 Lise Milne
Lise Milne Adrienne Ratushniak1,2
Adrienne Ratushniak1,2
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Child Adolesc. Psychiatry , 23 July 2024
Sec. Developmental Psychopathology and Mental Health
Volume 3 - 2024 | https://doi.org/10.3389/frcha.2024.1423451
This article is part of the Research Topic Women In Developmental Psychopathology and Mental Health View all 6 articles
Introduction: The well-being of trauma-affected children and youth in residential care settings is contingent upon the well-being of the workers who care for them, who are increasingly expected to provide care in a trauma-informed manner. The well-being of residential care workers (RCWs) may be impacted by their own histories of adversity, their capacity individually and collectively to navigate to resources that sustain their well-being (resilience), and current perceptions of their professional quality of life.
Objective: This study aimed to fill a research gap by canvassing the perspectives of RCWs to determine what and how they need to be supported in their work. We sought to better understand what personal (adverse childhood experiences, resilience) and professional (compassion satisfaction, burnout, secondary traumatic stress) experiences and capacities they bring into their work that might impact the quality of care they provide to children and youth.
Method: A sample of 226 residential care workers from four residential care organizations across three Canadian provinces completed a self-report questionnaire to provide a portrait of their history of adverse childhood experiences as measured by the ACE questionnaire, which included two additional questions reflecting the more nuanced and expanded understanding of potential adversity in childhood in the Canadian context; their resilience, as measured by the Adult Resilience Measure; and compassion satisfaction, burnout, and secondary traumatic stress, as measured by the Professional Quality of Life Measure. Mediation was conducted to examine whether and how resilience mediated the relationship between ACEs and professional quality of life indicators.
Results: (1) RCWs reported experiencing ACEs at rates much higher than general population and norm samples, especially regarding the experience of 4–5+ ACEs, known to be a threshold for increased severity in negative outcomes; (2) RCWs experienced levels of resilience and indicators of professional quality of life similar to those in other human services professions serving trauma-impacted individuals; and (3) RCW resilience significantly mediated the relationship between ACEs and compassion satisfaction, burnout, and secondary traumatic stress, and had a significant total effect for the relationship between ACEs and secondary traumatic stress. These results suggest the importance of enhancing RCW resilience in multiple ways, mainly in their professional contexts. Recommendations for resilience enhancement and suggestions for future research are provided.
Increasing attention in research and practice are being paid to the effective preparation and support of residential care workers (RCWs), who provide direct care to youth in out-of-home group care settings (1–5). Residential care is challenging work; youth in care frequently have complex histories of adverse childhood experiences (ACEs) (6–11), which can have a myriad of short- and long-term impacts on all spheres of functioning, primarily due to the impact of severe and chronic stress on the developing brain (12–16). Mental health issues are common among youth in residential care, such as depression, anxiety, post-traumatic stress, and dissociation (7, 10, 17). Behaviours that pose a risk to themselves and/or others include aggression, substance use, sexual behaviors (10, 13, 18–20), self-harm (17), and antisocial behaviours (21). Due to these challenging presentations, RCWs often feel anger, blame, a reduced sense of self-efficacy in their work, and may exhibit over-permissiveness or overreactions in their interactions with youth (22–24), in some cases using restraints and seclusion to manage behaviour (2, 25, 26).
These reactions from RCWs can be retraumatizing for youth (22, 23) and are counter to the overarching goal of trauma-informed care (TIC). TIC seeks to prevent re-traumatization and facilitate youth and RCW resilience through education on the prevalence and impacts of trauma, and the incorporation of key principles such as safety, stability, and trusting relationships (2, 27, 28). TIC training models have proliferated in recent years—particularly in child welfare settings (1, 3, 29). An emerging trend in these models is “helping the helpers” (30, 31)—the recognition that the well-being of youth in care is contingent on the well-being of those who provide that care (32).
As part of supporting RCW well-being, it is critical to better understand personal and professional experiences that might impact their ability to understand and apply TIC principles in their interactions with youth (3, 33). For example, relevant personal experiences or characteristics can include ACEs, attachment style, and resilience characteristics. It is probable that many RCWs carry with them their own experiences of childhood adversity, although to our knowledge no studies have examined the link between ACEs and entry into residential care work. However, studies have shown higher rates of ACEs among human service workers than those in general population samples. This includes a multi-site study with a sample of direct and indirect care child welfare professionals (N = 192) (34), and a systematic review of 17 studies with health and social care workers (N = 18,715) (35). In both studies, ACEs were reported at higher rates than those in general population samples from a global meta-analysis of 206 studies across 22 countries (N = 546,458) (36), as well as in the norm sample of the seminal Adverse Childhood Experiences study (N = 17,337) (37). Further, “direct care” child welfare professionals reported higher ACEs than indirect care child welfare professionals (34). To our knowledge, only one ACEs study included a sample of childcare staff in a residential setting (38), although the number of participants in the direct care role was not specified. The authors found higher prevalence of ACEs among their direct care child service provider sample than those in original ACE study samples (12, 39–41). Thus, to better understand potential adversity among RCWs, inquiring about ACEs and other experiences will help inform training and support programs for RCWs to optimally undertake their important and challenging work (34, 35).
Another crucial aspect of RCW capacity to understand and implement TIC can include perceptions of professional quality of life—“the quality one feels in relation to their work as a helper” [(42), p. 8], which might include peer and supervisory support (43–45), and the knowledge and attitudes they have towards TIC within their work (46, 47). Professional quality of life can impact and be impacted by work-related stressors. Literature supports higher prevalence among helping professionals of recurrent work-related stressors (31, 44, 48–55) that can contribute to burnout (gradual onset and lingering of feelings of hopelessness and fatigue that interfere with one's work performance), secondary traumatic stress (work-related secondary trauma exposure), and compassion fatigue (combination of burnout and secondary traumatic stress) (42). One major stressor is the very nature of the work with trauma-impacted children and youth (1, 34, 45, 54, 56–58). Residential care work involves significant emotional expectations. In interactions with children and youth, RCWs are frequently required to inauthentically suppress their emotions while emoting others, simultaneously maintaining strong empathetic connections (4, 56, 59). Working in a residential care facility can be emotionally and physically draining, exacerbated by disclosures of abuse, acts of aggression and violence, and other trauma responses by children or their families (52, 56, 57). It is common for affected workers to become detached or empathetically distant, consciously, or otherwise—defense mechanisms that ultimately negatively impact both themselves and the youth (31, 49, 57, 60). Often accompanying the challenge of working with trauma-impacted youth are unrealistic workloads, and/or insufficient training or administrative support (30, 47, 48, 61, 62). Helping professionals who have also had exposure to traumatic events such as ACEs are at higher risk of developing negative professional quality of life outcomes like burnout and secondary traumatic stress (1, 51, 53, 63). These can be experienced as psychological, physical, and social symptoms of these conditions, such as dysregulated emotions, brain fog, nightmares, headaches, social isolation, and anxiety (48, 52, 64).
Fortunately, resilience is thought to mediate some of the impacts of adversity in childhood (13), as well as the negative impacts of work-related stress (48, 65). A socio-ecological definition of resilience is defined as, “the capacity of individuals to navigate their way to the psychological, social, cultural, and physical resources that sustain their well-being, and their capacity individually and collectively to negotiate for these resources to be provided and experienced in culturally meaningful ways” [(66), p. 10]. Rather than emphasizing individual characteristics, current resiliency literature emphasizes a multisystemic perspective, where the focus is on the human interdependency with the socioeconomic systems in which we live (67, 68). Resilience-promoting organizational factors such as social support, healthy organizational culture, and manageable workloads, have been shown to mediate the impact of stress, as well as improve job satisfaction (45, 69). Similarly, the most protective factors have been shown within organizations that encouraged resilience, worker autonomy, and empowerment (34), with empowerment recommended specifically for direct care providers to manage the stress associated with working directly with traumatized individuals (70). Studies have also found that low resilience and unsupportive, controlling organizations were the most significant predictors for poor professional quality of life (34).
Examining resilience as a mediator may also help to understand some counter-intuitive results regarding the experience of ACEs and professional quality of life and other mental health outcomes. For example, a study involving mental health professionals found that higher ACEs were not significantly correlated with higher burnout, compassion fatigue, anxiety, or depression (71). Even more unexpected, Hiles Howard and colleagues’ (34) study found higher ACEs were in fact correlated with lower rates of burnout and higher rates of compassion satisfaction for child welfare professionals, with no significant correlation with secondary traumatic stress.
Much of the current literature on RCWs is related to TIC, including organizational implementation (2, 46), staff perceptions of TIC (33), and the impact of TIC training on the use of restraints (25). Other RCW research has focused on related areas such as primary or secondary trauma exposure and compassion fatigue (1, 52), training programs related to trauma or neurodevelopment (15), support programs that specifically support RCWs (4), the importance of workplace support, cohesion, stability (45), and the quality of youth-RCW relationships (18).
Considering gaps in research regarding deeper examinations of RCW personal and professional characteristics, the purpose of this study was to canvas RCWs to determine what and how they need to be supported. We sought to learn what experiences and capacities (i.e., ACEs and resilience) RCWs bring into their work that might impact their professional quality of life (i.e., compassion satisfaction, burnout, secondary traumatic stress), and in turn the quality of care—from a trauma-informed perspective—they can provide for trauma-impacted children and youth. We hypothesized that higher ACEs would be correlated with lower levels of resilience, compassion satisfaction, and higher levels of burnout and secondary traumatic stress. We further hypothesized that resilience would mediate the relationship between ACEs and compassion satisfaction, burnout, and secondary traumatic stress, such that higher levels of resilience would lead to improved professional quality of life outcomes.
This exploratory study used a survey methodology to obtain demographic details and information on personal and professional experiences and characteristics of RCW participants. Four Canadian organizations across three provinces (Quebec, Manitoba, Saskatchewan) that provide residential care services to youth participated in study, which included both community-based group homes and more secure residential units for youth ages 12–17 years. Research Ethics Board (REB) approval was granted for the overall project by the researcher's institution, as well as one organization's own REB. Planning took place with participating organization liaisons to distribute the informed consent and survey online (via online platform Qualtrics) or mailed with a stamped, return addressed envelope. To protect the confidentiality of participants, no identifying information was included in the online or hardcopy surveys, and the collection of IP addresses of online survey participants was disabled in Qualtrics. Given the sensitive nature of some of the questions, participants were provided region-specific resources should they require emotional support after completing the survey.
Participants were 226 RCWs. Their roles are described variably across jurisdictions (e.g., Educator, Child Care Worker, Youth Care Practitioner, etc.), but their common role is to provide direct care or support to children and/or adolescents living in residential care settings, usually over 8 or 12-h shifts. Inclusion criteria were that participants be over 18 years of age, and that at the time of recruitment they had worked a minimum of 6 months in a residential care facility.
The survey included five established measures (three of which are described in this paper), which took approximately 30–45 min to complete. Demographic information was collected for the participant's organization and unit; job title and status (full-time, part-time, casual/relief); gender; ethnicity; age; highest level of education and college/university program; years in child and youth work and current position; primary duties; education and training on the impacts of trauma and, more specifically, TIC; and whether the participant felt they had received adequate education and/or training on the impacts of trauma and/or TIC. At the close of the survey, six questions were posed to elicit participants' reactions to completing the survey, using a 5-point Likert scale with response categories ranging from strongly disagree to strongly agree. As shown in Table 1, majority of participants were female and most worked full-time. The average age was 37 years. Just over 80% of participants identified as Caucasian, Indigenous, or African Canadian. The majority had a college diploma or higher, with about half educated either in child and youth care or psychology. The mean years of experience in child and youth care work was just under 11 years. Most had education (83.3%) or on-the-job training (69.0%) on the impacts of trauma, with 61.9% of staff having been educated specifically in TIC (not shown in Table). The vast majority (86.1%) felt they either did not receive adequate training on TIC (30.9%), or had, but wanted more (55.2%). Finally, median scores for participant responses to completing the questionnaire included the following (on a 5-point scale): I found these study questions interesting (4); I found these study questions clear (4), I gained something from filling out this questionnaire (3), completing this questionnaire upset me more than expected (2), I found these study questions distressing (2), had I known in advance what completing this questionnaire would be like for me, I still would have agreed to participate (4) (not shown in Table).
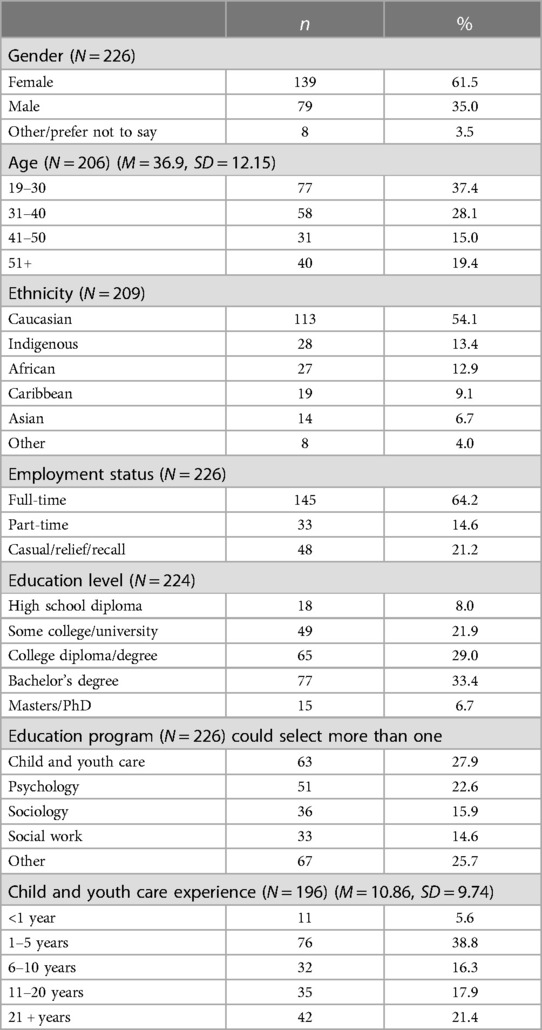
Table 1 Demographic information for residential care worker sample (N = 226).
The Adverse Childhood Experiences (ACE-Q) Questionnaire (12) is one of the most widely used retrospective measures of childhood adversity. The measure presents examples of childhood experiences expected to negatively affect individuals, including physical, emotional, or sexual abuse; physical or emotional neglect; and parental mental illness, substance dependence, incarceration, domestic violence, and/or separation/divorce. To reflect the more nuanced and expanded understanding of potential adversity in childhood (72), particularly within the Canadian context, two questions were added to the original ACEs questionnaire to reflect exposure to colonial or cultural trauma (i.e., personal or familial involvement in the ‘60s scoop1 or residential schools). Thus, results for this study are presented with 12 ACEs as opposed to the original 10 ACEs, although reference is made to the general findings of the ACE-10 for comparison purposes. Response categories include yes, no, or prefer not to say. Higher scores, represented by the frequency of “yes” responses for the 12 questions, indicate a greater number of adverse childhood experiences. The ACE-Q was found to have adequate internal and criterion validity and acceptable internal consistency in a sample of adolescents (α = 0.64) (75). Per standards put forth by some authors (76), in our sample internal consistency for the ACE-Q was considered “acceptable” to “good” for both the 12-item (α = .79) and the 10-item (α = .79) questionnaires.
The Adult Resilience Measure (RRC-ARM-2) (77), is a 28-item measure that assesses resilience from three perspectives: individual (personal skills, peer support, social skills); relational (physical caregiving and psychological caregiving), and contextual (spiritual, educational, and cultural). Participants respond on a 5-point Likert-type scale (not at all to a lot). Mean subscale and total scores are calculated, with higher scores indicating a higher amount of resilience in that area. Psychometric properties are reported as “strong” (78), although some authors have suggested revisions to improving the measure (79), particularly with regards to the concept of “connectedness” (79). Measure authors report a Cronbach's alpha of .88 (77). In our sample, internal consistency for the RRC-ARM-2 was excellent (α = .91).
The Professional Quality of Life Questionnaire (ProQOL-V.5) (42) is the most used measure of the positive and negative effects of helping trauma-impacted individuals (42). The 30-item instrument incorporates the effects of an individual's job/occupation into an overall assessment of how it is affecting the individual over the past 30 days. The measured positive aspect is compassion satisfaction, while the measured negative aspect is compassion fatigue, which is composed of the subscales of burnout and secondary traumatic stress. Participants rate their responses on a 5-point Likert-type scale (never to very often). Subscale scores are totaled, yielding corresponding levels (low, moderate, high). Internal reliability for both burnout and secondary traumatic stress are considered good to very strong (α = .84 −.90). In our sample, internal consistency was good for compassion satisfaction (α = .87) and secondary traumatic stress (α = .83), and acceptable-good for burnout (α = .79).
Data from surveys completed online were transferred from Qualtrics to SPSS (v. 26). Data from paper surveys was entered manually into the SPSS dataset. There was very little missing data (1.3% for the ProQOL, 2.7% for the RRC-ARM-2, 5.8% for the ACE-Q), considered acceptable to conduct the analyses (80). Frequencies, measures of central tendency, and correlations were conducted.
As shown in Figure 1, mediation analysis was conducted to examine whether resilience (RRC-ARM-2) significantly mediated the effects of ACEs (ACE-Q) on the professional quality of life (ProQOL) indicators (burnout, secondary traumatic stress, compassion satisfaction). Mediation is a third-variable effect to explain how two variables (i.e., ACEs and burnout, ACEs and secondary traumatic stress, and ACEs and compassion satisfaction) relate and in what way. Assumptions of mediation were met through tests of linearity and normality. The Sobel Test was used to estimate the statistical significance of indirect effect in the analysis (81).
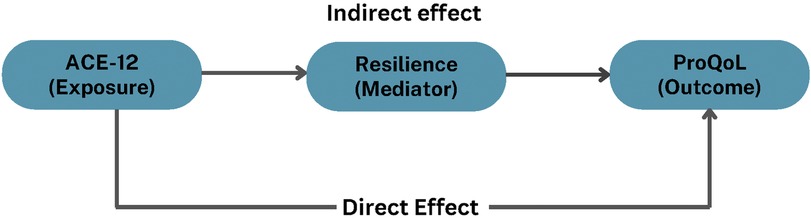
Figure 1 The mediation model.
Table 2 presents descriptive statistics for the measures used in the study.
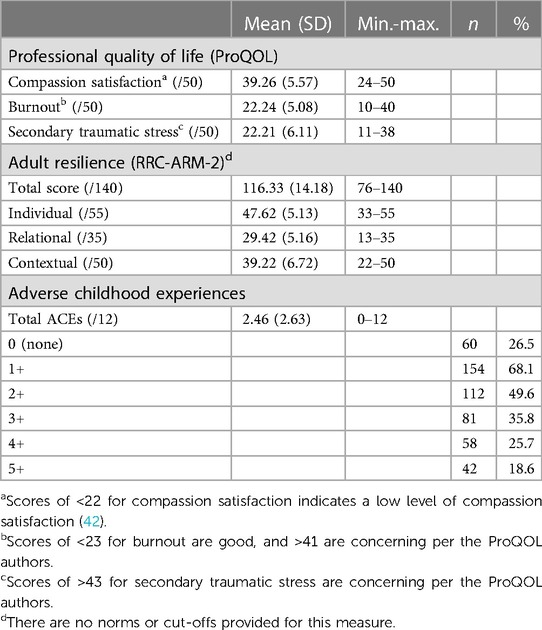
Table 2 Mean and range (minimum-maximum) for professional quality of life, adult resilience, and adverse childhood experiences measure scores.
Mean and range scores fell within moderate ranges per author guidelines (i.e., between 23 and 41) (42): compassion satisfaction (M = 39.26, SD = 5.57), burnout (M = 22.24, SD = 5.08), and secondary traumatic stress (M = 22.21, SD = 6.11).
The mean total resilience score was 116.33 (SD = 14.18) and the three subscale scores were: individual (M = 47.62, SD = 5.13), relational (M = 29.42, SD = 5.16), and contextual (M = 39.22, SD = 6.72).
The mean ACE-Q score for the sample was 2.46 (SD = 2.63), with scores ranging from 0 to 12. Though just over a quarter of the sample reported no ACEs, over a quarter of participants reported 4 or more ACEs, and nearly a fifth reported 5 or more. Participants reported all ACEs included in the measure: separation/divorce (40.2%), parental substance misuse (35.5%), parental mental illness/suicidality (30.2%), emotional abuse (28.8%), emotional neglect (21.4%), physical abuse (20.5%), parental domestic violence (16.4%), sexual abuse (14.4%), familial involvement in residential schools (11.6%), physical neglect (10.7%), parental incarceration (9.8%), and familial involvement in the 60s scoop (6.1%) (not shown in Table).
Though authors of the RRC-ARM-2 and ACE-Q do not provide cut-off scores, or other interpretations of the scores, comparisons of the results with other samples are provided in the Discussion section.
Prior to mediation, correlational analysis using Pearson's correlation was conducted to determine the relationship among the study variables. As shown in Table 3, as hypothesized, higher ACEs were significantly negatively correlated with resilience and positively correlated with secondary traumatic stress, albeit at low (weak) levels. Also as hypothesized, resilience was positively correlated with compassion satisfaction, and negatively correlated with burnout and secondary traumatic stress, all at the p < .001 level, although the coefficients were also low. Though non-significant, the correlation between ACEs and compassion was contrary to our hypothesis, in that higher ACEs were correlated with higher compassion satisfaction. The findings of highly significant but weak correlations suggest that indirect pathways and/or other determinants may be impacting the variable associations.

Table 3 Correlation matrix of adverse childhood experiences (ACE-Q), resilience (RRC-ARM-2), compassion satisfaction, burnout, and secondary traumatic stress (ProQOL).
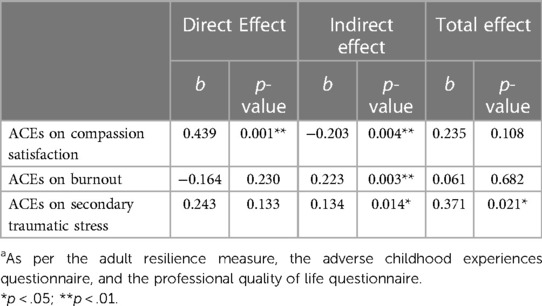
Table 4 The mediating effect of resilience on the relationship between adverse childhood experiences and professional quality of life indicators (compassion satisfaction, burnout, secondary traumatic stress)a.
Mediation analysis revealed that resilience significantly mediated the relationship between ACEs and all three ProQOL subscales (indirect effect on secondary traumatic stress, burnout, compassion satisfaction), but there was a significant total effect only for the model including secondary traumatic stress (see Figure 2).
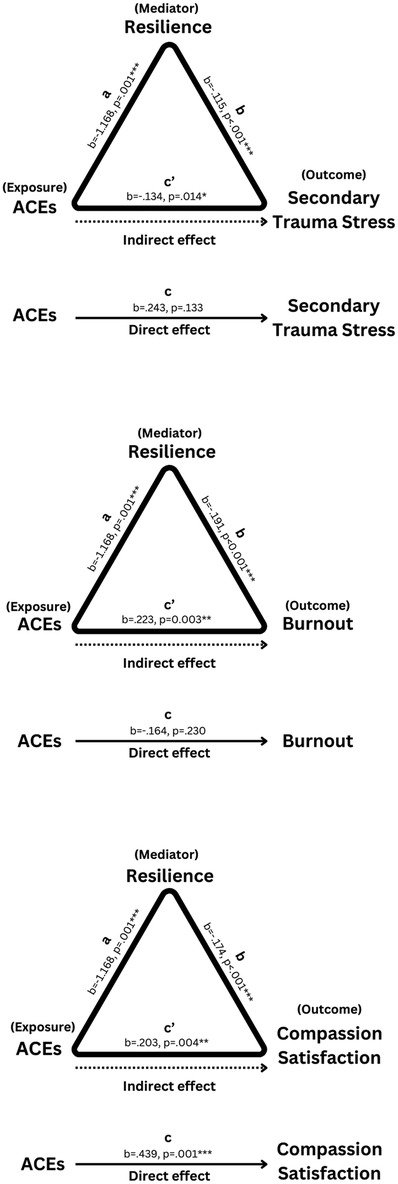
Figure 2 Mediation analysis—secondary traumatic stress, compassion satisfaction, burnout.
ACEs did not have a significant direct effect on secondary traumatic stress (i.e., higher ACEs did not directly lead to higher secondary traumatic stress), but had a significant indirect effect (B = 0.134, p = .014). Resilience significantly mediated the total effects of ACEs on secondary traumatic stress (B = 0.371, SE = .159, p = 0.021, 95% CI = 0.057, 0.685). To further investigate the mediator, the Sobel test was utilized to examine if resilience significantly mediated the relationship between ACEs and secondary traumatic stress. The results confirmed that resilience significantly mediated the relationship (Z = 2.468, SE = 0.054, p = .014). This suggests that the total effect of ACEs on secondary traumatic stress is driven by its negative effect on resilience, which is negatively associated with secondary traumatic stress.
ACEs did not have significant total effects for compassion satisfaction (B = .0235, SE = 0.145, p = .108, 95% CI = −0.052, −0.521). However, when entering resilience as a mediator, ACEs had both a significant direct (B = 0.439, SE = 0.136, p = .001, 95% CI = 0.170, 0.707) and indirect (B = −0.203, SE = 0.07, p = 0.004, 95% CI = −0.34, −0.066) effect on compassion satisfaction, such that higher ACEs resulted in lower compassion satisfaction through its negative effects on resilience, but when controlling for that negative effect, had a positive effect on compassion satisfaction (i.e., these effects balance each other out, resulting in a statistically nonsignificant total effect).
ACEs also did not have significant total effects for burnout (B = .061, SE = 0.148, p = .682, 95% CI = −0.231, −0.352). The direct effect of ACEs on burnout was nonsignificant (B = −.164, SE = 0.136, p = .230, 95% CI = −0.433, 0.105), but the indirect effect was significant (B = 0.223, SE = 0.076, p = 0.003, 95% CI = 0.075, 0.371), suggesting that higher ACEs resulted in higher burnout through their shared negative associations with resilience.
Mediation analysis was also run with the original ACE-10 scores to see whether the addition of the two items would affect the results. Results were very similar, and p-value significance/non-significance was maintained across all results.
As described earlier, internal consistency was established for all three measures used in the mediation analysis. The robustness of this mediation analysis was examined for convergent and discriminant validity using Pearson's correlation coefficient (see Table 3): resilience was positively correlated with compassion satisfaction (r = 0.401, p < .001) and negatively correlated with burnout (r = −0.454, p < .001) and secondary traumatic stress (r = 0.273, p < .001), demonstrating convergent validity. ACEs were not correlated with burnout or compassion satisfaction, and showed a significant but weak correlation with secondary traumatic stress (r = 0.158, p < .05). In addition, the direct effects of ACEs on this outcome were not significant in the mediation analysis. Instead, the relationship between ACEs and all three indicators of the ProQoL was mediated by resilience through indirect effects, supporting discriminant validity by showing that ACEs do not directly or strongly impact these outcomes.
This exploratory study aimed to fill a gap in research regarding our understanding of what personal and professional experiences and characteristics residential care workers (RCWs) bring into their work with trauma-impacted children and youth, in order to determine the conditions and supports necessary to enable them to provide trauma-informed care (TIC). The study examined whether and how RCW resilience mediates the associations between adverse childhood experiences (ACEs) and professional quality of life impacts, including compassion satisfaction, burnout, and secondary traumatic stress.
The study found that most RCWs reported at least one ACE, and over half reported at least two. Our ACE findings can be contextualized by comparing with other studies including similar professionals, as well as general population studies. Our RCW participants reported higher ACEs on the 12-item ACE-Q used in our study (M = 2.46, SD = 2.63) and the original ACE-10 (M = 2.26, SD = 2.42), than a child welfare professional sample (M = 2.18, SD = 2.13) (34). For individuals reporting four or more ACEs—the threshold that experts claim lead to a significant increase in prevalence of health and social negative outcomes (12, 82)—our RCW sample and the child welfare professional sample had similar findings (25.7% vs. 25.1%). These were significantly higher than a meta-analysis general population sample (16.1%) (36) and over double that of the general population sample in the original ACEs study (12.1%) (37). Our findings also support those of other studies (34), that found higher ACEs associated with higher levels of compassion satisfaction, though they may be less counter-intuitive than they first appear. The notion of RCWs as “wounded healers” may apply. Traumatic experiences are often characterized by a lack of control (83); by entering a helping profession related to one's previous trauma, individuals can feel or perceive more control over their circumstances, “an opportunity to face these situations from a position of strength, which may be alluring to populations with ACEs” [(34), p. 446]. Also, RCWs who experienced ACEs may have had positive experiences with support from other helpers, therefore may be more likely to follow careers in helping professions (34). Given that RCWs work mainly with trauma-impacted children and youth, it is critical that wounded healers “are supported to use their own wounds to help others and not become impaired professionals whose emotional problems adversely affect their work” [(84), p. 9].
Though the authors of the RRC-ARM-2 do not include cut-off scores, our findings showed that resilience scores were similar to those found among samples of workers in similar trauma-exposed work (e.g., police), as well as samples of individuals in marginalized conditions (e.g., exposed to natural disasters, residing in crime-ridden or socio-economically poor neighbourhoods) (85).
Findings on professional quality of life indicators (compassion satisfaction, burnout, secondary traumatic stress) were not considered to be “concerning” according to the ProQOL author (42). Compared to studies with child welfare (34) and Canadian protection worker (86) samples, mean compassion satisfaction scores in our study were similar (34) or slightly higher (86), and moderately higher than the ProQOL norm sample (42). Burnout scores were lower than both child welfare and Canadian child protection worker samples, and unexpectedly on par with the ProQOL norm sample. Finally, secondary traumatic stress scores were lower than the child welfare worker sample, higher than the Canadian child protection worker sample, and significantly higher than the ProQOL norm sample. These varying findings are not unique. Indeed, some researchers have suggested that the ProQOL would benefit from revisions. For example, the inclusion of a general factor has been recommended that would reflect the continuum from compassion fatigue to compassion satisfaction, given that these concepts characterize higher and lower levels of the same construct (86). Others have suggested improvement in the coding and specific items to improve the reliability and validity of the burnout and secondary traumatic stress scales (87), confirmed in a meta-analysis of 27 studies on the factor structure of the ProQOL (88). However, the scale has shown convergent validity in its strong correlation with measures of well-being and psychological distress at work (86), and while not a diagnostic tool, can highlight important areas of well-being and concern for workers in challenging contexts.
Finally, our mediation analysis findings showed a significant indirect relationship between ACEs and all three professional quality of life indicators, as mediated by resilience. This suggests that while ACEs may not directly affect outcomes such as burnout and secondary traumatic stress, their influence is exerted through changes in resilience. Further, there was a significant total mediating effect of resilience on the relationship between ACEs and secondary traumatic stress. The absence of significant total effects for compassion satisfaction and burnout suggests that the direct impact of ACEs on professional quality of life might be masked by other contributors, such as resilience. These indirect pathways underscore the importance of finding ways to foster resilience to mitigate ACEs' negative impact on professional well-being. This indicates the need for interventions and conditions to enhance resilience, potentially further increasing compassion satisfaction, and reducing burnout and secondary traumatic stress.
The literature is replete with recommendations to support resilience enhancement of RCWs, many of which begin with how resilience can be negatively impacted by working conditions. To reflect the increasing focus on the organizational context as critical in supporting resilience enhancement for helping professionals, the recommendations here will focus mainly on this area. Frontline staff from different countries and areas of human services work overwhelmingly agree that poor working conditions are the most common contributing factors impacting retention. These conditions include unmanageable workloads, being underpaid, and most importantly, being unsupported (44, 45, 55, 89–95). Though exposure to traumatic stress has commonly been considered the most significant factor for burnout (34), chronic organizational stressors (e.g., toxic workplace cultures, poor training quality, controlling leadership, and lack of administrative support) have been identified in recent literature as the most impactful contributing factors to rates of burnout (30, 47, 51, 61, 62, 91, 96–98). Staff retention and high turnover rates are also critical contributing factors to burnout, either as reflections of burnout, or as a result of working in an environment where turnover is problematic, leading to increased work pressures that can lead to burnout. As Brend and Sprang state, “Paradoxically, this relational proximity to the children in their care also puts RCWs at risk of harmful impacts associated with secondary exposure to adverse experiences—feeding the cycle of workforce instability” [(1), p. 3]. And though burnout and turnover directly affect RCWs, high rates of turnover are a significant barrier to the successful provision of TIC for children and youth, because structure, routine, and predictability are such essential components of TIC (89). Additionally, turnover can result in challenges for children and youth to form trusting and quality relationships with RCWs, as they require safe and stable relationships due to oft-disrupted attachments (22, 99).
Creating a trauma-informed workplace culture by fostering a team environment is critical for child- and youth-serving organizations. This involves hiring people who are a good “fit” (47), and having team meetings that include many levels of workers (e.g., frontline workers, supervisors, and upper management). Open and consistent communication between frontline workers and upper management facilitates team-building, and is important for staff morale, reducing turnover, and bolstering peer support systems (4, 65, 100, 101). Creating an inclusive work culture/environment is also crucial for the safety of all workers (50), but particularly for marginalized individuals (32, 64, 94, 101). Encouraging staff empowerment by allowing more control and autonomy around their own work is an additional protective factor that promotes resiliency through reduced stress and increased compassion satisfaction (34, 53, 62, 92, 101, 102). Having leaders and management who provide consistent, supportive supervision is a major protective factor against burnout and other work-related traumatic stress for frontline workers, including RCWs (44, 65). Supportive supervision has been described as an “act of care” because it makes workers feel safer and more valued, particularly in comparison to supervision that is superficial, tokenistic, or more preoccupied with risk and surveillance (43). Reflection and mindfulness have also been identified as protective factors for worker resiliency, particularly when conducted with supervision (2, 28, 59, 101, 103, 104). Debriefing and supervised reflection is critical for facilitating safe environments for workers to process their emotions and decisions in both formal and informal contexts (102, 104, 105). Organizations should also include training for supervisors and upper management to recognize the signs of burnout and traumatic stress in their staff and learn effective ways to help them manage their stress (94).
TIC approaches to child welfare are fundamentally about relationality (22, 45, 47, 102). They aim to reduce and repair the impacts of ACEs and childhood trauma through relational security and the development of self- and interpersonal capacities. Thus, other workplace social supports, including strong informal peer support networks, have been identified as an effective method for reducing many occupational risks in child welfare (30, 44, 45, 92, 106).
A clear result from the study was that the vast majority of staff wish to have more training in TIC, even if they feel their training was “adequate”. Training can include how the brain is impacted by trauma, and its relationship to child and youth externalizing behaviors and symptoms, as well as associated therapeutic interventions (15), such as the National Child Traumatic Stress Network (NCTSN) Trauma Training Toolkit; the Attachment, Self-Regulation Competency Manual (22); and activities suggested within the Neurosequential Model of Therapeutics for children and youth based on enriching, therapeutic, and essential needs (107). Research has shown that such training can improve individual attitudes related to TIC (29, 33, 47, 108, 109). However, a key element of TIC is that it be situated within and across the entirety of organizations, thus RCW training alone may have little value. To address this concern, Building Resilience Through Residential Communities, a SAMHSA-funded NCTSN Treatment Services and Adaptation Center, has developed a model aimed at organizations nationwide: Building Communities of Care (BCC). Geared to the unique needs of residential treatment centers (RTCs), the model is considered trauma- and evidence-informed and strengths-based. BCC components include training for all staff; increasing access to evidence-based practices in TIC, through intensive training and technical assistance; and building “a trauma-informed workforce…through education, training and technical assistance via both intensive RTC partnerships and national dissemination activities” (p. 1) (110).
Despite such a promising model, a recent systematic review of studies on organization-wide, trauma-informed care models in out-of-home care found only seven describing three models, namely Attachment, Self-Regulation Competency (ARC), Children and Residential Experiences (CaRE), and Sanctuary. Though the models were seen as promising, and were shown to have significantly positive effects on children and youth in out-of-home care, they are not yet considered by the authors to be evidence-based (109). Therefore, though TIC models continue to proliferate within child well-being sectors, it is critical that research on their components (109) and perceived efficacy by RCWs, be evaluated.
Finally, though many TIC models include aspects supporting resilience enhancement of workers, we could find few interventions or programs specifically aimed at enhancing RCW resilience. A large-scale randomized control trial is currently underway in the U.S. to compare interventions for RCWs at a group home-level (Integrated Resiliency Training and Task-sharing; IRTT) and organization-level (virtual Workplace Improvement Learning; WILC) (111). However, the interventions are targeted to RCWs in congregate care settings for adults with behavioral health disabilities. Wounded Warriors Canada has developed a Trauma-Resilience Training (TRT) program, but it is specifically geared to trauma-exposed professionals such as military and public safety personnel (112).
While providing valuable insights into the relationships between ACEs, resilience, and professional quality of life indicators among participants, the design and mediation analysis for this study have inevitable limitations. Though the sample included data from four organizations in three provinces to provide a tri-provincial perspective, variations in provincial and organizational contexts impacts the generalizability of the findings. Further, the cross-sectional design limits the ability to infer causality among the variables (113). The findings suggest associations, but cannot establish a temporal sequence necessary to confirm a causal relationship, except in confirming the occurrence of ACEs prior to adult resilience and professional quality of life. This concern is particularly significant in mediation models, where it is crucial to establish that the mediator (resilience) temporally precedes the outcome (professional quality of life indicators). As an analysis technique, the mediation model's assumption of linear relationships between variables may not adequately represent the complex, dynamic interactions of real-world data (114). For example, unobserved confounders (e.g., an unmeasured stressor) might influence both the mediator and the outcome (115). Also, the reliance on self-reported measures may introduce recall bias and/or social desirability effects (116). Future research should utilize interventional, longitudinal (prospective and/or retrospective) designs to establish causality more effectively and assess the efficacy of specific resilience-building approaches. The inclusion of qualitative data on the personal and professional contexts of participants would enrich our understanding of the quality of life of RCWs. Similarly, information on the mental and physical health of RCWs could provide a more holistic view of the impact of ACEs and resilience on professional quality of life. Finally, expanding the sample to include a more diverse demographic profile would improve the generalizability of the findings.
TIC in residential care is fundamentally contingent on the well-being of RCWs. Therefore, organizations must prioritize the creation of the structural conditions necessary for RCWs to thrive (4, 30, 45, 58). This study—the first of its kind to look specifically at how for RCWs resilience mediates the impact of ACEs on compassion satisfaction, burnout, and secondary traumatic stress—demonstrates the complex interplay between personal history and professional quality of life, suggesting that supporting resilience enhancement of RCWs is crucial for improving their capacity to support vulnerable residents effectively.
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
The studies involving humans were approved by University of Regina Research Ethics Board. The studies were conducted in accordance with the local legislation and institutional requirements. The participants provided their written informed consent to participate in this study.
LM: Conceptualization, Data curation, Formal Analysis, Funding acquisition, Investigation, Methodology, Project administration, Resources, Supervision, Validation, Visualization, Writing – original draft, Writing – review & editing. AR: Writing – original draft, Writing – review & editing. HN: Formal Analysis, Visualization, Writing – original draft.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article. This study was supported by the University of Regina and the RBC-McGill Centre for Research on Children and Families. Additional support to prepare the manuscript was provided by the University of Regina Child Trauma Research Centre. The funders were not involved in the study design, collection, analysis, interpretation of data, the writing of this article, or the decision to submit it for publication.
The authors would like to express their gratitude to all the residential care worker participants in the study, and the organizations and liaisons who supported the facilitation of this important work.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
1. ^Coined by Patrick Johnston (73), the phrase “60 s scoop” (spanning the years 1960 and the mid-1980s), “describes a period in Aboriginal history in Canada in which thousands of Aboriginal children were removed from birth families and placed in non-Aboriginal environments.” [(74), p. 65].
1. Brend DM, Sprang G. Trauma-informed care in child welfare: an imperative for residential childcare workers. Int J Child Adolesc Resil. (2020) 7(1):154–65. doi: 10.7202/1072595ar
2. Bryson SA, Gauvin E, Jamieson A, Rathgeber M, Faulkner-Gibson L, Bell S, et al. What are effective strategies for implementing trauma-informed care in youth inpatient psychiatric and residential treatment settings? A realist systematic review. Int J Ment Health Syst. (2017) 11(1):36. doi: 10.1186/s13033-017-0137-3
3. Collin-Vézina D, Brend DM, Black KR, Beeman I, Brown S. Impacts of child welfare and clientele characteristics on attitudes towards trauma informed care. Dev Child Welf. (2020) 2(3):244–61. doi: 10.1177/2516103220963139
4. Santos L, Miguel RR, Pinheiro MR, Rijo D. Fostering emotional and mental health in residential youth care facilities: a systematic review of programs targeted to care workers. Child Youth Serv Rev. (2023) 147:106839. doi: 10.1016/j.childyouth.2023.106839
5. Verhage V, Jansen DEMC, Wunderink C, Alma MA, Reijneveld SA, Grietens H. How the bachelor of social work (BSW) prepares one for working in a residential youth care setting: a thematic analysis of youth worker experiences in The Netherlands. Resid Treat Child Youth. (2023) 40(4):407–26. doi: 10.1080/0886571X.2023.2243211
6. Briggs EC, Greeson JKP, Layne CM, Fairbank JA, Knoverek AM, Pynoos RS. Trauma exposure, psychosocial functioning, and treatment needs of youth in residential care: preliminary findings from the NCTSN core data set. J Child Adolesc Trauma. (2012) 5(1):1–15. doi: 10.1080/19361521.2012.646413
7. Collin-Vézina D, Coleman K, Milne L, Sell J, Daigneault I. Trauma experiences, maltreatment-related impairments, and resilience among child welfare youth in residential care. Int J Ment Health Addict. (2011) 9(5):577–89. doi: 10.1007/s11469-011-9323-8
8. Hagaman JL, Trout AL, Chmelka MB, Thompson RW, Reid R. Risk profiles of children entering residential care: a cluster analysis. J Child Fam Stud. (2010) 19(4):525–35. doi: 10.1007/s10826-009-9325-3
9. Leloux-Opmeer H, Kuiper CH, Swaab HT, Scholte EM. Children referred to foster care, family-style group care, and residential care: (how) do they differ? Child Youth Serv Rev. (2017) 77:1–9. doi: 10.1016/j.childyouth.2017.03.018
10. Milne L, Collin-Vézina D, Wekerle C. Diverse trauma profiles of youth in group care settings: a cluster analysis. Child Abuse Negl. (2021) 120:105221. doi: 10.1016/j.chiabu.2021.105221
11. Zelechoski AD, Sharma R, Beserra K, Miguel JL, DeMarco M, Spinazzola J. Traumatized youth in residential treatment settings: prevalence, clinical presentation, treatment, and policy implications. J Fam Violence. (2013) 28(7):639–52. doi: 10.1007/s10896-013-9534-9
12. Felitti VJ, Anda RF, Nordenberg D, Williamson DF, Spitz AM, Edwards V, et al. Relationship of childhood abuse and household dysfunction to many of the leading causes of death in adults—the adverse childhood experiences (ACE) study. Am J Prev Med. (1998) 14(4):245–58. doi: 10.1016/s0749-3797(98)00017-8
13. Goldenson J, Kitollari I, Lehman F. The relationship between ACEs, trauma-related psychopathology and resilience in vulnerable youth: implications for screening and treatment. J Child Adolesc Trauma. (2021) 14:151–60. doi: 10.1007/s40653-020-00308-y
14. Hambrick EP, Brawner TW, Perry BD. Timing of early-life stress and the development of brain-related capacities. Front Behav Neurosci. (2019) 13:183. doi: 10.3389/fnbeh.2019.00183
15. Hendry L, Taylor E, Mackinlay L. Neuro trauma training: feasibility and acceptability of online training in executive function for residential childcare workers. Child Youth Serv. (2022) 43(2):104–33. doi: 10.1080/0145935X.2022.2078697
16. Strine TW, Dube SR, Edwards VJ, Prehn AW, Rasmussen S, Wagenfeld M, et al. Associations between adverse childhood experiences, psychological distress, and adult alcohol problems. Am J Health Behav. (2012) 36(3):408–23. doi: 10.5993/AJHB.36.3.11
17. Aderibigbe OO, Stewart SL, Hirdes SL, Hirdes JP, Perlman C. Substance use among youth in community and residential mental health care facilities in Ontario, Canada. Int J Environ Res Public Health. (2022) 19:1731. doi: 10.3390/ijerph19031731
18. Silva CS, Calheiros MM, Carvalho H, Magalhães E. Organizational social context and psychopathology of youth in residential care: the intervening role of youth–caregiver relationship quality. Appl Psychol. (2022) 71(2):564–86. doi: 10.1111/apps.12339
19. Gutterswijk RV, Kuiper CHZ, van der Horst FCP, Jongerling J, Harder AT, Prinzie P. Behavioural problems of adolescents in secure residential care: gender differences and risk factors. Child Fam Soc Work. (2023) 28:454–68. doi: 10.1111/cfs.12976
20. Steen JT, Senreich E, Straussner SLA. Adverse childhood experiences among licensed social workers. Fam Soc J Contemp Soc Serv. (2021) 102(2):182–93. doi: 10.1177/1044389420929618
21. Maneiro L, Gómez-Fraguela JA, López-Romero L, Cutrín O, Sobral J. Risk profiles for antisocial behaviour in adolescents placed in residential care. Child Youth Serv Rev. (2019) 103:278–86. doi: 10.1016/j.childyouth.2019.06.012
22. Blaustein ME, Kinniburgh KM. Treating Traumatic Stress in Children and Adolescents: How to Foster Resilience Through Attachment, Self-Regulation, and Competency. New York, NY: Guilford Publications (2018).
23. Briere JN, Lanktree CB. Treating Complex Trauma in Adolescents and Young Adults. Los Angeles, CA: Sage Publications (2011).
24. National Child Traumatic Stress Network. Creating Trauma-Informed Systems. UCLA and Duke University (2019). Available online at: https://www.nctsn.org/trauma-informed-care/creating-trauma-informed-systems.
25. Matte-Landry A, Collin-Vézina D. Patterns of change in restraints, seclusions and time-outs over the implementation of trauma-informed staff training programs in residential care for children and youth. Resid Treat Child Youth. (2022) 39(2):154–78. doi: 10.1080/0886571X.2021.1929660
26. Roy C, Castonguay A, Fortin M, Drolet C, Franche-Choquette G, Dumais A, et al. The use of restraint and seclusion in residential treatment care for youth: a systematic review of related factors and interventions. Trauma Violence Abuse. (2021) 22(2):318–38. doi: 10.1177/1524838019843196
27. Center for Behavioral Health Statistics and Quality. 2014 National Survey on Drug Use and Health: Methodological Summary and Definitions. Rockville, MD: Substance Abuse and Mental Health Services Administration (2015).
28. Diebold J, Sperlich M, Heagle E, Marris W, Green S. Trauma Talks: exploring personal narratives of trauma-informed care through podcasting. J Technol Hum Serv. (2021) 39(1):1–23. doi: 10.1080/15228835.2020.1820425
29. Lowenthal A. Trauma-informed care implementation in the child- and youth-serving sectors: a scoping review. Int J Child Adolesc Resil. (2020) 7(1):178–94. doi: 10.7202/1072597ar
30. Barnhill J, Fisher JW, Kimel-Scott K, Weil A. Trauma-informed care: helping the healthcare team thrive. In: Gerber MR. editors. Trauma-Informed Healthcare Approaches. Cham: Springer International Publishing. (2019) pp. 197–213. doi: 10.1007/978-3-030-04342-1_11
31. Cummings C, Singer J, Hisaka R, Benuto LT. Compassion satisfaction to combat work-related burnout, vicarious trauma, and secondary traumatic stress. J Interpers Violence. (2021) 36(9–10):NP5304–19. doi: 10.1177/0886260518799502
32. Lizano E, He AS. Inclusive work environments as a pathway to an engaged child welfare workforce that intends to stay. Child Youth Serv Rev. (2023) 155:107302. doi: 10.1016/j.childyouth.2023.107302
33. Galvin E, O’Donnell R, Mousa A, Halfpenny N, Skouteris H. Attitudes towards trauma-informed care in residential out-of-home care. Child Youth Serv Rev. (2020) 117:105346. doi: 10.1016/j.childyouth.2020.105346
34. Hiles Howard ARH, Parris S, Hall JS, Call CD, Razuri EB. An examination of the relationships between professional quality of life, adverse childhood experiences, resilience, and work environment in a sample of human service providers. Child Youth Serv Rev. (2015) 57:141–8. doi: 10.1016/j.childyouth.2015.08.003
35. Mercer L, Cookson A, Simpson-Adkins G, van Vuuren J. Prevalence of adverse childhood experiences and associations with personal and professional factors in health and social care workers: a systematic review. Psychol Trauma Theory Res Pract Policy. (2023) 15(Suppl 2):S231–45. doi: 10.1037/tra0001506
36. Madigan S, Deneault A, Racine N, Park J, Thiemann R, Zhu J, et al. Adverse childhood experiences: a meta-analysis of prevalence and moderators among half a million adults in 206 studies. World Psychiatry. (2023) 22:463–71. doi: 10.1002/wps.21122
37. Anda RF, Dong M, Brown DW, Felitti VJ, Giles WH, Perry GS, et al. The relationship of adverse childhood experiences to a history of premature death of family members. BMC Public Health. (2009) 9(1):106. doi: 10.1186/1471-2458-9-106
38. Esaki N, Larkin H. Prevalence of adverse childhood experiences (ACEs) among child service providers. Fam Soc J Contemp Soc Serv. (2013) 94(1):31–7. doi: 10.1606/1044-3894.4257
39. Dong M, Anda RF, Felitti VJ, Dube SR, Williamson DF, Thompson TJ, et al. The interrelatedness of multiple forms of childhood abuse, neglect, and household dysfunction. Child Abuse Negl. (2004) 28(7):771–84. doi: 10.1016/j.chiabu.2004.01.008
40. Dube SR, Anda RF, Felitti VJ, Chapman DP, Williamson DF, Giles WH. Childhood abuse, household dysfunction, and the risk of attempted suicide throughout the life span: findings from the adverse childhood experiences study. JAMA. (2001) 286(24):3089–96. doi: 10.1001/jama.286.24.3089
41. Felitti VJ, Anda RF. The relationship of adverse childhood experiences to adult medical disease, psychiatric disorders, and sexual behaviour: implications for healthcare. Impact Early Life Trauma Health Dis Hidden Epidemic. (2010) 77:87. doi: 10.1017/CBO9780511777042.010
42. Stamm BH. The professional quality of life scale: compassion satisfaction, burnout & compassion fatigue/secondary trauma scales. (2009). ID: ProQOL.org
43. Newcomb M. Supportive social work supervision as an act of care: a conceptual model. Br J Soc Work. (2022) 52:1070–88. doi: 10.1093/bjsw/bcab074
44. Sutton L, Rowe S, Hammerton G, Billings J. The contribution of organizational factors to vicarious trauma in mental health professionals: a systematic review and narrative synthesis. Eur J Psychotraumatol. (2022) 13:2022278. doi: 10.1080/20008198.2021.2022278
45. Brend DM, Collin-Vézina D. Stronger together: workplace social support among residential child welfare professionals. Child Abuse Negl. (2022) 130(3):105302. doi: 10.1016/j.chiabu.2021.105302
46. Baker CN, Brown SM, Wilcox PD, Overstreet S, Arora P. Development and psychometric evaluation of the attitudes related to trauma-informed care (ARTIC) scale. School Ment Health. (2016) 8:61–76. doi: 10.1007/s12310-015-9161-0
47. Bosk EA, Williams-Butler A, Ruisard D, MacKenzie MJ. Frontline staff characteristics and capacity for trauma-informed care: implications for the child welfare workforce. Child Abuse Negl. (2020) 110(3):104536. doi: 10.1016/j.chiabu.2020.104536
48. Beer OWJ, Phillips R, Quinn CR. Exploring stress, coping, and health outcomes among social workers. Eur J Soc Work. (2021) 24(2):317–30. doi: 10.1080/13691457.2020.1751591
49. Bercier ML, Maynard BR. Interventions for secondary traumatic stress with mental health workers: a systematic review. Res Soc Work Pract. (2015) 25(1):81–9. doi: 10.1177/1049731513517142
50. Deaver AH, Cudney P, Gillespie C, Morton S, Strolin-Goltzman J. Culture of safety: using policy to address traumatic stress among the child welfare workforce. Fam Soc J Contemp Soc Serv. (2020) 101(4):428–43. doi: 10.1177/1044389420912127
51. Fansher AK, Zedaker SB, Brady PQ. Burnout among forensic interviewers, how they cope, and what agencies can do to help. Child Maltreat. (2020) 25(1):117–28. doi: 10.1177/1077559519843596
52. Ireland CA, Keeley S, Lewis M, Bowden S. Vicarious trauma and compassion fatigue in residential care workers of traumatized children. Abuse Int Impact J. (2023) 3(1). ISSN: 2633-8742.
53. Jirek SL. Ineffective organizational responses to workers’ secondary traumatic stress: a case study of the effects of an unhealthy organizational culture. Hum Serv Organ Manag Leadersh Gov. (2020) 44(3):210–28. doi: 10.1080/23303131.2020.1722302
54. Nilsen KH, Lauritzen C, Vis SA, Iversen A. Factors affecting child welfare and protection workers’ intention to quit: a cross-sectional study from Norway. Hum Resour Health. (2023) 21(43). doi: 10.1186/s12960-023-00829-1
55. Trujillo KC, Bruce L, de Guzman A, Wilcox C, Melnyk A, Clark K. Preparing the child welfare workforce: organizational commitment, identity, and desire to stay. Child Abuse Negl. (2020) 110(Pt 3):105439. doi: 10.1016/j.chiabu.2020.104539
56. Hunt S, Goddard C, Cooper J, Littlechild B, Wild J. “If I feel like this, how does the child feel?” child protection workers, supervision, management and organisational responses to parental violence. J Soc Work Pract. (2016) 30(1):5–24. doi: 10.1080/02650533.2015.1073145
57. Lamothe J, Geoffrion S, Guay S. Investigating the cyclical hypothesis of client aggression as a “loss spiral”: can child protection worker distress lead to more client aggression? Health Soc Care Community. (2022) 30(1):275–83. doi: 10.1111/hsc.13401
58. Sage CAM, Brooks SK, Greenberg N. Factors associated with type II trauma in occupational groups working with traumatised children: a systematic review. J Mental Health. (2018) 27(5):457–67. doi: 10.1080/09638237.2017.1370630
59. Perry MA, Creavey K, Arthur E, Humer JC, Lundgren PJ, Rivera I. Cultivating emotional intelligence in child welfare professionals: a systematic scoping review. Child Abuse Negl. (2020) 110(Pt 3):104438. doi: 10.1016/j.chiabu.2020.104438
60. Hayes MW. The challenge of burnout: an ethical perspective. Ann Psychother Integr Health. (2013) 16:20–5. Semantic Scholar ID: 151445017.
61. Ashley-Binge S, Cousins C. Individual and organizational practices addressing social workers’ experiences with vicarious trauma. Practice. (2019) 32(3):191–207. doi: 10.1080/09503153.2019.1620201
62. Dombo EA, Blome WW. Vicarious trauma in child welfare workers: a study of organizational responses. J Public Child Welf. (2016) 10(5):505–23. doi: 10.1080/15548732.2016.1206506
63. Brown M. Hazards of our helping profession: a practical self-care model for community practice. Soc Work. (2020) 65(1):38–44. doi: 10.1093/sw/swz047
64. Oats F. You are not allowed to tell: organizational culture as a barrier for child protection workers seeking assistance for traumatic stress symptomology. Child Aust. (2019) 44:84–90. doi: 10.1017/cha.2019.12
65. Mack BM. Addressing social workers’ stress, burnout, and resiliency: a qualitative study with supervisors. Soc Work Res. (2022) 46(1):17–28. doi: 10.1093/swr/svab032
66. Ungar M. The social ecology of resilience: addressing contextual and cultural ambiguity of a nascent construct. Am J Orthopsychiatry. (2011) 81(1):1–17. doi: 10.1111/j.1939-0025.2010.01067.x
67. Twum-Antwi A, Jefferies P, Ungar M. Promoting child and youth resilience by strengthening home and school environments: a literature review. Int J Sch Educ Psychol. (2020) 8(2):78–89. doi: 10.1080/21683603.2019.1660284
68. Khanlou N, Wray R. A whole community: approach toward child and youth resilience promotion: a review of resilience literature. Int J Mental Health Addict. (2014) 12:64–79. doi: 10.1007/s11469-013-9470-1
69. McFadden P, Campbell A, Taylor B. Resilience and burnout in child protection social work: individual and organisational themes from a systematic literature review. Br J Soc Work. (2015) 45(5):1546–63. doi: 10.1093/bjsw/bct210
70. Lee E, Esaki N, Kim JH, Greene R, Mitchell-Herzfeld S, Kirkland K. Organizational climate and burnout among home visitors: a test of mediating effects of empowerment. Child Youth Serv Rev. (2013) 35:594–602. doi: 10.1016/j.childyouth.2013.01.011
71. Marcus S, Dubi M. The relationship between resilience and compassion fatigue in counselors. Vistas Online. (2006) 50:223–5. Semantic Scholar ID: 13115380.
72. Cronholm PF, Forke CM, Wade R, Bair-Merritt MH, Davis M, Harkins-Schwarz M, et al. Adverse childhood experiences: expanding the concept of adversity. Am J Prev Med. (2015) 49(3):354–61. doi: 10.1016/j.amepre.2015.02.001
73. Johnston P. Aboriginal Children and the Child Welfare System. Toronto: Canadian Council on Social Development (1983).
74. Sinclair R. Identity lost and found: lessons from the sixties scoop. First Peoples Child Fam Rev. (2007) 3(1):65–82. doi: 10.7202/1069527ar
75. Kovács-Tóth B, Oláh B, Kuritárné Szabó I, Fekete Z. Psychometric properties of the adverse childhood experiences questionnaire 10 item version (ACE-10) among Hungarian adolescents. Front Psychol. (2023) 14:1161620. doi: 10.3389/fpsyg.2023.1161620
76. George D, Mallery P. SPSS for Windows Step by Step: A Simple Guide and Reference. 11.0 Update. 4th ed. Boston: Allyn & Bacon (2003).
77. Liebenberg L, Moore JC. A social ecological measure of resilience for adults: the RRC-ARM. Soc Indic Res. (2018) 136(1):1–19. doi: 10.1007/s11205-016-1523-y
78. Resilience Research Centre. CYRM and ARM User Manual v2.5. Halifax, NS: Resilience Research Centre, Dalhousie University (2022). Available online at: http://www.resilienceresearch.org/.
79. Clark JN, Jefferies P. Measuring resilience and the importance of resource connectivities: revising the adult resilience measure (RRC-ARM). Soc Sci. (2023) 12(5):290. doi: 10.3390/socsci12050290
80. Bennett DA. How can I deal with missing data in my study? Aust N Z J Public Health. (2001) 25(5):464–9. doi: 10.1111/j.1467-842X.2001.tb00294.x
81. Fairchild AJ, McDaniel HL. Best (but oft-forgotten) practices: mediation analysis. Am J Clin Nutr. (2017) 105(6):1259–71. doi: 10.3945/ajcn.117.152546
82. Finkelhor D, Ormrod RK, Turner HA. Polyvictimization and trauma in a national longitudinal cohort. Dev Psychopathol. (2007) 19(1):149–66. doi: 10.1017/S0954579407070083
83. Beck JG, Jacobs-Lentz J, Jones JM, Olsen SA, Clapp JD. Understanding posttrauma cognitions and beliefs. In: Zoellner LA, Feeny NC, editors. Facilitating Resilience and Recovery Following Trauma. New York, NY: The Guilford Press (2014). p. 167–90.
84. Straussner SLA, Senreich E. Productive aging in the social work profession: a comparison of licensed workers 60 years and older with their younger counterparts. Clin Soc Work J. (2020) 48:196–210. doi: 10.1007/s10615-020-00747-y
85. Resilience Research Centre. CYRM/ARM: Properties. (n.d.). Available online at: https://cyrm.resilienceresearch.org/properties/.
86. Geoffrion S, Lamothe J, Morizot J, Giguère CÉ. Construct validity of the professional quality of life (ProQoL) scale in a sample of child protection workers. J Trauma Stress. (2019) 32(4):566–76. doi: 10.1002/jts.22410
87. Hemsworth D, Baregheh A, Aoun S, Kazanjian A. A critical enquiry into the psychometric properties of the professional quality of life scale (ProQOL-5) instrument. Appl Nurs Res. (2018) 39:81–8. doi: 10.1016/j.apnr.2017.09.006
88. Hotchkiss JT, Wong MYC. Factorial structure of the ProQOL—systematic meta-analysis and integration of 27 international factor analysis studies. Trends Psychol. (2022):1–32. doi: 10.1007/s43076-022-00184-5. [Epub ahead of print].
89. Steinkopf H, Nordanger D, Stige B, Milde AM. How do staff in residential care transform trauma-informed principles into practice? A qualitative study from a Norwegian child welfare context. Nordic Soc Work Res. (2020) 12(5):625–39. doi: 10.1080/2156857X.2020.1857821
90. Apgar D, Parada M. Missing the mark? Reframing NASW’s ethical mandate for self-care as a social justice issue. Adv Soc Work. (2022) 22(3):876–99. doi: 10.18060/25748
91. Burns DD, Langenderfer-Magruder L, Yelick A, Wilke DJ. What else is there to say? Reflections of newly-hired child welfare workers on retention status. Child Youth Serv Rev. (2023) 144:106731. doi: 10.1016/j.childyouth.2022.106731
92. Courcy F, Morin AJS, Madore I. The effects of exposure to psychological violence in the workplace on commitment and turnover intentions: the moderating role of social support and role stressors. J Interpers Violence. (2019) 34(19):4162–90. doi: 10.1177/0886260516674201
93. Hendrix E, Barusch A, Gringeri C. Eats me alive!: social workers reflect on practice in neoliberal contexts. Soc Work Educ. (2020) 40(2):161–73. doi: 10.1080/02615479.2020.1718635
94. Kim J, Pierce B, Park TK. Secondary traumatic stress and public child welfare workers’ intention to remain employed in child welfare: the interaction effect of job functions. Hum Serv Organ Manag Leadersh Gov. (2023) 48(2):136–49. doi: 10.1080/23303131.2023.2263518
95. Lushin V, Katz CC, Julien-Chinn FJ, Lalayants M. A burdened workforce: exploring burnout, job satisfaction and turnover among child welfare caseworkers in the era of COVID-19. Child Youth Serv Rev. (2023) 148. doi: 10.1016/j.childyouth.2023.106910
96. Beer OWJ, Phillips R, Letson MM, Wolf KG. Personal and professional impacts of work-related stress alleviation strategies among child welfare workers in child advocacy center settings. Child Youth Serv Rev. (2021) 122(2):105904. doi: 10.1016/j.childyouth.2020.105904
97. Newell JM, MacNeil GA. Professional burnout, vicarious trauma, secondary traumatic stress, and compassion fatigue: a review of theoretical terms, risk factors, and preventive methods for clinicians and researchers. Best Pract Mental Health Int J. (2010) 6(2):57–68.
98. Radey M, Wilke DJ. Client-perpetrated violence among frontline child welfare workers. J Interpers Violence. (2021) 36(11–12):NP6260–80. doi: 10.1177/0886260518812792
99. Wilson-Ching M, Berger E. Relationship building strategies within trauma informed frameworks in education al settings: a systematic literature review. Curr Psychol. (2023) 43(4):1–22. doi: 10.1007/s12144-023-04590-5
100. Katz CC, Julien-Chinn FJ, Wall E. Perceptions of agency leadership and intent to stay: an examination of turnover in the child welfare workforce. J Public Child Welf. (2022) 16(3):302–20. doi: 10.1080/15548732.2021.1876808
101. Ponic P, Varcoe C, Smutylo T. Trauma- (and violence-) informed approaches to supporting victims of violence: policy and practice considerations. Victims Crime Res Digest. (2016) 9:3–15.
102. Russ E, Lonne B, Lynch D. Increasing child protection workforce retention through promoting a relational-reflective framework for resilience. Child Abuse Negl. (2020) 110(Pt 3):104245. doi: 10.1016/j.chiabu.2019.104245
103. Kalergis KI. Lessons from the field: an evidence-informed resiliency model for child abuse organizations. Child Abuse Negl. (2020) 110(Pt 3):104266. doi: 10.1016/j.chiabu.2019.104266
104. Curry A, Epley P. “It makes you a healthier professional”: the impact of reflective practice on emerging clinicians’ self-care. J Soc Work Educ. (2022) 58(2):291–307. doi: 10.1080/10437797.2020.1817825
105. McCusker P. Critical mindfulness in social work: exploring the potential of reflexive self-care in the journey from student to social worker. Br J Soc Work. (2022) 52(1):334–53. doi: 10.1093/bjsw/bcaa246
106. Zhou Q, Jones AS. Improving retention in child welfare: comparing needed support for supervisors and caseworkers. Hum Serv Organ Manag Leadersh Gov. (2023) 48(2):181–95. doi: 10.1080/23303131.2023.2271045
107. Teicher MH, Munkbaatar O, Schore AN, Gatwiri K, Perry BD, Kickett G, et al. The Handbook of Therapeutic Care for Children: Evidence-Informed Approaches to Working with Traumatized Children and Adolescents in Foster, Kinship and Adoptive Care. London: Jessica Kingsley Publishers (2019).
108. Niimura J, Nakanishi M, Okumura Y, Kawano M, Nishida A. Effectiveness of 1-day trauma-informed care training programme on attitudes in psychiatric hospitals: a pre-post study. Int J Ment Health Nurs. (2019) 28(4):980–8. doi: 10.1111/inm.12603
109. Bailey C, Klas A, Cox R, Bergmeier H, Avery J, Skouteris H. Systematic review of organisation-wide, trauma-informed care models in out-of-home care (Oo HC) settings. Health Soc Care Community. (2019) 27(3):e10–22. doi: 10.1111/hsc.12621
110. Justice Resource Institute. Building Resilience Through Residential Communities. Communities: National Child Traumatic Stress Network Category II Treatment and Services Adaptation Center (2022). Available online at: https://jri.org/research-and-publications/research/building-resilience-through-residential-communities.
111. Patient-Centered Outcomes Research Institute. Effectiveness of Interventions to Improve Resiliency and Burnout in Behavioral Health Residential Staff. Washington, DC. (2024). Available online at: https://www.pcori.org/research-results/2022/effectiveness-interventions-improve-resiliency-and-burnout-behavioral-health-residential-staff (accessed April 12, 2024).
112. Wounded Warriors. Trauma Resilience Training. (2019). Available online at: https://woundedwarriors.ca/.
113. Maxwell SE, Cole DA. Bias in cross-sectional analyses of longitudinal mediation. Psychol Methods. (2007) 12(1):23. doi: 10.1037/1082-989X.12.1.23
114. Hofmann SG, Curtiss JE, Hayes SC. Beyond linear mediation: toward a dynamic network approach to study treatment processes. Clin Psychol Rev. (2020) 76:101824. doi: 10.1016/j.cpr.2020.101824
115. Lin Q, Nuttall AK, Qian Z, Frank KA. How do unobserved confounding mediators and measurement error impact estimated mediation effects and corresponding statistical inferences? Introducing the R package ConMed for sensitivity analysis. Psychol Methods. (2023) 28(2):339–58. doi: 10.1037/met0000567
Keywords: adverse childhood experiences, residential care workers, children and youth, resilience, trauma-informed care, compassion satisfaction, burnout, professional quality of life
Citation: Milne L, Ratushniak A and Nguyen H (2024) How adverse childhood experiences impact the professional quality of life of residential care workers: resilience as a mediator for burnout, secondary traumatic stress, and compassion satisfaction. Front. Child Adolesc. Psychiatry 3: 1423451. doi: 10.3389/frcha.2024.1423451
Received: 15 May 2024; Accepted: 24 June 2024;
Published: 23 July 2024.
Edited by:
Eva Möhler, Saarland University Hospital, GermanyReviewed by:
Erin Rappuhn, Eastern University, United States© 2024 Milne, Ratushniak and Nguyen. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Lise Milne, bGlzZS5taWxuZUB1cmVnaW5hLmNh
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.