
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Commun., 05 January 2022
Sec. Health Communication
Volume 6 - 2021 | https://doi.org/10.3389/fcomm.2021.785186
 Sarah Bauerle Bass1*
Sarah Bauerle Bass1* Ilene L. Hollin2
Ilene L. Hollin2 Patrick J. Kelly3Mohammed Alhajji1Paul D’Avanzo1Laurie Maurer4Avrum Gillespie5Dori Schatell6Heather Gardiner1
Patrick J. Kelly3Mohammed Alhajji1Paul D’Avanzo1Laurie Maurer4Avrum Gillespie5Dori Schatell6Heather Gardiner1Living donor kidney transplantation is a superior treatment option for those with end stage kidney disease, but most transplants are from deceased donors. Securing a living donor for living donor kidney transplantation requires effective, well-timed communication which many may find difficult or intimidating. This study uses segmentation analysis and an innovative marketing technique called perceptual mapping to create three dimensional models to compare living donor kidney transplant perceptions by self-reported health status in 160 end-stage kidney disease dialysis patients of two hospital-based dialysis units and an online forum through cross-sectional surveys. Findings indicate patients with poor self-reported health status are more concerned with not knowing what to say or being afraid a person would say no to living donor kidney transplantation. They are also concerned about the donor’s ability to care for family or donate in the future. They are, however, more likely to see benefits of living donor kidney transplantation, including the kidney lasting longer and having a greater quality of life. Findings reveal messages that could be emphasized in interventions to enhance the ability to ask for living donor kidney transplantation, especially in those assessed as having poor health status. Segmentation analysis and perceptual mapping methods can provide a more nuanced look at how best to develop intervention content to increase living donor kidney transplant.
Living donor kidney transplantation (LDKT) is the superior treatment option for those living with end-stage kidney disease (ESKD) as it reduces time waiting for a transplantable kidney, improves patient outcomes and quality of life, and is the most cost-effective modality compared to dialysis or deceased donor kidney transplant (DDKT) (Gozdowska et al., 2016; Landreneau et al., 2010). The majority (77.1%) of kidney transplants in 2020, however, were obtained from deceased donors [Organ Procurement and Transplantation Network/United Network for Organ Sharing (OPTN/UNOS, 2021)]. This may be because pursuing LDKT can be difficult (Barnieh et al., 2017). Effective, well-timed communication is central to recruiting potential living donors, however initiating, maintaining, and managing the logistics of these conversations have been major challenges cited by both potential donors and recipients (Weng et al., 2010).
While structural barriers do exist (Purnell et al., 2012; Sandal et al., 2019), such as lack of health insurance or access to nephrology specialists, often individuals with kidney disease avoid LDKT discussions or are unwilling to pursue LDKT due to misunderstandings and misperceptions of its risks and benefits (Rodrigue et al., 2008; Traino, 2014; Davis et al., 2017; Cabacungan et al., 2020). These communication barriers complicate the communicative processes needed to identify and recruit living donors, including the belief that receiving a donated kidney from a family member may take it away from another family member in the future (Rodrigue et al., 2008), concern for the health and wellbeing of the donor after donation, and being perceived as a burden (Alvaro et al., 2008). The socialized environment of dialysis, in which patients frequently come to a dialysis center and create relationships with other patients, has been expressed by some as another reason to not pursue transplants, including LDKT (Weng et al., 2010), while the desire to stop dialysis has motivated others to actively seek out potential living donors (Sajjad et al., 2007). The assumption that others will simply offer to donate their kidney without being asked is another reason why potential recipients do not discuss LDKT (Sajjad et al., 2007; Weng et al., 2010; DePasquale et al., 2021). Some potential recipients also note a preference for managing their health independently without involving a potential donor (Stothers et al., 2005; Weng et al., 2010). In contrast, the desire to survive to be present for family supersedes these concerns for others (Stothers et al., 2005).
Importantly, much existing work focuses on the donor’s perspective. Little research addresses the quick decisions that patients must make about asking a live donor or the process in which these patients make that request (Stothers et al., 2005). And conflicting findings on the role of the dialysis environment has indicated it actually fosters pursuing LDKT (Gillespie et al., 2017; Gillespie et al., 2021). This, along with evidence that potential recipients overestimate the struggles donors face when deciding to donate (Stothers et al., 2005), further demonstrates the need to explore potential recipients’ conceptualization of LDKT. It should be noted that researchers have developed interventions to educate potential recipients to change LDKT perceptions (Arriola et al., 2014; Weng et al., 2017; LaPoint et al., 2018; Boulware et al., 2021; Waterman, 2021) and a few are routinely offered by transplant centers outside of a research context (Waterman, 2021). But many of these interventions do not tailor the interventions to the specific needs of patients based on potential differences in LDKT perceptions.
To fill this gap, the primary objective of this study was to contextualize potential recipients’ perceptions of LDKT and compare them by self-perceived health status using two commercial marketing techniques: segmentation and perceptual mapping (Morgan et al., 2001). Perceptual mapping is grounded in two theoretical frameworks: Woelfel and Fink (1980) Self-Regulation Theory and Information-Communication Theory both based on the individual’s conceptual map of health threatening situations in which they form a mental representation of the condition (Leventhal et al., 2001; Cameron and Leventhal, 2003; Leventhal, 2004) what caused it, what its effects might be, how long it might last, and how to control it, and then acts or does not act on those perceptions. The resulting maps are three-dimensional perceptual models of decision and communication processes, and when using segmentation techniques, can be compared by demographic or psychographic (e.g., perceived health status) differences to help understand how best to target messages within interventions. The highly specific models allow for the positioning of the “Self”, based on the group aggregate, around a series of constructs. This helps us identify which concepts cluster close to the group of interest and are most important to the group, and which concepts cluster farther away and are less important. Previous research has demonstrated that this method can identify important intervention targets to focus on that are most likely to motivate and implement behavior change (Bass et al., 2012; Bass et al., 2018).
This method builds on the Galileo approach of Woelfel and Fink (1980) as a mathematical modeling tool to create persuasive communication interventions. Our study represents the first use of this novel methodology to visually represent salient factors most influential in the decision to pursue LDKT and how they are related to patients’ self-perceived health status. Results can be used to develop better interventions to assist patients with the difficult process of approaching potential donors for living kidney donation. The specific aim of this study is to identify the factors that influence the decision to pursue LDKT and compare across segments with different self-perceived health status.
To understand factors that influence interest in LDKT, a cross-sectional study was conducted using survey data collected from patients currently on dialysis. All protocols were approved by the Temple University Institutional Review Board (protocol number 11648).
Surveys were administered both in-person and online. For in-person administration, participants were recruited at two Pennsylvania urban hospital-based hemodialysis units and were approached in the hemodialysis units during their treatment. Online recruitment was done via a post on a private Facebook page dedicated to patients living with ESKD. A Qualtrics link was provide to members of the page and the link took them to the online version. Administration occurred over an 8 week period. All participants were provided information about the survey and its purpose, which was to understand perceptions of LDKT in those with ESKD.
The target population includes patients living with ESKD who are currently on dialysis. The accessible population includes patients living with ESKD who are currently on dialysis at two Pennsylvania urban hospital-based dialysis units or patients across the US engaged in a national, private Facebook group.
Participants were eligible if they were 18 or older and self-identified that they were currently on dialysis. The number who participated reflects a convenience sample of those who completed the survey in the time period.
The survey instrument was developed based on literature (Barnieh et al., 2009; Rodrigue et al., 2008; Barnieh et al., 2017), and our experience working with these populations (Gillespie et al., 2011; Gillespie et al., 2015; Traino et al., 2017). Kidney transplant specific questions included: self-reported health status, transplant candidacy status, years on dialysis, previous receipt of information about kidney transplant from a provider, previous experience asking someone to donate or being offered a kidney, history of kidney transplant (if applicable), and interest in receiving a LDKT and/or DDKT. The full instrument is provided in Supplement 1. Demographic information (gender, race, ethnicity, age, education level, insurance status, cohabitants, health literacy, and source of health information) was also collected via 10 multiple choice questions at the start of the survey. Health literacy was assessed with the Single Item Literacy Screener measure developed by Morris et al. (2006) by asking participants how confident they are filling out medical forms on their own. Five response options were consolidated into three levels of health literacy; often/always, sometimes, and never/rarely corresponded to high, moderate and low literacy, respectively.
Thirty items were developed for the perceptual mapping analysis, divided into five statement blocks to capture constructs important to the LDKT decision (Table 1), such as barriers, facilitators or beliefs. This is done so that perceptual maps can be constructed for each construct to aid in understanding potential persuasive messaging strategies and how the items are related to each other. Statement blocks included:
• Statement block 1: Seven items focused on concerns about approaching someone to discuss living donation of a kidney.
• Statement block 2: Six items centered on the risks of living donation to the donor.
• Statement block 3: Four items focused on benefits of receiving a kidney from a living donor compared to a deceased donor.
• Statement block 4: Six items focused on potential negative outcomes of transplantation.
• Statement block 5: Seven items that were positively framed reasons someone may not want a kidney transplant (i.e., satisfaction with current quality of life).

TABLE 1. LDKT survey statement blocks.
Participants responded to individual survey items by indicating how much they agree or disagree with each statement on a zero to 10 scale, with a zero indicating complete disagreement and 10 indicating complete agreement. A pictorial scale using “smiley faces” assisted the respondents in easily understanding the differences in the numbers of the scale and to encourage using numbers along the zero to 10 scale. The technique is simple to use and does not require respondents to make complex judgements about the statements, only how much they agree or disagree with each.
To confirm content validity, the draft survey was reviewed by a nephrologist and other professionals who work with dialysis patients. The instrument was pilot tested with 10 patients and modifications were made to ensure all items were distinct, understandable, and appropriate before full administration.
Descriptive statistics of the sample were done with SPSS v. 23 (IBM Corp, 2015). Perceptual mapping was used to support an understanding and visualization of the elements that facilitate and impede LDKT decision making and to assess how dialysis patients view the process of asking a potential donor for a kidney by their self-reported health status. This technique is widely applied in advertising and marketing and has been used by the authors to assess various public health decisions (Bass et al., 2012; Bass et al., 2016a; Bass et al., 2016b; Bass et al., 2016c; Bass et al., 2018a; Bass et al., 2018b).
Perceptual mapping was used to support an understanding and visualization of the elements that affect LDKT decision making among the three groups. The resulting maps produce a three-dimensional graphic display of how respondents perceive relationships among the items in each statement block. A multi-dimensional scaling software program created by the first author and based on the Galileo system as described by Woelfel and Fink (1980) converts the scaled judgments (i.e., zero to 10 scale on statements) into distances used in the mapping (Bass et al., 2018). Kruskal procedure forms the basis for the mathematical steps behind MDS, which uses the minimization of a cost function called “stress”, a measure of lack of fit between dissimilarities and distances (Buja et al., 2008). Stress is a residual sum of squares, where the outer square root is used to give greater spread to small values (Kruskal, 1964). To prepare data for input into the software, inter-item correlations of all elements are converted to a 0–10 scale base and “reflected” so that more important elements appear closer to the “self,” while those judged less important are farther away (Bass et al., 2016). The perceptual maps are then constructed with each element placed in the three-dimensional (mathematically n-dimensional) space based on its distance from (association with) the other concepts and from “Self.” In the maps, the “Self” variable is the aggregate of participants from that segment (i.e., self-perceived health status). The ability to construct and analyze maps for segmented representative subgroups is critical for extracting information needed for potential tailoring or targeting of messages in interventions.
The program then makes these associations and integrates them into a visual representation of the data, rather than into the usual statistical tables presented in survey studies. The maps thus provide a visual summary of the participants’ conceptualization of the situation, identifying the relative significance of various risks and benefits influencing the LDKT decision. This scaling method has been validated using physical space domain; if distances between American cities are entered into the program, a map that shows the cities in proper relative positions to each other is constructed with very little error (SSTRESS = 0.003) (Shiffman et al., 1981). Methodological details about the techniques used in this study are available at the first author’s website (Bass, 2021).
In-person participants were approached in the hemodialysis unit during their hemodialysis treatment. Informed consent was obtained in the treatment area and participants were given the option to take the survey themselves or have it administered to them by research staff. If opting for self-administration, the participant was given a clipboard, pen and paper survey and research staff were available to answer any questions. If opting for staff administration, research staff sat with the patient and verbally asked questions and entered responses on a paper copy of the survey. Online participants self-administered the survey in a location of their choosing with their own device. By clicking the Qualtrics survey link, online participants were prompted to read a description of the research containing required elements of consent; informed consent was indicated by proceeding to and completing the survey. No incentives were offered for participation.
The full sample (n = 160) was split between online (n = 126) and in-person (n = 34) participants. Sixty one percent of participants were female, with a mean age of 51 years. Sixty three percent had some post-secondary education or less (e.g., associate degree). The largest racial group represented was White (65%), following by African American/Black (24%); 7% identified as “other” or chose not to answer. Ninety-one percent identified as non-Hispanic/Latino. Thirty nine percent of participants had multiple health insurance types (e.g., Medicare and Medicaid), 24% had received a kidney transplant in the past but were currently on dialysis, and on average participants had been on dialysis for 6 years. Sixty-four percent indicated they had undergone evaluation for kidney transplant and 47% noted they were on a waiting list for a deceased donor kidney. Seventy percent expressed interest in receiving a live donor kidney transplant, 17% were not interested, 12% were unsure and 1% was missing. Twenty-nine percent considered their health to be at a poor or fair level (Table 2). A cross tab of health status by interest in LDKT indicated interest in LDKT was evenly distributed (χ 2.23; p = 0.321; not shown).
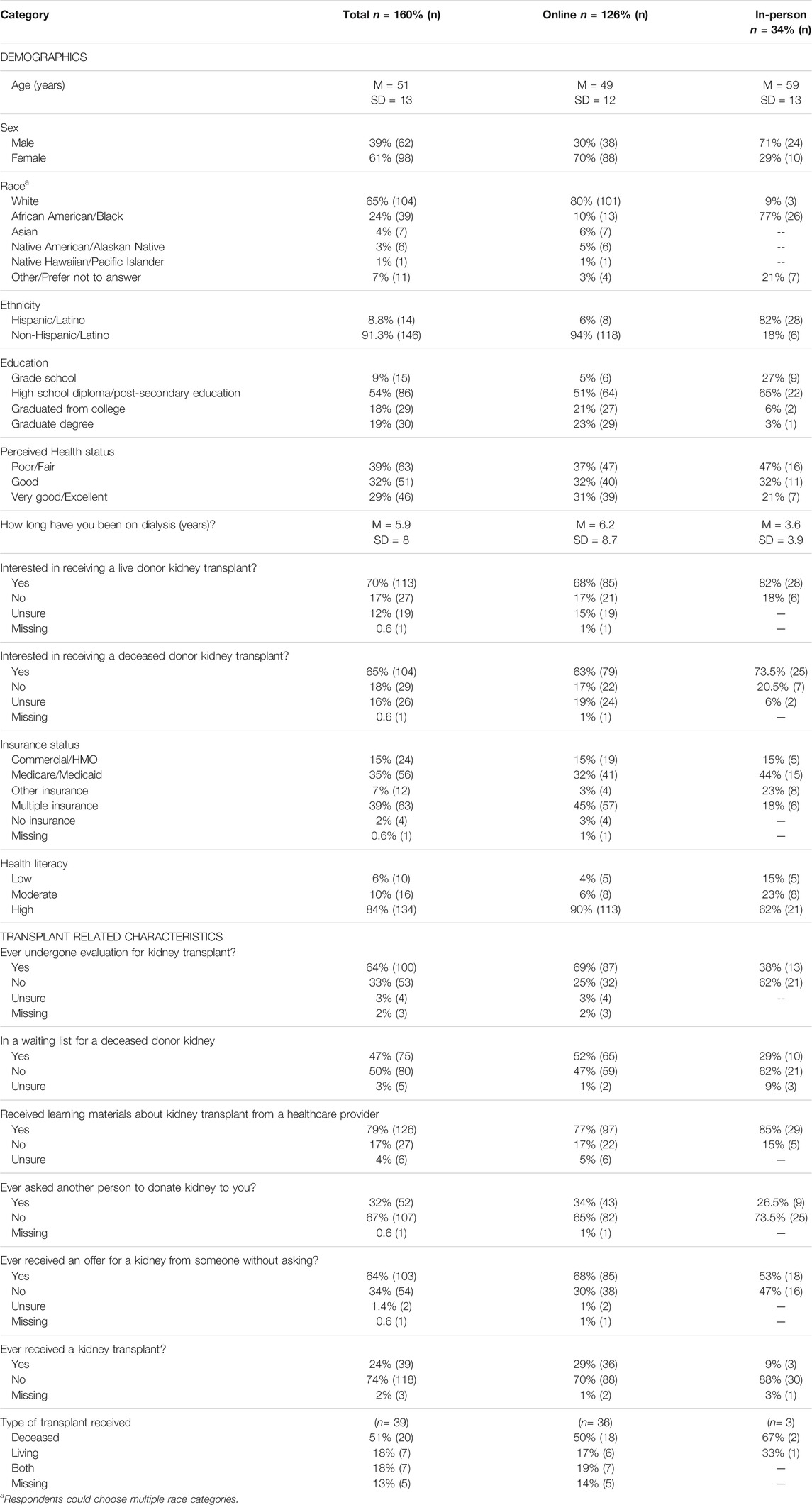
TABLE 2. Characteristics of participants.
Figures 1–3 are the perceptual maps for the first four statement blocks. Block five is not presented because there were no specific differences seen. The group “Self” variable is shown as a star. This variable represents all the participants’ responses in that group. Green boxes represent specific variables from the statement blocks that are closest to “Self”. These items are those most important to the group. Red boxes indicate items farther away from “Self” and thus not considered as important. Each map visually represents how respondents in each self-reported health status group relate to perceived risks and benefits of LDKT, as well as how participants perceive the variables related to one another.
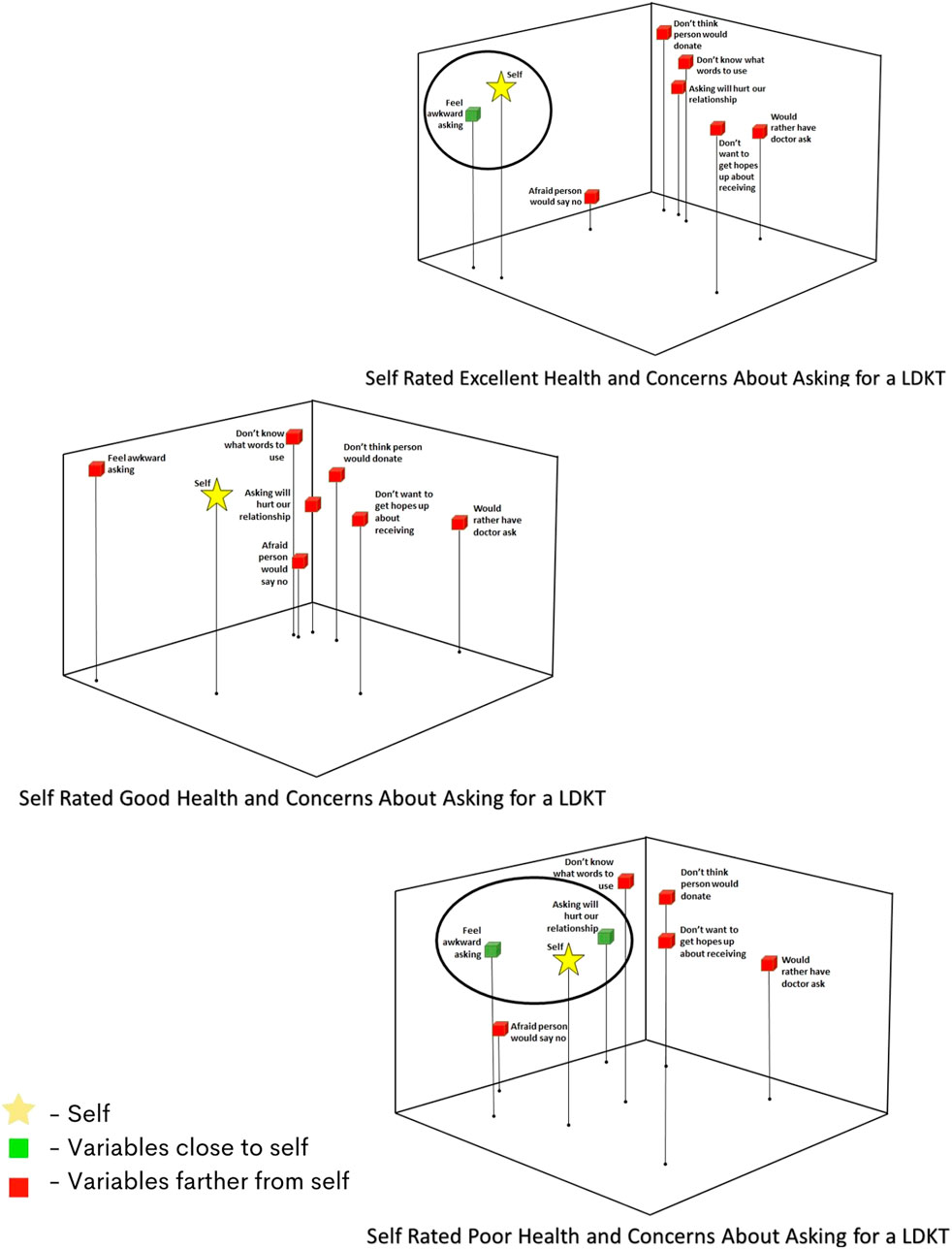
FIGURE 1. Perceptual maps for concerns about asking for LDKT by self-reported health status.
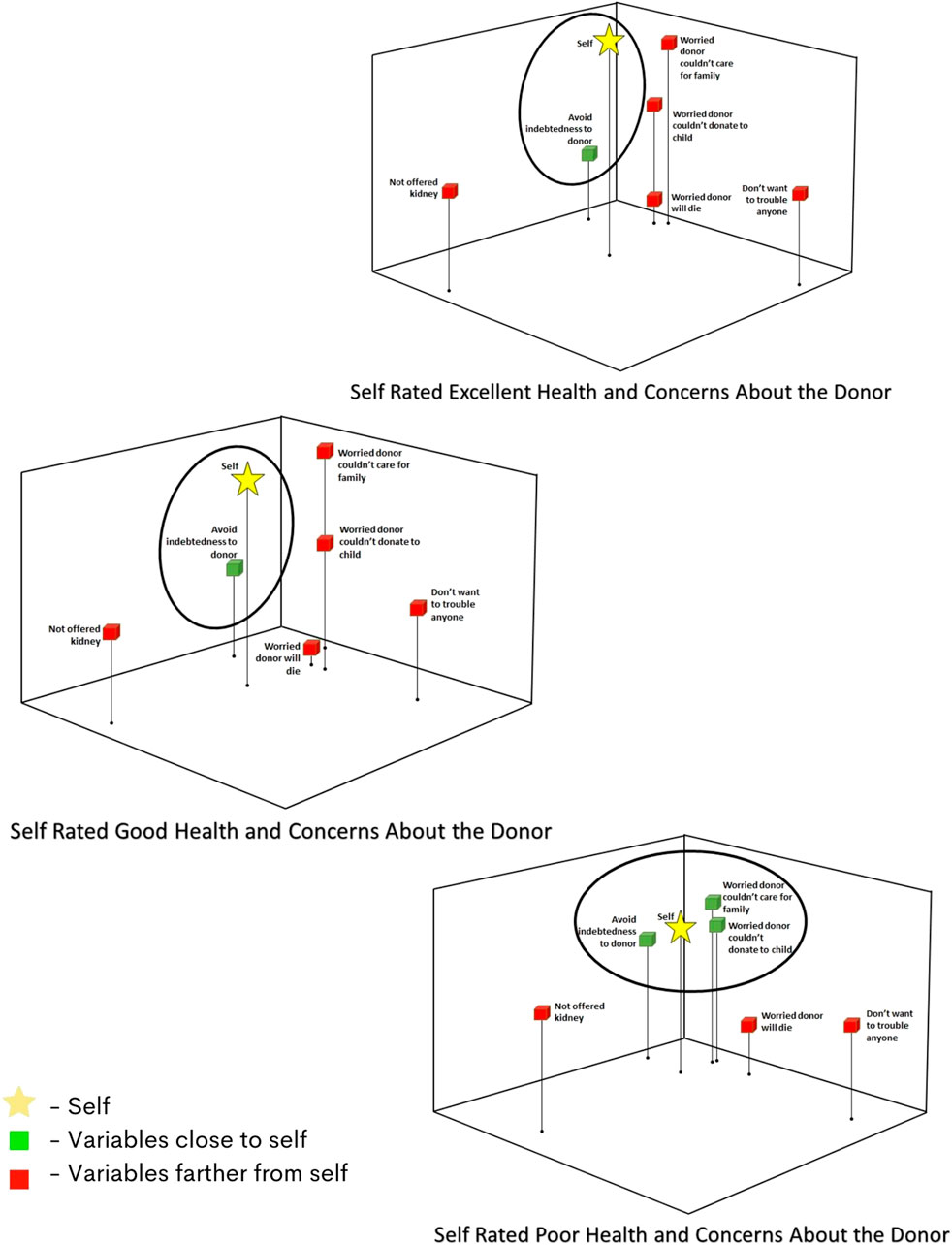
FIGURE 2. Perceptual maps for concerns about the donor by self-reported health status.
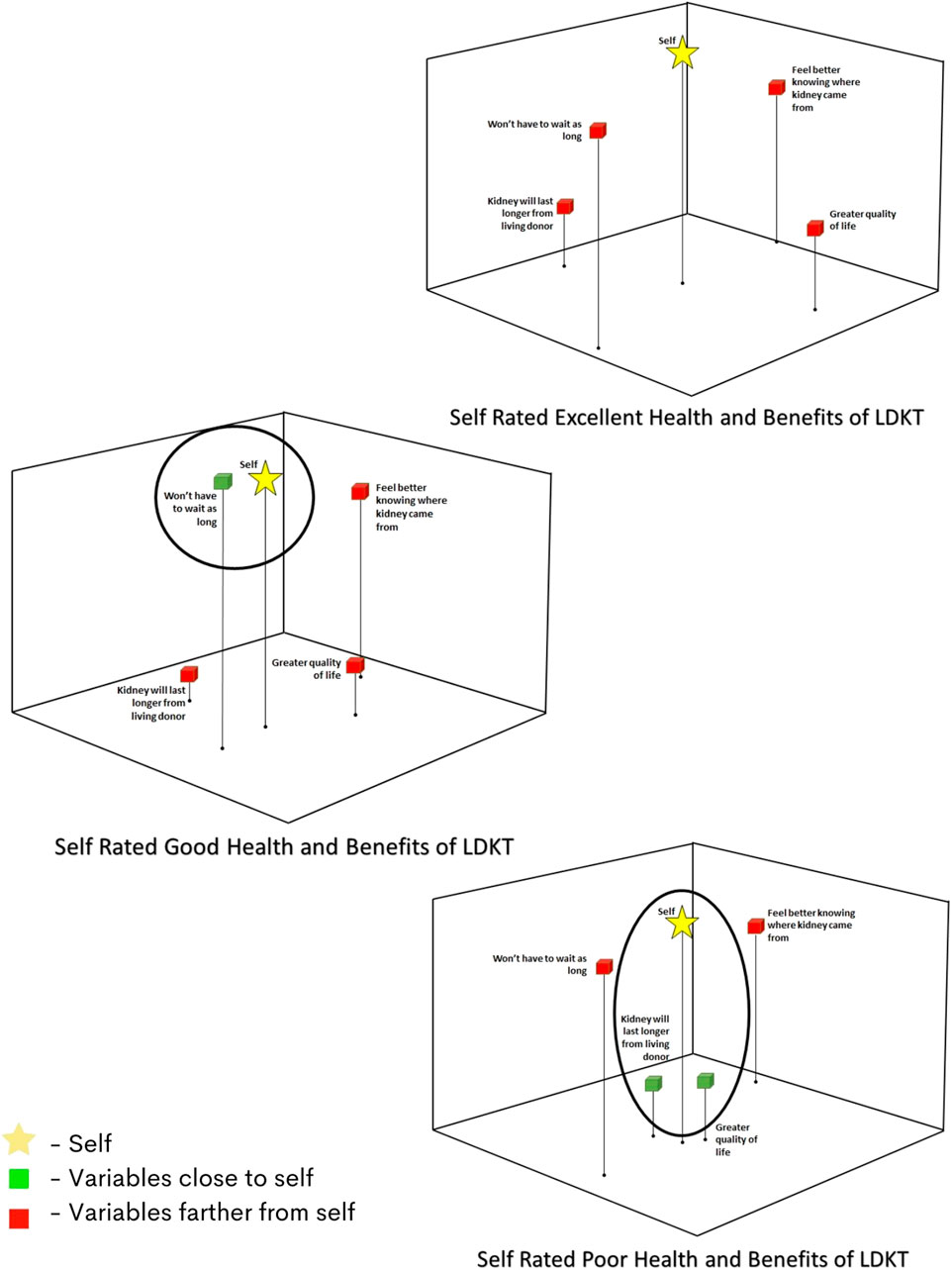
FIGURE 3. Perceptual maps for benefits of LDKT by self-reported health status.
Self-reported health status was defined as excellent or very good health (“excellent”), good health (“good”), and fair or poor health (“poor”). Across the three groups in the concerns about asking for a LDKT, “Self” is closest to feeling awkward approaching someone about a kidney. However, based on the positioning of “Self” and the “awkward” item, those with the best health more closely identify with feeling awkward about making an approach. This is also the only item from the block that is close to “Self” for those with excellent health. For those with poor health, on the other hand, “Self” is positioned more closely with issues of “being afraid that the person they speak to will say no”. They are also closer to the variable of “don’t know what words to use” (Figure 1).
When considering factors related to concerns about the donor, maps of those with poor health show “Self” and factors related to concern about the donor’s family much closer together than on maps of those with better self-reported health. Concerns about the donor’s family include worries that the donor would not be able to care for their family and that the donor would not be able to donate a kidney to a child or family member. Among healthier participants, these worries are not as close to “Self”. Another notable difference between groups is that while those with poor health relate equally to worry about the ability to care for their family and worry about the ability to make a future donation to a child or family member, those with better self-reported health more strongly identify with the concern of being indebted to the person who is donating (Figure 2).
Figure 3 illustrates benefits to LDKT across the groups. Those with self-reported excellent health are not close to any benefit variable in the map. Those with self-reported good health are closest to the concept of “won’t have to wait as long” for a transplant. Those with self-reported poor health, however, note two different concepts—that the kidney “will last longer” and the LDKT will give them a better quality of life. These variables are not close in the other two groups.
When considering barriers to LDKT (Figure 4), “Self” is positioned closest to the risk of ending up back on dialysis after transplant for all self-reported health status groups. This distance is shortest among those with the worst perceived health. Although not closely positioned to “Self” among participants in any health status, it is notable that worries about not surviving surgery and fear of pain from surgery are concepts that participants identify as conceptually related to one another. The strength of this grouping of risk concepts is strongest among those with the best perceived health and weakens as perceived health status decreases.
This study offers a unique graphic representation of patients’ cognitions about LDKT and donation as they relate to self-reported health status. An examination of the distances from the group “Self” and other concepts support several findings from past research, including patients’ struggles finding the best way to communicate their need for a kidney transplant and requesting living donation, and concerns about the well-being of potential donors (Alvaro et al., 2008; Weng et al., 2010). However, these analyses extend our understanding of patient-level facilitators and barriers to LDKT by further elucidating relationships among concepts related to living donation, and how they are alike or different based on self-reported health status. Other studies have noted potential differences in willingness to ask for or accept a donated kidney by gender (Gillespie et al., 2014; Gill et al., 2018), but our findings did not note a difference once you used the perceptual mapping analysis, which looks at how participants are looking at all the variables simultaneously. This supports the idea of looking beyond demographic variables to create messaging and findings could be important to developing patient level interventions that assist them in the request process.
One noteworthy finding was that patients’ concerns extended beyond risks to potential donors to include donors’ family and the ability of living donors to care for immediate family members. Thus, while potential donors give primacy to the short-term risks of donating in their decision making (Traino et al., 2016), potential recipients appear to take the long-term risks into consideration when making the decision to recruit potential donors. We also found group differences in the barriers and benefits of LDKT. While those interested in LDKT were evenly distributed across the three health-status groups, we see differences in perceived benefits of LDKT in those with self-reported poor health. This may indicate that this group especially could benefit from intervention in helping them think through the decision of whether and how to request a kidney.
Importantly, this study also used segmentation to provide a richer description of how the benefits and barriers of LDKT are conceptualized by an affected population. Use of segmentation to define subgroups with similar characteristics has been a common tool of commercial marketing (Morris and Schmolze, 2006; Lefebvre, 2013), and in health communication strategies in public health (Gordon et al., 2014), but have not often been used in intervention content development, especially in a clinical setting. However, segmentation can be useful in taking a seemingly homogenous group (i.e., all people on dialysis) and uncovering important attitudinal, personality, or behavioral variations that could make intervention content and messaging different. In this case, we looked at differences beyond simple demographics by examining perceived health status. This can be easily assessed in a clinical setting via a short survey. Customized training or intervention with patients to assist them with requesting LDKT based on these findings could be a useful and important contribution to both clinical practice and future research.
The multidimensional analyses identified important differences in perceptual maps by these segments. For instance, the distance between “Self” and concerns about approaching potential donors about living donation decreased with worsening health. Respondents reporting their health as excellent had generalized feelings of discomfort or “awkwardness” associated with the idea of talking to another person about donating a kidney. Feeling awkward about making approaches for living donation was a barrier to progressing along the steps to LDKT. However, the primary concerns of respondents reporting poor health turned to more logistical and content-related matters, such as concerns about refusals, not having the right words to say, or being afraid that asking would hurt the relationship. These go beyond feeling “awkward” to concerns about the process and outcome. While all the groups were concerned about feeling indebted to the donor, those reporting poorer health were also concerned about the donor being able to care for the family or not being able to donate in the future to a child. It is possible that, as a patient’s health declines and the time on dialysis awaiting a deceased donor kidney increases, an increasing sense of urgency for a transplant motivates a more nuanced consideration of requesting live donation. Patients may be more aware of the potential long-term consequences to the donor and not want the donor to be in a similar circumstance to them. These patients may have also made donation requests and have first-hand experience with these challenges, which then becomes an additional barrier to future conversations.
Differences in perceptual maps were also found in benefits and positively framed reasons for someone to not have a LDKT. Interestingly, those reporting excellent health saw no direct benefit to them to have a LDKT. Those with good and poor health believe that a benefit of LDKT was not having to wait as long for the kidney. An additional benefit for those with poorer health was the belief that an LDKT would provide a better quality of life. This is important, as current messaging about LDKT may not resonate with those who perceive their health as “excellent” and it may be harder to convince them to discuss LDKT with loved ones. Finally, it is important to note that all the groups believed that they were knowledgeable of the risks and benefits of LDKT, which may or may not be true. This indicates that more specific challenges—such as concerns about the conversation and about the donor - are far more important to whether they might be willing to approach a donor about an LDKT in the future than simply providing education on advantages of LDKT.
Challenges communicating the need for a transplantable kidney and low levels of knowledge about the risks and benefits of living donation are in fact well-known barriers to patients’ progress toward LDKT (Rodrigue et al., 2008; Lefebvre, 2013; DePasquale et al., 2021). In addition to providing validation to those findings, the utility of our multidimensional analyses lies in the implications to the development of messages to promote active pursuit of living donors (i.e., making requests for live donation). The maps depicting perceptions of approaching donors across the three levels of health status (Figure 3) indicate differential placement of the concepts in these maps, supporting the need for segmentation and the development of distinct messages for patients in each segment or category. These differences could be integrated into an intervention by assessing for perceived health status and content tailored to a patients’ needs, for example focusing more on the logistics of initiating a conversation about LDKT in those with perceived lower health status. The perceptual mapping method can thus provide a more nuanced look at how best to develop the message content that can increase “readiness” to pursue LDKT and motivate substantive behavior changes toward the receipt of LDKT (Rodrigue et al., 2014). In addition, because communication is transactional, another avenue for study would be to compare LDKT perceptions in those who have agreed to be live donors, or even those who have rejected requests to be a donor. This would allow researchers to understand how messages created for the requester might or might not be persuasive to the potential donor.
Our findings should be considered in light of some limitations. Our study was subject to selection bias, as those who chose to participate may not be representative of the target population, which could result in the misidentification of influential factors. This study was unfunded and the sample, by necessity, was one of convenience. Our sample primarily consisted of African American and White patients, while the burden of ESKD lies within African American and Hispanic communities [United States Renal Data System (USRDS, 2019)]. Although this lowers the generalizability of these findings, this study represents an initial attempt to visualize and segment cognitions about LDKT. Future research using these methods should attempt to secure a more diverse sample. The majority of respondents completed the survey online and we identified some demographic differences in this group. However, no significant differences in the maps were found between those groups, indicating similar response patterns across the groups. Approximately half of the sample reported being on the deceased donor transplant waiting list an average of 6 years, slightly higher than the median of 4.5 years (USRDS, 2021). Some may also have been ineligible for transplant; 11% reported their doctor had told them they could not get a transplant. In addition, we did not ask whether the respondent was on hemodialysis or peritoneal dialysis or both. While these issues may have affected responses, it is important to identify patients’ barriers to transplant and the use of perceived health status allowed for interesting comparisons across groups. Finally, the sample did include those who had previously had a kidney transplant, including some who had had a LDKT. These respondents may have answered items differently based on their personal experience with transplantation. However, all respondents were currently on dialysis and had significant negative health outcomes due to ESKD.
Understanding subtle differences in barriers and facilitators to approaching potential donors for a living donor kidney by a patient’s self-reported health status could be important to developing salient messaging that would assist patients with communicating their wishes with family and friends. With the growing public health need for diversity in options for those suffering from ESKD, this study’s findings can be used to develop more effective interventions to increase the number of live donor transplantations.
Reasonable requests for the data set used and analyzed during the current study are available from the corresponding author.
The studies involving human participants were reviewed and approved by the Temple University IRB. The patients/participants provided their written informed consent to participate in this study.
SB oversaw, conceptualized and designed the investigation and analyzed and interpreted the findings. SB was the primary author of the manuscript. IH interpreted the findings and contributed to writing the manuscript. PK contributed to developing the original draft of the background literature review as well as overall editing and preparation of visual elements. MA and PD’A conducted analyses. LM was involved with data collection and manuscript revisions. AG and DS provided resources for the investigation, interpreted findings, and reviewed the manuscript. HG conceptualized and validated the findings and was a contributor to writing the manuscript.
The authors declare that the research was conducted in the absence of any commercial or financial relationship that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Alvaro, E., Siegel, J., Turcotte, D., Lisha, N., Crano, W., and Dominick, A. (2008). Living Kidney Donation Among Hispanics: A Qualitative Examination of Barriers and Opportunities. Prog. Transplant. 18 (4), 243–250. doi:10.1177/152692480801800406
Arriola, K. R. J., Powell, C. L., Thompson, N. J., Perryman, J. P., and Basu, M. (2014). Living Donor Transplant Education for African American Patients with End-Stage Renal Disease. Prog. Transpl. 24 (4), 362–370. doi:10.7182/pit2014830
Barnieh, L., McLaughlin, K., Manns, B., Klarenbach, S., Yilmaz, S., and Hemmelgarn, B. (2009). Amp; Alberta Kidney Disease NetworkDevelopment of a Survey to Identify Barriers to Living Donation in Kidney Transplant Candidates. Prog. Transpl. 19 (4), 304–311. doi:10.1177/152692480901900404
Barnieh, L., Collister, D., Manns, B., Lam, N. N., Shojai, S., Lorenzetti, D., et al. (2017). A Scoping Review for Strategies to Increase Living Kidney Donation. Clin. J. Am. Soc. Nephrol. 12 (9), 1518–1527. doi:10.2215/CJN.01470217
Bass, S. B., Gordon, T. F., Ruzek, S. B., Wolak, C., Ruggieri, D., Mora, G., et al. (2012). Developing a Computer Touch-Screen Interactive Colorectal Screening Decision Aid for a Low-Literacy African American Population. Health Promot. Pract. 14 (4), 589–598. doi:10.1177/1524839912463394
Bass, S. B., Gordon, T. F., Maurer, L., Greener, J., Mora, G., Ruggieri, D., et al. (2016a). How Do Low-Literacy Populations Perceive "Dirty Bombs"? Implications for Preparedness Messages. Health Security 14 (5), 331–344. doi:10.1089/hs.2016.0037
Bass, S. B., Muñiz, J., Gordon, T. F., Maurer, L., and Patterson, F. (2016b). Understanding Help-Seeking Intentions in Male Military Cadets: An Application of Perceptual Mapping. BMC Public Health 16 (1), 413. doi:10.1186/s12889-016-3092-z
Bass, S. B., Wolak, C., Greener, J., Tedaldi, E., Nanavati, A., Ruppert, K., et al. (2016c). Using Perceptual Mapping Methods to Understand Gender Differences in Perceived Barriers and Benefits of Clinical Research Participation in Urban Minority HIV+ Patients. AIDS Care 28 (4), 528–536. doi:10.1080/09540121.2015.1112352
Bass, S. B., Jessop, A., Gashat, M., Maurer, L., Alhajji, M., and Forry, J. (2018a). Take Charge, Get Cured: The Development and User Testing of a Culturally Targeted mHealth Decision Tool on HCV Treatment Initiation for Methadone Patients. Patient Educ. Couns. 101 (11), 1995–2004. doi:10.1016/j.pec.2018.07.007
Bass, S. B., Jessop, A., Maurer, L., Gashat, M., Al Hajji, M., and Gutierrez, M. (2018b). Mapping the Barriers and Facilitators of HCV Treatment Initiation in Methadone Maintenance Therapy Patients: Implications for Intervention Development. J. Health Commun. 23 (1), 117–127. doi:10.1080/10810730.2017.1414902
Bass, S. B. (2021). Temple University Risk Communication Laboratory Methods. Available at: https://sites.temple.edu/turiskcommlab/methods. (Accessed December 20, 2021).
Boulware, L. E., Sudan, D. L., Strigo, T. S., Ephraim, P. L., Davenport, C. A., Pendergast, J. F., et al. (2021). Transplant Social Worker and Donor Financial Assistance to Increase Living Donor Kidney Transplants Among African Americans: The TALKS Study, a Randomized Comparative Effectiveness Trial. Am. J. Transpl. 21 (6), 2175–2187. doi:10.1111/ajt.16403
Buja, A., Swayne, D. F., Littman, M. L., Dean, N., Hofmann, H., and Chen, L. (2008). Data Visualization with Multidimensional Scaling. J. Comput. Graphical Stat. 17 (2), 444–472. doi:10.1198/106186008X318440
Cabacungan, A. N., Ellis, M. J., Sudan, D., Strigo, T. S., Pounds, I., Riley, J. A., et al. (2020). Associations of Perceived Information Adequacy and Knowledge with Pursuit of Live Donor Kidney Transplants and Living Donor Inquiries Among African American Transplant Candidates. Clin. Transpl. 34, e13799. doi:10.1111/ctr.13799
Cameron, L., and Leventhal, H. (2003). The Self-Regulation of Health and Illness Behavior. New York: Routledge.
Davis, L. A., Grogan, T. M., Cox, J., and Weng, F. L. (2017). Inter- and Intrapersonal Barriers to Living Donor Kidney Transplant Among Black Recipients and Donors. J. Racial Ethnic Health Disparities 4 (4), 671–679. doi:10.1007/s40615-016-0270-8
DePasquale, N., Ellis, M. J., Sudan, D. L., Ephraim, P. L., McElroy, L. M., Mohottige, D., et al. (2021). African Americans' Discussions about Living‐Donor Kidney Transplants with Family or Friends: Who, what, and Why Not? Clin. Transpl. 35 (4), e14222. doi:10.1111/ctr.14222
Gill, J., Joffres, Y., Rose, C., Lesage, J., Landsberg, D., Kadatz, M., et al. (2018). The Change in Living Kidney Donation in Women and Men in the United States (2005-2015): A Population-Based Analysis. J. Am. Soc. Nephrol. 29 (4), 1301–1308. doi:10.1681/ASN.2017111160
Gillespie, A., Hammer, H., Lee, J., Nnewihe, C., Gordon, J., and Silva, P. (2011). Lack of Listing Status Awareness: Results of a Single-center Survey of Hemodialysis Patients. Am. J. Transplanationt 11 (7), 1522–1526. doi:10.1111/j.1600-6143.2011.03524.x
Gillespie, A., Hammer, H., Kolenikov, S., Polychronopoulou, A., Ouzienko, V., Obradovic, Z., et al. (2014). Sex Differences and Attitudes toward Living Donor Kidney Transplantation Among Urban Black Patients on Hemodialysis. Clin. J. Am. Soc. Nephrol. 9 (10), 1764–1772. doi:10.2215/CJN.12531213
Gillespie, A., Hammer, H., Bass, S. B., Ouzienko, V., Obradovic, Z., Urbanski, M., et al. (2015). Attitudes towards Living Donor Kidney Transplantation Among Urban African American Hemodialysis Patients: A Qualitative and Quantitative Analysis. J. Health Care Poor Underserved 26 (3), 852–872. doi:10.1353/hpu.2015.0087
Gillespie, A., Fink, E. L., Traino, H. M., Uversky, A., Bass, S. B., Greener, J., et al. (2017). Hemodialysis Clinic Social Networks, Sex Differences, and Renal Transplantation. Am. J. Transpl. 17 (9), 2400–2409. doi:10.1111/ajt.14273
Gillespie, A., Fink, E. L., Gardiner, H. M., Gadegbeku, C. A., Reese, P. P., and Obradovic, Z. (2021). Does Whom Patients Sit Next to during Hemodialysis Affect whether They Request a Living Donation? Kidney360 2 (3), 507–518. doi:10.34067/KID.0006682020
Gordon, T. F., Bass, S. B., Ruzek, S. B., Wolak, C., Rovito, M. J., Ruggieri, D. G., et al. (2014). Developing a Typology of African Americans with Limited Literacy Based on Preventive Health Practice Orientation: Implications for Colorectal Cancer Screening Strategies. J. Health Commun. 19 (11), 1259–1277. doi:10.1080/10810730.2013.872725
Gozdowska, J., Zatorski, M., Torchalla, P., Białek, Ł., Bojanowska, A., Tomaszek, A., et al. (2016). Living-donor versus Deceased-Donor Kidney Transplantation: Comparison of Psychosocial Consequences for Recipients. Transplant. Proc. 48 (5), 1498–1505. doi:10.1016/j.transproceed.2016.01.075
IBM Corp (2015). IBM SPSS Statistics for Windows. (Version 23.0). [Computer software]. Armonk, NY: IBM Corp.
Kruskal, J. B. (1964). Nonmetric Multidimensional Scaling: A Numerical Method. Psychometrika 29 (2), 115–129. doi:10.1007/bf02289694
Landreneau, K., Lee, K., and Landreneau, M. D. (2010). Quality of Life in Patients Undergoing Hemodialysis and Renal Transplantation-Aa Meta-Analytic Review. Nephrol. Nurs. J. 37 (1), 37–44.
LaPoint, R. D., Geatrakas, S., Armenti, J., Tomback, A., Khaim, R., Porcello, L., et al. (2018). Increasing Living Donation by Implementing the Kidney Coach Program. Clin. Transpl. 33 (2), e13471. doi:10.1111/ctr.13471
Lefebvre, R. C. (2013). “Segmentation and Competition,” in Social Marketing and Social Change: Strategies and Tools for Improving Health, Well-Being, and the Environment. Editor R. C. Lefebvre (San Francisco, CA: John Wiley & Sons), 123–155.
Leventhal, H., Leventhal, E. A., and Cameron, L. (2001). “Representations, Procedures, and Affect in Illness Self-Regulation: A Perceptual-Cognitive Model,” in Handbook of Health Psychology. Editors A. Baum, T. Revenson, and J. Singer (Mahwah, NJ: Lawrence Erlbaum Associates), 19–48.
Leventhal, H. (2004). “Conceptualizing the Behavioral Process for Managing the Phasic and Tonic Features of Chronic Illness: A Contextualized Self-Regulation Approach,” in SAGE Handbook of Health Psychology. Editors S. Sutton, A. Baum, and M. Johnson (Thousand Oaks, CA: SAGE Publications), 60, 431–433.
Morgan, M. G., Fischhoff, B., Bostrom, A., and Atmanm, C. J. (2001). Risk Communication: A Mental Models Approach. Cambridge, England: Cambridge University Press.
Morris, L., and Schmolze, R. (2006). Consumer Archetypes: A New Approach to Developing Consumer Understanding Frameworks. J. Advertising Res. 46 (3), 289–300. doi:10.2501/S0021849906060284
Morris, N. S., MacLean, C. D., Chew, L. D., and Littenberg, B. (2006). The Single Item Literacy Screener: Evaluation of a Brief Instrument to Identify Limited reading Ability. BMC Fam. Pract. 7, 21. doi:10.1186/1471-2296-7-21
OPTN/UNOS (2021). Transplants by Donor Type: U.S. Transplants Performed. January 1, 1988 – April 30, 2021. Available at: https://optn.transplant.hrsa.gov/data/view-data-reports/national-data/#. (Accessed December 20, 2021).
Purnell, T. S., Hall, Y. N., and Boulware, L. E. (2012). Understanding and Overcoming Barriers to Living Kidney Donation Among Racial and Ethnic Minorities in the United States. Adv. Chronic Kidney Dis. 19 (4), 244–251. doi:10.1053/j.ackd.2012.01.008
Rodrigue, J., Cornell, D., Kaplan, B., and Howard, R. (2008). Patients' Willingness to Talk to Others about Living Kidney Donation. Prog. Transplant. 18 (1), 25–31. doi:10.1177/152692480801800107
Rodrigue, J. R., Paek, M. J., Egbuna, O., Waterman, A. D., Schold, J. D., Pavlakis, M., et al. (2014). Readiness of Wait-Listed Black Patients to Pursue Live Donor Kidney Transplant. Prog. Transpl. 24 (4), 355–361. doi:10.7182/pit2014337
Sajjad, I., Baines, L. S., Salifu, M., and Jindal, R. M. (2007). The Dynamics of Recipient-Donor Relationships in Living Kidney Transplantation. Am. J. Kidney Dis. 50 (5), 834–854. doi:10.1053/j.ajkd.2007.07.029
Sandal, S., Charlebois, K., Fiore, J. F., Wright, D. K., Fortin, M.-C., Feldman, L. S., et al. (2019). Health Professional-Identified Barriers to Living Donor Kidney Transplantation: A Qualitative Study. Can. J. Kidney Health Dis. 6, 205435811982838. doi:10.1177/2054358119828389
Shiffman, S., Reynolds, M., and Young, F. (1981). Introduction to Multidimensional Scaling: Theory, Methods, and Applications. Academic Press.
Stothers, L., Gourlay, W. A., and Liu, L. (2005). Attitudes and Predictive Factors for Live Kidney Donation: A Comparison of Live Kidney Donors versus Nondonors. Kidney Int. 67 (3), 1105–1111. doi:10.1111/j.1523-1755.2005.00176.x
Traino, H. M., Nonterah, C. W., Gupta, G., and Mincemoyer, J. (2016). Living Kidney Donors' Information Needs and Preferences. Prog. Transpl. 26 (1), 47–54. doi:10.1177/1526924816633943
Traino, H. M., West, S. M., Nonterah, C. W., Russell, J., and Yuen, E. (2017). Communicating about Choices in Transplantation (COACH). Prog. Transpl. 27 (1), 31–38. doi:10.1177/1526924816679844
Traino, H. M. (2014). Communication Self-Efficacy, Perceived Conversational Difficulty, and Renal Patients' Discussions about Transplantation. Patient Educ. Couns. 94 (2), 180–186. doi:10.1016/j.pec.2013.10.012
United States Renal Data System (2019). 2019 ADR Reference Tables. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases. Available at: https://www.usrds.org/reference.aspx. (Accessed December 20, 2021).
United States Renal Data System (2021). Incidence, Prevalence, Patient Characteristics, and Treatment Modalities. National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases. Available at: https://adr.usrds.org/2020/end-stage-renal-disease/1-incidence-prevalence-patient-characteristics-and-treatment-modalities. (Accessed December 20, 2021).
Waterman, A. (2021). ExploreTransplant. Available at: https://exploretransplant.org/. (Accessed December 20, 2021).
Weng, F. L., Reese, P. P., Mulgaonkar, S., and Patel, A. M. (2010). Barriers to Living Donor Kidney Transplantation Among Black or Older Transplant Candidates. Clin. J. Am. Soc. Nephrol. 5 (12), 2338–2347. doi:10.2215/CJN.03040410
Weng, F. L., Peipert, J. D., Holland, B. K., Brown, D. R., and Waterman, A. D. (2017). A Clustered Randomized Trial of an Educational Intervention during Transplant Evaluation to Increase Knowledge of Living Donor Kidney Transplant. Prog. Transpl. 27 (4), 377–385. doi:10.1177.152692481773202110.1177/1526924817732021
Keywords: living donor kidney transplantation, end-stage kidney disease, segmentation analysis, perceptual mapping analysis, patient-provider communication
Citation: Bass SB, Hollin IL, Kelly PJ, Alhajji M, D’Avanzo P, Maurer L, Gillespie A, Schatell D and Gardiner H (2022) Perceptions of Live Donor Kidney Transplantation Using Segmentation Analysis and Perceptual Mapping to Understand Differences by Self-Reported Health Status in People on Dialysis. Front. Commun. 6:785186. doi: 10.3389/fcomm.2021.785186
Received: 28 September 2021; Accepted: 13 December 2021;
Published: 05 January 2022.
Edited by:
Victoria Team, Monash University, AustraliaReviewed by:
Maria Beatriz Torres, Mercyhurst University, United StatesCopyright © 2022 Bass, Hollin, Kelly, Alhajji, D’Avanzo, Maurer, Gillespie, Schatell and Gardiner. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Sarah Bauerle Bass, c2Jhc3NAdGVtcGxlLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.