 Sara Alatrash
Sara Alatrash Tithi Paul2
Tithi Paul2 Melanie Penner
Melanie Penner Atena Roshan Fekr
Atena Roshan Fekr Azadeh Kushki
Azadeh Kushki
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
SYSTEMATIC REVIEW article
Front. Child Adolesc. Psychiatry , 23 July 2024
Sec. Autism and Other Neurodevelopmental Disorders
Volume 3 - 2024 | https://doi.org/10.3389/frcha.2024.1393231
This article is part of the Research Topic World Autism Awareness Day 2024 View all 7 articles
Introduction: Autism is characterized by social communication differences and repetitive behaviors, affecting 1%–2% of children. Irritability is a disabling condition affecting 19%–80% of autistic children. While extensive research has focused on interventions to reduce irritability symptoms, the underlying correlates remain poorly understood. To address this, we conducted a scoping review of the literature examining factors contributing to irritability in pediatric autistic populations.
Methods: A literature search of Embase, MEDLINE, PubMed, PsycINFO, and Web of Science was conducted in addition to manually retrieved papers from Google Scholar. Studies underwent title and abstract screening by one reviewer and full-text screening by two reviewers; disagreements were resolved through deliberation. The remaining studies underwent data extraction. The review was conducted using the PRISMA-ScR checklist.
Results: The search yielded 48 studies meeting the inclusion criteria. Correlates of irritability were categorized into eight themes: demographics/environmental, autism features, mental health, language, cognition, and function, neurobiological, physical health, physiological, and multidimensional factors. Findings revealed mixed associations with demographic factors, consistent positive associations with sensory differences and mental health symptoms, and varying associations with cognitive abilities and physical health factors. Neurobiological and physiological correlates were less explored.
Conclusion: This review revealed a significant gap in understanding sociodemographic, phenotypic, and neurobiological and physiological correlates of irritability in autism. There was also a significant gap in understanding the multi-dimensional irritability correlates. Positive associations between irritability and sensory differences and mental health symptoms suggest potential avenues for investigation of non-medication interventions.
Autism (autism spectrum disorder) is defined based on differences in social communication and the presence of intense interests and repetitive behaviors (1)1 and impacts 1%–2% of children (2, 3). Autism is more prevalent in males than females (4). Autism often co-occurs with other medical and psychiatric symptoms, such as mental health disorders, sleep difficulties, and gastrointestinal issues, which can contribute to increased experiences of distress and disability (5). Among these, irritability is prevalent and highly disabling and can often lead to a significant decline in quality of life (6).
Irritability is defined as “a feeling state characterized by reduced control over temper which usually results in irascible verbal or behavioral outbursts” (7). This umbrella term often encompasses various moods and behaviors including aggression, intense behavioral responses, and self-injury (8, 9), and is a major reason for referral of children and adolescents for psychiatric assessment and treatment (10, 11). Irritability can be highly disabling and associated with negative short- and long-term outcomes, including anxiety and depression (12), increased risk of suicidal thoughts or actions (11), academic difficulties, and economic hardship (11). Irritability can hinder a child's development, strain relationships, and decrease social and educational functioning (6).
The reported prevalence of irritability in autism is variable but estimates across studies range from 19%–80% (13–15), depending on the sample and measurement tools used. Irritability levels in females were higher than in males suggesting irritability to be more prevalent in autistic females (16). Much of the existing research on irritability has focused on pharmacological and behavioral interventions for reducing irritability symptoms (17). While irritability is the only symptom domain in autism for which medications are approved, these medications can have significant adverse effects (18). An improved understanding of the factors that contribute to irritability can ultimately help inform treatment targets for alternative medications or non-medication interventions. However, very few studies have investigated the correlates of irritability and the association with the core features of autism, co-occurring conditions, or biological mechanisms that may underlie these symptoms (19). These studies have produced mixed findings, and the correlates of irritability symptoms in autism remain poorly understood. To address this gap, we conducted a scoping review of the literature to enhance our understanding of the current state of research on irritability in pediatric autistic populations. Our specific research question for this review was: What is the scope and focus of the literature on factors associated with irritability in children diagnosed with autism?
Five online databases were searched targeting correlates and predictors of irritability in autism. The databases were Embase, MEDLINE, PubMed, PsycINFO, Web of Science in addition to manually retrieving papers from Google Scholar. Subject heading and key words were tailored to search for the population of interest (autism) and concept (irritability) using the Boolean operator “AND”. These terms were entered and truncated or broadened to ensure widespread coverage. For example, “irrita*” captures terms such as “irritability”, “irritable”, and “irritate”; while “autis*” captures terms such as “autism” and “autistic”. No date constraints were applied to the search in any of the databases. The search was completed in September 2023. The review was conducted using the PRISMA-ScR (Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews) checklist.
Inclusion criteria for the review were: (1) the study examined correlates/predictors of irritability, (2) study sample included individuals with an autism diagnosis, (3) study sample includes pediatric population (children from birth to 18 years of age), and (4) manuscript was written in English. Studies focusing on interventions and treatments, literature reviews, theses, conference abstracts, and books were excluded.
All articles were imported to Covidence for screening, review, risk of bias assessment, and extraction by the authors (screening and extraction: SA; full-text review: SA, TP). For full-text review, each study was assessed by two reviewers, and disagreements were resolved through deliberation. Inter-rater reliability was determined on a subset of 15 articles, achieving a Cohen's kappa of approximately 0.73, which indicates substantial agreement beyond chance between the two raters (20).
Data were extracted using custom extraction templates on Covidence. The extracted data included the following: title, author, year, country, aim, and sample characteristics [total sample size, sex (biological), gender (identity), age, social/economic status, and race/ethnicity]. Other data extracted included predictors/correlates of irritability, analysis methods, measures, informants, and key findings. During the data extraction, one reviewer extracted the data, and a second reviewer cross-checked the results. An adapted version of the Cochrane template was used for the risk of bias assessment (see Supplementary Table S1).
The literature search process is presented in Figure 1. Of the 6,020 articles identified by the search, 3,616 (60%) were identified as duplicates. The first screening of titles and abstracts eliminated 2,304 articles based on the inclusion criteria, leaving 100 articles for the full-text review. Following the full-text review, 51 articles were eliminated according to the exclusion criteria. The full text of one article was not retrieved. The final review included 48 studies summarized in Table 1 (see Supplementary Table S2 for more details on these studies).
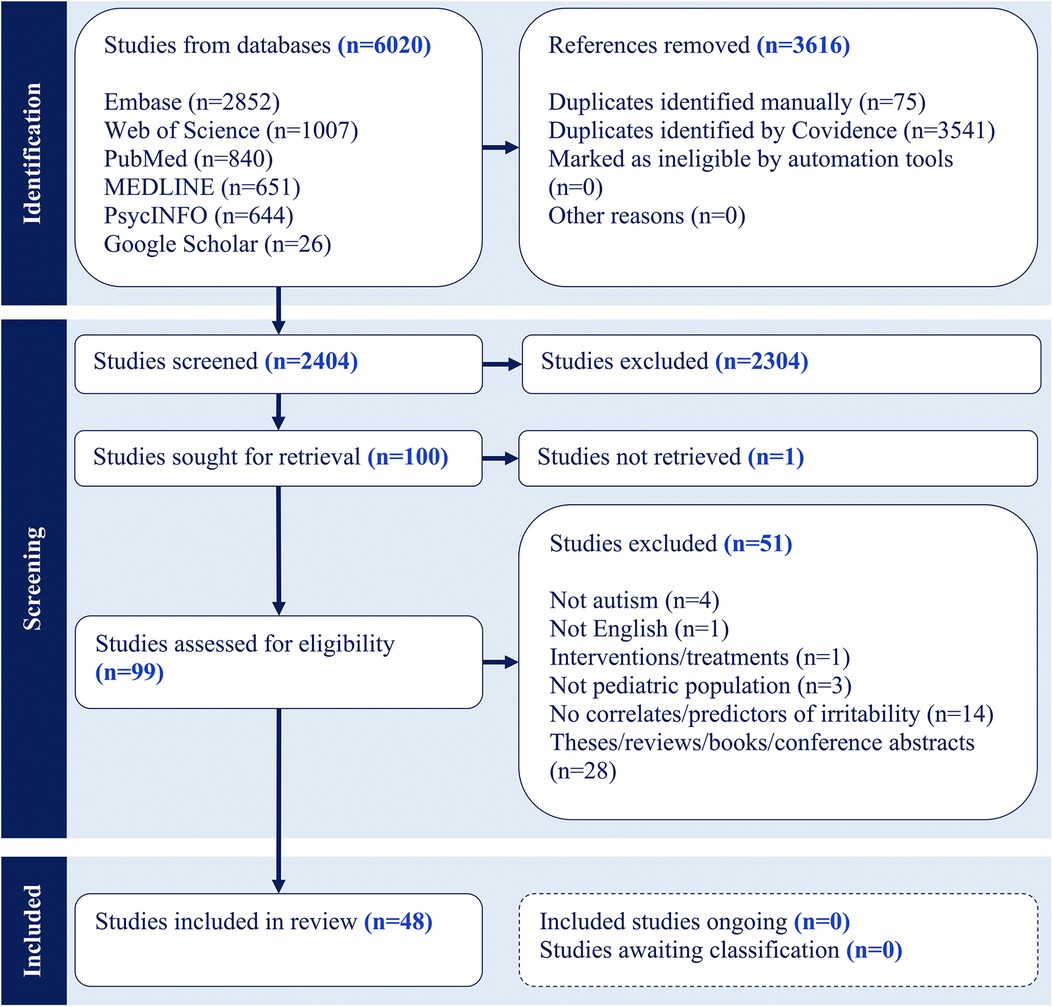
Figure 1 Scoping review PRISMA.
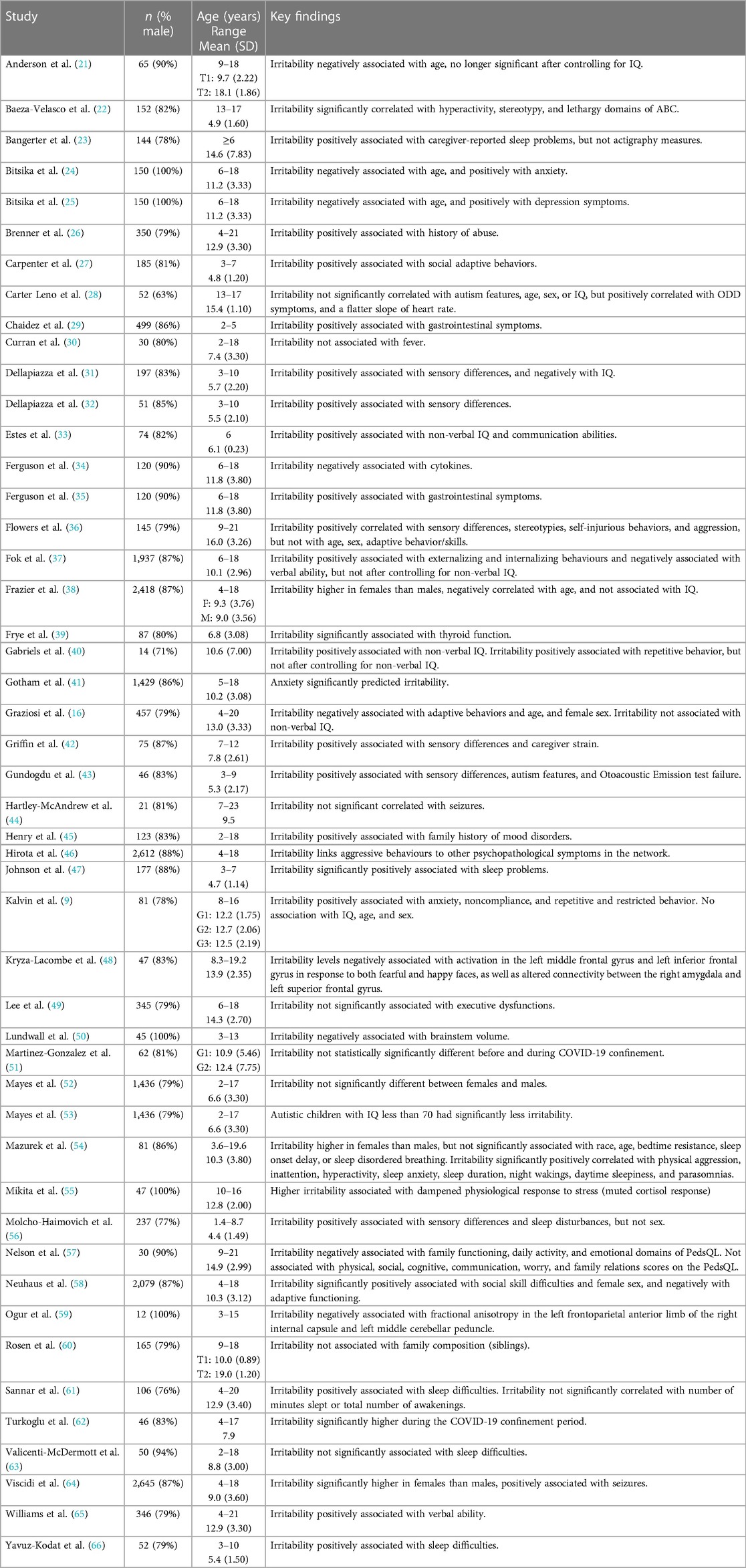
Table 1 Summary of characteristics of the reviewed studies.
There was a predominance of male participants in all the studies (85%). Most studies were completed in the United States of America (n = 33), followed by France (n = 4), Australia (n = 3), and Turkey (n = 3). None of the 48 studies reported gender identity, 27 reported race/ethnicity, and 18 reported on social/economic status. The irritability subscale of the Aberrant Behavior Checklist ABC-I was the most common measure of irritability (n = 39), followed by the Affective Reactivity Index ARI (n = 5). Figure 2 shows the number of reviewed studies across years.
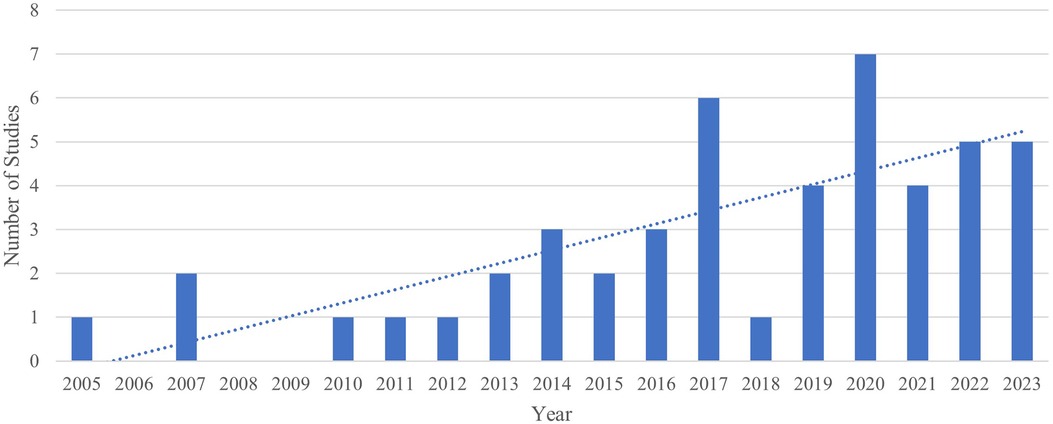
Figure 2 Number of studies across different years.
Among the studies reviewed, most (n = 36) were found to have a low risk of bias. Only eleven studies had a medium risk of bias, and one study had a high risk of bias. The most common sources of bias were related to sample selection and description, the description of statistical methods, and the reporting of statistical results.
The results are presented using a narrative approach. We grouped the predictors examined in the reviewed literature into 8 themes defined as follows (Table 2):
1. Demographics and environmental factors defined as variables that describe personal characteristics and external influences, including family history.
2. Autism features defined as variables that quantify core autism features, including social communication differences, intense interests, repetitive behaviors, and sensory differences.
3. Mental health factors defined as variables related to mental and emotional well-being, including internalizing and externalizing behaviors.
4. Language, Cognition, and Function factors defined as predictors that describe language and cognitive abilities include expressive and receptive language, Intelligence Quotient (IQ), and functioning.
5. Neurobiological factors defined as predictors that characterize brain structure, function, connectivity, and neurochemistry.
6. Physical health factors defined as predictors related to general well-being, and medical conditions impacting physical health.
7. Physiological factors defined as predictors that quantify the function of body organs and other physiological processes such as heart rate, heart rate variability, and skin conductance.
8. Multidimensional factors refer to the category of studies that considered multi-dimensional interactions among variables from the above categories.
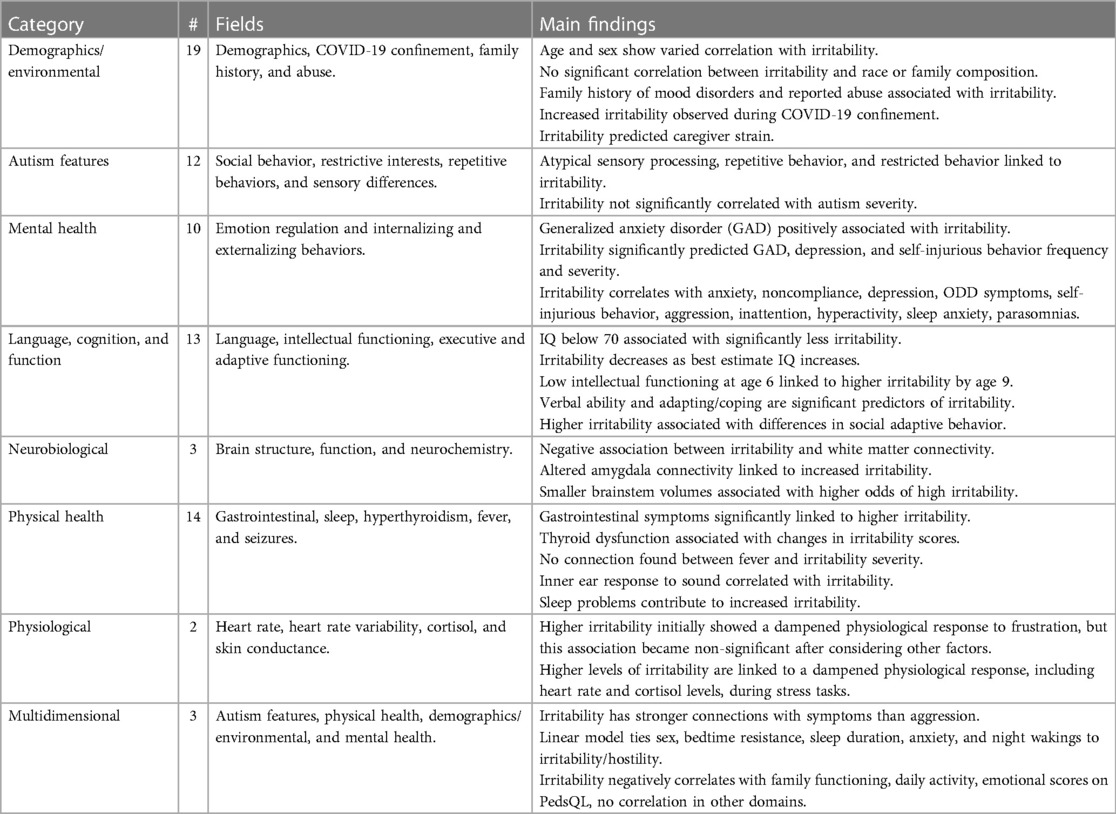
Table 2 Synthesis of review results.
Figure 3 shows the number of reviewed studies under each domain.
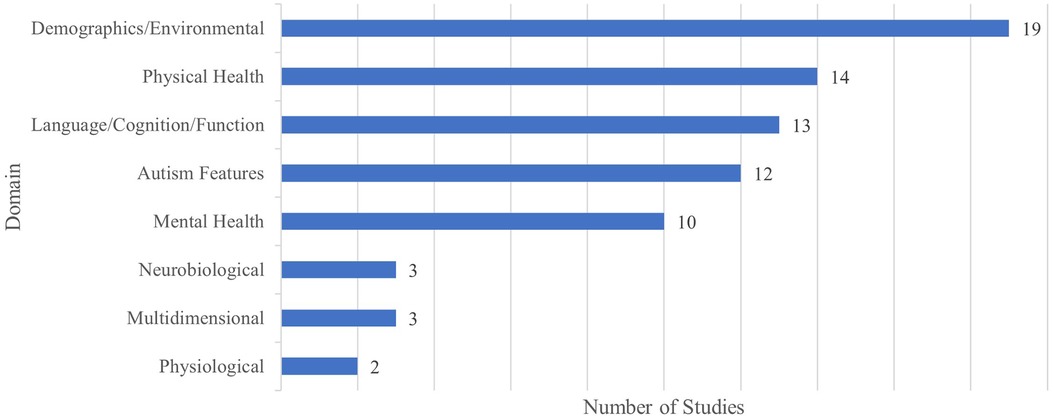
Figure 3 Number of studies under each domain.
Nineteen studies examined demographic and environmental factors as predictors of irritability, including age, sex, race, family composition, and family history of mental health challenges.
The most studied demographic factors were sex and age; however, the findings related to the association between these variables and irritability were mixed. Of the ten studies examining the association between sex and irritability, five studies found higher levels of irritability in females compared to males (16, 38, 54, 58, 64), while five found no significant sex differences in irritability levels (9, 28, 36, 52, 56). Eight studies examined the effect of age on irritability, with four studies reporting a significant negative association between age and irritability (16, 21, 24, 25), and four reporting no significant associations between the two variables (9, 28, 36, 54).
Only one study examined the effect of race on irritability (54), reporting no statistically significant association between the two variables. Family composition was also not found to be significantly associated with irritability (54, 60). Family history of mood disorders and caregiver strain were associated with increased irritability symptoms in one study (42, 45).
Other studies reported higher levels of irritability in those with a history of abuse (26), as well as during COVID-19 confinement period (51, 62).
Twelve studies investigated autism features as predictors of irritability. Among these, six studies examined the associations between irritability and differences in sensory processing, consistently suggesting a significant positive association between the two (31, 32, 36, 42, 43, 56). Two studies examined the association between irritability and the overall intensity of autism features (28, 58, 62); one did not find a statistically significant association between the variables (28), while the other reported a positive association (58). Functioning in the social domain was negatively associated with irritability in two studies (27, 58). Positive associations were also reported between irritability and repetitive behaviors in two studies (9, 40), although the association was no longer significant after correcting for non-verbal IQ (40).
Ten studies examined mental health symptoms as predictors of irritability. Overall, the results were consistent with a positive association between irritability and mental health challenges including anxiety (9, 24, 41, 55), depression (25), self-injury (36), oppositional defiant disorder (ODD) symptoms (28), hyperactivity, stereotypy, and lethargy (22), symptoms of attention deficit hyperactivity disorder (ADHD) (54), and internalizing and externalizing symptoms (37).
Thirteen studies investigated the association between irritability and language and cognitive abilities. Of these, seven focused on cognitive ability, reporting mixed results. In particular, one study found autistic children with IQ below 70 showed significantly less irritability (53), three studies found no association between IQ and irritability (9, 16, 28), and three found a negative association between irritability and IQ (31, 33, 40).
The results for the association of irritability and language were also mixed. Of the three papers reporting on this, one study found a positive association between irritability and verbal ability (65), and two studies found no significant association between the two domains after adjusting for non-verbal IQ (21, 37).
Three studies examined the association between adaptive functioning and irritability. No significant association was found in one study (36), while a negative association was reported in two other studies (16, 58).
Only one study examined the association between irritability and executive dysfunctions, reporting no significant association between the two domains (49).
Three studies investigated neurobiological correlates of irritability in autism (48, 50, 59). One study found a negative association between irritability and fractional anisotropy in the left frontoparietal anterior limb of the right internal capsule and left middle cerebellar peduncle (59). One study found that increased irritability levels in youths are associated with decreased activation in the left middle frontal gyrus and left inferior frontal gyrus in response to both fearful and happy faces, as well as altered connectivity between the right amygdala and left superior frontal gyrus during the perception of fearful and sad faces (48). Brainstem volumes were found to be negatively associated with irritability (50).
Fourteen studies explored physical health factors as correlates of irritability including sleep (23, 47, 54, 56, 61, 63, 66), gastrointestinal distress (29, 34, 35), hyperthyroidism (39), fever (30), and seizures (44, 64).
Seven studies reported on the association between irritability and sleep difficulties, consistently reporting positive associations between the two domains (23, 47, 54, 56, 61, 63, 66). Irritability and gastrointestinal problems were also found to be positively associated across three reviewed studies (29, 34, 35). Only two studies examined the association between seizures and irritability, reporting positive (64) or no associations (44).
Other physical health variables examined in the reviewed literature included thyroid function (significantly associated with irritability) (39) and fever (no association with irritability) (30).
Of the reviewed literature, two studies found that higher levels of irritability were associated with a dampened physiological response to frustration (28) and stress (55), including a decreased heart rate change (28) and a muted cortisol response (55); However, the association between heat rate change lost significance when controlling for IQ, autism features, and medication use as covariates (28).
Three studies investigated multi-dimensional predictors of irritability (46, 54, 57). In one study, irritability was predicted by the combined factors of sex and sleep difficulties (bedtime resistance, sleep duration, sleep anxiety, and night wakings) (54). In another study (57), irritability was negatively associated with the total score and subdomain scores on the family functioning, daily activity, and emotional domains of the Pediatric Quality of Life Inventory (PedsQL), while no associations were observed with physical, social, cognitive, communication, worry, and family relations scores on the PedsQL (57).
One study found that irritability may be a bridge linking aggressive behaviours and other symptoms (46). The study treated irritability and aggression as one construct, but irritability's stronger connections to other behaviors suggest they might be distinct concepts.
We conducted this scoping review to examine the existing literature on the correlates of irritability in autism. Our review identified 48 published studies that investigated the correlates in eight categories of demographic/environmental factors, autism features, mental health, language and cognitive abilities, neurobiological features, physical health, and multidimensional analysis. Overall, the review identified significant gaps in understanding irritability correlates in autism. This gap was particularly evident in understanding the association of irritability with demographic variables, core and co-occurring features of autism, and neurobiological and physiological factors.
In terms of demographic correlates of irritability, the reviewed literature was focused on age and sex, reporting highly mixed results. This likely reflects the heterogeneity in study samples, differences in the definition of irritability and analytical approaches, and the complexity of the association of irritability with sex and age. For example, sex and gender are suggested to influence, as mediators or moderators, the phenotypic expression of core and co-occurring features and their developmental trajectories in autism (67), which can in turn be associated with irritability levels. At the same time, developmental trajectories of autism are highly heterogeneous and can be impacted by both biological and environmental factors (67). This suggests that the investigation of sex and age differences cannot happen in silo and should consider the interactions of these factors with phenotypic and environmental variables.
Our review revealed significant gaps in the reporting and investigation of gender identity as well as other demographic factors such as race, socioeconomic status, and other dimensions of identity. This is a critical avenue for future research as these variables contribute to disparities in access to resources and services that can significantly impact the experiences and expressions of distress (68, 69).
In terms of autism features, the most consistent findings suggested a positive association between sensory differences and irritability. This is not surprising given the significant negative impact of adverse sensory experiences in autistic individuals (70, 71). This highlights the importance of considering sensory needs and environmental accommodations in management of irritability symptoms in autism. At the time, future research is needed to examine the association of irritability with individual differences in sensory experiences and whether specific sensory profiles may enhance the likelihood or intensity of irritability symptoms. Our review revealed very few studies examining the association of irritability with other core features of autism (social communication, repetitive behaviors/intense interests).
There is a consistent positive association between irritability and various mental health challenges, including anxiety, depression, self-injury, symptoms of ODD, and symptoms of ADHD, which highlights the complexity of emotional well-being and behavioral outcomes in the autistic population. These findings suggest that autistic individuals who experience heightened levels of anxiety or depressive symptoms, as well as those with symptoms of ADHD, may be at increased likelihood for exhibiting irritability. Moreover, the correlation between irritability and hyperactivity, stereotypy, lethargy, and externalizing symptoms further emphasizes the diverse pathways through which emotional dysregulation manifests. These results must be interpreted cautiously in the context of the significant construct overlap between irritability and mental health symptoms (e.g., externalizing behaviours). Future studies are also needed to examine the directionality of this association to inform potential intervention targets.
Surprisingly, the results of studies examining the association of cognitive and language abilities with irritability were highly mixed, suggesting positive, null, and negative associations. This may be a result of differences in the ranges of IQ considered, thresholds used for IQ dichotomization, or variability in the analytic approaches, including covariates used. Nevertheless, the lack of consistent findings in this area is particularly concerning given that antipsychotic medications, approved for treatment of irritability in autism, are prescribed at higher rates in individuals with intellectual disability (ID) compared to those without, and were the most commonly used medication class in this group (72). This highlights the significant need for future studies clarifying the construct and assessment of irritability in those with lower scores and IQ tests, as well as the interaction of cognitive ability with other factors that may impact the perceived levels of irritability (e.g., communication ability, access to other interventions).
In the domain of physical health, sleep difficulties and gastrointestinal distress were consistently associated with increased irritability. Again, future work is needed to elucidate the directionality of these associations. Other than sleep, very few physical health domains were examined.
Our review also found very few studies examining the neurobiological and physiological correlates of irritability in autism. Further investigation of these factors is critically needed to enhance our understanding of the mechanistic process underlying irritability, potentially informing new intervention targets. A promising avenue in this direction is improved characterization of arousal modulation and its association with irritability (both non-medication and medication approaches exist for arousal modification). While there are significant gaps in understanding the association of irritability and arousal modulation, there is a large body of evidence suggesting atypical arousal processes in autism, including physiological hyperarousal and dampened reactivity to stressful tasks (73–75).
Finally, one of the most critical limitations of the existing literature is that correlates of irritability are almost always considered in silos. However, many of the predictors reviewed above can be highly correlated (for example, sex and symptom domains, mental health and core symptoms, IQ, and mental health). Studying these predictors in silos makes it very challenging to identify and isolate factors that may drive irritability. Multi-dimensional investigations of irritability are critically needed to address this gap.
Future research should further investigate the predictors and physiological associations of irritability in autistic individuals, particularly the multi-dimensional associations between irritability and demographics, autism features, sensory processing, emotion regulation, and internalizing and externalizing problems. Understanding these associations can inform targeted intervention strategies and highlight priority areas for support. Additionally, examining the link between physiological arousal and irritability can provide insights into underlying mechanisms, again informing targeted interventions. Understanding the predictors of irritability in pediatric autistic populations holds significant implications for clinical practice. It can facilitate the early identification of individuals with a higher likelihood of having irritability, enable the tailoring of interventions based on specific predictors identified in the study, and enhance overall care strategies for children experiencing irritability. These insights have the potential to improve diagnostic accuracy, optimize treatment effectiveness, and ultimately enhance patient outcomes in clinical settings.
This review had various strengths. It synthesizes the current body of literature to identify gaps and highlight areas for future research on irritability in autism. A notable strength is its adherence to standard review methodologies, as demonstrated by the use of two independent reviewers who examined each citation and article and met regularly to resolve any conflicts. One notable limitation of this review is its exclusive focus on studies conducted in English, with the majority of reviewed studies conducted in the United States. This limits the generalizability of results to diverse cultural contexts where the presentation and interpretation of irritability among autistic individuals may vary.
This review revealed a significant paucity of literature examining the sociodemographic, phenotypic, and neurobiological and physiological correlates of irritability in autism. There was also a significant gap in understanding the multi-dimensional irritability correlates. Consistent positive associations were found between irritability and sensory differences and mental health symptoms, suggesting potential avenues for investigation of non-medication interventions.
The original contributions presented in the study are included in the article/Supplementary Material, further inquiries can be directed to the corresponding author.
SA: Conceptualization, Data curation, Formal Analysis, Methodology, Writing – original draft, Writing – review & editing. TP: Conceptualization, Methodology, Project administration, Writing – review & editing. JC: Writing – review & editing. MP: Writing – review & editing. AR: Writing – review & editing. AK: Conceptualization, Funding acquisition, Resources, Supervision, Writing – review & editing.
The author(s) declare financial support was received for the research, authorship, and/or publication of this article.
We thank the Canadian Institutes of Health Research (CIHR) for their funding support, which enabled this research.
We wish to express our gratitude for the collective effort and contributions of all individuals involved in the preparation of this review. Each author's dedication and expertise have been invaluable in shaping the research design, data collection, analysis, and manuscript drafting and revision process.
AK is the inventor of a software called the “Anxiety Meter”. She is involved in commercialising the Anxiety Meter [patents US 9,844,332 B2 and US 16/276,208 (pending)] and will financially benefit from its sales. AK served on the board of advisors for Shaftesbury, a media company developing virtual reality products for autistic children, from February 2020 – February 2021, and was compensated financially for this role. AK is also involved in development and evaluation of virtual reality technologies for children and may financially benefit from their commercialization. AK has received donations of hardware for her research program from Samsung Canada.
The remaining authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declared that they were an editorial board member of Frontiers, at the time of submission. This had no impact on the peer review process and the final decision.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/frcha.2024.1393231/full#supplementary-material
1. ^We recognize that there are differences in language conventions for referring to the autistic identity. In this paper, identity-first language (“autistic children”) will be used.
ABC, aberrant behavior checklist; ADHD, attention deficit hyperactivity disorder; ARI, affective reactivity index; ID, intellectual disability; IQ, intelligence quotient; ODD, oppositional defiant disorder; PedsQL, pediatric quality of life inventory; PRISMA, preferred reporting items for systematic reviews and meta-analysis.
1. Hodges H, Fealko C, Soares N. Autism spectrum disorder: definition, epidemiology, causes, and clinical evaluation. Transl Pediatr. (2020) 9(S1):S55–65. doi: 10.21037/tp.2019.09.09
2. Public Health Agency of Canada. Autism spectrum Disorder: Highlights from the 2019 Canadian Health Survey on Children and Youth. Ottawa, oN: Public Health Agency of Canada=Agence de la santé publique du Canada (2022).
3. Ofner M, Coles A, Decou ML. Autism Spectrum Disorder Among Children and Youth in Canada 2018: A Report of the National Autism Spectrum Disorder Surveillance System. Ottawa, oN, Canada: Public Health Agency of Canada (2018).
4. Lai MC, Baron-Cohen S, Buxbaum JD. Understanding autism in the light of sex/gender. Mol Autism. (2015) 6(1):24. doi: 10.1186/s13229-015-0021-4
5. Geschwind DH. Advances in autism. Annu Rev Med. (2009) 60(1):367–80. doi: 10.1146/annurev.med.60.053107.121225
6. Menezes M, Mazurek MO. Associations between domains of health-related quality of life and co-occurring emotional and behavioral problems in youth with autism spectrum disorder. Res Autism Spectr Disord. (2021) 82:101740. doi: 10.1016/j.rasd.2021.101740
7. Snaith RP, Taylor CM. Irritability: definition, assessment and associated factors. Br J Psychiatry. (1985) 147(2):127–36. doi: 10.1192/bjp.147.2.127
8. Vidal-Ribas P, Brotman MA, Valdivieso I, Leibenluft E, Stringaris A. The status of irritability in psychiatry: a conceptual and quantitative review. J Am Acad Child Adolesc Psychiatry. (2016) 55(7):556–70. doi: 10.1016/j.jaac.2016.04.014
9. Kalvin CB, Gladstone TR, Jordan R, Rowley S, Marsh CL, Ibrahim K, et al. Assessing irritability in children with autism spectrum disorder using the affective reactivity index. J Autism Dev Disord. (2021) 51(5):1496–507. doi: 10.1007/s10803-020-04627-9
10. Peterson BS, Zhang H, Lucia RS, King RA, Lewis M. Risk factors for presenting problems in child psychiatric emergencies. J Am Acad Child Adolesc Psychiatry. (1996) 35(9):1162–73. doi: 10.1097/00004583-199609000-00014
11. Brotman MA, Kircanski K, Leibenluft E. Irritability in children and adolescents. Annu Rev Clin Psychol. (2017) 13(1):317–41. doi: 10.1146/annurev-clinpsy-032816-044941
12. Grasser LR, Erjo T, Goodwin MS, Naim R, German RE, White J, et al. Can peripheral psychophysiological markers predict response to exposure-based cognitive behavioral therapy in youth with severely impairing irritability? A study protocol. In Review (2023). Available online at: https://www.researchsquare.com/article/rs-3396443/v1 (cited October 10, 2023).
13. Lecavalier L. Behavioral and emotional problems in young people with pervasive developmental disorders: relative prevalence, effects of subject characteristics, and empirical classification. J Autism Dev Disord. (2006) 36(8):1101–14. doi: 10.1007/s10803-006-0147-5
14. Green J, Gilchrist A, Burton D, Cox A. Social and psychiatric functioning in adolescents with Asperger syndrome compared with conduct disorder. J Autism Dev Disord. (2000) 30:279–93. doi: 10.1023/a:1005523232106
15. Mayes SD, Calhoun SL, Murray MJ, Ahuja M, Smith LA. Anxiety, depression, and irritability in children with autism relative to other neuropsychiatric disorders and typical development. Res Autism Spectr Disord. (2011) 5(1):474–85. doi: 10.1016/j.rasd.2010.06.012
16. Graziosi G, Perry A. Age and sex differences in problem behaviours in youth with autism spectrum disorder. Res Autism Spectr Disord. (2023) 100. doi: 10.1016/j.rasd.2022.102075
17. Salazar de Pablo G, Jordá CP, Vaquerizo-Serrano J, Moreno C, Cabras A, Arango C, et al. Systematic review and meta-analysis: efficacy of pharmacological interventions for irritability and emotional dysregulation in autism Spectrum disorder and predictors of response. J Am Acad Child Adolesc Psychiatry. (2023) 62(2):151–68. doi: 10.1016/j.jaac.2022.03.033
18. Elbe D, Lalani Z. Review of the pharmacotherapy of irritability of autism. J Can Acad Child Adolesc Psychiatry. (2012) 21(2):130–46.22548111
19. Sukhodolsky DG, Gladstone TR, Marsh CL. Irritability in autism. In: Volkmar FR, editor. Encyclopedia of Autism Spectrum Disorders. Cham: Springer International Publishing (2021). p. 2561–4. doi: 10.1007/978-3-319-91280-6_102263
20. McHugh ML. Interrater reliability: the kappa statistic. Biochem Med (Zagreb). (2012) 22(3):276–82. doi: 10.11613/BM.2012.031
21. Anderson DK, Maye MP, Lord C. Changes in maladaptive behaviors from midchildhood to young adulthood in autism spectrum disorder. Am J Intellect Dev Disabil. (2011) 116(5):381–97. doi: 10.1352/1944-7558-116.5.381
22. Baeza-Velasco C, Michelon C, Rattaz C, Baghdadli A. Are aberrant behavioral patterns associated with the adaptive behavior trajectories of teenagers with autism spectrum disorders? Res Autism Spectr Disord. (2014) 8(3):304–11. doi: 10.1016/j.rasd.2013.12.004
23. Bangerter A, Chatterjee M, Manyakov NV, Ness S, Lewin D, Skalkin A, et al. Relationship between sleep and behavior in autism spectrum disorder: exploring the impact of sleep variability. Front Neurosci. (2020) 14(101478481):211. doi: 10.3389/fnins.2020.00211
24. Bitsika V, Sharpley C. Which aspects of challenging behaviour are associated with anxiety across two age groups of young males with an autism Spectrum disorder? J Dev Phys Disabil. (2016) 28(5):685–701. doi: 10.1007/s10882-016-9502-4
25. Bitsika V, Sharpley CF. How is challenging behaviour associated with depression in boys with an autism Spectrum disorder? Int J Disabil Dev Educ. (2017) 64(4):391–403. doi: 10.1080/1034912X.2016.1250872
26. Brenner J, Pan Z, Mazefsky C, Smith KA, Gabriels R. Behavioral symptoms of reported abuse in children and adolescents with autism Spectrum disorder in inpatient settings. Autism and developmental disorders inpatient research collaborative (ADDIRC), editor. J Autism Dev Disord. (2018) 48(11):3727–35. doi: 10.1007/s10803-017-3183-4
27. Carpenter KLH, Davis NO, Spanos M, Sabatos-DeVito M, Aiello R, Baranek GT, et al. Adaptive behavior in young autistic children: associations with irritability and ADHD symptoms. J Autism Dev Disord. (2022). doi: 10.1007/s10803-022-05753-2
28. Carter Leno V, Forth G, Chandler S, White P, Yorke I, Charman T, et al. Behavioural and physiological response to frustration in autistic youth: associations with irritability. J Neurodevelop Disord. (2021) 13(1):27. doi: 10.1186/s11689-021-09374-1
29. Chaidez V, Hansen RL, Hertz-Picciotto I. Gastrointestinal problems in children with autism, developmental delays or typical development. J Autism Dev Disord. (2014) 44(5):1117–27. doi: 10.1007/s10803-013-1973-x
30. Curran LK, Newschaffer CJ, Lee LC, Crawford SO, Johnston MV, Zimmerman AW. Behaviors associated with fever in children with autism spectrum disorders. Pediatrics. (2007) 120(6):e1386–92. doi: 10.1542/peds.2007-0360
31. Dellapiazza F, Michelon C, Robel L, Schoenberger M, Chatel C, Vesperini S, et al. The impact of atypical sensory processing on adaptive functioning and maladaptive behaviors in autism spectrum disorder during childhood: results from the ELENA cohort. J Autism Dev Disord. (2020) 50(6):2142–52. doi: 10.1007/s10803-019-03970-w
32. Dellapiazza F, Michelon C, Picot MC, Baghdadli A. A longitudinal exploratory study of changes in sensory processing in children with ASD from the ELENA cohort. Eur Child Adolesc Psychiatry. (2022) 31(7):1–10. doi: 10.1007/s00787-021-01746-1
33. Estes AM, Dawson G, Sterling L, Munson J. Level of intellectual functioning predicts patterns of associated symptoms in school-age children with autism spectrum disorder. Am J Mental Retardat. (2007) 112(6):439–49. doi: 10.1352/0895-8017(2007)112[439:LOIFPP]2.0.CO;2
34. Ferguson BJ, Marler S, Altstein LL, Lee EB, Mazurek MO, McLaughlin A, et al. Associations between cytokines, endocrine stress response, and gastrointestinal symptoms in autism spectrum disorder. Brain Behav Immun. (2016) 58(bbi, 8800478):57–62. doi: 10.1016/j.bbi.2016.05.009
35. Ferguson B, Marler S, Altstein L, Lee E, Akers J, Sohl K, et al. Psychophysiological associations with gastrointestinal symptomatology in autism Spectrum disorder. Autism Res. (2017) 10(2):276–88. doi: 10.1002/aur.1646
36. Flowers J, Lantz J, Hamlin T, Simeonsson RJ. Associated factors of self-injury among adolescents with autism spectrum disorder in a community and residential treatment setting. J Autism Dev Disord. (2020) 50(8):2987–3004. doi: 10.1007/s10803-020-04389-4
37. Fok M, Bal VH. Differences in profiles of emotional behavioral problems across instruments in verbal versus minimally verbal children with autism spectrum disorder. Autism Res. (2019) 12(9):1367–75. doi: 10.1002/aur.2126
38. Frazier TW, Georgiades S, Bishop SL, Hardan AY. Behavioral and cognitive characteristics of females and males with autismin the Simons simplex collection. J Am Acad Child Adolesc Psychiatry. (2013) 53(3):329–40.e1. doi: 10.1016/j.jaac.2013.12.004
39. Frye RE, Wynne R, Rose S, Slattery J, Delhey L, Tippett M, et al. Thyroid dysfunction in children with autism spectrum disorder is associated with folate receptor alpha autoimmune disorder. J Neuroendocrinol. (2017) 29(3). doi: 10.1111/jne.12461
40. Gabriels RL, Cuccaro ML, Hill DE, Ivers BJ, Goldson E. Repetitive behaviors in autism: relationships with associated clinical features. Res Dev Disabil. (2005) 26(2):169–81. doi: 10.1016/j.ridd.2004.05.003
41. Gotham K, Bishop SL, Hus V, Huerta M, Lund S, Buja A, et al. Exploring the relationship between anxiety and insistence on sameness inautism spectrum disorders. Autism Res. (2012) 6(1):33–41. doi: 10.1002/aur.1263
42. Griffin ZAM, Boulton KA, Thapa R, DeMayo MM, Ambarchi Z, Thomas E, et al. Atypical sensory processing features in children with autism, and their relationships with maladaptive behaviors and caregiver strain. Autism Res. (2022) 15(6):1120–9. doi: 10.1002/aur.2700
43. Gundogdu U, Aksoy A, Eroglu M. Sensory profiles, behavioral problems, and auditory findings in children with autism spectrum disorder. Int J Dev Disabil. (2023) 69(3):442–51. doi: 10.1080/20473869.2023.2200592
44. Hartley-McAndrew M, Weinstock A. Autism spectrum disorder: correlation between aberrant behaviors, EEG abnormalities and seizures. Neurol Int. (2010) 2(1):42–7. doi: 10.4081/ni.2010.e10
45. Henry CA, Nowinski L, Koesterer K, Ferrone C, Spybrook J, Bauman M. Low rates of depressed mood and depression diagnoses in a clinic review of children and adolescents with autistic disorder. J Child Adolesc Psychopharmacol. (2014) 24(7):403–6. doi: 10.1089/cap.2014.0024
46. Hirota T, Deserno M, McElroy E. The network structure of irritability and aggression in individuals with autism Spectrum disorder. J Autism Dev Disord. (2020) 50(4):1210–20. doi: 10.1007/s10803-019-04354-w
47. Johnson CR, Smith T, DeMand A, Lecavalier L, Evans V, Gurka M, et al. Exploring sleep quality of young children with autism spectrum disorder and disruptive behaviors. Sleep Med. (2018) 44(100898759):61–6. doi: 10.1016/j.sleep.2018.01.008
48. Kryza-Lacombe M, Iturri N, Monk CS, Wiggins JL. Face emotion processing in pediatric irritability: neural mechanisms in a sample enriched for irritability with autism spectrum disorder. J Am Acad Child Adolesc Psychiatry. (2020) 59(12):1380–91. doi: 10.1016/j.jaac.2019.09.002
49. Lee KS, Gau SSF, Tseng WL. Autistic symptoms, irritability, and executive dysfunctions: symptom dynamics from multi-network models. J Autism Dev Disord. (2023). doi: 10.1007/s10803-023-05981-0
50. Lundwall RA, Stephenson KG, Neeley-Tass ES, Cox JC, South M, Bigler ED, et al. Relationship between brain stem volume and aggression in children diagnosed with autism spectrum disorder. Res Autism Spectr Disord. (2017) 34(101300021):44–51. doi: 10.1016/j.rasd.2016.12.001
51. Martinez-Gonzalez AE, Moreno-Amador B, Piqueras JA. Differences in emotional state and autistic symptoms before and during confinement due to the COVID-19 pandemic. Res Dev Disabil. (2021) 116(8709782, rid):104038. doi: 10.1016/j.ridd.2021.104038
52. Mayes SD, Castagna PJ, Waschbusch DA. Sex differences in externalizing and internalizing symptoms in ADHD, autism, and general population samples. J Psychopathol Behav Assess. (2020) 42(3):519–26. doi: 10.1007/s10862-020-09798-4
53. Mayes SD, Baweja R, Waschbusch DA, Calhoun SL. Relationship between IQ and internalizing and externalizing symptoms in children with autism and children with ADHD. J Ment Health Res Intellect Disabil. (2022) 15(2):95–110. doi: 10.1080/19315864.2022.2029643
54. Mazurek MO, Sohl K. Sleep and behavioral problems in children with autism spectrum disorder. J Autism Dev Disord. (2016) 46(6):1906–15. doi: 10.1007/s10803-016-2723-7
55. Mikita N, Hollocks MJ, Papadopoulos AS, Aslani A, Harrison S, Leibenluft E, et al. Irritability in boys with autism spectrum disorders: an investigation of physiological reactivity. J Child Psychol Psychiatry. (2015) 56(10):1118–26. doi: 10.1111/jcpp.12382
56. Molcho-Haimovich A, Tikotzky L, Meiri G, Ilan M, Michaelovski A, Schtaierman H, et al. Sleep disturbances are associated with irritability in ASD children with sensory sensitivities. J Neurodev Disord. (2023) 15(1):21. doi: 10.1186/s11689-023-09491-z
57. Nelson MA, Shaffer RC, Schmitt LM, Coffman MC, Horn PS, Reisinger DL, et al. Health related quality of life in autistic youth and their families. J Autism Dev Disord. (2023). doi: 10.1007/s10803-023-06054-y
58. Neuhaus E, Webb SJ, Bernier RA. Linking social motivation with social skill: the role of emotion dysregulation in autism spectrum disorder. Dev Psychopathol. (2019) 31(3):931–43. doi: 10.1017/S0954579419000361
59. Ogur T, Boyunaga OL. Relation of behavior problems with findings of cranial diffusion tensor MRI and MR spectroscopy in autistic children. Int J Clin Exp Med. (2015) 8(4):5621–30.26131145
60. Rosen NE, Schiltz HK, Lord C. Sibling influences on trajectories of maladaptive behaviors in autism. J Clin Med. (2022) 11(18). doi: 10.3390/jcm11185349
61. Sannar EM, Palka T, Beresford C, Peura C, Kaplan D, Verdi M, et al. Sleep problems and their relationship to maladaptive behavior severity in psychiatrically hospitalized children with autism spectrum disorder (ASD). Siegel M, autism and developmental disorders inpatient research collaborative (ADDIRC), editors. J Autism Dev Disord. (2018) 48(11):3720–6. doi: 10.1007/s10803-017-3362-3
62. Turkoglu S, Ucar HN, Cetin FH, Guler HA, Tezcan ME. The relationship between irritability and autism symptoms in children with ASD in COVID-19 home confinement period. Int J Clin Pract. (2021) 75(11):e14742. doi: 10.1111/ijcp.14742
63. Valicenti-McDermott M, Lawson K, Hottinger K, Seijo R, Schechtman M, Shulman L, et al. Sleep problems in children with autism and other developmental disabilities: a brief report. J Child Neurol. (2019) 34(7):387–93. doi: 10.1177/0883073819836541
64. Viscidi EW, Johnson AL, Spence SJ, Buka SL, Morrow EM, Triche EW. The association between epilepsy and autism symptoms and maladaptivebehaviors in children with autism spectrum disorder. Autism. (2013) 18(8):996–1006. doi: 10.1177/1362361313508027
65. Williams DL, Mazefsky CA, Siegel M, Erickson C, Gabriels RL, Kaplan D, et al. Problem behaviors in autism spectrum disorder: association with verbal ability and adapting/coping skills. J Autism Dev Disord. (2018) 48(11):3668–77. doi: 10.1007/s10803-017-3179-0
66. Yavuz-Kodat E, Reynaud E, Geoffray M-M, Limousin N, Franco P, Bonnet-Brilhault F, et al. Disturbances of continuous sleep and circadian rhythms account for behavioural difficulties in children with autism Spectrum disorder. J Sleep Res. (2020) 29(SUPPL 1). doi: 10.3390/jcm9061978
67. Simonoff E, Kent R, Stringer D, Lord C, Briskman J, Lukito S, et al. Trajectories in symptoms of autism and cognitive ability in autism from childhood to adult life: findings from a longitudinal epidemiological cohort. J Am Acad Child Adolesc Psychiatry. (2020) 59(12):1342–52. doi: 10.1016/j.jaac.2019.11.020
68. Ver Ploeg M, Perrin E, editors. Panel on DHHS collection of race and ethnicity data. Eliminating Health Disparities: Measurement and Data Needs. Washington, DC: National Academies Press (2004). Available online at: http://www.nap.edu/catalog/10979 (cited February 6, 2024).
69. Aylward BS, Gal-Szabo DE, Taraman S. Racial, ethnic, and sociodemographic disparities in diagnosis of children with autism spectrum disorder. J Dev Behav Pediatr. (2021) 42(8):682–9. doi: 10.1097/DBP.0000000000000996
70. MacLennan K, O’Brien S, Tavassoli T. In our own words: the complex sensory experiences of autistic adults. J Autism Dev Disord. (2022) 52(7):3061–75. doi: 10.1007/s10803-021-05186-3
71. Milner V, McIntosh H, Colvert E, Happé F. A qualitative exploration of the female experience of autism spectrum disorder (ASD). J Autism Dev Disord. (2019) 49(6):2389–402. doi: 10.1007/s10803-019-03906-4
72. Yoshida K, Lunsky Y, Müller DJ, Desarkar P. Prevalence of psychotropic medication use and psychotropic polypharmacy in autistic adults with or without intellectual disability. J Autism Dev Disord. (2024). doi: 10.1007/s10803-023-06208-y
73. Kushki A, Brian J, Dupuis A, Anagnostou E. Functional autonomic nervous system profile in children with autism spectrum disorder. Mol Autism. (2014) 5(1):39. doi: 10.1186/2040-2392-5-39
74. Arora I, Bellato A, Ropar D, Hollis C, Groom MJ. Is autonomic function during resting-state atypical in autism: a systematic review of evidence. Neurosci Biobehav Rev. (2021) 125:417–41. doi: 10.1016/j.neubiorev.2021.02.041
Keywords: autism, irritability, correlate, predictor, pediatric
Citation: Alatrash S, Paul T, Carbone J, Penner M, Roshan Fekr A and Kushki A (2024) Predictors of irritability in pediatric autistic populations: a scoping review. Front. Child Adolesc. Psychiatry 3: 1393231. doi: 10.3389/frcha.2024.1393231
Received: 1 March 2024; Accepted: 9 July 2024;
Published: 23 July 2024.
Edited by:
Adham Atyabi, University of Colorado Colorado Springs, United StatesReviewed by:
Marco Lamberti, South Tyrol Health Service, Italy© 2024 Alatrash, Paul, Carbone, Penner, Roshan Fekr and Kushki. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Azadeh Kushki, YWt1c2hraUBob2xsYW5kYmxvb3J2aWV3LmNh
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.