 Damian Muszyński1
Damian Muszyński1 Robert Kucharski2,3
Robert Kucharski2,3 Natalia Marek-Trzonkowska4,5Magdalena Kalinowska1,6Aleksandra Brzóska1Marika Bolcewicz2
Natalia Marek-Trzonkowska4,5Magdalena Kalinowska1,6Aleksandra Brzóska1Marika Bolcewicz2 Leszek Kalinowski2,7*
Leszek Kalinowski2,7* Karolina Kaźmierczak-Siedlecka2*
Karolina Kaźmierczak-Siedlecka2*- 1Scientific Circle of Studies Regarding Personalized Medicine Associated with Department of Medical Laboratory Diagnostics, Medical University of Gdansk, Gdansk, Poland
- 2Department of Medical Laboratory Diagnostics – Fahrenheit Biobank BBMRI.pl, Medical University of Gdansk, Gdansk, Poland
- 3Neodentica Dentistry Center, Gdansk, Poland
- 4International Centre for Cancer Vaccine Science, University of Gdansk, Gdansk, Poland
- 5Laboratory of Immunoregulation and Cellular Therapies, Department of Family Medicine, Medical University of Gdansk, Gdansk, Poland
- 6University of Social Sciences and Humanities, Warsaw, Poland
- 7BioTechMed Center, Department of Mechanics of Materials and Structures, Gdansk University of Technology, Gdansk, Poland
Sjögren’s syndrome is an autoimmune disease characterized by lymphatic infiltration of secretory tissues. The disease results in dryness of the eyeball or mouth, which often occur simultaneously. Agents used to treat Sjögren’s syndrome may improve oral hydration and the patient’s quality of life. There are several pharmacological and non-pharmacological agents used to treat significant problem like xerostomia. The use of appropriate medicines (i.e. pilocarpine and cevimeline) may cause changes in the local microbiome, which is very sensitive to quantitative changes in water. As a result of Sjögren’s syndrome, a new balance of the microbiome is established in the oral cavity, which, if disturbed by medical measures, may increase the risk of oral lesions (such as periodontopathies or caries) or reduce this risk. Overall, the knowledge regarding microbiological aspects and agents treating oral dryness is still not well described but initial results indicate some microbial alterations.
Introduction
Sjögren’s syndrome (SS) is a systemic chronic autoimmune disease, which touches connective tissues (André and Böckle, 2022). It has been established that 1-3% of the general population may suffer from this disease (Bayetto and Logan, 2010). Often, it is diagnosed between the 5th and the 7th decade of life and occurs eight times more frequently (about eight times more often) in women than in men (Bayetto and Logan, 2010; André and Böckle, 2022). The etiology of this disease is unknown, but environmental factors are suspected to play a key role (André and Böckle, 2022). Risk factors include viral diseases (Epstein-Barr virus, HCV, human lymphocyte leukemia virus), genetic predisposition and sex hormones (Bayetto and Logan, 2010). However, the greatest impact appears to be exerted by the Epstein-Barr virus, which is found in biopsy materials taken from the lacrimal glands, as well as in salivary gland and saliva specimens (Negrini et al., 2022).Viral infection most likely promote the production of auto-antibodies, ultimately leading to cross-reactivity of immune elements with host antigens (Bayetto and Logan, 2010). It is assumed that the genetic predisposition to Sjögren’s syndrome can be diagnosed if this disease occurs in at least two family members (Bayetto and Logan, 2010). The relationships between polymorphic major histocompatibility complex (MHC) genes are expected to play an important role here (Bayetto and Logan, 2010).The disproportion in the incidence of SS allows us to put forward the theory that sex hormones play an important role in etiology. Research show that estrogens influence the immune response by increasing the production of antibodies by B cells. The menopause period in women is the most common age range in which SS occurs, which may indicate an indirect effect of estrogens on the development of this disease (Bayetto and Logan, 2010).
Sjögren’s syndrome could be primary (pSS) or secondary (sSS) but both is likely similar (Bayetto and Logan, 2010). Their difference resides in that sSS is an element of other autoimmune diseases, most often systemic lupus erythematosus (15-36%), rheumatoid arthritis (20-32%) or progressive and limited systemic sclerosis (11-24%) (Stefanski et al., 2017). pSS is not correlated with any autoimmune diseases (Bayetto and Logan, 2010). There are general symptoms of dryness, known as dryness syndrome (xerostomia, xerophthalmia) (Bayetto and Logan, 2010; Zeron et al., 2013). The pathogenesis is still unknown (Negrini et al., 2022). However, the main role in the development might be played by elements of the immune system (T and B cells) (Bayetto and Logan, 2010; Tian et al., 2021). Excessive activation of B cells located in the exocrine glands causes the production of anti-SSA and anti-SSB autoantibodies (0–70% patients with pSS) (Bayetto and Logan, 2010; Tian et al., 2021). T cells, on the other hand, infiltrate the exocrine glands and increase the extremity of cytokines, thus leading to damage to the lobular cells and ultimately to xerostomia (Tian et al., 2021).
The concerns of Sjögren’s syndrome center on disorders of the exocrine glands (Tian et al., 2021). Most commonly, patients report symptoms such as dry eyes and dry mouth (89% of them experience both) (Negrini et al., 2022). In the aspect of the oral cavity, dysphagia, pain and burning are frequently noticeable, which is related to reduced saliva production (Negrini et al., 2022). Often, a physical examination also reveals dental caries and periodontal disease, as well as frequently recurrent Candida albicans infections (occurring 10 times more often than in the normal population) (Stefanski et al., 2017; Negrini et al., 2022). In sSS, symptoms of fatigue and joint pain may also manifest (6). Usually treating Sjögren’s syndrome is symptomatic (Baer and Walitt, 2018). It is crucial to stay hydrated, quit smoking, apply fluoride to prevent dental caries and avoid fatigue (among others, good sleep hygiene) (Baer and Walitt, 2018). Pharmacological treatment typically relies on muscarinic agonists, such as pilocarpine and cevimeline, which enhance the production of saliva and tears (Baer and Walitt, 2018). However, these drugs have cholinergic side effects, such as flushing chills, and excessive sweating (Baer and Walitt, 2018). To prevent this, moisturization of the oral tissues can also be achieved by using artificial saliva (Bayetto and Logan, 2010).
Oral healthy microbiome
The oral microbiome, being one of the most diverse microbial communities in the human body, plays a crucial role in maintaining human health (Zhou et al., 2023). The human oral microbiome encompasses all microorganisms found in the oral cavity—including distinct habitats such as teeth, gingival sulcus, attached gingiva, tongue, cheek, lip, hard palate, and soft palate—and its contiguous extensions like the tonsils, pharynx, esophagus, Eustachian tube, middle ear, trachea, lungs, nasal passages, and sinuses, though most studies and samples focus on the oral cavity itself (Dewhirst et al., 2010). The oral cavity contains over 700 different species of bacteria, fungi, viruses, archaea, and protozoa. Bacteria are the most extensively studied microorganisms in the oral cavity, yet only 57% of the bacterial species present have been named (Kozak and Pawlik, 2023). In healthy individuals, the oral microbiome predominantly comprises facultative anaerobic Gram-positive bacteria (Kozak and Pawlik, 2023). 16S rDNA profiling of a healthy oral cavity identified six major bacterial phyla: Firmicutes, Actinobacteria, Proteobacteria, Fusobacteria, Bacteroidetes, and Spirochaetes (Verma et al., 2018). Brief descriptions of the more important bacteria are provided below.
One of the most important representatives of Firmicutes is Streptococcus mutans, which lives mainly on tooth surfaces (Lemos et al., 2019; Sedghi et al., 2021). Its ability to metabolize carbohydrates, create low-pH acids and finally produce glucans (an important component for the backbone of dental plaque), which makes it one of the existing etiological factors of caries (Lemos et al., 2019). Actinomyces, belonging to Actinobacteria, are the natural flora of the oral cavity, living on the surfaces of mucous membranes (Könönen and Wade, 2015). They constitute (A. oris, A. naeslundi) quite an important element of the oral biofilm, and may also participate in the development of dental caries (Könönen and Wade, 2015). As a result of the microbiological balance in the oral cavity, there may be a sudden increase in the occurrence of Actinomyces, causing actinomycosis (Smego and Foglia, 1998; Könönen and Wade, 2015). Haemophilus, which belong to the Proteobacteria, cause a wide range of infections that require blood-derived factors for their growth (Musher, 1996). A natural component of the oral cavity is H. aphrophilus, which under specific conditions can cause bacterial endocarditis (Musher, 1996). Porphyromonas gingivalis is an anaerobic gram-negative bacterium, classified as Bacteroidetes, strongly associated with periodontal disease (Zhou and Luo, 2019). By regulating the human’s immune response, it disrupts its chomesotasis, which contributes to the occurrence of gum diseases (Zhou and Luo, 2019). These actions are due to a series of protein adhesins, binding proteinases and hemin. More and more often, you can also find information about the connection between P. gingivalis and the occurrence of cancers, among others. squamous cell carcinoma of the oral cavity or esophagus (Zhou and Luo, 2019). Fusobacterium nucleatum is a Gram-negative rod-shaped bacterium, belonging to Fusobacteria, commonly found in the oral cavity. It plays a crucial role in dental plaque biofilm formation (McIlvanna et al., 2021). Although traditionally not considered pathogenic in the oral cavity, it has emerged as an important player in driving inflammation and may act as an opportunistic pathogen in extra-oral sites (McIlvanna et al., 2021). F. nucleatum acts as a “bridging” bacterium, facilitating interactions between early and late colonizers in dental plaque and has the potential to bind to various cell types, thus contribute to carcinogenesis through its adhesins FadA and Fap2 (McIlvanna et al., 2021). Treponema denticola, belonging to Spirochaetes play a significant role in oral diseases such as periodontitis, necrotizing ulcerative gingivitis, and acute pericoronitis (Yousefi et al., 2020). These bacteria contribute to tissue destruction through direct bacterial action and by triggering an exaggerated host inflammatory response (Yousefi et al., 2020).
Bacteria are the primary focus of research on the human oral microbiome and constitute the majority of biomass in the oral environment, whereas fungi are estimated to make up as little as less than 0.1% of it (Baker et al., 2017). The initial study examining the composition of the fungal component oral in healthy individuals’ microbiota found that the most commonly identified fungal genera were Candida, Cladosporium, Aureobasidium, Saccharomycetales, and Aspergillus (Ghannoum et al., 2010). Fungi in the oral cavity have been studied mainly in relation to diseases, and their role in maintaining a healthy oral ecology remains largely unknown (Krom et al., 2014). The review exploring current knowledge on fungi-bacteria interactions likewise highlights the needs for further research to understand fungi’s contribution to oral health (Krom et al., 2014). The oral virome in healthy individuals consists mainly of bacteriophages, which are more numerous than eukaryotic viruses (Baker et al., 2017). Compared to the oral bacteriome, oral virome is characterised by significant individual variability while remaining stable over time (Baker et al., 2017). Despite of technological advancements, studying the human virome is challenging due to the low abundance of viral nucleic acids, the difficulty in purifying unknown virions, and the complexities in analyzing and identifying novel viruses (Bikel et al., 2015). The viruses causing symptoms are well-studied, while the vast, symptomless majority remains poorly understood (Lecuit and Eloit, 2013).
Oral microbiome in xerostomia of Sjögren’s syndrome
Reduced amount of saliva plays an important role in Sjögren’s syndrome (Bayetto and Logan, 2010; van der Meulen et al., 2018b; Negrini et al., 2022). First, it cleanses the oral cavity - dilutes food remains and washes out bacteria from the surface of the mucous membranes (Lynge Pedersen and Belstrøm, 2019). In SS, the persistence of food and microorganisms is prolonged (sugar clearance is also reduced), which leads to changes in the composition of the flora, promoting the growth of acid-forming and tolerant bacteria. Acidic environment, in particular Streptococcus mutans, Streptococcus sobrinus and Lactobacilli, which produce acids from retained carbohydrates and increase the risk of developing caries (Li et al., 2022). S. mutans may have a close correlation with the occurrence of Candida albicans (Li et al., 2022). Moreover, in a study conducted by Nadig et al., which concerned determining the relationship between salivary flow rate and the number of Candida in xerostomia, a correlation was observed between low SFR and an increase in the number of Candida, in which C. albicans was the most common (Nadig et al., 2017). Analysis of the interactions between these two species showed that protein genes related to carbohydrate metabolism in C. albicans were enhanced (Li et al., 2022). What’s more, as a result of this culture, the mass of the total biofilm increased (Li et al., 2022). Another issue are mucins present in saliva (Lynge Pedersen and Belstrøm, 2019). They prevent the adhesion and formation of a biofilm by microorganisms such as staphylococci, streptococci or Candida and participate in the binding of, for example, Porphyromonas gingivalis (Li et al., 2022). The coating formed from saliva is important in preventing the colonization of various surfaces of the oral cavity (Li et al., 2022). The topic of the role of saliva is very complex. We know that its impact on the microbiome is influenced by among others, salivary amylase, the salivary peroxidation system, salivary lysosomes, lactoferrin, rich proteins in proline, staterin, cystatin, histatin and immunoglobulins (Lynge Pedersen and Belstrøm, 2019). In recent years, many studies have been carried out aiming to describe the differences between the microbiome in people with Sjögren’s syndrome, people with xerostomia for other reasons and healthy patients. In a study by Huang YF et al. statistically significant differences were observed - a decrease in the Bacteroides genus and a significant increase in the Firmicutes genus (Huang et al., 2019). Another study suggests that a high ratio of Firmicutes to Proteobacteria (taco) may be a characteristic indicator of xerostomia (van der Meulen et al., 2018a). In addition, a higher total number of microorganisms of the genus Candida, Streptococcus mutans, lactobacilli was noticed (Myers, 2015). Although impaired salivary secretion has been shown to be the dominant contributor to the change in oral microflora in SS, differences were reported in the microbiota between people with xerostomia and Sjögren’s syndrome (van der Meulen et al., 2018b). Similary, the same that could be used in treatment and diagnosis (Sembler-Møller et al., 2019), however not all studies confirm this. Example of which is a lower relative number of Granulicatella and Bergeyella in patients with compared to Sjögren’s syndrome (van der Meulen et al., 2018a). A study conducted on a small group using PCR methods allowing the division of microorganisms even into their species showed significant differences (Rusthen et al., 2019). First of all, a lower percentage of Streptococci, Neisseria, Actinomyces lingnae and Haemophilus was observed in people with Sjögren’s syndrome, and a higher percentage of Porphyromonas pasteri, Megasphaera micronuciformis (Rusthen et al., 2019). The study’s authors emphasize that their findings may in the future be used to detect SS based on the examination of the oral microbiome as a specific biomarker of the disease, and prove that the changes in oral flora in Sjögren’s syndrome are caused not only by reduced salivary secretion, but also by other factors that have not yet been described (Rusthen et al., 2019). Another publication describes Lactobacillus and Streptococcus as potential biomarkers (Kim et al., 2022). It also suggests that in the future it may be possible to treat the symptoms of Sjögren’s syndrome by using prebiotics, which is already being conducted in the treatment of other autoimmune diseases such as rheumatism (Zamani et al., 2016). Interestingly, there are publications suggesting that changes in the oral microbiome may indirectly lead to the development of Sjögren’s syndrome (Tsigalou et al., 2018). Therefore, monitoring the oral microflora could be more specific in prevention, but the exact pathomechanism of this disease has not yet been clarified (Tsigalou et al., 2018). This is an interesting direction for future research on the links between Sjögren’s syndrome and the oral microbiome (Tsigalou et al., 2018). A comparison of the microbiome in xerostomia with the healthy oral cavity is presented in the Table 1.
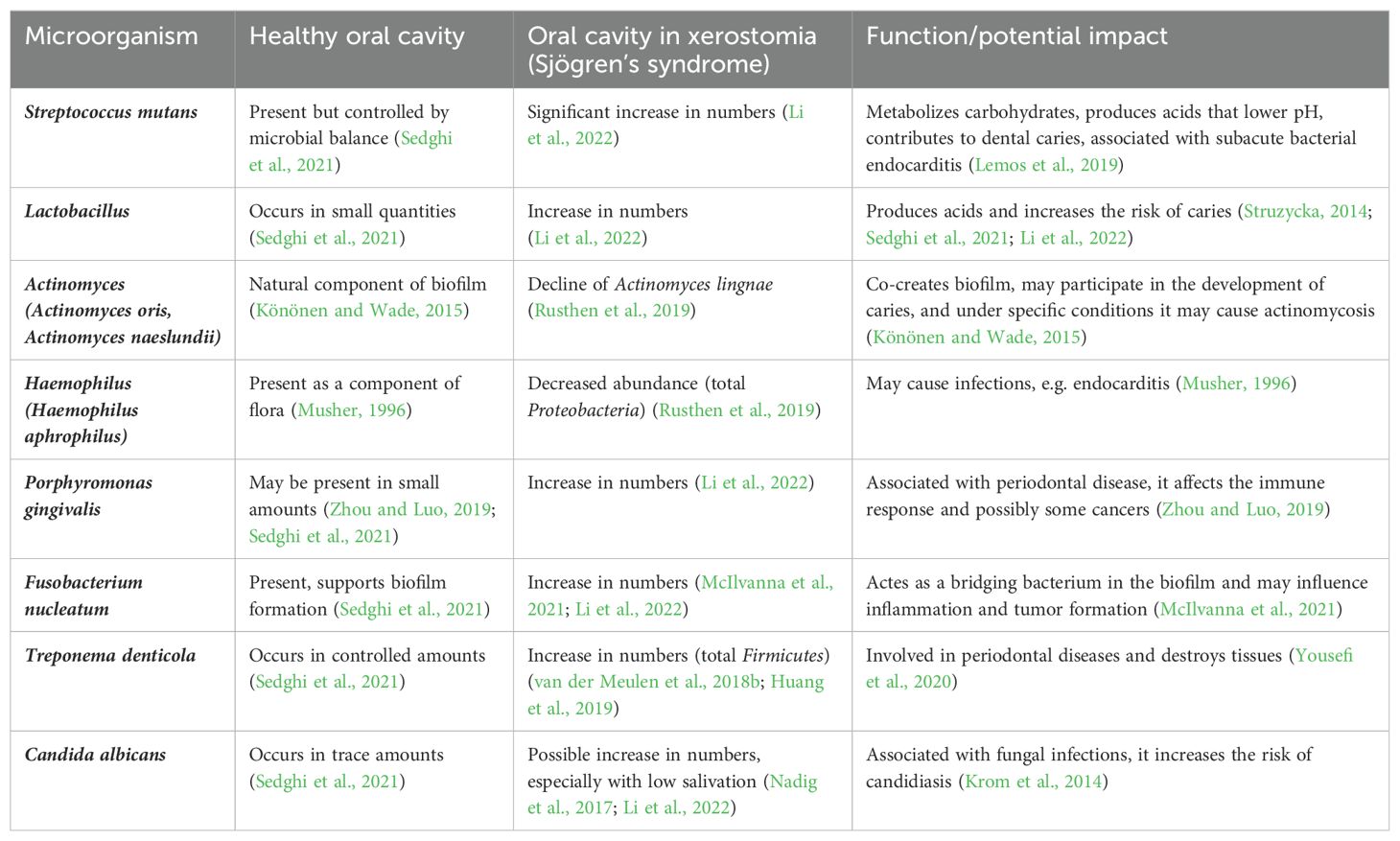
Table 1. Comparison of the occurrence of more important microorganisms in a healthy oral cavity and in xerostomia, taking into account the most important functions of microorganisms.
Agents used to treat xerostomia of Sjögren’s syndrome and their impact on the oral microbiome
Sjögren’s syndrome often causes decreased salivation – xerostomia (Bayetto and Logan, 2010; Baer and Walitt, 2018). It is estimated that 88% of patients with SS have decreased salivary secretion, which ultimately resulted in xerostomia in around 75-92% of patients (Cartee et al., 2015). These symptoms can be treated with agents that lead to produce more saliva (sugar-free chewing gum, pilocarpine, cevimyelin) or with artificial saliva, which may play a similar role (Bayetto and Logan, 2010). These pharmacological and non-pharmacological agents are described below.
Pilocarpine
One of the basic pharmacological agents used to treat xerostomia occurring in Sjögren’s syndrome is pilocarpine (Watanabe et al., 2018). It is a muscarinic agonist that imitates the action of acetylcholine (Bayetto and Logan, 2010). Pilocarpine binds to the muscarinic acetylcholine receptor located in the acinar cells of the salivary glands (Kapourani et al., 2022). It is able to activate all five subtypes of the aforementioned receptors, although the therapeutic effect is mostly related to receptor M3R (Kapourani et al., 2022). After oral administration, there is an increase in the rate of saliva secretion, which may persist for 1-2 hours (Wiseman and Faulds, 1995). Despite saliva stimulation, pilocarpine does not reduce the risk of caries in patients with xerostomia (Hsu et al., 2019). An observational study by Hsu CY et al. among patients suffering from new-onset primary Sjögren’s syndrome, taking pilocarpine and individuals not taking it, showed that the risk of caries does not differ significantly between both studied groups (Hsu et al., 2019). A similar situation could be observed in the case of the risk of periodontitis and oral candidiasis (Hsu et al., 2019). Candida albicans is mainly responsible for the occurrence of candidiasis in the oral cavity, and P. gingivalis is responsible for periodontitis (Hellstein and Marek, 2019; Di Stefano et al., 2022). Dental caries is caused by bacteria such as Streptococcus mutans, Actinomyces, and Lactobacillus (Struzycka, 2014). The above-mentioned study shows that the risk of candidiasis, periodontitis and caries does not change significantly, which leads to the conclusion that the use of pilocarpine does not significantly affect the above-mentioned elements of the oral microbiome of patients with SS (Hsu et al., 2019).
Cevimeline
Another drug used to treat xerostomia occurring in Sjögren’s syndrome is cevimeline (Cevimeline). It is an acetylcholine analogue that stimulates the salivary glands via muscarinic receptors (Bayetto and Logan, 2010; Cevimeline). Cevimeline, similarly as pilocarpine, binds the M3R and M1R receptors (also found in the salivary glands); Their activation intensifies the work of the secretory glands, resulting in an increase in the amount of produced saliva and, consequently, a reduction in the symptoms of xerostomia (Fife et al., 2002). Rose F et al. showed that cevimeline reduces the feeling of subjective dry mouth while increasing saliva flow (Fife et al., 2002). However, there was no data regarding the composition of stimulated saliva or changes in the potential risk of caries or candidiasis in patients with SS (Fife et al., 2002). The effect of cevimeline on the oral microbiome is still unclear. It can only be assumed that, since its effects are similar to those of pilocarpine, cevimeline may also slightly change the oral microbiome in patients with Sjögren’s syndrome. The main difference between cevimyelin and pilocarpine is that the former binds to M2R receptors to a lesser extent, resulting in reduced of cardiac tissue (Bayetto and Logan, 2010). A study conducted by Ono K. et al. comparing the effects of cevimeline and pilocarpine in rats showed that cevimeline and pilocarpine increase Ca(2+) concentration to similar quantities, but the cevimeline increases it at a steeper rate (Ono et al., 2012). What is more, cevimeline inhibits water intake, which is supposed to contrast with the effect of pilocarpine (Ono et al., 2012). Possibly due to its slightly different effect on stimulated saliva, cevimeline may cause changes in the oral microbiome in people with xerostomia.
Sugar-free gum
Saliva stimulation is also provided by consuming sugar-free chewing gum, which results in dislodging debrits and the mechanical bacterial clearance (Bayetto and Logan, 2010; Maintaining the Oral Health of Patients With Sjögren’s Syndrome, 2018). When chewing it, the gleeking phenomenon increases, during which the muscles of the tongue and the muscles connected to it are used to stimulate saliva, especially in the submandibular and sublingual glands (Maintaining the Oral Health of Patients With Sjögren’s Syndrome, 2018). Moreover, chewing gum neutralize acids due to its baking soda content (Maintaining the Oral Health of Patients With Sjögren’s Syndrome, 2018). Sugar-free chewing gum owes its action to polyalcohols, the most common of which are xylitol, sorbitol, and mannitol (Imfeld, 1994). The most popular ingredient is xylitol – a pentol that is not metabolized by cariogenic bacteria, including S. mutans. Critically, xylitol may reduce the presence of these bacteria in the oral cavity and thanks to this, reduce the risk of caries (Imfeld, 1994; Janket et al., 2019). A study conducted by Chen SY et al. regarding xylitol also showed that it has an inhibitory effect on Porphyromonas gingivalis - the bacterium responsible for the occurrence of periodontal disease (Chen et al., 2023). However, the inhibitory process itself remains unclear; some sources claim that there is a relationship between the dose of xylitol and the quantitative change of P. gingivalis, others have shown an effect on the expression of cytokines induced by P. gingivalis (Chen et al., 2023). Instead of xylitol, sugar-free chewing gum can include sorbitol, which is a heksykol often used as a sweetener (Imfeld, 1994; Liauw and Saibil, 2019). Oza S. et al. showed that sorbitol gum is effective in reducing lactic acid bacteria comparably to that of xylitol gum, although it is not as effective in reducing the number of streptococci (Oza et al., 2018). Sorbitol has a reducing effect on Lactobacillus, but not comparable to that of xylitol on S. mutans (Oza et al., 2018). Regarding mannitol, another hexitol, there is the least amount of research (Imfeld, 1994). JH. Shaw determined that mannitol, like sorbitol, is unable to increase caries activity in rats in the presence of starch. It is also known that mannitol, like other polyalcohols, does not have an acid-forming effect (Imfeld, 1994). All polyalcohols work in a similar way to xylitol, so it is possible that all of them, including mannitolol, reduce the amount of S. mutans in dental plaque to some extent (Imfeld, 1994; Janket et al., 2019). However, further research is required to determine the specific effect on the remaining bacteria that can cause caries.
Artificial saliva
Artificial saliva’s ingredients should resemble the saliva secreted by human salivary glands by adding appropriate remineralizing and antimicrobial agents (Mystkowska et al., 2018; Maintaining the Oral Health of Patients With Sjögren’s Syndrome, 2018). Its closeness to natural saliva depends on the ingredients used to produce it (Niemirowicz-Laskowska et al., 2020). For example, according to the study of Mystkowska J. et al., preparations based mainly on mucin render parameters most similar to those of human saliva (Mystkowska et al., 2018). Niemirowicz-Laskowska K. et al. allows us to see that different preparations inhibit the multiplication of oral pathogens to varying degrees (Niemirowicz-Laskowska et al., 2020). Selected pathogens (fungal or bacterial) incubated on the medium in the presence of tested artificial saliva preparations (Niemirowicz-Laskowska et al., 2020). Interestingly, in the case of only one of the preparations used, a significant reduction in the growth of microorganisms could be observed (Niemirowicz-Laskowska et al., 2020). The preparations had a particular effect on Pseudomonas auroginosa and C. albicans. However, the impact on S. mutans was negligible, as none of the tested preparations influenced its multiplication (Niemirowicz-Laskowska et al., 2020). In the aforementioned study, it was also possible to observe that the use of nanoparticles in artificial saliva preparations reduces the adhesion process by up to 65% for gram-positive bacteria and fungi and by 45% for gram-negative bacteria, which ultimately resulted in a reduction of E. coli by 70% and by 40% P. auroginosa and C. albicans (Niemirowicz-Laskowska et al., 2020). Moreover, the study conducted by Silva MP et al. showed that artificial saliva containing carboxymethylcellulose reduces the presence of Candida albicans more effectively than artificial saliva consisting of lactoferrinins, lysozyme, cactoperoxidase (Silva et al., 2012). Nevertheless, artificial saliva still does not provide satisfactory results (Kho, 2014). A ramdomized study conducted by Cifuentes M. et al. showed that the use of pilocarpine is more effective than the use of artificial saliva in people suffering from Sjögren’s syndrome (Cifuentes et al., 2018). A summary of the above information is provided in Table 2.
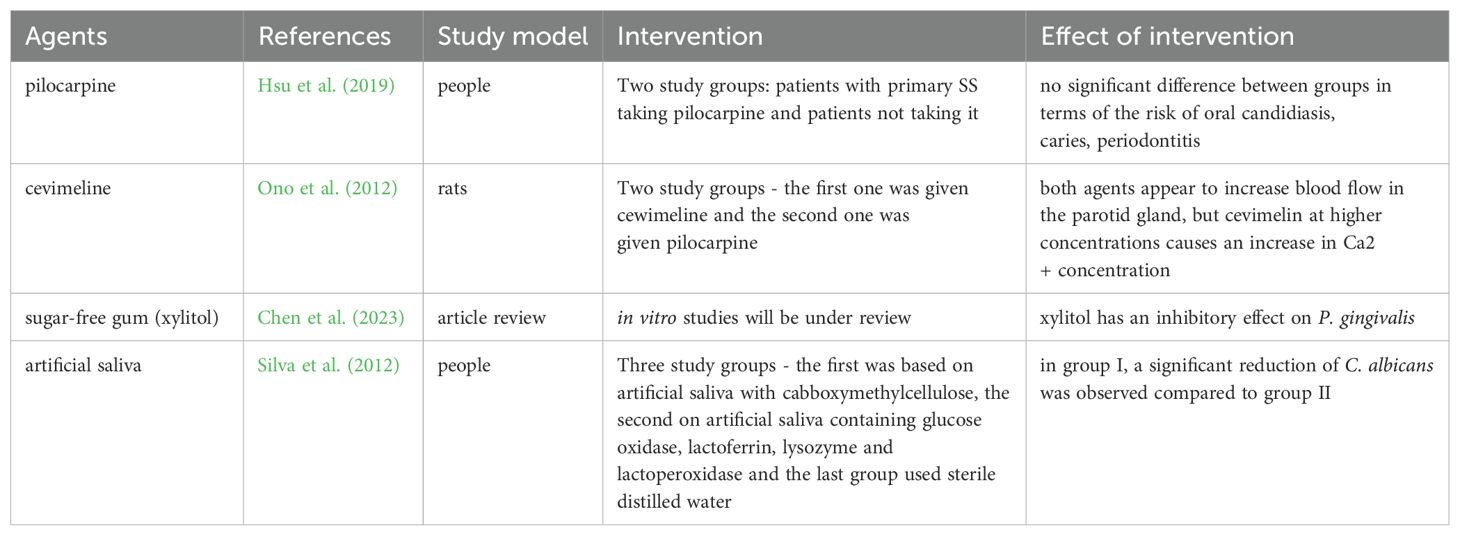
Table 2. Comparison of test results for individual anti-xerostomia agents against microorganisms.
Biological treatment
Biological treatment is an increasingly common method of treating various types of diseases. This also applies to Sjögren’s syndrome, but only under specific conditions (Marinho et al., 2023). For example, rituxinab (RTX) is not recommended for symptoms of dryness, but is recommended as a first-line drug in patients with SS combined with severe general symptoms and a risk of lymphoma (Marinho et al., 2023). It is also possible to recommend the use of RTX as a second-line therapy in cases where the drug has not been previously used and the disease has a severe general course (Marinho et al., 2023). Due to such restrictive use of biological drugs, it is difficult to determine the impact of RTX on the oral microbiome.
Conclusions
Agents used in the treatment of Sjögren’s syndrome, especially in case of xerostomia, have a real impact on the composition of the oral microbiome. However, some of them, such as pilocarpine, despite providing relief from dry mouth, do not significantly affect the risk of periodontopathy or tooth decay, even though they are considered one of the best means of treating this disease. It should be emphasized that this field is not well discovered. Further research is needed to determine the impact of individual agents, in particular cevimeline, on the oral microbiome. Research on artificial saliva is also necessary due to the general treatment of its effect on xerostomia, without taking into account the division into xerostomia caused by Sjögren’s syndrome, radiotherapy or chemotherapy. This is especially important in the context of the current discussion of similarities and differences in the oral microbiome resulting from the above-mentioned factors.
Author contributions
DM: Conceptualization, Writing – review & editing, Writing – original draft. RK: Conceptualization, Writing – original draft. NM: Conceptualization, Writing – original draft. MK: Writing – original draft. AB: Writing – original draft. MB: Writing – original draft. LK: Writing – original draft, Writing – review & editing. KK: Conceptualization, Writing – review & editing.
Funding
The author(s) declare that financial support was received for the research and/or publication of this article. This research was funded by the Ministry of Science and Higher Education, grant no. 2/566516/SPUB/SP/2023.
Acknowledgments
Acknowledgment for Martyna Wolańska and Jan Opalko for providing supporting fresh point of view of this topic.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
André, F., Böckle, B. C. (2022). Sjögren’s syndrome. J. Dtsch. Dermatol. Ges. 20, 980–1002. doi: 10.1111/ddg.14823
Baer, A. N., Walitt, B. (2018). Update on sjögren syndrome and other causes of sicca in older adults. Rheum. Dis. Clin. North Am. 44, 419–436. doi: 10.1016/j.rdc.2018.03.002
Baker, J. L., Bor, B., Agnello, M., Shi, W., He, X. (2017). Ecology of the oral microbiome: beyond bacteria. Trends Microbiol. 25, 362–374. doi: 10.1016/j.tim.2016.12.012
Bayetto, K., Logan, R. (2010). Sjögren’s syndrome: a review of aetiology, pathogenesis, diagnosis and management. Aust. Dental J. 55, 39–47. doi: 10.1111/j.1834-7819.2010.01197.x
Bikel, S., Valdez-Lara, A., Cornejo-Granados, F., Rico, K., Canizales-Quinteros, S., Soberón, X., et al. (2015). Combining metagenomics, metatranscriptomics and viromics to explore novel microbial interactions: towards a systems-level understanding of human microbiome. Comput. Struct. Biotechnol. J. 13, 390–401. doi: 10.1016/j.csbj.2015.06.001
Cartee, D. L., Maker, S., Dalonges, D., Manski, M. C. (2015). Sjögren’s syndrome: oral manifestations and treatment, a dental perspective. Am. Dental Hygienists’ Assoc. 89, 365–371.
Cevimeline. Available online at: https://go.drugbank.com/drugs/DB00185 (Accessed July 18, 2024).
Chen, S. Y., Delacruz, J., Kim, Y., Kingston, R., Purvis, L., Sharma, D. (2023). Effect of xylitol on Porphyromonas gingivalis: A systematic review. Clin. Exp. Dent. Res. 9, 265–275. doi: 10.1002/cre2.724
Cifuentes, M., Del-Barrio-Díaz, P., Vera-Kellet, C. (2018). Pilocarpine and artificial saliva for the treatment of xerostomia and xerophthalmia in Sjögren syndrome: a double-blind randomized controlled trial. Br. J. Dermatol. 179, 1056–1061. doi: 10.1111/bjd.16442
Dewhirst, F. E., Chen, T., Izard, J., Paster, B. J., Tanner, A. C. R., Yu, W.-H., et al. (2010). The human oral microbiome. J. Bacteriol. 192, 5002–5017. doi: 10.1128/JB.00542-10
Di Stefano, M., Polizzi, A., Santonocito, S., Romano, A., Lombardi, T., Isola, G. (2022). Impact of oral microbiome in periodontal health and periodontitis: A critical review on prevention and treatment. Int. J. Mol. Sci. 23, 5142. doi: 10.3390/ijms23095142
Fife, R. S., Chase, W. F., Dore, R. K., Wiesenhutter, C. W., Lockhart, P. B., Tindall, E., et al. (2002). Cevimeline for the treatment of xerostomia in patients with sjögren syndrome: A randomized trial. Arch. Internal Med. 162, 1293–1300. doi: 10.1001/archinte.162.11.1293
Ghannoum, M. A., Jurevic, R. J., Mukherjee, P. K., Cui, F., Sikaroodi, M., Naqvi, A., et al. (2010). Characterization of the oral fungal microbiome (mycobiome) in healthy individuals. PloS Pathog. 6, e1000713. doi: 10.1371/journal.ppat.1000713
Hellstein, J. W., Marek, C. L. (2019). Candidiasis: red and white manifestations in the oral cavity. Head Neck Pathol. 13, 25–32. doi: 10.1007/s12105-019-01004-6
Hsu, C.-Y., Hung, K.-C., Lin, M.-S., Ko, C.-H., Lin, Y.-S., Chen, T.-H., et al. (2019). The effect of pilocarpine on dental caries in patients with primary Sjögren’s syndrome: a database prospective cohort study. Arthritis Res. Ther. 21, 251. doi: 10.1186/s13075-019-2031-7
Huang, Dr. Y.-F., Weng, Mr. C.-T., Yang, D., Huang, D., Wei, D. (2019). Oral microbiota in xerostomia patients-a preliminary report. Oral. Surgery. Oral. Medicine. Oral. Pathol. Oral. Radiol. 128, e34–e35. doi: 10.1016/j.oooo.2019.02.058
Imfeld, T. N. (1994). Clinical caries studies with polyalcohols. A literature review. Schweiz Monatsschr. Zahnmed. 104, 941–945.
Janket, S.-J., Benwait, J., Isaac, P., Ackerson, L. K., Meurman, J. H. (2019). Oral and systemic effects of xylitol consumption. Caries. Res. 53, 491–501. doi: 10.1159/000499194
Kapourani, A., Kontogiannopoulos, K. N., Barmpalexis, P. (2022). A review on the role of pilocarpine on the management of xerostomia and the importance of the topical administration systems development. Pharmaceuticals 15, 762. doi: 10.3390/ph15060762
Kho, H.-S. (2014). Understanding of xerostomia and strategies for the development of artificial saliva. Chin. J. Dent. Res. 17, 75–83.
Kim, D., Jeong, Y. J., Lee, Y., Choi, J., Park, Y. M., Kwon, O. C., et al. (2022). Correlation between salivary microbiome of parotid glands and clinical features in primary sjögren’s syndrome and non-sjögren’s sicca subjects. Front. Immunol. 13. doi: 10.3389/fimmu.2022.874285
Könönen, E., Wade, W. G. (2015). Actinomyces and related organisms in human infections. Clin. Microbiol. Rev. 28, 419–442. doi: 10.1128/CMR.00100-14
Kozak, M., Pawlik, A. (2023). The role of the oral microbiome in the development of diseases. Int. J. Mol. Sci. 24, 5231. doi: 10.3390/ijms24065231
Krom, B. P., Kidwai, S., Ten Cate, J. M. (2014). Candida and other fungal species: forgotten players of healthy oral microbiota. J. Dent. Res. 93, 445–451. doi: 10.1177/0022034514521814
Lecuit, M., Eloit, M. (2013). The human virome: new tools and concepts. Trends Microbiol. 21, 510–515. doi: 10.1016/j.tim.2013.07.001
Lemos, J. A., Palmer, S. R., Zeng, L., Wen, Z. T., Kajfasz, J. K., Freires, I. A., et al. (2019). The biology of streptococcus mutans. Microbiol. Spectr. 7. doi: 10.1128/microbiolspec.GPP3-0051-2018
Li, X., Liu, Y., Yang, X., Li, C., Song, Z. (2022). The oral microbiota: community composition, influencing factors, pathogenesis, and interventions. Front. Microbiol. 13. doi: 10.3389/fmicb.2022.895537
Lynge Pedersen, A. M., Belstrøm, D. (2019). The role of natural salivary defences in maintaining a healthy oral microbiota. J. Dent. 80 Suppl 1, S3–S12. doi: 10.1016/j.jdent.2018.08.010
Maintaining the Oral Health of Patients With Sjögren’s Syndrome (2018). Dimensions of dental hygiene. Available online at: https://dimensionsofdentalhygiene.com/article/maintaining-oral-health-patients-sjogrens/ (Accessed July 11, 2024).
Marinho, A., Delgado Alves, J., Fortuna, J., Faria, R., Almeida, I., Alves, G., et al. (2023). Biological therapy in systemic lupus erythematosus, antiphospholipid syndrome, and Sjögren’s syndrome: evidence- and practice-based guidance. Front. Immunol. 14. doi: 10.3389/fimmu.2023.1117699
McIlvanna, E., Linden, G. J., Craig, S. G., Lundy, F. T., James, J. A. (2021). Fusobacterium nucleatum and oral cancer: a critical review. BMC Cancer 21, 1212. doi: 10.1186/s12885-021-08903-4
Musher, D. M. (1996).Haemophilus species. In: Medical Microbiology (Galveston (TX: University of Texas Medical Branch at Galveston). Available online at: http://www.ncbi.nlm.nih.gov/books/NBK8458/ (Accessed January 31, 2025).
Myers, C. (2015). Characterization Of Oral Microbiota In Xerostomic Versus Non-Xerostomic Volunteers And In Daily Samples Following Standard Oral Hygiene Practices (Wayne State University Theses). Available at: https://digitalcommons.wayne.edu/oa_theses/433.
Mystkowska, J., Car, H., Dąbrowski, J. R., Romanowska, J., Klekotka, M., Milewska, A. J. (2018). Artificial mucin-based saliva preparations - physicochemical and tribological properties. Oral. Health Prev. Dent. 16, 183–193. doi: 10.3290/j.ohpd.a40304
Nadig, S. D., Ashwathappa, D. T., Manjunath, M., Krishna, S., Annaji, A. G., Shivaprakash, P. K. (2017). A relationship between salivary flow rates and Candida counts in patients with xerostomia. J. Oral. Maxillofac. Pathol. 21, 316. doi: 10.4103/jomfp.JOMFP_231_16
Negrini, S., Emmi, G., Greco, M., Borro, M., Sardanelli, F., Murdaca, G., et al. (2022). Sjögren’s syndrome: a systemic autoimmune disease. Clin. Exp. Med. 22, 9–25. doi: 10.1007/s10238-021-00728-6
Niemirowicz-Laskowska, K., Mystkowska, J., Łysik, D., Chmielewska, S., Tokajuk, G., Misztalewska-Turkowicz, I., et al. (2020). Antimicrobial and physicochemical properties of artificial saliva formulations supplemented with core-shell magnetic nanoparticles. Int. J. Mol. Sci. 21, 1979. doi: 10.3390/ijms21061979
Ono, K., Inagaki, T., Iida, T., Wakasugi-Sato, N., Hosokawa, R., Inenaga, K. (2012). Distinct effects of cevimeline and pilocarpine on salivary mechanisms, cardiovascular response and thirst sensation in rats. Arch. Oral. Biol. 57, 421–428. doi: 10.1016/j.archoralbio.2011.09.013
Oza, S., Patel, K., Bhosale, S., Mitra, R., Gupta, R., Choudhary, D. (2018). To determine the effect of chewing gum containing xylitol and sorbitol on mutans streptococci and lactobacilli count in saliva, plaque, and gingival health and to compare the efficacy of chewing gums. J. Int. Soc. Prev. Community Dent. 8, 354–360. doi: 10.4103/jispcd.JISPCD_54_18
Rusthen, S., Kristoffersen, A. K., Young, A., Galtung, H. K., Petrovski, B.É., Palm, Ø., et al. (2019). Dysbiotic salivary microbiota in dry mouth and primary Sjögren’s syndrome patients. PloS One 14, e0218319. doi: 10.1371/journal.pone.0218319
Sedghi, L., DiMassa, V., Harrington, A., Lynch, S. V., Kapila, Y. L. (2021). The oral microbiome: Role of key organisms and complex networks in oral health and disease. Periodontol 2000 87, 107–131. doi: 10.1111/prd.12393
Sembler-Møller, M. L., Belstrøm, D., Locht, H., Enevold, C., Pedersen, A. M. L. (2019). Next-generation sequencing of whole saliva from patients with primary Sjögren’s syndrome and non-Sjögren’s sicca reveals comparable salivary microbiota. J. Oral. Microbiol. 11, 1660566. doi: 10.1080/20002297.2019.1660566
Silva, M. P., Chibebe Junior, J., Jorjão, A. L., MaChado, A. K., da, S., de, L. D., et al. (2012). Influence of artificial saliva in biofilm formation of Candida albicans in vitro. Braz. Oral. Res. 26, 24–28. doi: 10.1590/s1806-83242012000100005
Smego, R. A., Foglia, G. (1998). Actinomycosis. Clin. Infect. Dis. 26, 1255–1261. doi: 10.1086/516337
Stefanski, A.-L., Tomiak, C., Pleyer, U., Dietrich, T., Rüdiger Burmester, G., Dörner, T. (2017). The diagnosis and treatment of sjögren’s syndrome. Dtsch. Arztebl. Int. 114, 354–361. doi: 10.3238/arztebl.2017.0354
Struzycka, I. (2014). The oral microbiome in dental caries. Pol. J. Microbiol. 63, 127–135. doi: 10.33073/pjm-
Tian, Y., Yang, H., Liu, N., Li, Y., Chen, J. (2021). Advances in pathogenesis of sjögren’s syndrome. J. Immunol. Res. 2021, 5928232. doi: 10.1155/2021/5928232
Tsigalou, C., Stavropoulou, E., Bezirtzoglou, E. (2018). Current insights in microbiome shifts in sjogren’s syndrome and possible therapeutic interventions. Front. Immunol. 9. doi: 10.3389/fimmu.2018.01106
van der Meulen, T. A., Harmsen, H. J. M., Bootsma, H., Liefers, S. C., Vich Vila, A., Zhernakova, A., et al. (2018a). Dysbiosis of the buccal mucosa microbiome in primary Sjögren’s syndrome patients. Rheumatol. (Oxford). 57, 2225–2234. doi: 10.1093/rheumatology/key215
van der Meulen, T. A., Harmsen, H. J. M., Bootsma, H., Liefers, S. C., Vich Vila, A., Zhernakova, A., et al. (2018b). Reduced salivary secretion contributes more to changes in the oral microbiome of patients with primary Sjögren’s syndrome than underlying disease. Ann. Rheum. Dis. 77, 1542–1544. doi: 10.1136/annrheumdis-2018-213026
Verma, D., Garg, P. K., Dubey, A. K. (2018). Insights into the human oral microbiome. Arch. Microbiol. 200, 525–540. doi: 10.1007/s00203-018-1505-3
Watanabe, M., Yamada, C., Komagata, Y., Kikuchi, H., Hosono, H., Itagaki, F. (2018). New low-dose liquid pilocarpine formulation for treating dry mouth in Sjögren’s syndrome: clinical efficacy, symptom relief, and improvement in quality of life. J. Pharm. Health Care Sci. 4, 4. doi: 10.1186/s40780-018-0099-x
Wiseman, L. R., Faulds, D. (1995). Oral pilocarpine: A review of its pharmacological properties and clinical potential in xerostomia. Drugs 49, 143–155. doi: 10.2165/00003495-199549010-00010
Yousefi, L., Leylabadlo, H. E., Pourlak, T., Eslami, H., Taghizadeh, S., Ganbarov, K., et al. (2020). Oral spirochetes: Pathogenic mechanisms in periodontal disease. Microb. Pathog. 144, 104193. doi: 10.1016/j.micpath.2020.104193
Zamani, B., Golkar, H. R., Farshbaf, S., Emadi-Baygi, M., Tajabadi-Ebrahimi, M., Jafari, P., et al. (2016). Clinical and metabolic response to probiotic supplementation in patients with rheumatoid arthritis: a randomized, double-blind, placebo-controlled trial. Int. J. Rheum. Dis. 19, 869–879. doi: 10.1111/1756-185X.12888
Zeron, P. B., Retamozo, S., Bové, A., Kostov, B. A., Sisó, A., Ramos-Casals, M. (2013). Diagnosis of liver involvement in primary sjögren syndrome. J. Clin. Transl. Hepatol. 1, 94–102. doi: 10.14218/JCTH.2013.00011
Zhou, L.-J., Chen, B.-Y., Li, Y.-L., Duan, S.-Z. (2023). Oral microbiome and systemic diseases. Sichuan. Da. Xue. Xue. Bao. Yi. Xue. Ban. 54, 1–6. doi: 10.12182/20230160504
Keywords: Sjögren’s syndrome, oral microbiome, xerostomia, pilocarpine, cevimeline, artificial saliva
Citation: Muszyński D, Kucharski R, Marek-Trzonkowska N, Kalinowska M, Brzóska A, Bolcewicz M, Kalinowski L and Kaźmierczak-Siedlecka K (2025) Treatment of xerostomia in Sjögren’s syndrome – what effect does it have on the oral microbiome? Front. Cell. Infect. Microbiol. 15:1484951. doi: 10.3389/fcimb.2025.1484951
Received: 22 August 2024; Accepted: 10 March 2025;
Published: 14 April 2025.
Edited by:
Jacek Tabarkiewicz, University of Rzeszow, PolandReviewed by:
Preethi Prajod, National Dental Centre of Singapore, SingaporeAgnieszka Bojarska-Junak, Medical University of Lublin, Poland
Copyright © 2025 Muszyński, Kucharski, Marek-Trzonkowska, Kalinowska, Brzóska, Bolcewicz, Kalinowski and Kaźmierczak-Siedlecka. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Leszek Kalinowski, bGVzemVrLmthbGlub3dza2lAZ3VtZWQuZWR1LnBs; Karolina Kaźmierczak-Siedlecka, bGVva2FkaWFAZ3VtZWQuZWR1LnBs