 Alicia Macias1
Alicia Macias1 Paloma Martín2
Paloma Martín2 Mayte Pérez-Olmeda3,4Beatriz Fernández-Martínez5,6
Mayte Pérez-Olmeda3,4Beatriz Fernández-Martínez5,6 Diana Gómez-Barroso5,6Esperanza Fernández7Julian Mauro Ramos8Laura Herrero3Saray Rodríguez1Elena Delgado7Maria Paz Sánchez-Seco3,4Miguel Galán1Antonio Jesús Corbacho7Manuel Jimenez1
Diana Gómez-Barroso5,6Esperanza Fernández7Julian Mauro Ramos8Laura Herrero3Saray Rodríguez1Elena Delgado7Maria Paz Sánchez-Seco3,4Miguel Galán1Antonio Jesús Corbacho7Manuel Jimenez1 Cristian Montero-Peña9Antonio Valle1
Cristian Montero-Peña9Antonio Valle1 Ana Vázquez3,6*
Ana Vázquez3,6*- 1Servicios de Microbiología y Medicina Interna, Hospital Don Benito-Villanueva de la Serena, Don Benito, Badajoz, Spain
- 2Servicio de Microbiología , Hospital Universitario de Badajoz, Badajoz, Spain
- 3Centro Nacional de Microbiología, Instituto de Salud Carlos III (CNM-ISCIII), Madrid, Spain
- 4CIBER de Enfermedades Infecciosas (CIBERINFEC), Madrid, Spain
- 5Centro Nacional Epidemiología, Instituto de Salud Carlos III (CNE-ISCIII), Madrid, Spain
- 6CIBER de Epidemiología y Salud Pública (CIBERESP), Madrid, Spain
- 7Banco de Sangre de Extremadura, Junta de Extremadura, Mérida, Badajoz, Spain
- 8Subdirección de Epidemiología, Servicio Extremeño de Salud, Mérida, Badajoz, Spain
- 9Servicio Medicina Familiar y Comunitaria, Centro de Salud Don Benito Oeste, Hospital Don Benito-Villanueva, Don Benito, Badajoz, Spain
In Spain, the largest human West Nile virus (WNV) outbreak among humans was reported in 2020, constituting the second most important outbreak in Europe that season. Extremadura (southwestern Spain) was one of the affected areas, reporting six human cases. The first autochthonous human case in Spain was reported in Extremadura in 2004, and no other human cases were reported until 2020. In this work, we describe the first WNV human outbreak registered in Extremadura, focusing on the most important clinical aspects, diagnostic results, and control actions which followed. In 2020, from September to October, human WNV infections were diagnosed using a combination of molecular and serological methods (an in-house specific qRT-PCR and a commercial ELISA for anti-WNV IgM and IgG antibodies) and by analysing serum, urine, and/or cerebrospinal fluid samples. Serological positive serum samples were further tested using commercial kits against related flaviviruses Usutu and Tick-borne encephalitis in order to analyse serological reactivity and to confirm the results by neutralisation assays. In total, six cases of WNV infection (five with neuroinvasive disease and one with fever) were identified. Clinical presentation and laboratory findings are described. No viral RNA was detected in any of the analysed samples, but serological cross-reactivity was detected against the other tested flaviviruses. Molecular and serological methods for WNV detection in various samples as well as differential diagnosis are recommended. The largest number of human cases of WNV infection ever registered in Extremadura, Spain, occurred in 2020 in areas where circulation of WNV and other flaviviruses has been previously reported in humans and animals. Therefore, it is necessary to enhance surveillance not only for the early detection and implementation of response measures for WNV but also for other emerging flaviviruses that could be endemic in this area.
Introduction
West Nile virus (WNV) is an important zoonotic virus with symptoms ranging from mild fever to severe lethal neuroinvasive disease in humans. The virus is maintained in an enzootic cycle among mosquitoes belonging to the Culex genus and birds, with mammals (equids and humans) being dead-end hosts. In humans, most of the infections are asymptomatic (80%) and those who develop disease, after an incubation period of 2 to 14 days, usually have mild symptoms such as fever, headache, fatigue, malaise, myalgia, arthralgia, rash, lymphadenopathy, and gastrointestinal symptoms (anorexia, nausea, vomiting, or diarrhoea) (Gray and Webb, 2014; Barzon et al., 2015; Bai et al., 2019). Less than 1% of infected cases develop a neuroinvasive disease (WNND) such as encephalitis, meningitis, and acute flaccid paralysis, frequently associated with risk factors such as aging, solid organ transplant, diabetes, hypertension, and other immunosuppression conditions related to fatal outcome (Lindsey et al., 2012). Moreover, atypical or rare presentations of WNV disease (WNVD) such us myocarditis, pancreatitis, hepatitis, cerebellitis, rhabdomyolysis, and ocular manifestations have also been described (Hasbun et al., 2016; Konjevoda et al., 2019; Velasco et al., 2020). WNVD has sometimes been associated with several sequelae, the most frequent being muscle weakness, fatigue, myalgia, memory loss, depression, and difficulty doing activities of daily living (Carson et al., 2006; Hughes et al., 2007). There is no vaccine for humans, and treatment is supportive as there are no specific antiviral drugs.
In humans, the peak of viraemia is 4–8 days post-infection (dpi). Antibodies can be detected in serum after 3–9 dpi, and the WNV IgM generally persists for over 6 months and may still be detectable for up to 1 year (Barzon et al., 2015). The laboratory-based diagnostic approaches are composed of virus isolation, RT-PCR, serology, and pathological examination. The most commonly used molecular diagnostic technique is real-time reverse transcription polymerase chain reaction (qRT-PCR), as it is a very fast and reliable technique, which also quantifies the viral genome. Serologically, diagnosis is based on the detection of IgM and IgG antibodies against WNV. As cross-reactivity with other flaviviruses may occur, the virus neutralisation tes by virus neutralisation tes against WNV remains the gold standard because of its high specificity and ability to detect and quantify neutralising antibodies to the virus (Tardei et al., 2000; Lustig et al., 2018). The limitation of this assay is that it takes a week to obtain results and, in Europe, a biosafety level 3 laboratory is required.
Since its discovery, WNV has caused human and animal disease outbreaks all over the world, except in Antarctica. In Europe, the virus is endemic and emerging in multiple countries. Over the last two decades, there have been notable increases in the number and extension of human and equine cases. Several genetic lineages of the virus have been detected (Vázquez et al., 2010), but lineages 1 and 2 have been mainly responsible for the disease in humans and equids in European countries. According to reports by the European Center for Disease Prevention and Control (ECDC), a significant increase in the number of human cases was observed in 2018 in Europe, eight times higher than in 2017 (ECDC, 2019). Most locally acquired cases were reported by Italy, Greece, and Romania, representing 39%, 20%, and 18% of EU cases, respectively. During 2020, EU/EEA and EU-neighbouring countries reported 336 locally acquired human cases of WNVD, mostly in Greece, Spain, and Italy (ECDC, 2020). Later, in 2021 (ECDC, 2022a) and 2022 (ECDC, 2022b), 139 and 965 human cases respectively were reported in Europe. In Spain, WNV fever is a notifiable disease. The first two notified human cases were detected in Andalusia in 2010 (García-Bocanegra et al., 2011), although the first known human case—diagnosed retrospectively—occurred in 2004 in Badajoz (Extremadura) (Kaptoul et al., 2007). Three additional cases were notified in Andalusia in 2016 (López-Ruiz et al., 2018), and no autochthonous human cases were reported from 2017 to 2019 in Spain. In the summer of 2020, the greatest number of WNV cases in humans in Spain was described (García San Miguel Rodríguez-Alarcón et al., 2021), with 77 cases detected in southwest Spain (71 from Andalusia and 6 from Extremadura) in areas where the virus was detected in previous years in humans, animals, and/or mosquitoes. Between 2021 and 2022, 10 human cases were reported in Spain, eight in Andalusia, and two in Catalonia, but none in Extremadura (ISCIII, 2022). Several studies in Spain have revealed the circulation of WNV in Andalusia during at least the last two decades. Moreover, the presence of WNV through seroprevalence studies is being detected in other Spanish regions (Extremadura, Catalonia, Castilla La Mancha, Castilla León, Comunidad Valenciana, and Mallorca) in birds, horses, and other mammals (Vanhomwegen et al., 2017; Napp et al., 2021; Casades-Martí et al., 2023).
In 2020 in Extremadura, where WNV human cases had not been reported since 2004, six autochthonous WNVD were described in Badajoz province. These cases were detected in areas where circulation of WNV and other flaviviruses, such as Usutu (USUV) and Tick-borne encephalitis (TBEV), has been described in birds, horses, and/or dogs (García-Bocanegra et al., 2018; Bravo-Barriga et al., 2021; Guerrero-Carvajal et al., 2021). Moreover, in 2020, when the WNV human outbreak occurred, USUV RNA was detected in mosquitoes and USUV-specific antibodies were detected in wild birds close to rural and urban areas, which is indicative of an active circulation and represents a public health threat (Bravo-Barriga et al., 2023). In 2021, no WNV human cases or animal outbreaks were reported through the veterinary surveillance system, and in 2022, there were only three equine outbreaks in Badajoz (Ministry of Agriculture and Fisheries and Food, 2023a; Ministry of Agriculture and Fisheries and Food, 2023b).
Materials and methods
Outbreak detection
On 22/09/2020, the National Reference Laboratory for Arboviruses in Spain (NRL), of the National Center for Microbiology (NCM-ISCIII), confirmed a WNV human case in a patient in the province of Badajoz (Extremadura). In the following 4 weeks, five more cases were detected in surrounding areas, one of them by additional epidemiological investigations and retrospective serological analyses from patients with neurological disease of unknown but suspected viral aetiology. No travel history was described for the six detected WNV human cases.
The data available from the Ministry of Agriculture and Fisheries and Food (Ministry of Agriculture and Fisheries and Food, 2023a; Ministry of Agriculture and Fisheries and Food, 2023b) regarding animal surveillance and human cases were consulted, and a map was made with spatial distribution in livestock regions (sanitary areas concerning veterinary health). This map was created with free software QGIS v.3.18.
Case definition
In Spain, WNVD has been notifiable since 2010. The detection of a single case is considered a Public Health Alert. Epidemiological data are provided as soon as it is available and updated according to the evolution of the cases, following National Guidelines, which contain case definition, public health measures such us seasonal active surveillance of meningoencephalitis cases in certain regions considered at risk, and response in case of an outbreak together with standardised survey of cases. According to the National Guidelines and the European Union case definition, a WNVD human case is suspected when a person lives in/or has visited a high-risk area, or has been bitten by mosquitoes and presents at least one of the following signs or symptoms with or without fever (>38.5°C): encephalitis, meningitis, acute flaccid paralysis, or Guillain-Barré syndrome. Laboratory case definitions and diagnostic algorithms for WNV human infections are defined as laboratory-confirmed or probable cases. At least one laboratory criterion is required to confirm the case: isolation of the virus, nucleic acid detection in a clinical sample, IgM detection in cerebrospinal fluid (CSF), or WNV IgM and IgG detection in sera confirmed by the neutralisation assay. The presence of WNV-specific antibodies in a serum sample allows only probable case classification. Laboratory results need to be interpreted according to flavivirus vaccination status (European Commission, 2018; ISCIII, 2021).
Ethical statement
The cases reported in this study were investigated with routine procedures according to the national surveillance plan for WNV infection. A unique ID to ensure the anonymity of patients and no patient identifiers were included in the study. The study was approved by the Ethical Committee of ISCIII (No. CEI PI 06_2023).
Microbiological investigations
In the regional hospitals, the acute serum samples were tested by serological methods to detect recent infection due to Borrelia spp., Leptospira spp. and Coxiella burnetii, and by molecular methods to detect herpes simplex virus, varicella zoster virus, enterovirus, and cytomegalovirus in the central nervous system (CNS). The CSF samples were also biochemically analysed.
For WNV diagnosis, the samples were sent to the NCM-ISCIII. Molecular and serological methods were used in serum, urine, and CSF samples. The presence of WNV RNA was investigated in serum, urine, and CSF acute samples using a specific WNV qRT-PCR (Vázquez et al., 2016). Anti-WNV immunoglobulin M (IgM) and immunoglobulin G (IgG) antibodies were determined in human CSF by sera acute and convalescent samples, using WNV IgM Capture DxSelect and WNV IgG DxSelect ELISA kits (Focus Diagnostics, Cypress, California, USA).
Specimens found positive for WNV antibodies were also tested against other flaviviruses (USUV and TBEV) to exclude possible cross-reactivity. The methods used were USU IgG ELISA Euroimmun assay and TBE IgG and IgM indirect immunofluorescence assays (IFA) (Flavivirus Mosaic 1, Euroimmun, Lübeck, Germany) for TBEV. These assays were performed according to the manufacturer’s instructions. WNV IgM-positive results were confirmed performing the WNV IgM assay, which was carried out in parallel in the presence and absence of antigen.
To confirm the specificity of the antibody response, positive or indeterminate sera in both WNV IgG and IgM ELISA tests were assayed by neutralisation test (NT) against WN (strain HU6365/08), USU (strain HU10279/09), and TBE (strain Neudorfl) viruses. For this purpose, samples were tested in duplicate. Briefly, serum samples were inactivated at 56°C for 30 min and then twofold dilutions (25 µl) of the samples ranging from 1:8 to 1:512 were placed in a 96-well tissue culture microplate (Nunc A/S, Roskilde, Denmark) and mixed with 25 µl containing 100 tissue culture infectivity doses (100 TCID50) of the virus. After 1 h of incubation in a 5% CO2 incubator at 37°C, 50 µl of a Vero E6 cell suspension containing 4 × 105 cells/ml was added to each well. Cultures were maintained for 7 days at 37°C and 5% CO2, and microscopic evaluation of the cytopathic effect was carried out 3, 5, and 7 days after inoculation. The titres of neutralising antibodies were defined as the highest serum dilution that showed >90% neutralisation of the virus challenge. Neutralising antibody titres ≥1:16 were considered positive. Specific responses to viruses were based on the comparison of NT titres obtained in parallel against the three flaviviruses, and the neutralising immune response observed was considered specific when NT titres for a given virus were >fourfold higher than the titre obtained for the other viruses. All these procedures were performed in a biosafety level 3 laboratory.
The WNV NAT (Nucleic Acid Testing) screening in blood donations in Extremadura was performed on individual samples using the commercial cobas® WNV Test on the cobas 6800 System (Roche Diagnostics). This screening was performed until the end of the WNV season attending to the recommendations of official organisms.
Results
Description of human cases of WNV infection
Between September and October 2020, six human cases of WNV infection were identified. The first WNV case was diagnosed on 22 September and the last one on 16 October. Symptom onset occurred between 1 and 30 September. All the patients were over 50 years old, and the average age was 64 (range 51 to 80). Two were women and four were men. No epidemiological link according to municipality of infection was found. All cases were admitted to the hospital and presented fever and other WNVD-related symptoms such as headache (n = 3), malaise (n = 2), dizziness (n = 2), diarrhoea (n = 1), vomiting (n = 1), cough (n = 1), hypertension (n = 1), and arthromyalgia (n = 1). Five of them presented WNND and the other one fever with arthromyalgia, headache, lymphopenia, and thrombopenia. Several complications such as asthenia, hypertension, unstable gait, muscle pains, bradypsychia, fever, dizziness, tremors, arthralgia, hydrocephalus, and cognitive impairment were observed, and three patients with previous pathologies presented worse disease evolution. There were no deaths, and all cases were discharged by 23 October. The mean length of stay was 16 days (range 6 to 29) (Table 1).
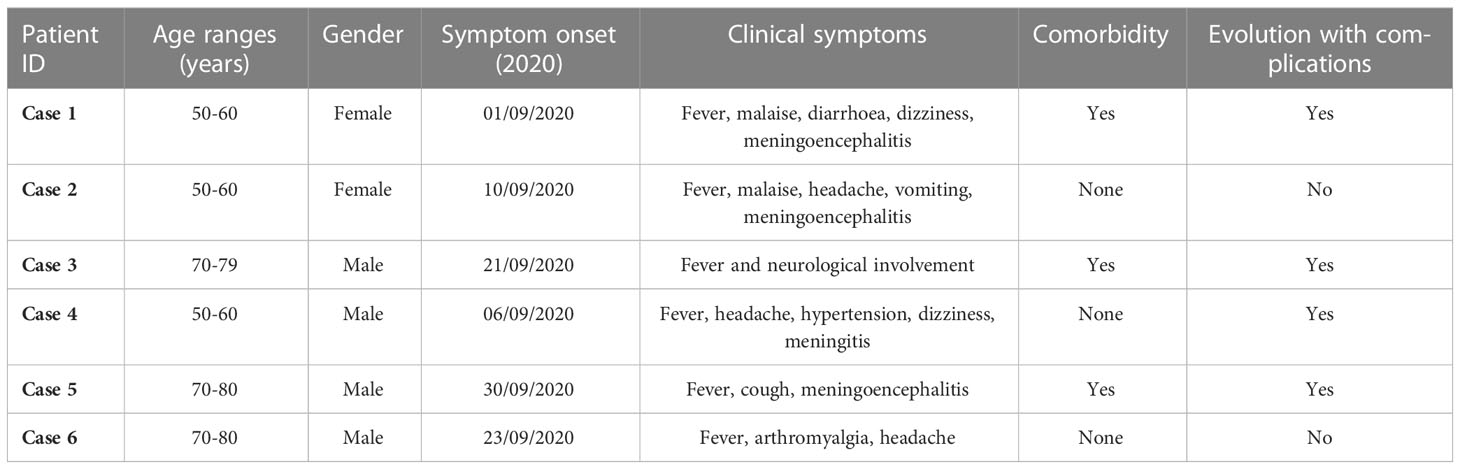
Table 1 Summary of clinical data of the patients infected with West Nile virus in Extremadura, Spain, 2020.
None of the patients had a history of travel abroad during the incubation period, and none had been vaccinated against other flaviviruses such as TBEV, yellow fever (YFV), or Japanese encephalitis (JEV).
Patients’ epidemiological, clinical, and laboratory data are presented in Tables 1, 2.
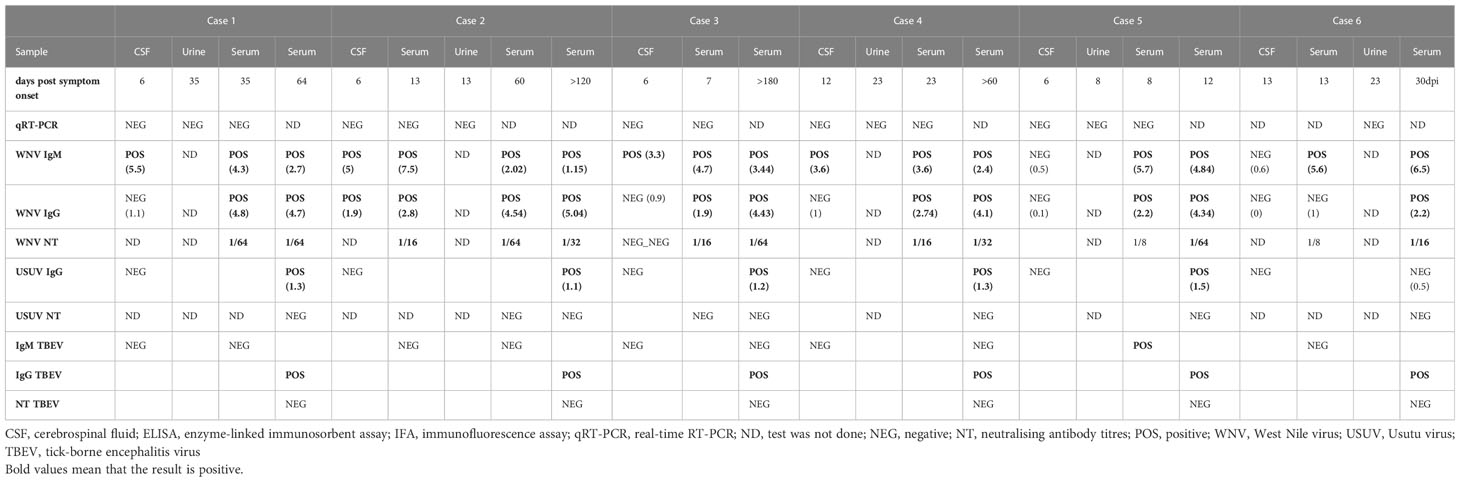
Table 2 Summary of the molecular and serological results obtained from the analysis carried out in the samples obtained from the patients.
Laboratory results
In total, 24 samples belonging to the six patients were analysed. The acute serum samples were negative for detecting recent infection due to Borrelia spp., Leptospira spp., Coxiella burnetii, herpes simplex virus, varicella zoster virus, enterovirus, and cytomegalovirus. In the CSF, the bacterial culture was negative and the CSF analysis typically showed mononuclear pleocytosis (>15 leucocytes/µl) with elevated protein concentration and a normal glucose level.
There were 15 samples (sera, CSF and urine) examined by qRT-PCR for WNV, none of which were positive (Table 2). All the cases were confirmed by detection of neutralising antibodies against WNV by the neutralisation assay in serum samples, although in four out of six cases, diagnosis was also confirmed by detection of IgM antibodies in CSF. The titre of the neutralising WNV antibodies was low, in a range from 1/16 to 1/64. A convalescent serum was obtained in four patients, and a slight rise in the neutralisation titre was found. All the human serum samples showed IgM positivity for WNV and seroconversion or a rise of the IgG level. IgM against TBEV was also tested in some acute and convalescent serum samples by IFI giving negative results, except one sample that showed positive immunofluorescent signal at 8 days post-symptom onset (dpo). However, all convalescent samples IgG positive for WNV showed cross-reactivity in IgG against TBEV and USUV, showing a high degree of cross-reactivity in these assays between these flaviviruses, but no neutralising antibodies against TBEV or USUV were detected.
Outbreak control measures
After the first human case diagnosis on 22 September, a control of the blood and organs donation system was activated, according to the Ministry of Health regulations, the National Transplant Organization, and the European Commission directive 2014/110/UE (Scientific Committee for Transfusion Safety, 2021). Regarding the measures adopted to prevent the transmission of the virus through blood donations in risk areas, once the first confirmed WNV case was detected, all donations in the affected areas were blocked during the incubation period of the first case. Moreover, blood collections were cancelled in high-risk areas until September 29 when WNV NAT screening was introduced. This measure to control donations was maintained until the end of the virus circulation season. All the samples tested by NAT screening were negative. Moreover, an active surveillance was established by epidemiological surveillance units and Hospital Clinical Services, and all clinicians were alerted through the Extremadura Health Service. A retrospective search for possible WNVD human cases (undiagnosed meningitis and meningoencephalitis from Badajoz province) was intensified after the first case, identifying five probable cases of which one was confirmed by laboratory methods. Additional measures were activated, including information campaigns on mosquito bite prevention, cleaning potential mosquito-breeding sites, recommendations for tissue-sample handling, postmortem examination, and safety in transfusions and transplants. Additionally, at a Regional level, an entomological surveillance was established. Furthermore, at a National level, a review and update of the national guidelines for surveillance and rapid risk assessments was performed (Spanish Ministry of Health, 2020).
According to the data available from the Ministry of Agriculture and Fisheries and Food (2023a) and (2023b) regarding animal surveillance, seven cases of WNV were reported in horses belonging to three livestock regions (sanitary areas concerning veterinary health), between 4 September and 23 October in six areas in Extremadura (Caceres and Badajoz), all very close to the affected area where the human cases were detected (Figure 1). Of the seven horses, five (71%) were detected in Badajoz province and two (29%) in Caceres province. Five of them (71%) were diagnosed in September and three of them a few days before the first human case (Table 3).
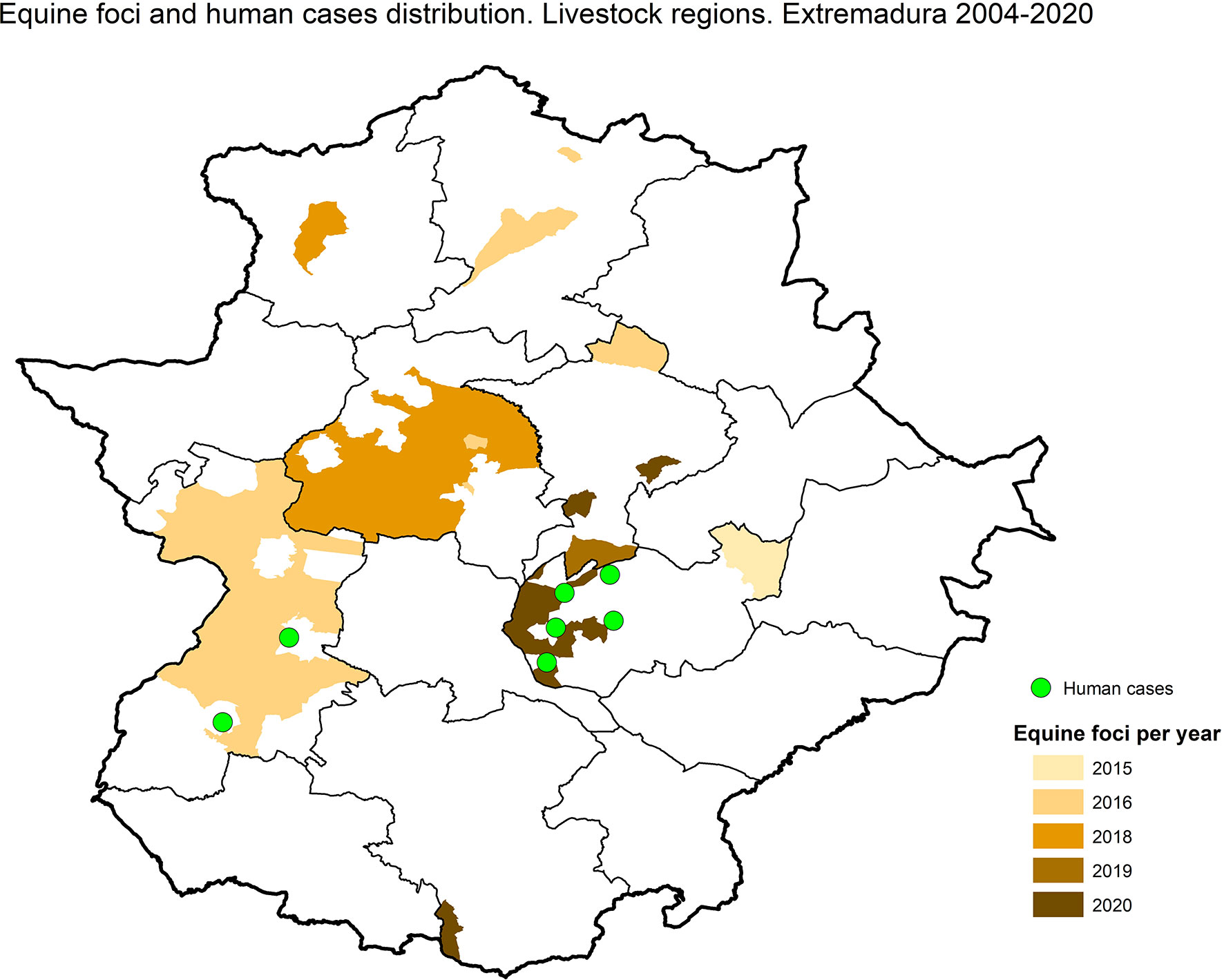
Figure 1 Areas with WNV equine foci or human cases. Data from 2004 to 2020.
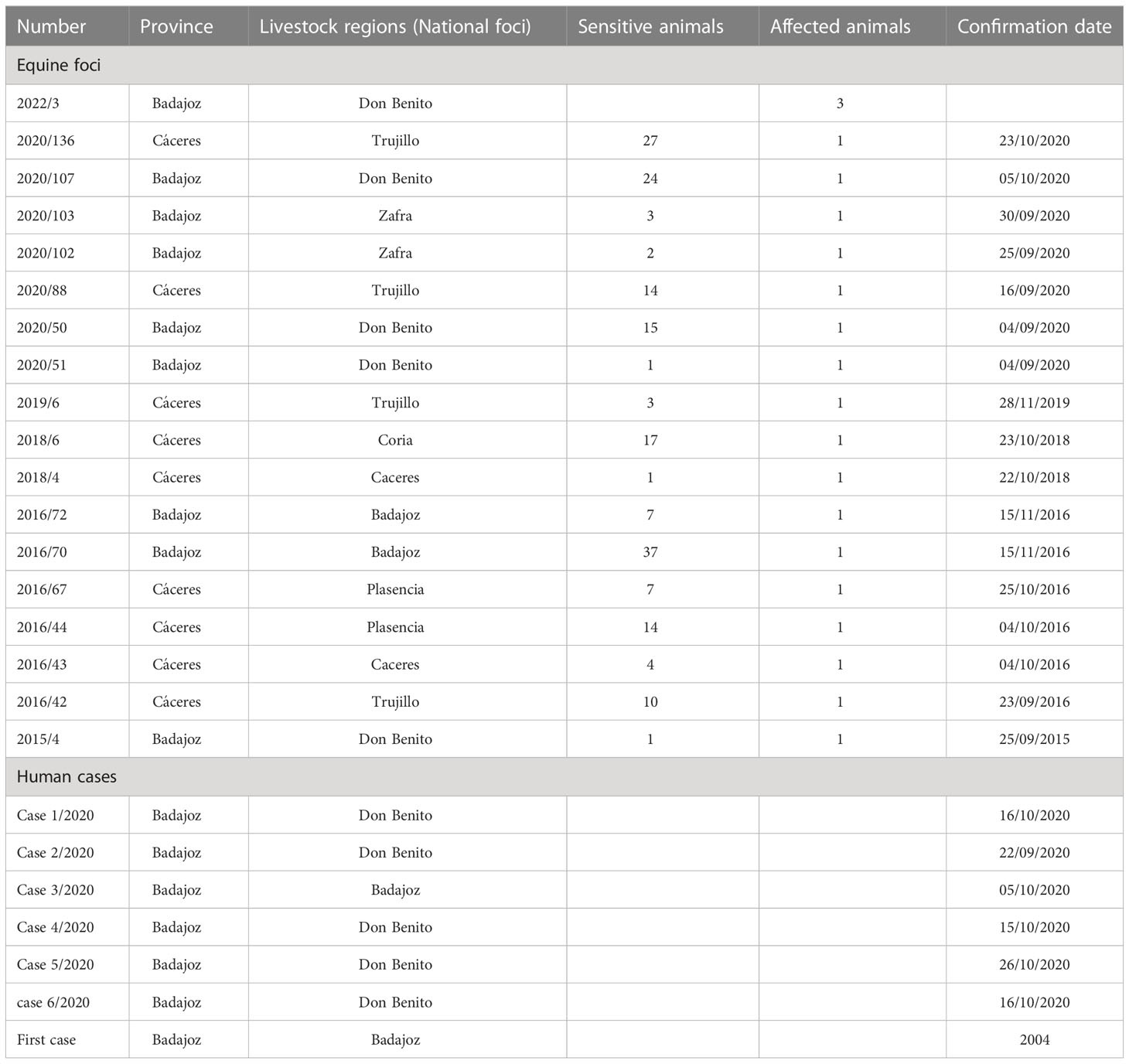
Table 3 Epidemiological information of the equine and human cases in Extremadura, Spain.
Discussion
During the 2020 WNV transmission season, Spain was the second country with more human WNV infections in Europe, registering the highest human WNV outbreak ever in the country with a total of 77 cases. Six patients were infected in Extremadura, the region where the first autochthonous human case was retrospectively identified in 2004 and no other cases had been reported until 2020. The absence of human cases reported in previous seasons in this area could be explained by a lack of clinical suspicion as most infections are asymptomatic (80%). Even when WNV infection is suspected, the diagnosis is complicated and a combination of molecular and serological assays is necessary. Generally, patients with severe clinical symptoms seek medical care, therefore the probability of detecting and reporting them is higher. In this outbreak, the six described cases exhibited fever, the most common clinical signs of the infection, and five of them (83%) presented neurological disease. Taking into account that less than 1% of infected cases develop a WNND, a high number of WNV infections would have gone undiagnosed. Thus, educational plans targeting citizens, clinicians, public health workers, and decision makers should be carried out in order to increase the awareness of WNV and other emerging diseases.
WNVD in humans is associated with mild symptoms (fever, headache, chill, malaise, myalgia, arthralgia, rash, vomiting, nausea, anorexia), most of which were present in the patients described in this outbreak. However, atypical or rare presentations such as myocarditis, pancreatitis, hepatitis, cerebellitis, rhabdomyolysis, and ocular manifestations were not observed even though the patients described in this work presented several of the risk factors related with worse disease evolution and aftermath such as the age (ranging between 50 and 80), living in rural areas in contact with animals, diabetes, hypertension, cardiovascular disease, and chronic lymphocytic leukaemia. In fact, several sequelae have been described in some of these patients such as unstable gait, muscle pains, bradipsychia, dizziness, tremors, forgetfulness, asthenia, hydrocephalus, arthralgia, muscle paints, dyspnoea, and cognitive impairment, especially in patients with chronic morbidities. In general, age and gender are the main intrinsic predisposing factors related to WNVD. It has been reported that individuals older than 50 years of age are more susceptible to severe infections with neurological involvement and that patients older than 75 generally succumb to the infection (Gray and Webb, 2014). The latter could be explained by age-related innate immunosenescence. Regarding gender, more men have been described among WNVD cases, probably because they have more outdoor occupations and are more exposed to mosquito bites. In fact, in rural areas, WNV outbreaks and disease incidence and prevalence have been linked with agricultural activities. In the outbreak described in this work, although there were more men infected, we cannot draw conclusions due to the small number of cases. Other major risk factors are preexisting medical conditions such as cancers, cardiovascular diseases, and diabetes (chronic morbidities), and immunosuppressed individuals have a 40 times higher risk of contracting the disease and dying from WNV infection (Lindsey et al., 2012).
WNV diagnosis was possible in all cases by serological assays. From all patients, CSF, sera, and urine samples were available and analysed. Although all acute samples (<7 dpo) were available in four of the six patients, no positive results were obtained by qRT-PCR. Urine samples from different dpo (from 8 to 35) were analysed by PCR because in several studies viral RNA was detected in urine for much longer (including up to a month postinfection) than in plasma and with higher viral load (Barzon et al., 2014). However, all of the urine samples analysed in this work were negative.
In Extremadura, viral information about the WNV human and equine cases has not been available yet, even though sporadic WNV outbreaks in horses have been reported at least since 2015 (Ministry of Agriculture and Fisheries and Food, 2023a; Ministry of Agriculture and Fisheries and Food, 2023b). A recent study carried out in birds of this region (Bravo-Barriga et al., 2021) revealed WNV lineage 1 circulation, the same lineage that was detected previously in neighbouring areas in birds (Castilla La Mancha, 2007), mosquitoes (Andalusia, 2008; and 2020), and horses (Andalusia, 2010) (Sotelo et al., 2009; García-Bocanegra et al., 2011; Vázquez et al., 2011). These studies showed a high prevalence (18.23%) and active circulation of WNV in wild birds during the period 2017–2019. These seroprevalence levels are higher than those found in other European countries and very similar to those detected in birds from Doñana National Park, an endemic WNV area in Andalusia (López et al., 2011). Another study carried out in dogs in the southwest of Spain revealed the presence of neutralising antibodies against WNV and TBEV, demonstrating the circulation of these viruses in these areas (García-Bocanegra et al., 2018). Moreover, the recent detection of USUV (RNA in mosquitoes and USUV-specific antibodies in birds) and an undetermined flavivirus highlights the widespread circulation of WNV in this endemic area and its co-circulation with USUV and other flaviviruses (Bravo-Barriga et al., 2023). In the six patients studied in this work, cross-reactive IgG antibodies against USUV and TBEV were detected in all the convalescent sera samples tested, but not in the CSF. Although the presence of cross-reactive antibodies against the three flaviviruses was observed in the ELISA and IFA assays, confirmation of WNV infection was possible by neutralisation assays. Taking into account flavivirus co-circulation and the serological cross-reactivity described among these viruses, the laboratory findings should be carefully addressed and a combination of molecular and serological techniques is necessary for a complete diagnosis of this infection. Therefore, although no human infections by USUV or TBEV have been reported in Extremadura until now, when a human WNV infection is suspected in this area, a differential diagnosis should be carried out against these flaviviruses—which may also be endemic in this area—and serological cross-reactions should be excluded.
The history of detection of WNV for more than 15 years both in birds and horses, as well as the increase in human cases described in this work, indicates its establishment and spread in Extremadura, Spain. Moreover, the recent detection of USUV close to urban areas represents a public health threat that requires inclusion in the differential diagnoses in patients with compatible symptoms. Therefore, it is necessary to establish surveillance programs for these emerging flaviviruses and to develop coordinated national plans integrating multisectoral and interregional participation from a one-health approach.
Data availability statement
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
Ethics statement
The studies involving human participants were reviewed and approved by Instituto de Salud Carlos III. Written informed consent for participation was not required for this study in accordance with the national legislation and the institutional requirements.
Author contributions
AV coordinated the study. AM, PM, and SR performed the laboratory screening and biochemical analysis in the regional Hospitals. AV, LH, MS-S, and MP-O performed the laboratory analysis, confirmation, and interpretation of results. AntV, MG, MJ and CM-P performed the clinical case management and description. BFM participated in the epidemiological investigations. DG-B designed and graphed the map of human and animal cases. JR, EF, ED, and AC contributed to the surveillance and epidemiological investigations. All authors contributed to the article and approved the submitted version.
Funding
This research was partially funded by the project PI19CIII_00014 from the Instituto de Salud Carlos III.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Bai, F., Thompson, E. A., Vig, P. J. S., Leis, A. A. (2019). Current understanding of West Nile virus clinical manifestations, immune responses, neuroinvasion, and immunotherapeutic implications. Pathogens 8, 193. doi: 10.3390/pathogens8040193
Barzon, L., Pacenti, M., Franchin, E., Squarzon, L., Sinigaglia, A., Ulbert, S., et al. (2014). Isolation of West Nile virus from urine samples of patients with acute infection. J. Clin. Microbiol. 52, 3411–3413. doi: 10.1128/JCM.01328-14
Barzon, L., Pacenti, M., Ulbert, S., Palù, G. (2015). Latest developments and challenges in the diagnosis of human West Nile virus infection. Expert Rev. Anti Infect. Ther. 13, 327–342. doi: 10.1586/14787210.2015.1007044
Bravo-Barriga, D., Aguilera-Sepúlveda, P., Guerrero-Carvajal, F., Llorente, F., Reina, D., Pérez-Martín, J. E., et al. (2021). West Nile and usutu virus infections in wild birds admitted to rehabilitation centres in extremadura, western Spain 2017–2019. Vet. Microbiol. 255, 109020. doi: 10.1016/j.vetmic.2021.109020
Bravo-Barriga, D., Ferraguti, M., Magallanes, S., Aguilera-Sepúlveda, P., Llorente, F., Pérez-Ramírez, E., et al. (2023). Identification of usutu virus Africa 3 lineage in a survey of mosquitoes and birds from urban areas of Western Spain. Transbound Emerg. Dis. 2023, 10. doi: 10.1155/2023/6893677
Carson, P. J., Konewko, P., Wold, K. S., Mariani, P., Goli, S., Bergloff, P., et al. (2006). Long-term clinical and neuropsychological outcomes of West Nile virus infection. Clin. Infect. Dis. 43, 723–730. doi: 10.1086/506939
Casades-Martí, L., Holgado-Martín, R., Aguilera-Sepúlveda, P., Llorente, F., Pérez-Ramírez, E., Jiménez-Clavero, M. Á, et al. (2023). Risk factors for exposure of wild birds to West Nile virus in a gradient of wildlife-livestock interaction. Pathogens 12 (1), 83. doi: 10.3390/pathogens12010083
ECDC (2019) West Nile Virus infection. annual epidemiological report for 2018 (Stockholm). Available at: https://www.ecdc.europa.eu/en/publications-data/west-nile-virus-infection-annual-epidemiological-report-2018 (Accessed January 29, 2023).
ECDC (2020) Epidemiological update: West Nile virus transmission season in Europe 2020. Available at: https://www.ecdc.europa.eu/en/news-events/epidemiological-update-west-nile-virus-transmission-season-europe-2020 (Accessed January 29, 2023).
ECDC (2022a) Epidemiological update: West Nile virus transmission season in Europe 2021. Available at: https://www.ecdc.europa.eu/en/news-events/epidemiological-update-west-nile-virus-transmission-season-europe-2021.
ECDC (2022b) Weekly updates: 2022 West Nile virus transmission season. Available at: https://www.ecdc.europa.eu/en/west-nile-fever/surveillance-and-disease-data/disease-data-ecdc.
European Commission (2018)Commission implementing decision (EU) 2018/945 of 22 June 2018 on the communicable diseases and related special health issues to be covered by epidemiological surveillance as well as relevant case definitions (Accessed January 29, 2023).
García-Bocanegra, I., Jaén-Téllez, J. A., Napp, S., Arenas-Montes, A., Fernández-Morente, M., Fernández-Molera, V., et al. (2011). West Nile Fever outbreak in horses and humans, spai. Emerg. Infect. Dis. 17, 2397–2399. doi: 10.3201/eid1712.110651
García-Bocanegra, I., Jurado-Tarifa, E., Cano-Terriza, D., Martínez, R., Pérez-Marín, J. E., Lecollinet, S. (2018). Exposure to West Nile virus and tick-borne encephalitis virus in dogs in Spain. Transbound Emerg. Dis. 65, 765–772. doi: 10.1111/tbed.12801
García San Miguel Rodríguez-Alarcón, L., Fernández-Martínez, B., Sierra Moros, M. J., Vázquez, A., Julián Pachés, P., García Villacieros, E., et al. (2021). Unprecedented increase of West Nile virus neuroinvasive disease, Spain, summer 2020. Eurosurveillance 26 (19), pii=2002010. doi: 10.2807/1560-7917.ES.2021.26.19.2002010
Gray, T., Webb, C. E. (2014). A review of the epidemiological and clinical aspects of West Nile virus. Int. J. Gen. Med. 7, 193–203. doi: 10.2147/IJGM.S59902
Guerrero-Carvajal, F., Bravo-Barriga, D., Martín-Cuervo, M., Aguilera-Sepúlveda, P., Ferraguti, M., Jiménez-Clavero, M. Á., et al. (2021). Serological evidence of co-circulation of West Nile and usutu viruses in equids from western Spain. Transbound Emerg. Dis. 68, 1432–1444. doi: 10.1111/tbed.13810
Hasbun, R., Garcia, M. N., Kellaway, J., Baker, L., Salazar, L., Woods, S. P., et al. (2016). West Nile Virus retinopathy and associations with long term neurological and neurocognitive sequelae. PloS One 11, e0148898. doi: 10.1371/journal.pone.0148898
Hughes, J. M., Wilson, M. E., Sejvar, J. J. (2007). The long-term outcomes of human West Nile virus infection. Clin. Infect. Dis. 44, 1617–1624. doi: 10.1086/518281
ISCIII (2021) Fiebre del nilo occidental. Available at: https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Documents/PROTOCOLOS/Protocolo%20vigilancia%20fiebre%20Nilo%20occidental_RENAVE.pdf (Accessed May 10, 2021).
ISCIII (2022). Informe epidemiológico sobre la situación de la fiebre del nilo occidental en españa. años 2021 y 2022 (Instituto de Salud Carlos III: Centro Nacional de Epidemiología). Available at: https://www.isciii.es/QueHacemos/Servicios/VigilanciaSaludPublicaRENAVE/EnfermedadesTransmisibles/Documents/archivos%20A-Z/Fiebre_Nilo_Occidental/INFORME_RENAVE_FNO%202021-2022.pdf.
Kaptoul, D., Viladrich, P. F., Domingo, C., Niubó, J., Martínez-Yélamos, S., de Ory, F., et al. (2007). West Nile Virus in Spain: report of the first diagnosed case (in Spain) in a human with aseptic meningitis. Scand. J. Infect. Dis. 39, 70–71. doi: 10.1080/00365540600740553
Konjevoda, S., Dzelalija, B., Canovic, S., Pastar, Z., Savic, V., Tabain, I., et al. (2019). West Nile Virus retinitis in a patient with neuroinvasive disease. Rev. Soc. Bras. Med. Trop. 52, e20190065. doi: 10.1590/0037-8682-0065-2019
Lindsey, N. P., Staples, J. E., Lehman, J. A., Fischer, M. (2012). Medical risk factors for severe West Nile virus disease, united states 2008–2010. Am. J. Trop. Med. Hyg 87, 179–184. doi: 10.4269/ajtmh.2012.12-0113
López, G., Jiménez-Clavero, M. Á., Vázquez, A., Soriguer, R., Gómez-Tejedor, C., Tenorio, A., et al. (2011). Incidence of West Nile virus in birds arriving in wildlife rehabilitation centers in southern Spain. Vector-Borne Zoonotic Dis. 11, 285–290. doi: 10.1089/vbz.2009.0232
López-Ruiz, N., Montaño-Remacha, M., del, C., Durán-Pla, E., Pérez-Ruiz, M., Navarro-Marí, J. M., et al. (2018). West Nile Virus outbreak in humans and epidemiological surveillance, west Andalusia, spai. Eurosurveillance 23 (14), pii=17-00261. doi: 10.2807/1560-7917.ES.2018.23.14.17-00261
Lustig, Y., Sofer, D., Bucris, E. D., Mendelson, E. (2018). Surveillance and diagnosis of West Nile virus in the face of flavivirus cross-reactivity. Front. Microbiol. 9. doi: 10.3389/fmicb.2018.02421
Ministry of Agriculture and Fisheries and Food (2023a). Available at: https://www.mapa.gob.es/es/ganaderia/temas/sanidad-animal-higiene-ganadera/sanidad-animal/enfermedades/fiebre-nilo-occidental/F_O_Nilo.aspxhttps://www.mapa.gob.es/es/ganaderia/temas/sanidad-animal-higiene-ganadera/sanidad-animal/enfermedades/fiebre-nilo-occidental/F_O_Nilo.aspx.
Ministry of Agriculture and Fisheries and Food (2023b) Actualización de la situación epidemiológica de la fiebre del nilo occidental (West Nile fever). Available at: https://www.mapa.gob.es/es/ganaderia/temas/sanidad-animal-higiene-ganadera/informefno_tcm30-435293.pdf.
Napp, S., Llorente, F., Beck, C., Jose-Cunilleras, E., Soler, M., Pailler-García, L., et al. (2021). Widespread circulation of flaviviruses in horses and birds in northeastern Spain (Catalonia) between 2010 and 2019. Viruses 13 (12), 2404. doi: 10.3390/v13122404
Scientific Committee for Transfusion Safety (2021) Virus del nilo occidental (Madrid). Available at: https://www.mscbs.gob.es/profesionales/saludPublica/medicinaTransfusional/acuerdos/docs/Virus_Nilo_Occidental.pdf (Accessed January 29, 2023).
Sotelo, E., Fernandez-Pinero, J., Llorente, F., Agüero, M., Hoefle, U., Blanco, J. M., et al. (2009). Characterization of West Nile virus isolates from Spain: new insights into the distinct West Nile virus eco-epidemiology in the Western Mediterranean. Virology 395, 289–297. doi: 10.1016/j.virol.2009.09.013
Spanish Ministry of Health (2020) Meningoencefalitis por el virus del nilo occidental en españa (2a actualización-cierre de temporada). Available at: https://www.mscbs.gob.es/profesionales/saludPublica/ccayes/alertasActual/docs/20201203_ERR_Nilo_Occidental.pdf (Accessed January 29, 2023).
Tardei, G., Ruta, S., Chitu, V., Rossi, C., Tsai, T. F., Cernescu, C. (2000). Evaluation of immunoglobulin m (IgM) and IgG enzyme immunoassays in serologic diagnosis of West Nile virus infection. J. Clin. Microbiol. 38, 2232–2239. doi: 10.1128/JCM.38.6.2232-2239.2000
Vanhomwegen, J., Beck, C., Desprès, P., Figuerola, A., García, R., Lecollinet, S., et al. (2017). Circulation of zoonotic arboviruses in equine populations of mallorca island (Spain). Vector Borne Zoonotic Dis. 17 (5), 340–346. doi: 10.1089/vbz.2016.2042
Vázquez, A., Herrero, L., Negredo, A., Hernández, L., Sánchez-Seco, M. P., Tenorio, A. (2016). Real time PCR assay for detection of all known lineages of West Nile virus. J. Virol. Methods 236, 266–270. doi: 10.1016/j.jviromet.2016.07.026
Vázquez, A., Ruiz, S., Herrero, L., Moreno, J., Molero, F., Magallanes, A., et al. (2011). West Nile And usutu viruses in mosquitoes in Spain 2008-2009. Am. J. Trop. Med. Hyg 85, 178–181. doi: 10.4269/ajtmh.2011.11-0042
Vázquez, A., Sánchez-Seco, M. P., Ruiz, S., Molero, F., Hernández, L., Moreno, J., et al. (2010). Putative new lineage of West Nile virus, Spain. Emerg. Infect. Dis. 16, 549–552. doi: 10.3201/eid1603.091033
Keywords: West Nile virus, human infection, flaviviruses, diagnosis, molecular and serological methods, surveillance
Citation: Macias A, Martín P, Pérez-Olmeda M, Fernández-Martínez B, Gómez-Barroso D, Fernández E, Ramos JM, Herrero L, Rodríguez S, Delgado E, Sánchez-Seco MP, Galán M, Corbacho AJ, Jimenez M, Montero-Peña C, Valle A and Vázquez A (2023) West Nile virus emergence in humans in Extremadura, Spain 2020. Front. Cell. Infect. Microbiol. 13:1155867. doi: 10.3389/fcimb.2023.1155867
Received: 31 January 2023; Accepted: 19 May 2023;
Published: 04 July 2023.
Edited by:
Josep Quer, Vall d’Hebron Research Institute (VHIR), SpainReviewed by:
Francesca Rovida, University of Pavia, ItalyFrancesco Cerutti, Ospedale Amedeo di Savoia, Italy
Copyright © 2023 Macias, Martín, Pérez-Olmeda, Fernández-Martínez, Gómez-Barroso, Fernández, Ramos, Herrero, Rodríguez, Delgado, Sánchez-Seco, Galán, Corbacho, Jimenez, Montero-Peña, Valle and Vázquez. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Ana Vázquez, YS52YXpxdWV6QGlzY2lpaS5lcw==