 Dee Xi
Dee Xi- Department of Clinical Laboratory, The First College of Clinical Medical Science, China Three Gorges University, Yichang Central People’s Hospital, Yichang, China
Francisella philomiragia is a Gram-negative coccobacillus, which is a very rare human opportunistic pathogen causing pneumonia and systemic infection. It is difficult to identify this bacterium through conventional Gram-staining and biochemical methods due to an amorphous Gram stain appearance after 24 h culture and its relatively fastidious and slow growth giving weak and/or delayed reactions in biochemical tests. It is often misidentified as other bacteria including Haemophilus spp., Pseudomonas aeruginosa, or Sphingomonas paucimobilis. False identification may delay the therapy of the patients and even endanger the patient’s life. Here, we report a case of a 34-year-old man with acute lymphoblastic leukemia infected by F. philomiragia, which was almost misdiagnosed. This case describes our identification of a patient with a systemic F. philomiragia infection. To our knowledge, this is the first such case reported in China.
1 Introduction
Francisella philomiragia is a strictly aerobic, Gram-negative coccobacillus, which is a very rare human opportunistic pathogen. There are just 22 human infected cases reported around the world until now (Wenger et al., 1989; Sicherer et al., 1997; Friis-Møller et al., 2004; Mailman and Schmidt, 2005; Kreitmann et al., 2015; Relich et al., 2015; Robles-Marhuenda et al., 2018; Froböse et al., 2020; Chua et al., 2021). F. philomiragia infection historically has been reported in patients with underlying conditions including CGD, hematological malignancy, or near-drowning events (Wenger et al., 1989; Sicherer et al., 1997; Friis-Møller et al., 2004; Mailman and Schmidt, 2005; Relich et al., 2015; Robles-Marhuenda et al., 2018; Froböse et al., 2020). As a member of the Francisella genus, F. philomiragia is an opportunistic pathogen causing fever, pneumonia, and systemic infection such as bacteremia. Different from its more virulent relative Francisella tularensis, F. philomiragia infection related to saltwater exposure usually occurs in immunocompromised or near-drowning people (Wenger et al., 1989; Sicherer et al., 1997; Friis-Møller et al., 2004; Mailman and Schmidt, 2005; Kreitmann et al., 2015; Relich et al., 2015; Robles-Marhuenda et al., 2018; Froböse et al., 2020; Chua et al., 2021) while tularemia transmitted by the bite of arthropods, contacting infected animals, consuming contaminated water and food, or inhalation of contaminated aerosols (Fooladfar and Moradi, 2023) always occurs in people with normal immunity apart from a few cases with abnormal immunity (Wenger et al., 1989). Confusion with F. tularensis may lead to false biohazard alarms. F. tularensis is a Risk Group 3 pathogen and a potential biological weapon (Mailman and Schmidt, 2005) because of its strong virulence and easy diffusion through aerosol, and because it exists in the environment for a long time (Wenger et al., 1989; Mailman and Schmidt, 2005; Freudenberger Catanzaro and Inzana, 2020), potentially leading to high numbers of secondary tularemia cases. Limited awareness of F. philomiragia has caused delayed diagnosis, therapeutic failures, and bad outcomes. Here, we present the first case of F. philomiragia infection reported in China. A 34-year-old man with acute lymphoblastic leukemia was infected by F. philomiragia after 16 days’ chemotherapy.
2 Case presentation
A 34-year-old man was admitted to a local hospital because of fever and fatigue. The results of a routine blood test showed that the patient had a high white blood cell count (WBC; 16.4 × 109/L) and a very high percentage of immature granular cells (72%), and a low red blood cell count (RBC; 2.42 × 1012/L) and a low blood platelet count (PLT; 16 × 109/L). Then, the patient was given other examinations including bone marrow hemocytology (original cells 73%, and peroxidase staining <3%), cellular immunology (flow cytometry detected 82% of abnormal cells expressing the following biomarkers: HLA-DR, CD10, CD19, CD20, CD22, CD34, CD38, CD58, CD123, CD79a, and TdT), and gene detection [BCR/ABL1(P190) fusion gene was positive]. On the basis of these results, the patient was diagnosed with acute lymphoblastic leukemia and was admitted to our hospital. Chemotherapy with Dasatinib plus DVP was started 2 days after his admission. After 16 days’ chemotherapy, the patient complained of chest tightness, shortness of breath, dyspnea, cough and expectoration, blood in phlegm, edema of both lower extremities, weakness of limbs, and fever with a maximum body temperature of 39.2°C. Physical examination revealed moist crackles in both lower lungs, obvious on the right side, and the blood oxygen saturation decreased to 86%. The empirical treatment with antibacterial cefoperazone-sulbactam and antifungal fluconazole was initiated. Computed tomography examination of the lungs showed multiple patchy shadows in both lungs, mainly in the lower right lung, with partial consolidation and bilateral pleural effusion (Figure 1). Blood routine test revealed the following levels: leukocyte, 0.36 × 109 cells/L; erythrocyte, 1.96 × 1012 cells/L; hemoglobin, 61 g/L; platelets, 46 × 109 cells/L; and neutrophil, 0.26 × 109 cells/L. Elevated levels of procalcitonin (0.211 ng/ml) and CRP (54.23 mg/L) were also noted. Four bottles of blood culture samples were drawn at once. One of the aerobic bottles of blood cultures signaled positively after approximately 22.2 h of incubation in the blood culture instrument (BacT/Alert 3D, Biomérieux, France). Gram stain of broth from this bottle showed Gram-negative coccobacilli (Figure 2). The blood culture broth was subcultured with a blood and a chocolate agar plate. Medium-sized (diameter approximately 5 mm), glossy, convex colonies grew on the plates (Figure 3A) after 24 h of incubation in the incubator at 35°C in 5% CO2. Gram stain of the single colony showed Gram-negative coccobacilli (Figure 3B), the same as those seen in the blood culture smear. The bacteria were identified as Sphingomonas paucimobilis by the automatic microbial identification and antimicrobial susceptibility testing system (Vitek 2 Compact, Biomérieux, France). The mass spectrometer (Vitek MS, Biomérieux, France) did not yield an identification result. The discrepancy in identification between the Vitek 2 Compact and mass spectrometer data might have reflected underlying differences in the databases associated with each testing type, and thus, further testing to identify the bacterium in the blood culture was undertaken. 16S rRNA gene sequencing identified the pathogen as F. philomiragia. At the same time, NGS (next-generation sequencing) (MGISEQ-200, BGI, China) detected F. philomiragia and Legionella in the bronchoalveolar lavage fluid of the patient. After the bacteria were identified, the clinician replaced the antibiotics with moxifloxacin and azithromycin. The patient’s symptoms gradually improved.
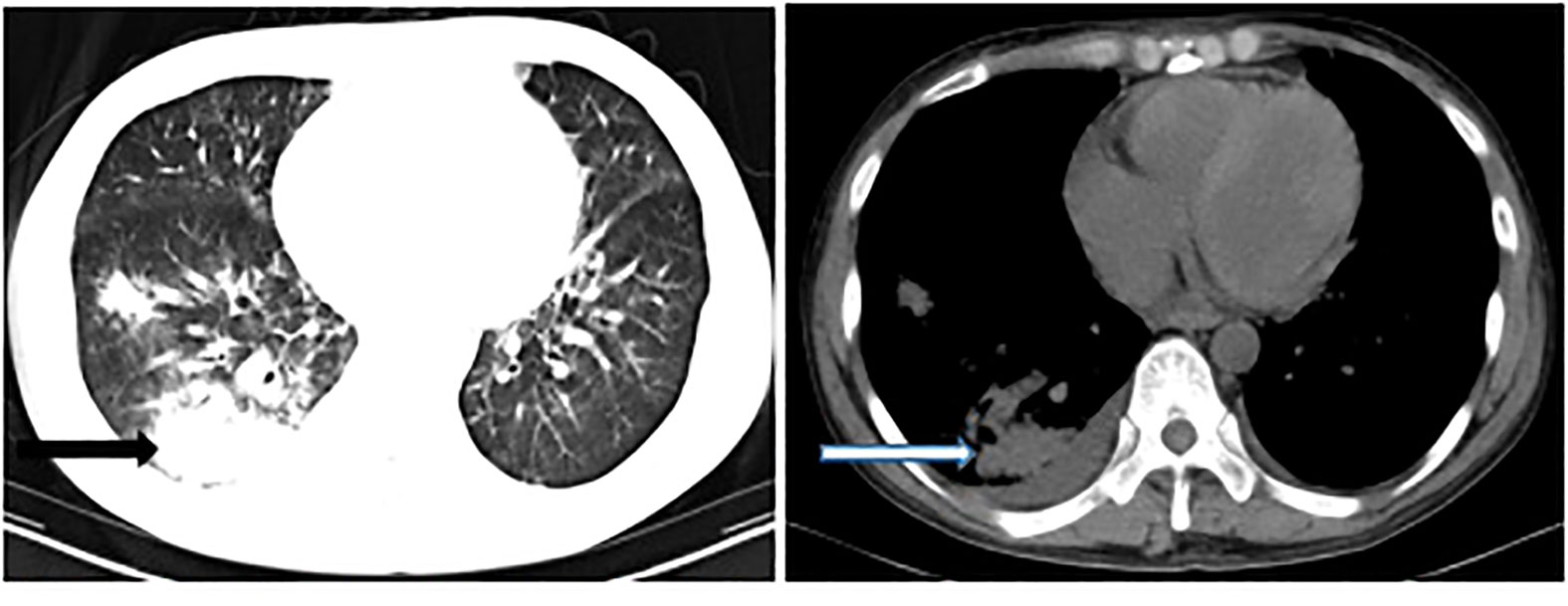
Figure 1 Computed tomography examination of the lungs showed multiple patchy shadows, especially in the right lung (arrow).
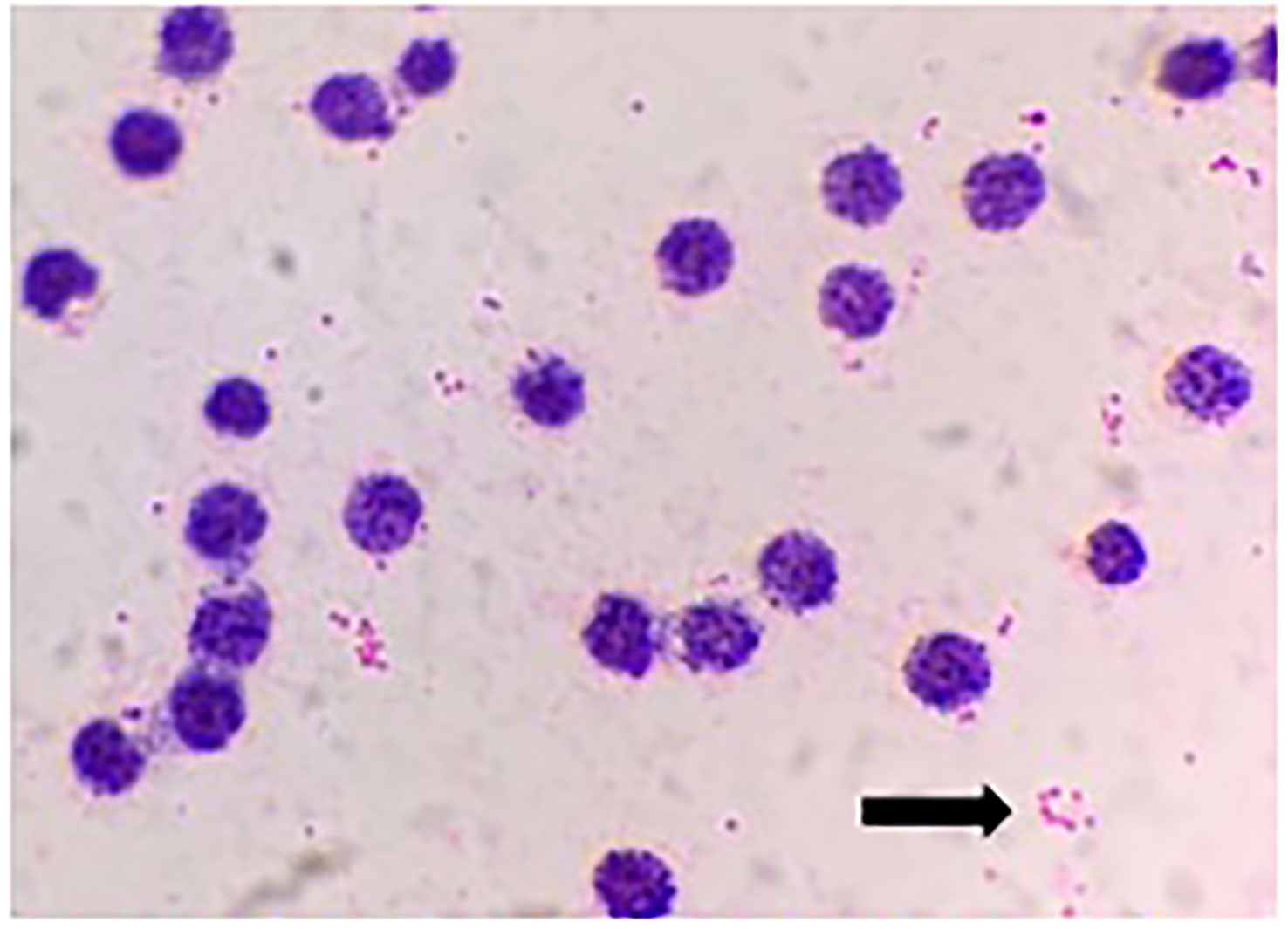
Figure 2 Gram stain of blood culture both showed Gram-negative coccobacilli (arrow).
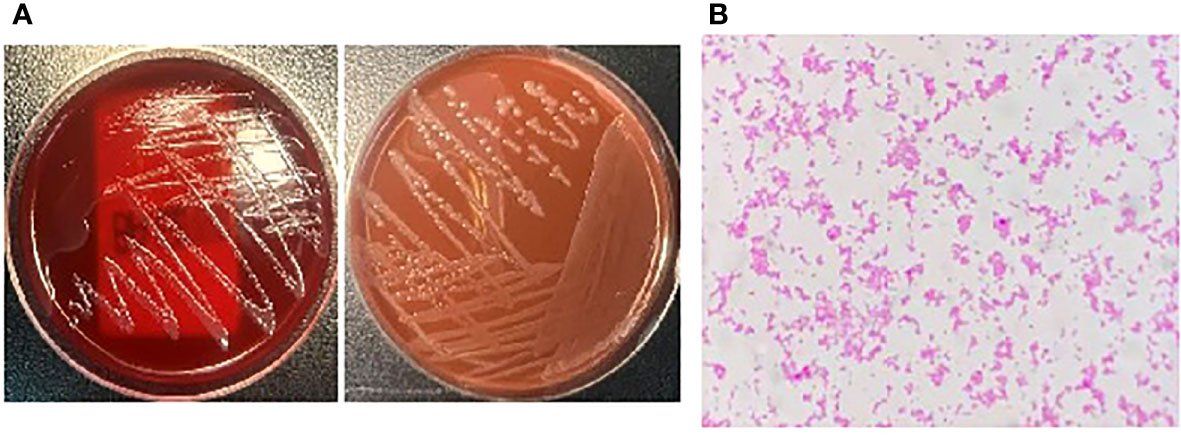
Figure 3 The bacteria was incubated in the incubator at 35°C in 5% CO2 for 24h, (A) The plates grew medium-sized (diameter about 5mm), glossy, convex colonies. (B) Gram stain of the single colony showed Gram-negative coccobacilli.
3 Discussion
F. philomiragia is an intracellular Gram-negative non-motile coccobacillus (Propst et al., 2016), belonging to the Gammaproteobacteria class and Francisellaceae family (John et al., 2019). F. philomiragia seems to like aquatic environments as it has been found near bodies of water, particularly brackish or saltwater in the mainland United States (Hollis et al., 1989; Berrada and Telford, 2010; Siddaramappa et al., 2012) and coastal waters in Norway (Duodu et al., 2012). F. philomiragia is a very rare human opportunistic pathogen, which has been isolated from water, muskrats, dogs, and humans (Hollis et al., 1989; Cora et al., 2010). F. philomiragia infection mainly occurs in immunocompromised patients, such as CGD patients who fail to produce superoxide anion and other oxygen metabolites including H2O2 to kill catalase-producing microorganisms (e.g., Staphylococcus aureus, Pseudomonas aeruginosa, enteric bacilli, and Aspergillus spp.) because of defective oxidase function in the circulating phagocytes (Wenger et al., 1989; Friis-Møller et al., 2004), patients with hematologic malignancies who receive long-term chemotherapy drugs (Kreitmann et al., 2015), and the patient with polycystic kidney receiving long-term immunosuppressive agents after renal transplantation (Relich et al., 2015). Exposure to seawater is also more prone to be infected by F. philomiragia. Some CGD patients had F. philomiragia infection after a seaside vacation (Friis-Møller et al., 2004; Robles-Marhuenda et al., 2018; Froböse et al., 2020). A 10-year-old CGD patient was infected by F. philomiragia because of a facial abrasion caused by a seawater crab tossed by the patient’s friend (Mailman and Schmidt, 2005). The most common symptoms of F. philomiragia infection are fever and pneumonia (Wenger et al., 1989; Friis-Møller et al., 2004; Mailman and Schmidt, 2005; Kreitmann et al., 2015; Relich et al., 2015; Robles-Marhuenda et al., 2018; Froböse et al., 2020; Chua et al., 2021), and meningitis and peritonitis have also been reported (Relich et al., 2015; Robles-Marhuenda et al., 2018). Deaths due to sepsis have also been reported (Fooladfar and Moradi, 2023). It was found that F. philomiragia could infect healthy lung tissue via alveolar macrophages or epithelial cells, which explains why pneumonia is the common symptom after F. philomiragia infection in patients (Propst et al., 2016). Generally speaking, patients are prone to be infected by F. philomiragia through saltwater exposure. Some reports have suggested infection via aerosols or insect bites, although these claims are not well-supported (Kreitmann et al., 2015). In this case, the patient became infected during hospitalization. However, the patient had gone to the city near a sea before admission; it was possible that he had contact with seawater or a marine organism, which was a possible source of infection. F. philomiragia and Legionella were both detected in the bronchoalveolar lavage fluid of the patient, which would suggest the patient may have been infected by exposure to seawater/aerosols contaminated by both bacterial species; a case like this has never been reported before. F. philomiragia was found not only in blood but also in the bronchoalveolar lavage fluid of the patient, which would suggest a possible respiratory source for the bacteremia.
Incubated with aquatic amoebae, F. philomiragia can form robust biofilms to exist in water for a long time (Verhoeven et al., 2010). That may explain the prevalence of F. philomiragia infection in patients contacting seawater and marine organisms. Furthermore, one study showed that F. philomiragia was able to infect the human hepatocyte-like cell line HepG2 cells. This finding suggested that F. philomiragia might replicate in the liver of near-drowning victims, so the sequelae of infected patients should be closely observed (Propst et al., 2016).
Originally assigned to the genus Yersinia, F. philomiragia is closely related to F. tularensis (Relich et al., 2015), a tier 1 select agent (Freudenberger Catanzaro and Inzana, 2020), and confusion in identification might lead to unnecessary biohazard alarms (Mailman and Schmidt, 2005). As there are differences in biochemical reactions between F. philomiragia and F. tularensis (Table 1), they can be readily distinguished from one another. F. philomiragia is frequently detected in the blood of patients (Wenger et al., 1989; Friis-Møller et al., 2004; Kreitmann et al., 2015; Relich et al., 2015; Robles-Marhuenda et al., 2018; Chua et al., 2021), and is also found in lymph node tissue (Mailman and Schmidt, 2005; Chua et al., 2021), lung biopsy, cerebrospinal fluid, and thoracoabdominal fluid (Wenger et al., 1989), while the detection in sputum and alveolar lavage fluid is uncommon.
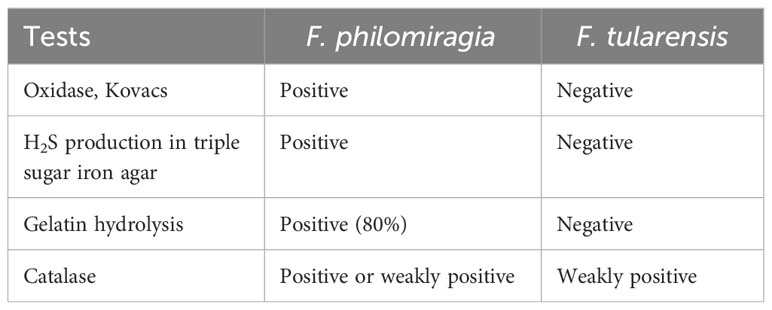
Table 1 Biochemical differences between F. philomiragia and F. tularensis.
It is not easy to obtain accurate identification of F. philomiragia. On the one hand, Gram staining shows very small coccobacillus with diverse morphology, fine sand-like scattered distribution, and F. philomiragia may be even mistaken for impurities in the background of blood culture smear to be neglected. Repeated isolation of cultures on solid medium made F. philomiragia more visible with Gram staining due to their small ball and rod-shaped morphology (Friis-Møller et al., 2004). On the other hand, difficulty exists in conventional biochemical identification of the isolate probably due to its relatively fastidious nature with slow growth giving weak and delayed reactions, so it is easy to identify F. philomiragia as other bacteria (Relich et al., 2015). In this report, F. philomiragia was wrongly identified as S. paucimobilis by GN card (Vitek 2 GN, Biomérieux, France). Additionally, the mass spectrometer (Vitek MS, Biomérieux, France) did not yield an identification result because this bacterium was not in the database of the instrument. However, F. philomiragia identified by the mass spectrometer (Bruker Daltonics, Bremen, Germany) has been reported, and the results were in accordance with that of gas chromatography and 16S rRNA gene sequencing (Froböse et al., 2020). Some mass spectrometers cannot identify F. philomiragia probably because this bacterium is not within their databases, and the identification becomes possible when adding F. philomiragia spectra in the database. The identification of F. philomiragia needs to be confirmed by 16S rRNA gene sequencing (Friis-Møller et al., 2004; Mailman and Schmidt, 2005; Robles-Marhuenda et al., 2018; Froböse et al., 2020). F. philomiragia is very rare in daily practice, which is not well known by us, so it may be neglected or identified by mistake. With the development of advanced technologies in molecular biology and more knowledge about this bacterium, it will become easier to identify F. philomiragia.
In clinical practice, if you encounter the very small Gram-negative coccobacillus with unusual morphology just like that in Figures 2, 3B, which was identified as S. paucimobilis or other bacteria by GN card, you must be particularly careful. In order to ensure the accuracy of the identification, it is best to perform 16S rRNA gene sequencing to confirm the result. False identification may lead to incorrect treatment, which will delay the patient’s disease course and may even lead to death in severe cases.
To date, there is no standardized guideline for the treatment of F. philomiragia. Hollis et al. found that the isolates of F. philomiragia were sensitive to aminoglycosides, tetracycline, chloramphenicol, cefoxitin, and cefotaxime but were resistant to ampicillin; 79% of the isolates were moderately sensitive to erythromycin, and all produced β-lactamase (Wenger et al., 1989). Robles-Marhuenda et al. found that most of the isolates were susceptible to quinolones, chloramphenicol, and carbapenems but resistant to ampicillin, and all produced β-lactamase. Third-generation cephalosporins, aminoglycosides, and tetracyclines may also be useful (Robles-Marhuenda et al., 2018). Froböse et al. found that the isolate of F. philomiragia was resistant to trimethoprim/sulfamethoxazole and sensitive to meropenem and ciprofloxacin (Froböse et al., 2020). Antimicrobial susceptibility testing with the human antimicrobial peptide LL-37 and the mouse antimicrobial peptide mCRAMP showed that these peptides were highly active against F. philomiragia and could kill bacteria in vitro. However, the antimicrobial peptide host defense mechanism was clearly not sufficient to control infected cells or F. philomiragia infection in vivo (Propst et al., 2016). The treatment of F. philomiragia varies greatly, mainly depending on the patient’s disease status and underlying conditions. Among the previously reported cases of F. philomiragia infection, one patient with fever and pleuritis was treated without antibiotics, and in the other cases, the patients were given two to four antibiotics (Relich et al., 2015).
Data availability statement
The raw data supporting the conclusions of this article will be made available by the authors, without undue reservation.
Ethics statement
Informed consent was obtained from all subjects involved in the study. Written informed consent was obtained from the participant/patient(s) for the publication of this case report.
Author contributions
The author confirms being the sole contributor of this work and has approved it for publication.
Conflict of interest
The author declares that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abbreviations
F. philomiragia, Francisella philomiragia; S. paucimobilis, Sphingomonas paucimobilis; F. tularens, Francisella tularens.
References
Berrada, Z. L., Telford, S. R., 3rd (2010). Diversity of Francisella species in environmental samples from Martha's Vineyard, Massachusetts. Microb. Ecol. 59 (2), 277–283. doi: 10.1007/s00248-009-9568-y
Chua, H. S., Soh, Y. H., Loong, S. K., AbuBakar, S. (2021). Francisella philomiragia bacteremia in an immunocompromised patient: a rare case report. Ann. Clin. Microbiol. Antimicrob. 20 (1), 72. doi: 10.1186/s12941-021-00475-2
Cora, M. C., Neel, J. A., Tarigo, J., Post, K., Barnes, J. (2010). Francisella philomiragia septicemia in a dog. J. Vet. Intern. Med. 24 (4), 969–972. doi: 10.1111/j.1939-1676.2010.0545.x
Duodu, S., Larsson, P., Sjödin, A., Forsman, M., Colquhoun, D. J. (2012). The distribution of Francisella-like bacteria associated with coastal waters in Norway. Microb. Ecol. 64 (2), 370–377. doi: 10.1007/s00248-012-0023-0
Fooladfar, Z., Moradi, F. (2023). Francisella and tularemia in western Asia, Iran: a systematic review. New Microbes New Infect. 52, 101092. doi: 10.1016/j.nmni.2023.101092
Freudenberger Catanzaro, K. C., Inzana, T. J. (2020). The francisella tularensis polysaccharides: what is the real capsule? Microbiol Mol. Biol. Rev. 84 (1), e00065–e00019. doi: 10.1128/MMBR.00065-19
Friis-Møller, A., Lemming, L. E., Valerius, N. H., Bruun, B. (2004). Problems in identification of Francisella philomiragia associated with fatal bacteremia in a patient with chronic granulomatous disease. J. Clin. Microbiol. 42 (4), 1840–1842. doi: 10.1128/JCM.42.4.1840-1842.2004
Froböse, N. J., Masjosthusmann, K., Huss, S., Correa-Martinez, C. L., Mellmann, A., Schuler, F., et al. (2020). A child with soft-tissue infection and lymphadenitis. New Microbes New Infect. 38, 100819. doi: 10.1016/j.nmni.2020.100819
Hollis, D. G., Weaver, R. E., Steigerwalt, A. G., Wenger, J. D., Moss, C. W., Brenner, D. J. (1989). Francisella philomiragia comb. nov. (formerly Yersinia philomiragia) and Francisella tularensis biogroup novicida (formerly Francisella novicida) associated with human disease. J. Clin. Microbiol. 27 (7), 1601–1608. doi: 10.1128/jcm.27.7.1601-1608.1989
John, E., Raphael, D., Martin, J. (2019). Mandell, douglas, and Bennett’s principles and practice of infectious diseases. 9th ed (Philadelphia: Churchill Living stone), 4176.
Kreitmann, L., Terriou, L., Launay, D., Caspar, Y., Courcol, R., Maurin, M., et al. (2015). Disseminated infection caused by francisella philomiragia, France, 2014. Emerg. Infect. Dis. 21 (12), 2260–2261. doi: 10.3201/eid2112.150615
Mailman, T. L., Schmidt, M. H. (2005). Francisella philomiragia adenitis and pulmonary nodules in a child with chronic granulomatous disease. Can. J. Infect. Dis. Med. Microbiol. 16 (4), 245–248. doi: 10.1155/2005/486417
Propst, C. N., Pylypko, S. L., Blower, R. J., Ahmad, S., Mansoor, M., van Hoek, M. L. (2016). Francisella philomiragia Infection and Lethality in MamMalian Tissue Culture Cell Models, Galleria mellonella, and BALB/c Mice. Front. Microbiol. 7, 696. doi: 10.3389/fmicb.2016.00696
Relich, R. F., Humphries, R. M., Mattison, H. R., Miles, J. E., Simpson, E. R., Corbett, I. J., et al. (2015). Francisella philomiragia bacteremia in a patient with acute respiratory insufficiency and acute-on-chronic kidney disease. J. Clin. Microbiol. 53 (12), 3947–3950. doi: 10.1128/JCM.01762-15
Robles-Marhuenda, A., Vaca, M., Romero, P., Ferreira, A., López-Granados, E., Arnalich, F. (2018). Francisella philomiragia: think of chronic granulomatous disease. J. Clin. Immunol. 38 (3), 257–259. doi: 10.1007/s10875-018-0498-7
Sicherer, S. H., Asturias, E. J., Winkelstein, J. A., Dick, J. D., Willoughby, R. E. (1997). Francisella philomiragia sepsis in chronic granulomatous disease. Pediatr. Infect. Dis. J. 16 (4), 420–422. doi: 10.1097/00006454-199704000-00021
Siddaramappa, S., Challacombe, J. F., Petersen, J. M., Pillai, S., Kuske, C. R. (2012). Genetic diversity within the genus Francisella as revealed by comparative analyses of the genomes of two North American isolates from environmental sources. Genomics 13, 422. doi: 10.1186/1471-2164-13-422
Verhoeven, A. B., Durham-Colleran, M. W., Pierson, T., Boswell, W. T., Van Hoek, M. L. (2010). Francisella philomiragia biofilm formation and interaction with the aquatic protist Acanthamoeba castellanii. Biol. Bull. 219 (2), 178–188. doi: 10.1086/BBLv219n2p178
Keywords: Francisella philomiragia, acute lymphoblastic leukemia, 16S rRNA, blood culture, bacteremia, antibiotics
Citation: Xi D (2023) Case report: Francisella philomiragia bacteremia in a patient with acute lymphoblastic leukemia. Front. Cell. Infect. Microbiol. 13:1206972. doi: 10.3389/fcimb.2023.1206972
Received: 16 April 2023; Accepted: 18 August 2023;
Published: 14 September 2023.
Edited by:
Joseph B. McPhee, Ryerson University, CanadaReviewed by:
Andrew Clark, University of Texas Southwestern Medical Center, United StatesMax Maurin, Université Grenoble Alpes, France
Copyright © 2023 Xi. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Dee Xi, MjcwNTY4NTA3QHFxLmNvbQ==