 Yojiro Umezaki
Yojiro Umezaki Akiko Yamashita
Akiko Yamashita Fusanori Nishimura
Fusanori Nishimura Toru Naito1†
Toru Naito1†
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMIC REVIEW article
Front. Clin. Diabetes Healthc. , 25 February 2025
Sec. Diabetes Multiorgan Complications
Volume 6 - 2025 | https://doi.org/10.3389/fcdhc.2025.1541145
This article is part of the Research Topic Diabetes and Oral Health View all 3 articles
Background: Diabetes mellitus (DM) is linked to complications such as retinopathy, nephropathy, neuropathy, and cardiovascular disease, impacting patient quality of life and increasing healthcare costs. Periodontal disease, more prevalent in diabetic patients, is associated with worsened glycemic control and systemic inflammation, suggesting a possible bidirectional relationship. While some studies indicate periodontal treatment may improve glycemic control and reduce inflammation, overall evidence is inconsistent. It remains unclear if periodontal therapy reliably enhances diabetes outcomes or if certain patient subgroups benefit more than others.
Objective: To systematically review randomized controlled trials (RCTs) evaluating the effects of periodontal therapy on glycemic control (HbA1c) and systemic inflammation (CRP) in type 1 and type 2 diabetes patients.
Methods: Following PRISMA guidelines, a comprehensive PubMed search identified RCTs comparing HbA1c and CRP outcomes in diabetic patients with periodontal therapy versus controls. Inclusion criteria required at least three to six months of follow-up. Meta-analyses using a random effects model were conducted for HbA1c and CRP changes.
Results: Eleven studies met inclusion criteria. Meta-analyses showed significant reductions in HbA1c at three months (-0.64; CI95%=-0.96 to -0.32; I2 = 73%) and six months (-0.33; CI95%=-0.65 to -0.01; I2 = 12%). CRP also declined significantly, indicating an improvement in systemic inflammation.
Conclusion: Periodontal therapy appears to significantly reduce HbA1c and CRP levels over short-term periods in diabetic patients, suggesting potential as a beneficial adjunct to diabetes management. These findings support incorporating periodontal care into diabetes treatment to reduce systemic inflammation and potentially lower healthcare costs. Future long-term, standardized RCTs are needed to confirm sustained effects and investigate responses in diverse patient populations.
Diabetes mellitus is known to cause complications such as retinopathy, nephropathy, and neuropathy, and is also known to be involved in the onset and progression of arteriosclerotic diseases such as ischemic heart disease and stroke. These complications not only significantly reduce the quality of life of patients, but also impose a heavy medical and economic burden on society, for which countermeasures are required.
In the oral cavity, periodontal disease is also recognized as a complication because of its high frequency in diabetic patients, and many studies have been conducted on the relationship between diabetes and periodontal disease. The “Guidelines for Periodontal Treatment of Diabetic Patients, Revised Third Edition 2023,” (1) published by the Japanese Society of Periodontology, states that diabetic patients, whether type 1 or type 2, have a significantly higher incidence of periodontal disease than non-diabetic patients. A meta-analysis of cohort studies on the bidirectional association between periodontal disease and diabetes reported a 24% increased incidence of periodontal disease in diabetic patients and a 26% increased relative risk of developing diabetes in patients with periodontitis (2). A recent review by the European Federation of Periodontology (EFP) and the American Academy of Periodontology (AAP) (3) also found that those with periodontitis were more likely to develop type 2 diabetes (hazard ratio 1.19-1.33) than those without the disease. In other words, type 1 and type 2 diabetics are significantly more likely to develop periodontal disease than non-diabetics.
Diabetes has also been shown to be a risk factor involved in the progression of periodontal disease. For example, cross-sectional studies examining the relationship between duration of diabetes and periodontal disease have shown that attachment loss is greater and periodontal disease worsens when duration of type 1 and type 2 diabetes exceeds 5 years (4, 5).
In a study of 7042 U.S. National Nutrition Examination Survey (NHANES III) (6) physical examiners with periodontal examination findings and fasting blood glucose data, the HbA1c of patients with periodontal disease was 5.9, compared with 5.6 in patients without periodontal disease and 5.6 in patients with diabetes mellitus. In a study of the relationship between glycemic control status and periodontal disease, the HbA1c of patients with periodontal disease was 5.9, compared with 5.6 in patients without periodontal disease. In the case of diabetic patients, the HbA1c values increased to 7.4 and 7.0 in periodontal patients and non-diabetic patients, respectively, and the condition of periodontal tissues deteriorated in patients with HbA1c≥8.0 in terms of glycemic control status. In addition, previous reports also showed that the glycemic control status of periodontal tissues deteriorated in patients with HbA1c≥8.0. In an earlier report (7), the risk of periodontitis was 2.9 times higher in type 2 diabetics with extremely poor glycemic control (HbA1c > 9%) than in non-diabetics, but there was no statistically significant difference in the risk in patients with HbA1c ≤ 9%, although there was a trend toward more advanced periodontitis than in non-diabetics. Furthermore, it has been shown that the risk of alveolar bone resorption is higher in very poor type 2 diabetics with HbA1c ≥ 9% (8). With regard to glycemic control in type 1 diabetes, it has been reported that alveolar bone resorption is more common in poorly glycemic controlled diabetics compared to those with good glycemic control (9).
On the other hand, the relationship between improvement of diabetes and periodontal treatment is controversial. Grossi et al. (10) reported that periodontal therapy improved diabetes in a randomized control trial, and many other reports have been published, but some reports (11, 12) showed that the effect of periodontal therapy on diabetes is negative. In this study, we conducted a systematic review of previous reports on the improvement of diabetes mellitus and periodontal treatment.
This systematic review adhered to the Preferred Reporting Items for Systematic Reviews and Meta-analysis (PRISMA) guidelines (13). The PICO question we investigated in this review was formed according to the rules of PRISMA.
“Do the patients with Type 2 Diabetes Mellitus (P) with periodontal therapy (I), compared to without treatment (C), improve HbA1c (O1) or CRP (O2).”
Studies were included, if they (1) were randomized controlled studies (2); included patients over the age of 20 (3); observed at least 3 or 6 months. Studies were excluded if they (1) did not report on any of the predefined outcomes (2); were animal studies (3); were inadequate article types, such as notes, reviews, letters or conference abstracts (4); had high risk of bias.
For this review, a PubMed search was first conducted, and in filtering, the literature was narrowed down using Clinical Trial, considering the nature of this clinical question. The complete search key used was the following: (“Periodontitis” [MeSH Terms] OR “Periodontal Diseases” [MeSH Terms]) AND (“Diabetes Mellitus” [MeSH Terms]) AND (“Glycemic Control” [All Fields] OR “Hemoglobin A1c [MeSH Terms]) AND (“Periodontal Therapy” [All Fields]) AND (“Intervention” [All Fields]), filters: (“Humans”, “English” and “Clinical trial”). The databases were screened on Sep 1, 2021.
For references that were deemed appropriate for inclusion in the PubMed search, we further reviewed similar articles in PubMed, examined the titles of references cited in the article, and conducted additional literature searches. The final pool of included studies was decided upon completing the full-text selection procedure.
Two authors independently extracted the required data. The following information was collected: first, the year of publication; second, the authors’ names; and third, the study title. Data on changes in HbA1c, CRP, PCR, BoP, and PPD were compiled. Some studies also reported hs-CRP results, which were extracted as well. The results and conclusions of each study were summarized to facilitate easier comparison and make the findings more readily accessible. Quality assessment was conducted in accordance with Cochrane guidelines (14). Any disagreements between the two authors were resolved through discussion with the corresponding author to reach a consensus.
We assessed changes in HbA1c levels and CRP from baseline to post-treatment as primary outcomes, reflecting treatment-related improvement. Weighted mean difference and corresponding 95% confidence intervals (CI) were calculated by the forest plot. A random effect model was employed, and studies were weighed by a classical inverse variance method (15). Heterogeneity was examined using I2 value. Review Manager (Revman) version 5.4 for Windows from Cochrane collaboration was used to perform all analyses. Statistical significance has been defined as a P value < 0.05.
From the systematic search 77 articles were retrieved and assessed by title and abstract selection. Conducting the full text selection, 11 RCTs fulfilled the eligibility criteria and were processed for data extraction. The databases were screened on Sep 1, 2021. No additional eligible studies were found at the manual hand searches of the reference lists. The detailed selection procedure can be found in Figure 1. The characteristics of the 11 RCTs were shown in Table 1. Among them, 10, 6, 2 and 2 studies reported 3-months outcomes for HbA1c, 6-months outcomes for HbA1c, 3-months outcomes for CRP and 6-months outcomes for CRP, respectively. There were 3 studies (19, 24, 25) that compared three groups between two kinds of treatment and controls. Two (19, 25) of these studies manually combined the treatment groups and considered 2-group comparisons. In the remaining study (24), one of the subgroups was not considered clinically meaningful, so we excluded the corresponding group and dealt with as a two-group comparison.
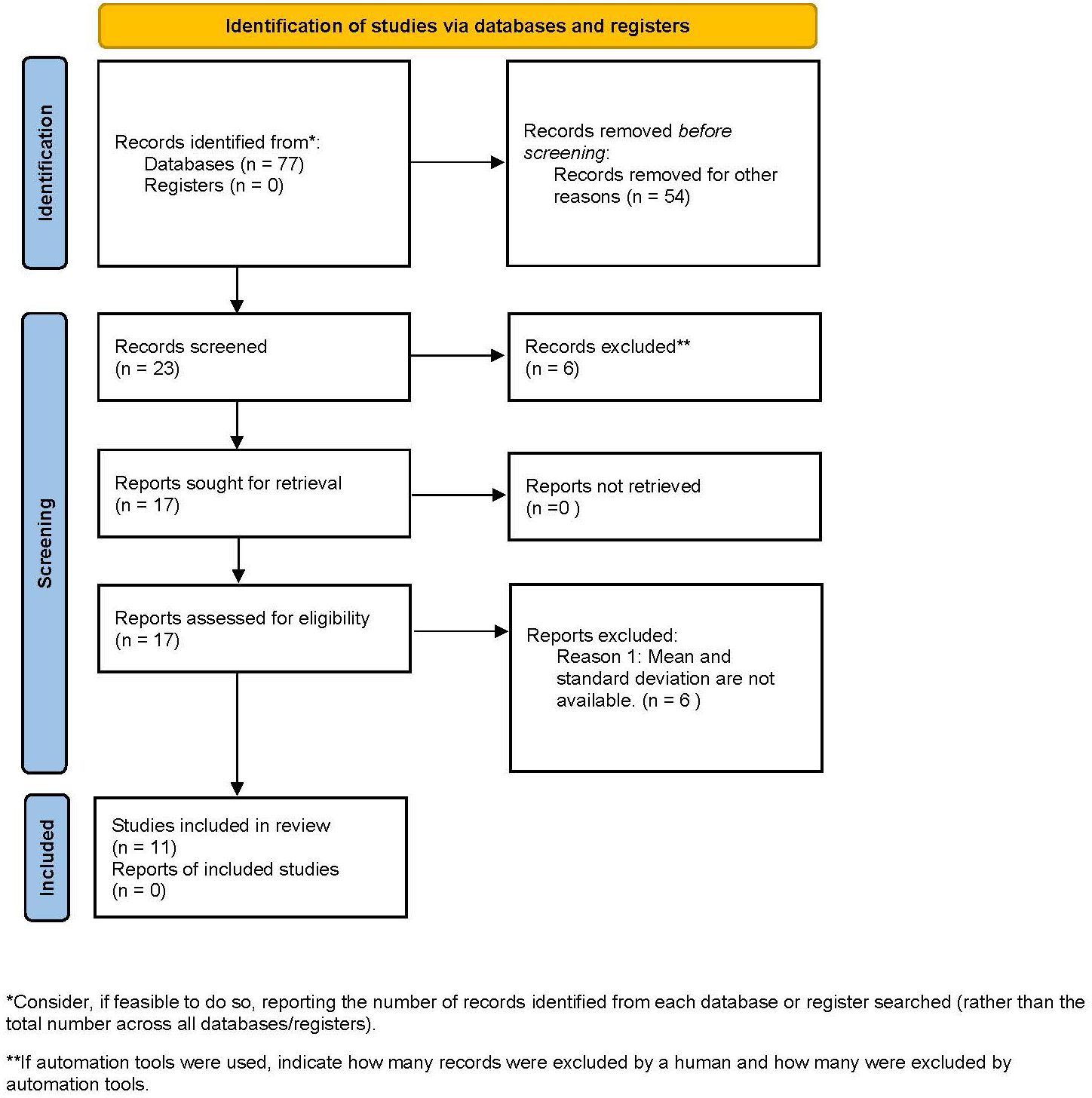
Figure 1. Flow chart of the literature search and screening process.
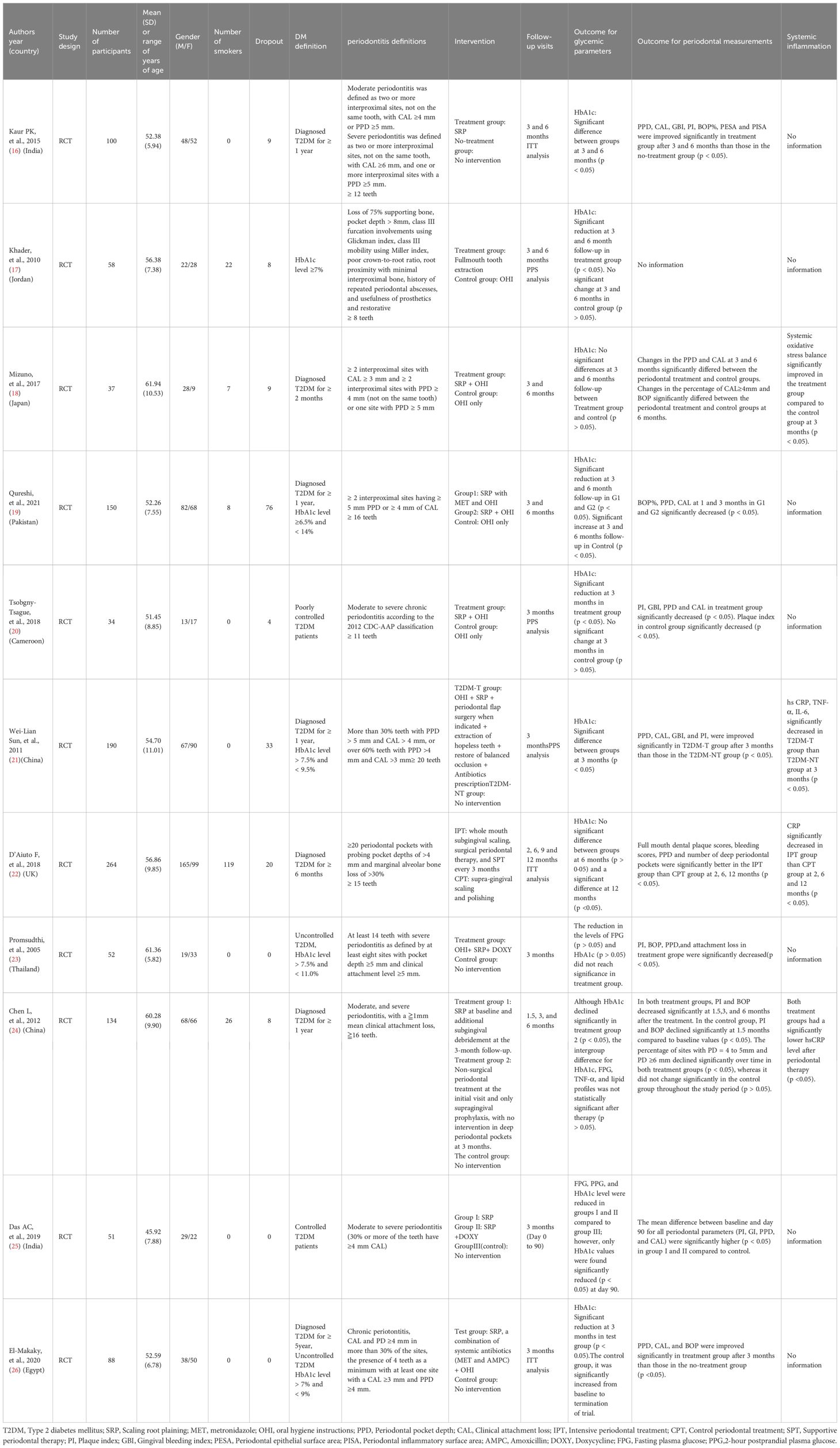
Table 1. Study characteristics (n=11).
In studies with 3-months follow-up time for the change of HbA1c, the number of patients ranged from 30 (20) to 190 (21) with medically diagnosed type 2 DM. Mean age ranged from 45.9 (25) to 61.9 (18) years, and proportion of females varied from 24.3% (18) to 63.5% (23). Six studies did not include smokers, but other 4 studies included smokers ranging from 5.3% (19) to 37.9% (17) of the participants. In most of the studies, the participants did not receive any periodontal treatment for at least 3 months, whereas 2 studies (17, 19) not providing its information. As for studies with 6 months follow-up time for the change of HbA1c, sample size was from 37 (18) to 264 (22). The mean age was ranging from 52.3 (19) to 61.9 (18) years old. Four studies had equal proportions of male and female participants, but 2 studies had relatively low proportions of female participants, 24.3% (18) and 37.5% (22), respectively. Most of studies included smokers ranging from 5.3% (19) to 45.1% (22), but a study excluded smokers (16). Three studies (16, 18, 24) excluded the patients receiving periodontal treatment prior at least 6 months, while the other studies had no information on it.
On the other hand, 2 studies reported 3 months follow-up for CRP. The number of patients were ranging from 134 (24) to 190 (21). The mean ages were 60.3 (24) and 54.7 (21). Both studies had similar ratios of male to female. And 2studies showed the result of the change of CRP for 6 months follow up. The sample size was from 134 (24) to 264 (22). The mean ages were 60.3 (24) and 56.9 (22) years old. Female ratios were 49.3% (24) and 37.5% (22).
Eight studies were classified as having a low risk of bias, while the remaining two studies were categorized as having some concerns. No study was identified as having a high risk of bias (Figure 2). Most trials detailed their randomization process, often utilizing computer-generated random numbers, permuted block method, and opaque envelopes for allocation concealment. The primary sources of potential bias were related to the lack of blinding of participants or personnel and the loss of follow-up data.
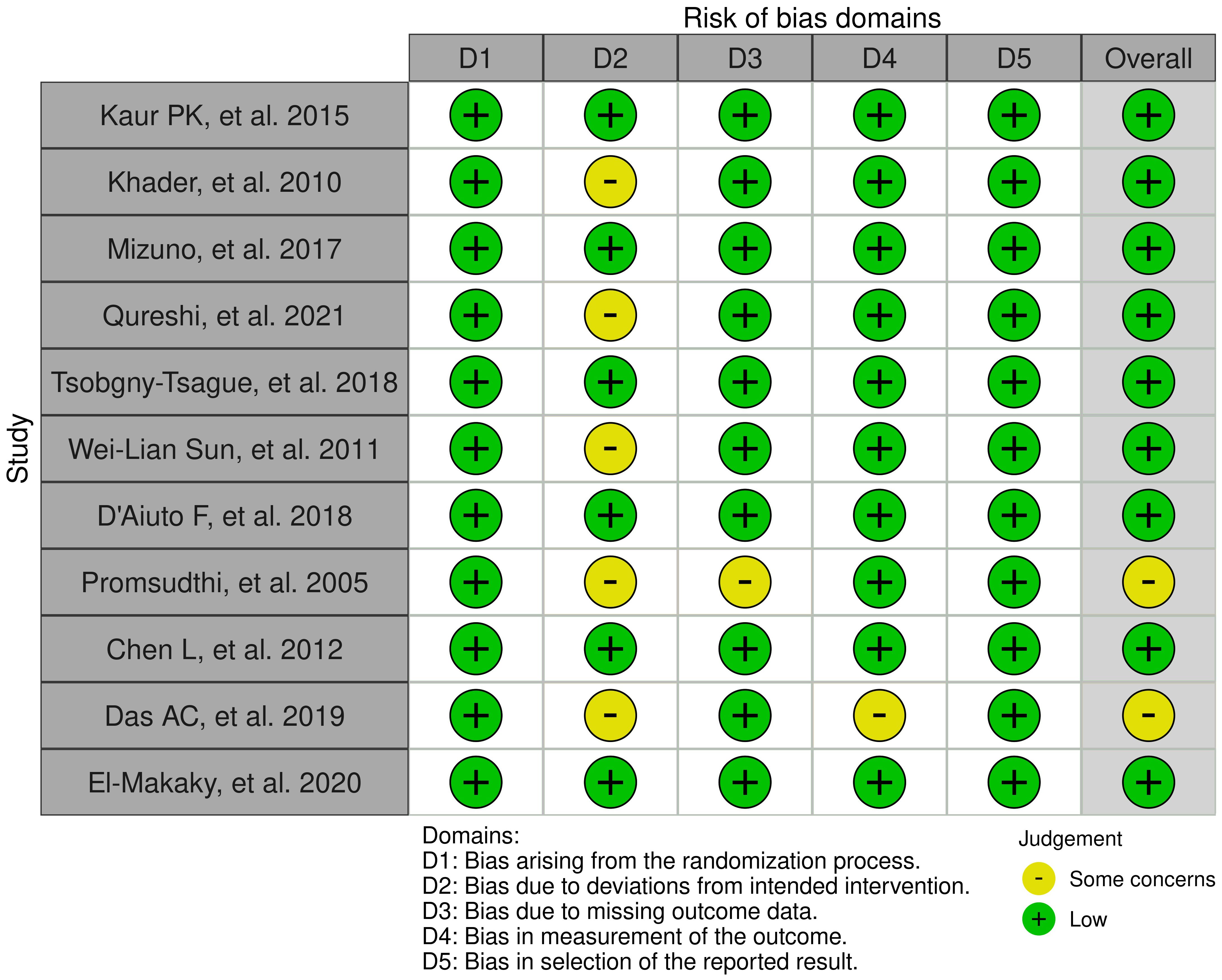
Figure 2. Summary of the risk of bias.
There were 10 studies included in the meta-analysis of HbA1c changes in 3 months (16–21, 23–26). A total of 332 subjects in the control group and 390 subjects in the treatment group were analyzed for changes of HbA1c levels using random effect model. There was a statistically significant difference between patients in control group and treatment group with a result of -0.64 (CI95%=-0.96; -0.32). The between study heterogeneity was considered moderate; I2 = 73% (Figure 3).
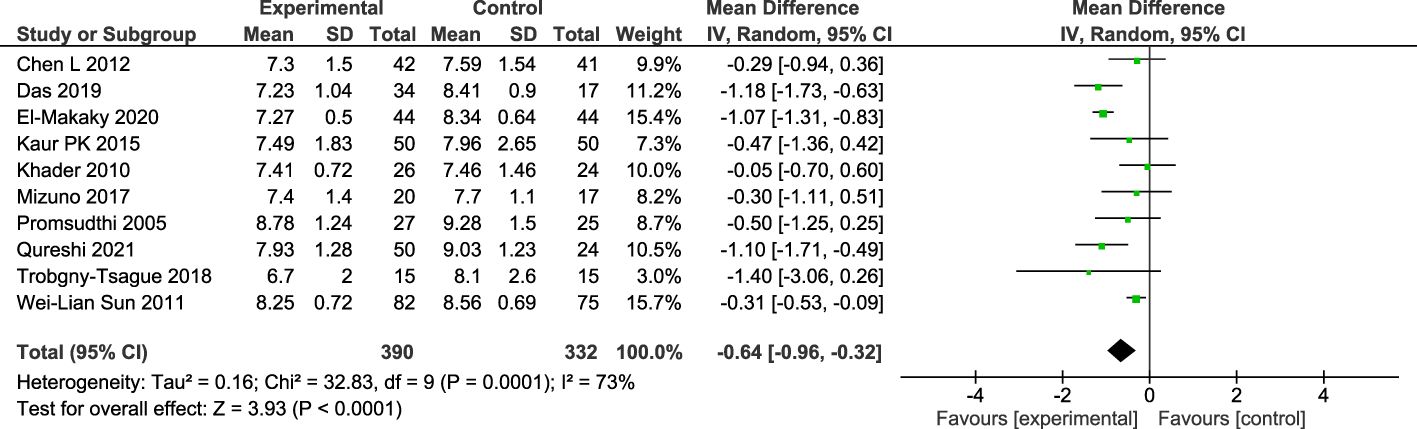
Figure 3. Forest plot for the change of HbA1c between baseline and 3-months follow-up.
As for 6 months changes in HbA1c, there were 6 studies (16–19, 22, 24) included in the meta-analysis. A total of 287 subjects in the control group and 321 subjects in treatment group were analyzed using random effect model. There was a statistically significant difference between patients in the control group and treatment group with a result of -0.33 (CI95%=-0.65; -0.01). The between study heterogeneity was considered low; I2 = 12% (Figure 4).
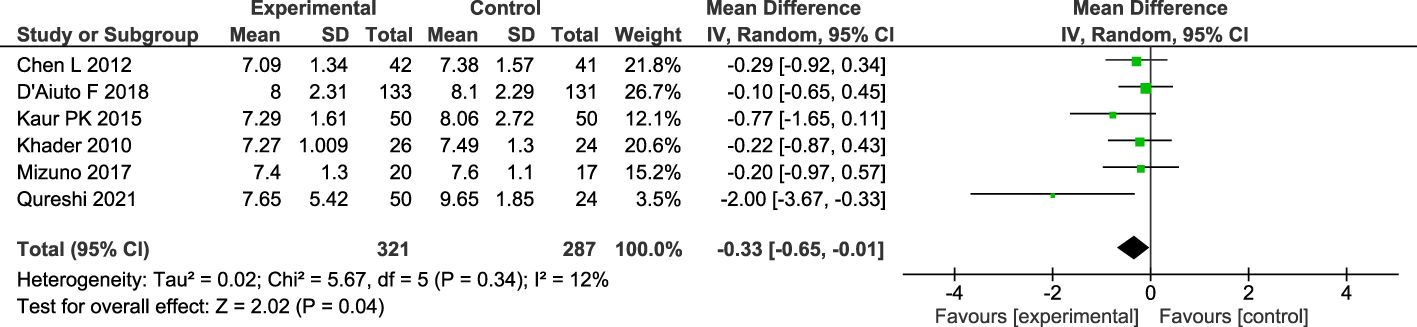
Figure 4. Forest plot for the change of HbA1c between baseline and 6-months follow-up.
There were 2 studies included in the meta-analysis of CRP changes in 3 months (21, 24). A total of 116 subjects in the control group and 124 subjects in treatment group were analyzed using random effect model. There was a statistically significant difference between patients in control group and treatment group with a result of -0.52 (CI95%=-0.86; -0.18). The between study heterogeneity was considered low; I2 = 0% (Figure 5).

Figure 5. Forest plot for the change of CRP between baseline and 3-months follow-up.
As for 6 months changes in CRP, there were 2 studies included in the meta-analysis of CRP changes in 6 months (22, 24). A total of 172 subjects in the control group and 175 subjects in treatment group were analyzed using random effect model. There was a statistically significant difference between patients in control group and treatment group with a result of -1.24 (CI95%=-1.76; -0.71). The between study heterogeneity was considered low; I2 = 0% (Figure 6).

Figure 6. Forest plot for the change of CRP between baseline and 6-months follow-up.
In the present systematic review and meta-analysis, it was concluded that periodontal initial treatment was beneficial for HbA1c levels and CRP of the patients with DM in the 3-months and 6-months follow-up period. When the screening of the literatures, 17 studies met the inclusion and exclusion criteria. During quality assessment process, there were 6 studies without available mean and standard deviation. 11 studies with available data were eventually included in the meta-analysis. Examining the individual studies that constitute the forest plot for the change of HbA1c at 3-months, some found that periodontal treatment significantly improved HbA1c (19, 21, 25, 26), while others did not achieve a significant difference (16–18, 20, 23, 24). This discrepancy in results was also observed for HbA1c at 6 months. However, by conducting a meta-analysis, we were able to consolidate the results of several articles and conclude that initial periodontal treatment led to a significant improvement in HbA1c. Similar to our study, the recent Cochrane report showed the effectiveness of periodontal therapy for reduction of HbA1c and CRP in type 1 and 2 diabetic patients (27). Different from the Cochrane report, our study included only type 2 diabetic patients. As for type 1 diabetes, there is no clear-cut report of HbA1c reduction by periodontal treatment, and it is classically known that elevated inflammatory markers such as CRP are related to insulin resistance (HOMA-IR) rather than insulin secretion capacity (HOIMA-β) (28). We therefore focused our study only on type 2 diabetes. We believe that this meta-analysis provided novel and clear-cut findings. We could not perform meta-analysis at the period of 12 months or longer because of lack of available data. However, a study observing changes in HbA1c and CRP at 12 months showed that improvements in HbA1c and CRP at 6 months persisted at 12 months (22), suggesting that the results of the meta-analysis at 6 months would persist at 12 months.
Removing the source of infection in the oral cavity by periodontal treatment not only improves periodontal condition and long-term prognosis of teeth, but also contributes to improvement of HbA1c without significant side effects. SRP is not a simple alternative for hypoglycemic drugs, but as a reference, we present an example of cost-effectiveness comparison as below. The cost of full-mouth SRP is about 15,000 yen (about 4,500 yen if 70% of the cost is covered by insurance) in Japan. In diabetic patients with severe periodontal disease, the improvement in HbA1c obtained with initial periodontal treatment has been reported to be generally around 0.5%. On the other hands, as to drug therapy, there are seven types of hypoglycemic drugs currently available in Japan. Among them, metformin, a biguanide (the first-line drug for diabetes treatment by the American Diabetes Association and the European Association for the Study of Diabetes) 1500 mg/day for 26 weeks has been reported to improve HbA1c by 0.56% (29). If metformin is used for 6 months, which is the most common period of reports for periodontal treatment and HbA1c, the prescription, dispensing, and drug costs would be approximately 20,214 yen (approximately 6,064 yen if 70% of the cost is covered by insurance). Thus, from a medico-economic point of view, the effect of periodontal treatment on diabetes might have significant advantages.
Periodontitis is a localized inflammatory condition that can trigger low-grade chronic inflammation. This occurs through the spread of periodontal bacteria via the bloodstream or the release of inflammatory mediators from periodontal tissues into circulation (30). As a result, it adds to the overall systemic inflammatory load, increasing the risk of various chronic diseases such as cardiovascular disease cardiovascular disease (CVD) (30), T2DM (31), kidney disease (32), cancer, and neurodegenerative disorders (33). Based on one possible mechanism mentioned above, the benefits of periodontal treatment are not limited to diabetes but are expected to spread to various inflammatory diseases in light of the principle that removal of the source of infection improves systemic inflammation. In fact, Luthra et al. (34) reviewed and concluded that treatment for periodontitis reduced CRP of various systemic inflammation disease at the 6-months timepoint. Our results, that periodontal treatment reduced both HbA1c and CRP, support the mechanism. However, since RCTs with longer follow-up periods are lacking, further studies will be required.
In this meta-analysis, intervention is integrated into periodontal treatment, but a detailed description reveals a mixture of treatments: some studies included SRP alone (16), others included SRP + OHI (18, 20, 23), others included SPR + OHI + MET (19, 26), and still others included periodontal surgery as indicated (21, 22). As for the control group, some studies included no intervention (16, 21, 23–25), while others included OHI (17–20). Particularly heterogeneous is the study by Khader et al. (17) in which full-mouth extractions were performed as intervention. This meta-analysis summarizes 10 RCTs on periodontal treatment for HbA1c reduction at 3 months, but even if the Khader paper were excluded from the analysis, the results of a significant reduction in HbA1c would still be validated (data not shown). In the future, a meta-analysis should be performed, if possible, to collect studies in which the intervention and control groups have more homogeneous conditions.
Several limitations should be noted. Firstly, pooled effects of meta-analysis could be influenced due to confounding factors, such as gender, experiences of periodontal therapy and BMI. However, there were limited studies that we could include in meta-analysis, we could not show the influence of them. Secondary, this meta-analysis only captured changes in diabetes-related items between the intervention and non-intervention groups, and did not provide detailed individualized classification of genetic or congenital responsiveness to periodontal treatment. Third, the data may be subject to error due to the mix of ITT and PPS analyses. More RCTs with a unified methodology are also needed in the future.
There is robust evidence indicating that periodontal treatment reduces HbA1c and CRP levels at the 3- and 6-month timepoints. It is suggested that periodontal treatment could be beneficial rather than existing pharmacotherapy for diabetes, both in terms of side effects and in terms of medico-economic point of view. Future research should determine whether (a) the systemic effects following periodontitis treatment are sustained over time and (b) these effects hold true when assessed using a standardized methodology.
YU: Data curation, Formal Analysis, Investigation, Methodology, Software, Visualization, Writing – original draft, Writing – review & editing. AY: Data curation, Investigation, Resources, Visualization, Writing – original draft, Writing – review & editing. FN: Conceptualization, Project administration, Supervision, Validation, Writing – original draft, Writing – review & editing. TN: Conceptualization, Formal Analysis, Funding acquisition, Methodology, Project administration, Resources, Software, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This study was supported in part by the JSPS KAKENHI (grant number 21K10292 and 17K12001).
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Periodontal treatment guidelines for patients with diabetes. Revised version 3. Tokyo: Ishiyaku Shuppan (2023).
2. Stöhr J, Barbaresko J, Neuenschwander M, Schlesinger SA-O. Bidirectional association between periodontal disease and diabetes mellitus: a systematic review and meta-analysis of cohort studies. Sci. Rep. (2021) 11:13686. doi: 10.1038/s41598-021-93062-6
3. Graziani F, Gennai S, Solini A, Petrini M. A systematic review and meta-analysis of epidemiologic observational evidence on the effect of periodontitis on diabetes An update of the EFP-AAP review. J. Clin. Periodontol. (2018) 45:167–87. doi: 10.1111/jcpe.12837
4. Al-Shammari KF, Al-Ansari JM, Moussa NM, Ben-Nakhi A, Al-Arouj M, Wang HL. Association of periodontal disease severity with diabetes duration and diabetic complications in patients with type 1 diabetes mellitus. J. Int. Acad. Periodontol. (2006) 8(4):109–14.
5. Cerda J, Vázquez de la Torre C, Malacara JM, Nava LE. Periodontal disease in non-insulin dependent diabetes mellitus (NIDDM). The effect of age and time since diagnosis. J. Periodontol. (1994) 65:991–5. doi: 10.1902/jop.1994.65.11.991
6. Garcia D, Tarima-S-Fau-Okunseri C, Okunseri C. Periodontitis and glycemic control in diabetes: NHANES 2009 to 2012. J. Periodontol. (2015) 86:499–506. doi: 10.1902/jop.2014.140364
7. Tsai C, Hayes C, Taylor GW. Glycemic control of type 2 diabetes and severe periodontal disease in the US adult population. Community Dent. Oral. Epidemiol. (2002) 30:182–92. doi: 10.1034/j.1600-0528.2002.300304.x
8. Taylor GW, Burt BA, Becker MP, Genco RJ, Shlossman M. Glycemic control and alveolar bone loss progression in type 2 diabetes. Ann. Periodontol. (1998) 3:30–9. doi: 10.1902/aape.1998.3.issue-1
9. Tervonen T, Karjalainen K, Knuuttila M, Huumonen S. Alveolar bone loss in type 1 diabetic subjects. J. Clin. Periodontol. (2000) 27:567–71. doi: 10.1034/j.1600-051x.2000.027008567.x
10. Grossi SG, Skrepcinski FB, DeCaro T, Robertson DC, Ho AW, Dunford RG, et al. Treatment of periodontal disease in diabetics reduces glycated hemoglobin. J. Periodontol. (1997) 68:713–9. doi: 10.1902/jop.1997.68.8.713
11. Jones JA, Miller DR, Wehler CJ, Rich SE, Krall-Kaye EA, McCoy LC, et al. Does periodontal care improve glycemic control? The Department of Veterans Affairs Dental Diabetes Study. J. Clin. Periodontol. (2007) 34(1):46–52. doi: 10.1111/j.1600-051X.2006.01002.x
12. Katagiri S, Nitta H, Nagasawa T, Uchimura I, Izumiyama H, Inagaki K, et al. Multi-center intervention study on glycohemoglobin (HbA1c) and serum, high-sensitivity CRP (hs-CRP) after local anti-infectious periodontal treatment in type 2 diabetic patients with periodontal disease. Diabetes Res. Clin. Pract. (2009) 83:308–15. doi: 10.1016/j.diabres.2008.10.016
13. Page MJ, McKenzie JE, Bossuyt PM, Boutron I, Hoffmann TC, Mulrow CD, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. (2021) 372:n71. doi: 10.1136/bmj.n71
14. Chandler J, Cumpston M, Li T, Page MJ, Welch V. Cochrane handbook for systematic reviews of interventions. Hoboken: Wiley (2019).
15. DerSimonian R, Laird N. Meta-analysis in clinical trials. Control Clin. Trials. (1986) 7:177–88. doi: 10.1016/0197-2456(86)90046-2
16. Kaur PK, Narula SC, Rajput R, Ks R, Tewari S. Periodontal and glycemic effects of nonsurgical periodontal therapy in patients with type 2 diabetes stratified by baseline HbA1c. J. Oral. Sci. (2015) 57:201–11.
17. Khader YS, Al Habashneh R, Al Malalheh M, Bataineh A. The effect of full-mouth tooth extraction on glycemic control among patients with type 2 diabetes requiring extraction of all remaining teeth: a randomized clinical trial. J. Periodontal Res. (2010) 45:741–7. doi: 10.1111/j.1600-0765.2010.01294.x
18. Mizuno H, Ekuni D, Maruyama T, Kataoka K, Yoneda T, Fukuhara D, et al. The effects of non-surgical periodontal treatment on glycemic control, oxidative stress balance and quality of life in patients with type 2 diabetes: A randomized clinical trial. PloS One. (2017) 12:e0188171. doi: 10.1371/journal.pone.0188171
19. Qureshi A, Bokhari SAH, Haque Z, Baloch AA, Zaheer S. Clinical efficacy of scaling and root planing with and without metronidazole on glycemic control: three-arm randomized controlled trial. BMC Oral. Health. (2021) 21:253. doi: 10.1186/s12903-018-0479-5
20. Tsobgny-Tsague NF, Lontchi-Yimagou E, Nana ARN, Tankeu AT, Katte JC, Dehayem MY, et al. Effects of nonsurgical periodontal treatment on glycated haemoglobin on type 2 diabetes patients (PARODIA 1 study): a randomized controlled trial in a sub-Saharan Africa population. BMC Oral. Health. (2018) 18:28. doi: 10.2169/internalmedicine.50.5166
21. Sun WL, Chen LL, Zhang SZ, Wu YM, Ren YZ, Qin GM. Inflammatory cytokines, adiponectin, insulin resistance and metabolic control after periodontal intervention in patients with type 2 diabetes and chronic periodontitis. Intern. Med. (2011) 50:1569–74. doi: 10.1371/journal.pone.0188171
22. D’Aiuto F, Gkranias N, Bhowruth D, Khan T, Orlandi M, Suvan J, et al. Systemic effects of periodontitis treatment in patients with type 2 diabetes: a 12 month, single-centre, investigator-masked, randomised trial. Lancet Diabetes Endocrinol. (2018) 6:954–65. doi: 10.1016/S2213-8587(18)30038-X
23. Promsudthi A, Pimapansri S, Deerochanawong C, Kanchanavasita W. The effect of periodontal therapy on uncontrolled type 2 diabetes mellitus in older subjects. Oral. Dis. (2005) 11:293–8. doi: 10.1111/j.1600-0765.2010.01294.x
24. Chen L, Luo G, Xuan D, Wei B, Liu F, Li J, et al. Effects of non-surgical periodontal treatment on clinical response, serum inflammatory parameters, and metabolic control in patients with type 2 diabetes: a randomized study. J. Periodontol. (2012) 83:435–43. doi: 10.1902/jop.2011.110327
25. Das AC, Das SJ, Panda S, Sharma D, Taschieri S, Fabbro MD. Adjunctive effect of doxycycline with conventional periodontal therapy on glycemic level for chronic periodontitis with type 2 diabetes mellitus subjects. J. Contemp Dent. Pract. (2019) 20:1417–23. doi: 10.2334/josnusd.57.201
26. El-Makaky Y, Shalaby HK. The effects of non-surgical periodontal therapy on glycemic control in diabetic patients: A randomized controlled trial. Oral. Dis. (2020) 26:822–9. doi: 10.1111/odi.13256
27. Simpson TC, Clarkson JE, Worthington HV, MacDonald L, Weldon JC, Needleman I, et al. Treatment of periodontitis for glycaemic control in people with diabetes mellitus. Cochrane Database Syst. Rev. (2022) 4:CD004714. doi: 10.1002/14651858.CD004714.pub4
28. Festa A, Hanley Aj, Tracy RP, D’Agostino R Jr, Haffner SM. Inflammation in the prediabetic state is related to increased insulin resistance rather than decreased insulin secretion. Circulation. (2003) 108:1822–30. doi: 10.1161/01.CIR.0000091339.70120.53
29. Umpierrez G, Tofe Povedano S, Perez Manghi F, Shurzinske L, Pechtner V. Efficacy and safety of dulaglutide monotherapy versus metformin in type 2 diabetes in a randomized controlled trial (AWARD-3). Diabetes Care. (2014) 37:2168–76. doi: 10.2337/dc13-2759
30. Tonetti MS, Van Dyke TE. Periodontitis and atherosclerotic cardiovascular disease: consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J. Periodontol. (2013) 84:S24–9. doi: 10.1111/jcpe.2013.40.issue-s14
31. Chapple IL, Genco R. Diabetes and periodontal diseases: consensus report of the Joint EFP/AAP Workshop on Periodontitis and Systemic Diseases. J. Periodontol. (2013) 84:S106–12. doi: 10.1111/jcpe.12077
32. Sharma P, Dietrich T, Ferro CJ, Cockwell P, Chapple IL. Association between periodontitis and mortality in stages 3-5 chronic kidney disease: NHANES III and linked mortality study. J. Clin. Periodontol. (2016) 43:104–13. doi: 10.1111/jcpe.2016.43.issue-2
33. Furman DA-O, Campisi J, Verdin EA-O, Carrera-Bastos P, Targ S, Franceschi C, et al. Chronic inflammation in the etiology of disease across the life span. Nat. Med. (2019) 25:1822–. doi: 10.1038/s41591-019-0675-0
Keywords: periodontology, diabetes mellitus, periodontal initial treatment, hemoglobinA1c, C-reactive protein
Citation: Umezaki Y, Yamashita A, Nishimura F and Naito T (2025) The role of periodontal treatment on the reduction of hemoglobinA1c, comparing with existing medication therapy: a systematic review and meta-analysis. Front. Clin. Diabetes Healthc. 6:1541145. doi: 10.3389/fcdhc.2025.1541145
Received: 07 December 2024; Accepted: 06 February 2025;
Published: 25 February 2025.
Edited by:
Zoe Xiaofang Zhu, Tufts University, United StatesCopyright © 2025 Umezaki, Yamashita, Nishimura and Naito. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Yojiro Umezaki, dW1lemFraUBmZGNuZXQuYWMuanA=
†ORCID: Yojiro Umezaki, orcid.org/0000-0003-0249-1977
Akiko Yamashita, orcid.org/0000-0001-8845-8048
Fusanori Nishimura, orcid.org/0000-0003-1572-2180
Toru Naito, orcid.org/0009-0004-1902-6726
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.