 Jane Shi
Jane Shi Helen V. Danesh-Meyer
Helen V. Danesh-Meyer
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
MINI REVIEW article
Front. Cell. Infect. Microbiol. , 17 January 2024
Sec. Virus and Host
Volume 14 - 2024 | https://doi.org/10.3389/fcimb.2024.1345683
This article is part of the Research Topic COVID-19 and Vaccination-Associated Ocular Complications View all 7 articles
Background: It has become increasingly clear that the severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) can affect most organs in the human body, including the neurologic and ophthalmic systems. Vaccination campaigns have been developed at rapid pace around the world to protect the population from the fast-mutating virus. This review seeks to summarise current knowledge of the neuro-ophthalmic manifestations of both COVID-19 infection and vaccination.
Evidence acquisition: Electronic searches for published literature were conducted using EMBASE and MEDLINE on the 30th of July 2023. The search strategy comprised of controlled vocabulary and free-text synonyms for the following terms in various combinations: “coronavirus, COVID-19, SARS-CoV-2, 2019-nCoV, vaccination, vaccine, immunisation and neuro-ophthalmology”. No time range limits were set for the literature search. Published English abstracts for articles written in a different language were screened if available.
Results: A total of 54 case reports and case series were selected for use in the final report. 34 articles documenting neuro-ophthalmic manifestations following COVID-19 infection and 20 articles with neuro-ophthalmic complications following COVID-19 vaccination were included, comprising of 79 patients in total. The most commonly occurring condition was optic neuritis, with 25 cases following COVID-19 infection and 27 cases following vaccination against COVID-19.
Conclusions: The various COVID-19 vaccines that are currently available are part of the global effort to protect the most vulnerable of the human population. The incidence of neuro-ophthalmic consequences following infection with COVID-19 is hundred-folds higher and associated with more harrowing systemic effects than vaccination against the virus.
SARS-CoV-2 took the world by storm at the dawn of 2020. The novel single-stranded RNA beta coronavirus affected the health and livelihoods of millions across the globe on a scale only encountered once approximately every 100 years (Wesselingh and Wesselingh, 2023). There is currently a plethora of case reports and case series of neuro-ophthalmic manifestations of COVID-19 and its vaccine counterparts (Luís et al., 2020; Betsch and Freund, 2021; Tisdale et al., 2021). As the end of this pandemic is reached, this review seeks to summarise the current knowledge of neuro-ophthalmic manifestations of both COVID-19 infection and vaccination.
Electronic searches for published literature were conducted using EMBASE and MEDLINE on the 30th of July 2023, see Figure 1. The search strategy comprised of controlled vocabulary and free-text synonyms for the following terms in various combinations: “coronavirus, COVID-19, SARS- CoV-2, 2019-nCoV, vaccination, vaccine, immunisation and neuro-ophthalmology”. No time range limits were set for the literature search. Published English abstracts for articles written in a different language were screened if available.
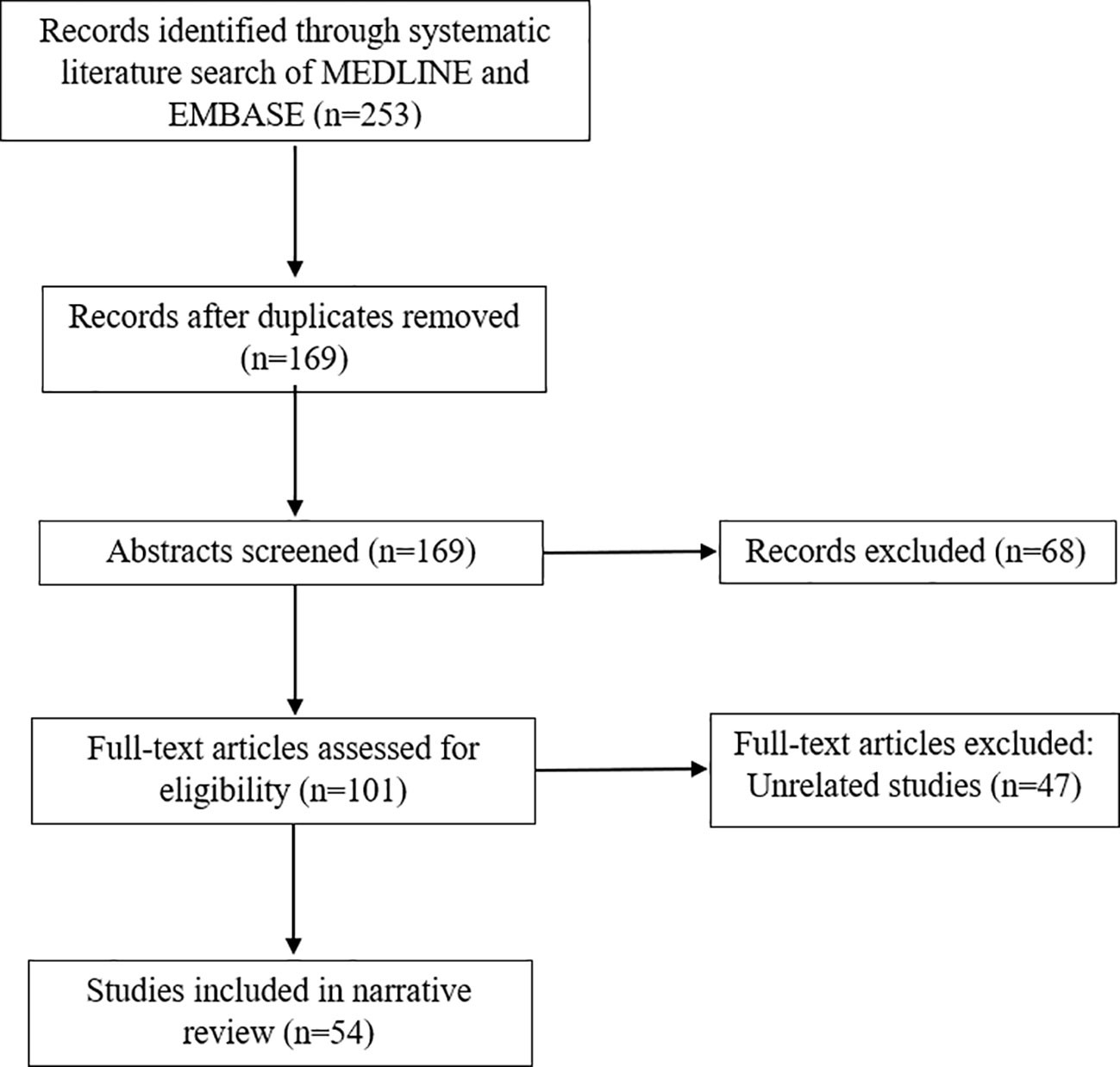
Figure 1 Summary of literature search.
There has been a wide spectrum of neuro-ophthalmic manifestations of COVID-19 infection reported in the literature. Of the reports surveyed, there were 25 cases of newly diagnosed optic neuritis (16 unilateral, 9 bilateral), 10 of which were seropositive for MOG IgG, one demonstrated MOG positivity in the cerebrospinal fluid (CSF), and one seropositive for AQP4 IgG indicative of neuromyelitis optica spectrum disorder (NMOSD), 14 cases of idiopathic intracranial hypertension (also known as pseudotumour cerebri), three cases of posterior reversible encephalopathy syndrome, one case of myasthenia gravis, one case of occipital stroke, one case of orbital inflammation and optic perineuritis, one case of infarction of left optic nerve due to thrombosis of left internal carotid artery, one case of papillophlebitis, one case of acute macular neuroretinopathy, one case of non-arteritic anterior ischemic optic neuropathy.
The timing of onset of visual symptoms ranged from being concurrent with active COVID-19 infection to seven months following infection.
Both unilateral and bilateral presentations of optic neuritis have been reported at higher frequencies since the onset of the COVID-19 pandemic (Przybek-Skrzypecka et al., 2022). Of the 25 cases included in this review, the average time to symptomatic onset following infection is 32.8 days (range 0 – 210 days). All 25 cases with new-onset optic neuritis following or concurrent with COVID-19 infection had at least one MRI throughout their disease (Supplementary Table 1). A suspicion of multiple sclerosis (MS) was initially documented in seven cases, but further evaluation either through neuroimaging or lumbar puncture did not confirm a diagnosis of MS. Furthermore, 11 of the cases of optic neuritis demonstrated antibody positivity to myelin oligodendrocyte glycoprotein and one case was seropositive for aquaporin-4 (AQP4). High dose intravenous Methylprednisolone (IVMP) followed by oral steroid taper was administered in all patients except three [one of whom was suspected for having Vogt-Koyanagi-Harada disease due to concurrent severe intraocular inflammation (Benito-Pascual et al., 2020) and one in whom treatment was not mentioned (Borrego-Sanz et al., 2021)]. The mean visual acuity at presentation was 6/30 and mean visual acuity after treatment was 6/9. Visual acuity remained poor in one case despite prompt initiation of IVMP (Rodríguez-Rodríguez et al., 2021). Vision was also poor in another case, however IVMP was not promptly initiated and the patient was instead treated with topical and ocular corticosteroids due to concurrent panuveitis (François et al., 2021). Visual outcomes were not mentioned in three cases.
A subset of COVD-19 related optic neuritis demonstrated myelin oligodendrocyte glycoprotein antibody positivity. MOG antibody disease is an inflammatory central nervous system (CNS) disorder that manifests as unilateral or bilateral optic neuritis, with or without multi-focal demyelination and inflammation of the brain and spinal cord.
Ten of the patients in this review were seropositive for MOG IgG either concurrent with or following COVID-19 infection, with one further case demonstrating MOG positivity through CSF analysis. Seven cases were unilateral, four bilateral. On neuroimaging, eight cases had signal abnormalities of the optic nerve, four had additional lesions of the spinal cord, and two cases had lesions in the brain parenchyma. All 11 patients received IVMP, with two cases further requiring plasma exchange (PLEX) (Feizi et al., 2022; Johnsson et al., 2022). Mean visual acuity at presentation of the MOG IgG positive cohort was 6/19, which improved to a mean visual acuity of 6/6 following treatment.
There were 14 cases of newly diagnosed IIH identified in this review. The mean time of onset following COVID-19 infection is 8.7 days (range 0 to 42 days). Eleven of the 14 cases had neuroimaging with normal brain parenchyma, one further case was an 11-year-old girl initially diagnosed with multisystem inflammatory syndrome prior to IIH who had hyperintensities on FLAIR/T2 sequences and restricted diffusion in the splenium of the corpus callosum on MRI (Sofuoğlu et al., 2021). Neuroimaging was not mentioned in two cases. 13 of the 14 cases of IIH described in this review underwent a lumbar puncture with elevated opening pressure and normal CSF constituents, which fulfils the revised diagnostic criteria of IIH in adults and children (Friedman et al., 2013). The remaining case declined a lumbar puncture and was diagnosed based on clinical findings and neuroimaging.
Both generalised (Restivo et al., 2020) and ocular MG have been reported to be triggered by COVID-19 (Sriwastava et al., 2021). One case described in this review had a confirmed diagnosis of ocular MG through both positive acetylcholine receptor (AChR) antibodies and single fibre electromyography (EMG) (De Giglio et al., 2023). Another case of ocular MG concurrent with COVID-19 reported by Sriwastava et al. also demonstrated AChR antibody positivity and EMG findings consistent with a neuromuscular transmission deficit (Sriwastava et al., 2021). Three further cases were described by Restivo et. al, two of whom also reported systemic in addition to ocular symptoms of MG including general diplopia, ptosis, muscular fatigability, hypophonia, and dysphagia concurrent with COVID-19 and had their diagnosis confirmed through positive AChR antibody titres and EMG findings of postsynaptic deficit of neuromuscular transmission (Restivo et al., 2020).
A series of three cases of PRES were described in this review, with mean time of symptomatic onset being 20 days (range 9 to 39 days) following the development of COVID-19 symptoms (Hixon et al., 2021). All three cases presented with seizure-like activity, with two demonstrating visual field deficits on examination. All three cases had neuroimaging which showed T2/FLAIR hyperintensities spread throughout the brain parenchyma, two of which did not have corresponding diffusion restriction on diffusion-weighted imaging. Humphrey visual field (HVF) testing at six-month follow-up revealed a persistent left homonymous hemianopia for one patient and was declined by the other patient. Cerebrospinal fluid testing was not completed in all three patients.
Two large population studies have proposed that COVID-19 increases the risks of developing neurological diseases. The first study utilised the US department of Veteran Affairs records to create a cohort of 154,068 patients with COVID-19, 5,638,795 contemporary controls and 5,859,621 historical controls (Xu et al., 2022). The burden of neurological complications was calculated to be the number of additional cases per 1000 persons at 12 months. They found that the hazard ratio (HR) of any neurologic sequelae in the post-acute phase of COVID-19 was 1.42 (95% confidence intervals 1.38, 1.47) and burden 70.69 (95% confidence interval 63.54, 78.01) additional sequelae per 1000 persons at 12 months. They investigated the risks of developing neurological disorders at 12 months following COVID-19 infection, and found an increased risk of a multitude of disorders including ischemic stroke [HR 1.50 (1.41, 1.61); burden 3.40 (2.75, 4.09)], haemorrhagic stroke [HR 2.19 (1.29, 5.62); burden 0.21 (0.11, 0.35)] cognition and memory disorders [HR 1.77 (1.68, 1.85); burden 10.07 (9.00, 11.20)], extrapyramidal movement disorders such as Parkinson-like disease [HR 1.50 (1.28, 1.7s; burden 0.89 (0.50, 1.34)], Guillain-Barré syndrome [HR 2.16 (1.40, 3.35); burden 0.11 (0.04, 0.22)], encephalitis and encephalopathy [HR 1.82 (1.16, 2.84); burden 0.07 (0.01, 0.16)] (Xu et al., 2022).
The second study is an analysis of two-year retrospective cohort studies extracted from TriNetX electronic health records network with a cohort of 1,284,437 propensity score matched patients recently infected with COVID-19 versus controls with another respiratory infection (Taquet et al., 2022). They found increased risks of cognitive deficit [HR 1.36 (1.33, 1.39)], dementia [HR 1.33 (1.26, 1.41)], intracranial haemorrhage [HR 1.09 (1.01, 1.18)], ischemic stroke [HR 1.11 (1.06, 1.17)], and epilepsy [HR 1.14 (1.09, 1.19)], whilst hazard ratios of encephalitis, GBS, nerve root, plexus disorder and parkinsonism were less than 1 (Taquet et al., 2022).
Vaccination campaigns are integral to the prevention of widespread infectious disease (Lotan et al., 2022). Development of vaccination campaigns drew from previous experiences in dealing with MERS and SARS-CoV, specifically the latter as SARS-CoV-2 and SARS-CoV are 79% genetically similar and both target the human Angiotensin Converting Enzyme 2 (hACE2) on the host cell (Kaur and Gupta, 2020). Post-vaccination neuro-ophthalmic manifestations were previously considered to be rare (Lotan et al., 2022), with optic neuritis following vaccination being the main complication reported (DeStefano et al., 2003; Stübgen, 2013; Karussis and Petrou, 2014; Cheng and Margo, 2022a).
As of 30th March 2023, the World Health Organisation summarised that there are 183 vaccines in clinical development and 199 in pre-clinical development (WHO, 2023a). The 9 leading candidates are as follows: The Pfizer-BioNTech (BNT162b2) and the Moderna (mRNA-1273) messenger RNA (mRNA) vaccines, the AstraZeneca (AZD1222, ChAdOx1 nCoV-19, Vaxzevria), Janssen (Johnson & Johnson, Ad26.COV2.S), and Gamaleya (Sputnik V) non-replicating viral vector vaccines, the Sinovac (CoronaVac), Covaxin and Sinopharm (BBIBP-CorV) inactivated viral vaccines and the Novavax (NVX-CoV-2373) protein subunit vaccine (Kaur and Gupta, 2020; Li et al., 2021; Rawat et al., 2021; Hadj Hassine, 2022).
Safety data from phase 3 clinical trials have not highlighted neuro-ophthalmic diseases as a notable complication of the available COVID-19 vaccines (Palacios et al., 2020; Polack et al., 2020; Baden et al., 2021; Sadoff et al., 2021; Voysey et al., 2021). However, these trials are usually conducted over a limited time period and enrol no more than tens of thousands of participants, hence do not capture all the possible post-vaccination complications (Lotan et al., 2022).
Of the literature surveyed in this review, 31 cases of adverse neuro-ophthalmic events following COVID-19 vaccination were reported. 15 cases occurred following vaccination with Pfizer-BioNTech, nine cases following AstraZeneca, three cases following Moderna, two cases following Coronavac, and two cases following Sinopharm.
There were 27 cases of optic neuritis identified in this review, 17 had unilateral and 10 had bilateral involvement. Four cases were seropositive for MOG-IgG whilst two were seropositive for AQP4. 25 cases were of new-onset optic neuritis, whereas two cases had a history of optic neuritis; one had an episode of retrobulbar optic neuritis in 2014 and the other a history of multiple sclerosis with two previous episodes of optic neuritis (Shemer et al., 2023). The average time to symptom onset is 37 days (range 0.08 days (2 hours) to 180 days) following vaccination. Four cases were suspected of optic neuritis secondary to multiple sclerosis based on neuroimaging and CSF findings (Matsuo et al., 2023; Shemer et al., 2023). IVMP was commenced for all 27 cases, with three cases further requiring PLEX (Helmchen et al., 2022; Bhatti et al., 2023; Shemer et al., 2023). Improvement in visual function was noted for all except one case of unilateral NMO-associated optic neuritis where vision remained poor with optic atrophy observed following the second attack.
The incidence of neuro-ophthalmic sequelae following COVID-19 disease is far greater than that following vaccination against the virus. As of December 2023, there have been more than 770 million confirmed cases of COVID-19 (including nearly 7 million deaths) reported to WHO (2023b). At the same timepoint, 13 billion vaccine doses had been administered, with nearly 5.6 billion people vaccinated with a complete primary series. The 48 cases of adverse neuro-ophthalmic sequelae following infection and 31 cases following vaccination included in this review must be viewed in the context of the significant difference in denominator between these two groups.
It is difficult to conclude direct causation as opposed to correlation between COVID-19 and the neuro-ophthalmic sequelae, as the literature currently available primarily consists of individual case reports and small case series. Optic neuritis was the most frequently reported neuro-ophthalmic sequelae following COVID-19 infection and vaccination in this review, and prior to the onset of the pandemic is known to occur at a stable rate in the general population (Braithwaite et al., 2020). Optic neuritis can be associated with specific identifiable causes, such as multiple sclerosis, infection, or may be idiopathic, and the onset may seem to develop randomly without a trigger or cause. With neuro-ophthalmic conditions developing at a spontaneous low rate in the population at any time, many of the reported neurological sequelae following COVID-19 infection and vaccination in this review may have simply been unrelated coincidences.
In their multi-centre observational study, Zhao et al. analysed the rates of diagnosis of neuro-ophthalmic conditions as well as retinal detachment (RD) and acute angle closure glaucoma (AACG) (Zhao et al., 2024). They found that all conditions were diagnosed at higher rates following the introduction of COVID-19 vaccines compared to pre-COVID and pre-vaccine periods. The authors discuss that a likely explanation for the increased diagnostic rates following introduction of vaccinations is that patients tended to postpone seeking treatment even for acute ocular conditions such as RD and AACG during the pandemic, with clinic visit rates only noted to increase when vaccines became available to protect against the virus. Unlike neuro-ophthalmic conditions such as optic neuritis and cranial neuropathies, RD and AACG do not have plausible causal mechanisms in association with COVID-19 infection and vaccination, therefore the parallel fluctuation in diagnostic rates may point more towards correlation as opposed to causation. Nevertheless, the temporal association of the neuro-ophthalmic events occurring concurrent with or after SARS-CoV-2 infection or vaccination has led to the proposition of various causal pathomechanisms.
One theory of the pathogenesis of optic neuritis following COVID-19 infection is through direct viral inflammation of the optic nerve, subsequently causing myelin damage (Deane et al., 2021). This was demonstrated in mice inoculated with the mouse hepatitis virus MHV-A59 whereby upon isolation, the optic nerve sheaths and parenchyma were infiltrated with inflammatory cells (Shindler et al., 2008). It has been suggested that a similar mechanism may underlie optic neuritis as a result of COVID-19 infection as the mouse hepatitis virus shares a common genus with SARS-CoV-2 (Körner et al., 2020). An alternate theory is optic nerve ischemia secondary to a systemic state of hypercoagulability associated with SARS-CoV-2 infection. The increased thrombin generation and endothelial inflammation results in a hypoxic state which may induce an ischemic optic neuropathy (Deane et al., 2021). However, ischemia is less likely to be reversible, therefore the observation that most cases of optic neuritis concurrent with or following COVID-19 infection demonstrated improvement after treatment detracts from the likelihood of ischemia being the underlying causal mechanism.
Eleven of the 25 cases of new-onset optic neuritis in this review demonstrated MOG antibody positivity. It has been hypothesised that much like other viral infections, the aberrant post-infectious immune response following COVID-19 triggers the onset of a para-infectious demyelinating process (Tenembaum et al., 2007; Bosello et al., 2023). One suggested mechanism is through molecular mimicry, where viral antigens induce a pathological immune response against CNS antigens including antibodies against MOG (Tisdale et al., 2021; Bosello et al., 2023). However, it has also been pointed out that despite auto-antibodies targeting MOG, molecular mimicry is unlikely the cause due to lack of homology between the COVID-19 viral protein and the MOG protein (Johnsson et al., 2022). Instead, loss of self-tolerance in the context of an activated adaptive immune system is suggested to be culprit (Wesselingh and Wesselingh, 2023).
There are many cases in the literature of new-onset IIH following COVID-19 infection, with a limited consideration of how CSF hydrodynamics is affected by COVID-19 infection. Under physiological conditions, the choroid plexus secretes CSF (Wang et al., 2022) and is a known site of blood brain barrier breakdown in COVID-19 (Fullard et al., 2021; Yang et al., 2021). SARS-CoV-2 has tropism for the choroid plexus epithelium, meninges, and brain vasculature as the SARS-CoV-2 entry proteins ACE2 and TMPRSS2 are both expressed at these sites, which has been suggested as the underlying mechanism of dysregulated CSF hydrodynamics seen in COVID-19 (Yang et al., 2021). Endothelial dysfunction in COVID-19 also impairs CSF absorption via the arachnoid villi and astrocytic foot processes surrounding cerebral vasculature (Wang et al., 2022). Additionally, COVID-19 leads to a systemic state of hyperviscosity and hypercoagulability which increases venous pressure and induces formation of cerebral venous sinus thromboses, also leading to increased intracranial pressure (Al-Mufti et al., 2021; Mukharesh et al., 2022).
The pathogenesis of myasthenia gravis following COVID-19 is under investigation (Sriwastava et al., 2021). It is known that a systemic state of inflammation such as that following SARS-CoV-2 infection reduces the availability of AChRs at the postsynaptic neuromuscular junction (Koneczny and Herbst, 2019). Additionally, an external virus induces antibody production, which evokes an immune response that subsequently cross-reacts with AChRs as a result of molecular resemblance (Sriwastava et al., 2021). The affinity of COVID-19 for the ACE2 receptor found on multiple organs including the brain, lungs, and heart leads to the formation of autoantibodies and subsequently a downstream cascade involving proinflammatory cytokines, chemokines, depletion of B and T cells, and increased interleukins and TNF-a (Baig et al., 2020). This increases the risk of a cross-reactive autoimmune attack against the body’s own receptors (Baig et al., 2020). The treatment target is to improve symptoms, control antibody production and reduce disease severity, and typically encompasses pyridostigmine and immunosuppressive agents (Sriwastava et al., 2021).
PRES occurs due to cerebral oedema secondary to endothelial dysfunction that presents as visual disturbance, headache, seizures and altered consciousness (Triplett et al., 2022). SARS-CoV-2 has affinity for the viral receptor ACE2, which is also expressed at the capillary endothelium. The inflammatory nature of COVID-19 infection leading to vascular endothelial injury is suggested to be the causal mechanism of PRES development. The literature of PRES following COVID-19 infection present with similar symptoms to the three cases described in this review including altered mental status, seizure activity, visual impairment and visual agnosia (Franceschi et al., 2020; Kaya et al., 2020; Kishfy et al., 2020; Hixon et al., 2021). Neuroimaging in these three cases is also comparative with that described in the literature of T2/FLAIR hyperintensities diffusely distributed in the cerebral white matter without corresponding diffusion restriction on DWI (Hixon et al., 2021). The limiting factor is that none of the three cases underwent cerebrospinal fluid testing, hence direct infection resulting in the development of PRES cannot be excluded despite its uncommon occurrence.
Concerns for neurological complications of the vaccines began arising in 2020 when two patients developed transverse myelitis following the AstraZeneca vaccine (Goss et al., 2021). Serious systemic complications have been reported after vaccination, such as cerebral venous thrombosis as well as specific immune-mediated conditions such as myocarditis, pericarditis and thrombocytopenia (Chen et al., 2022). Most adverse neurological sequelae occurred after AstraZeneca vaccinations, followed by Pfizer-BioNTech and Moderna vaccines (Sriwastava et al., 2022). However the rates of each vaccination vary widely, for example as of November 2023, the total vaccine doses administered in the European Union were Pfizer-BioNTech 654 million, Moderna 155 million, AstraZeneca 67 million, Johnson & Johnson 19 million, Sinopharm/Beijing 2 million, Sputnik V 2 million (Mathieu et al., 2021). In this review, Pfizer-BioNTech was associated with nearly half of the neuro-ophthalmic complications reported, followed by AstraZeneca and Moderna, but it is clearly difficult to compare the rates of complications between vaccines when the absolute risks are so low and the numbers of vaccine doses administered varied so widely.
Optic neuritis was the most common complication following COVID-19 vaccination in this review. Optic neuritis following vaccine administration has previously been reported for other anti-viral vaccines, including but not limited to measles/mumps/rubella, influenza, rabies, tetanus/diphtheria/pertussis, hepatitis B and Herpes Zoster (Stübgen, 2013; Cheng and Margo, 2022a; Bhatti et al., 2023). There is no definitive causal relationship between vaccination and optic neuritis onset (Bhatti et al., 2023), although propositions of the etiopathogenesis include reaction to a vaccine component (e.g. protein or preparation adjuvant), molecular mimicry, production of proinflammatory cytokines, and/or activation of the innate and adaptive immune system (Bhatti et al., 2023). Nevertheless, reports of serious neurological sequelae following COVID-19 vaccination are still considered rare, especially in comparison with that caused by COVID-19 infection which has been found to be 617-fold higher in an analysis from the vaccine adverse event reporting system (VAERS) (Frontera et al., 2022).
As we approach the end of the SARS-CoV-2 pandemic, there is an increased awareness of the neuro-ophthalmic complications brought on by viral insult. The various COVID-19 vaccines that are currently available are part of the global effort to protect the most vulnerable of the human population. The incidence of neuro-ophthalmic consequences following infection with COVID-19 is hundred-folds higher and associated with more harrowing systemic effects than that following vaccination against the virus. Several proposed causal mechanisms are discussed in this review, but larger studies are required to make any definitive conclusions. As we approach the post-COVID era, neuro-ophthalmic presentations should nevertheless always necessitate careful exploration of COVID-19 infection history and vaccination status.
JS: Writing – original draft. HD: Writing – review & editing.
The author(s) declare that no financial support was received for the research, authorship, and/or publication of this article.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
The reviewer JG declared a past co-authorship with the author HD-M to the handling editor.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcimb.2024.1345683/full#supplementary-material
Supplementary Table 1 | Summary of case reports of neuro-ophthalmic events following COVID-19 infection and vaccination. Key: MRI, magnetic resonance imaging; MRV, magnetic resonance venography; FLAIR, fluid attenuated inversion recovery; MOG, myelin oligodendrocyte glycoprotein; AQP4, aquaporin-4; CT, computed tomography; IV, intravenous; IVMP, intravenous Methylprednisolone; RAPD, relative afferent pupillary defect; w/wo, with/without; PLEX, plasma exchange; CF, counting fingers; HVF, Humphrey visual field; BP, blood pressure; RE, right eye; LE, left eye; R, right; L, left; VA, visual acuity; CSF, cerebrospinal fluid; IPH, intraparietal haemorrhage; DWI, diffusion-weighted imaging; OCT, optical coherence tomography; CNS, central nervous system.
Al-Mufti, F., Amuluru, K., Sahni, R., Bekelis, K., Karimi, R., Ogulnick, J., et al. (2021). Cerebral venous thrombosis in COVID-19: A New York metropolitan cohort study. AJNR Am. J. Neuroradiol. 42 (7), 1196–1200. doi: 10.3174/ajnr.A7134
Arnao, V., Maimone, M. B., Perini, V., Giudice, G. L., Cottone, S. (2022). Bilateral optic neuritis after COVID vaccination. Neurol. Sci. 43 (5), 2965–2966. doi: 10.1007/s10072-021-05832-9
Baden, L. R., El Sahly, H. M., Essink, B., Kotloff, K., Frey, S., Novak, R., et al. (2021). Efficacy and safety of the mRNA-1273 SARS-CoV-2 vaccine. N. Engl. J. Med. 384 (5), 403–416. doi: 10.1056/NEJMoa2035389
Baig, A. M., Khaleeq, A., Ali, U., Syeda, H. (2020). Evidence of the COVID-19 virus targeting the CNS: tissue distribution, host–virus interaction, and proposed neurotropic mechanisms. ACS Chem. Neurosci. 11 (7), 995–998. doi: 10.1021/acschemneuro.0c00122
Balendra, R., North, M., Kumar, G., Qutab, S., Raouf, H. A., Delamont, S. S., et al. (2022). Raised intracranial pressure (pseudotumour cerebri) associated with severe acute respiratory syndrome coronavirus 2. J. Neuroophthalmol. 42 (2), e459–ee62. doi: 10.1097/WNO.0000000000001469
Benito-Pascual, B., Gegúndez, J. A., Díaz-Valle, D., Arriola-Villalobos, P., Carreño, E., Culebras, E., et al. (2020). Panuveitis and optic neuritis as a possible initial presentation of the novel coronavirus disease 2019 (COVID-19). Ocul. Immunol. Inflamm. 28 (6), 922–925. doi: 10.1080/09273948.2020.1792512
Betsch, D., Freund, P. R. (2021). Neuro-ophthalmologic manifestations of novel coronavirus. Adv. Ophthalmol. Optom. 6, 275–288. doi: 10.1016/j.yaoo.2021.04.017
Bhatti, M. T., Gilbert, A. L., Watson, G., Waheed, M., Spencer, D. (2023). Shot in the dark. Surv. Ophthalmol. 68 (4), 821–829. doi: 10.1016/j.survophthal.2022.09.003
Borrego-Sanz, L., Guermes-Villahoz, N., Fernández-Tresguerres, F., Santos-Bueso, E. (2021). Optic neuropathy in a COVID-19 patient. J. Fr. Ophtalmol. 44 (8), 1271–1273. doi: 10.1016/j.jfo.2021.04.002
Bosello, F., Marastoni, D., Pizzini, F. B., Zaffalon, C., Zuliani, A., Turri, G., et al. (2023). Atypical myelin oligodendrocyte glycoprotein antibody–associated optic neuritis and acute demyelinating polyneuropathy after SARS-CoV-2 infection: Case report and literature review. J. Neuroimmunol. 375, 578011. doi: 10.1016/j.jneuroim.2022.578011
Braithwaite, T., Subramanian, A., Petzold, A., Galloway, J., Adderley, N. J., Mollan, S. P., et al. (2020). Trends in optic neuritis incidence and prevalence in the UK and association with systemic and neurologic disease. JAMA Neurol. 77 (12), 1514–1523. doi: 10.1001/jamaneurol.2020.3502
Caudill, G. B., Wolin, M. J. (2023). Myelin oligodendrocyte glycoprotein and neuromyelitis optica/aquaporin-4 antibody negative COVID-19-associated optic neuritis. J. Neuroophthalmol. 43 (1), e1–e2. doi: 10.1097/WNO.0000000000001364
Chen, Y., Xu, Z., Wang, P., Li, X. M., Shuai, Z. W., Ye, D. Q., et al. (2022). New-onset autoimmune phenomena post-COVID-19 vaccination. Immunology 165 (4), 386–401. doi: 10.1111/imm.13443
Cheng, J. Y., Margo, C. E. (2022a). Ocular adverse events following vaccination: overview and update. Surv. Ophthalmol. 67 (2), 293–306. doi: 10.1016/j.survophthal.2021.04.001
Chuang, T. Y., Burda, K., Teklemariam, E., Athar, K. (2021). Tolosa-Hunt syndrome presenting after COVID-19 vaccination. Cureus 13 (7), e16791. doi: 10.7759/cureus.16791
Deane, K., Sarfraz, A., Sarfraz, Z., Valentine, D., Idowu, A. R., Sanchez, V. (2021). Unilateral optic neuritis associated with SARS-CoV-2 infection: A rare complication. Am. J. Case Rep. 22, e931665. doi: 10.12659/AJCR.931665
De Giglio, L., Sadun, F., Roberti, C., Polidori, L., Gilardi, M., Altavista, M. C., et al. (2023). Post-COVID simultaneous onset of Graves’ disease and ocular myasthenia gravis in a patient with a complex ocular motility impairment. Eur. J. Ophthalmol. 33 (3), Np49–np51. doi: 10.1177/11206721221077800
DeStefano, F., Verstraeten, T., Jackson, L. A., Okoro, C. A., Benson, P., Black, S. B., et al. (2003). Vaccinations and risk of central nervous system demyelinating diseases in adults. Arch. Neurol. 60 (4), 504–509. doi: 10.1001/archneur.60.4.504
Dinkin, M., Feinberg, E., Oliveira, C., Tsai, J. (2022). Orbital inflammation with optic perineuritis in association with COVID-19. J. Neuroophthalmol. 42 (1), e300–e3e1. doi: 10.1097/WNO.0000000000001229
Duran, M., Aykaç, S. (2023). Optic neuritis after COVID-19 infection: A case report. J. Fr. Ophtalmol. 46 (1), e4–e7. doi: 10.1016/j.jfo.2022.09.005
Elnahry, A. G., Asal, Z. B., Shaikh, N., Dennett, K., Abd Elmohsen, M. N., Elnahry, G. A., et al. (2023). Optic neuropathy after COVID-19 vaccination: a report of two cases. Int. J. Neurosci. 133 (8), 901–907. doi: 10.1080/00207454.2021.2015348
Feizi, P., Sharma, K., Pasham, S. R., Nirwan, L., Joseph, J., Jaiswal, S., et al. (2022). Central nervous system (CNS) inflammatory demyelinating diseases (IDDs) associated with COVID-19: A case series and review. J. Neuroimmunol. 371, 577939. doi: 10.1016/j.jneuroim.2022.577939
Franceschi, A. M., Ahmed, O., Giliberto, L., Castillo, M. (2020). Hemorrhagic posterior reversible encephalopathy syndrome as a manifestation of COVID-19 infection. AJNR Am. J. Neuroradiol. 41 (7), 1173–1176. doi: 10.3174/ajnr.A6595
François, J., Collery, A. S., Hayek, G., Sot, M., Zaidi, M., Lhuillier, L., et al. (2021). Coronavirus disease 2019–associated ocular neuropathy with panuveitis: A case report. JAMA Ophthalmol. 139 (2), 247–249. doi: 10.1001/jamaophthalmol.2020.5695
Friedman, D. I., Liu, G. T., Digre, K. B. (2013). Revised diagnostic criteria for the pseudotumor cerebri syndrome in adults and children. Neurology 81 (13), 1159–1165. doi: 10.1212/WNL.0b013e3182a55f17
Frontera, J. A., Tamborska, A. A., Doheim, M. F., Garcia-Azorin, D., Gezegen, H., Guekht, A., et al. (2022). Neurological events reported after COVID-19 vaccines: An analysis of VAERS. Ann. Neurol. 91 (6), 756–771. doi: 10.1002/ana.26339
Fullard, J. F., Lee, H. C., Voloudakis, G., Suo, S., Javidfar, B., Shao, Z., et al. (2021). Single-nucleus transcriptome analysis of human brain immune response in patients with severe COVID-19. Genome Med. 13 (1), 118. doi: 10.1186/s13073-021-00933-8
Gilardi, M., Cortese, A., Ferraro, E., Rispoli, M., Sadun, R., Altavista, M. C., et al. (2023). MOG-IgG positive optic neuritis after SARS-CoV-2 infection. Eur. J. Ophthalmol. 33 (5), Np87–np90. doi: 10.1177/11206721221136319
Goss, A. L., Samudralwar, R. D., Das, R. R., Nath, A. (2021). ANA Investigates: Neurological complications of COVID-19 vaccines. Ann. Neurol. 89 (5), 856–857. doi: 10.1002/ana.26065
Hadj Hassine, I. (2022). Covid-19 vaccines and variants of concern: A review. Rev. Med. Virol. 32 (4), e2313. doi: 10.1002/rmv.2313
Helmchen, C., Buttler, G. M., Markewitz, R., Hummel, K., Wiendl, H., Boppel, T. (2022). Acute bilateral optic/chiasm neuritis with longitudinal extensive transverse myelitis in longstanding stable multiple sclerosis following vector-based vaccination against the SARS-CoV-2. J. Neurol. 269 (1), 49–54. doi: 10.1007/s00415-021-10647-x
Hixon, A. M., Thaker, A. A., Pelak, V. S. (2021). Persistent visual dysfunction following posterior reversible encephalopathy syndrome due to COVID-19: Case series and literature review. Eur. J. Neurol. 28 (10), 3289–3302. doi: 10.1111/ene.14965
Ide, T., Kawanami, T., Eriguchi, M., Hara, H. (2022). SARS-CoV-2-related myelin oligodendrocyte glycoprotein antibody-associated disease: A case report and literature review. Intern. Med. 61 (8), 1253–1258. doi: 10.2169/internalmedicine.8709-21
Insausti-García, A., Reche-Sainz, J. A., Ruiz-Arranz, C., López Vázquez, Á, Ferro-Osuna, M. (2022). Papillophlebitis in a COVID-19 patient: Inflammation and hypercoagulable state. Eur. J. Ophthalmol. 32 (1), Np168–Nnp72. doi: 10.1177/1120672120947591
Jarius, S., Bieber, N., Haas, J., Wildemann, B. (2022). MOG encephalomyelitis after vaccination against severe acute respiratory syndrome coronavirus type 2 (SARS-CoV-2): case report and comprehensive review of the literature. J. Neurol. 269 (10), 5198–5212. doi: 10.1007/s00415-022-11194-9
Johnsson, M., Asztely, F., Hejnebo, S., Axelsson, M., Malmeström, C., Olausson, T., et al. (2022). SARS-COV-2 a trigger of myelin oligodendrocyte glycoprotein-associated disorder. Ann. Clin. Transl. Neurol. 9 (8), 1296–1301. doi: 10.1002/acn3.51609
Jossy, A., Jacob, N., Sarkar, S., Gokhale, T., Kaliaperumal, S., Deb, A. K. (2022). COVID-19-associated optic neuritis - A case series and review of literature. Indian J. Ophthalmol. 70 (1), 310–316. doi: 10.4103/ijo.IJO_2235_21
Kang, M., Kim, S., Park, J. S., Seok, H. Y. (2023). Myelin oligodendrocyte glycoprotein antibody-associated optic neuritis following third dose of BNT162b2 COVID-19 vaccine in a patient with systemic lupus erythematosus. Neurol. Sci. 44 (7), 2247–2249. doi: 10.1007/s10072-023-06715-x
Karam, E. Z., Ríos Macias, P., Chahin, G., Kattah, J. C. (2022). Inflammatory sixth nerve palsy post-COVID-19 vaccination: Magnetic resonance imaging findings. Neuroophthalmology 46 (5), 314–318. doi: 10.1080/01658107.2022.2037661
Karussis, D., Petrou, P. (2014). The spectrum of post-vaccination inflammatory CNS demyelinating syndromes. Autoimmun. Rev. 13 (3), 215–224. doi: 10.1016/j.autrev.2013.10.003
Kaur, S. P., Gupta, V. (2020). COVID-19 Vaccine: A comprehensive status report. Virus Res. 288, 198114. doi: 10.1016/j.virusres.2020.198114
Kaya, Y., Kara, S., Akinci, C., Kocaman, A. S. (2020). Transient cortical blindness in COVID-19 pneumonia; a PRES-like syndrome: Case report. J. Neurol. Sci. 413, 116858. doi: 10.1016/j.jns.2020.116858
Khalid, M. F., Micieli, J. A. (2022). Idiopathic intracranial hypertension associated with SARS-CoV-2 B.1.1.7 variant of concern. Can. J. Neurol. Sci. 49 (3), 472–473. doi: 10.1017/cjn.2021.129
Kishfy, L., Casasola, M., Banankhah, P., Parvez, A., Jan, Y. J., Shenoy, A. M., et al. (2020). Posterior reversible encephalopathy syndrome (PRES) as a neurological association in severe Covid-19. J. Neurol. Sci. 414, 116943. doi: 10.1016/j.jns.2020.116943
Kivanany, P. B., Raviskanthan, S., Mortensen, P. W., Lee, A. G. (2022). Antiaquaporin 4-related optic neuritis and myelitis post-COVID-19 infection. J. Neuroophthalmol. 42 (4), e571–e5e3. doi: 10.1097/WNO.0000000000001347
Kogure, C., Kikushima, W., Fukuda, Y., Hasebe, Y., Takahashi, T., Shibuya, T., et al. (2021). Myelin oligodendrocyte glycoprotein antibody-associated optic neuritis in a COVID-19 patient: A case report. Med. (Baltimore). 100 (19), e25865. doi: 10.1097/MD.0000000000025865
Koneczny, I., Herbst, R. (2019). Myasthenia gravis: pathogenic effects of autoantibodies on neuromuscular architecture. Cells 8 (7), 671. doi: 10.3390/cells8070671
Körner, R. W., Majjouti, M., Alcazar, M. A. A., Mahabir, E. (2020). Of mice and men: The Coronavirus MHV and mouse models as a translational approach to understand SARS-CoV-2. Viruses 12 (8), 880. doi: 10.3390/v12080880
Leber, H. M., Sant’Ana, L., Konichi da Silva, N. R., Raio, M. C., Mazzeo, T., Endo, C. M., et al. (2021). Acute thyroiditis and bilateral optic neuritis following SARS-CoV-2 vaccination with CoronaVac: A case report. Ocul. Immunol. Inflamm. 29 (6), 1200–1206. doi: 10.1080/09273948.2021.1961815
Lee, W. A. (2022). COVID-19 vaccine-associated optic neuritis. Qjm 115 (10), 683–685. doi: 10.1093/qjmed/hcac208
Li, L., Guo, P., Zhang, X., Yu, Z., Zhang, W., Sun, H. (2021). SARS-CoV-2 vaccine candidates in rapid development. Hum. Vaccin. Immunother. 17 (3), 644–653. doi: 10.1080/21645515.2020.1804777
Lotan, I., Lydston, M., Levy, M. (2022). Neuro-ophthalmological complications of the COVID-19 vaccines: A systematic review. J. Neuroophthalmol. 42 (2), 154–162. doi: 10.1097/WNO.0000000000001537
Luís, M. E., Hipólito-Fernandes, D., Mota, C., Maleita, D., Xavier, C., Maio, T., et al. (2020). A review of neuro-ophthalmological manifestations of human coronavirus infection. Eye Brain. 12, 129–137. doi: 10.2147/EB.S268828
Mathieu, E., Ritchie, H., Ortiz-Ospina, E., Roser, M., Hasell, J., Appel, C., et al. (2021). A global database of COVID-19 vaccinations. Nat. Hum. Behav. 5 (7), 947–953. doi: 10.1038/s41562-021-01122-8
Matsuo, T., Okubo, K., Mifune, H., Imao, T. (2023). Bilateral optic neuritis and hypophysitis with diabetes insipidus 1 month after COVID-19 mRNA vaccine: Case report and literature review. J. Investig. Med. High Impact Case Rep. 11, 23247096231186046. doi: 10.1177/23247096231186046
Micieli, J. A., Yu, C. W. (2022). Optic neuritis associated with SARS-CoV-2 B.1.1.7 variant of concern. Can. J. Neurol. Sci. 49 (4), 591–592. doi: 10.1017/cjn.2021.183
Mohamed, A., Tzoulis, P., Kossler, A. L., Dosiou, C. (2022). New onset or deterioration of thyroid eye disease after mRNA SARS-CoV-2 vaccines: Report of 2 cases and literature review. J. Clin. Endocrinol. Metab. 108 (4), 979–985. doi: 10.1210/clinem/dgac606
Mukharesh, L., Bouffard, M. A., Fortin, E., Brann, D. H., Datta, S. R., Prasad, S., et al. (2022). Pseudotumor cerebri syndrome with COVID-19: A case series. J. Neuroophthalmol. 42 (3), e545–e5e7. doi: 10.1097/WNO.0000000000001467
Nagaratnam, S. A., Ferdi, A. C., Leaney, J., Lee, R. L. K., Hwang, Y. T., Heard, R. (2022). Acute disseminated encephalomyelitis with bilateral optic neuritis following ChAdOx1 COVID-19 vaccination. BMC Neurol. 22 (1), 54. doi: 10.1186/s12883-022-02575-8
Palacios, R., Patiño, E. G., de Oliveira Piorelli, R., Conde, M. T. R. P., Batista, A. P., Zeng, G., et al. (2020). Double-blind, randomized, placebo-controlled phase III clinical trial to evaluate the efficacy and safety of treating healthcare professionals with the adsorbed COVID-19 (inactivated) vaccine manufactured by Sinovac – PROFISCOV: A structured summary of a study protocol for a randomised controlled trial. Trials 21 (1), 853. doi: 10.1186/s13063-020-04775-4
Pirani, V., Pelliccioni, P., Carpenè, M. J., Nicolai, M., Barbotti, F., Franceschi, A., et al. (2023). Optic neuritis following COVID-19 vaccination: Do autoimmune diseases play a role? Eur. J. Ophthalmol. 33 (4), Np46–np50. doi: 10.1177/11206721221118736
Polack, F. P., Thomas, S. J., Kitchin, N., Absalon, J., Gurtman, A., Lockhart, S., et al. (2020). Safety and efficacy of the BNT162b2 mRNA Covid-19 vaccine. N. Engl. J. Med. 383 (27), 2603–2615. doi: 10.1056/NEJMoa2034577
Przybek-Skrzypecka, J., Szewczuk, A., Kamińska, A., Skrzypecki, J., Pyziak-Skupień, A., Szaflik, J. P. (2022). Effect of COVID-19 lockdowns on eye emergency department, increasing prevalence of uveitis and optic neuritis in the COVID-19 era. Healthcare (Basel). 10 (8), 1422. doi: 10.3390/healthcare10081422
Rajabi, M. T., Rafizadeh, S. M., Aghajani, A. H., Pirzadeh, M. (2022). Idiopathic intracranial hypertension as a neurological manifestation of COVID-19: A case report. J. Fr. Ophtalmol. 45 (7), e303–e3e5. doi: 10.1016/j.jfo.2022.02.019
Rawat, K., Kumari, P., Saha, L. (2021). COVID-19 vaccine: A recent update in pipeline vaccines, their design and development strategies. Eur. J. Pharmacol. 892, 173751. doi: 10.1016/j.ejphar.2020.173751
Restivo, D. A., Centonze, D., Alesina, A., Marchese-Ragona, R. (2020). Myasthenia gravis associated with SARS-CoV-2 infection. Ann. Intern. Med. 173 (12), 1027–1028. doi: 10.7326/L20-0845
Rodríguez-Rodríguez, M. S., Romero-Castro, R. M., Alvarado-de la Barrera, C., González-Cannata, M. G., García-Morales, A. K., Ávila-Ríos, S. (2021). Optic neuritis following SARS-CoV-2 infection. J. Neurovirol. 27 (2), 359–363. doi: 10.1007/s13365-021-00959-z
Roy, M., Chandra, A., Roy, S., Shrotriya, C. (2022). Optic neuritis following COVID-19 vaccination: Coincidence or side-effect? - A case series. Indian J. Ophthalmol. 70 (2), 679–683. doi: 10.4103/ijo.IJO_2374_21
Sadoff, J., Gray, G., Vandebosch, A., Cárdenas, V., Shukarev, G., Grinsztejn, B., et al. (2021). Safety and efficacy of single-dose Ad26.COV2.S vaccine against Covid-19. N. Engl. J. Med. 384 (23), 2187–2201. doi: 10.1056/NEJMoa2101544
Sainath, D., Paul, A., Krishnagopal, S., Kumar, A. (2021). Acute bilateral retrobulbar optic neuritis - an atypical sequela of COVID-19. Indian J. Ophthalmol. 69 (12), 3761–3764. doi: 10.4103/ijo.IJO_2155_21
Sawalha, K., Adeodokun, S., Kamoga, G. R. (2020). COVID-19-induced acute bilateral optic neuritis. J. Investig. Med. High Impact Case Rep. 8, 2324709620976018. doi: 10.1177/2324709620976018
Sharma, A., KudChadkar, U. S., Shirodkar, R., Usgaonkar, U. P. S., Naik, A. (2021). Unilateral inferior altitudinal visual field defect related to COVID-19. Indian J. Ophthalmol. 69 (4), 989–991. doi: 10.4103/ijo.IJO_3666_20
Shemer, A., Greenbaum, A., Toledano, A., Biron, R., Dubinsky-Pertzov, B., Or, L. (2023). Optic neuritis after SARS-CoV-2 vaccination. J. Neuroophthalmol. 43 (1), 29–33. doi: 10.1097/WNO.0000000000001811
Shindler, K. S., Kenyon, L. C., Dutt, M., Hingley, S. T., Das Sarma, J. (2008). Experimental optic neuritis induced by a demyelinating strain of mouse hepatitis virus. J. Virol. 82 (17), 8882–8886. doi: 10.1128/JVI.00920-08
Shukla, A. K., Peter, A., Bhargava, J. K., Arya, V., Gupta, M. K., Yadav, N., et al. (2022). Sarcoidosis presenting as bilateral optic neuritis after ChAdOx1 nCoV-19 vaccination. Monaldi Arch. Chest Dis. 93 (1). Available at: https://www.monaldi-archives.org/index.php/macd/article/view/2279.
Sinha, A., Dwivedi, D., Dwivedi, A., Bajaj, N. (2021). Optic neuritis as a presenting symptom of post-COVID-19 multisystem inflammatory syndrome in children (MIS-C). Indian J. Pediatr. 88 (12), 1269. doi: 10.1007/s12098-021-03921-3
Sitaula, S., Poudel, A., Gajurel, B. P. (2022). Non-arteritic anterior ischemic optic neuropathy in COVID-19 infection - A case report. Am. J. Ophthalmol. Case Rep. 27, 101684. doi: 10.1016/j.ajoc.2022.101684
Sofuoğlu, A., Akçay, N., Şevketoğlu, E., Bektaş, G. (2021). Pseudotumor cerebri syndrome as a neurologic involvement of multisystem inflammatory syndrome in children: A case report. J. Trop. Pediatr. 67 (4), fmab075. doi: 10.1093/tropej/fmab075
Sriwastava, S., Sharma, K., Khalid, S. H., Bhansali, S., Shrestha, A. K., Elkhooly, M., et al. (2022). COVID-19 vaccination and neurological manifestations: A review of case reports and case series. Brain Sci. 12 (3), 407. doi: 10.3390/brainsci12030407
Sriwastava, S., Tandon, M., Kataria, S., Daimee, M., Sultan, S. (2021). New onset of ocular myasthenia gravis in a patient with COVID-19: a novel case report and literature review. J. Neurol. 268 (8), 2690–2696. doi: 10.1007/s00415-020-10263-1
Stübgen, J.-P. (2013). A literature review on optic neuritis following vaccination against virus infections. Autoimmun. Rev. 12 (10), 990–997. doi: 10.1016/j.autrev.2013.03.012
Taquet, M., Sillett, R., Zhu, L., Mendel, J., Camplisson, I., Dercon, Q., et al. (2022). Neurological and psychiatric risk trajectories after SARS-CoV-2 infection: an analysis of 2-year retrospective cohort studies including 1 284 437 patients. Lancet Psychiatry 9 (10), 815–827. doi: 10.1016/S2215-0366(22)00260-7
Tavakoli, M., Sotoudeh, H., Rezaei, A., Saadatpour, Z., Vaphides, M. S., Kline, L. B. (2022). Optic nerve infarction in a patient with Coronavirus disease 2019. J. Neuroophthalmol. 42 (1), e347–e3e8. doi: 10.1097/WNO.0000000000001232
Tenembaum, S., Chitnis, T., Ness, J., Hahn, J. S. (2007). Acute disseminated encephalomyelitis. Neurology 68 (16 suppl 2), S23–S36. doi: 10.1212/01.wnl.0000259404.51352.7f
Tisdale, A. K., Dinkin, M., Chwalisz, B. K. (2021). Afferent and efferent neuro-ophthalmic complications of coronavirus disease 19. J. Neuroophthalmol. 41 (2), 154–165. doi: 10.1097/WNO.0000000000001276
Triplett, J. D., Kutlubaev, M. A., Kermode, A. G., Hardy, T. (2022). Posterior reversible encephalopathy syndrome (PRES): diagnosis and management. Pract. Neurol. 22 (3), 183–189. doi: 10.1136/practneurol-2021-003194
Verkuil, L. D., Liu, G. T., Brahma, V. L., Avery, R. A. (2020). Pseudotumor cerebri syndrome associated with MIS-C: a case report. Lancet 396 (10250), 532. doi: 10.1016/S0140-6736(20)31725-6
Virgo, J., Mohamed, M. (2020). Paracentral acute middle maculopathy and acute macular neuroretinopathy following SARS-CoV-2 infection. Eye (Lond). 34 (12), 2352–2353. doi: 10.1038/s41433-020-1069-8
Voysey, M., Clemens, S. A. C., Madhi, S. A., Weckx, L. Y., Folegatti, P. M., Aley, P. K., et al. (2021). Safety and efficacy of the ChAdOx1 nCoV-19 vaccine (AZD1222) against SARS-CoV-2: an interim analysis of four randomised controlled trials in Brazil, South Africa, and the UK. Lancet 397 (10269), 99–111. doi: 10.1016/S0140-6736(20)32661-1
Wang, M. T. M., Bhatti, M. T., Danesh-Meyer, H. V. (2022). Idiopathic intracranial hypertension: Pathophysiology, diagnosis and management. J. Clin. Neurosci. 95, 172–179. doi: 10.1016/j.jocn.2021.11.029
Wang, J., Huang, S., Yu, Z., Zhang, S., Hou, G., Xu, S. (2022). Unilateral optic neuritis after vaccination against the coronavirus disease: two case reports. Doc. Ophthalmol. 145 (1), 65–70. doi: 10.1007/s10633-022-09880-0
Wesselingh, R., Wesselingh, S. L. (2023). An eye to the future: Acute and long-term neuro-ophthalmological and neurological complications of COVID-19. Clin. Exp. Ophthalmol. 51 (4), 370–379. doi: 10.1111/ceo.14221
WHO (2023a). “COVID-19 vaccine tracker and landscape,” (Geneva: World Health Organisation). Available at: https://www.who.int/publications/m/item/draft-landscape-of-covid-19-candidate-vaccines.
WHO (2023b). “WHO Coronavirus (COVID-19) dashboard,” (Geneva: World Health Organisation). Available at: https://covid19.who.int/.
Xu, E., Xie, Y., Al-Aly, Z. (2022). Long-term neurologic outcomes of COVID-19. Nat. Med. 28 (11), 2406–2415. doi: 10.1038/s41591-022-02001-z
Yang, A. C., Kern, F., Losada, P. M., Agam, M. R., Maat, C. A., Schmartz, G. P., et al. (2021). Dysregulation of brain and choroid plexus cell types in severe COVID-19. Nature 595 (7868), 565–571. doi: 10.1038/s41586-021-03710-0
Yıldız Tascı, Y., Nalcacoglu, P., Gumusyayla, S., Vural, G., Toklu, Y., Yesılırmak, N. (2022). Aquaporin-4 protein antibody-associated optic neuritis related to neuroendocrine tumor after receiving an inactive COVID-19 vaccine. Indian J. Ophthalmol. 70 (5), 1828–1831. doi: 10.4103/ijo.IJO_2494_21
Zhang, J., Joiner, D., Zhang, C. (2023). Hyperacute optic neuritis in a patient with COVID-19 infection and vaccination: a case report. BMC Ophthalmol. 23 (1), 80. doi: 10.1186/s12886-023-02825-4
Zhao, D., Li, X., Carey, A. R., Henderson, A. D. (2024). Optic neuritis and cranial neuropathies diagnosis rates before coronavirus disease 2019, in the initial pandemic phase, and post-vaccine introduction. Ophthalmology 131 (1), 78–86. doi: 10.1016/j.ophtha.2023.08.021
Keywords: coronavirus, Covid-19, SARS-CoV-2, 2019-nCoV, vaccination, vaccine, immunization, neuro-ophthalmology
Citation: Shi J and Danesh-Meyer HV (2024) A review of neuro-ophthalmic sequelae following COVID-19 infection and vaccination. Front. Cell. Infect. Microbiol. 14:1345683. doi: 10.3389/fcimb.2024.1345683
Received: 28 November 2023; Accepted: 03 January 2024;
Published: 17 January 2024.
Edited by:
Xinyuan Zhang, Capital Medical University, ChinaReviewed by:
Jesse Gale, Cambridge University Hospitals NHS Foundation Trust, United KingdomCopyright © 2024 Shi and Danesh-Meyer. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Jane Shi, amFuZS5zaGlAYXVja2xhbmQuYWMubno=
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.