
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Clin. Diabetes Healthc. , 22 March 2022
Sec. Diabetes Health Services and Health Economics
Volume 3 - 2022 | https://doi.org/10.3389/fcdhc.2022.830183
This article is part of the Research Topic Highlights in Diabetes Health Services and Health Economics 2021/2022 View all 4 articles
 Elena Toschi1,2*
Elena Toschi1,2* Jennifer Leblanc1Samar Hafida1Sanjeev Mehta1
Jennifer Leblanc1Samar Hafida1Sanjeev Mehta1 Marilyn Ritholz1Robert Gabbay3
Marilyn Ritholz1Robert Gabbay3 Lori Laffel1,2
Lori Laffel1,2Aims: A multidisciplinary team of clinicians and researchers, patients and family members, and representative from national advocacy groups and research organization met to review the literature, highlight gaps, and identify best practices to improve adult care delivery for young adults (YA) with diabetes.
Methods: The participants prepared presentations in advance, rotated through sessions, and contributed to group discussions in three areas: physical health, mental health, and quality of life (QoL). Session moderators and scribes used thematic analysis to summarize discussions for each topic.
Results: Thematic analysis revealed four foci for addressing physical health, mental health and QoL: 1) best practices to facilitate the process of transfer; 2) age-specific curricula and guidelines for prevention and management of comorbidities and complications; 3) collaboration with behavioral health clinicians to address diabetes distress and mental health disorders; and 4) research on the impact of diabetes on QoL in YA.
Conclusion: There was substantial interest and need among adult clinicians to work in concert with pediatric and mental health professionals to identify best practices and future directions to improve healthcare process and diabetes-related outcome measures in YA with diabetes.
Young adults (YA) with diabetes often experience deterioration of glycemic control, a rise in hospitalizations for acute complications, and frequent loss of follow-up (1, 2). Young adulthood is a dynamic developmental stage of life where changes occur personally, socially, and emotionally. This developmental stage also entails increasing independence from parents, change in financial status, and potential onset of psychosocial issues and risk-taking behaviors (3). During this time, healthcare is often fragmented, especially upon transfer from pediatric to adult care settings (4). Importantly, clinical trials focusing on the transition process from pediatric to adult care in YA with diabetes have yet to identify a consistently successful pathway (5–7).
The current guidelines on the transition process from pediatric to adult care systems are limited and rely heavily on expert opinion (8). Moreover, many adult clinicians lack the developmental training to engage effectively with YA in need of support in their diabetes management. Further, an increased prevalence of behavioral challenges and psychiatric disorders that may interfere with diabetes self-care have been described in YA (9–11). Lastly, quality of life (QoL) is often poor in YA with diabetes (12). A multidisciplinary team of pediatric and adult-focused clinicians, researchers, persons with diabetes, family members, and representatives from national advocacy groups convened over a 2-day meeting to review the literature, highlight gaps, discuss best practices, and identify needs for future research to improve care delivery and outcomes for YA in adult care settings. This report is the summary of the salient findings and recommendations from this roundtable conference.
On December 5-7, 2019, the Joslin Diabetes Center organized and hosted a roundtable conference, gathering over 50 interdisciplinary thought leaders from the US and Canada to focus on delivering optimal care for YA with diabetes. The team included: pediatric endocrinologists (n=8), adult endocrinologists (n=20), family medicine physicians (n=2), nurse practitioners (n=2), nurses (n=2), certified diabetes educators (n=4), and behavioral health specialists (n=6). Many were also clinical researchers with a focus on the transition period and care of YA in adult care. Persons with diabetes, family members, and representatives from national advocacy groups and funding organizations (JDRF, ADA, Helmsley Charitable Trust, NIH, CDN, NIDDK, and the Endocrine Society) also participated in the roundtable discussions.
Three moderators were assigned to lead discussions focused on one of three sessions: 1) promoting physical health (SH), 2) optimizing mental health (MDR), and 3) preserving quality of life (SM). All participants were divided into three cohorts and rotated through each of the three topic areas. In addition, three other facilitators (LML, JL, ET) accompanied a single cohort through all three topic areas. Each session lasted two hours. Participants were asked in advance to prepare a 10-minute power-point presentation based on their experience, research, clinical approaches, and/or literature review related to Assessment, Engagement, or Intervention of one topic (physical health, mental health, or quality of life).
Following each presentation, there was a 30-minute group discussion led by the moderator and accompanying facilitator. More than 80% of the clinical participants presented a topic during the sessions. Participants contributed to group discussions in all three areas. Scribes were present in each group to take notes.
Following the day of group sessions, the session moderator, scribe, and facilitator met to discuss session findings based on the content of the presentations and the scribes’ notes to identify common themes by consensus. The next day, session moderators presented the themes to all participants for further discussion and derived consensus on each topic.
We present a summary of themes identified from the presentations and discussions that occurred over the 2-day meeting of interdisciplinary participants. The 3 topics included: 1) promoting physical health, 2) optimizing mental health, and 3) preserving quality of life. In addition, the process of transfer of care from pediatric to adult care settings became a fundamental topic for discussion during the 2-day meeting and is presented first.
The process of transfer of care, defined as “the planned, purposeful movement of young adults from child-centered to adult-oriented healthcare systems” (4), occurs during a time of change and maturation. Currently, this process remains challenging and the few randomized control studies focusing on this process have yielded little improvement in appointment attendance and glycemic control (5–7).
The participants identified three major gaps in the process of transfer: 1) a defined, straightforward, uniform process to facilitate communication between pediatric and adult clinicians, 2) clinical tools to assess maturation and readiness of YA; and 3) age-specific educational materials to help training adult clinicians in their efforts to establish a trusting relationship with YA in diabetes care delivery.
Several attendees shared their experiences in overcoming the challenge of transfer. They reported ongoing collaborations with their colleagues on the “other side”, either pediatric or adult clinicians, in efforts to establish and improve communication within and between institutions. However, these were local and isolated efforts, which relied on single providers, were time-consuming, and not yet formalized. These efforts did not address the needs of many YA who relocate geographically for school or work. The YA and parents participating in the roundtable reported that the major challenge of transfer was moving care from a familiar team to a new, unknown team, with potentially different goals and expectations.
Participants envisioned the creation of a communication system between pediatric and adult providers at different institutions, ideally incorporating a shared nationwide electronic medical record system to help communication between institutions and to track visit attendance. This effort may require several years of development and funding, while a more standardized clinical note to share – yielding a “warm handoff” – between pediatric and adult clinicians could help welcome YA into the adult care environment.
Next, participants discussed assessment of maturation. During adolescence and young adulthood, development of executive function – the ability to take on complicated tasks like diabetes self-care – occurs; this is a dynamic process that happens differently among individuals (13). The lack of or delayed maturation of executive function may lead to poor glycemic control, loss of follow-up care, low clinic attendance rates, and participation in high risk behaviors (14). Currently, there are few clinical tools for assessing maturation and readiness for self-care (15) that have been empirically validated to guide clinicians in identifying patients ready to transfer and engage in their own diabetes care. The participants recommended the development of tools for evaluation of cognitive and emotional readiness for independent self-care.
Moreover, it was recognized that adult care systems and adult clinicians are not prepared to work with YA and their family members and address the specific socioeconomic challenges of this age group (16). Participants proposed the development of a specific competency curriculum for providers who work with the YA. This curriculum would focus on helping adult providers better understand the psychosocial challenges and barriers YA face and provide guidance to adult clinicians regarding establishing trusting, interactive relationships with YA. Clinicians should also be taught to modulate their expectations to better fit the realities of this developmental stage and recognize the physical, social, and emotional burdens YA face while collaboratively identifying strategies to help improve physical and psychosocial outcomes.
The participants recognized the need to develop age-specific guidelines for screening, prevention, and treatment of comorbidities and complications specific to the YA needs. They identified two major issues related to physical health: 1) the deterioration of glycemic control and increased risk of acute complications and 2) age-specific assessment, prevention, and management of comorbidities and long-term complications.
During late adolescence, glycemic control can deteriorate and often remains sub-optimal during the early years of young adulthood (17, 18). Sub-optimal glycemic control is often the result of several factors, including competing social and economic (19) demands and the ongoing maturation process, among others (20).
Among potential tools to improve glycemic control, the use of diabetes technologies – insulin pumps and Continuous Glucose Monitoring (CGM) — were identified. Many participants reported the use of CGM as best practice in this age group, especially given recent evidence of the benefits of CGM use in YA (21–23).
Participants also recommended the use of communication technologies which are commonly used by YA; i.e. text messaging, video calling, social networking, etc. (24). They sought to increase use of telehealth and text messaging to support and reinforce positive self-care behavior in between face-to-face visits and potentially to develop a web-based platform to increase peer-to-peer support. Further research in this area is needed.
Screening, assessment, and management of long-term micro- and macro-vascular complications were discussed at length for both T1D and T2D, especially given the focus on this area in adult diabetes care and the limited, if not absent, attention by pediatric providers (25, 26). Participants recognized the need and challenge of maintaining annual eye exams and kidney function testing in YA.
Cardiovascular disease (CVD) prevention was discussed. Several modifiable risk factors, like overweight/obesity and elevated blood pressure or lipids (27, 28), may already be present in YA, along with non-modifiable factors, like age of diabetes onset (29) and family history. The current clinical guidelines for prevention of CVD were developed from data in adults with T2D, and limited attention is given to YA (30). A study in adolescents on the use of statins and ACE inhibitors for early prevention of CVD did not yield benefit (31). Thus far, there is no clear indication of when and how to start prevention of CVD in YA. Moreover, statins and ACE inhibitors are contraindicated in pregnancy, making them challenging to use in women of childbearing age.
The need for further investigation in this area to elucidate how to best prevent micro and macro-vascular complications in this age group was noted (Table 1)
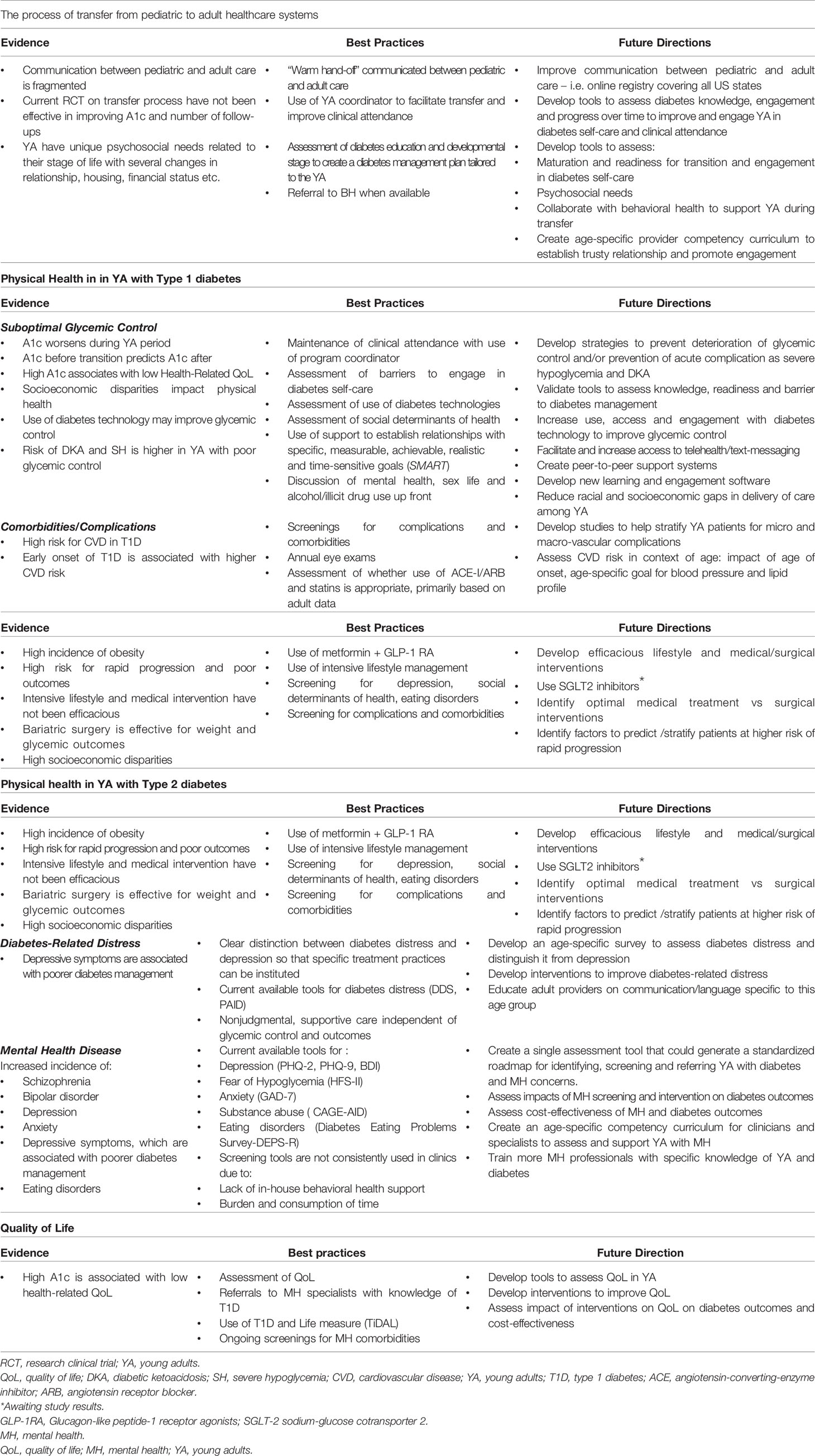
Next, participants focused on physical health in youth-onset T2D. YA with T2D are a growing population (32) with high rates of obesity and substantial socioeconomic disadvantage (33, 34). The clinical course, management, response to treatment, and outcomes of youth-onset T2D are different compared to adult-onset T2D. A faster loss of beta-cell function and a greater degree of insulin resistance have been described in this age group (35). The response to lifestyle modification, metformin, and insulin is poor in many cases (2). Use of a GLP1-agonist (36) and bariatric surgery (37) may be more beneficial; however there are limited long-term data. Again, transfer to adult care is associated with deterioration of glycemic control (34). Participants agreed that there is a lack of tailored guidelines and educational materials to care for persons with youth-onset T2D. Moreover, there is a need to identify best treatment options and to develop markers to identify patients with rapidly progressive T2D (2). Long-term data from the TODAY Study are forthcoming (Table 1).
YA with diabetes are a particularly vulnerable group for mental health (MH) concerns. An increase in psychosocial issues and risk-taking behaviors, and a disruption in continuity of care have been described in this age group (38, 39). Indeed, this age group has the highest rates of MH concerns across the adult lifespan and diseases such as schizophrenia and bipolar disorders may emerge during this time (10). Notably, YA with diabetes are a greatly understudied population as they often do not participate in research. Thus, there are gaps in the literature.
At present, the MH research literature focuses mainly on depression, diabetes distress, eating disorders, anxiety, and substance abuse (40) with specific assessment tools for each concern: depression (PHQ-2, PHQ-9, BDI) (41, 42), diabetes distress (DDS, PAID) (43), eating disorders (DEPS-R) (44), Fear of Hypoglycemia (HFS-II) (45), anxiety (GAD-7) (46), and substance abuse (CAGE-AID) (47), but assessment of these multiple MH concerns can be time-consuming and burdensome for both clinicians and patients. Furthermore, there is a lack of qualified MH providers to follow-up on concerning assessments (48). The participants recommended the creation of a single assessment tool that could generate a standardized roadmap for identifying, screening, and referring YAs with diabetes for MH concerns. Moreover, they highlighted the importance of distinguishing between depression and diabetes distress in order to determine specific treatment recommendations and practices for such concerns.
Another topic discussion was how the use of language is important in all diabetes management interactions but is especially critical with this age group. Providers need to acknowledge and understand that communication and words chosen to communicate can help creating a partnership in care for this population (49). In this context, presenters highlighted the use of autonomy-supportive communication strategies such as motivational interviewing.
Intervention strategies for optimizing MH care in the YA should begin with the specific embedding of MH in overall diabetes care. It was suggested that providers meet YA where they are at and use on-demand/drop-in services, late afternoon/evening hour meetings, texting, telehealth, or other modes of communication. Other suggestions included the use of Telehealth treatment (24), enhancing YA-provider communication and problem-solving (50), structured occupational therapy (51), Peer Support/Peer Group Education (52), and a multi-component program such as LEAP (Let’s Empower and Prepare) (53). In addition, given the links between parental support and MH in childhood and adolescence (54), it was recommended that utilizing a pediatric-like family approach, including family, peers, and significant others in adult medical appointments and management decisions may permit more supportive, engaged ongoing treatment for YA with diabetes and thus may address some of the gaps in care and encourage return visits.
Furthermore, the participants agreed upon the need to develop clinical strategies that can assist YA with moving from assessment/referral to actual clinical care visits for diabetes and MH concerns. Some suggestions to aid this movement to clinical care included paying attention to and aiding patients with navigating their insurance coverage and using telehealth practices (virtual visits, virtual screenings), especially given recent reimbursement. However, many recognized the importance of ongoing Face- to-Face visits, especially in urgent MH situations. Ideally, YA with executive function deficits should receive help to navigate the health care system from care ambassadors or patient navigators, however these staff members are limited in adult care (55).
Adult providers also need to be aware that these YA might participate in risk-taking behaviors (e.g., alcohol, drugs, unprotected sex) along with their peers, who likely do not have diabetes. Suggestions for addressing these risk-taking behaviors and providing support to the YA is important; this includes maintaining a non-judgmental attitude while providing education and resources about how to manage diabetes during these situations (Table 1).
Finally, participants discussed the following challenges to optimizing MH treatment for YA with diabetes: limited access to care, time constraints, limited number of trained MH providers with knowledge of diabetes, long waiting lists, gaps in continuity of care, and inadequate reimbursement. Discussion also highlighted the need to assess socioeconomic status for this YA group since such deficiencies can create high risk and reduce treatment opportunities. Participants agreed that more research was needed to understand particular challenges facing YA with diabetes from lower socioeconomic backgrounds or from racial/ethnic minority groups, especially given the increased awareness of potential for care disparities (19).
Quality of life (QoL) relates to perceptions of people’s position in life in the context of culture and values in relation to their goals and expectations (56). Generally, QoL has multiple constructs (e.g., general, health-related, or diabetes-specific) and domains (physical, psychological, and/or social functioning). Any intervention aimed at preserving QoL must be explicit in its focus using appropriate, clinically-validated current measures.
Despite the availability of multiple, validated QoL measures, there are gaps, which may impact our ability to systematically and meaningfully assess QoL in YA with diabetes. First, few measures are specifically targeted to the YA (57, 58). It is possible that meaningful insights for this age group may be lost when using measures validated across the adult lifespan. QoL measures commonly face ceiling effects in which persons, despite meaningful stresses in their lives, report high QoL. The participants recommended the use of specific, validated quality of life measures, like the Type 1 Diabetes and Life (T1DAL) measures (58), which were created to ensure they remain current to modern day clinical practice and personal experience.
It has been shown that factors related to fear of diabetes-related complications can contribute to or correlate with higher or lower levels of QoL (59). The group acknowledged that routine and systematic collection of self-reported QoL and its contributing factors is a major barrier to developing clinic-based assessments and interventions to ensure preservation of QoL in this vulnerable population. The time and resources needed to capture this information are major barriers to large-scale quality improvement or clinical research efforts. There is a limited evidence base for interventions targeting QoL preservation for YA with diabetes. Not unexpectedly, there is little to no literature on the clinical efficacy and cost-effectiveness of these interventions.
Current guidelines focus on routine assessment of more narrowly-defined constructs (e.g. diabetes distress, fear of hypoglycemia, and family conflict) with appropriate referrals to knowledgeable specialists. Further, the guidelines recognize the vulnerability of this period and recommend preventative MH visits at key transition points to focus on YA issues. The limited number of trained MH professionals who work with diabetes highlights the need to provide basic training to primary care and specialty healthcare professionals to screen, provide anticipatory guidance, and potentially intervene on common factors with may adversely impact QoL (Table 1).
On a practical, immediately actionable level, the participants recommended assessing diabetes-related factors interfering with QoL and developing a plan to address those factors over time. This will increase the likelihood that the clinical encounter was patient-centered and impactful. Future studies are needed to develop clinic-based, scalable interventions to address critical risk factors which may jeopardize the QoL of YA with diabetes.
YA with diabetes face unique challenges in their management] and have a high risk of poor outcomes that can negatively impact physical health, MH, QoL and life expectancy. Thus, it is imperative for pediatric and adult clinicians to continue working in concert on targeted interventions that focus on this age group to reduce the risk of acute and long-term complications and to support and improve YA MH and QoL.
YA with diabetes have suboptimal glycemic control and are at high risk for adverse outcomes that become magnified at the time of transfer from pediatric to adult care systems. Our unique multidisciplinary participants reviewed the current literature, identified gaps, shared best practices, and highlighted needs for future research with the goal of improving the healthcare process and diabetes-related clinical outcomes for YA with diabetes.
There was substantial interest among adult providers in working with pediatric providers and MH professionals to identify best practices and to plan for future studies specific to the YA population. The results of this two-day meeting discussion are summarized in this article with the intent to be used for development of best practices and future research projects aimed at overcoming current gaps in knowledge and improving both healthcare processes and outcomes for YA with diabetes.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
ET, JL, RB, and LL contributed to study concept and design. ET, JL, SH, SM, and MR contributed to data acquisition, analysis, and interpretation, ET, JL, SH, SM, MR, and MM, drafted the manuscript. ET and LL critically revised the manuscript for important intellectual content. ET is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and accuracy of the data analysis.
We thank an anonymous philanthropic donor for this work.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. Pettus JH, Zhou FL, Shepherd L, Preblick R, Hunt PR, Paranjape S, et al. Incidences of Severe Hypoglycemia and Diabetic Ketoacidosis and Prevalence of Microvascular Complications Stratified by Age and Glycemic Control in U.S. Adult Patients With Type 1 Diabetes: A Real-World Study. Diabetes Care (2019) 42(12):2220–7. doi: 10.2337/dc19-0830
2. Group TS, Zeitler P, Hirst K, Pyle L, Linder B, Copeland K, et al. A Clinical Trial to Maintain Glycemic Control in Youth With Type 2 Diabetes. N Engl J Med (2012) 366(24):2247–56. doi: 10.1056/NEJMoa1109333
3. Arnett JJ. Emerging Adulthood. A Theory of Development From the Late Teens Through the Twenties. Am Psychol (2000) 55(5):469–80.
4. Blum RW, Garell D, Hodgman CH, Jorissen TW, Okinow NA, Orr DP, et al. Transition From Child-Centered to Adult Health-Care Systems for Adolescents With Chronic Conditions. A Position Paper of the Society for Adolescent Medicine. J Adolesc Health (1993) 14(7):570–6. doi: 10.1016/1054-139X(93)90143-D
5. Steinbeck KS, Shrewsbury VA, Harvey V, Mikler K, Donaghue KC, Craig ME, et al. A Pilot Randomized Controlled Trial of a Post-Discharge Program to Support Emerging Adults With Type 1 Diabetes Mellitus Transition From Pediatric to Adult Care. Pediatr Diabetes (2015) 16(8):634–9. doi: 10.1111/pedi.12229
6. Spaic T, Robinson T, Goldbloom E, Gallego P, Hramiak I, Lawson ML, et al. Closing the Gap: Results of the Multicenter Canadian Randomized Controlled Trial of Structured Transition in Young Adults With Type 1 Diabetes. Diabetes Care (2019) 42(6):1018–26. doi: 10.2337/dc18-2187
7. White M, O'Connell MA, Cameron FJ. Clinic Attendance and Disengagement of Young Adults With Type 1 Diabetes After Transition of Care From Paediatric to Adult Services (TrACeD): A Randomised, Open-Label, Controlled Trial. Lancet Child Adolesc Health (2017) 1(4):274–83. doi: 10.1016/S2352-4642(17)30089-5
8. Chiang JL, Maahs DM, Garvey KC, Hood KK, Laffel LM, Weinzimer SA, et al. Type 1 Diabetes in Children and Adolescents: A Position Statement by the American Diabetes Association. Diabetes Care (2018) 41(9):2026–44. doi: 10.2337/dci18-0023
9. Ducat L, Rubenstein A, Philipson LH, Anderson BJ. A Review of the Mental Health Issues of Diabetes Conference. Diabetes Care (2015) 38(2):333–8. doi: 10.2337/dc14-1383
11. Hagger V, Hendrieckx C, Cameron F, Pouwer F, Skinner TC, Speight J. Diabetes Distress Is More Strongly Associated With HbA1c Than Depressive Symptoms in Adolescents With Type 1 Diabetes: Results From Diabetes MILES Youth-Australia. Pediatr Diabetes (2018) 19(4):840–7. doi: 10.1111/pedi.12641
12. Stahl-Pehe A, Landwehr S, Lange KS, Bachle C, Castillo K, Yossa R, et al. Impact of Quality of Life (QoL) on Glycemic Control (HbA1c) Among Adolescents and Emerging Adults With Long-Duration Type 1 Diabetes: A Prospective Cohort-Study. Pediatr Diabetes (2017) 18(8):808–16. doi: 10.1111/pedi.12487
13. Vloemans AF, Eilander MMA, Rotteveel J, Bakker-van Waarde WM, Houdijk E, Nuboer R, et al. Youth With Type 1 Diabetes Taking Responsibility for Self-Management: The Importance of Executive Functioning in Achieving Glycemic Control: Results From the Longitudinal DINO Study. Diabetes Care (2019) 42(2):225–31. doi: 10.2337/dc18-1143
14. Berg CA, Wiebe DJ, Suchy Y, Turner SL, Butner J, Munion A, et al. Executive Function Predicting Longitudinal Change in Type 1 Diabetes Management During the Transition to Emerging Adulthood. Diabetes Care (2018) 41(11):2281–8. doi: 10.2337/dc18-0351
15. Goethals ER, Volkening LK, Tinsley L, Laffel LM. Ready or Not? Greater Readiness for Independent Self-Care Predicts Better Self-Management But Not HbA1c in Teens With Type 1 Diabetes. Diabetes Med (2020) 38(5):e14507. doi: 10.1111/dme.14507
16. Garvey KC, Telo GH, Needleman JS, Forbes P, Finkelstein JA, Laffel LM. Health Care Transition in Young Adults With Type 1 Diabetes: Perspectives of Adult Endocrinologists in the U.S. Diabetes Care (2016) 39(2):190–7. doi: 10.2337/dc15-1775
17. Foster NC, Beck RW, Miller KM, Clements MA, Rickels MR, DiMeglio LA, et al. State of Type 1 Diabetes Management and Outcomes From the T1D Exchange in 2016-2018. Diabetes Technol Ther (2019) 21(2):66–72. doi: 10.1089/dia.2018.0384
18. Toschi E, Bailey RJ, Miller KM, Calhoun PM. Improvement in A1c Levels in Early Adulthood in the T1D Exchange: Impact of Racial, Socioeconomic, and Clinical Factors. J Clin Endocrinol Metab (2021) 106(5):1294–302. doi: 10.1210/clinem/dgab077
19. Agarwal S, Kanapka LG, Raymond JK, Walker A, Gerard-Gonzalez A, Kruger D, et al. Racial-Ethnic Inequity in Young Adults With Type 1 Diabetes. J. Clin. Endocrinol. Metab (2020) 105(8):e2960–9. doi: 10.1210/clinem/dgaa236
20. Young Adults and the Affordable Care Act: Protecting Young Adults and Eliminating Burdens on Businesses and Families FAQs. Available at: https://www.dol.gov/agencies/ebsa/about-ebsa/our-activities/resource-center/faqs/young-adult-and-aca.
21. Juvenile Diabetes Research Foundation Continuous Glucose Monitoring Study, G, Tamborlane WV, Beck RW, Bode BW, Buckingham B, Chase HP, et al. Continuous Glucose Monitoring and Intensive Treatment of Type 1 Diabetes. N Engl J Med (2008) 359(14):1464–76. doi: 10.1056/NEJMoa0805017
22. Laffel LM, Kanapka LG, Beck RW, Bergamo K, Clements MA, Criego A, et al. Effect of Continuous Glucose Monitoring on Glycemic Control in Adolescents and Young Adults With Type 1 Diabetes: A Randomized Clinical Trial. JAMA (2020) 323(23):2388–96. doi: 10.1001/jama.2020.6940
23. Toschi E, Atakov-Castillo A, Clift A, Bennetti M, Gabbay RA. CGM and Glycemic Control in Young Adults With Type 1 Diabetes: Benefit for Even the Simplest Insulin Administration Methods. Diabetes Technol Ther (2021) 23(8):586–9. doi: 10.1089/dia.2020.0624
24. Raymond JK, Berget CL, Driscoll KA, Ketchum K, Cain C, Fred Thomas JF. CoYoT1 Clinic: Innovative Telemedicine Care Model for Young Adults With Type 1 Diabetes. Diabetes Technol Ther (2016) 18(6):385–90. doi: 10.1089/dia.2015.0425
25. Katz M, Giani E, Laffel L. Challenges and Opportunities in the Management of Cardiovascular Risk Factors in Youth With Type 1 Diabetes: Lifestyle and Beyond. Curr Diabetes Rep (2015) 15(12):119. doi: 10.1007/s11892-015-0692-4
26. Buckloh LM, Lochrie AS, Antal H, Milkes A, Canas JA, Hutchinson S, et al. Diabetes Complications in Youth: Qualitative Analysis of Parents' Perspectives of Family Learning and Knowledge. Diabetes Care (2008) 31(8):1516–20. doi: 10.2337/dc07-2349
27. Lurbe E, Redon J, Kesani A, Pascual JM, Tacons J, Alvarez V, et al. Increase in Nocturnal Blood Pressure and Progression to Microalbuminuria in Type 1 Diabetes. N Engl J Med (2002) 347(11):797–805. doi: 10.1056/NEJMoa013410
28. Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents; National Heart, Lung, and Blood Institute. Expert Panel on Integrated Guidelines for Cardiovascular Health and Risk Reduction in Children and Adolescents: Summary Report. Pediatrics (2011) 128(Suppl 5):S213–56. doi: 10.1542/peds.2009-2107C
29. Rawshani A, Sattar N, Franzen S, Rawshani A, Hattersley AT, Svensson AM, et al. Excess Mortality and Cardiovascular Disease in Young Adults With Type 1 Diabetes in Relation to Age at Onset: A Nationwide, Register-Based Cohort Study. Lancet (2018) 392(10146):477–86. doi: 10.1016/S0140-6736(18)31506-X
30. American Diabetes, A. Cardiovascular Disease and Risk Management: Standards of Medical Care in Diabetes-2020. Diabetes Care (2020) 43(Suppl 1):S111–34. doi: 10.2337/dc20-S010
31. Marcovecchio ML, Chiesa ST, Bond S, Daneman D, Dawson S, Donaghue KC, et al. ACE Inhibitors and Statins in Adolescents With Type 1 Diabetes. N Engl. J. Med (2017) 377(18):1733–45. doi: 10.1056/NEJMoa1703518
32. Dabelea D, Mayer-Davis EJ, Saydah S, Imperatore G, Linder B, Divers J, et al. Prevalence of Type 1 and Type 2 Diabetes Among Children and Adolescents From 2001 to 2009. JAMA (2014) 311(17):1778–86. doi: 10.1001/jama.2014.3201
33. Arslanian S, Bacha F, Grey M, Marcus MD, White NH, Zeitler P. Evaluation and Management of Youth-Onset Type 2 Diabetes: A Position Statement by the American Diabetes Association. Diabetes Care (2018) 41(12):2648–68. doi: 10.2337/dci18-0052
34. Agarwal S, Raymond JK, Isom S, Lawrence JM, Klingensmith G, Pihoker C, et al. Transfer From Paediatric to Adult Care for Young Adults With Type 2 Diabetes: The SEARCH for Diabetes in Youth Study. Diabetes Med (2018) 35(4):504–12. doi: 10.1111/dme.13589
35. Consortium R. Impact of Insulin and Metformin Versus Metformin Alone on Beta-Cell Function in Youth With Impaired Glucose Tolerance or Recently Diagnosed Type 2 Diabetes. Diabetes Care (2018) 41(8):1717–25. doi: 10.2337/dc18-0787
36. Tamborlane WV, Barrientos-Perez M, Fainberg U, Frimer-Larsen H, Hafez M, Hale PM, et al. Liraglutide in Children and Adolescents With Type 2 Diabetes. N Engl. J. Med (2019) 381(7):637–46. doi: 10.1056/NEJMoa1903822
37. Inge TH, Laffel LM, Jenkins TM, Marcus MD, Leibel NI, Brandt ML, et al. Comparison of Surgical and Medical Therapy for Type 2 Diabetes in Severely Obese Adolescents. JAMA Pediatr (2018) 172(5):452–60. doi: 10.1001/jamapediatrics.2017.5763
38. Cummings DM, Kirian K, Howard G, Howard V, Yuan Y, Muntner P, et al. Consequences of Comorbidity of Elevated Stress and/or Depressive Symptoms and Incident Cardiovascular Outcomes in Diabetes: Results From the REasons for Geographic And Racial Differences in Stroke (REGARDS) Study. Diabetes Care (2016) 39(1):101–9. doi: 10.2337/dc15-1174
39. Johnson B, Eiser C, Young V, Brierley S, Heller S. Prevalence of Depression Among Young People With Type 1 Diabetes: A Systematic Review. Diabetes Med (2013) 30(2):199–208. doi: 10.1111/j.1464-5491.2012.03721.x
40. Delamater AM, de Wit M, McDarby V, Malik JA, Hilliard ME, Northam E, et al. ISPAD Clinical Practice Consensus Guidelines 2018: Psychological Care of Children and Adolescents With Type 1 Diabetes. Pediatr. Diabetes (2018) 19(Suppl 27):237–49. doi: 10.1111/pedi.12736
41. Thombs BD, Benedetti A, Kloda LA, Levis B, Nicolau I, Cuijpers P, et al. The Diagnostic Accuracy of the Patient Health Questionnaire-2 (PHQ-2), Patient Health Questionnaire-8 (PHQ-8), and Patient Health Questionnaire-9 (PHQ-9) for Detecting Major Depression: Protocol for a Systematic Review and Individual Patient Data Meta-Analyses. Syst Rev (2014) 3:124. doi: 10.1186/2046-4053-3-124
42. Rauwerda NL, Tovote KA, Peeters A, Sanderman R, Emmelkamp PMG, Schroevers MJ, et al. WHO-5 and BDI-II Are Acceptable Screening Instruments for Depression in People With Diabetes. Diabetes Med (2018) 35(12):1678–85. doi: 10.1111/dme.13779
43. Polonsky WH, Anderson BJ, Lohrer PA, Welch G, Jacobson AM, Aponte JE, et al. Assessment of Diabetes-Related Distress. Diabetes Care (1995) 18(6):754–60. doi: 10.2337/diacare.18.6.754
44. Markowitz JT, Butler DA, Volkening LK, Antisdel JE, Anderson BJ, Laffel LM. Brief Screening Tool for Disordered Eating in Diabetes: Internal Consistency and External Validity in a Contemporary Sample of Pediatric Patients With Type 1 Diabetes. Diabetes Care (2010) 33(3):495–500. doi: 10.2337/dc09-1890
45. Polonsky WH, Davis CL, Jacobson AM, Anderson BJ. Correlates of Hypoglycemic Fear in Type I and Type II Diabetes Mellitus. Health Psychol (1992) 11(3):199–202. doi: 10.1037/0278-6133.11.3.199
46. Spitzer RL, Kroenke K, Williams JB, Lowe B. A Brief Measure for Assessing Generalized Anxiety Disorder: The GAD-7. Arch. Intern Med (2006) 166(10):1092–7. doi: 10.1001/archinte.166.10.1092
47. Ewing JA. Detecting Alcoholism. The CAGE Questionnaire. JAMA (1984) 252(14):1905–7. doi: 10.1001/jama.1984.03350140051025
48. Young-Hyman D, de Groot M, Hill-Briggs F, Gonzalez JS, Hood K, Peyrot M. Psychosocial Care for People With Diabetes: A Position Statement of the American Diabetes Association. Diabetes Care (2016) 39(12):2126–40. doi: 10.2337/dc16-2053
49. Dickinson JK, Guzman SJ, Maryniuk MD, O'Brian CA, Kadohiro JK, Jackson RA, et al. The Use of Language in Diabetes Care and Education. Diabetes Care (2017) 40(12):1790–9. doi: 10.2337/dci17-0041
50. Majumder E, Cogen FR, Monaghan M. Self-Management Strategies in Emerging Adults With Type 1 Diabetes. J Pediatr Health Care (2017) 31(1):29–36. doi: 10.1016/j.pedhc.2016.01.003
51. Pyatak EA, Carandang K, Vigen CLP, Blanchard J, Diaz J, Concha-Chavez A, et al. Occupational Therapy Intervention Improves Glycemic Control and Quality of Life Among Young Adults With Diabetes: The Resilient, Empowered, Active Living With Diabetes (REAL Diabetes) Randomized Controlled Trial. Diabetes Care (2018) 41(4):696–704. doi: 10.2337/dc17-1634
52. Markowitz JT, Laffel LM. Transitions in Care: Support Group for Young Adults With Type 1 Diabetes. Diabetes Med (2012) 29(4):522–5. doi: 10.1111/j.1464-5491.2011.03537.x
53. Sequeira PA, Pyatak EA, Weigensberg MJ, Vigen CP, Wood JR, Ruelas V, et al. Let's Empower and Prepare (LEAP): Evaluation of a Structured Transition Program for Young Adults With Type 1 Diabetes. Diabetes Care (2015) 38(8):1412–9. doi: 10.2337/dc14-2577
54. Wysocki T, Greco P. Social Support and Diabetes Management in Childhood and Adolescence: Influence of Parents and Friends. Curr Diabetes Rep (2006) 6(2):117–22. doi: 10.1007/s11892-006-0022-y
55. Katz ML, Volkening LK, Butler DA, Anderson BJ, Laffel LM. Family-Based Psychoeducation and Care Ambassador Intervention to Improve Glycemic Control in Youth With Type 1 Diabetes: A Randomized Trial. Pediatr Diabetes (2014) 15(2):142–50. doi: 10.1111/pedi.12065
56. Available at: https://www.who.int/tools/whoqol.
57. Hilliard ME, Herzer M, Dolan LM, Hood KK. Psychological Screening in Adolescents With Type 1 Diabetes Predicts Outcomes One Year Later. Diabetes Res Clin Pract (2011) 94(1):39–44. doi: 10.1016/j.diabres.2011.05.027
58. Hilliard ME, Minard CG, Marrero DG, de Wit M, Thompson D, DuBose SN, et al. Assessing Health-Related Quality of Life in Children and Adolescents With Diabetes: Development and Psychometrics of the Type 1 Diabetes and Life (T1DAL) Measures. J Pediatr Psychol (2020) 45(3):328–39. doi: 10.1093/jpepsy/jsz083
Keywords: young adults, adult care, transition, mental health, physical health, quality of life
Citation: Toschi E, Leblanc J, Hafida S, Mehta S, Ritholz M, Gabbay R and Laffel L (2022) Caring for Young Adults With Diabetes in the Adult Care Setting: Summary of a Multidisciplinary Roundtable. Front. Clin. Diabetes Healthc. 3:830183. doi: 10.3389/fcdhc.2022.830183
Received: 06 December 2021; Accepted: 31 January 2022;
Published: 22 March 2022.
Edited by:
Stavros Liatis, Laiko General Hospital of Athens, GreeceReviewed by:
Petros Thomakos, Hygeia General Hospital, GreeceCopyright © 2022 Toschi, Leblanc, Hafida, Mehta, Ritholz, Gabbay and Laffel. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Elena Toschi, ZWxlbmEudG9zY2hpQGpvc2xpbi5oYXJ2YXJkLmVkdQ==
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.