 Scott B. Greeves
Scott B. Greeves Rhesa N. Ledbetter
Rhesa N. Ledbetter- Department of Biological Sciences, Idaho State University, Pocatello, ID, United States
Radio broadcasting is an integral medium for the public understanding of science. Yet, as a poorly recognized health disorder, mental health was not commonly discussed in U.S radio broadcasts until the early 1980s. Since then, mental health has increasingly been the subject of societal discourse and is now frequently the topic of focus for radio programming. Despite the increased attention on mental health, little academic inquiry has considered how science communicators may navigate locally complex and sensitive themes, such as those related to mental health. To address this gap, we discuss our experiences in producing a radio series on mental health called MindTap. Using the exemplar of MindTap, we explore models of science communication and their application within radio communication. Specifically, we suggest that topics, such as mental health, are best approached using the dialogue model of communication, which recognizes the value of integrating experiential and culturally situated knowledge with that of expert knowledge. We also illustrate how this form of communication supports narrative creation, and as such, identify practical insights for practitioners seeking to produce a mental health radio series.
Introduction
Radio broadcasting has been central to the dissemination of information for nearly a century (Hickling, 1992) and is influential in enhancing public understanding of science and in shaping opinions (Grilli et al., 2001). Science-based radio programming that centers on health education can increase audience knowledge levels and positively modify health behaviors (Smith et al., 2011). However, the scientific literature lacks practical insights for communication concerning mental health via radio.
As a poorly recognized health disorder, mental health ailments and challenges were not commonly discussed in U.S radio broadcasts until the early 1980s (Hickling, 1992). Some of the earliest psychiatry talk shows were criticized for their sensationalistic content and unethical practices (Hickling, 1992), however, both the American Psychiatric Association (1977) and the American Psychological Association (1981) swiftly published guidelines for clinical experts participating in media activities. These guidelines cautioned clinicians against diagnosing or treating mental disorders while on the air and endeavored to support the ethical discussion of mental health topics.
Today, topics of mental health are regularly discussed in many factions of society. Mental health was mentioned numerous times in the United Nations 2015 Sustainable Development Goals (Izutsu et al., 2015) and has been discussed as a potential global emergency (Tucci and Moukaddam, 2017). Likewise, topics of mental health have become widespread in broadcast media. Notably, since 2018, the Mental Health Minute has brought together many British and U.S based radio stations to broadcast “a unique, one-minute message on the importance of talking about mental health issues, reaching out, and listening to each other” (Mental Health Minute, 2022). In 2021, the Mental Health Minute was observed by over 500 radio stations and was intended to bring attention to the annual mental health awareness week (Sawyer, 2021).
Mental health was also the subject of a National Public Radio's (NPR) special series in 2008, which presented ten episodes on topics ranging from the alarming rate of suicide among African American youths to dealing with post-traumatic stress disorder (Mental Health (NPR), 2008). Additionally, topics of mental health are frequently featured in NPR's Life Kit, which is an audio series that provides advice for listeners on everyday situations and challenges. Similarly, many regional NPR partnered stations broadcast weekly programming dedicated to mental health topics. KCUR (the NPR partnered station for Kansas City) airs a weekly talk show on mental health and has explored topics ranging from depression in children to social isolation in rural communities (Mental Health (KCUR), 2022). Additionally, smaller NPR partnered stations are increasingly incorporating features on mental health into programs that more broadly discuss health. For instance, Aspen Public Radio frequently integrates local stories regarding mental health into its Health and Wellness reporting (Health and Wellness, 2022), and WHCR (Harlem) lists mental health as one of the major topics of discussion on its weekly talk shows (WHCR, 2022).
While studies have demonstrated the aptitude of dedicated mental health radio broadcasting to reach a significant portion of the population, raise awareness, and reduce stigma (Interactive Radio Program Report, 2016; Cocksedge et al., 2019), few have explored how communicators can effectively navigate the complex and challenging themes of mental health. Equally, few studies have provided practical insights for broadcasters seeking to effectively communicate the scientific information relating to mental health topics. To address these issues, we discuss our experiences in producing a radio series on mental health called MindTap. In this context, we discuss models for science communication and make linkages to practical insights. Ultimately, this study intends to support other communication professionals in their efforts to communicate and disseminate information relating to topics of mental health.
MindTap: Overview and Timeline
MindTap is a radio series that aired 17 episodes on KISU-FM between September 2020 and January 2021 (https://www.kisu.org/show/mind-tap). KISU-FM is an NPR partnered radio station that operates in collaboration with Idaho State University (ISU), with its independent offices and studios located on the ISU Pocatello campus. KISU-FM broadcasts a diverse selection of talk, music, and news programs, and reaches an audience of ~230,000 Eastern Idahoans. In addition to the live broadcast, KISU-FM's programming is freely available online via both a listen-live feature and an on-demand catalog of archived content.
The motivation for the creation of the MindTap series was driven by Dr. Rhesa Ledbetter, a Professor of Microbiology at ISU, and former Science Reporter for Utah Public Radio. Dr. Ledbetter recruited a small group of Biology students. The three successful candidates comprised one student from each the undergraduate, masters, and doctoral level. Students were selected based not on their experience in broadcast journalism but rather for their passion for the topic and interest in science communication.
Following the establishment of the MindTap team, there was a consultation with KISU-FM management to confirm the foundational objectives of the radio series and the audio presentation format. This process formalized the objectives of the MindTap series as to bring awareness and attention to important mental health topics, which were determined to be pertinent to the local communities within the broadcast radius. Additionally, it was confirmed that MindTap would air as a weekly series during a time-flexible eight-minute slot on Tuesday mornings. Regarding ethical considerations, it was discussed that all episodes should be considerate of the challenging themes. Additionally, all guests were informed of the intent and purpose of the series, as well as when they were on the record. Finally, by asking open ended questions, guests could take interviews in a direction they felt most comfortable with.
The first MindTap episode aired on Tuesday, September 15, 2020. The series aired a new episode weekly for 17 iterations, with the final broadcast airing on Tuesday, January 5, 2021 (Table 1). The shortest episode was 5 min 57 s and the longest was 15 min 17 s. The average episode length was 8 min 11 s.
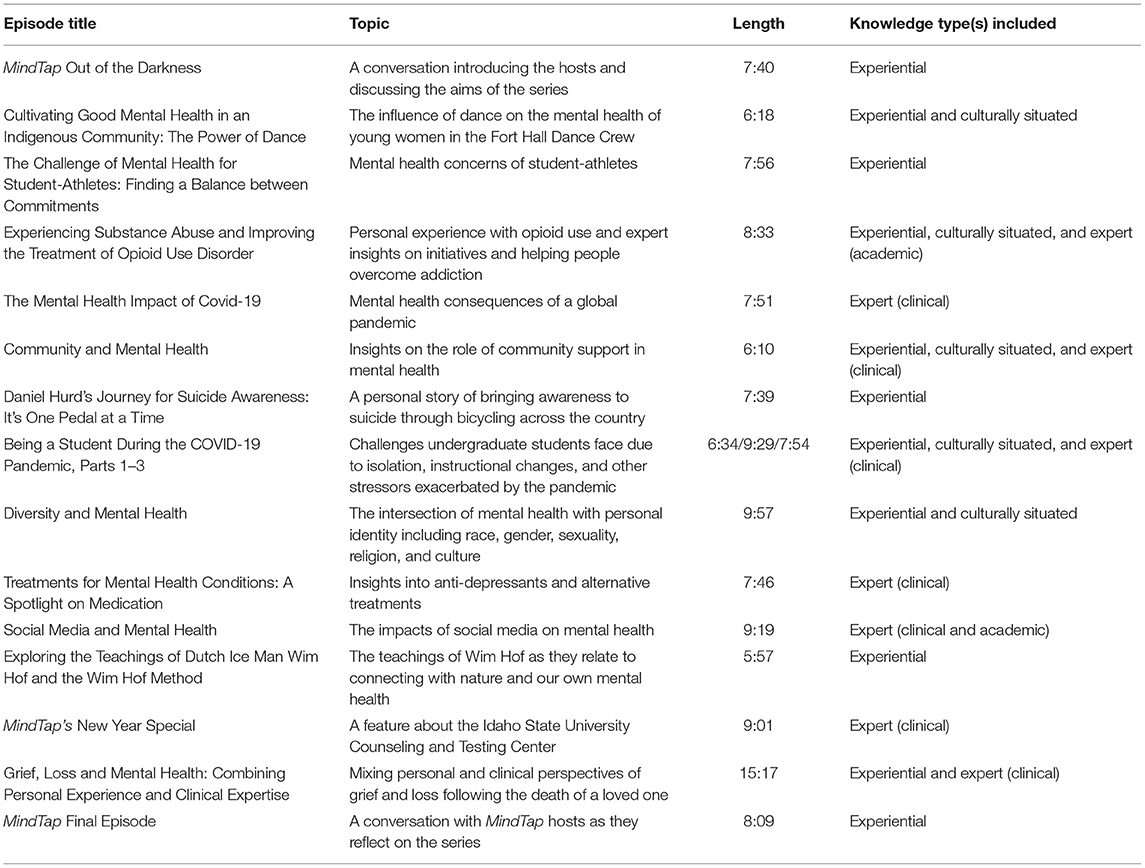
Table 1. MindTap episode titles, topics, lengths, and knowledge types included.
Models For Science Communication: Radio And Mental Health
Three models of science communication dominate communication theory: the dissemination model (often called the deficit model), the dialogue model, and the participation model (Hetland, 2014). Here, we explore the suitability of each model to support the communication of mental health topics via the medium of radio.
The oldest of the three models is the deficit model of science communication. It assumes that public uncertainty and skepticism toward any particular scientific topic is caused by a lack of relevant information or knowledge (Dickson, 2005). To overcome this knowledge gap, the deficit model suggests that a one-way flow or transfer of information from experts to the public will remove the knowledge deficit and shift public attitudes to more closely align with those held by the experts (Suldovsky, 2017). However, many scholars argue that expert knowledge is not the only nor the most important means to understanding (Funtowicz and Ravetz, 1993), with many studies highlighting the value of experiential and culturally situated knowledge (Strachan, 2012; Wyllie de Echeverria and Thornton, 2019; Pauli et al., 2021). Simply, we define experiential knowledge as knowledge gained through experience and culturally situated knowledge as knowledge gained from one's cultural experiences. Indeed, the deficit model has been criticized for failing to recognize these elements, which ultimately works to undermine expert produced information and deepen the perceived divisions between experts and the public (Fricker, 2002).
Instead, most modern communication scholars advocate for a bi-directional or two-way form of science communication (Fischhoff and Scheufele, 2013; Yuan et al., 2017). In this context, the dialogue model (also known as the public engagement with science model) represents an alternative model for science communication. This model integrates non-scientific forms of knowledge, including experiential knowledge and culturally situated knowledge. By treating these non-scientific forms of knowledge as valuable, the dialogue model addresses many of the criticisms of the deficit model (Reincke et al., 2020). A central tenet of the dialogue model is that both experts and the public may express their views, values, experiences, and concerns in a manner that promotes mutual learning (McCallie et al., 2009).
Building from the dialogue model, the participation model allows the public to partake and assist with the scientific work, including in fundamental tasks such as the identification of research questions and the interpretation of results (Trench, 2008). As a primary distinction, the dialogue model centers on the discussion of the implications of knowledge, while the participation model focuses on the co-production of knowledge between experts and the public (Bartock, 2015). Notably, the participation model has been credited with furthering public epistemic and moral trust in science, and enhancing the perceived democratic legitimacy of the scientific process (Kappel and Holmen, 2019).
In the context of radio communication, it may be assumed that due to the features of the medium, most science-based radio programs may deploy a deficit model style of one-way communication. However, as various technological advancements have connected the audience with radio management, it has been suggested that a “mediamorphosis” has occurred within radio (Achmad and Ida, 2019). Owing to these improvements in interactivity, modern radio practices are more consistent with the dialogue model. In the simplest form, many radio programs seek and actively promote audience interactivity, such as online listener feedback pathways, which are subsequently used to tailor content and better reflect the needs and wishes of the listenership (Interactive Radio Program Report, 2016). More directly, some science-based radio shows deliberately incorporate a diverse range of speakers who possess differing knowledge types. For instance, a study regarding a longstanding BBC Radio Cornwall Mental Health program, noted that the show routinely incorporated listener call-ins (Cocksedge et al., 2019). The authors noted that callers often shared their own experiences in addition to asking questions of experts, which added “to a useful and interesting discussion,” with some discussions relating to local services (Cocksedge et al., 2019). Consistent with the dialogue model, the integration of listener call-ins with traditional expert speakers supported the communication of traditional expert knowledge, experiential, and culturally situated knowledge.
Consistent with the above findings of Cocksedge et al. (2019), the dialogue model of science communication is recognized as particularly valuable when considering complex social systems or phenomena (Reincke et al., 2020). As such the dialogue model of communication may be best placed to address the many social considerations of mental health topics. For instance, a cultural stigmatization exists around mental health (Bharadwaj et al., 2017) and negative perceptions about mental illness vary greatly between communities (Choudhry et al., 2016). It is well established that marginalized communities frequently suffer poorer mental health than other communities for preventable reasons, such as healthcare accessibility and affordability (Silberholz et al., 2017). Similarly, varying cultural perceptions of mental health, which are often shaped by religious ideas, influence how likely people are to seek mental health treatments (Schieman et al., 2013). Moreover, since the beginning of the COVID-19 pandemic, mental health challenges have been exacerbated by a rise in social isolation and loneliness (Cullen et al., 2020; Pfefferbaum and North, 2020).
However, as these concepts relate to radio communication, it's important to reiterate that only the dialogue model focuses on the transmission of knowledge, while the participation model focuses on knowledge co-production. As such, we suggest that the dialogue model of communication is more applicable than the participation model. Despite some science-based radio shows, such as Audio Lab (Starling and Tanswell, 2018), explicitly identifying co-production of knowledge and other creative outputs as project goals, most scientific radio programming centers on the transmission of knowledge. Demonstrating this, a survey of European science-based radio broadcasters identified that their program's primary purpose was to be informative (Merzagora et al., 2006).
In the context of radio communication, a supporting argument for the adoption of the dialogue model relates its consistency with the established features of radio programming. At its core, the dialogue model supports conversation between various stakeholders, which is a common feature of science radio (Alda et al., 2005). However, further to this, the dialogue model supports storytelling and narrative presentation, which is a communication strategy deployed by prominent science communication programming (Alda et al., 2005). By providing a foundation into which traditional expert knowledge can be interweaved, experiential and cultural situated knowledge can be combined to naturally weave together threads of science and community (Bayer and Hettinger, 2019).
Indeed, as radio broadcasters have long known, storytelling is an inherently persuasive and powerful communication tactic. Broadly, narrative communication is characterized by a sequential plot of interconnected events, which include a beginning, middle, and end that all follow a basic structure (Fisher, 1985). Complementary to the narrative paradigm of communication theory, which suggests that human beings are natural storytellers and that all meaningful communication occurs through storytelling (Fisher, 1985), a dialogue model approach avoids the tendency for scientific information to be presented in a manner disconnected from real-world application. This relates to Fisher's continued explanation of the narrative paradigm, which states that narrative rationality considers coherence (the degree to which a story makes sense) and fidelity (the degree to which a story matches lived experience), and is central to successful communication (Fisher, 1989). As this paradigm relates to science communication, there is much evidence to suggest that storytelling is intrinsically persuasive (Dahlstrom, 2010; Bilandzic and Busselle, 2013), and the tactic presents science communicators with a powerful tool in persuading otherwise resistant non-expert audiences (Dahlstrom, 2014).
Radio And Mental Health Communication: The Case of MindTap
At the inception of the MindTap series, models for science communication were not explicitly discussed. Instead, a significant portion of time was devoted to identifying locally important mental health issues that represented potential episode topics. Equally, a focus was placed on training activities, particularly in relation to audio production, interviewing, and on-air speaking styles.
Early consideration for communication style centered on a preconceived need to replicate the stylistic features of established science radio programming, such as WNYC's Radiolab and WBEZ's This American Life. At this time, we noted that most science-based shows operated within a storytelling approach. Also, it was discussed that due to a sense of relative inexperience in both interviewing and editing, team members felt most comfortable developing an episode using just one form of expertise (clinical, personal, or culturally situated) per episode. This is readily identifiable in several episodes and is outlined in Table 1.
As the series progressed, team members gained experience and confidence in their production abilities, which lent a sense of creative freedom. Connectedly, team members increasingly sought to incorporate more than more point of view/knowledge type in each story (Table 1). Notably, the episode titled “Experiencing Substance Abuse and Improving the Treatment of Opioid Use Disorder,” which was aired early in the MindTap series, combined both personal experience and expert insights on opioid use disorder with local initiatives that support people to overcome addiction. This episode highlighted to the MindTap team the strengths of interweaving multiple forms of knowledge. Furthermore, the episode demonstrated that it was possible to maintain a consistent narrative structure using varied and complementary forms of knowledge. As such, it was discussed that where possible, at least two differing forms of knowledge should be presented in each episode.
Yet, as the series progressed, it became increasingly apparent that local and cultural knowledge is challenging to identify, particularly considering the sensitive nature of mental health topics. While expert knowledge, including that held by clinicians and researchers, was readily identifiable, an apparent lack of identifiable local knowledge was discussed as a limitation by the MindTap team. However, as the series progressed and gained traction among the estimated listenership of 6,000 people, multiple individuals contacted the radio station expressing their desire to contribute to the series. Perhaps the most notable example of this was Daniel Hurd, who contacted the radio station and subsequently featured in an episode titled “Daniel Hurd's Journey for Suicide Awareness: It's One Pedal at a Time.” Importantly, individuals representing marginalized communities also contacted the radio station expressing their desire to bring voice to underrepresented groups. For instance, Simon Studevant contacted the radio station as a representative for the Sexuality and Gender Club at ISU, and expressed a desire to contribute to an episode considering the intersectionality of race, gender, sexuality, and culture as they relate to mental health. This culminated in an episode titled “Diversity and Mental Health.”
While culturally situated knowledge was invaluable to our communication on mental health, it also brought our attention to locally pertinent topics that we had previously overlooked, such as diversity and intersectionality. For instance, after learning about the substantial size of the Sexuality and Gender Club at ISU, the prominence of mental health challenges within that community, and the confounding religious considerations within the local community, the topic clearly warranted our attention.
Upon reflection, MindTap heavily relied on local participation but did not actively promote pathways for community engagement. It is a testament to the East Idaho community that they sought out channels of communication in order to participate in the series, but it would have been preferable to both provide and actively encourage local participation through a designated channel, such as a MindTap email address. Doing so would have likely yielded additional local knowledge for the topics discussed in the series and may have identified further topics to expand the scope of the series.
A Community Driven Approach: A MindTap Episode Exemplar
To further explore the practical application of communication models and theory, we present an episode case study. The episode titled “Grief, Loss and Mental Health: Combining Personal Experience and Clinical Expertise” aired on January 5, 2021 and represents the penultimate episode in the MindTap series.
This episode explores themes of grief and loss in the context of a loved-one's death and intertwines expert knowledge and experiential knowledge types. The expert perspective is presented by Hannah Brisner, an ISU Doctoral Counseling Candidate, who specializes in grief and holds an M.A in School Counseling. The experiential perspective is presented by Dr. Rhesa Ledbetter, a Professor of Microbiology. Rhesa speaks not from her professional perspective as a former science radio reporter, but rather from her personal experiences following the sudden and unexpected death of her husband, Tim. The flow and direction of the conversation was moderated with a basic outline of anticipated topics prepared in advance by the host.
Below is an extract from the episode transcript. For context, it is time stamped and followed a brief introduction on each guest.
Start of Transcript
Host (1:46): Hannah, it would be great to start from your clinical perspective of what grief can actually look like.
Hannah (1:57): Yeah, grief is going to look very different for every person. As a counselor, I have had the privilege of serving a lot of different individuals who have gone through grief, and it looks different for each of them. There are these five traditional stages of grief. Typically, it goes from denial to anger to sadness to bargaining and then to acceptance. However, as we know, those stages aren't linear. So if you imagine in your head a train track, that might be what you're expecting in terms of grief, but it really looks like your three year old took some crayons and scribbled across the paper with five different colors. It's going to look so different and you can bounce in and out of the stages. Some people really like to talk about their loss and that's really important to them. Other people don't want to talk about it at all. And so it is really going to depend on the person.
Host (2:50): Rhesa, does that sound similar to your experience of grief?
Rhesa (2:54): Grief to me—I heard this one time at a seminar that I went to—“that grief is just love with nowhere to go'. I thought that was so beautiful because I think that's exactly what I've experienced with the loss of Tim, is that my grief has been like an intense beautiful love and is essentially the way that I still love Tim now, even though that he's gone. And I can tell you it's absolutely brutal. As I grieved, the sadness and the pain that I've experienced is unlike anything that I could have imagined before this happened. And I remember feeling in the immediate aftermath, how was I even going to do life without my partner and my best friend? I can tell you that this thought often crosses my mind. I can't believe that Tim is never coming home. But one of the other things I've found through this process is that as brutal as the grief process is, it's also been so beautiful for me and in the midst of this tragedy I've been able to see beautiful elements intertwined with all the sadness. For example, I swear I feel Tim's presence sometimes and people might look at me like I'm crazy and that's okay. But, I've also had things that I think are signs and I just have to look up and smile and say Tim I think that was you. And those types of things have just filled my heart with joy, in addition to the kindness and outpouring of love that I've received from my family and friends as well as from strangers, it's been incredible.
As I've gone through and continue to go through this grief process, I've often wondered if I need some more clinical help?
Hannah (4:41): Right. So often I think we [clinicians] like to say that there's this threshold of grief, that all of a sudden after six months of grieving you will move into reaching the stage of acceptance. And if you don't, then suddenly you need the support of a counselor. And that's just not true. As we [clinicians] know, grief is different for everyone. Someone might need support a year into the process and someone might need support two years into the process. We [clinicians] often don't like to have someone who is grieving begin counseling right away because you are so stuck in the shock and denial of that experience. You're just working to survive at that point and that can last for quite some time. Sometimes grief might move into what we [clinicians] call complicated grief, which is when we [the grieving patient] have not properly dealt with a situation so it begins to permeate into our lives in areas it normally wouldn't. At that time, its normally good to get extra support but it's going to depend on every person.
Host (5:41): So Hannah, would it be a counselor who would help a person decide if they are experiencing depression or grief?
Hannah (5:46): Yeah, again, it totally depends, and I think the important thing to highlight with this is that grief is not a diagnosis. You cannot diagnose grief in the DSM.
Host (6:00): For our listeners, the DMS is?
Hannah (6:03): Oh yeah, the Diagnostic and Statistics Manual of Mental Disorders. So grief is not a mental disorder. With depression there are more of the characteristic signs or symptoms that you can see, like lack of motivation, no interest or pleasure in certain things, feeling hopeless. These are many of the same things that you will experience with grief. However, if you've just experienced a loss, you need to take into consideration that the grief is likely causing that, not the depression. And I think that's really important to highlight. So yeah, I think it's really important to have a mental health professional assess that.
Host (6:38): So Rhesa, in your experience, have you considered the distinction between depression, anxiety, and the grief you've been experiencing?
Rhesa (6:49): Absolutely, I've thought about that a lot. I feel personally that I've definitely had anxiety throughout this process, perhaps bouts of depression—I'm not sure—but the anxiety I'm quite certain of. You know, there are so many factors that are involved with trauma of any kind and in my case it wasn't just the loss of Tim, you know there is dealing with Tim's estate, planning a memorial, wondering what I'm going to do for the rest of my life, and even worrying that Tim might be forgotten over time. I think that one of the greatest fears of losing someone. I'll always remember Tim, but I worry about him sort of being lost to everything around me and all of that brings a lot of anxiety on top of what is already being experienced with the loss.
End of Transcript
This extract highlights the strengths of the dialogue model and narrative paradigm, through the integration of Rhesa's personal story of losing her husband and Hannah's clinical expertise as a graduate student studying grief counseling. Notable is Hannah and Rhesa's detailed interaction, which allowed Hannah to present her clinical knowledge within Rhesa's personal story. This resulted in a more well-rounded exploration of the topic, which consistent with components of narrative coherence and fidelity (Fisher, 1989), is likely more relatable and sensical to listeners. An examination of the extract reveals interesting themes that support this interpretation.
In particular, it is notable that Hannah and Rhesa use contrasting language styles but nonetheless discuss shared themes. Take, for example, Hannah's formal explanation of grief, which features an analysis of the various stages, which she quickly notes “aren't linear,” as some might believe. Rhesa's viewpoint, however, describes grief informally, relating it to a form of love. While each perspective is distinct, it should be noted that these two different forms of knowledge complement one another. Specifically, both Rhesa and Hannah affirm each other's contention that the linear 5-stage model of grief is antiquated and the lived reality is rather more like a non-linear path, which is comparable to a child's scribble on a piece of paper. Highlighting the strengths of a dialogue model approach, Hannah and Rhesa's conversation works to ground science in reality. Notably, Hannah ties her expert interpretation to Rhesa's lived experience, suggesting that it is okay to be experiencing feelings similar to anxiety and depression after losing a loved one, as Rhesa mentioned she was.
Considering not just the presented extract but the full episode, it is possible to identify the application strategies consistent with the narrative paradigm. Specifically, Rhesa's lived experiences are presented in a manner consistent with a sequential plot of interconnected events. The beginning of Rhesa's story is characterized by her recollection of her husband, the middle by his sudden death, and the ending by subsequent experiences with grief and loss. Throughout the latter parts of the story, Hannah is able to insert her expert knowledge and contribute to a meaningful dialogue relating to Rhesa's experiences, which likely supports listener interpretation and understanding of grief and loss. Similar to the strengths of the dialogue model, this technique places expert analysis within a real-world narrative, which listeners can not only learn from, but likely identify with on some level.
Summary And Practical Insights
Mental health represents a challenging but important topic for radio communication. Using the lens of our experiences in producing the MindTap series, we have explored the application of communication models as they relate to producing a radio series on mental health. Foundationally, we suggest that locally and culturally complex topics, such as mental health, are best approached using the dialogue model of communication. The dialogue model acknowledges the value of non-expert knowledge and provides scope to interweave various means of understanding, often in a complimentary manner. Connectedly, this form of communication supports narrative creation, which is both familiar to radio listeners and represents an established means of science communication. As such, we identify a few practical insights for practitioners seeking to produce a mental health radio series:
1. Where possible, integrate more than one form of knowledge. Practically, this may require a level of creativity as it relates to combining different forms of information. However, the resultant product can represent a well-rounded and narrative driven piece.
2. Actively provide and promote pathways for listeners to contact you and get involved with your series. Typically, expert knowledge is easier to identify and recruit, whereas experiential knowledge is less readily identifiable. Therefore, it's important to continually encourage listener participation.
3. Local and culturally situated knowledge is valuable in both contributing to stories but also in guiding editorial oversight regarding topics of interest and focus. Many locally pertinent mental health topics may be overlooked if local expertise is not consulted.
4. For science communicators new to radio or podcasts, it is important to build a holistic understanding of the production process. Remove the inclination to produce simplistic content by being familiar with editorial and production processes.
These insights are presented with the intention of supporting other professionals tasked with communicating health topics. However, we suggest that the insights produced may be applicable within broader contexts. Owing to their non-specific connection to health communication and radio messaging, insights one, two, and three, may be utilized as a communication framework for non-health related topics and other forms of media such as print and digital. While the dialogue approach, incorporating varying knowledge types, may translate well into these other forms of communication, it important to recognize that our insights may need to adapted to each specific context. For example, while audio content lends itself well to direct conversation, print media relies on the voice of the writer to capture each perspective.
Data Availability Statement
The original contributions presented in the study are included in the article/supplementary material, further inquiries can be directed to the corresponding author/s.
Author Contributions
SG: primary contributor to the creation of the MindTap radio series and contributed to both the writing and the editing of the manuscript. RL: project director of the MindTap radio series and contributed to both the writing and the editing of the manuscript. All authors contributed to the article and approved the submitted version.
Funding
Funding for MindTap was provided by the Idaho National Laboratory Community Donation with corporate funds from the Battelle Energy Alliance and Idaho State University's Career Path Intern Program.
Conflict of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher's Note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Acknowledgments
Thank you to the following individuals for their contributions to the MindTap radio series. Jessica Whitaker-Fornek and Christian Powell for assisting with reporting and production. Jamon Anderson, general manager of KISU-FM, for valuable feedback and technical expertise. Finally, to the guests willing to share their voices and stories.
References
Achmad, Z., and Ida, R. (2019). The shifting role of the listeners in the mediamorphosis process of culture radio: a case study of Jodhipati 106.1 FM. Masy. Kebud. Dan Polit. 32, 240–250. doi: 10.20473/MKP.V32I32019.240-250
Alda, A., Bass, E. R., Chedd, G., Constantinou, C., O'Connell, C., and Schneider, H. (2005). Storytelling Techniques in Radio Lab. Alan Alda Center for Communicating Science: Stony Brook University. Available online at: https://ir.stonybrook.edu/xmlui/bitstream/handle/11401/8226/lessonsfromradiolabpcrstorytelling.pdf?sequence=1 (accessed May 3, 2022).
American Psychiatric Association (1977). Joint Commission on Public Affairs: guidelines for psychiatrists working with the communications media. Am. J. Psychiatry 134, 609–661.
American Psychological Association (1981). Ethical principles of psychologists working in the communications media. Am. Psychol. 36,633–638.
Bartock, L. (2015). Walking the talk? Examining the practical application of models of science communication in long-term ecological research sites (Master's thesis). Syracuse, NY: State University of New York.
Bayer, S., and Hettinger, A. (2019). Storytelling: a natural tool to weave the threads of science and community together. Bull. Ecol. Soc. Am. 100, 1–6. doi: 10.1002/bes2.1542
Bharadwaj, P., Pai, M. M., and Suziedelyte, A. (2017). Mental health stigma. Econ. Lett. 159, 57–60. doi: 10.1016/j.econlet.2017.06.028
Bilandzic, H., and Busselle, R. (2013). “Narrative persuasion,” in The SAGE Handbook of Persuasion: Developments in Theory and Practice, Vol. 2, eds J. P. Dillard and L. Shen (London: Sage Publications, Inc), 200–219.
Choudhry, F. R., Mani, V., Ming, L. C., and Khan, T. M. (2016). Beliefs and perception about mental health issues: a meta-synthesis. Neuropsychiatr. Dis. Treat. 12, 2807. doi: 10.2147/NDT.S111543
Cocksedge, K. A., Guliani, J., Henley, W., Anderson, T., Roberts, S., Reed, L., et al. (2019). Local radio to promote mental health awareness: a public health initiative. BJPsych Open 5, e60. doi: 10.1192/bjo.2019.51
Cullen, W., Gulati, G., and Kelly, B. D. (2020). Mental health in the COVID-19 pandemic. QJM Int. J. Med. 113, 311–312. doi: 10.1093/qjmed/hcaa110
Dahlstrom, M. F. (2010). The role of causality in information acceptance in narratives: an example from science communication. Commun. Res. 37, 857–875. doi: 10.1177/0093650210362683
Dahlstrom, M. F. (2014). Using narratives and storytelling to communicate science with nonexpert audiences. Proc. Natl. Acad. Sci. USA 111, 13614–13620. doi: 10.1073/pnas.1320645111
Dickson, D. (2005). The case for a ‘deficit model' of science communication. SciDev. Available online at: https://earthscience.rice.edu/wp-content/uploads/2018/01/dickinson-2005-deficit-model-scinet.pdf (accessed May 4, 2022).
Fischhoff, B., and Scheufele, D. A. (2013). The science of science communication. Proc. Natl. Acad. Sci. USA 110, 14031–14032. doi: 10.1073/pnas.1312080110
Fisher, W. (1989). Human Communication as Narration: Toward a Philosophy of Reason, Value, and Action. University of South Carolina Press. Available online at: https://hdl.handle.net/2027/heb.31801 (accessed May 4, 2022).
Fisher, W. R. (1985). The narrative paradigm: an elaboration. Commun. Monogr. 52, 347–367. doi: 10.1080/03637758509376117
Fricker, E. (2002). Trusting others in the sciences: a priori or empirical warrant? Stud. Hist. Philos. Sci. Part A 33, 373–383. doi: 10.1016/S0039-3681(02)00006-7
Funtowicz, S. O., and Ravetz, J. R. (1993). Science for the post-normal age. Futures 25, 739–755. doi: 10.1016/0016-3287(93)90022-L
Grilli, R., Ramsay, C., and Minozzi, S. (2001). Mass media interventions: effects on health services utilisation. Cochrane Database Syst. Rev. 1, CD000389. doi: 10.1002/14651858.CD000389
Health Wellness. (2022). Aspen Public Radio. Available online at: https://www.aspenpublicradio.org/health-and-wellness (accessed February 26, 2022).
Hetland, P. (2014). Models in science communication policy. Nord. J. Sci. Technol. Stud. 2, 5–17. doi: 10.5324/njsts.v2i2.2144
Hickling, F. W. (1992). Radio psychiatry and community mental health. Psychiatr. Serv. 43, 739–741. doi: 10.1176/ps.43.7.739
Interactive Radio Program Report (2016). Ottawa, Ontario, Canada: Farm Radio International. Available online at: https://www.mhinnovation.net/sites/default/files/downloads/innovation/reports/FRI%20MH%20PROGRAM%20RADIO%20REPORT_FINAL%20%281%29.pdf (accessed February 26, 2022).
Izutsu, T., Tsutsumi, A., Minas, H., Thornicroft, G., Patel, V., and Ito, A. (2015). Mental health and wellbeing in the Sustainable Development Goals. Lancet Psychiatry 2, 1052–1054. doi: 10.1016/S2215-0366(15)00457-5
Kappel, K., and Holmen, S. J. (2019). Why science communication, and does it work? A taxonomy of science communication aims and a survey of the empirical evidence. Front. Commun. 4, 55. doi: 10.3389/fcomm.2019.00055
McCallie, E., Bell, L., Lohwater, T., Falk, J. H., Lehr, J. L., Lewenstein, B. V., et al. (2009). Many Experts, Many Audiences: Public Engagement with Science and Informal Science Education. Washington, DC: Center for Advancement of Informal Science Education (CAISE). Available online at: https://www.informalscience.org/many-experts-many-audiences-public-engagement-science (accessed February 26, 2022).
Mental Health Minute. (2022). Radiocentre. Available online at: https://www.radiocentre.org/commercial-radio-people/mental-health-minute/ (accessed February 26, 2022).
Mental Health (KCUR). (2022). KCUR. Available online at: https://www.kcur.org/tags/mental-health (accessed February 26, 2022).
Mental Health (NPR). (2008). NPR. Available online at: https://www.npr.org/series/88201937/mental-health (accessed February 26, 2022).
Merzagora, M., Mazzonetto, M., and Tola, E. (2006). “SCIRAB: Science in radio broadcasting,” in 9th International Conference on Public Communication of Science and Technology (PCST) (Seoul, South Korea), 7.
Pauli, N., Williams, M., Henningsen, S., Davies, K., Chhom, C., van Ogtrop, F., et al. (2021). “Listening to the sounds of the water”: bringing together local knowledge and biophysical data to understand climate-related hazard dynamics. Int. J. Disaster Risk Sci. 12, 326–340. doi: 10.1007/s13753-021-00336-8
Pfefferbaum, B., and North, C. S. (2020). Mental health and the Covid-19 pandemic. N. Engl. J. Med. 383, 510–512. doi: 10.1056/NEJMp2008017
Reincke, C. M., Bredenoord, A. L., and van Mil, M. H. (2020). From deficit to dialogue in science communication: the dialogue communication model requires additional roles from scientists. EMBO Rep. 21, e51278. doi: 10.15252/embr.202051278
Sawyer, M. (2021). The week in audio: the best of Mental Health Awareness Week. The Guardian. Available online at: https://www.theguardian.com/tv-and-radio/2021/may/15/mental-health-awareness-week-radio-x-jazz-fm-chilldabeats-blindboy-super-brain-how-do-you-cope-elis-john (accessed February 26, 2022).
Schieman, S., Bierman, A., and Ellison, C. G. (2013). “Religion and mental health,” in Handbook of the Sociology of Mental Health (Berlin: Springer), 457–478.
Silberholz, E. A., Brodie, N., Spector, N. D., and Pattishall, A. E. (2017). Disparities in access to care in marginalized populations. Curr. Opin. Pediatr. 29, 718–727. doi: 10.1097/MOP.0000000000000549
Smith, M. L., Menn, M., and McKyer, E. L. J. (2011). Effectiveness of the radio as a health information source. J. Radio Audio Media 18, 196–211. doi: 10.1080/19376529.2011.615776
Starling, B., and Tanswell, J. (2018). Diversifying audiences and producers of public involvement in scientific research: the AudioLab. Res. Involv. Engagem. 4, 39. doi: 10.1186/s40900-018-0122-2
Strachan, L. M. (2012). The Bedouin Know: Using local knowledge to understand the effects of development at the Wadi Rum Protected Area in Southern Jordan (dissertation). Hamilton, Ontario, Canada: McMaster University.
Suldovsky, B. (2017). “The information deficit model and climate change communication,” in Oxford Research Encyclopedia of Climate Science (Oxford: Oxford University Press).
Trench, B. (2008). “Towards an analytical framework of science communication models,” in Communicating Science in Social Contexts: New Models, New Practices, eds. D. Cheng, M. Claessens, T. Gascoigne, J. Metcalfe, B. Schiele, and S. Shi (Dordrecht: Springer Netherlands), 119–135. doi: 10.1007/978-1-4020-8598-7_7
Tucci, V., and Moukaddam, N. (2017). We are the hollow men: the worldwide epidemic of mental illness, psychiatric and behavioral emergencies, and its impact on patients and providers. J. Emerg. Trauma Shock 10, 4–6. doi: 10.4103/0974-2700.199517
WHCR. (2022). Available online at: https://whcr.org/ (accessed February 26, 2022).
Wyllie de Echeverria, V. R., and Thornton, T. F. (2019). Using traditional ecological knowledge to understand and adapt to climate and biodiversity change on the Pacific coast of North America. Ambio 48, 1447–1469. doi: 10.1007/s13280-019-01218-6
Keywords: radio, mental health, science communication, dialogue model, narrative paradigm
Citation: Greeves SB and Ledbetter RN (2022) Science Communication in Public Radio: The Case Study of MindTap. Front. Commun. 7:889207. doi: 10.3389/fcomm.2022.889207
Received: 03 March 2022; Accepted: 16 May 2022;
Published: 13 June 2022.
Edited by:
Diyako Rahmani, Massey University, New ZealandReviewed by:
Kelly E. Tenzek, University at Buffalo, United StatesJudith Borghouts, University of California, Irvine, United States
Copyright © 2022 Greeves and Ledbetter. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Rhesa N. Ledbetter, cmhlc2EubGVkYmV0dGVyQGhhc3RpbmdzLmVkdQ==