
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
BRIEF RESEARCH REPORT article
Front. Cell. Infect. Microbiol. , 21 January 2025
Sec. Clinical Infectious Diseases
Volume 14 - 2024 | https://doi.org/10.3389/fcimb.2024.1513408
This article is part of the Research Topic Perspectives in Clinical Infectious Diseases: 2024/2025 View all articles
 Evelyn Kramme1*†
Evelyn Kramme1*† Nadja Käding2,3†
Nadja Käding2,3† Tobias Graf4
Tobias Graf4 Karolin Schmoll4Heidi Linnen5Katharina Nagel2Esther Grote-Levi2
Karolin Schmoll4Heidi Linnen5Katharina Nagel2Esther Grote-Levi2 Susanne Hauswaldt2
Susanne Hauswaldt2 Dennis Nurjadi2,3
Dennis Nurjadi2,3 Jan Rupp1,2,3
Jan Rupp1,2,3Objectives: To evaluate the impact of rapid diagnostic testing (RDT) combined with immediate infectious disease (ID) consultation on the treatment of septic patients with positive blood cultures in intensive care units in a setting without 24/7 service.
Methods: Adult ICU patients in a tertiary care hospital with positive blood cultures were included from January 2019 to December 2020. The control group underwent routine laboratory testing, and for the intervention group, RDT was applied with immediate ID consultation.
Results: In 77 out of the 91 patients in the intervention group, the pathogen was identified by RDT. Regarding antimicrobial susceptibility testing (AST), genotypic testing (ePlex®) was successful for Gram-positive cocci, but inadequate for Gram-negative rods. Phenotypic resistance testing with the Accelerate PhenoTest® took too long to be successfully integrated into the intervention. Adaptation of empirical antibiotic therapy was recommended for 72.7% of the patients. Adherence to the ID consultation post-RDT results was high at 82.3%. In the control group, adaptation of the initial antibiotic therapy would have been recommended for 81.8% of patients, if the species identification had been available. Overall adherence to the local antibiotic therapy guideline for sepsis was significantly lower in the control than in the intervention group (27.8% versus 89.3%, p<0.001).
Conclusion: Integration of an RDT system in the microbiological workflow for septic patients in ICU combined with a standardized ID intervention led to a significantly higher percentage of adequate antimicrobial treatment and greater adherence to local antibiotic therapy recommendations, even in a setting where 24/7 service is not available.
Sepsis is associated with high morbidity and mortality. Every hour of treatment delay decreases the survival rate by 7.6% (Kumar et al., 2006). The need for early appropriate antimicrobial therapy leads to the use of broad-spectrum antibiotics. A commitment to de-escalation is essential to reduce side effects in patients (Niederman et al., 2021) (e.g., microbiome, Clostridioides difficile infection) (Ravi et al., 2019) and the development of resistance. Early adaptation to targeted therapy is facilitated by rapid pathogen identification and timely infectious disease (ID) counseling (Neuner et al., 2016) in patients with sepsis.
Molecular analysis techniques, representing a combination of bacterial culture and molecular diagnostics, are on the rise (Banerjee et al., 2015). Rapid molecular identification of pathogens (< 1.5 h) and accelerated phenotypic antimicrobial susceptibility testing (AST) (< 7 h) led to comparable results to culture methods in 24-36 h. The cost-effectiveness of rapid diagnostics has been shown for bloodstream infections (BSIs) in combination with antimicrobial stewardship (AMS) (Pliakos et al., 2018). In both Gram-positive and Gram-negative BSIs, the introduction of rapid diagnostic tests (RDTs) and AMS reduced the time to targeted antibiotic therapy (Beal et al., 2015).
In Gram-negative BSIs, the proportion of optimally treated patients increased, especially among those who received ID consultations (Claeys et al., 2020). Yet 24/7 laboratory service and ID consultation are rarely available in German hospitals. Evidence supporting the clinical impact of rapid identification and AST is limited and controversial for sepsis patients with bacteremia.
The aim of this study was to evaluate the integration of an RDT system into the microbiological workflow for septic patients with blood culture results. Our goal was the timely achievement of targeted therapy to improve treatment outcomes and avoid the collateral damage of a broad-spectrum therapy even though no 24/7 service was available.
We conducted a prospective cohort study of patients with positive blood cultures and sepsis in two ICUs in the tertiary care University Hospital of Schleswig-Holstein in Lübeck between August 2018 and December 2020. In the intervention group patients’ blood cultures underwent RDT and immediate ID consultation. The standard of care group underwent conventional microbiological diagnostics (Figure 1). The study was approved by the local ethics committee (University of Lübeck, Az 18-261).
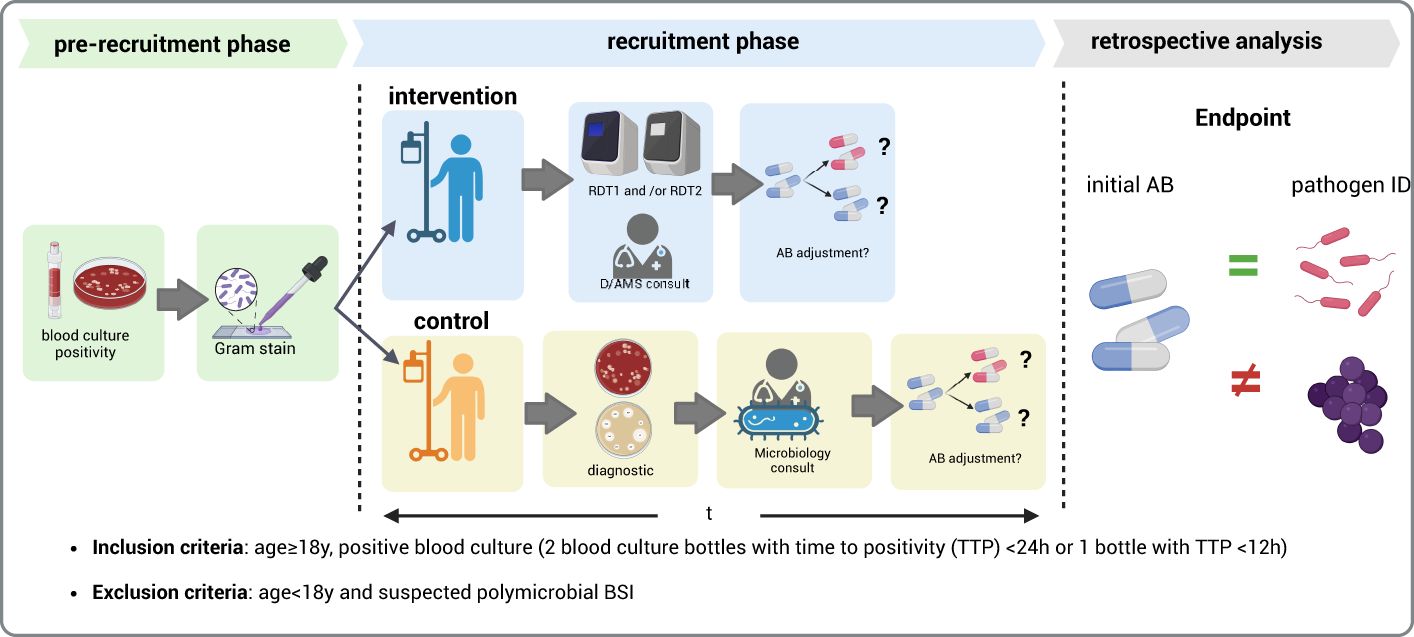
Figure 1. Overview of study design. Comparison of rapid diagnostic testing (RDT) using ePlex® (RDT1) and Accelerate® (RDT2) on the time to effective therapy as defined by the pathogen spectrum covered by the initial antibiotic therapy. (Figure created with Biorender.
Microbiological, clinical, laboratory, and treatment-related data were collected from the index blood cultures. Patients were stratified into the intervention and standard of care study arms upon the detection of blood culture positivity during routine microbiological diagnostics. In the intervention group, RDT was conducted using ePlex® and Accelerate® on the basis of Gram staining. The results were conveyed to the attending physician by the infectious disease/antimicrobial stewardship (ID/AMS) consult team. If required according to the RDT results, adjustments to antibiotic (AB) therapy were recommended (Supplementary Table S1). In the standard of care group, the microbiology specialist reported the Gram staining results to the attending physician and suggested antibiotic adjustments. Adherence to the recommendations for AB adjustment was assessed upon completion of the study through a review of patient charts and microbiology results (Figure 1).
Routine laboratory diagnostic procedures were conducted according to local microbiology laboratory protocols using the BacT/Alert (bioMérieux, Nürtingen, Germany) automated system. The results of the Gram stains were immediately communicated to the attending physicians for both the control and intervention group by the clinical microbiology specialist. Species identification was performed using MALDI-TOF mass spectrometry (Bruker Daltonics, Germany). AST was performed using a VITEK®2 (bioMérieux, Germany) and was interpreted according to the valid EUCAST clinical breakpoints of the respective year (www.eucast.org/ast_of_bacteria v 8.1, v 9.0, v 10.0).
Rapid diagnostic for species identification and AST was performed with the Accelerate® PhenoTest™ BC kit (Accelerate Diagnostic, Tucson, Arizona) and the ePlex® system (GenMark Diagnostics, Carlsbad, CA) according to the manufacturer’s instructions. The Accelerate Pheno® system is based on microbial identification by fluorescence in situ hybridization (FISH) combined with AST assessments (BC kit), while ePlex® is based on a multiplex microarray assay. Both Accelerate® and ePlex® testing were simultaneously started following the results of the Gram staining if the inclusion criteria were met.
A hospital-wide AMS program has been implemented at the hospital since 2011, combining treatment recommendations based on resistance data and review of and feedback on antimicrobial treatment on weekly ward rounds. Recommendations following blood culture results were not routinely performed. In this study, pathogen-related treatment recommendations were additionally implemented. After revising RDT results concerning plausibility, the ID consultant advised the attending ICU physician on therapy adaptation. Laboratory and clinical staff were trained on the intervention.
The adherence to the recommendation for AB adjustment was reviewed by AMS team members based on patient charts and microbiology results.
The distribution of sociodemographic and clinical variables was analyzed based on the diagnostic methods used for bloodstream infections. In the intervention group, rapid diagnostic methods (ePlex® and/or Accelerate Pheno®) were employed, while the control group utilized conventional blood culture. Differences between the two groups were assessed under the null hypothesis (H₀) that no significant differences exist in the distribution of these variables. Appropriate statistical tests were applied: the chi-squared test for categorical (dichotomous) variables and the Wilcoxon Rank-Sum test for continuous variables that were not normally distributed, as indicated in the footnotes of Table 1. The normal distribution of continuous variables was determined using the Shapiro–Wilks test for normality.

Table 1. Patient demographics, clinical parameters, comorbidities, and outcomes.
We used univariable and multivariable logistic regressions to calculate the likelihood of lethal outcome using the variables sex, chronic obstructive pulmonary disease (COPD), and thrombocyte count as potential confounders as indicated by the p-values of the chi-squared test to calculate the odds ratio and the 95% confidence interval in Table 1. Statistical analyses were performed using STATA 17 (Stata Corp, USA). P-values for categorical values were calculated using the chi-squared test. P-values of <0.05 were considered statistically significant.
Overall, 91 patients were recruited for the intervention group and 44 for the standard of care group. In the intervention group, 82 showed a monomicrobial culture and were included in the microbiological analysis. Furthermore, 77 of these 82 (94%) patients had RDT results with either the ePlex® or Accelerate PhenoTest® or both (Supplementary Figure 1B). For 48 out of the 77 (62.3%) patients, results from both RDT systems were obtained, in contrast to 23/77 (29.9%) from the ePlex® system only and 6/77 (7.8%) from the Accelerate PhenoTest® only. The reasons for the unavailability of results were either that RDT was not performed due to logistics reasons (ePlex® 4/82, Accelerate® 14/82), that the pathogen identified in the blood culture was not included in the test panel (ePlex® 3/82, Accelerate® 3/82), or that the pathogen was not identified (ePlex® 4/82, Accelerate® 10/82). There was one incorrect species identification with the Accelerate® system (coagulase-negative staphylococci instead of S. pyogenes). All results from the ePlex® system were correct compared to the gold standard (routine cultural diagnostics). The baseline characteristics of the patients included in the analysis are summarized in Table 1. The species distribution identified by culture in both study arms is displayed in Supplementary Figure 1A.
Identification results of both RDT systems and molecular resistance markers of the ePlex® system were available approximately 2 hours after the Gram stain. For species identification, both RDT systems would be suitable for delivering timely results to optimize ID/AMS consultations. While the multidrug-resistant (MDR) phenotype of staphylococci and enterococci could be reliably predicted using the detection of van or mec genes, genotypic-phenotypic AST correlation may not be accurate due to the diverse resistance mechanisms in Gram-negative rods. Furthermore, phenotypic resistance testing with the Accelerate PhenoTest® was too time-consuming (>7h) to be successfully integrated into our intervention.
Thirteen patients developed BSIs caused by MDR pathogens: 10 of 77 (13.0%) in the intervention group and 3 of 44 (6.8%) in the standard-of-care group. The MDR pathogens included vancomycin-resistant Enterococcus (VRE), methicillin-resistant Staphylococcus aureus (MRSA), and third-generation cephalosporin-resistant Enterobacterales (3GCR-E). Based on the blood culture results, the initial/empirical broad-spectrum antibiotic therapy covered the pathogen spectrum in 63.6% (49/77) and 72.7% (32/44) in the intervention group and standard of care group, respectively. Adaptation to targeted antibiotic therapy was recommended in 56 of 77 cases (72.7%) based on the RDT result. De-escalation was performed in 42.8% (33/77) of the intervention group versus 22.7% (10/44) of the standard of care group. Adherence to the ID consultation postRDT results was very high, with 82.3% (50/56). In the standard of care group, an adaptation of the initial antibiotic therapy would have been recommended for 36/44 (81.8%) patients, if the species identification had been available (Supplementary Figure 1B). However, the adherence to local antibiotic therapy recommendation for sepsis (Supplementary Table S1) was significantly lower than in the intervention group (10/36; 27.8% versus 50/56; 89.3%, p<0.001, chi-squared test, H0=no difference between the two groups). There were no significant effects on mortality, even after adjusting for potential confounders (sex, COPD and thrombocyte count, odds ratio=1.2, 95% confidence interval 0.6-2.7, p=0.6).
Although the introduction of RDT in most studies leads to decreased time to effective therapy (Neuner et al., 2016), a review demonstrated that only RDT with antimicrobial stewardship programs and ID interventions decreased the mortality in both Gram-positive and Gram-negative BSIs. Although we could not show an effect on mortality due to a small number of patients with several comorbidities (Table 1), the length of ICU stay was reduced both in all and in non-fatal cases. Another important aspect of therapy adaptation is to reduce the resistance pressure of broad-spectrum therapy (Niederman et al., 2021). In our intervention group, de-escalation was performed more frequently than in our standard of care group. RDT combined with a subsequent ID consultation led to a reduction of the length of stay and to a better adherence to therapy recommendations and local therapy guidelines. This corresponds to the results of a large study showing significantly more frequent de-escalation following a rapid multiplex polymerase chain reaction-based blood culture identification panel combined with automatic ID consults for BSIs (Timbrook et al., 2017; Britt et al., 2023). Thus, implementation of rapid diagnostics should in general be conducted with an ID consultation to achieve the greatest benefit.
Our study has limitations. The assessment of the clinical impact of RDT/ID consultation on the mortality or clinical outcome was deemed inappropriate due to the small sample size and confounders, e.g. age >60 years and comorbidities, which significantly impact recovery and survival (Fay et al., 2020). We assume that patients with good prospects of recovery benefit most from RDT/ID consultation. However, staff availability in an ICU setting impacts timely ID consultation, a main requirement for such a study. Nonetheless, even with a relatively small sample size and simple study design, we could demonstrate that better integration of microbiological diagnostics with an ID intervention led to significantly greater adherence to antibiotic therapy recommendations and local guidelines.
Our study indicates that weekly AMS rounds and standard diagnostic stewardship alone are insufficient to ensure adequate therapy adjustments in septic patients. Combining diagnostic stewardship with an ID consultation seems to be an important requirement for high compliance with therapy recommendations for targeted therapy in septic patients.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding author.
The studies involving humans were approved by Ethikkommission der Universität zu Lübeck Ratzeburger Allee 160, Haus 70, 23562 Lübeck, ethikkommission(at)uni-luebeck(dot)de. The studies were conducted in accordance with the local legislation and institutional requirements. Written informed consent for participation in this study was provided by the participants’ legal guardians/next of kin.
EK: Conceptualization, Project administration, Supervision, Writing – original draft, Writing – review & editing. NK: Conceptualization, Data curation, Methodology, Supervision, Writing – original draft. TG: Investigation, Validation, Writing – review & editing. KS: Investigation, Validation, Writing – review & editing. HL: Investigation, Validation, Writing – review & editing. KN: Data curation, Formal analysis, Investigation, Writing – review & editing. EG: Data curation, Investigation, Writing – review & editing. SH: Conceptualization, Data curation, Formal analysis, Investigation, Methodology, Project administration, Validation, Writing – original draft, Writing – review & editing. DN: Conceptualization, Formal analysis, Software, Supervision, Visualization, Writing – original draft, Writing – review & editing. JR: Conceptualization, Project administration, Resources, Supervision, Writing – original draft, Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
We thank the ICU teams including Prof. Maria Deja, Marion Hansen and Henning Braasch, the microbiological laboratory team including Simone Weikert-Asbeck and Dirk Friedrich, the MD student Lisa Höltig and the Infectious Diseases consultation team including Alexander Mischnik. The authors thank Accelerate Diagnostics and GenMark Dx for providing devices and supplied panels for testing as well as for their technical support.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The author(s) declare that no Generative AI was used in the creation of this manuscript.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcimb.2024.1513408/full#supplementary-material
Banerjee, R., Teng, C. B., Cunningham, S. A., Ihde, S. M., Steckelberg, J. M., Moriarty, J. P., et al. (2015). Randomized trial of rapid multiplex polymerase chain reaction-based blood culture identification and susceptibility testing. Clin. Infect. Dis. 61, 1071–1080. doi: 10.1093/cid/civ447
Beal, S. G., Thomas, C., Dhiman, N., Nguyen, D., Qin, H., Hawkins, J. M., et al. (2015). Antibiotic utilization improvement with the Nanosphere Verigene Gram-Positive Blood Culture assay. Proc. (Bayl Univ Med. Cent) 28, 139–1438. doi: 10.1080/08998280.2015.11929214
Claeys, K. C., Heil, E. L., Hitchcock, S.., Johnson, K. J., Leekha, S.. Management of Gram-Negative Bloodstream Infections in the Era of Rapid Diagnostic Testing: Impact With and Without Antibiotic Stewardship. Open Forum Infect Dis. (2020) 7 (10), ofaa427. doi: 10.1093/ofid/ofaa427
Britt, N. S., Khader, K., He, T., Willson, T. M., Effiong, A., Timbrook, T. T., et al. (2023). Examining the clinical impact of rapid multiplex polymerase chain reaction-based diagnostic testing for bloodstream infections in a national cohort of the Veterans Health Administration. Pharmacotherapy 43, 24–34. doi: 10.1002/phar.2747
Fay, K., Sapiano, M. R. P., Gokhale, R., Dantes, R., Thompson, N., Katz, D. E., et al. (2020). Assessment of health care exposures and outcomes in adult patients with sepsis and septic shock. JAMA Netw. Open 3, e206004. doi: 10.1001/jamanetworkopen.2020.6004
Kumar, A., Roberts, D., Wood, K. E., Light, B., Parrillo, J. E., Sharma, S., et al. (2006). Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit. Care Med. 34, 1589–1596. doi: 10.1097/01.CCM.0000217961.75225.E9
Neuner, E. A., Pallotta, A. M., Lam, S. W. (2016). Experience with rapid microarray-based diagnostic technology and antimicrobial stewardship for patients with gram-positive bacteremia. Infect. Control Hosp Epidemiol 37, 1361–1366. doi: 10.1017/ice.2016
Niederman, M. S., Baron, R. M., Bouadma, L., Calandra, T., Daneman, N., DeWaele, J., et al. (2021). Initial antimicrobial management of sepsis. Crit. Care 25, 307. doi: 10.1186/s13054-021-03736-w
Pliakos, E. E., Andreatos, N., Shehadeh, F., Ziakas, P. D., Mylonakis, E. (2018). The cost-effectiveness of rapid diagnostic testing for the diagnosis of bloodstream infections with or without antimicrobial stewardship. Clin. Microbiol. Rev. 31, e00095–e00017. doi: 10.1128/CMR.00095-17
Ravi, A., Halstead, F. D., Bamford, A., Casey, A., Thomson, N. M., van Schaik, W. (2019). Loss of microbial diversity and pathogen domination of the gut microbiota in critically ill patients. bioRxiv 9, 151–236. doi: 10.1099/mgen.0.000293
Keywords: sepsis, rapid diagnostic testing, infectious diseases consultation, adequate antibiotic therapy, blood stream infection (BSI), antimicrobial stewardship (AMS)
Citation: Kramme E, Käding N, Graf T, Schmoll K, Linnen H, Nagel K, Grote-Levi E, Hauswaldt S, Nurjadi D and Rupp J (2025) Rapid diagnostic testing combined with an immediate infectious disease consultation increases the rate of septic intensive care unit patients on targeted antibiotic therapy. Front. Cell. Infect. Microbiol. 14:1513408. doi: 10.3389/fcimb.2024.1513408
Received: 18 October 2024; Accepted: 20 December 2024;
Published: 21 January 2025.
Edited by:
Lorena V. N. Oliveira, University of Massachusetts Medical School, United StatesReviewed by:
Marie Louise Guadalupe Attwood, North Bristol NHS Trust, United KingdomCopyright © 2025 Kramme, Käding, Graf, Schmoll, Linnen, Nagel, Grote-Levi, Hauswaldt, Nurjadi and Rupp. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Evelyn Kramme, RXZlbHluLktyYW1tZUB1a3NoLmRl
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.