 Gillian F. Black1*
Gillian F. Black1* Euzebiusz Jamrozik2
Euzebiusz Jamrozik2 Wesaal Khan3Stephanie Peralta4
Wesaal Khan3Stephanie Peralta4 Benjamin Havenga3
Benjamin Havenga3 Maria W. Merritt4Maureen Kelley5
Maria W. Merritt4Maureen Kelley5- 1Sustainable Livelihoods Foundation, Cape Town, South Africa
- 2Ethox and Pandemic Sciences Institute, Nuffield Department of Population Health, Oxford, United Kingdom
- 3Faculty of Science, Stellenbosch University, Stellenbosch, South Africa
- 4Berman Institute of Bioethics and Bloomberg School of Public Health (Department of International Health), Johns Hopkins University, Baltimore, MD, United States
- 5Wake Forest University, Winston-Salem, NC, United States
Advancing climate change is an urgent global driver of human disease with some of the world’s most marginalized communities being at highest risk. In response to this compound threat, scientific studies exploring the intersections of climate and health are gaining momentum, yet sparse attention is currently paid to models of research that engage and involve those who are most affected. This is a crucial moment for the global health field to take up valuable lessons from the relatively few climate-health studies that have purposefully brought scientists together with communities and members of the wider public, via established approaches such as community-based participatory research and citizen science, to reduce health risks and better understand the deeper determinants of disease. Through a scoping literature review of PubMed and qualitative framework analysis, we investigate scientific, ethical, and social justice rationales that have motivated scientists to involve communities, including Indigenous groups, and other public stakeholders in climate-driven health research to varying degrees in different global contexts. We also examine the benefits of diverse forms of engagement and show that involving communities in research at the climate-health nexus has, for example, generated co-produced adaptation strategies that respond appropriately and effectively to priority health hazards. In addition, our findings demonstrate limitations, challenges, and ethical considerations that can arise when engaging communities in climate-health research. We argue that ethically engaging and involving communities and the wider public in research at the intersection of climate change and health is imperative for identifying relevant research priorities, promoting responsiveness that can appropriately fill gaps in at-risk settings, and advancing social justice. Our paper offers a range of examples of research designs and activities to guide scientists working in this emerging interdisciplinary field, inform funders seeking to support innovative and potentially transformative research, and contribute to global health policy.
Introduction
As the urgency of climate change becomes unavoidable, an emerging area of global health research attempts to respond by focusing on climate-drivers of disease (Romanello et al., 2023). Among the structural causes of global health disparities such as poverty and violent conflict, climate change starkly illustrates how overlapping disadvantages can accelerate poor health outcomes for the worst off. Layered burdens of poor physical and mental health, disability, and death attributable to climate change, disproportionately affect people living in poverty whose communities have historically done the least to cause it. An urgent priority for climate-health research is to improve understanding and catalyze responsiveness to burdens of ill-health in places that are being increasingly hit hard by climate change, especially marginalized settings in the Global South. In recognizing the need for an effective response to climate change threats based on the best available scientific knowledge, the United Nations Framework Convention on Climate Change (United Nations Framework Convention on Climate Change, 2015) calls for the inclusion of ‘non-Party stakeholders’, including civil society, local communities and Indigenous peoples for the mobilization of stronger and more ambitious climate action.
The 2030 Agenda and Sustainable Development Goals offer a framework that links community involvement to global objectives for climate resilience and health equity, emphasizing collaborative action to foster sustainable, inclusive, and resilient societies. Beyond the climate context, there have been long-standing efforts across multiple research disciplines to enhance research knowledge and activate responsiveness to community needs by bringing scientists together with at-risk communities and members of the wider public, through approaches such as community-based participatory research (CBPR) (Viswanathan et al., 2004)and citizen science (Kruger and Shannon, 2000). Numerous studies have confirmed that drawing on the knowledge and capacities of Indigenous and local people is often pivotal for designing relevant and culturally appropriate research and implementing it in ways that are acceptable and effective in local settings (Wheeler and Root-Bernstein, 2020). Engaging and involving affected community members in scientific research is also crucial for characterizing problems through lived experience, bringing local perspectives to the complexities and deeper determinants of development challenges, and addressing social injustice (Yuan et al., 2021).
The field of ecology has long embraced a more holistic conceptual understanding of the intimate links between environment and human activity. Sixteen years ago, in their ecology and environmental research, Minkler et al. (2008) demonstrated the role of community driven participatory research in promoting environmental justice. Community health, public health and global health models have also more recently broadened to include considerations of the social determinants of health. Furthermore, through their theoretical framework approach, Langmaid et al. (2021) have highlighted potential gaps in health promotion theory and practice in terms of the natural environment and health and emphasize the need for a paradigm shift to embed ecological and cultural determinants along with other determinants of health. Indigenous paradigms have demonstrated the fundamental connection between a healthy environment and community health (Martello, 2008). The enduring knowledge of Indigenous peoples is increasingly informing global climate strategy and action although important disparities have been identified regarding the geographic distribution of these efforts and the risk of reinforcing harmful stereotypes (Carmona et al., 2023; Petzold et al., 2020). Evidence shows that engaging and involving those who are most affected by health challenges can improve respect, trust, and the relevance of research (Holzer et al., 2014). Furthermore, community engagement and involvement (CEI) can enhance contextual knowledge about complex health burdens, strengthen community awareness around disease prevention and treatment, and help to define research priorities that best align with community health needs (Adhikari et al., 2017; Karris et al., 2020). In the context of infectious disease, robust CEI can strengthen the reflexivity and ethical conduct of health science research during periods of rapid change as it improves communication and feedback (Bedson et al., 2020). Vigorous CEI can also strengthen trust between communities and scientific teams, as exemplified in diverse contexts during the COVID-19 pandemic (Tindana et al., 2020; Ngwenya et al., 2022; Sahoo et al., 2023).
Given the rapidly evolving changes in our global environment, there is an increasing need for more dynamic study designs in the health sciences, including social science research and clinical research. For example, research during the COVID-19 pandemic sparked increased use of adaptive designs in clinical trials to allow researchers to revise and adapt study arms, sites, cohorts, and even research questions in response to emerging data, although not without challenges (Berry, 2011; Bothwell and Kesselheim, 2017; Butler et al., 2023). This is a crucial moment for the global health field to take up valuable lessons from the relatively few climate-health studies that have purposefully brought scientists together with communities and other members of society to reduce health risks and better understand the deeper determinants of disease. Through a scoping literature review and framework analysis (Gale et al., 2013; Pope et al., 2000) we investigate scientific, ethical, and social justice rationales that have motivated scientists to involve communities, including Indigenous groups, and members of the broader public in climate-driven health research to varying degrees in different global contexts. We examine the nature, benefits, challenges, and ethical implications of different approaches to engaged research as conveyed across the articles under review. Via this analysis we illustrate the main advantages of engaging community members and other public stakeholders in research at the nexus of climate change and health. We offer both impetus and examples to guide scientists working in this emerging and critical interdisciplinary field, inform funders seeking to support innovative and potentially transformative research, contribute to global health policy, and advance social justice.
Methods
Our scoping literature review and qualitative analysis were informed by our research questions: Q1: What models and examples of scientific-community partnerships have been published by teams working at the interface of climate change and health and what approaches have they taken? Q2: What arguments and rationales are given for involving communities at the climate-health interface? Q3: What considerations or challenges arise, including ethical or social justice considerations, if discussed?
Drawing on these research questions and test articles we developed our MeSH search string, shown in Table 1. Eligible articles needed to be peer-reviewed scientific papers, include some form of community involvement and focus on climate and health. Applying this string we conducted an initial search of English-language, peer-reviewed health science publications in PubMed to identify examples of community-science partnerships and engagement around climate change and health from 2000 to 2019, updated to 2023 prior to publication. Using Covidence review software to organize and review abstracts, authors SP and MK independently reviewed abstracts to eliminate papers not meeting inclusion criteria, resulting in 433 papers. Additional papers were excluded and borderline cases discussed: with no full text available, no details on community engagement, lack of combined focus on climate and health, misplaced reference to ‘environment’, or not meeting inclusion criteria, resulting in 51 papers. Authors GB and MK then conducted a second independent review of abstracts and full text, further eliminating papers that did not report sufficient details on the community engagement approach, did not clearly link health and climate change, or were purely theoretical and did not contribute to a rationale for community engagement in the climate-health context. A total of 51 pdfs were identified and stored on Zotero for qualitative review. (For PRISMA diagram see Supplemental material).
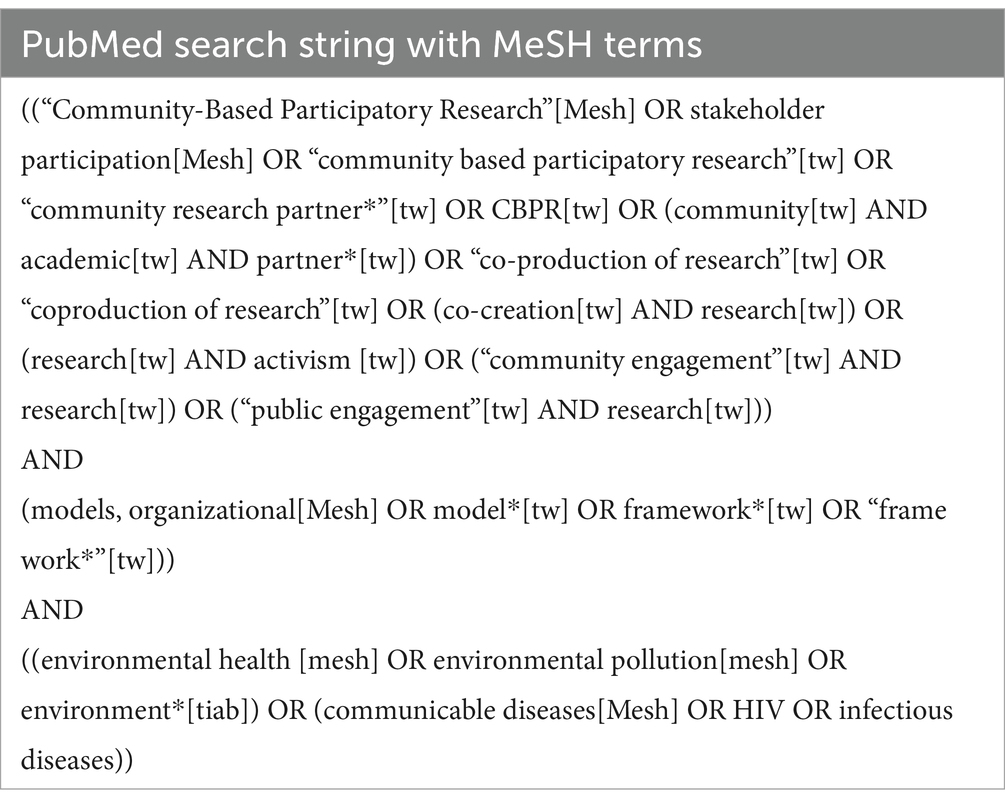
Table 1. PubMed search string.
In the qualitative review phase, MK and GB developed and applied a qualitative thematic framework analysis in a close read of the 51 papers. This is an iterative technique used in qualitative analysis that systematically guides the identification of more precise deductive themes from one’s research questions and emergent themes from the data source(s). In this case the data sources were the content of the papers, including background, methods, results, discussion, and figures (Gale et al., 2013; Pope et al., 2000).
Table 2 shows the final thematic analytic framework which GB and MK completed independently for the 51 papers, with a balanced allocation of papers between them. The results of this analysis were thoroughly cross-checked by GB and MK prior to deciding which papers were to be included in the final analysis. Several articles were found to be outside the scope of the central research questions shown above. For example, several of the articles reported on ecology studies that had no reference to human health. Others included mention of community involvement in the abstract, but upon in-depth review, no meaningful involvement of community members was described.
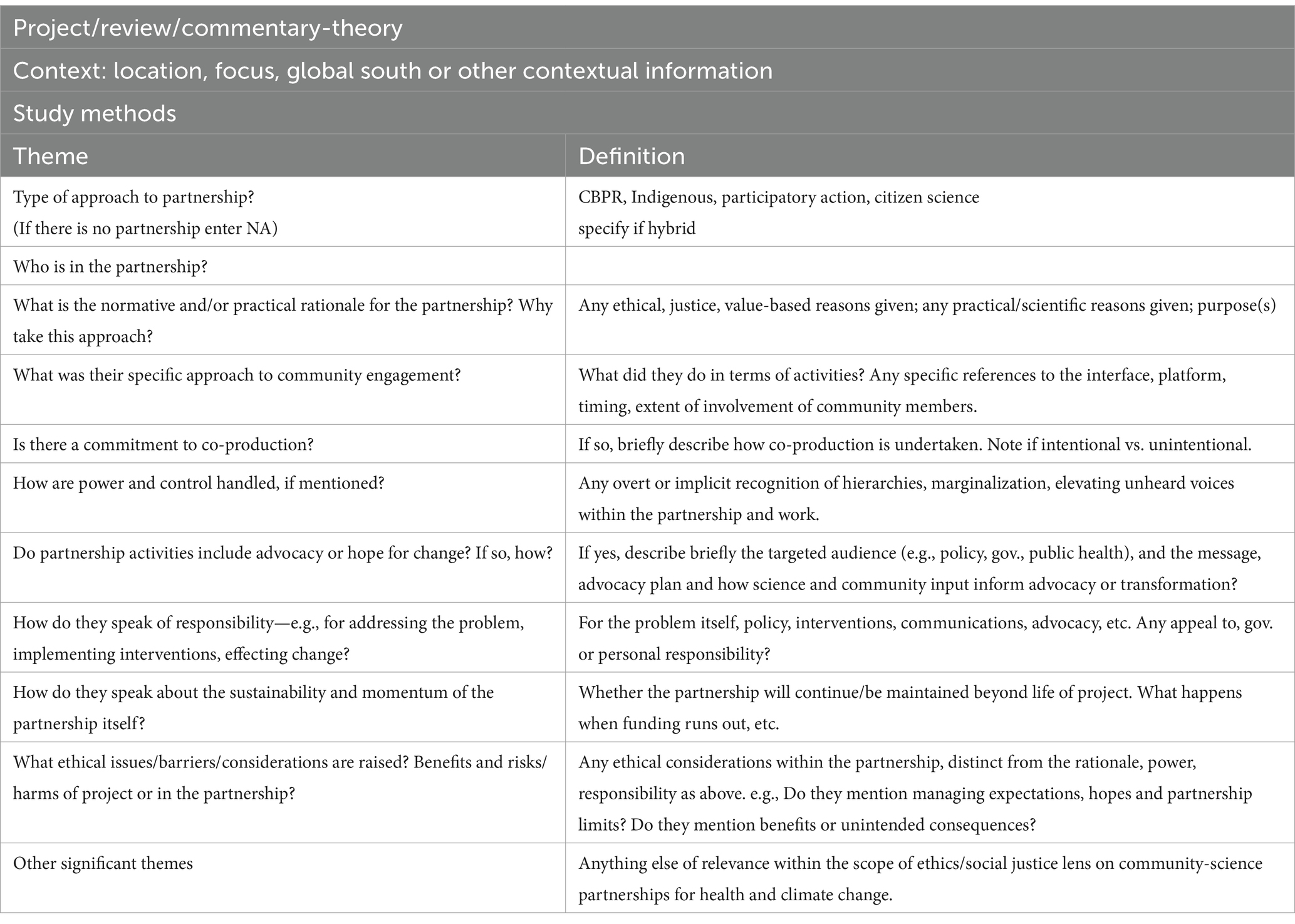
Table 2. Qualitative thematic framework showing refined queries used for analysis.
Papers not focused on the intersection of climate change and human health, or not involving community members, were excluded. Through this framework analysis we identified nine projects that closely fit these criteria. In addition, we identified four review articles and four conceptual/theoretical articles that robustly answered our questions about what rationales can be offered for science-community partnerships in climate-health research, even if they did not focus on a single project. Thus, a total of 17 papers (Table 3) were taken forward into the third phase of our qualitative and normative analysis as presented in our Results section.
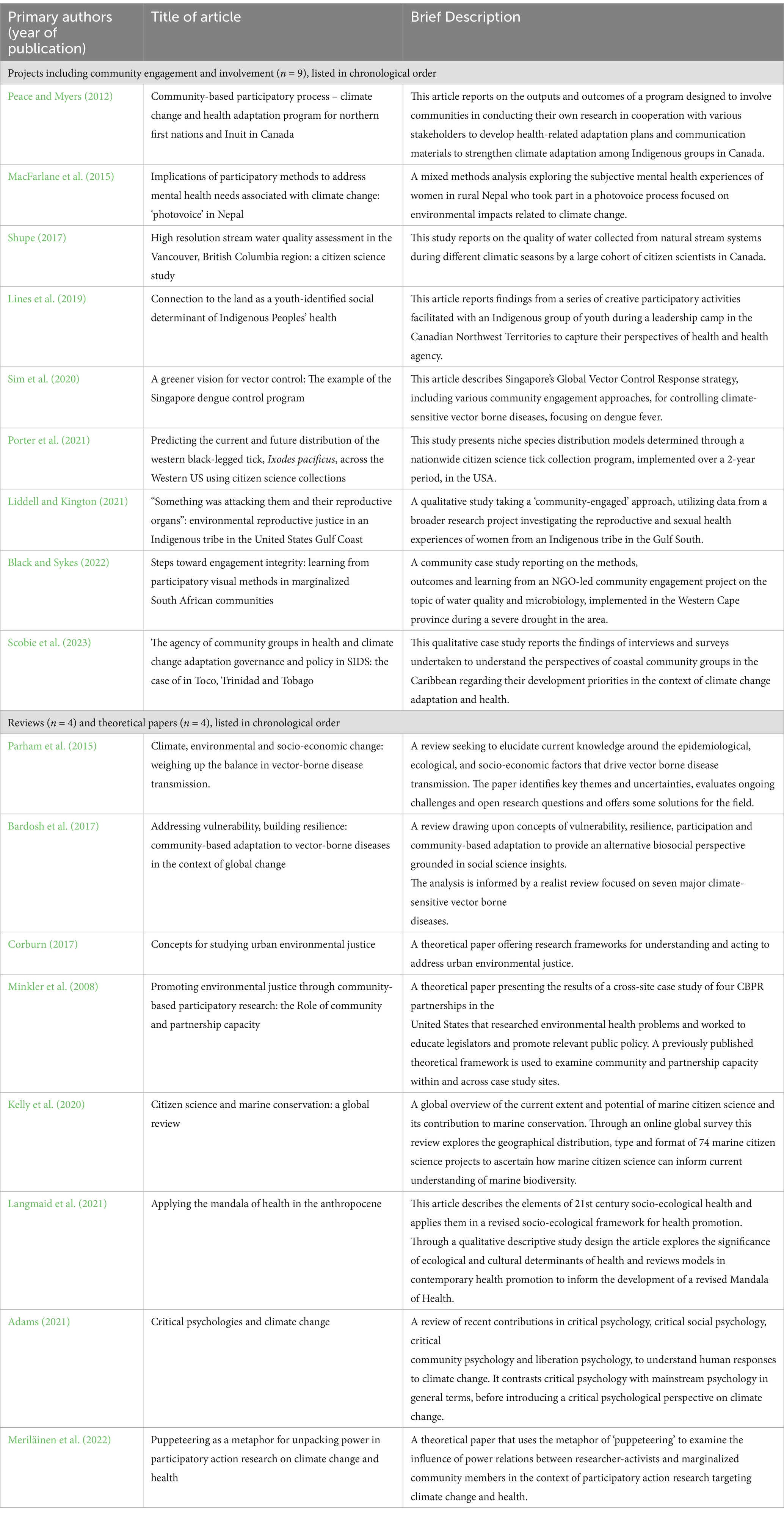
Table 3. Brief summaries of papers identified through full-text review using framework analysis (n = 17).
Results
Following an in-depth qualitative review of the total 17 projects, reviews, and theoretical papers shown in Table 3, we return to our research questions and discuss our findings. In section 1, focusing on the 9 project papers, we describe what has been done to engage and involve communities and members of the wider public in research on climate and human health, including innovative examples of community-based activities. To help shed light on why these approaches deserve greater consideration, in section 2 we present any normative and scientific rationales offered across all papers for involving communities in climate driven health research. In section 3 we describe findings across all papers on limitations, challenges, or ethical considerations that arise when involving communities in climate-health research. In Sections 2 and 3 we also draw upon some landmark publications that are of broader scope than those yielded by our searches, yet offer illuminating perspectives on our findings, for example, the references to Martello (2008).
To what extent have scientists who work at the interface of climate change and health been involving communities in their work and what approaches have they taken?
Tackling the dual challenges of health and climate change through community-science partnerships is a new and evolving area of interest, bridging two long-standing but largely separate areas of research: global health and environmental/ecological research. While we found many examples of community engagement in clinical health research or environmental research on non-health related topics, there are still relatively few published accounts of community-science partnerships on climate change and health. We focus on lessons learned through the nine projects that explicitly described engaging or involving communities or members of the wider public in research aimed at addressing the impacts of climate change on health. These studies spanned a range of approaches to involving community members or members of the wider public, and often mixed different techniques and activities, drawing on aspects of community-based participatory research and action research, visual methods, citizen science, science communication and knowledge exchange. For the purposes of our analysis, we have used CEI as a broader umbrella term describing a range of processes where people who live in a defined geographical area (from an entire country to a small informal settlement) have been engaged or involved in research, beyond simply being recruited as a study participant.
Climate change and health adaptation: Canada
Peace and Myers (2012) reported on a community-based participatory research (CBPR) process integrated into a climate change and health adaptation program for Northern First Nations and Inuit in Canada. The program aimed to develop information and tools for decision-making at various levels concerning human health and a changing environment. It focused on capacity-building by funding communities to conduct their own research in collaboration with Aboriginal associations, academics, and governments. The program mandated that participatory research include studying climate change impacts on health, combining traditional knowledge and science, developing locally appropriate adaptation plans and tools, and communicating results to the community and beyond. Program activities involved 15 community visits and three capacity-building workshops, conducted in five locations to reach various rural communities. These workshops, in partnership with Aboriginal organizations, aimed to familiarize Northerners with climate change impacts on health and guide them in developing research proposals and budgets. Participants shared their observations of community changes and related concerns, collaborating with researchers to identify climate-related health effects. As participants became more acquainted with climate-health intersections, they were encouraged to develop projects to mitigate these effects and were guided on research questions and study design. Workshop participants, in small or whole group formats, designed CBPR projects relevant to their communities and developed appropriate budgets. The CBPR activities included photovoice (Wang and Burris, 1997), community-driven collaborative filmmaking, capacity-building workshops, and various forms of citizen science (though the term was not explicitly used). These efforts aimed to empower communities to address climate change impacts on health through locally driven research and adaptation strategies.
Climate change and mental health: Nepal
Macfarlane et al. (2015) report on a mixed-methods study, using photovoice, undertaken in Nepal to explore subjective mental health experiences focused on participants’ encounters with climate change. The study also aimed to assess whether a 4- to 5-day photovoice training could increase environmental awareness and resilience to climate change. Ten women subsistence farmers from Jumla, recruited by a key informant from the Transcultural Psychosocial Organization, voluntarily participated in the study. All the women participated in three study components: ‘photovoice’, in-depth interviews immediately after the final photovoice session and at a follow-up two weeks later, and self-report questionnaires. The photovoice process involved training participants to use digital cameras, discussing ethics and group norms, and formulating questions about climate change and mental health. One such question developed by participants was, “How will water scarcity affect our well-being and livelihood?” After the initial training session, participants took photographs related to their questions and shared their favorite images in analysis sessions. They deconstructed selected images using the SHOWED method (Gant et al., 2009), which prompts reflection on what is seen, its relevance to their lives, underlying concerns, and potential actions. Photovoice facilitation was culturally tailored and supported by a Nepali research assistant. The photovoice process culminated in two community photography exhibitions showcasing the women’s photographs and narratives. Self-reported mental health, specifically symptoms of depression, was assessed using the Nepali version of the Beck Depression Inventory before and after the photovoice intervention.
Fresh water watch: Canada
One of the significant health impacts of climate change is on shrinking, or changes in the cleanliness, of local water sources. Shupe (2017) describes citizen science undertaken as part of a high-resolution stream water quality assessment project in the Vancouver, British Columbia region of Canada. Between June 2013 and May 2016, field-based workshops were held multiple times a year to train community volunteers in water sampling methods. The goal was for citizens to collect stream data as part of the Fresh Water Watch Program. A total of 192 volunteers, referred to as citizen scientist leaders (CSLs), were trained. During training days, multiple sample measurements were made by teams of volunteers and compared to those taken by instructors. As part of their training, participants were required to pass an online training quiz. Trained volunteers were provided with testing kits and written instruction sheets and given access to an online, on demand training video for review of the appropriate methods. After the training CSLs were assigned sampling locations in streams within their local or nearby community and instructed to sample in the immediate vicinity of the site. They had been trained to carefully draw water from accessible areas on stream banks or bridges using a bucket. In total, the volunteers assisted in the collection of 750 samples across 81 sampling sites representing 49 streams. Shupe (2017) points out that the assistance of the trained volunteers allowed a significant number of measurements to be made which contributed to a better understanding of the seasonal and spatial dynamics of stream water quality. The author emphasizes the value of citizen science in freshwater research.
Indigenous youth leadership: Canada
Lines et al. (2019) present a project carried out in 2016 wherein fifteen Yellowknives Dene First Nation (YKDFN) youth in the Canadian Northwest Territories participated in the ‘On-the-Land Health Leadership Camp’. The authors explain that social determinants of Indigenous health are known to include structural determinants such as history, political climate, environmental and social contexts. They argue that relationships, interconnectivity, and community are fundamental to these determinants and that understanding these determinants from the perspective of Indigenous youth is vital to identifying means of alleviating future inequities in a changing environment. The project was framed to engage youth in Indigenous traditions around a deep respect for and connection with the land of one’s community and ancestors. Using a strength- and community-based participatory approach through an Indigenous research lens, the YKDFN Wellness Division and university researchers crafted a week-long event, the “Youth Health Leadership On-the-Land Workshop” which included sharing circles, photovoice and mural art activities. The qualitative research formed part of a wide mixed-methods research approach that also included two quantitative surveys (a short electronic ‘clicker’ polling survey and a longer iPad survey that employed Likert scale questions on demographics and health). The workshop provided an opportunity for youth to practice cultural skills and convey their perspectives on health and health agency. Views on what a healthy community looks like, health issues, and health priorities were expressed through sharing circles, photovoice, mural art and a modified ‘nominal group’ technique, and recoded through observations, field notes, and personal reflections. In the photovoice project, youth walked around their community to capture images reflecting health issues and priorities in photos or videos. Participatory analysis was done in groups of 3–6 participants, and the discussions were facilitated by the researchers and research assistants. The collective analysis was guided by the SHOWED method (Gant et al., 2009).
Dengue vector control: Singapore
Dengue fever, exacerbated by climate change, poses significant personal and population-level morbidity, especially due to a minority of cases that produce clinically severe disease. Effective public health surveillance is crucial for global response efforts. Sim et al. (2020) detail Singapore’s dengue control program, initiated in the 1960s and managed by the National Environment Agency (NEA). This program integrates multiple principles from the WHO Global Vector Control Response (GVCR) strategy, which advocates for effective, locally adaptive, and sustainable vector control (World Health Organization & Special Programme for Research and Training in Tropical Diseases, 2017). Key GVCR actions include strengthening inter- and intra-sectoral collaboration and community engagement. The Singaporean program leverages existing community structures, such as the People’s Association, grassroots organizations, and Neighborhood Committees, to mobilize residents in checking for mosquito breeding activity and reducing infection sources through the ‘5-Step Mozzie Wipeout’ model. The NEA also trains community members and emergency response teams as Dengue Prevention Volunteers, who educate residents on dengue prevention through household visits, distributing educational materials, supporting roadshows, co-ordinating community-wide eradication events, organizing ‘block parties’ and implementing the mozzie wipeout strategy. In addition to nationwide general messaging, the program also targets specific population groups to encourage them to play a greater role in mosquito control. Focused campaigns engage specific groups, including domestic helpers, construction workers, the elderly, and school children, to enhance their role in mosquito control. Routine house-to-house inspections by NEA officers serve as additional awareness-raising measures. The program includes a research arm led by the Environmental Health Institute, which involves community engagement to disseminate accurate knowledge about transmission vectors and risk reduction. Various methods evaluate community knowledge, attitudes, and practices over time to measure the program’s effectiveness.
Black legged tick distribution: Western United States
Increased average temperatures due to climate change have resulted in a longer season for tick reproduction in many tick-prone regions, resulting in an increase in tick-borne diseases. Porter et al. (2021) presented an interesting example of citizen-science related to the climate-health nexus in their study of the black-legged tick, Ixodes pacificus (I. pacificus), in the Western United States. Measures of tick bite disease risk have traditionally relied on active vector surveillance, requiring researchers to collect ticks from the environment. Given increased climate-driven shifts in tick distribution with serious implications for public health, they argue that it has become vital to more extensively monitor vector and disease distributions, coverage that is difficult and costly for a small scientific team. Responding to this need, Porter et al. (2021) recruited citizen scientists across the Western US into a large-scale tick collection program. Citizens were recruited through a public relations campaign and public website. The citizen scientists participated in the program by mailing collected ticks and associated data to the research laboratory at Northern Arizona University. The submission form covered information related to the characteristics of tick exposure, including date, the human activity being undertaken at the time of exposure, location, and the type of environment in which the ticks were collected. Since the objective of the research program was to raise awareness about tick bite disease and about the study, individuals and public awareness groups disseminated information though social media and other advertising platforms. The details of the citizen science tick collection program are published elsewhere (Nieto et al., 2018). In their article the authors share detailed results obtained through analyzing 18,881 ticks submitted by citizen scientists working over a two-year period. Their findings are presented in the form of niche models predicting the current and future distribution of I. pacificus.
Environmental reproductive justice: United States Gulf Coast
Liddell and Kington (2021) led a CBPR study that was nested within a broader research project investigating the reproductive and sexual health experiences of women from an Indigenous tribe in the American South, Gulf Coast region. The study explored the intersection of environmental justice and reproductive justice with a focus on the ability to have and raise children among Indigenous groups, especially in the Gulf South. These groups are particularly vulnerable to environmental injustice and harm due to climate change, including land loss and oil company exploitation. For tribes that are non-federally recognized and therefore lack political recognition and power, these issues hit hardest. The research team used a descriptive research methodology with semi-structured, in-depth qualitative interviewing as their primary research method. The authors state that they “employed best practices to ensure a just and decolonizing research project.” The community engagement approach involved the establishment of a community-advisory board (CAB) composed of two women leaders of a Gulf Coast Indigenous tribe who helped to develop and pilot the interview questions and assisted throughout the process with recruitment and dissemination of results. The interview guide was designed collaboratively with CAB members to ensure that questions which were most relevant to tribal members were included. CAB members also identified initial seed participants for interviews.
Water microbiology: South Africa
South Africa, like many African nations, faces severe drought due to climate change, leading to significant water shortages and worsening health outcomes, particularly in impoverished communities. In their case study, Black and Sykes (2022) discuss “Bucket Loads of Health” (BLH), a science engagement project facilitated by the Sustainable Livelihoods Foundation (SLF) in the Western Cape province during the 2018 drought. The project focused on water microbiology research and the water-health nexus. Over 12 months, the authors facilitated bi-directional engagement between environmental microbiologists at Stellenbosch University and members of two marginalized communities, one being a research site. Twenty-seven adults from the two communities participated in BLH, co-producing the engagement process design. This included opportunities for knowledge exchange and co-leading exhibition events with the microbiologists. A participatory visual methods approach fostered collective learning. Microbiologists used personalized hand maps to introduce themselves and explain the importance of their research on water quality in informal settlements and townships. During knowledge exchange sessions, scientists delivered bespoke presentations on their research and provided guided tours of their laboratory and microbiology department for the community groups. Community members created maps to highlight local areas and facilities most affected by contaminated water and water shortages, along with personalized body maps and digital stories to depict their embodied experiences of living with these conditions. Exhibition events attended by community residents, researchers, and students showcased the visual materials created by the participating community groups and the microbiology science posters. These events provided an opportunity for shared experiences and reflections on the project’s impact, emphasizing the value of integrating community perspectives in scientific research on water microbiology and health in drought-stricken regions.
Community groups agency in health and climate adaptation: Trinidad and Tobago
In this case study in the rural northeast of Trinidad and Tobago, Scobie et al. (2023) sought to contribute to better understanding community-led action on health and climate change adaptation by investigating community groups’ perceptions of the challenges faced and addressed by their community. The authors explain that Toco was chosen for the study because of the deep connections between the people of Toco and their environment, and because of the long history of community action in this coastal community. The core purpose of the study was to register the voices and perspectives of coastal community groups in the context of a new impetus for action around climate change adaptation and health in the Caribbean region. In their methodology, the researchers built upon the findings of an initial literature review to formulate prompts for ‘elite’ semi-structured interviews and to design an online survey. Local people involved in community development suggested potential participants for both the interviews and surveys. The research team identified 12 active Toco community development groups and held semi-structured interviews with one leader or member of each group, as selected by the groups themselves. Thirty-four active representatives of agencies, groups, or organizations that had been serving the Toco communities for five to over fifty years completed the online surveys. In reporting their findings, the research team focuses on themes of agency, poverty, external agency and support, immediate needs, policy co-production and capacity building. In discussing agency and power, Scobie et al. (2023) raise the concern that whereas practitioners may empower local agency while facilitating communication between different actors, there is a risk that local, participants may lose agency and become the ‘mouthpieces’ of researchers and stakeholders. The authors also highlight the disconnect between local voices and the urgency around mainstreaming mitigation strategies into regional and national climate change adaptation policies.
What reasons are offered for engaging and involving communities in research on climate change and human health?
The range of activities described in the projects identified in this review required extra time, expense, and effort beyond the core scientific work involved. It is helpful to consider the reasons why some research teams go to these additional lengths to involve communities or citizens in their research at the intersection of climate and health and why some believe researchers should go to these extra lengths. While some authors explicitly argued for these efforts, others provided indirect motivations by citing tangible benefits gained through community involvement. Here, we draw on the nine project papers summarized above as well as the eight closely related review and theoretical papers to help interpret the experiences shared by the project teams.
Involving communities can improve science, especially in climate-health research
Consistent with the wider literature supporting community and public engagement in science and considering the distinctive challenges raised by the climate and health context, several teams demonstrated how involving communities can strengthen science. Community involvement improves the relevance of research priorities and research questions through attention to community knowledge and informs methods to ensure that approaches fit the context of community health and environmental burdens, especially for marginalized populations. Several teams also emphasized the distinctive value of involving communities in climate-health research, improving the overall responsiveness and adaptability of the research to rapidly changing environmental determinants of health in specific regions. Often teams cite or illustrate more than one of these rationales.
To illustrate how community involvement can strengthen research priorities and questions, for example, the Singapore Dengue project showed how local knowledge and specific observations gained only through local partnerships helped inform responsive interventions to a persistent vector borne disease (VBD) that has resisted eradication (Sim et al., 2020). Through a partnership with the Singapore Contractors Association Limited (SCAL), public health scientists were able to study and respond to the role that construction sites play as a driver of dengue transmission, “since rainwater-filled land excavation holes, construction materials, and equipment (e.g., water tanks, skips, canvas sheeting) can become Aedes habitats.” (Sim et al., 2020). Parham et al. point out that the next generation of risk assessment methods should take the complexity of VBD transmission dynamics into account, including the effects of broader societal contexts in which pathogen transmission occurs, if more reliable evaluations of the effects of climate change on VBDs are to be undertaken (Parham et al., 2015).
Other projects illustrated how advice from communities can help to characterize the nature of a health problem, identify infection pathways, or shape practical solutions in ways that are more responsive to community needs in the face of rapid climate-health crises. The Northern First Nations and Inuit climate change and health adaptation program offered a powerful example of community shaped research, with supported projects being directly designed by community groups and directly responsive to health burdens prioritized by the community (Peace and Myers, 2012). The South African BLH project helped the microbiologists involved to appreciate how informal settlement dwellers were impacted by water shortages, difficulties faced in safe water storage, and other issues that have informed their subsequent research design. Specifically, participating in knowledge exchange sessions with community members who were residing in the microbiology research setting highlighted to the team the importance of engaging and involving community representatives prior to embarking on a research project. In the tick-borne disease citizen science project, the team was clear that the scale of surveillance needed to study the problem would not have been possible without citizen volunteers—the involvement of citizens extended the reach of the scientific work, and shortened the time needed for data collection at scale.
Bardosh et al. (2017) argue that tackling VBDs driven in part by climate change requires a paradigm shift, away from simple disease-models to a more dynamic and ‘biosocial’ model of public health research with greater investment in “meaningful public participation, strengthening of health systems, sustainable development, wider institutional changes and attention to the social determinants of health, including the drivers of co-infection.” For example, the Nepalese project on mental health offered powerful insights into a stigmatizing and under-reported health effect of climate change (Macfarlane et al., 2015). Similarly, the Gulf South project documented underreported environmental impacts on marginalized Indigenous women’s reproductive health (Liddell and Kington, 2021).
All projects in the review illustrated reasons for involving communities and members of the public that were distinctive to the intersecting problems of climate and health. Across the projects and theoretical discussions, teams conveyed how understanding the environment’s role in health requires engaging the people who live within it. Shupe (2017) describes how community members and citizens can contribute valuable background knowledge about climate-health patterns over time or gather environmental observations from locations that may be difficult for researchers to reach [for example, Porter et al. (2021) and Shupe (2017)]. Other teams noted that climate-driven disease patterns can be difficult to predict without the help of citizens. Porter et al. (2021) hypothesize that changing ecological conditions, including those driven by the changing climate, will result in an inevitable shift in tick dispersal and patterns of tick bite disease. They claim that predicting the potential future distribution of ticks will provide insight into significant shifts of pathogens and disease and enable public health agencies to anticipate and combat these threats—engaging the public through observational assistance will be critical for tracking shifting patterns. In the face of shifting climate patterns, Peace and Myers argued that community members can provide insights about specific environmental barriers and facilitators to consider in the design of local climate adaptation strategies (Peace and Myers, 2012).
Last, involving the public can help bring interventions and adaptation strategies to scale (Sim et al., 2020). As Porter et al. (2021) discuss, the low cost, continuous, rapid, extensive, and spatially diverse sample collection made possible by a large-scale citizen science approach has an important role to play in mitigating climate sensitive disease. In response to concerns that citizens might lack the relevant scientific expertise to bring interventions to scale, Shupe (2017) draws on the perspectives of other experts in claiming that with appropriate capacity development and oversight, volunteers can often collect data of equal quality to those collected by ‘experts’ (Danielsen et al., 2014). Research referred to by Kelly et al. (2020) in their review argues that citizen scientists can develop into collaborating experts when enabled by scientists to engage and communicate as ‘equals’.
Involving communities in research strengthens both community and researcher knowledge around climate and health science
Beyond improving science, the projects presented demonstrated direct benefits to the communities involved in research, particularly around knowledge and learning. Involving communities in climate-health research can raise awareness of the effects of climate change, impacts on health, and potential mitigation efforts (Bardosh et al., 2017). Specifically, authors reported better understanding by community members about the objectives, methods and value of climate-related field studies being undertaken within their communities (Black and Sykes, 2022). The two research projects that involved Indigenous groups in Canada provide examples of transformative learning through community-science engagement activities, including shifts in perspective about the land and environment. As Lines et al. (2019) describe, the YKDFN youth recognized that participating in cultural activities which strengthened their connection to the land could result in better health for their community. Indigenous participants also realized the importance of their active role in shaping future health research and their agency to address priority environmental-health issues.
These transformational shifts in community awareness and knowledge can be transferred and sustained over time. The program described by Peace and Myers (2012) offers an example of how CBPR at the intersection of climate and health can be implemented across multiple communities and sustained over many years. The climate change and health adaptation program they describe provided opportunities for participants to develop their own research proposals and budgets and widely showcase the results of their work across Indigenous community networks (Peace and Myers, 2012). The initiative resulted in the development of extensive community-driven climate adaptation strategies engaging infrastructure (including a media research lab focusing on women’s health and workstations designed to build local skills in ice monitoring) and culturally relevant tools. Indigenous participants engaged through the program conveyed that their involvement had transformed their knowledge about the links between climate change and health (Peace and Myers, 2012). In turn, Martello (2008) argued that the Inuit live closely with the environment; hold valuable environmentally rooted knowledge and traditions important for diet, spirituality, culture, and economics.
Other articles further demonstrated how engaging and involving communities in programmatic interventions led to decreased health threats in at-risk settings. By engaging residents in dengue control through household inspections, the NEA discovered that ‘holders’ supporting bamboo poles assembled outside high-rise apartments for drying clothes were harboring substantial numbers of Aedes mosquito larvae. The subsequent re-design of the clothes drying system, contributed to source reduction efforts by diminishing mosquito breeding grounds and furthermore made the process of hanging out laundry physically safer for residents (Sim et al., 2020).
Research teams also gained important learning through their efforts to engage and involve communities in their work. Black and Sykes (2022) note that a role play performed by community participants “opened a difficult but needed conversation” about how environmental water science was being perceived by community members living in a research setting. The conversation helped the participating scientists to understand what people living in informal settlements and facing the impacts of climate on health consider to be priorities for research. MacFarlane et al. (2015) highlight the enjoyment of a photovoice process amongst Nepali women photographers. The authors emphasize that the approach taken to engaging and involving communities in research has important implications for their experience of participation and this extends to how methodology can influence the mental health of those taking part. The authors report a significant reduction in depression following the photovoice sessions. MacFarlane et al. (2015) conclude that photovoice could be applied as a community-based and participatory mental health intervention in the context of climate change and be used as a “well-accepted” method for building needed social capital.
Involving communities is ‘the right thing to do’
While all projects demonstrated the added value of community involvement to enhance scientific and community knowledge, some teams went further and discussed or demonstrated important ethical or social justice considerations to motivate community involvement. Authors highlighted that respecting and responding to local knowledge can equip communities to monitor and modify their environment, increasing their agency over their community’s health and well-being (Peace and Myers, 2012; Bardosh et al., 2017; Scobie et al., 2023). Demonstrating respect for persons within and across a community requires their meaningful involvement in shaping priorities for future climate-health research that best align with community needs (Black and Sykes, 2022). The BLH project in South Africa was planned to support the participating research team in learning about the perceptions and acceptability of their water research in an informal settlement. The CBPR project in the Northern territories of Canada (Peace and Myers, 2012) was designed to foster ownership of the research by the community participants and ensure their meaningful contribution to the pool of knowledge gathered for shaping climate change mitigation strategies. One of the community-based researchers reported that they appreciated having a “space provided where communities can share their knowledge, their research, and their plans of how to deal with the changes through adaptation plans.” Kelly et al. (2020) suggest that ownership of research in the context of citizen science may be bolstered by engaging citizen participants in promoting and communicating about a research project, and in disseminating its results. Complementing scientific rationales, is a call to acknowledge and to act upon local insights about how the impacts of climate change are affecting public health, not only to ensure more responsive research, but importantly to foster citizen’s agency to be part of the solution through community activist groups (Lines et al., 2019). Scobie et al. (2023) discuss the disillusioning effect of tokenistic engagement for agenda setting and policy co-production on the agency of committed community development groups.
Beyond the scientific importance of understanding structural determinants of health, some teams embraced an overt appeal to social justice. Bardosh et al. (2017) observe that climate change “disproportionately impacts people in tropical climates with inadequate access to health services, poor housing, weak governance structures, and socio-economic underdevelopment.” They acknowledge the regional and global impact caused by vector-borne disease epidemics, but they also “enact a quieter ‘hidden’ endemic toll on local communities, perpetuating poverty, disability, malnutrition, and social isolation” (Bardosh et al., 2017). Traditional epidemiological disease models have not adequately considered “how local communities adapt in the context of an epidemic, or how they use socio-cultural capital to mitigate endemic disease challenges” (Bardosh et al., 2017).
Liddell and Kington (2021) sought to understand the contribution of settler colonialism and historical oppression to environmental reproductive injustice among an Indigenous tribe in the Gulf South of the United States. The underpinnings of these structural determinants on the ability of women to have and raise children, and further implications of climate change, were central to the research inquiry. Further, reparative justice required shifting research practices to correct colonial power imbalances in the way the research was carried out. Tribal leaders played a crucial role as community advisors in developing interview questions, assisting with recruitment of interviewees, and supporting the dissemination of the research findings. For example, researchers followed the advice of tribal advisors to take a life-history-type approach to the interviews, and ethical approval to undertake the research was sought from both a University Institutional Review Board and a tribal council.
In another Indigenous health project, CBPR was seen as a way of breaking the cycle of health inequities; as Lines et al. (2019) expressed, “the perspective of Indigenous youth is vital to identifying the means of alleviating future inequities.” The authors took a decolonizing CBPR approach, grounded by Indigenous community relations, to understand youth insights on the social determinants of Indigenous health, including their viewpoints on history and politics. The researchers aimed to challenge the oppressive acts of colonization by reconstructing concepts of health to include Indigenous knowledge. The research process integrated multiple interactive components including photovoice and mural art to involve youth participants in generating and analyzing data. Thus, unique Indigenous worldviews informed the prioritization of health solutions. A perhaps deeper intention highlighted by the authors was to provide opportunities for the participating youth to “practice cultural skills” around connections to ancestral land, skills that had nearly been lost to colonial attempts to eradicate ancestral practices (Lines et al., 2019). For Peace and Myers (2012), regained cultural skills included “how to observe the land and its changes, how to hunt and respect the land and wildlife, which helped to develop valuable attributes such as patience, respect, self-sufficiency, self-esteem and traditional knowledge on how their natural world is changing.” Corburn argues that researchers should begin urban environmental justice research by asking how historical institutional decisions may have influenced current inequitable burdens and how multiple institutions may have had intersecting and aggregated impacts on ‘communities of color’ (Corburn, 2017).
As Martello (2008) reflected, the history of environmental science research with Indigenous peoples reflects the deeper social and political tensions of colonialism and reparation: “Recent analyses of climate change in the Arctic are intersecting, with long histories belonging to Indigenous peoples – histories of adaptation, ingenuity, resourcefulness, community, spirituality, and strength, but also of occupation, oppression, racism, and social, economic, and health problems. Environmental science has had its own role in these histories” (Martello, 2008). Examples of early and ongoing efforts to support community participatory research in partnership with Arctic Indigenous peoples, argues Martello, have shifted perceptions of what counts as scientific expertise and who may speak with authority in climate sciences.
Participatory research was also described as a tool for interrogating political drivers of environmental health impacts on the community. Confronting the political underpinnings of access to safe water, sanitation and hygiene was a key conceptual driver for the BLH project in South Africa (Black and Sykes, 2022). A core objective was for participating community members to bring the everyday health related impacts of water shortage in their communities to the attention of local government authorities, through a striking visual methods approach that would be difficult to ignore. These techniques were also used to elevate politically hidden voices around the impacts of climate change on health. Similarly, the primary rationale of MacFarlane et al. (2015) for engaging and involving community members in their research was to elicit perspectives of climate change as seen directly through the eyes of women subsistence farmers living in a high-risk context in Nepal, using photovoice to tell their story through collectively curated images.
The Singaporean project on dengue control takes an overtly political stance on the involvement of citizens in the ongoing public health surveillance and research. The approach mirrors other aspects of Singaporean public life, relying on centralized control and planning and a strong sense of collective responsibility for maintaining a healthy environment. Government legislative and punitive power are leveraged for behavior change—including the use of policies, penalties, and fines (Sim et al., 2020). Responsibility, however, is shared between citizens and government. Local politicians are expected to prevent outbreaks of dengue in their constituencies, describing how they include communication about the importance of dengue prevention to residents during walkabout sessions. This collective responsibility for the environment and health, Sim et al. (2020) explain, reflects efforts over the past 60 years to share a vision of Singapore as a ‘City in a Garden’, where biodiversity and a green environment are seen as solutions to improving the health, well-being, and economic competitiveness of its citizens. Bardosh et al. (2017) also underscore the power of ‘social responsibility’ as a lever for galvanizing biosocial change in the face of climate driven disease, citing the pivotal Alma Ata Declaration of 1978 as a watershed agreement in global health (International Conference on Primary Health Care, 1978). Similar to the Singaporean model, they argue that responsibility must truly be shared between citizens and government to effect sustainable change: “Communities respond best when they see that civil authorities are taking responsibility for infrastructure issues, such as water provision and drainage problems” (Bardosh et al., 2017).
What limitations, challenges, or ethical considerations arise when involving communities in climate-health research?
Across the nine projects featured in this review, teams shared valuable cautionary lessons when involving communities and members of the broader public in research at the intersection of climate and health. While involving members of the public in data collection can strengthen research by bolstering the amount of data available for analysis and geographical reach of data collection, there are important limitations when considering a community’s technological capacity and potentially limited resources. For example, Shupe (2017) acknowledges that the citizen scientist model of water sampling may not be appropriate for more resource-intensive data necessary to fully explore the quality of surface water given the scarcity of resources in the study communities. Citizen science projects often require citizens to undergo training and upload data via the internet. Both citizen science projects in this review (Shupe, 2017; Porter et al., 2021) required interested members of the public to register and be trained on project websites. In the water collection project, citizen science leaders tested samples in the field and used smart phones to enter data into an online app.
These research activities required participants to have strong and reliable access to the internet. The success of the tick collection program in the Western US also relied on a well-functioning mail system. As cost-free access to the internet is often constrained or non-existent in marginalized communities in many low- and low-to-middle-income countries, and this is coupled with a failing postal system, the possibility for citizen science approaches of this nature to be taken up at a global scale in at-risk settings is questionable without additional investment in community infrastructure. As Bardosh et al. (2017) underscored the importance of government-citizen shared responsibility they also acknowledged that “a major constraint for vector-borne disease control is that there are still relatively limited examples of how to institutionalize participatory approaches in developing countries in the context of limited resources and weak institutional support.”
A central ethical principle of CEI in research is to ‘do no harm’ with the intention that people take part of their own free will in the absence of coercion, punishment, or increased vulnerability (UNICEF, 2020). Sim et al. (2020) acknowledge that the dengue control activities in Singapore have been accompanied by government legislation and law enforcement, which the NEA use alongside community engagement to enhance public compliance in the vector reduction strategy. Operations teams are authorized by the government to enter households to conduct inspections, and residents are subject to “monetary penalties” if mosquitos at certain stages of the life cycle are found on the premises. The authors further refer to the use of a ‘carrot and stick’ approach to source reduction in behavior change campaigns led by a communications division of national government. While the NEA approach to vector reduction has been effective in decreasing dengue transmission, its achievements have to some degree been reliant on punitive measures and the approach also risks stigmatization of households.
Reflecting on the principle of ‘do no harm’, Black and Sykes (2022) report body mapping as an effective approach for community members to illustrate their embodied experiences of climate change impacts on health, yet the technique is not benign. The authors explain that immersive visual techniques can stir participants to share deeply personal experiences and emphasize that great care should be taken to support and safeguard those taking part in visual methods processes. This finding resonates with the views of MacFarlane et al. (2015) regarding the potential for CEI in research to impact the mental health of affected community members and that the need for adequate care mechanisms should be in place to support those who need them.
Citizen and community involvement in research occurs alongside everyday lives, obligations, and commitments. It requires substantial time and opportunity costs for participants. It has long been argued that community members who make efforts to engage in research and be involved in its progress should be compensated for their time (Black et al., 2013) yet there was little mention of compensation across the projects showcased here. For payment to be feasible, and payment amounts to be meaningful to participants, research budgets need to include resources for this, which currently is not always the case. Peace and Myers (2012) also highlight the duration of funding as a major challenge for the climate change and health adaptation program for Northern First Nations and Inuit in Canada. The program was limited to funding of 1 year at a time and delays in receipt of funds brought about serious challenges for community-driven research. In a similar vein, Black and Sykes (2022) have argued that funders and research institutions need to match professed commitments to engagement with training and resources to support researchers and community members in responding to the needs and aspirations surfaced through community engagement efforts. These authors introduce the concept of ‘engagement integrity’ to highlight the gap between recommended standards of community engagement and what is realistically achievable in projects that are constrained by funding, time, and political will. Liddell and Kington (2021) also raise the issue of policy engagement. They state that their findings around environmental reproductive justice in Gulf South imply that local Jumla policy should be adapted to support women “in place” and that dedicated resources are needed for this. Their research process did not, however, include an advocacy component, so the possibility of this happening remains uncertain.
A further significant challenge identified by Peace and Myers (2012) was the requirement for ethics review for the CBPR activities which largely required the same standards as western-based laboratory or medical research. These requirements did not consider the distinctive nature of CBPR and the integration of traditional knowledge, which needs to be protected. The authors argue that these and other distinctive ethical considerations be incorporated in ethics review processes to recognize the unique nature of CBPR.
Sim et al. (2020) highlight the efforts of the Singaporean dengue control program to identify novel public health messaging techniques to prevent ‘engagement fatigue’. The global fight against HIV showed that mass media interventions may be useful in reducing global HIV/AIDS disparities because of their reach and effectiveness (LaCroix et al., 2014). Awareness raising approaches around climate-health challenges will require constant efforts to stay current and be compelling and effective, and this will be strengthened through the consultation and participation of community and public stakeholders.
Discussion
Climate-health science represents a rapidly emerging area of cross-disciplinary research (Romanello et al., 2023). As the field grows, we can expect to see more published work on innovative study designs, including those involving communities. As the reviewed projects demonstrate, engaging and involving communities and the wider public in research at the climate-health nexus can make crucial contributions to mitigating the health impacts of climate change by improving the responsiveness and reach of science and reinforcing the knowledge, awareness, and agency of citizens and communities to effect change. The projects and programs featured illustrate the overlapping scientific and community benefits, as well as important appeals to social justice. Taking a range of methodological approaches, including citizen science, CBPR, visual methods, and other engagement strategies, these examples demonstrate how CEI has been undertaken to develop appropriate climate adaptation and mitigation strategies (Peace and Myers, 2012), understand how approaches to community engagement in climate-health research can influence participants’ mental health (Macfarlane et al., 2015), investigate the quality and conditions of the environment (Shupe, 2017), foster health agency among Indigenous persons (Lines et al., 2019), control the spread of climate-related disease (Sim et al., 2020) estimate the distribution of disease-causing vectors (Porter et al., 2021), explore the intersections of health and environmental justice (Liddell and Kington, 2021) and elucidate perceptions of research and health priorities in settings at high risk of climate-driven disaster (Black and Sykes, 2022). Climate-driven disease, itself, is an emerging cross-sectional area of research; as such, the far-reaching health impacts of climate change are still poorly understood (Romanello et al., 2023). Several of the projects illustrated how community involvement in research can shed light on otherwise hidden aspects of this emerging disease burden, improving the quality and accuracy of global epidemiology with important implications for directing resources to marginalized communities.
The breadth and complexity of climate-health challenges necessitates interdisciplinary research whereby expertise in multiple fields is integrated for the identification of effective solutions (Schipper et al., 2021). Given the intricate links between the changing climate, human activity, human health, and ecosystem health, it follows that research approaches ought to reflect and account for cross-cutting considerations such as environment-human-genetic interactions, the importance of multi-disease models, and the significance of health systems analysis (Bardosh et al., 2017). Alongside the need to engage communities and members of the wider public in health science research there is a parallel requirement for CEI in environmental research, ecology, engineering, architecture, and city planning (for example) as these other climate-related research areas will also benefit from contextual knowledge, lived experiences and local insight into problem solving. The requirement for more inclusive research design also extends to clinical trials, some of which have already taken up an adaptive design approach (Berry, 2011) which could be expanded to incorporate community feedback. It has been shown that CBPR with people who are living with the impacts of hazardous environments can not only support the identification of locally driven solutions but also unpack mechanisms of intervention, distinct groupings of accountability and defined forms of collaboration (Black et al., 2023).
There are several bi-directional benefits — for research teams and for the community — that echo well established rationales for community engagement in health research more generally. These include enhancing both the relevance and the methodology of research (Sprague Martinez et al., 2018). As seen with the rise of citizen science, involving citizens in data collection and observations, with the proper training, can extend the reach of studies that would otherwise not be possible (Shupe, 2017; Porter et al., 2021). Unique to climate-health science is the need to have ongoing, rapid observations within communities during cyclical and dynamic environmental events and disease outbreaks (Bardosh et al., 2017). The nature of relationships that are critical for more sensitive approaches to CEI in research, such as participatory visual methods, require time and funding to meaningfully involve participants in shaping science and to build trusting, sustainable partnerships between scientific teams and communities (Black et al., 2017; Treffry-Goatley et al., 2021).
The extent to which researchers can engage and involve communities and members of the wider public in research studies is strongly dependent on research contexts. The breadth and depth of engagement and involvement that is possible may depend on whether research is being conducted at hyper-local, local, provincial, district or national levels, as well as the scale, engagement experience, and commitment of the research teams and other stakeholders (organizations) concerned. Depending on their circumstances, scientific teams have varying access to technology, infrastructure, services, expertise and support. Moreover, the availability of financial resources will be dependent on the research sponsor. The variation observed in the extent of CEI in the projects we have reviewed here may be instructive in demonstrating that not all projects can or should take a deep dive approach to engagement. The Singapore case study is interesting in its longevity—several decades long—yet the program took a fairly high-level approach to involving community members in shaping the science. Similarly, teams adopting citizen science methods may be able to adopt some of the benefits of CEI, including bi-directional learning about climate change and health, more responsive sampling, and wider reach, when deeper investments in communities are not feasible or ethically appropriate. It was clear from the studies explored here that one size does not fit all. It was also clear that important ethical considerations need to be made when researchers commit to in-depth CEI, such as CBPR. For example, whilst Scobie et al. convey the potential of practitioners and experts to empower local agency by facilitating communication between multiple stakeholders at different scales, they also highlight the following barrier:
‘[However] in relationships of inequality, there is a risk that local, weaker actors may lose agency and become the mouthpieces (ventriloquists, marionettes, or puppets) of researchers and others external actors’ (Meriläinen et al., 2022).
Perhaps most compelling when exploring all papers in depth were the direct and indirect appeals to more normative reasons for CEI, including appeals to climate justice, restorative justice, and epistemic justice. Several of the studies and reviews argued that embedding CEI in climate-health studies is especially important for people living in marginalized and at-risk settings, given the knowledge and power sharing inherent in thoughtful CEI approaches. Kelly et al. point out that the power dynamics evident in engaged research stem from levels of knowledge or ‘expertise’ as scientists typically establish and lead projects. The authors highlight the need to improve understanding around power in citizen science, for example (Kelly et al., 2020). Consistent with the wider literature on community engagement in global health research, there was a cross-cutting appreciation that research conducted in marginalized communities ought to actively engage and involve leaders and members of that community. This is best captured in a familiar mantra from Charlton’s earlier work on community engagement in global health, “nothing about us, without us” (Charlton, 1998). This idea that communities ought to have a say in research that is conducted in relation to them, takes their time, samples and effort, and potentially exposes them to the risks of research is equally important in climate-health research, especially as it begins to track the rapidly growing climate-health burden in the Global South. The fact that only four out of the nine featured projects were undertaken in the Global South underscores the need to extend these efforts much further into the majority world.
The climate crisis is disproportionately impacting those who live in places with constrained health care facilities, inadequate services, poor infrastructure, and insufficient local resources to adapt to changing weather patterns. Many of these at-risk communities have suffered historical and contemporary injustice (Black and Sykes, 2022). The urgent need to advance climate literacy and prioritize research that involves and consults people living in marginalized settings beset with environmental hazards is supported by appeals for restorative justice (Liddell and Kington, 2021). Arguments from epistemic justice also recognize that knowledge is power, and that greater acknowledgement should be given to the potential of local knowledge for promoting the ethical scientific study of broad and complex health challenges (Pratt and De Vries, 2023). Former oppression of Indigenous communities provides a powerful example of the need for restorative justice and more rigorous commitment to CBPR. Engaging and involving Indigenous people in research on climate and health will deepen the integration of unique and important worldviews into health solutions based on community strengths and capacities for action. This supports an overall evolving recognition that Indigenous peoples’ conceptions of the world and problem-solving approaches offer distinctive, innovative solutions to colonial health effects when integrated into the foundation of health programs. As illustrated in two of the featured Indigenous health projects, there is a crucial role for involving youth in defining health meaning and priorities in the face of environmental change that are connected to culture, land, and specific to ways of life (Peace and Myers, 2012; Lines et al., 2019).
In the context of climate change, it has been proposed that work toward more equitable global health outcomes is likely to require intersectoral collaborations and support for affected communities (Markle et al., 2023). Sim et al. (2020) emphasize that the success of the dengue control program in Singapore has been dependent on the close collaboration of the NEA with other government ministries, town councils, the private sector, and academic and research institutions. Scobie et al. (2023) highlight the capability of community leaders in Toco to mobilize community resources that can help to bridge a ‘local-national policy gap’ and facilitate community participation in the implementation of local adaptation policy. Supportive and effective collaborations to address climate health impacts will require knowledge exchange through transdisciplinary partnerships and agreements about roles, responsibilities and potential interventions, between research teams, community members, government officials and other societal stakeholders (Wright et al., 2021). It is crucial to emphasize that engaging and involving community members and public stakeholders in research can raise tensions around responsibility and accountability for responding to emergent action plans and implementing solutions identified through participatory processes (Shaw, 2017). Minkler et al. (2008) highlight the need for participants in the action phase of CBPR to gain increased policy engagement skills and better knowledge about the policy-making process, and encourage trainings from “policy mentors” and other learning approaches to increase community capacity in this area. They also emphasize the critical need to augment the level of institutional funding available for CBPR partnerships aiming to achieve environmental justice.
Of growing concern are the psychological and emotional impacts of climate change and how these are likely to have uneven impacts on communities and individuals, depending on place-based, economic, geographic and cultural differences; impacts that may give rise to experiences of disempowerment, inequality and injustice (Adams, 2021). Our findings show that the mental health implications of engaging and involving at-risk community members in research at the intersection of climate and health raise important ethical considerations. It has previously been suggested that psychiatrists and community health workers have an important role to play in integrating mental health services into primary care, promoting community resilience, and educating communities about the mental health effects of climate change (Maughan et al., 2014). Furthermore, research groups often lack the funding, capacity, and resources to address the clear need for vast structural changes conveyed by affected community members during research engagement activities, which can leave researchers feeling powerless and ethically conflicted (Black and Sykes, 2022). Discussion forums including debriefing and ethics discussion groups (Kelley et al., 2016; Molyneux et al., 2021) could support researchers to navigate distress and vulnerability that may arise during CEI at the intersection of climate and health. It has also been shown that building community networks around ongoing research helps build solidarity around common public health burdens (Pratt et al., 2020; Khirikoekkong et al., 2023).
An important limitation of this review is that it likely underrepresents the prevalence of community-science partnerships in the climate change and health field. Because community engagement is not necessarily considered part of the scientific methodology of a project and is perceived by some researchers to be a formative, preparatory or obligatory phase of work, community engagement efforts may not always be reported and described in scientific papers. While our initial literature review found a large number of papers, very few reported sufficient details on either the approach to community involvement or rationale for community involvement, details necessary for an in-depth qualitative review (see Supplemental material). Furthermore, it may be that other projects from the Global South exist that were not identified in our search for English-language publications. Thus, it is possible that our sample underestimates how many scientific teams are involving communities in their climate-health work. Nonetheless, it is critical to report on examples, successes and challenges.
In acknowledging the barriers and limitations of CEI, it is essential to be cognizant of the costs, effort, and time involved for community members, public stakeholders, and scientific teams to participate in engaged research, as well as the ethical considerations, especially when it is not possible to sustain community-science partnerships or act on community aspirations for climate adaptation measures. Meaningfully and effectively integrating communities’ vital contributions requires a significant shift in how impactful research is designed and funded and will require institutional change (Markle et al., 2023). In recognizing these requirements and being open to change, the scientific community can play a profound and critical role in addressing the health impacts of climate change, responding to climate inequality, and advancing social justice.
Conclusion
In the face of rising heat, increasing water shortage and regular flooding events, there is an escalating need for research spanning and connecting with the fields of climate change and health to be designed more inclusively. We have argued that science at the intersection of climate and health should incorporate the experience, insights, priorities, and capacities of communities and the wider public into research design and practice. Our conclusion is supported by overlapping scientific, social justice and ethical reasons shared by scientific teams and community participants engaged in this work. The ethical conduct of engagement and involvement with at-risk populations will be strengthened through building equitable partnerships between researchers and community members. This will enable a more attuned investigation of causal pathways of disease while simultaneously involving communities and citizens in improving the effectiveness of interventions, raising awareness, and where appropriate advocating for social and political change. Perhaps most importantly in confronting a global climate threat, involving communities meaningfully in science can be galvanizing, instilling a sense of fellowship in a threat facing all of us.
Author contributions
GB: Conceptualization, Data curation, Formal analysis, Methodology, Writing – original draft. EJ: Conceptualization, Writing – review & editing. WK: Conceptualization, Writing – review & editing. SP: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Writing – review & editing. BH: Writing – review & editing. MM: Conceptualization, Funding acquisition, Project administration, Resources, Writing – review & editing. MK: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Supervision, Writing – original draft.
Funding
The author(s) declare that financial support was received for the research, authorship, and/or publication of this article. This project was supported by the Wellcome Trust [203132], [221719], and [216355] and by a Greenwall Foundation Making A Difference grant entitled, “Dilemmas of health equity in global health research: a study of research on climate-sensitive infectious disease.” The Trust and Confidence research programme at the Pandemic Sciences Institute at the University of Oxford is supported by an award from the Moh Foundation.
Acknowledgments
The authors would like to extend special thanks to: Claire Twose, MLS (Lead Informationist, Welch Medical Library, Johns Hopkins Medical Institutions, and Associate Scientist, Department of Health Policy and Management, Johns Hopkins Bloomberg School of Public Health) for her essential contributions to the literature review design; Professor Lisa Rasmussen for her expert input on Citizen Science; and colleagues across the Oxford-Johns Hopkins Global Infectious Disease Ethics Collaborative (GLIDE) for their input during earlier presentations of this work.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Supplementary material
The Supplementary material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fclim.2024.1456417/full#supplementary-material
References
Adams, M. (2021). Critical psychologies and climate change. Curr. Opin. Psychol. 42, 13–18. doi: 10.1016/j.copsyc.2021.01.007
Adhikari, B., Pell, C., Phommasone, K., Soundala, X., Kommarasy, P., Pongvongsa, T., et al. (2017). Elements of effective community engagement: lessons from a targeted malaria elimination study in Lao PDR (Laos). Glob. Health Action 10:1366136. doi: 10.1080/16549716.2017.1366136
Bardosh, K. L., Ryan, S., Ebi, K., Welburn, S., and Singer, B. (2017). Addressing vulnerability, building resilience: Community-based adaptation to vector-borne diseases in the context of global change. Infect. Dis. Poverty. 6:166. doi: 10.1186/s40249-017-0375-2
Bedson, J., Jalloh, M. F., Pedi, D., Bah, S., Owen, K., Oniba, A., et al. (2020). Community engagement in outbreak response: Lessons from the 2014-2016 Ebola outbreak in Sierra Leone. BMJ Global Health. 5:e002145. doi: 10.1136/bmjgh-2019-002145
Berry, D. A. (2011). Adaptive clinical trials: the promise and the caution. J. Clin. Oncol. 29, 606–609. doi: 10.1200/JCO.2010.32.2685
Black, G. F., Davies, A., Iskander, D., and Chambers, M. (2017). Reflections on the ethics of participatory visual methods to engage communities in global health research. Global Bioethics 29, 22–38. doi: 10.1080/11287462.2017.1415722
Black, G. F., Dick, L., Petersen, L., and Mpofu-Mketwa, T. (2023). Participatory visual methods and the mobilization of community knowledge: working towards more equitable research processes. Global Health Network Collect. doi: 10.21428/3d48c34a.34c18e04
Black, G. F., and Sykes, P. (2022). Steps toward engagement integrity: learning from participatory visual methods in marginalized South African communities. Front. Public Health 10:4905. doi: 10.3389/fpubh.2022.794905
Black, K. Z., Hardy, C. Y., De Marco, M., Ammerman, A. S., and Corbie-Smith, G.Council, B, et al. (2013). Beyond incentives for involvement to compensation for consultants: increasing equity in CBPR approaches. Prog. Community Health Partner. 7, 263–270. doi: 10.1353/cpr.2013.0040
Bothwell, L. E., and Kesselheim, A. S. (2017). The real‐world ethics of adaptive‐design clinical trials. Hastings Cent. Rep. 47, 27–37. doi: 10.1002/hast.783
Butler, C. C., Hobbs, F. D. R., Gbinigie, O. A., Rahman, N. M., Hayward, G., Richards, D. B., et al. (2023). Molnupiravir plus usual care versus usual care alone as early treatment for adults with COVID-19 at increased risk of adverse outcomes (PANORAMIC): an open-label, platform-adaptive randomised controlled trial. Lancet 401, 281–293. doi: 10.1016/S0140-6736(22)02597-1
Carmona, R., Reed, G., Thorsell, S., Dorough, D. S., MacDonald, J. P., Rai, T. B., et al. (2023). Analysing engagement with indigenous peoples in the intergovernmental panel on climate Change’s sixth assessment report. npj Climate Action. 2:29. doi: 10.1038/s44168-023-00048-3
Charlton, J. I. (1998). Nothing about us without us: Disability oppression and empowerment. 1st Edn. Berkeley, Califonia: University of California Press.
Corburn, J. (2017). Concepts for studying urban environmental justice. Curr. Envir. Health Rpt. 4, 61–67. doi: 10.1007/s40572-017-0123-6
Danielsen, F., Jensen, P. M., Burgess, N. D., Altamirano, R., Alviola, P. A., Andrianandrasana, H., et al. (2014). A multicountry assessment of tropical resource monitoring by local communities. BioScience. 64, 236–251. doi: 10.1093/biosci/biu001
Gale, N. K., Heath, G., Cameron, E., Rashid, S., and Redwood, S. (2013). Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med. Res. Methodol. 13:117. doi: 10.1186/1471-2288-13-117
Gant, L. M., Shimshock, K., Allen-Meares, P., Smith, L., Miller, P., Hollingsworth, L. A., et al. (2009). Effects of Photovoice: civic engagement among older youth in urban communities. J. Community Pract. 17, 358–376. doi: 10.1080/10705420903300074
Holzer, J. K., Ellis, L., and Merritt, M. W. (2014). Why we need community engagement in medical research. J. Investig. Med. 62, 851–855. doi: 10.1097/JIM.0000000000000097
International Conference on Primary Health Care (1978). Declaration of Alma-Ata. WHO Chron. 32, 428–430.
Karris, M. Y., Dubé, K., and Moore, A. A. (2020). What lessons it might teach us? Community engagement in HIV research. Curr. Opin. HIV. AIDS. 15, 142–149. doi: 10.1097/COH.0000000000000605
Kelley, M. C., Brazg, T., Wilfond, B. S., Lengua, L. J., Rivin, B. E., Martin-Herz, S. P., et al. (2016). Ethical challenges in research with orphans and vulnerable children: a qualitative study of researcher experiences. Int. Health 8, 187–196. doi: 10.1093/inthealth/ihw020
Kelly, R., Fleming, A., Pecl, G. T., Von Gönner, J., and Bonn, A. (2020). Citizen science and marine conservation: a global review: citizen science and marine conservation. Phil. Trans. Royal Society B 375:20190461. doi: 10.1098/rstb.2019.0461
Khirikoekkong, N., Asarath, S., Nosten, S., Hanboonkunupakarn, B., Jatupornpimol, N., Roest, J., et al. (2023). Culturally responsive research ethics: How the socio-ethical norms of Arr-nar/Kreng-jai inform research participation at the Thai-Myanmar border. PLOS Global Public Health. 3:e0001875. doi: 10.1371/journal.pgph.0001875
Kruger, L. E., and Shannon, M. A. (2000). Getting to know ourselves and our places through participation in civic social assessment. Soc. Nat. Resour. 13, 461–478. doi: 10.1080/089419200403866
LaCroix, J. M., Snyder, L. B., Huedo-Medina, T. B., and Johnson, B. T. (2014). Effectiveness of mass media interventions for HIV prevention, 1986–2013. J. Acquir. Immune Defic. Syndr. 66, S329–S340. doi: 10.1097/QAI.0000000000000230
Langmaid, G., Patrick, R., Kingsley, J., and Lawson, J. (2021). Applying the mandala of health in the Anthropocene. Health Promot. J. Austr. 32, 8–21. doi: 10.1002/hpja.434
Liddell, J. L., and Kington, S. G. (2021). “Something was attacking them and their reproductive organs”: environmental reproductive justice in an indigenous tribe in the United States Gulf Coast. Int. J. Environ. Res. Public Health 18, 1–17. doi: 10.3390/ijerph18020666
Lines, L. A., Division, Y. D. F. N. W., and Jardine, C. G. (2019). Connection to the land as a youth-identified social determinant of indigenous peoples’ health. BMC Public Health 19:176. doi: 10.1186/s12889-018-6383-8
Macfarlane, E. K., Shakya, R., Berry, H. L., and Kohrt, B. A. (2015). Implications of participatory methods to address mental health needs associated with climate change: “photovoice” in Nepal. Bjpsych International 12, 33–35. doi: 10.1192/S2056474000000246
Markle, H., Black, G., Khan, W., Kelley, M., Meritt, M., and Jamrozik, E. (2023). Ethics, equity, climate change, and infectious disease research: a scoping review. Wellcome Open Res. 8:581. doi: 10.12688/wellcomeopenres.19957.1
Martello, M. L. (2008). Arctic indigenous peoples as representations and representatives of climate change. Soc. Stud. Sci. 38, 351–376. doi: 10.1177/0306312707083665
Maughan, D., Berry, H., and Davison, P. (2014). What psychiatrists should know about environmental sustainability and what they should be doing about it. Int. Psychiatry 11, 27–30. doi: 10.1192/s1749367600004306
Meriläinen, E., Kelman, I., Peters, L. E. R., and Shannon, G. (2022). Puppeteering as a metaphor for unpacking power in participatory action research on climate change and health. Clim. Dev. 14, 419–430. doi: 10.1080/17565529.2021.1930509
Minkler, M., Vásquez, V. B., Tajik, M., and Petersen, D. (2008). Promoting environmental justice through community-based participatory research: the role of community and partnership capacity. Health Educ. Behav. 35, 119–137. doi: 10.1177/1090198106287692
Molyneux, S., Sukhtankar, P., Thitiri, J., Njeru, R., Muraya, K., Sanga, G., et al. (2021). Model for developing context-sensitive responses to vulnerability in research: managing ethical dilemmas faced by frontline research staff in Kenya. BMJ Glob. Health 6, 1–14. doi: 10.1136/bmjgh-2021-004937
Ngwenya, N., Ilo Van Nuil, J., Nyirenda, D., Chambers, M., Cheah, P. Y., Seeley, J., et al. (2022). A network of empirical ethics teams embedded in research programmes across multiple sites: opportunities and challenges in contributing to COVID-19 research and responses. Wellcome Open Res. 7:48. doi: 10.12688/wellcomeopenres.17548.1
Nieto, N. C., Porter, W. T., Wachara, J. C., Lowrey, T. J., Martin, L., Motyka, P. J., et al. (2018). Using citizen science to describe the prevalence and distribution of tick bite and exposure to tick-borne diseases in the United States. PLoS One 13:e0199644. doi: 10.1371/journal.pone.0199644
Parham, P. E., Waldock, J., Christophides, G. K., Hemming, D., Agusto, F., Evans, K. J., et al. (2015). Climate, environmental and socio-economic change: weighing up the balance in vector-borne disease transmission. Phil. Trans. Royal Society B 370, 1–17. doi: 10.1098/rstb.2013.0551
Peace, D. M. C., and Myers, E. (2012). Community-based participatory process - climate change and health adaptation program for northern first nations and Inuit in Canada. Int. J. Circumpolar Health 71, 1–8. doi: 10.3402/ijch.v71i0.18412
Petzold, J., Andrews, N., Ford, J. D., Hedemann, C., and Postigo, J. C. (2020). Indigenous knowledge on climate change adaptation: A global evidence map of academic literature. Environ. Res. Lett. 15:1130. doi: 10.1088/1748-9326/abb330
Pope, C., Ziebland, S., and Mays, N. (2000). Qualitative research in health care: Analysing qualitative data. BMJ 320, 114–116. doi: 10.1136/bmj.320.7227.114
Porter, W. T., Barrand, Z. A., Wachara, J., DaVall, K., Mihaljevic, J. R., Pearson, T., et al. (2021). Predicting the current and future distribution of the western black-legged tick, Ixodes pacificus, across the Western US using citizen science collections. PLoS ONE. 16:e0244754. doi: 10.1371/journal.pone.0244754
Pratt, B., Cheah, P. Y., and Marsh, V. (2020). Solidarity and community engagement in Global Health research. Am. J. Bioeth. 20, 43–56. doi: 10.1080/15265161.2020.1745930
Pratt, B., and De Vries, J. (2023). Where is knowledge from the global south? An account of epistemic justice for a global bioethics. J. Med. Ethics 49, 325–334. doi: 10.1136/jme-2022-108291
Romanello, M., Napoli, C.Di, Green, C., Kennard, H., Lampard, P., Scamman, D., et al. (2023). The 2023 report of the lancet countdown on health and climate change: the imperative for a health-centred response in a world facing irreversible harms. Lancet, 402, 2346–2394. doi: 10.1016/S0140-6736(23)01859-7
Sahoo, K. C., Sahay, M. R., Dubey, S., Nayak, S., Negi, S., Mahapatra, P., et al. (2023). Community engagement and involvement in managing the COVID-19 pandemic among urban poor in low-and middle-income countries: a systematic scoping review and stakeholders mapping. Glob. Health Action. 16:2133723. doi: 10.1080/16549716.2022.2133723
Schipper, E. L. F., Dubash, N. K., and Mulugetta, Y. (2021). Climate change research and the search for solutions: rethinking interdisciplinarity. Clim. Chang. 168:18. doi: 10.1007/s10584-021-03237-3
Scobie, M., Gopinathan, U., Kelman, I., and Myhre, S. L. (2023). The agency of community groups in health and climate change adaptation governance and policy in SIDS: the case of in Toco, Trinidad and Tobago. Environ. Sci. Pol. 147, 116–125. doi: 10.1016/j.envsci.2023.05.006
Shaw, J. (2017). Pathways to accountability from the margins: Reflections on participatory video practice. Brighton: Institute of Development Studies. Available at: https://opendocs.ids.ac.uk/opendocs/bitstream/handle/123456789/13149/PartipVideos_Report_Online.pdf (Accessed March 3, 2024).
Shupe, S. M. (2017). High resolution stream water quality assessment in the Vancouver, British Columbia region: a citizen science study. Sci. Total Environ. 603-604, 745–759. doi: 10.1016/j.scitotenv.2017.02.195
Sim, S., Ng, L. C., Lindsay, S. W., and Wilson, A. L. (2020). A greener vision for vector control: The example of the Singapore dengue control programme. PLOS Negl. Trop. Dis. 14:e0008428. doi: 10.1371/journal.pntd.0008428
Sprague Martinez, L., Carolan, K., O’Donnell, A., Diaz, Y., and Freeman, E. R. (2018). Community engagement in patient-centered outcomes research: benefits, barriers, and measurement. J. Clin. Transl. Sci. 2, 371–376. doi: 10.1017/cts.2018.341
Tindana, P. O., DeVries, J., and Kamuya, D. (2020). Ethical challenges in community engagement practices in research during the COVID-19 pandemic in Africa. AAS Open Res. 3:23. doi: 10.12688/aasopenres.13084.1
Treffry-Goatley, A., Moletsane, R., de Oliveira, T., Seeley, J., and Lessells, R. (2021). Using the Emanuel framework to explore the ethical issues raised in a participatory visual research project in rural South Africa. J. Empir. Res. Hum. Res. Ethics 16, 3–14. doi: 10.1177/1556264620987034
UNICEF. (2020). Minimum quality standards and indicators in community engagement. UNICEF. Available at: https://www.unicef.org/mena/reports/community-engagement-standards (Accessed June 7, 2024).
United Nations Framework Convention on Climate Change. (2015). Paris Agreement. Available at: https://unfccc.int/sites/default/files/english_paris_agreement.pdf (Accessed November 1, 2024).
Viswanathan, M., Ammerman, A., Eng, E., Gartlehner, G., Lohr, K. N., Griffith, D., et al. (2004). Community-based participatory research: Assessing the evidence. Evidence Report/Technology Assessment No. 99. Rockville, MD: Agency for Healthcare Research and Quality. Available at: https://www.ncbi.nlm.nih.gov/books/NBK37280/ (Accessed June 7, 2024).
Wang, C., and Burris, M. A. (1997). Photovoice: concept, methodology, and use for participatory needs assessment. Health Educ. Behav. 24, 369–387. doi: 10.1177/109019819702400309
Wheeler, H. C., and Root-Bernstein, M. (2020). Informing decision-making with Indigenous and local knowledge and science. J. Appl. Ecol. 57, 1634–1643. doi: 10.1111/1365-2664.13734
World Health Organization & Special Programme for Research and Training in Tropical Diseases. (2017). WHO vector control response strategy 2017 - 2030. World Health Organization. Available at: https://www.who.int/publications/i/item/9789241512978 (Accessed June 7, 2024).
Wright, C. Y., Moore, C. E., Chersich, M., Hester, R., Schwerdtle, P. N., Mbayo, G. K., et al. (2021). A transdisciplinary approach to address climate change adaptation for human health and well-being in Africa. Int. J. Environ. Res. Public Health 18:4258. doi: 10.3390/ijerph18084258
Keywords: climate-health nexus, community engagement and involvement, indigenous people, equitable partnerships, social justice
Citation: Black GF, Jamrozik E, Khan W, Peralta S, Havenga B, Merritt MW and Kelley M (2024) Making the case for community involvement in research on climate and health: opportunities and lessons. Front. Clim. 6:1456417. doi: 10.3389/fclim.2024.1456417
Edited by:
Louis Nyahunda, University of Venda, South AfricaReviewed by:
Veronica Matthews, The University of Sydney, AustraliaShingirai S. Mugambiwa, University of Limpopo, South Africa
Copyright © 2024 Black, Jamrozik, Khan, Peralta, Havenga, Merritt and Kelley. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Gillian F. Black, Z2lsbC5ibGFja0BsaXZlbGlob29kcy5vcmcuemE=; Z2lsbC5ibGFja0BlbmdhZ2VkcmVzZWFyY2guZW1haWw=