to this question (2%). A small number of participants indicated “other” (e.g., working as a teaching speech therapist or being in education; 1.7%). Table 1 shows the demographic data.
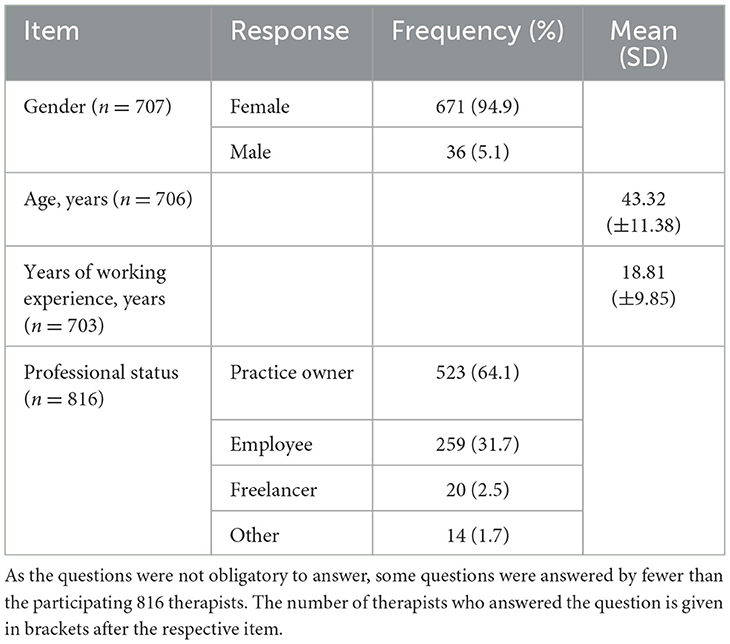
Table 1. Participants' demographics in Study 1.
The original questionnaire consisted of 52 question groupings (forced-choice, multiple response and free-form response), grouped into seven categories.
1. Implementation of videoconferencing, as inclusion criteria (2 question groupings),
2. Sociodemographic data (7 question groupings),
3. Resources used for videoconferencing (7 question groupings),
4. Technology use (5 question groupings),
5. Current implementation of videoconferencing (21 question groupings), and
6. Adoption of videoconferencing in future health care delivery (9 question groupings), plus
7. General feedback to the questionnaire (1 question).
The questions were created in accordance with literature about technology use in SLT (e.g., Molini-Avejonas et al., 2015; Pitt et al., 2018; Tyagi et al., 2018; Leinweber and Schulz, 2019). Each grouping was structured as a question with multiple response options, e.g., “in which contexts have you used video therapy”. Answers consisted of closed multiple choice options, plus a free text field, e.g., “individual therapy”; “group therapy”; “individual counseling”; “group counseling”; “other (text field)”. Respondents could select any and all responses that were relevant. These question groupings were then recoded into unique binary questions for the statistical analysis (see below). The questionnaire used will be published in a separate article.
In preparing the data used for the regression, five of the adoption questions were deemed appropriate and were combined for the dependent variable; these related to: regarding usefulness of video therapy (VT), increased frequency of VT use, making VT standard practice, whether VT is as successful as in person therapy and whether VT affects the relationship with the patient. Seven of the question groupings concerning technology acceptance (TA) and eight groupings concerning technology competence (TC) were selected for independent variables, informed by past literature. The same TA and TC question groupings were then used in the factor analysis.
All calculations were performed with the IBM SPSS program version 27 (IBM Corp, 2020). All multi-answer question groupings were dummy-coded into individual binary response questions, to facilitate the use of stronger statistical analyses. No data was lost in this recoding process.
To examine what influences the prospective adoption of video therapy by speech and language therapists, a regression analysis was planned. However, as the dependent variable was found to be significantly non-normally distributed and could not be sufficiently rectified via standard correction methods, a statistically weaker but more robust logistical ordinal regression was performed.
To form the dependent variable, the five questions regarding the participants' views on video therapy adoption (mentioned above in Measure) were recoded into positive (+1), negative (−1) and neutral (0) and summed together to form a general “Opinion of Video Therapy” variable (see Table 2), ranging from +5 (all positive) to −5 (all negative). This resulted in a single variable with a distribution that could be statistically analyzed.
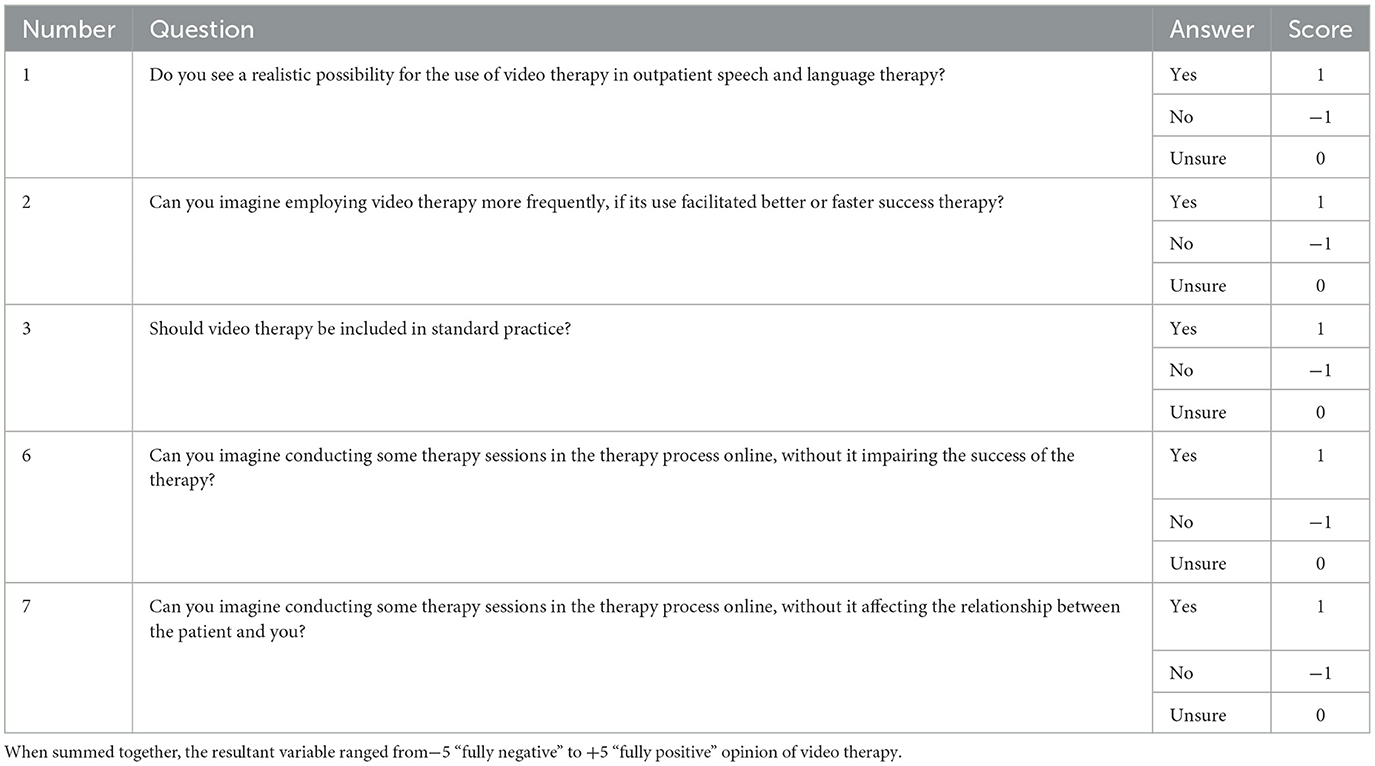
Table 2. Question responses informing the independent variable “Opinion of Video Therapy”.
As independent variables, the regression included all binary recoded question items from the factor analysis (89 individual question items in all).
To investigate the constructs underlying the attitudes of users toward technology acceptance and technology competence in the context of SLT, the data were analyzed using principal axis factoring with varimax rotation. As one of the 15 question groupings did not load on any factor due to insufficient variance in the responses, it was excluded from further examination. Thus 14 question groupings from the questionnaire were included in the final analysis. See Table 3 for a complete list of included questions, with the excluded item marked in gray.
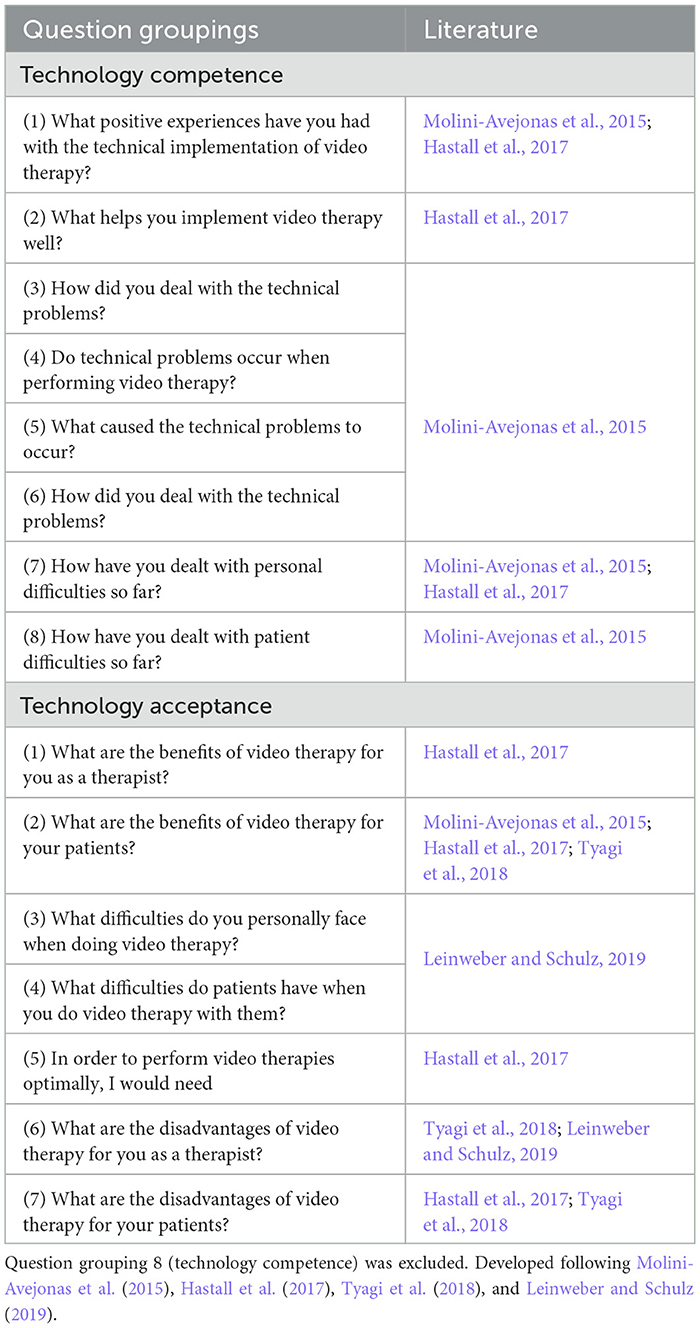
Table 3. Question groupings representing video therapy acceptance and competence in Study 1.
Although the data were not all perfectly normally distributed, due to the robust nature of the analysis and the use of binary independent variable items, the data was deemed to be acceptable for the analysis. A preliminary factor analysis was originally conducted which was limited to 25 iterations; the resultant Scree plot identified four primary factors before tailing off, thus the final factor analysis was limited to four factors. This four factor analysis is presented in the Results section.
To investigate the technology acceptance of speech and language therapists, the UTAUT was chosen as a basis. The constructs Attitude of Colleagues (AoC), Digitality at Work (DaW), Self-Assessment of Digital Competencies (SAoDC), and Attitude and Affect toward the Use of Digital Media (AUDM) were included as additional variables.
The following research questions were investigated by Study 2:
c. To what extent are speech and language therapists intending to use ICT in therapy in the future?
d. To what extent do Performance Expectancy, Effort Expectancy, Social Influence, and Facilitating Conditions, as well as additional factors, predict speech language therapists' Behavioral Intention to Use digital media in therapy?
The development of the used online questionnaire took place in the department of Inclusive Education for speech, language, and communication needs at the University of Bremen (Germany). The survey period ran from mid-July to November 2020.
The questionnaire was made available via LimeSurvey (Limesurvey GmbH). Respondents were asked to participate if they were providing SLT in an outpatient setting in Germany at the time of the survey or had done so prior to the COVID-19 pandemic. Use of digital media or delivery of video therapy during the COVID-19 pandemic did not constitute inclusion criteria. Recruitment was conducted through German SLT associations and networks as well as personal contacts of the authors. Participants were informed of the study content and were required to provide informed consent before beginning the survey. Participation could be discontinued at any time during the survey. The data is stored on the university server and will remain stored until 2030, and only project-internal employees will have access to it.
In total 79 individuals took part in the survey, of which 75 were female and four male (94.9% and 5.1%, respectively). Respondents ranged in age from 22 to 67 years (M = 43.37 years, SD = 10.9). Work experience was reported between one and 40 years (M = 16.39 years, SD = 9.6). 69 of the respondents indicated a speech/language therapy practice as their workplace (87.3%). Other places of employment included (interdisciplinary) therapy centers, early intervention centers, and a social pediatric center. Two respondents reported working in three different facilities in combination (see Table 4).
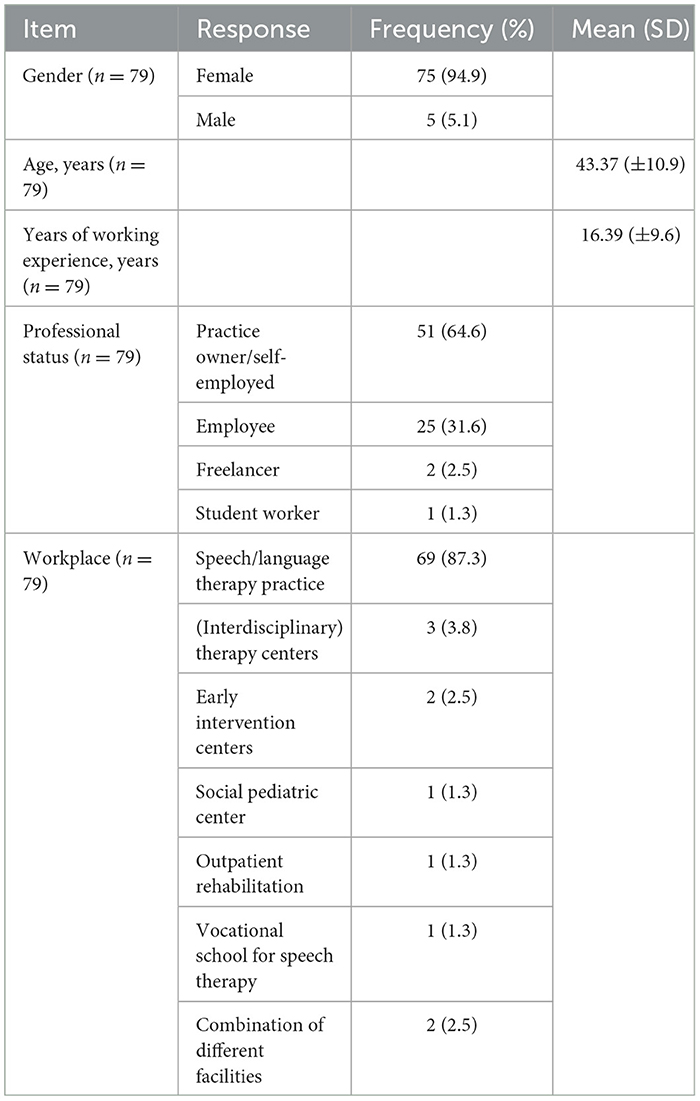
Table 4. Respondents' demographics in Study 2.
The majority of respondents (64.6%) were self-employed in their own practice. Nearly one-third were not self-employed/employed (31.6%). In addition, two freelancers working on a fee basis (2.5%) and one student worker (1.3%) participated in the survey.
At the University of Bremen in early 2020, a theory-based questionnaire was created to examine technology use, personal experiences regarding technology use in everyday work, and technology acceptance of SLT. The questionnaire also included a general part with questions on socio-demographic information. The data used for the presented study came from the questionnaire section on technology acceptance and the experience with digital media use.
Different items were used to query technology acceptance. 14 of the items used were German translations and modifications of the adapted UTAUT items validated by Teo (2009, 2010), which have their origin in Venkatesh et al. (2003). They are shown in the Table 5. All items were Likert items which were summarized in 5 Likert scales following past literature (Harpe, 2015). The five response options were: 0 = does not apply at all; 1 = mostly does not apply; 2 = undecided; 3 = mostly applies; 4 = applies fully.
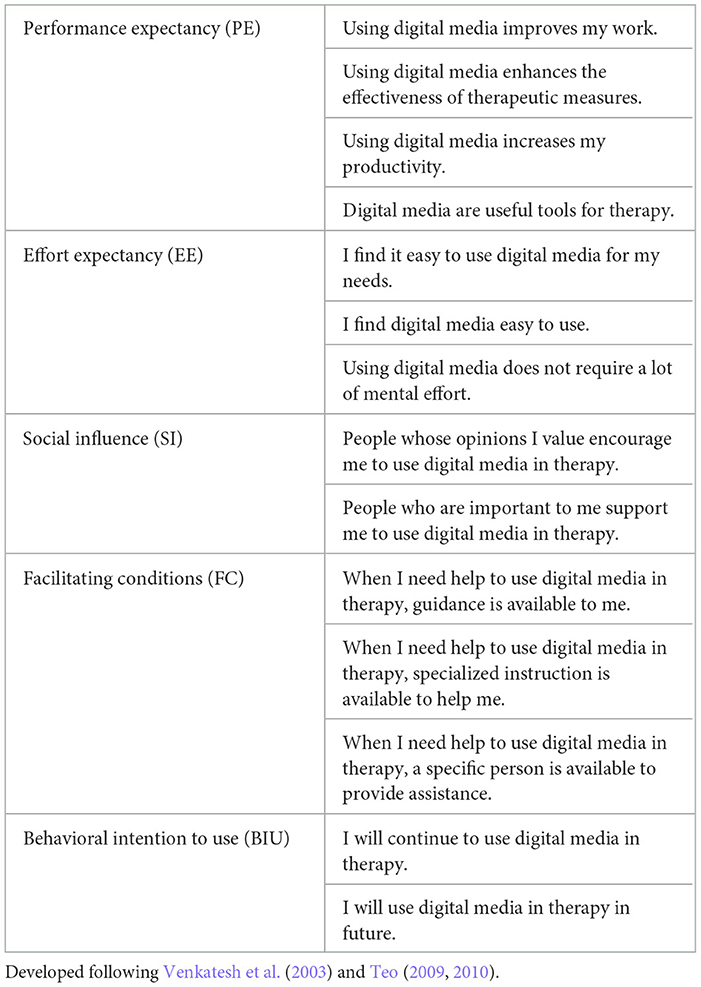
Table 5. Technology acceptance items used in Study 2.
The internal consistency of the 14 used UTAUT items was determined by Cronbach's alpha. With a value of α = 0.892, internal consistency was high (Cortina, 1993). The internal consistencies were also calculated for the individual Likert scales of the four predictors of the UTAUT model which also turned out to be high: PE α = 0.890; SI α = 0.813; FC α = 0.899. The value for EE was acceptable: α = 0.769.
In addition to the UTAUT items, a total of 25 items were developed for the constructs of Attitude of Colleagues (AoC), Digitality at Work (DaW), Self-Assessment of Digital Competence (SAoDC), and Attitude and Affect toward the Use of Digital Media (AUDM) and included in the questionnaire. The items on these constructs were developed from theory and generated as Likert items (Harpe, 2015) according to the used UTAUT items.
Factor analyses (principal axis analyses; VARIMAX, 50 iterations) were conducted to identify appropriate items related to the constructs developed from theory. The 25 items of the additional constructs as well as the 12 items of the latent constructs Performance Expectancy (PE), Effort Expectancy (EE), Social Influence (SI), and Facilitating Conditions (FC) of the UTAUT were included, while the two items capturing the dependent variable Behavioral Intention to Use (BIU) were not included in the factor analysis. In this way, a total of 37 items were incorporated into the factor analysis. Data from 63 to 68 participants could be analyzed for this purpose because some respondents did not answer some questions. In the course of the repeated calculation, items that loaded higher on more than one factor were identified and excluded. By excluding nine items for the reason just mentioned, 26 items were finally identified that showed a loading of >0.5 and clearly loaded on one of the eight factors. By the described procedure, the 12 UTAUT items (Teo, 2009, 2010) could be confirmed as well as 14 items could be identified which addressed the four additionally included constructs (see Table 6).
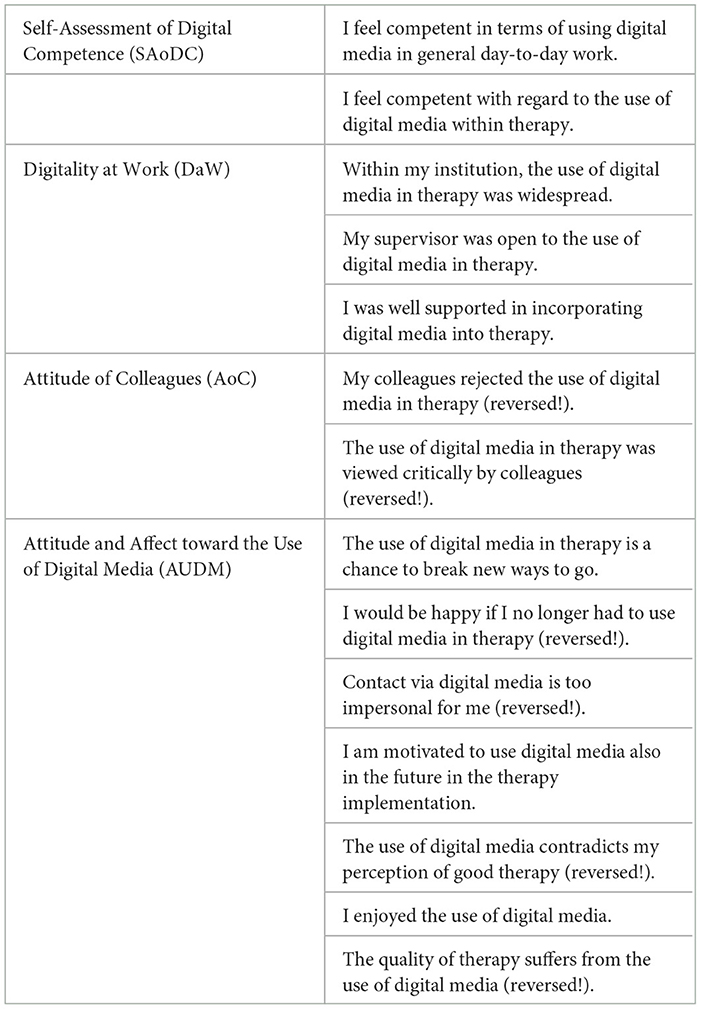
Table 6. Items used for the four additional influence variables in Study 2.
Internal consistency was also checked for these individual scales: SAoDC α = 0.851; DaW α = 0.818; AoC α =0.841; AUDM α =0.918. These constructs also showed a high value in terms of internal consistency.
All calculations were performed with the program SPSS program version 26 (IBM Corp, 2019).
To examine technology acceptance in the form of Behavioral Intention to Use (BIU) among therapists, the calculations and considerations of the mean and dispersion measures of the single variables of UTAUT and the new constructs were performed.
To answer the second question, the respective items of the variables were summarized using their mean values as in other studies on the UTAUT. The recommendations in using the averaged values of Likert scales as interval scaled data were fulfilled (Harpe, 2015). For age and work experience, the response values of the respondents were used (age in years, work experience in years). Multiple linear regressions in a three-block hierarchy (forced entry) were used to test the influence of the different independent variables on BIU. All assumptions for the analysis were fulfilled, including multicollinearity, heteroscedasticity, or nonlinearity (see Results). In order to take into account the possible influence of the variables age and work experience, these were also included in the regression calculations. Due to the low participation of males (n = 4), the gender factor could not be examined.
In a first step, the correlations between all individual variables included were checked. The variable Attitude of Colleagues (AoC) was then excluded from further calculations as it did not show any correlations with the dependent variable BIU or the other predictors.
In the first block of the multiple linear regression, age and work experience (WE) were included in the model. In the second block of the regression, the established predictors of the UTAUT—PE, EE, SI and FC—were included to check the basic model. In the last step, the UTAUT modification variables AUDM, SAoDC and DaW were added. For 12 of the 79 respondents not all values were available, because at the time of the survey they were not undergoing any therapies and therefore certain data were not feasible (n = 11) or there were missing values in a part of the included items (n = 1). Thus, the data of 67 persons could be used for this analysis. Since collinearity between the predictors Performance Expectancy (PE) and Attitude and Affect toward the Use of Digital Media (AUDM) was found in the last model, AUDM was excluded in a new model calculation to avoid distortions of the model.
In the final step, the same statistical procedure was followed as just mentioned, excluding the variable AUDM.
Numerous factors were initially identified by SPSS due to having eigenvalues < 1; however, after examining the Scree Plot of Eigenvalues table (see Supplementary material), it was decided that the first four were legitimate factors and all factors thereafter were the beginning of the tail and could be discarded. Thus, four factors were identified in the questionnaire, accounting for 21.7% of variance in the data. Each factor is independent of all others, as demonstrated by the low correlation scores in the Factor Correlation Matrix (see Table 7).
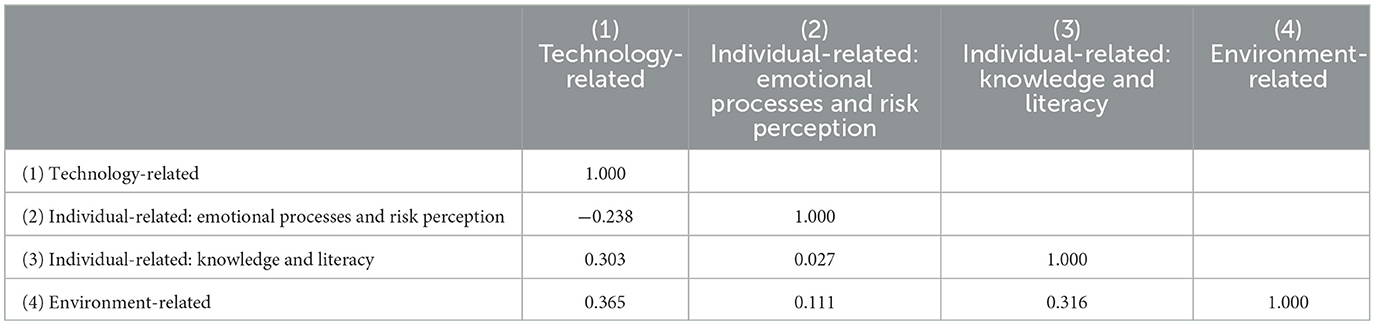
Table 7. Factor correlation matrix (Study 1).
As mentioned above, it was not possible to conduct a multiple regression analysis as planned, due to the significant deviations from normality of the independent variable, which therefore violated the assumptions necessary for multiple regression. An ordinal logistic regression was therefore conducted. Significance was determined at the standard p < 0.05.
The −2 Log Likelihood model was significantly significant (χ2 = 447.775, df = 89, p < 0.001), indicating that the full model was a significant improvement in the predictive capacity of the full model over the intercept only model. Similarly, both the Pearson (χ2 = 4,469.677, df = 6971, p = 1.00) and Deviance (χ2 = 1,107.218, df = 6,971, p = 1.00). Goodness of Fit tests indicated that the model was a good fit for the data.
a. What factors correlate with the prospective adoption of video therapy by speech and language therapists?
The regression results indicate a variety of factors which correlate with the adoption of video therapy in the future. Overall, 14 items contributed significantly to the model—see Table 8 for details. Among these items, increased difficulty in any category was associated with a reduced likelihood of a higher adoption score. Technical difficulties [−0.583, Wald χ2 (1) = 4.947, p = 0.026], a lack of training [−1.594, Wald χ2 (1) = 6.916, p = 0.009], a lack of prior experience [−0.849, Wald χ2 (1) = 4.784, p = 0.029] and a perceived limitation of methods [−0.811, Wald χ2 (1) = 4.846, p = 0.028] all significantly reduced a respondent's opinion of video therapy. Comparatively, perceived benefits like health protection of patients [1.461, Wald χ2 (1) = 14.533, p < 0.001], increased range of therapy options [1.406, Wald χ2 (1) = 26.750, p < 0.001], and new skill acquisition [0.655, Wald χ2 (1) = 6.823, p = 0.009] all significantly increased a respondent's opinion about video therapy.

Table 8. Significant response items identified for video therapy adoption in Study 1.
Time was variously positive and negative. A reported perception of increased preparation time [0.978, Wald χ2 (1) = 7.873, p = 0.005] actually improved respondent opinion, as did the reduced travel time for patients [0.557, Wald χ2 (1) = 3.391, p = 0.047]; however, high follow-up time [−0.916, Wald χ2 (1) = 5.982, p = 0.014] reduced respondent opinion.
Motivation also seemed to influence respondent opinions—respondents with increased motivation [0.756, Wald χ2 (1) = 5.025, p = 0.025] reported higher opinions, however those who sought professional help to fix technical problems time [−0.841, Wald χ2 (1) = 5.020, p = 0.025] and those who gave up on video therapy when faced with technical problems time [−1.268, Wald χ2 (1) = 4.837, p = 0.028] had a reduced opinion of video therapy.
b. What constructs underlie the attitudes of users toward technology acceptance and technology competence in the context of SLT?
Based on the rotation matrix produced during the factor analysis, the items either loaded uniquely on one of the four factors identified or did not load on any of the four primary factors, with one exception where one item loaded on two factors. All questions contained at least one item that contributed to a factor. Based on the items that contributed to each factor, the four factors were identified as “technology”, “emotional processes”, “knowledge” and “environment”. How these factors relate to previous research will be addressed in the discussion. See Table 9 for a list of which questions contributed to which factors.

Table 9. Rotation matrix to the factor analysis of 14 question items in Study 1.
c. To what extent are speech and language therapists intending to use ICT in therapy in the future?
With regard to the acceptance of the use of digital media within therapy, a heterogeneous picture emerged among the German therapists. The Behavioral Intention to Use (BIU) scores ranged from 0.5 to the maximum achievable 4 points. The average for the entire group is 2.92 (SD = 0.895), which is within the range of “mostly applies” on the Likert scale used.
All predictors showed average values between 2 and around 3. This corresponds to values between the answer options “undecided” and “mostly applies”. The predictors also showed a large dispersion across the sample and thus very different expressions in the individual therapists. The lowest mean value was achieved by the predictor Facilitation Conditions (FC) (M = 2.03, SD = 1.14), the highest mean value was shown by Digitality at Work (DaW) (M = 3.09; SD = 1.08) (see Table 10).
d. To what extent do Performance Expectancy (PE), Effort Expectancy (EE), Social Influence (SI), and Facilitating Conditions (FC), as well as additional factors, predict speech and language therapists' Behavioral Intention to Use (BIU) digital media in therapy?
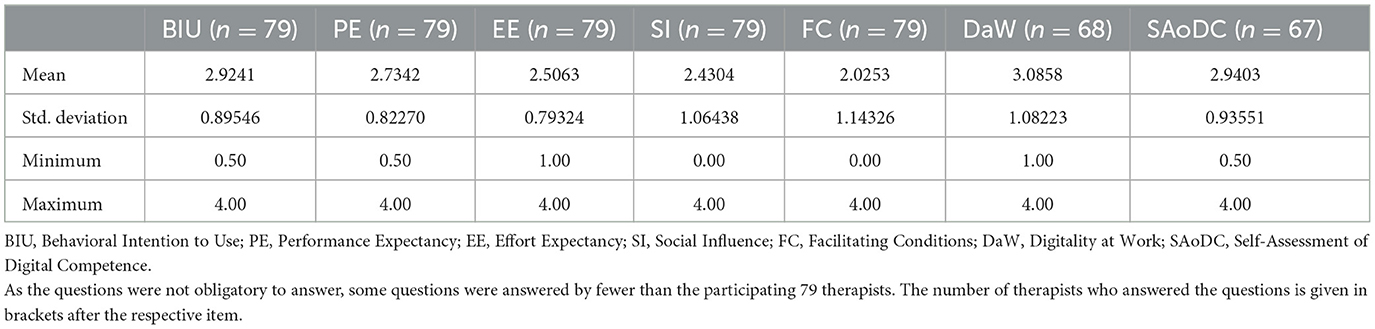
Table 10. Descriptive measures of the variables included (Study 2).
In terms of the included moderator variables of age and work experience (WE), there were isolated significant correlations found. Age correlated significantly with work experience (WE), Behavioral Intention to Use (BIU), Performance Expectamcy (PE) and Effort Expectancy (EE), while WE also correlated significantly with EE. All correlations are shown in Table 11.

Table 11. Correlations between the included variables (Study 2).
Model 3, which included all of the variables, explains 58.8% of the variability. The elucidation of variability was increased by including the variables Digitality at Work (DaW) and Self-Assessment of Digital Competencies (SAoDC) into the UTAUT-model but not significantly. Table 12 provides an overview of the multiple linear regression results.

Table 12. Results of the multiple linear regression (Study 2).
The generalizability of the models is given. The F-statistic shows highly significant values (p < 0.001) for model 2 as well as model 3, so both models (basic UTAUT and extended UTAUT) predict BIU significantly.
Table 13 shows the regression coefficients of model 3 (extended UTAUT).
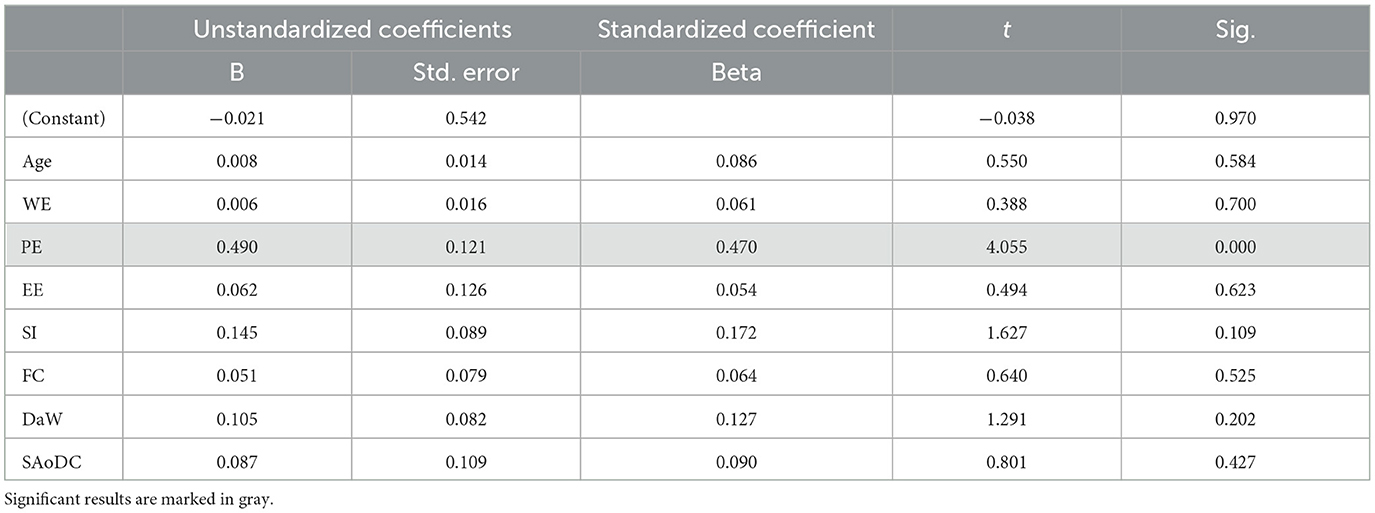
Table 13. Linear model of the predictors of BIU (Model 3; Study 2).
Performance Expectancy (PE) is a significant predictor of Behavioral Intention to Use (BIU) in German speech language therapists. There was no evidence of multicollinearity, heteroscedasticity, or nonlinearity. In addition, no case had an excessive influence on the model and the normal distribution of the residuals was given.
Study 1 aimed to investigate the use and success of video therapy in German Speech Language Therapy (SLT), based on the technology adoption approach outlined by Hastall et al. (2017). Therefore, the study investigated possible correlations and influences on the prospective attitudes of speech and language therapists toward video therapy as identified via preselected questionnaire items. The significant results included items related to perceived benefits, time and motivation as being impactful to the respondents and therefore for the successful adoption of video therapy in the context of SLT. These factors can have both inhibiting and facilitating outcomes in the adoption and future use of video therapy in SLT, which has also been demonstrated in numerous previous studies (Bilda et al., 2020; Lauer, 2020; Schwinn et al., 2020; Tenforde et al., 2020; Barthel et al., 2021a,b; Eslami Jahromi et al., 2022; Shahouzaie and Gholamiyan Arefi, 2022; Bayati and Ayatollahi, 2023).
Hastall et al. (2017), for example, argued that attention to human-driven factors can promote the adoption of technology—that is, video therapy adoption in SLT in the context of this study. Focusing on the three dimensions of relevant influences from Hastall et al. (2017): (1) individual-related factors, (2) environment-related factors, and (3) technology-related factors provided a good framework for investigating video therapy as an innovative digital medium in German SLT. However, the current analysis identified four factors from among the significant questionnaire items: technology (Factor 1), emotional processes (Factor 2), knowledge (Factor 3) and environment (Factor 4). Following the approach by Hastall et al. (2017) those four factors can give an idea of which human and technology driven factors could impact the use of video therapy. All significant items had at least a moderate impact on the outcome variable here, implying that all four factors are relevant for a successfully implemented adoption of video therapy technology.
With relation to the technology-related factors (Factor 1), therapists indicated the disadvantages of video therapy by the perception of negative aspects. Aspects of time, such as “follow-up time” and “preparation time”, are factors that could inhibit the use of video therapy in SLT. This is in line with the literature investigating advantages and disadvantages for the implementation of video therapy in Germany (Bilda et al., 2020; Lauer, 2020; Schwinn et al., 2020; Mörsdorf and Beushausen, 2021; Hecht et al., 2022) as well as in line with international studies (Tenforde et al., 2020; Shahouzaie and Gholamiyan Arefi, 2022; Bayati and Ayatollahi, 2023).
In contrast, the advantages of video therapy were more driven by emotional processes (Factor 2), which compare with the individual-related factors in Hastall et al. (2017). Positive aspects such as travel time, therapy and health protection are in line with the literature and can facilitate the prospective use of video therapy (Lauer, 2020; Schwinn et al., 2020). Following the approach of Hastall et al. (2017) human behavior is driven by emotions in the context of digital media use in health care. More specifically, emotions can play a critically role when being confronted with health vs. sickness (Hastall et al., 2017). In the case of video therapy, the context of health protection seems to be a relevant factor for implementation and was especially relevant during the COVID-19 pandemic (Barthel et al., 2021a,b).
Items related to knowledge (Factor 3) about video therapy seem to stem from negative feelings like insufficiency in knowledge and training. Those who report insufficient training in video therapy or software systems as well as a lack of previous experience in their implementation are more likely to report a low future intention to adopt video therapy. Hastall et al. (2017) emphasized that this factor is not only the missing technology-related foreknowledge but also the access to information about health technology, even of the existence and range of available options. They summarized that not only is appropriate knowledge, experience, and user competences needed in health-related ICT, but likely also knowledge about effective motivating education strategies (Hastall et al., 2017). Both emotional processes and knowledge factors (2 and 3) are highly individual-related and support the technology acceptance literature more broadly (Hastall et al., 2017), with supportive behavior and avoidance behavior combining to influence an individual's attitude.
Factor 4 included items based on environment-related factors, in particular the barriers preventing video therapy adoption that stem from geographical factors. Literature has constantly noted that challenges to video therapy adoption in Germany often include technical difficulties, such as unstable internet connections, service availability or continuity problems (Bilda et al., 2020; Lauer, 2020; Schwinn et al., 2020). Unsurprisingly, an unstable internet connection or intermittent connection failure can make video therapy difficult or even impossible. In many speech and language therapy sessions, high transmission quality is crucial, as the assessment of linguistic or facial aspects can only be accurate with good image and sound quality.
The four presented factors, when taken together, can help to inform those who wish to implement video therapy successfully. Firstly, parties who wish to implement video therapy as a regular and reliable healthcare service should aim to maximize adoption-facilitating conditions, like the personal and emotional benefits to patients and therapists; simultaneously they should aim to minimize rejection-facilitating conditions (Wade et al., 2014), for example by supplementing individual experience with quality training and by supporting therapists in their time investment. All of this requires substantial knowledge about the patients and therapists to bring together.
Study 2 investigated factors influencing the therapists' intention to use digital media in SLT in the future. The results show that German therapists are mostly willing to use ICT in therapy in the future. However, there was a certain heterogeneity within the sample. Thus, while many definitely want to use digital media in the future, there is also a significant minority who does not. Speech language therapists who show little or no interest in using digital media in therapy cannot seriously fulfill their mandate to provide digital participation for patients for whom digitalization is important to their lives (Steiner, 2023).
Of the individual factors, Digitality at Work (DaW) showed the highest mean value. This can be explained by the video therapies performed during the COVID-19 pandemic. These were temporarily the only possibilities to offer therapy for many patients and were therefore integrated in most practices. At the same time, however, there was a lack of support systems, as shown by Facilitating Conditions' (FC) low average score. This is consistent with the results of the first study.
For the purpose of identifying the impact of different influencing factors, six possible influencing factors (four original UTAUT and two supplementary) were included in the full analysis of study 2 along with age and work experience (WE). Age correlated significantly with WE, Behavioral Intention to Use (BIU), Performance Expectancy (PE) and Effort Expectancy (EE), while WE correlated significantly with age and EE. The correlation between age and WE is not surprising, as older speech and language therapists typically have more WE than younger therapists. Beyond this effect, there appears to be an interaction effect of age and WE in parts of the model.
In their meta-analysis, Dwivedi et al. (2019) were able to demonstrate a direct influence of attitude on BIU. Moreover, they found that attitude partially mediated the effects of all UTAUT-predictors on behavioral intention as well. This fits with the overlap, found in this research, between PE and Attitude and Affect toward Use of Digital Media (AUDM). This evidence supports the inclusion of attitude as a mediator in future studies.
While all the results demonstrated a significant relationship between Behavioral Intention to Use (BIU) and all of the checked factors, Performance Expectancy (PE) showed significant and distinct influence in the present study. PE also represented the highest influencing factor on BIU. This suggests that, in their opinions on ICT in therapy, speech therapists are most impacted by the perceived performance outcomes from utilizing that technology. These results match results from past studies (e.g., Venkatesh et al., 2003; Teo and Noyes, 2014). If speech language therapists consider the use of digital media as beneficial for their work, the intention to use digital media in the future increases.
Social influence (SI) on BIU has also been highlighted previously, particularly among women (Morris and Venkatesh, 2000; Teo and Noyes, 2014). Given the very high proportion of female therapists, both in this study and in the field in general, this factor should not be underrated; however, due to this high ratio among the respondents, this study could not isolate the SI effect from the sex effect. The included variables Self-Assessment of Digital Competencies (SAoDC) and Digitality at Work (DaW) could additionally improve the prediction of BIU in the model. However, a significant direct influence on the BIU could not be proven for the present sample.
The results of both studies show parallels. Influencing factors demonstrated for technology use in general (Study 2) can also be shown in the specific area of video therapy use (Study 1). Study 1 provides specific evidence regarding which factors increase acceptance of video therapy among speech and language therapists. Respondents indicated advantages in terms of Performance Expectancy (PE), disadvantages in terms of Effort Expectancy (EE), training (SAoDC, FC), and experience (DaW) as supporting and negative influencing factors, respectively. These determinants are also found in the UTAUT and were surveyed in Study 2 for general media use in therapy. The parallels noted are not surprising, as both studies looked at technology acceptance of speech and language therapists (see Figure 2).
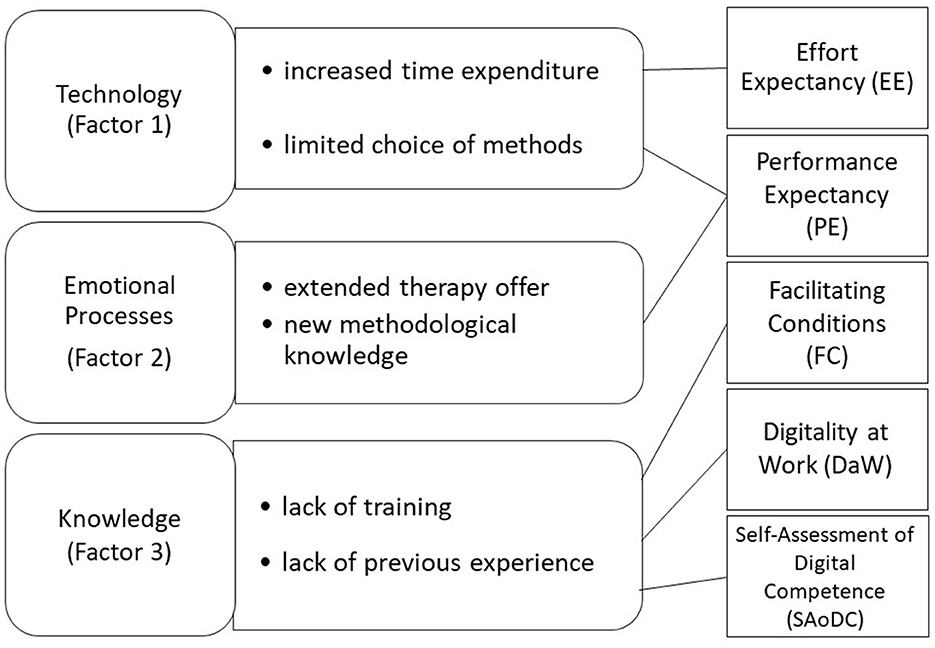
Figure 2. Comparable constructs of both studies underlying the attitudes of users toward technology acceptance and technology competence in the context of SLT.
Across the two studies, one of the biggest factors influencing future ICT adoption was support—especially in the form of education and training. A lack of training and experience can lead to frustration with the technology (De Joode et al., 2012; Liu et al., 2015; Gagnon et al., 2016), while an increase in troubleshooting knowledge and experience can improve satisfaction (Tucker, 2012). Professionals themselves have frequently highlighted the importance they place on training and the availability of support (Hill and Breslin, 2016; Burke et al., 2022; Kearns and Kelly, 2022). This highlights the importance of education in the industry going forward.
This change in education is multifaceted. With regards to the education of new practitioners, there is a need to integrate both theory-based content and practical digital skills in the curricula (Edwards and Dukhovny, 2017; European Health Parliament, 2020). In the spirit of lifelong learning, other training concepts should be tailored to suit currently active therapists—to expand their digital skills in a professional context and to implement them in their everyday practice (Lin et al., 2021). These are essential prerequisites to be able to advance professionalization in speech therapy in line with current developments (Theodoros, 2012). The implementation of the aforementioned content and factors faces the additional challenge in Germany that there are different training paths (e.g., vocational school vs. university) and professional groups (e.g., speech language therapists or academic speech therapists). Therefore, the authors provide concrete factors to consider and ideas for implementation that can be applied in all education and training contexts of speech language therapy.
From one perspective, therapists must have specific digital competencies in order to responsibly and meaningfully incorporate ICT into therapy. For example, the suitability and adaptation of programs must be tailored to the individual patient, their embedding must be planned and implemented in a goal-oriented manner, and their use must be continuously reflected upon and subsequently evaluated (Brennan et al., 2010; Alber et al., 2020; Alber and Starke, 2021a; Wirths et al., 2022). Further education and training should also focus on dealing with questions on Performance Expectancy (PE), as this could promote a positive Behavioral Intention to Use (BIU). Therapists should receive information and gain experience in this context, which would show them how ICT can improve and support the fulfillment of individual tasks in therapeutic work. This includes, among other things, focusing on the benefits and opportunities that the technology can bring to the therapy situation itself. To ensure that the technologies being taught, including video therapy, will be meaningfully incorporated into the therapists' repertoires, educators should focus in particular on the deeper functional aspects with a high proportion of practical exercises.
Besides the consideration of PE, educators should be aware of the importance of Social Influence (SI), as the valued opinions of other respected individuals have an impact, often serving as role models of technology use. These role models can include other students or educators in SLT-training (Teo and Noyes, 2014). Digitally supported didactics should be practiced and play an essential role in case management in the area of context assessment, goal setting, therapy planning and implementation, and evaluation and modification (Steiner, 2023). Possible approaches could include the use of case studies or therapy videos in which the use of ICT is exemplified, collegial case consultations with a focus on ICT-supported therapy, or problem-based learning, which brings the use of ICT into the trainees' focus. Additionally, education and training could include formats for exchange between speech and language therapists, e.g. through videoconferencing. In this way, positive experiences can be shared with peers, awareness can be raised and people can also benefit from the experiences of others.
By trying out digital media independently in a protected setting, the expectation of effort can be lowered and the therapists' self-efficacy of dealing with technology can be experienced. Thus, technology acceptance can be promoted within the consideration of both Effort Expectancy (EE) and Self-Assessment of Digital Competence (SAoDC). Practical exercises in video therapy could thus reduce inhibiting factors for video therapy in the area of technology, as well as knowledge and skills. Appropriate training and educational content must first be specifically designed, piloted, made easily accessible, and continually updated. To further support EE and reduce inhibiting factors at the emotional and knowledge levels, it may be useful to focus on therapy-relevant programs and devices and to use applications with easy-to-use interfaces that hide the complexity of the hardware and software. These considerations should also be taken into account when developing specific software for use in therapeutic settings (Teo and Noyes, 2014).
Beyond education, Facilitating Conditions (FC) and Digitality at Work (DaW) are factors that need to be supported more on a structural level. The development and expansion of support systems for the use of digital media in general, and for video therapy in particular, in everyday speech therapy is a challenge. On a structural level, the possibility of billing for video therapies introduced in Germany during the COVID-19 pandemic led to an improvement in the conditions for the use of digital media (Bilda et al., 2020). However, the therapeutic use of video therapies was an uncertain factor during this period; one that was allowed for a certain period of time with a couple of extensions and therefore inhibited the further development of sustainable hybrid (face-to-face therapy in combination with video therapy) or virtual (full video therapy) telepractice offerings (Lauer, 2020). Since September, 2022, video therapy is again possible in Germany due to a transitional arrangement, but it is still not implemented in the regular speech and language therapy service. In line with the literature, unstable reimbursement policies by insurance companies present a barrier to teletherapy implementation (Rettinger et al., 2021). The challenge of purchasing and maintaining suitable hardware and software is also financial. Until now, these costs have been shouldered predominantly by the practices themselves or the individual therapists.
The provision of paid working time for ICT familiarization and implementation is thus another facet of FC. In Germany, speech therapists are paid individually by health insurance companies for each hour of therapy provided. The level of remuneration is also low. Further education and training, as well as familiarization with new technologies is usually voluntary, so that a high level of motivation and personal commitment appears necessary to advance digitalization in a professional context (Hilbert and Paulus, 2018), because the introduction of ICT is often time-consuming, even though the use of ICT can save time in the long run (Gagnon et al., 2016; Burke et al., 2022).
In addition to FC and DaW, other structural factors can also have an impact. The lack of widespread, reliable availability of high-speed Internet can influence the use of digital media in SLT negatively (Schwinn et al., 2020). However, this will not be presented in more detail here, as it was not specifically investigated in the studies presented. Similarly, previous papers (e.g., Alber and Starke, 2021b) found that although German speech and language therapists increased their use of digital technology during the COVID-19 pandemic, this was largely concentrated in the use of video therapy; the use of apps or educational software in therapy did not significantly change over the COVID-19 pandemic period. These factors could be considered in future investigations.
Maximizing facilitation triggers and reducing inhibiting conditions should be the intention, for an optimal health service delivery to patients. A better digital participation for patients is only possible if technology acceptance in speech and language therapists increases by the described possibilities of individual-related, social and environment-related as well as technology-related factors and therefore allows a satisfying health technology adoption in SLT.
The results of both studies presented here are based on an online survey of therapists. The samples were obtained from SLT professionals working in outpatient settings in Germany, so it was consciously accepted that therapists working in other contexts, like hospitals or non-German therapists, would be excluded. In addition, both studies used an online questionnaire for the survey, which means that it cannot be ruled out that therapists were more likely to participate who had a minimum level of affinity for and competence in technology. Accordingly, a certain bias in the results cannot be discounted. Due to the pandemic situation and the associated restrictions at the time of the studies, a different procedure was not possible.
The results of Study 1 demonstrated facilitating and inhibiting factors for video therapy adoption based on a high number of participants. However, on a structural level, data did not allow for a more acute examination due to failing certain statistical assumptions, which means that a more precise relationship between the constructs cannot be defined, only trends. Additionally, due to the large test size and breadth of analysis, the cumulative variance accounted for by the factor analysis was low. A follow-up study with fewer but more precisely keyed questions would help. Regarding the interpretation, the results were not as highly interrelated as other literature (e.g., Hastall et al., 2017). This could be due to the methodological limitations, or due to the structure of the questionnaire questions selected, but this limits the connections that can be drawn with the three factors (individual-related, environment-related and technology-related factors) derived from the technology adoption approach of other models.
The generalizability of results of Study 2 is not given due to the sample size. Structural equation modeling was also not possible due to the limited sample size. The moderating variables “age” and “work experience” of the original UTAUT model were therefore included as predictor variables to take their influence into account. The uneven distribution of respondents with regard to gender did not allow this factor to be considered. However, the proportion of male respondents is not surprising, as more than 90% of speech and language therapists in Germany are female (Gesundheitsberichterstattung des Bundes., 2022). Because of the occasional proven correlations between age/work experience and other variables there seems to be moderating effects in parts of the model. These effects should be investigated in more detail in future studies.
Due to statistical evidence, two additional factors derived from theory had to be excluded from the final analysis (Attitude of Colleagues and Attitude and Affect toward the Use of Digital Media). This was the only way to ensure a methodologically adequate procedure.
Despite the limitations mentioned above, it was possible to obtain initial indications regarding the technology acceptance among SLT professionals in Germany, which can be used for future studies in this area. First hints for possible supporting factors emerge, which can be applied for practice and planning of further education and training.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
This study was approved by the committee for research ethics of the University of Applied Sciences and Arts (HAWK) Hildesheim/Holzminden/Göttingen. On the first page of the online-survey, all participants were informed about the study contents and data privacy and gave their informed consent. No data was collected without prior consent. Likewise, all participants of Study 2 were informed about the study content and data privacy on the first page of the online-survey and gave their informed consent. The survey itself and its evaluation were anonymous, and it was not possible to draw conclusions about the respondents at any time during the survey or the evaluation.
JL, MB, BB, and SW designed Study 1. MB, JL, and SW oversaw data collection. MB and AW performed the statistical analysis from Study 1. BA and AS designed Study 2 and oversaw data collection. BA performed the statistical analysis from Study 2. All authors contributed to writing the manuscript, read, and approved the submitted version.
Grant support for the Study 1 was received from the German Federal Association of Speech and Language Therapy (Deutscher Bundesverband für Logopädie e.V.) for research to SW.
We would like to thank the therapists who gave their time to respond to the questionnaires and Nele Vöcks and Judith Krämer for preparing data analysis of Study 1.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcomm.2023.1176827/full#supplementary-material
Alber, B., and Starke, A. (2021a). Digitale Kompetenzen von Sprachtherapeut*innen - Therapieren (DiKoST-T). Forschung Sprache 9, 3–11.
Alber, B., and Starke, A. (2021b). “Einsatz digitaler Medien in der Sprachtherapie vor und während der Pandemiebeschränkungen,” in Poster at the 22nd Scientific Symposium of the German Federal Association for Academic Speech and Language Therapy (Frankfurt: Deutscher Bundesverband für akademische Sprachtherapie und Logopädie, dbs).
Alber, B., Starke, A., Griffel, J., and Leinweber, J. (2020). Qualität von Apps in der Logopädie/Sprachtherapie. Der Bewertungskatalog für Apps in Sprachtherapie und Sprachförderung (BAS). Forum Logopädie 34, 12–13.
Albudoor, N., and Pena, E. D. (2021). Factors influencing US speech and language therapists' use of technology for clinical practice. Int. J. Lang. Commun. Disord. 56, 567–582. doi: 10.1111/1460-6984.12614
Barthel, M., Schwinn, S., Borgetto, B., and Leinweber, J. (2021a). Digitalisierungschancen - Spurensuche nach Evidenz. Ergebnisse der Videointeraktionsanalyse aus dem Forschungsprojekt “ViTaL”. Forum Logopädie 35, 34–39.
Barthel, M., Wittmar, S., Einfeldt, A.-K., and Borgetto, B. (2021b). Digitalisierungschancen nutzen! Kernaussagen und Empfehlungen für die Nutzung von Videotherapien in der ambulanten logopädischen/sprachtherapeutischen Versorgung (Kurzfassung). Forum Logopädie 35, 49–50.
Bayati, B., and Ayatollahi, H. (2023). Speech therapists' perspectives about using tele-speech therapy: a qualitative study. Disabil. Rehabil. 18, 621–626. doi: 10.1080/17483107.2021.1900933
Beaudry, A., and Pinsonneault, A. (2005). Understanding user responses to information technology: a coping model of user adaption. MIS Quart. 29, 493–525. doi: 10.2307/25148693
Beushausen, U., and Sippel, S. (2021). Videotherapie vs. Präsenztherapie in der Stimmfunktionstherapie: Klinische RCT-Studie zum Vergleich der Wirksamkeit. Forum Logopädie 35, 12–15.
Bilda, K., Dörr, F., Urban, K., and Tschuschke, B. (2020). Digitale logopädische Therapie. Ergebnisse einer Befragung zum aktuellen Ist-Stand aus der Sicht von logopädische. Logos 28, 13–20.
Birch, A., and Irvine, V. (2009). Preservice teachers acceptance of ICT integration in the classroom: applying the UTAUT model. Educ. Media Int. 46, 295–315. doi: 10.1080/09523980903387506
Böhm, S. (2019). Logopädie 4.0 - Therapeutische Hausaufgaben mit dem Tablet: Assistive digitale Systeme sind im Kommen - das Beispiel SpeechCare. Forum Logopädie 33, 6–9.
Boudreau, M., and Robey, D. (2005). Enacting integrated information technology: A human agency perspective. Organizat. Sci. 16, 3–18. doi: 10.1287/orsc.1040.0103
Brennan, D., Tindall, L., Theodoros, D., Brown, J., Campbell, M., Christiana, D., et al. (2010). A Blueprint for telerehabilitation guidelines. Int. J. Telerehabilitat. 2, 31–34. doi: 10.5195/ijt.2010.6063
Buabbas, A. J., Albahrouh, S. E., Alrowayeh, H. N., and Alshawaf, H. (2022). Telerehabilitation during the COVID-19 pandemic: patients and Physical Therapists' Experiences. Medical principles and practice. Int. J. Kuwait University, Health Sci. Centre 31, 156–164. doi: 10.1159/000523775
Burke, J., Palmer, R., and Harrison, M. (2022). What are the factors that may influence the implementation of self-managed computer therapy for people with long term aphasia following stroke? A qualitative study of speech and language therapists' experiences in the Big CACTUS trial. Disabil. Rehabil. 44, 3577–3589. doi: 10.1080/09638288.2020.1871519
Bürkle, L., Collasius, V., Djuric, A., Hecht, A., Krämer, J., Kraus, C., et al. (2021). PatientInnen-Zufriedenheit mit der Videotherapie bei Sprach-, Sprech- und Stimmstörungen während der COVID-19-Pandemie - Eine Zwischenbilanz der Studie PaZu-Video. Forum Logopädie 35, 16–19.
Cason, J. (2009). A pilot telerehabilitation program: delivering early intervention services to rural families. Int. J. Telerehabilitat. 1, 29–38. doi: 10.5195/ijt.2009.6007
Compeau, D. R., and Higgins, C. A. (1995). Computer self-efficacy: Development of a measure and initial test. MIS Quart. 19, 189–211. doi: 10.2307/249688
Compeau, D. R., Higgins, C. A., and Huff, S. (1999). Social cognitive theory and individual reactions to computing technology: a longitudinal study. MIS Quart. 23, 145–158. doi: 10.2307/249749
Cortina, J. M. (1993). What is coefficient alpha? An examination of theory and applications. J. Appl. Psychol. 78, 98–104. doi: 10.1037/0021-9010.78.1.98
Davis, F. D., Bagozzi, R. P., and Warshaw, P. R. (1989). User acceptance of computer technology: a comparison of two theoretical models. Manage. Sci. 35, 982–1002. doi: 10.1287/mnsc.35.8.982
Davis, F. D., Bagozzi, R. P., and Warshaw, P. R. (1992). Extrinsic and intrinsic motivation to use computers in the workplace. J. Appl. Soc. Psychol. 22, 1111–1132. doi: 10.1111/j.1559-1816.1992.tb00945.x
De Joode, E. A., van Boxtel, M. P. J., Verhey, F. R., and van Heugten, C. M. (2012). Use of assistive technology in cognitive rehabilitation: exploratory studies of the opinions and expectations of healthcare professionals and potential users. Brain Injury 26, 1257–1266. doi: 10.3109/02699052.2012.667590
Dwivedi, Y. K., Rana, N. P., Jeyaraj, A., and Clement, M. (2019). Re-examining the unified theory of acceptance and use of technology (UTAUT): towards a revised theoretical model. Informat. Syst. Front. 21, 719–734. doi: 10.1007/s10796-017-9774-y
Edwards, J., and Dukhovny, E. (2017). Technology training in speech-language pathology: a focus on tablets and apps. Persp. ASHA Special Interest Groups 2, 33–48. doi: 10.1044/persp2.SIG10.33
El-Gayar, O. F., Wills, M., and Bennett, D. (2008). Examining healthcare professionals' acceptance of electronic medical records using UTAUT. Issues in Inform. Syst. IX, 396–401.
Eslami Jahromi, M., Farokhzadian, J., and Ahmadian, L. (2022). Two-sided perspective on tele-speech therapy: experiences of stuttering patients, and their parents. Assist. Technol. 34, 717–724. doi: 10.1080/10400435.2021.1937378
European Health Parliament (2020). Recommendations by the Next Generation. Available online at: https://www.healthparliament.eu/wp-content/uploads/2020/09/EHP_Recommendations_by_the_next_Generation.pdf (accessed June 22, 2023).
Fairweather, G. C., Lincoln, M. A., and Ramsden, R. (2016). Speech-language pathology teletherapy in rural and remote educational settings: decreasing service inequities. Int. J. Speech-Lang. Pathol. 18, 592–602. doi: 10.3109/17549507.2016.1143973
Fishbein, M., and Ajzen, I. (1975). Belief, Attitude, Intention and Behavior: An Introduction to Theory and Research. Reading, MA: Addison Wesley Pub.
Freckmann, A., Hines, M., and Lincoln, M. (2017). Clinicians' perspectives of therapeutic alliance in face-to-face and telepractice speech-language pathology sessions. Int. J. Speech-Lang. Pathol. 19, 287–296. doi: 10.1080/17549507.2017.1292547
Gačnik, M., Starčič, A. I., Zaletelj, J., and Zajc, M. (2018). User-centred app design for speech sound disorders interventions with tablet computers. Univ. Access in the Inform. Soc.y 17, 821–832. doi: 10.1007/s10209-017-0545-9
Gagnon, M.-P., Ngangue, P., Payne-Gagnon, J., and Desmartis, M. (2016). m-Health adoption by healthcare professionals: a systematic review. J. Am. Med. Inform. Assoc. 23, 212–220. doi: 10.1093/jamia/ocv052
Gesundheitsberichterstattung des Bundes. (2022). Gesundheitspersonal nach Geschlecht, Einrichtung, Beruf . Available online at: https://www.gbe-bund.de/gbe/!pkg_olap_tables.prc_set_orientation?p_uid=gastandp_aid=98491274andp_sprache=Dandp_help=2andp_indnr=89andp_ansnr=79577105andp_version=2andD.000=1andD.003=2andD.734=3andD.489=2 (accessed February 10, 2022).
Hall, N., Boisvert, M., and Steele, R. (2013). Telepractice in the assessment and treatment if individuals with aphasia: a systematic review. J. Telerehabilitat. 5, 27–38. doi: 10.5195/ijt.2013.6119
Harpe, S. E. (2015). How to analyze Likert and other rating scale data. Curr. Pharm. Teach. Learn. 7, 836–850. doi: 10.1016/j.cptl.2015.08.001
Hastall, M. R., Dockweiler, C., and Mühlhaus, J. (2017). “Achieving End User Acceptance: Building Blocks for an Evidence-Based User-Centered Framework for Health Technology Development and Assessment,” in Universal Access in Human-Computer Interaction. Human and Technological Environments, eds. M. Antona and C. Stephanidis (Cham: Springer International Publishing), 13–25. doi: 10.1007/978-3-319-58700-4_2
Hecht, A., Wargers, I., Leinweber, J., and Borgetto, B. (2022). “Videotherapie in der ambulanten logopädischen Versorgung – empirisch begründete Handlungsempfehlungen,” in 21. Deutscher Kongress für Versorgungsforschung (DKVF). Potsdam.
Hilbert, J., and Paulus, W. (2018). Logopädie zwischen Digitalisierung und Unterfinanzierung. Ein Bericht aus der Praxis. Forschung aktuell 8, 1–13.
Hill, A. J., and Breslin, H. M. (2016). Refining an asynchronous telerehabilitation platform for speech-language pathology: engaging end-users in the process. Front. Human Neurosci. 10, 640. doi: 10.3389/fnhum.2016.00640
Jakob, H., Görtz, K., and Späth, M. (2018). Evaluation des neuen Tablet-basierten Therapieverfahrens “neolexon”. Sprachtherapie aktuell: Forschung - Wissen – Transfer 7, 1–5.
Jesus, L. M., Santos, J., and Martinez, J. (2019). The table to tablet (T2T) speech and language therapy software development roadmap. JMIR Res. Prot. 8, e11596. doi: 10.2196/11596
Jockisch, M. (2010). “Das Technologieakzeptanzmodell,” in Das ist gar kein Modell!: Unterschiedliche Modelle und Modellierungen in Betriebswirtschaftlehre und Ingenieurswissenschaften, eds. G. Bandow and H. H. Holzmüller (Cham: Springer Gabler), 233–354.
Jung, S.-I., Lim, S., Jo, E., Sim, H. S., Sung, J. E., and Kim, Y. T. (2020). The efficacy of telepractice intervention for children and adolescents with speech, language and hearing impairments: a meta-analysis. Commun. Sci. Disord. 25, 976–986. doi: 10.12963/csd.20756
Kearns, Á., and Kelly, H. (2022). ICT usage in aphasia rehabilitation – beliefs, biases, and influencing factors from the perspectives of speech and language therapists. Aphasiology 37, 456–478. doi: 10.1080/02687038.2022.2030462
Khechine, H., Lakhal, S., Pascot, D., and Bytha, A. (2014). “To elluminate or not to elluminate? That is the question,” in Proceedings of the 5th International Conference on Education, Training and Informatics (ICETI 2014). Orlando, FL.
Kollmann, T. (1999). Das Konstrukt der Akzeptanz im Marketing. Wirtschaftswissenschaftliches Studium (WiSt) 3, 125–130.
Lakhal, S., Khechine, H., and Pascot, D. (2013). Student behavioural intentions to use desktop video conferencing in a distant course: integration of autonomy to the UTAUT model. J. Comp Higher Educ. 25, 93–121. doi: 10.1007/s12528-013-9069-3
Lauer, N. (2020). Teletherapie - hat die Logopädie eine digitale Zukunft? Ergebnisse eines qualitativen Forschungsprojekts des Studiengangs Logopädie der OTH Regensburg. Forum Logopädie 34, 12–17.
Leinweber, J., and Barthel, M. (2022). Digital Health-Leistungen als Motor einer verbesserten Gesundheitsversorgung. Sprache Stimme Gehör. 46, 19–27. doi: 10.1055/a-1706-8883
Leinweber, J., and Schulz, K. (2019). Digitalisierung in der Aphasietherapie - eine ethische Betrachtung. Aphasie und verwandte Gebiete 46, 34–41.
Lin, Y., Lemos, M., and Neuschaefer-Rube, C. (2021). Digital health and digital learning experiences across speech-language pathology, phoniatrics, and otolaryngology: interdisciplinary survey study. JMIR Med. Educ. 7, e30873. doi: 10.2196/30873
Liu, L., Cruz, A. M., Rincon, A. R., and Buttar, V. (2015). What factors determine therapists' acceptance of new technologies for rehabilitation – a study using the Unified Theory of Acceptance and Use of Technology (UTAUT). Disab. Rehabilitat. 37, 447–455. doi: 10.3109/09638288.2014.923529
McGill, M., Noureal, N., and Siegel, J. (2019). Telepractice treatment of stuttering: a systematic review. Telemed. J. E-health. 25, 359–368. doi: 10.1089/tmj.2017.0319
Millmann, Z., and Hartwick, J. (1987). The impact of automated office systems in middle managers and their work. MIS Quart. 11, 479–491. doi: 10.2307/248977
Molini-Avejonas, D. R., Rondon-Melo, S., La Amato, C. A., de, H., and Samelli, A. G. (2015). A systematic review of the use of telehealth in speech, language and hearing sciences. J. Telemed. Telecare 21, 367–376. doi: 10.1177/1357633X15583215
Morris, M. G., and Venkatesh, V. (2000). Age difference in technology adoption decisions: Implications for a changing workforce. Personell Psychol. 53, 375–403. doi: 10.1111/j.1744-6570.2000.tb00206.x
Mörsdorf, L., and Beushausen, U. (2021). Teletherapie und Telemedizin in Deutschland. Studienlage zur Wirksamkeit sprachtherapeutischer Teletherapie im neurologischen Bereich. Neurologie und Rehabilitation 27, 111–118. doi: 10.14624/NR2102004
Nichol, L., Pitt, R., Wallace, S. J., Rodriguez, A. D., and Hill, A. J. (2022). “There are endless areas that they can use it for”: speech-language pathologist perspectives of technology support for aphasia self-management. Disabil. Rehabilitat. Assist. Technol. 2, 1–16. doi: 10.1080/17483107.2022.2037758
Nordness, A. S., and Beukelmann, D. R. (2010). Speech practice patterns of childen with speech sound disorders: The impact of parental record keeping and computer-led practice. J. Med. Speech-Lang Pa. 18, 104–108.
Olszewski, A., Smith, E., and Franklin, A. D. (2022). Speech-Language Pathologists' Feelings and Practices Regarding Technological Apps in School Service Delivery. Lang. Speech Hear Servi. Schools 53, 1051–1073. doi: 10.1044/2022_LSHSS-21-00150
Oprandi, M. C., Bardoni, A., Corno, L., Marchetti Guerrini, A., Molatore, L., Negri, L., et al. (2021). Feasibility and acceptability of a real-time telerehabilitation intervention for children and young adults with acquired brain injury during the covid-19 pandemic: an experience report. Int. J. Telerehabilitat. 13, 1–25. doi: 10.5195/ijt.2021.6423
Orlikowski, W. J. (2000). Using technology and constituting structures: A practice lens for studying technology in organizations. Organizat. Sci. 11, 404–428. doi: 10.1287/orsc.11.4.404.14600
Pitt, R., Hill, A. J., Theodoros, D., and Russell, T. (2018). “I definitely think it's a feasible and worthwhile option”: perspectives of speech-language pathologists providing online aphasia group therapy. Aphasiology 32, 1031–1053. doi: 10.1080/02687038.2018.1482403
Preßler, L. (2019). PhonoLo: digitaler Begleiter durch die Phonologie-Therapie. Neue App unterstützt Therapie nach dem P.O.P.T.-Ansatz. Forum Logopädie 33, 10–13.
Rangarathnam, B., Gilroy, H., and McCullough, G. H. (2016). Do patients treated for voice therapy with telepractice show similar changes in voice outcome measures as patients treated face-to-face? EBP Briefs 11, 1–6.
Rettinger, L., Klupper, C., Werner, F., and Putz, P. (2021). Changing attitudes towards teletherapy in Austrian therapists during the COVID-19 pandemic. J. Telemed. Telecare 29, 406–414. doi: 10.1177/1357633X20986038
Schrepp, M. (2016). “Datenqualität bei Online-Fragebögen sicherstellen,” in Mensch und Computer 2016 – Usability Professionals, eds. S. Hess, and H. Fischer (Aachen).
Schwinn, S., Barthel, M., and Leinweber, J. (2020). Digitalisierungschancen – Umsetzung von Videotherapie im Lockdown. Ergebnisse der Online-Befragung aus dem Forschungsprojekt ViTaL”. Forum Logopädie 34, 36–40.
Scott Kruse, C., Karem, P., Shifflett, K., Vegi, L., Ravi, K., and Brooks, M. (2018). Evaluating barriers to adopting telemedicine worldwide: a systematic review. J. Telemed. Telecare 24, 4–12. doi: 10.1177/1357633X16674087
Shahouzaie, N., and Gholamiyan Arefi, M. (2022). Telehealth in speech and language therapy during the COVID-19 pandemic: a systematic review. Disabil. Rehabilitat. Assist. Technol. 2022, 1–8. doi: 10.1080/17483107.2022.2122605
Simon, B. (2001). “E-Learning an Hochschulen,” in Gestaltungsräume und Erfolgsfaktoren von Wissensmedien. Köln: Josef Eul Verlag.
Standing, C., Standing, S., McDermott, M.-L., Gururajan, R., and Kiani Mavi, R. (2016). The paradoxes of telehealth: a review of the literature 2000-2015. Syst. Res. 35, 90–101. doi: 10.1002/sres.2442
Starke, A., and Leinweber, J. (2019). Apps in der Sprachtherapie, in Unterstützte Kommunikation bei Kindern und Erwachsenen, eds. C. Lüke and S. Vock (Berlin: Springer), 221–35.
Steiner, J. (2023). Digitale Teilhabe als Auftrag in der Logopädie: Grundlegung, Begriffserklärungen und Befragung von Praktiker*innen. Forum Logopädie 37, 18−23.
Sutherland, R., Trembath, D., and Roberts, J. (2018). Telehealth and autism: A systematic search and review of the literature. Int. J. Speech-Lang. Pathol. 20, 324–336. doi: 10.1080/17549507.2018.1465123
Taylor, S., and Todd, P. A. (1995a). Assessing IT usage: the role of prior experience. MIS Quart. 19, 561–570. doi: 10.2307/249633
Taylor, S., and Todd, P. A. (1995b). Understanding information technology usage: a test of competing models. Inform. Syst. Res. 6, 144–176. doi: 10.1287/isre.6.2.144
Tenforde, A. S., Borgstrom, H., Polich, G., Steere, H., Davis, I. S., Cotton, K., et al. (2020). Outpatient physical, occupational, and speech therapy synchronous telemedicine: a survey study of patient satisfaction with virtual visits during the COVID-19 pandemic. Am. J. Phys. Med. Rehabil. 99, 977–981. doi: 10.1097/PHM.0000000000001571
Teo, T. (2009). Modelling technology acceptance in education: a study of pre-service teachers. Comp. Educ. 52, 302–312. doi: 10.1016/j.compedu.2008.08.006
Teo, T. (2010). A path analysis of pre-service teachers' attitudes to computer use: applying and extending the technology acceptance model in an educational context. Interact. Learn. Environm. 18, 65–79. doi: 10.1080/10494820802231327
Teo, T., and Noyes, J. (2014). Explaning the intention to use technology among pre-service teachers: a multi-group analysis of the Unified Theory of Acceptance and Use of Technology. Interact. Learn. Environm. 22, 51–66. doi: 10.1080/10494820.2011.641674
Theodoros, D. (2012). A new era in speech-language pathology practice: innovation and diversification. Int. J. Speech-Lang. Pathol. 14, 189–199. doi: 10.3109/17549507.2011.639390
Thompson, R. L., Higgins, C. A., and Howell, J. M. (1991). Personal computing: toward a conceptual model of utilization. MIS Quart. 15, 124–143. doi: 10.2307/249443
Tucker, J. K. (2012). Perspectives of speech-languagepathologists on the use of telepractice in schools: quantitative survey results. Int. J. Telerehabilitat. 4, 61–71. doi: 10.5195/ijt.2012.6100
Tyagi, S., Lim, D. S. Y., Ho, W. H. H., Koh, Y. Q., Cai, V., Koh, G. C. H., et al. (2018). Acceptance of tele-rehabilitation by stroke patients: perceived barriers and facilitators. Arch. Phys. Med. Rehabil. 99, 2472–2477.e2. doi: 10.1016/j.apmr.2018.04.033
Venkatesh, V., and Bala, H. (2008). Technology acceptance model 3 and a research agenda on interventions. Deci. Sci. 39, 273–315. doi: 10.1111/j.1540-5915.2008.00192.x
Venkatesh, V., and Davis, F. D. (2000). A theoretical extension of the technology acceptance model: four longitudinal field studies. Manage. Sci. 46, 186–204. doi: 10.1287/mnsc.46.2.186.11926
Venkatesh, V. J. Y. L, and Thong Xu, X. (2016). Unified theory of acceptance and use of technology: a synthesis and the road ahead. J. Assoc. Informat. Syst. 17, 328–376. doi: 10.17705/1jais.00428
Venkatesh, V., Morris, M. G., Davis, G. B., and Davis, F. D. (2003). User acceptance of information technology: towards a unified view. MIS Quart. 27, 425–478. doi: 10.2307/30036540
Wade, V. A., Eliott, J. A., and Hiller, J. E. (2014). Clinician acceptance is the key factor for sustainable telehealth services. Qual. Health Res. 24, 682–694. doi: 10.1177/1049732314528809
Wahl, M., Steiner, J., and Mühlhaus, J. (2018). “Neue Medien in der Sprachtherapie. Chancen für eine ressourenorientierte therapeutische Versorgung,” in Ressourcenorientierte Logopädie, ed. J. Steiner (Bern: Hogrefe), 161–72.
Wales, D., Skinner, L., and Hayman, M. (2017). The efficacy of telehealth-delivered speech and language intervention for primary school-age children: a systematic review. Int. J. Telerehabilitat. 9, 55–70. doi: 10.5195/ijt.2017.6219
Warshaw, P. R., and Davis, F. D. (1985). Disentangling behavioral intention and behavioral expectation. J. Exp. Social Psychol. 21, 213–228. doi: 10.1016/0022-1031(85)90017-4
Weidner, K., and Lowman, J. (2020). Telepractice for adult speech-language pathology services: a systematic review. Persp. ASHA Spec. Inter. Groups 5, 326–338. doi: 10.1044/2019_PERSP-19-00146
Welch, V., Petkovic, J., Pardo Pardo, J., Rader, T., and Tugwell, P. (2016). Interactive social media interventions promote health equity: an overview of reviews. Health Prom. Chronic Dis. Prevent. Canada 36, 63–75. doi: 10.24095/hpcdp.36.4.01
Williams, M. D., Rana, N. P., and Dwivedi, Y. K. (2014). The unified theory of acceptance and use of technology (UTAUT): a literature review. J. Enterp. Inform. Manage. 28, 443–488. doi: 10.1108/JEIM-09-2014-0088
Keywords: technology acceptance, technology adoption, technology use, digital media use, digital participation, speech and language therapy, video therapy, Unified Theory of Acceptance and Use of Technology
Citation: Leinweber J, Alber B, Barthel M, Whillier AS, Wittmar S, Borgetto B and Starke A (2023) Technology use in speech and language therapy: digital participation succeeds through acceptance and use of technology. Front. Commun. 8:1176827. doi: 10.3389/fcomm.2023.1176827
Received: 28 February 2023; Accepted: 27 September 2023;
Published: 24 October 2023.
Edited by:
Kristina Jonas, University of Cologne, GermanyReviewed by:
Michael Wahl, Humboldt University of Berlin, GermanyCopyright © 2023 Leinweber, Alber, Barthel, Whillier, Wittmar, Borgetto and Starke. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Juliane Leinweber, anVsaWFuZS5sZWlud2ViZXJAaGF3ay5kZQ==; Birte Alber, YmlydGUuYWxiZXJAdW5pLWJyZW1lbi5kZQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.