
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cell. Infect. Microbiol., 12 June 2023
Sec. Clinical Microbiology
Volume 13 - 2023 | https://doi.org/10.3389/fcimb.2023.1155320
This article is part of the Research TopicAntibiotics Overuse as the Driving Force behind Antimicrobial ResistanceView all 6 articles
 Anna Maria Azzini1*
Anna Maria Azzini1* Giorgia Be1,2Laura Naso3Lorenza Lambertenghi1Nicola Duccio Salerno1Ilaria Coledan1,4Alda Bazaj5Massimo Mirandola1Jessica Miotti6
Giorgia Be1,2Laura Naso3Lorenza Lambertenghi1Nicola Duccio Salerno1Ilaria Coledan1,4Alda Bazaj5Massimo Mirandola1Jessica Miotti6 Fulvia Mazzaferri1
Fulvia Mazzaferri1 Simone Accordini6Giuliana Lo Cascio3,7†
Simone Accordini6Giuliana Lo Cascio3,7† Evelina Tacconelli1†
Evelina Tacconelli1†Introduction: Residency in LTCFs increases the likelihood of colonization with multidrug resistant Gram-negative bacteria (MDR-GNB). We assessed the prevalence and risk factors for enteric colonization by III-generation cephalosporins-resistant and carbapenem-resistant (CR) GNB in a large group of LTCFs in a high endemic setting. We also assessed the prevalence and risk factors for C. difficile colonization.
Methods: A point prevalence survey with rectal screening (RS) was conducted in 27 LTCFs in north Italy. Epidemiological and clinical variables on the survey day, history of hospitalization and surgery within one year, and antibiotics within three months, were collected. The presence of III-generation cephalosporin resistant and CR GNB was assessed using a selective culture on chromogenic medium and PCR for carbapenemase detection. The presence of C. difficile was assessed using ELISA for GDH and RT-PCR to identify toxigenic strains. Multi-variable analyses were performed using two-level logistic regression models.
Results: In the study period 1947 RSs were performed. The prevalence of colonization by at least one GNB resistant to III-generation cephalosporin was 51% (E. coli 65%, K. pneumoniae 14% of isolates). The prevalence of colonization by CR GNB was 6%. 6% of all isolates (1150 strains) resulted in a carbapenem-resistant K. pneumoniae, and 3% in a carbapenem-resistant E. coli. KPC was the most frequent carbapenemase (73%) identified by PCR, followed by VIM (23%). The prevalence of colonization by C. difficile was 11.7%. The presence of a medical device (OR 2.67) and previous antibiotic use (OR 1.48) were significantly associated with III-generation cephalosporin resistant GNB colonization. The presence of a medical device (OR 2.67) and previous hospitalization (OR 1.80) were significantly associated with CR GNB. The presence of a medical device (OR 2.30) was significantly associated with C. difficile colonization. Main previously used antibiotic classes were fluoroquinolones (32% of previously treated subjects), III-generation cephalosporins (21%), and penicillins (19%).
Conclusion: Antimicrobial stewardship in LTCFs is a critical issue, being previous antibiotic treatment a risk factor for colonization by MDR-GNB. The prevalence of colonization by III-generation cephalosporin and CR GNB among LTCF residents also underlines the importance to adhere to hand hygiene indications, infection prevention and control measures, and environmental hygiene protocols, more achievable than rigorous contact precautions in this type of social setting.
The increase in the elderly population in a social context characterized by the ever-decreasing availability and possibility of support and care within the family nucleus, have determined the strengthening of assistance in ad hoc long-term care facilities (LTCFs), such as nursing homes, residential care centers, chronic disease hospitals, and rehabilitation centers (Strausbaugh et al., 1996; OECD, 2011; Suetens, 2012). Although the numbers vary from country to country, approximately 2–5% of the developed world’s older population resides in some type of LTCFs (Ribbe et al., 1997).
The elderly has an increased risk of developing infections (van Duin, 2012), due both to physiological changes linked to aging (Castle, 2000; Heppner et al., 2013), to the onset of chronic diseases (Juthani-Mehta and Quagliarello, 2010; Falcone et al., 2021), and to the need for medical devices (e.g., urinary catheter) (Wang et al., 2012). Infections are the most common cause of LTCFs’ residents morbidity and mortality and transfers to acute care hospitals (Burns et al., 2015; Childs et al., 2019), therefore, it is not surprising that antibiotics are among the most prescribed medications in this setting (Nicolle et al., 2000; Latour et al., 2012). According to point prevalence surveys (PPSs) in Europe, USA, and Australia, between 3% and 15% of LTCF residents are given antibiotics at any time (McClean et al., 2012; Stuart et al., 2012; van Buul et al., 2012), and there is a 40-70% likelihood of exposure to at least one course of antibiotics for residents who remain in a nursing home for at least 6 months (Benoit et al., 2008). Around half of these treatments are inappropriate or unnecessary thus increasing the potential for the selection of multi-drug resistant bacteria (Loeb, 2000; Nicolle et al., 2000; Gavazzi and Krause, 2002; McClean et al., 2011; Rotjanapan et al., 2011; Drinka et al., 2013). In 2013 the PPS on healthcare associated infections and antimicrobial use in European LTCFs (HALT 2) documented that 4.4% of the subjects admitted to the involved LTCFs were taking at least one antibiotic, but in half of the cases in the absence of a healthcare-related infection (ECDC-WHO). Similar results were described by HALT 3 in 2017 (Ricchizzi et al., 2018), with common causes of antibiotic misuse in LTCFs the unnecessary antibiotic treatments for bacterial colonization (e.g., asymptomatic bacteriuria), for urinary tract infection prophylaxis, or for viral infections (e.g., influenza), and the longer-than-necessary antibiotic’s course duration in the absence of treatment reassessment at around day 3 after its prescription (Dyar et al., 2015).
Prior antibiotic treatments, as well as the total dependence of residents on nurse care for their daily living activities, expose them both to the selection and horizontal transmission of antibiotic resistant organisms, in a generally understaffed residential setting where is difficult to strictly adhere to infection prevention and control strategies and to hand hygiene indications (Arena et al., 2018; Ambretti et al., 2019).
The emergence of multidrug-resistant organisms (MDROs) is a major public health concern (Infectious Diseases Society of America (IDSA) et al., 2011). In 2020 in Italy, as in other south-eastern EU-EEA countries, more than 25% of E. coli and more than 50% of K. pneumoniae invasive isolates were resistant to III-generation cephalosporins, percentages of carbapenem resistance above 10% were reported in P. aeruginosa and even higher in K. pneumoniae (25%-50%) and in Acinetobacter spp. (> 50%), thus describing a highly endemic setting (European Centre for Disease Prevention and Control, 2022).
Multi-drug antibiotic resistance also affects residents in LTCFs that, infected or colonized, become a reservoir (Willemsen et al., 2015; Ruiz-Garbajosa et al., 2016; van den Dool et al., 2016; Nucleo et al., 2018; Nguyen et al., 2019): extended-spectrum ß-lactamase (ESBL) Enterobacterales, carbapenem-resistant Enterobacterales, multidrug resistant P. aeruginosa and A. baumannii are increasing in prevalence inside LTCFs (Perez et al., 2007; Willemsen et al., 2015; Ruiz-Garbajosa et al., 2016; van Duin and Paterson, 2016; Nucleo et al., 2018; Horcajada et al., 2019). Although it is not an MDRO, also Clostridioides difficile represents a worldwide public health concern, as it is one of the major causes of antibiotic-associated infections in healthcare settings, especially among older people living in nursing homes (Barbut et al., 2011; Rodriguez et al., 2014).
Knowledge of individual level risk factors for colonization in LTCFs’ residents is mainly limited to small groups. A recent systematic review identified studies with a small sample size and LTCFs across countries differing in case-mix, age and care provided (Flokas et al., 2017), hampering the possibility of defining the exact burden of the problem. The aim of the present study was to describe the prevalence and risk factors for enteric colonization by C. difficile, III-generation cephalosporin resistant gram-negative bacteria (GNB) and CR GNB in a large sample of residents of 27 LTCFs in Veneto, a Northern Italian region.
Between July 2018 and June 2019, we conducted a PPS to assess both the frequency of healthcare-related infections and the enteric colonization status by MDR Gram negative bacteria and C. difficile in the population of elderly residents of 27 LTCFs in the Veneto Region. Participation in the survey was voluntary, but at least one facility for each province of the region was enrolled. The 27 facilities were not involved simultaneously but at different times based on the local Ethic Committee’s approval, the willingness of local personnel to collaborate with researchers in the collection of the study-specific biological samples and the possibility of the reference microbiology laboratory to accept and process the samples. The survey was proposed to all patients living full-time in the LTCF, present in the facility on the day of the PPS and admitted at least 48 hours before the survey. Only patients who were able to provide written informed consent, or whose legal representative consented, were enrolled. The survey was carried out in a single day for each facility. In the case of facilities with more than 50 residents living in different wards, the survey lasted several consecutive days, however, all the beds in one ward had to be surveyed on the same day. For each enrolled patient, the variables measured included the type and etiology of concurrent infections and respective antibiotic therapy, any antibiotic treatments in the previous 3 months, hospital admissions and surgery in the previous 12 months and case mix factors, such as presence of urinary catheter, vascular catheter, pressure sores, skin wounds other than bedsores, urinary and/or fecal incontinence, low mental status, and impaired mobility. For each enrolled host, a rectal swab was performed to assess the status of colonization by MDR Gram negative bacteria (Enterobacterales and non-fermenting GNB resistant to III-generation cephalosporin and/or carbapenem). On the PPS day, from each enrolled resident and independently from the presence of acute gastrointestinal symptoms, a fecal sample was also taken in sterile collection cups, refrigerated and transported to the laboratory within 24 hours to assess the C.difficile colonization status.
For screening of III-generation cephalosporin and carbapenem-resistant GNB, rectal swabs were inoculated onto ChromID ESBL agar (bioMerieux, Marcy l’Etoile, France) with an Ertapenem disk (10ug) and on Mac Conkey agar with a Meropenem disk (10ug) (Carrër et al., 2010). Plates were incubated at 35 ± 2°C under aerobic conditions for 24h. Isolates were identified at the species level using the MALDI-TOF Vitek MS System (bioMerieux, Marcy l’Etoile, France). Resistance to carbapenems were interpreted according EUCAST criteria and Italian AMCLI (Associazione Microbiologi Clinici Italiani) recommendations (Eucast; Aschbacher et al., 2020). A diameter zone < 30 mm for meropenem on MacConkey and/or < 28 mm for ertapenem on ChromID ESBL agar were considered suspicious for carbapenem resistance and the colony growth within this size zone was confirmed with immunochromatographic lateral flow assay NG-test Carba5 (NG Biotech) (from now Carba5 test). The Vitek2 system (bioMerieux, Marcy l’Etoile, France) was used to perform antimicrobial susceptibilities and to confirm carbapenem resistance in the selected strains (Hrabák et al., 2014).
All carbapenem-resistant strains detected by screening culture and confirmed by Carba5 test were further investigated by a home-made PCR using published primers and conditions (Poirel et al., 2011), targeting blaKPC, blaVIM, blaIMP, blaOXA-48, blaNDM, blaOXA-23 and blaOXA-24 type genes, to identify on single isolated strains the presence of specific genes encoding for carbapenemase. All fecal samples were analyzed with Premier C. difficile GDH qualitative enzyme immunoassay (Meridian Bioscience Europe S.r.l.- Italy) screening test to detect Clostridioides difficile glutamate dehydrogenase (GDH) (Terveer et al., 2017; Leitner et al., 2020). All GDH-positive specimens were further tested with Illumigene® (Meridian Bioscience Europe S.r.l.- Italy), a loop-mediated isothermal amplification assay (LAMP) to detect a gene segment of the tcdA gene in the pathogenicity locus (PaLoc) present in all known toxigenic C. difficile strains.
Continuous variables were summarized as means with standard deviations (SD). Percentages were calculated for categorical variables. Two-level (level 1 unit: subject; level 2 unit: LTCF) random-intercept logistic regression models were used to assess the association of surgery in the previous 12 months, presence of at least one device, antibiotic treatment in the previous 3 months, and hospitalizations in the previous 12 months (potential risk factors) with rectal colonization by III-generation cephalosporins-resistant GNB, by carbapenem-resistant GNB, or by C. difficile (three different outcomes). Gender and age were included as adjustment variables in the three models. Tetrachoric or biserial correlation coefficients were computed to assess collinearity of two covariates. Surgery in the previous 12 months was dropped from the models because of collinearity with previous hospitalizations (tetrachoric correlation coefficient = 0.85) and because of data sparseness (only 3% of the subjects had undergone surgical procedures in the past year). All statistical analyses were performed using STATA software, version 17 (College Station, TX: StataCorp LP).
This study was approved by the Ethics Committee for Clinical Trials of the Provinces of Verona and Rovigo: n° 25294, 26/04/2018.
27 LTCFs were included in the survey. Based on the patient’s frailty degree and consequently on the intensity of requested daily assistance, half of these LTCFs (12 facilities) were classified as general nursing homes (providing principally care to seniors with severe illnesses or injuries), 8 as residential homes (usually providing personal care, housekeeping and three meals a day), 4 as mixed LTCF (providing mixed services for elderly or other resident populations, such as those who necessitate rehabilitation or palliative care) (Nucleo et al., 2018). For the remaining 3 facilities the typology of assistance was not provided. At the time of the PPS, the facilities had an average of 162 total beds (mean, SD ± 202), with an occupancy rate of 96.2%. All facilities offered continuous and permanent nursing care, with a mean of 27 nurses available 24h/24h (median 16.5), joined by a mean of 64 (median 45) auxiliary healthcare staff responsible mainly for carrying out the personal hygiene of the hosts. None of the facilities provided an internal medical doctor, but nearly all of them offered medical assistance through the support of external general practitioners associated to the facility by means of a formal agreement with the local public health authority.
From an overall population of 2983 subjects, 1947 residents were enrolled: 1440 women and 507 men (Table 1). The frequency of participation to the study fluctuated between 59% and 76% in 25 of the 27 structures involved; in a single facility with 150 residents, it reached 94%, while the lowest adhesion (38%) was obtained in a facility hosting 90 individuals. Participation in the study was mainly influenced by the difficulty in obtaining the informed consent from a population of subjects with cognitive impairment and/or without a legal representative. The mean age of the population was 84.97 years (range 38-115; SD ± 9.71), and more than half were older than 85 years. About 85% (1673/1947) of the subjects resided in the facility for at least 12 months, with an average LTCF-stay of 5.19 years (SD ± 14.77). 14% (282/1947) of residents had been hospitalized at least once during the previous twelve months: half of the hospitalizations occurring in a medical or geriatric setting and lasting an average of 17 days, and one fifth occurring in a specialized medical setting. 8% of residents had been hospitalized in a surgical setting, but only 60 subjects (3%) had undergone surgery in the previous year and 11 (0.5%) in the previous month. 25% (488/1947) of the enrolled patients were totally bedridden and 54% (1061/1947) showed mobility impairment; bedsores and trophic ulcers interested 346 patients (18%). Nearly two-thirds of the studied population presented fecal (1304/1947) and/or urinary (1328/1947) incontinence and more than 75% (1502/1947) had mental impairment from mild severity to stupor and confusion. On the day the survey was conducted, 382 residents (19%) had in place at least one medical device, and 118 of them had more than one. As described in Table 2, the most frequently used medical device was the urinary catheter, followed by endovascular catheter, and percutaneous endoscopic gastrostomy. There were no patients carrying abdominal drainage.
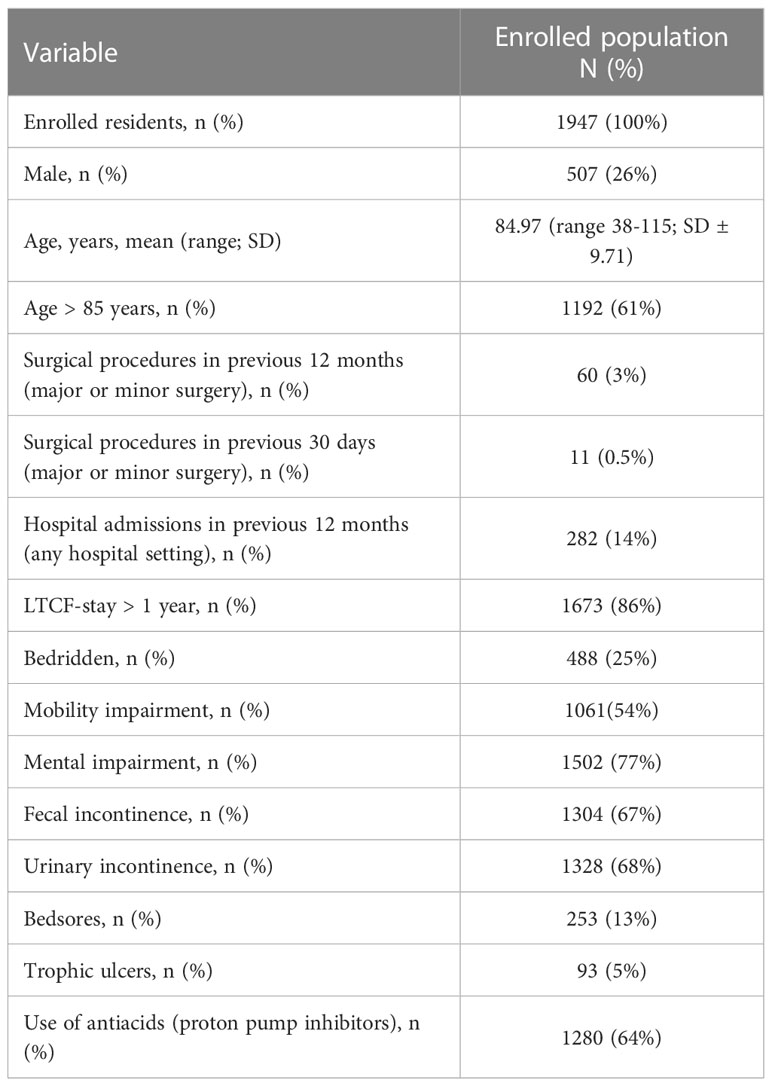
Table 1 Characteristics of the Long-Term Care Facilities’ enrolled patients.
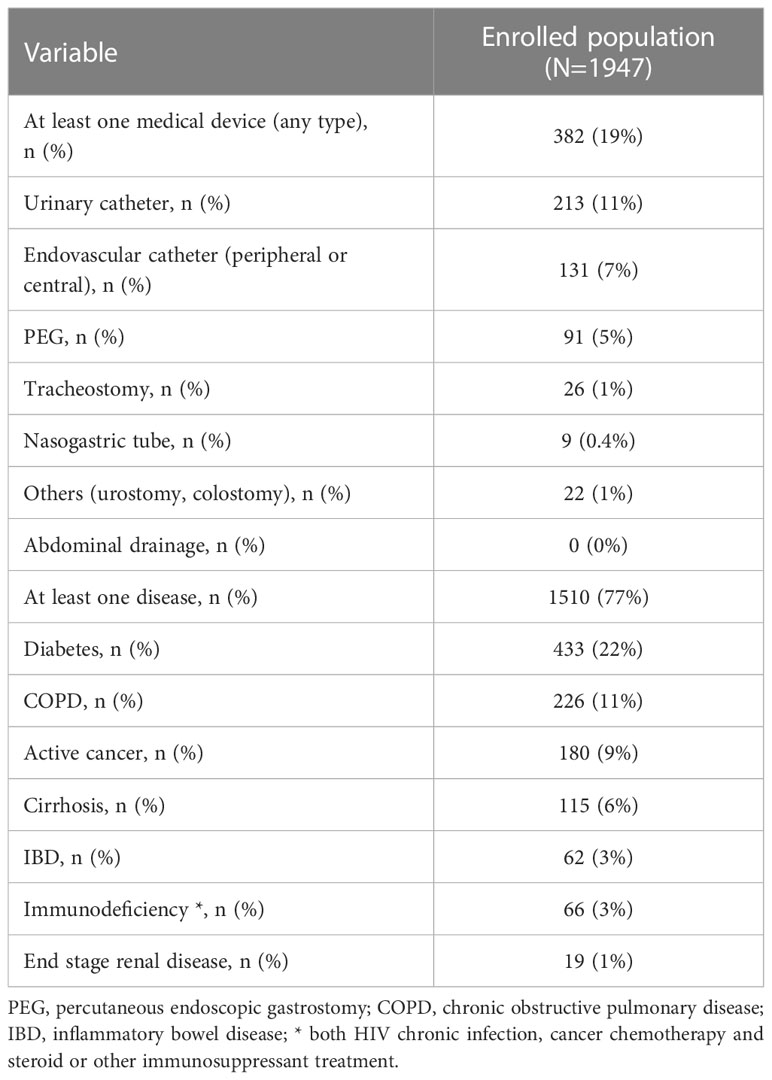
Table 2 Enrolled populations’ medical devices and underlying health impairment.
In our sample, 1510 patients (77%) presented at least one cause of health impairment (Table 2), diabetes was the most represented (22%, 433/1947), followed by COPD (11%, 226/1947) and active cancer (9%, 180/1947). Immunodeficiency secondary to active antineoplastic treatment or steroids or other immunosuppressant drugs interested 3% (57/1947) of the population. 9 subjects had chronic HIV infection.
On the PPS day, only 22 subjects (1%) were on antimicrobial therapy. All of them had at least one healthcare associated infection, for a total of 25 separate infective episodes (Table 3). Etiological diagnosis was rarely available; almost all the infectious episodes except one had been acquired within the facility.
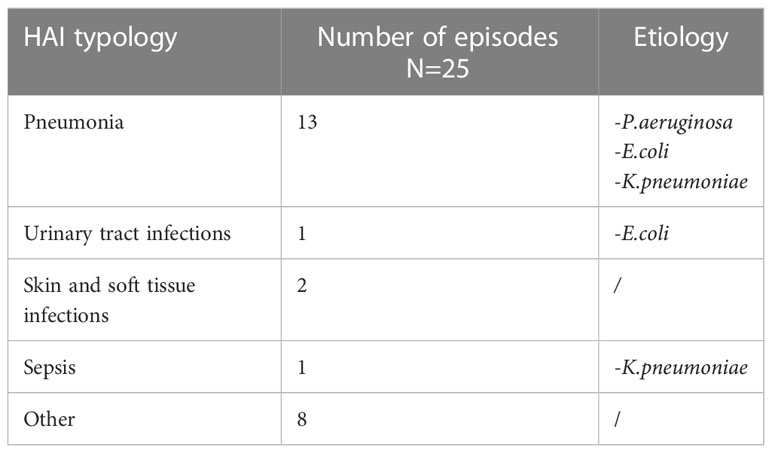
Table 3 Healthcare associated infections (HAI).
567 subjects (29%) had taken at least one antibiotic in previous 90 days, 61% of which only one drug. The preferred route of administration had been the oral one (68%, 596/873 prescribed molecules), followed by the intravenous one (29%, 255/873). 76% of all 873 prescribed drugs had a therapeutic indication, mainly for respiratory tract infections (43%) and lower urinary tract infections (33%), but in 12% of them it was not possible to trace the actual indication. The remaining 179 prescriptions had a prophylactic indication, above all for the prevention of urinary tract infection in catheterized patient (25%) and of enteritis in patients with relapsing diarrhea (25%), but a clear indication was not available in about half of these prescriptions. Almost the totality of all prescriptions had been made inside the LTCFs (91%), while the rest had been prescribed in hospital, during previous hospitalization. Table 4 describes all the antibiotics prescribed in previous 90 days for any indication.
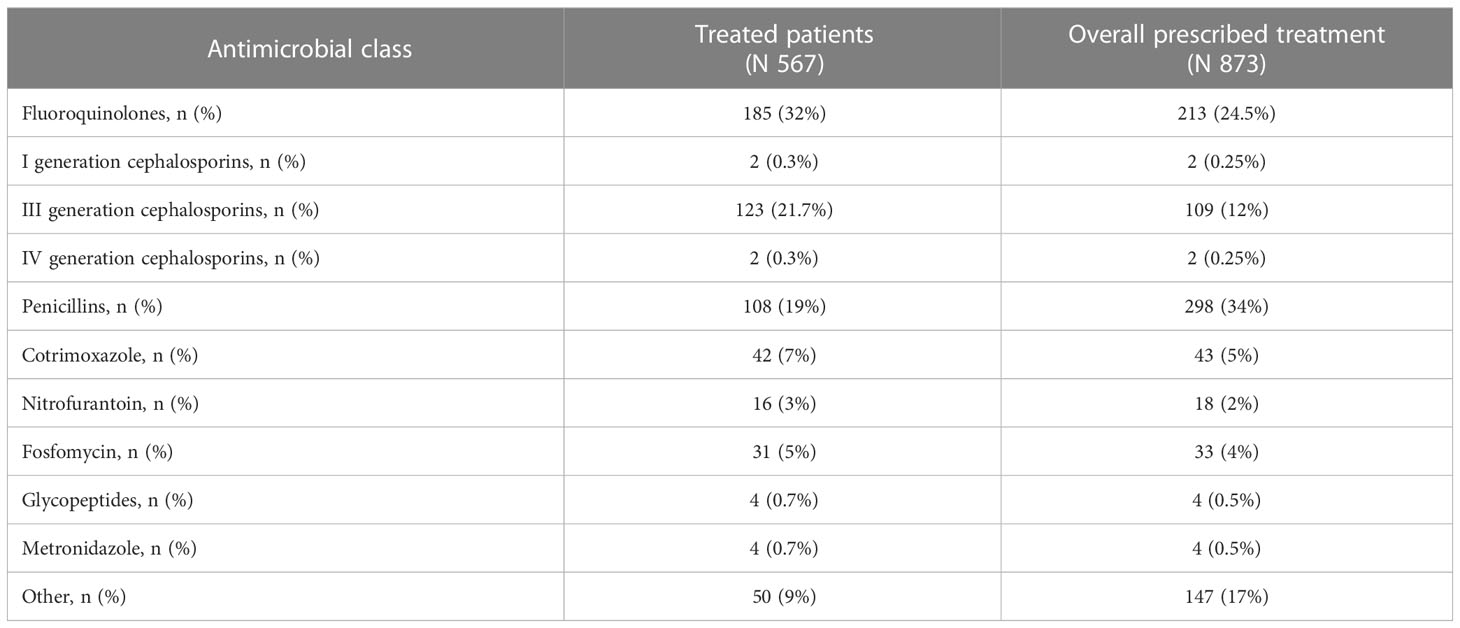
Table 4 Antibiotics prescribed in previous 90 days, any indication.
Overall, 1947 rectal swabs were collected, one for each enrolled patient. By selective culture, 991 (51%) subjects were colonized by at least one strain resistant to III-generation cephalosporins, in 15% of colonized subjects the rectal swab tested positive for two, and in 2% for three different strains. 119 patients (6% of the entire enlisted population) were colonized by at least one CR GNB.
Overall, 1150 gram-negative strains growing on ChromID ESBL agar were identified (Figure 1), 125 of which (11%) resulted carbapenem-resistant on ertapenem-meropenem disk diffusion test (Figure 2).
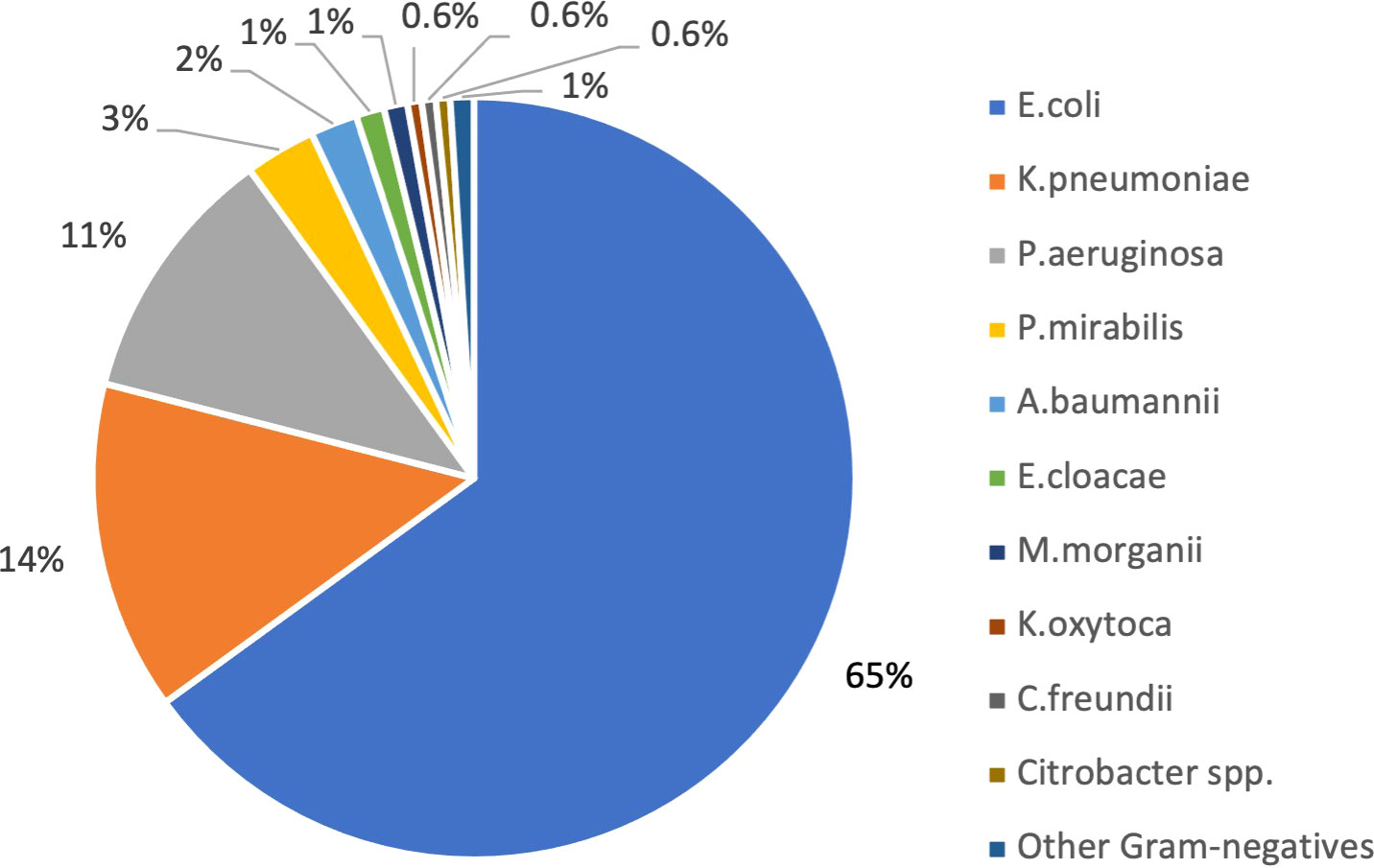
Figure 1 Gram negative bacteria isolated on rectal swab by selective ChromID ESBL agar medium (N 1150).
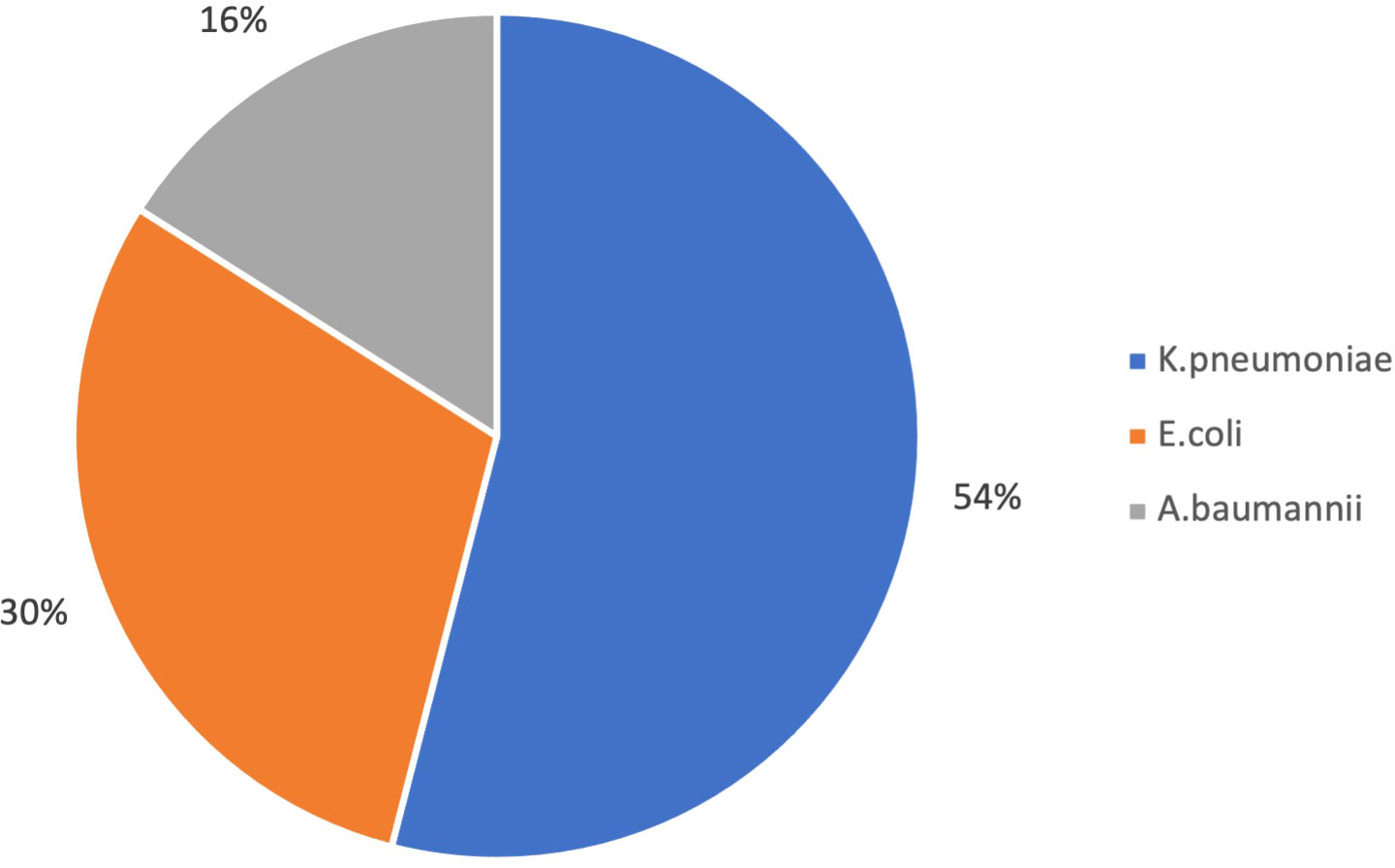
Figure 2 Carbapenem-resistant Gram negative bacteria isolated on rectal swab by selective culture (N 125).
Carba5 test showed the presence of carbapenemases in 78 of them, corresponding to a prevalence of 3.5% patients colonized by at least one carbapenemase-producing micro-organisms. In particular Carba5 test detected a carbapenemase in 75% of carbapenem-resistant Enterobacterales and, as expected, in 0% of A.baumannii strains carbapenem-resistant on selective culture (Table 5).
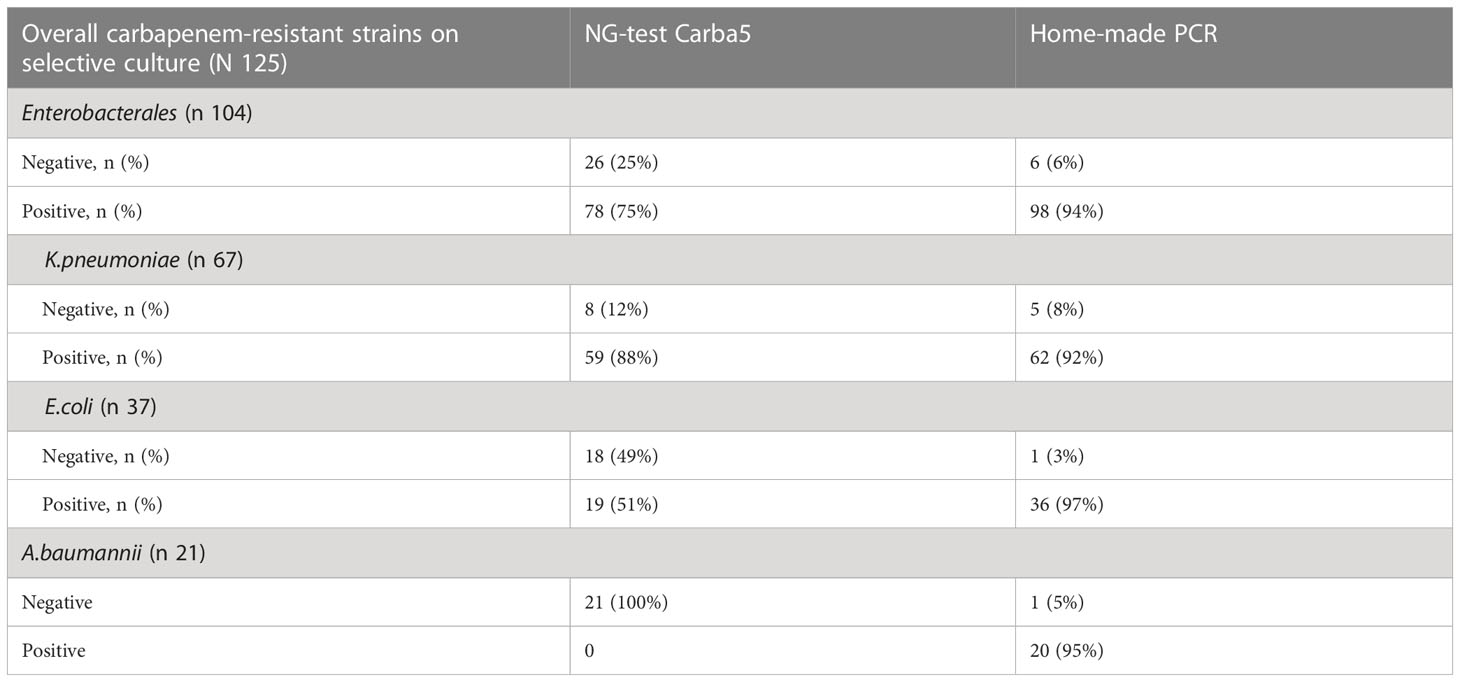
Table 5 Comparison between NG-test Carba5 and home-made PCR results performed on carbapenem-resistant Gram-negative bacteria isolated on rectal swab by selective culture.
Results of home-made PCR targeting blaKPC-, blaVIM-, blaIMP-, blaOXA-, blaNDM- type genes on the 125 carbapenem-resistant strains detected by culture did not find any resistant-gene encoding for carbapenemase in 7 strains (5 K. pneumoniae, 1 E.coli and 1 A. baumannii) and at least a resistant-gene encoding for carbapenemase in 98 (94%) of carbapenem-resistant Enterobacterales and in 20 (95%) of carbapenem-resistant A.baumannii (Table 5).
Carba5 test found KPC in 57 carbapenem-resistant strains (73%), followed by VIM in 23% (18 strains). Only two strains tested positive for NDM and one for OXA-48-like carbapeneamase (Table 6).
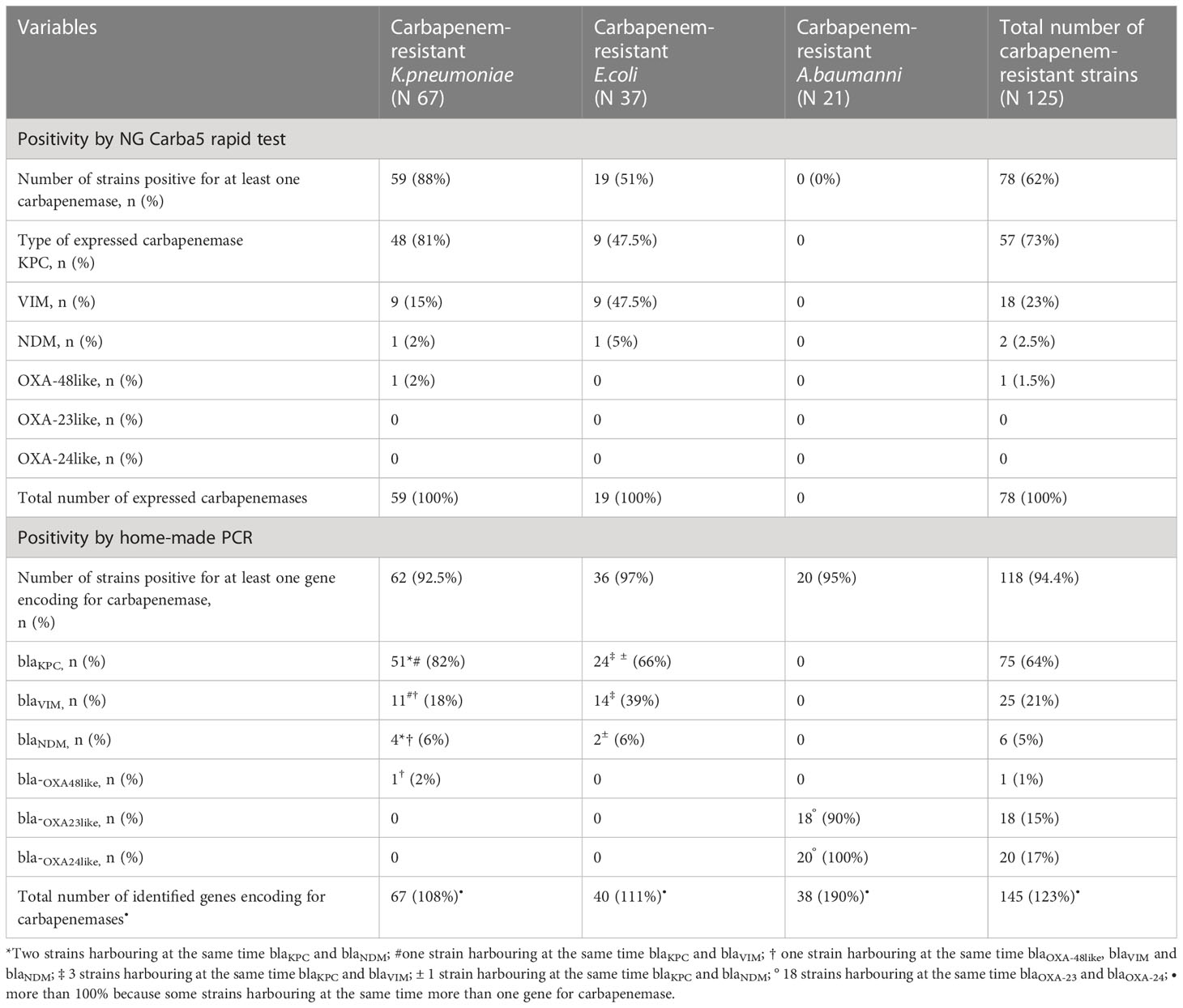
Table 6 Carbapenemases identified in carbapenem-resistant Gram-negative bacteria isolated on selective culture by NG Carba5 rapid test and genes encoding for carbapenemases identified in carbapenem-resistant Gram-negative bacteria isolated on selective culture by home-made PCR.
Home-made PCR identified blaKPC in 75 strains (64%), blaVIM in 25 (21%), blaNDM in 6 strains (5%) blaOXA-23-like in 18 strains (15%), blaOXA-24-like in 20 strains (17%), and blaOXA-48-like in only one strain (Table 6). Both blaKPC and blaVIM were found in 4 strains and both blaKPC and blaNDM in 3 strains. Finally, one K. pneumoniae strain tested positive for blaOXA-48-like /blaNDM/blaVIM simultaneously (Table 6).
Overall, 1147 (59%) of the enrolled residents provided a sample, 134 (11.7%) of which tested positive for GDH. Real time PCR tested positive for toxins A-B genes in 21 GDH-positive strains (15.7%).
The presence of at least one device resulted significantly associated with all outcomes: enteric colonization by III-generation cephalosporin-resistant Gram-negative bacteria, enteric colonization by carbapenem-resistant Gram-negative bacteria end enteric colonization by C.difficile (Table 7). Antibiotic treatment in the previous 3 months was significantly associated only with colonization by III-generation cephalosporin resistant Gram-negative bacteria. Hospitalizations in the previous year was significantly associated only with colonization by carbapenem-resistant Gram-negative bacteria.
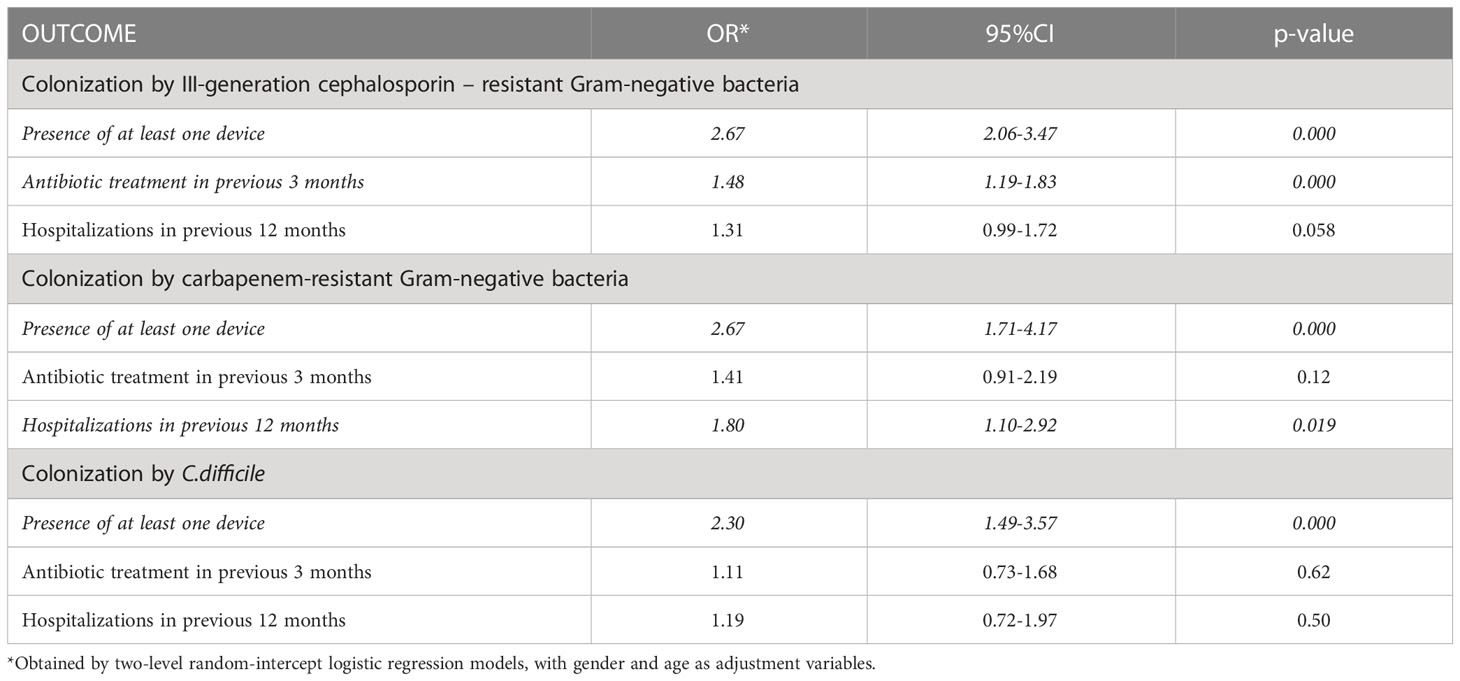
Table 7 Risk factors for enteric colonization by III-generation resistant Gram-negative bacteria, carbapenem-resistant Gram-negative bacteria and by C.difficile.
The LTCFs participating in this study have similar characteristics to those described by HALT2 and HALT3, both in terms of type of facility (general/mixed nursing homes), and of occupancy rate and care organization (European Centre for Disease Prevention and Control, 2014; Ricchizzi et al., 2018). The population described also has characteristics comparable to those of other PPSs (Arvand et al., 2013; McKinnell et al., 2019; Broussier et al., 2020; McKinnell et al., 2020; Kohler et al., 2022), being composed predominantly of females with an average age close to 85 years, and with a length of stay in the structure exceeding one year. Furthermore, the subjects housed in LTCFs prove to be clinically complex, with more than two thirds affected by concomitant chronic pathologies and presenting a high degree of disability, documented by both cognitive and motor impairment. The prevalence of fecal and urinary incontinence above 50% is also similar to that found in other studies (European Centre for Disease Prevention and Control, 2014; Ricchizzi et al., 2018; Broussier et al., 2020). Compared to Boussier et al., on the other hand, a greater frequency of bed rest (25% vs 9%) and a more frequent use of devices (20% vs 6%) was reported, although urinary catheter remains the most used device. Hospitalization in the previous year involves 14% of subjects, in accordance with Arvand et al, but lower than 23%, as reported by Boussier. Exposure to antibiotic therapy in the previous 3 months is significant (about 30% of subjects), lower than that reported in France (41%) but decidedly higher than Austria (16%) (Arvand et al., 2013; Broussier et al., 2020). In our survey, moreover, the use of fluoroquinolones and III-generation cephalosporins is higher, 32% vs 4% and 22% vs 12% respectively. The characteristics described in the examined population confirm not only the complexity and fragility of the elderly subjects resident in LTCFs but also define a population which is constitutively at risk of colonization by MDR germs, being advanced age, the presence of medical devices, the presence of mental and mobility impairment, previous hospitalization and previous antibiotic use, known risk factors for colonized status (Rodríguez-Villodres et al., 2021). Of note in our study the antibiotics mainly prescribed in the previous three months are fluoroquinolones, III-generation cephalosporins and penicillins, antibiotic classes of extensive use within LTCFs due to their broad spectrum of activity and their handling, but also known as independent risk factors for enteric colonization by multi-antibiotic resistant microorganisms (Rodríguez-Villodres et al., 2021).
In this multicenter PPS, a remarkably high rate of colonization with MDR-GNB is observed among LTCF residents in the Veneto region. Just over half (51%) of included residents are colonized with GNB resistant to III generation cephalosporins and 6% with GNB resistant to carbapenems.
In comparison with previous investigations, the colonization rate by III-generation resistant GNB is strikingly higher than that found in Japanese (Nakai et al., 2022) and in other European countries (Jonsson et al., 2011; Arvand et al., 2013; Kohler et al., 2022), although our findings are in line with other Italian reports (Aschbacher et al., 2016; Aschbacher et al., 2020). In the present study, this high rate is mostly due to E.coli (65%), suggesting that LTCFs might be a reservoir of this microorganism for the healthcare system.
As already described elsewhere (Cherubini et al., 2022), most of the E. coli strains isolated from our population belong to ST131 lineage, mainly of the O25b:H4 serotype and H30 subclone, and ESBL production is mainly attributed to enzymes of the CTX-M -1 group (CTX-M-1, CTX-M-3 and CTX-M-15). In the analysed strains, however, other resistance genes were also found, ST131 representing an incubator of fluoroquinolones, and other antibiotic resistance genes (Cherubini et al., 2022). These results are in line with previous studies conducted in Italian and European acute-care hospitals, indicating that the CTX-M types have disseminated in E.coli species. This reflects the selective pressure exerted by frequent and repeated antibiotic therapies especially with fluoroquinolones and III-generation cephalosporins, as already widely described (Urbánek et al., 2007; Fuzi et al., 2020) and documented also by our case series. Furthermore, the high colonization rate can be attributed to the increased probability of horizontal transmission favoured by the care needs of this population, especially for personal hygiene, and by LTCFs’ setting itself, generally characterized by understaffing and sub-optimal hydro alcoholic’s consumption for hand-hygiene (European Centre for Disease Prevention and Control, 2014; Ricchizzi et al., 2018). In line with that described in other surveys, also in our case the recent consumption of antibiotics was found to be risk factors for colonization by Gram negatives resistant to III-generation cephalosporins (Aschbacher et al., 2016; Aschbacher et al., 2020; Broussier et al., 2020).
As recently described, the prevalence of CR GNB colonization within LTCFs is extremely heterogeneous, ranging from 6% to 30% in the USA, 0% to 23% in Asia and reaching 12% in Israel (Chen et al., 2021). In Europe, the reported frequencies range from 0% in Belgium and the Netherlands to 0.3% in Switzerland; in Italy a prevalence of carbapenemase-producing Enterobacterales of 6.3% in 2008 and of 1% in 2015 has been reported (Aschbacher et al., 2016). Our population documents a CR GNB colonization rate of 6%, mainly due to carbapenemase encoding GNB as documented by PCR results. These data reflect the frequency of carbapenem-resistant strains also described in the latest EARSS report and related to invasive infections (European Centre for Disease Prevention and Control, 2022). The high frequency of carbapenemase-producing Enterobacterales, especially K.pneumoniae, is also in line with the EuSCAPE study, according to which the carbapenemase-producing Enterobacterales (CPE) colonization/infection rate is higher in the Mediterranean region with a particularly high incidence in Italy (5.96/10,000 hospital admissions) (Grundmann et al., 2017), and are also in accordance with recently described results from Spain (Callejón Fernández et al., 2022). Therefore, our finding of recent hospitalization as a risk factor for colonization by CR GNB is not surprising, although we do not have local epidemiological data on the frequency of colonization/infection by CR GNB in patients admitted between June 2018 and June 2019 in the reference acute care hospitals for the LTCFs included in the present study. With this limit it is not possible to exactly define the circulation of CR GNB between LTCFs and acute care hospitals within the Veneto region. In our study, recent antibiotic use is not associated with colonization by carbapenem-resistant germs. Since the colonization by CR GNB detected through selective culture and immuno-enzymatic test has been considered as an outcome variable, this lack of association could be the consequence of the underestimation of patients colonized by carbapenemase-producing Enterobacterales using this method if compared to home-made PCR results. In accordance with other series, K. pneumoniae was the most frequently isolated carbapenem-resistant micro-organism (Chen et al., 2021). As already described elsewhere (Piccirilli et al., 2021), in this study the most widespread clones were represented by ST307 and ST512 and the more detected carbapenemases were the KPC variants (KPC-2, KPC-3, and KPC-9), followed by VIM-1. This reflects the Italian epidemiology, both with respect to acute care hospitals and to LTCFs (Aschbacher et al., 2020), and documents how LTCFs represent an important incubator not only of ESBLs but also of carbapenemases.
Finally, the colonization by C. difficile is higher than that documented by Giufrè et al. (11.7% vs 5.1%) (Giufrè et al., 2017), despite the lower sensitivity of GDH qualitative enzyme immunoassay adopted as screening test in asymptomatic subjects compared with selective culture used by the other group. Only 2% of C.difficile strains was toxigenic, in line with that described by Leitner (Leitner et al., 2018), but clearly lower than, above all, US, and Canadian epidemiology (Donskey et al., 2018; Mallia et al., 2018). This could be linked both to the low sensitivity of the adopted screening test and to the small sample size, since it was possible to collect the samples of only half of the enrolled residents.
This study has several limitations. The point-prevalence design did not consider the dynamics of ESBL and carbapenemasescarbapenems epidemiology, but it was chosen because of its feasibility when applied in settings with limited resources for antimicrobial resistance surveillance, as is the case for LTCFs. We also did not have local epidemiological data to assess the frequency of infection/colonization by III-generation cephalosporin- and carbapenem-resistant Enterobacterales and non-lactose fermenters bacteria in individuals admitted in the same period (2018–2019) in the acute-care hospitals of reference for the LTCFs involved in the present study. Furthermore, the screening of healthcare workers and staff was not performed, therefore their role in the MDR-GNB transmission can be only hypothesised but cannot be assessed.
The strengths of this survey include the use of a standardized protocol across all participating LTCFs, the collection of detailed data on the LTCF characteristics and the inclusion of a wide variety of LTCF residents and data on their antimicrobial use. The survey is characterized by a broad participation and a very large sample size, providing a good overall picture of antimicrobial use and MDR GNB colonization’s rate. Finally, we performed Whole Genomic Sequencing on a subset of E.coli and K.pneumoniae strains isolated by selective culture (data shown elsewhere) (Piccirilli et al., 2021; Cherubini et al., 2022).
LTCFs are important reservoirs for MDR organisms, mainly III-generation cephalosporins-resistant Enterobacterales but also carbapenem-resistant GNB, which can be selected as a result of the antibiotic pressure exerted by repeated antibiotic treatments and/or derive from horizontal transmission mechanisms. Both events may occur within the LTCF or within the acute care hospital on previous admissions.
To contrast the horizontal spread of these microorganisms, the identification and screening of residents coming from nursing homes at hospital admission must be considered (Chen et al., 2021). According to LTCF infection prevention and control guidelines, active surveillance of MDROs in LTCFs by culture methods or by using molecular amplification assays should not imply routine screening of residents at the time of admission to the facility, nor should it be repeated on a periodic basis, in the absence of an epidemic of infections by MDROs, because the application of standard precautions, as applied to all residents, is sufficient (Smith et al., 2008). Carbapenemase-producing Enterobacterales, especially KPC-producing K. pneumoniae, are epidemically spread in Italy, and infection control and prevention measures in LTCFs is an effective strategy to reduce carbapenem-resistant Enterobacterales acquisition and transmission in high endemicity epidemiological setting, such as this one (Toth et al., 2017). The ESCMID-EUCIC clinical guidelines do not recommend routine decolonization of these microorganisms (Tacconelli et al., 2019) because of the potential of increased antimicrobial resistance to decolonizing agents (Tacconelli et al., 2019). Rigorous application of contact precautions has been effective in controlling carbapenem-resistant Enterobacterales (Mody et al., 2013), however they are not practical for most LTCFs’ residents due to concerns for unique harms in this setting, which is perceived and experienced as a home (Mody et al., 2013). Focusing on other type of effective measures, such as the importance of better environmental cleaning protocols, more rigorous application of routine infection prevention protocols, and adherence to hand hygiene indications, is of extreme importance.
Antimicrobial use in LTCFs is a critical issue as well (Ricchizzi et al., 2018). Antimicrobial stewardship programs are needed to control the selection of multidrug resistant organisms, supporting physicians not only in the implementation of updated antibiotic treatment guidelines for the most frequent infective syndromes (e.g. upper/lower respiratory tract infections, urinary tract infections, skin and soft tissue infections), but also in the adoption, for example, of point of care diagnostic tests and/or diagnostic algorithms to reduce unnecessary use of antibiotics in LTCFs (Oliva et al., 2018).
The original contributions presented in the study are included in the article/supplementary materials, further inquiries can be directed to the corresponding author/s.
The studies involving human participants were reviewed and approved by Ethics Committee for Clinical Trials of the Provinces of Verona and Rovigo -Approval n° 25294, 26/04/2018. The patients/participants provided their written informed consent to participate in this study.
AMA conceived the study, organized the collection of biological samples and clinical data, supervised the statistical analysis, and drafted the manuscript. GB participated in the collection of biological samples and clinical data, participated in the statistical analysis, and drafted the manuscript. GLC, LN and AB performed the microbiological analysis. JM and MM conducted the statistical analysis. IC, NDS and LL collected biological samples and clinical data, all of them also participated in data entry. FM helped in the coordination of sample and clinical data collection. ET and GLC conceived the study. All authors reviewed and approved the final manuscript. All authors contributed to the article and approved the submitted version.
This project was funded by Regione Veneto (Italy): DGR 1656; 17/10/2017. The funds were used to transport the biological samples from the LTCFs to the reference laboratory and to carry out the microbiological tests necessary for carrying out the project The correspondence author will use her own Institutional Funds for open access publication fees.
Thanks to Ruth Davis for the revision of the text in English. Thanks to Ercole Concia and to Giuseppe Cornaglia for having supported this study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Ambretti, S., Bassetti, M., Clerici, P., Petrosillo, N., Tumietto, F., Viale, P., et al. (2019). Screening for carriage of carbapenem-resistant enterobacteriaceae in settings of high endemicity: a position paper from an Italian working group on CRE infections. Antimicrob. Resist. Infect. Control 8, 136. doi: 10.1186/s13756-019-0591-6
Arena, F., Vannetti, F., Di Pilato, V., Fabbri, L., Colavecchio, O. L., Giani, T., et al. (2018). Diversity of the epidemiology of carbapenemase-producing enterobacteriaceae in long-term acute care rehabilitation settings from an area of hyperendemicity, and evaluation of an intervention bundle. J. Hosp Infect. 100 (1), 29–34. doi: 10.1016/j.jhin.2018.05.025
Arvand, M., Moser, V., Pfeifer, Y. (2013). Prevalence of extended-spectrum-β-lactamase-producing escherichia coli and spread of the epidemic clonal lineage ST131 in nursing homes in hesse, Germany. J. Antimicrob. Chemother. 68 (11), 2686–2688. doi: 10.1093/jac/dkt226
Aschbacher, R., Pagani, E., Confalonieri, M., Farina, C., Fazii, P., Luzzaro, F., et al. (2016). Review on colonization of residents and staff in Italian long-term care facilities by multidrug-resistant bacteria compared with other European countries. Antimicrob. Resist. Infect. Control 5, 33. doi: 10.1186/s13756-016-0136-1
Aschbacher, R., Pagani, L., Migliavacca, R., Pagani, L. (2020). GLISTer (Gruppo di lavoro per lo studio delle infezioni nelle residenze sanitarie assistite e strutture assimilabili) working group. recommendations for the surveillance of multidrug-resistant bacteria in Italian long-term care facilities by the GLISTer working group of the Italian association of clinical microbiologists (AMCLI). Antimicrob. Resist. Infect. Control 9 (1), 106. doi: 10.1186/s13756-020-00771-0
Barbut, F., Jones, G., Eckert, C. (2011). Epidemiology and control of clostridium difficile infections in healthcare settings: an update. Curr. Opin. Infect. Dis. 24 (4), 370–376. doi: 10.1097/QCO.0b013e32834748e5
Benoit, S. R., Nsa, W., Richards, C. L., Bratzler, D. W., Shefer, A. M., Steele, L. M., et al. (2008). Factors associated with antimicrobial use in nursing homes: a multilevel model. J. Am. Geriatr. Soc 56 (11), 2039–2044. doi: 10.1111/j.1532-5415.2008.01967.x
Broussier, M., Gbaguidi-Haoré, H., Rachidi-Berjamy, F., Bertrand, X., Slekovec, C. (2020). Prevalence, genetic diversity of and factors associated with ESBL-producing enterobacterales carriage in residents of French nursing homes. J. Hosp Infect. 104 (4), 469–475. doi: 10.1016/j.jhin.2019.12.008
Burns, K., Roche, F., Donlon, S. (2015). Healthcare-associated infections and antimicrobial use in long-term care facilities: the Irish experience with the HALT surveys. J. Hosp. Infect. 89 (4), 276–280. doi: 10.1016/j.jhin.2014.12.006
Callejón Fernández, M., Madueño Alonso, A., Abreu Rodríguez, R., Aguirre-Jaime, A., Castro Hernández, M. B., Ramos-Real, M. J., et al. (2022). Risk factors for colonization by carbapenemase-producing bacteria in Spanish long-term care facilities: a multicentre point-prevalence study. Antimicrob. Resist. Infect. Control 11 (1), 163. doi: 10.1186/s13756-022-01200-0
Carrër, A., Fortineau, N., Nordmann, P. (2010). Use of ChromID extended-spectrum β-lactamase medium for detecting carbapenemase-producing. Enterobacteriaceae. J. Clin. Microbiol. 48 (5), 1913–1914. doi: 10.1128/JCM.02277-09
Castle, S. C. (2000). Impact of age-related immune dysfunction on risk of infections. Z. Gerontol. und Geriatrie. 33 (5), 341–349. doi: 10.1007/s003910070030
Chen, H. Y., Jean, S. S., Lee, Y. L., Lu, M. C., Ko, W. C., et al. (2021). Carbapenem-resistant enterobacterales in long-term care facilities: a global and narrative review. Front. Cell Infect. Microbiol. 11, 601968. doi: 10.3389/fcimb.2021.601968
Cherubini, S., Perilli, M., Azzini, A. M., Tacconelli, E., Maccacaro, L., Bazaj, A., et al. (2022). Resistome and virulome of multi-drug resistant e. coli ST131 isolated from residents of long-term care facilities in the northern Italian region. Diagn. (Basel). 12 (1), 213. doi: 10.3390/diagnostics12010213
Childs, A., Zullo, A. R., Joyce, N. R., McConeghy, K. W., van Aalst, R., Moyo, P., et al. (2019). The burden of respiratory infections among older adults in long-term care: a systematic review. BMC Geriatr. 19 (1), 210. doi: 10.1186/s12877-019-1236-6
Donskey, C. J., Sunkesula, V. C. K., Stone, N. D., Gould, C. V., McDonald, L. C., Samore, M., et al. (2018). Transmission of clostridium difficile from asymptomatically colonized or infected long-term care facility residents. Infect. Control Hosp Epidemiol. 39 (8), 909–916. doi: 10.1017/ice.2018.106
Drinka, P. J., Crnich, C. J., Nace, D. A. (2013). An antibiotic prescription induces resistance at the individual level more than the group level. J. Am. Med. Dir Assoc. 14 (9), 707–708. doi: 10.1016/j.jamda.2013.05.007
Dyar, O. J., Pagani, L., Pulcini, C. (2015). Strategies and challenges of antimicrobial stewardship in long-term care facilities. Clin. Microbiol. Infect. 21 (1), 10–19. doi: 10.1016/j.cmi.2014.09.005
ECDC-WHO. Europe COVID-19 surveillance explorer. Available at: https://worldhealthorg.shinyapps.io/euro-covid19/ (Accessed February 24, 2023).
Eucast. Resistance Mechanisms. European Committee on Antimicrobial Susceptibility Testing. Available at: https://www.eucast.org/resistance_mechanisms (Accessed March 10, 2023).
European Centre for Disease Prevention and Control (2014) Point prevalence survey of healthcare-associated infections and antimicrobial use in European long-term care facilities (Publications Office) (Accessed March 8, 2023).
European Centre for Disease Prevention and Control (2022). Antimicrobial resistance in the EU/EEA (EARS-net) Annual Epidemiological Report 2020. Stockholm: ECDC.
Falcone, M., Meier, J. J., Marini, M. G., Caccialanza, R., Aguado, J. M., Del Prato, S., et al. (2021). Diabetes and acute bacterial skin and skin structure infections. Diabetes Res. Clin. Practice. 174, 108732. doi: 10.1016/j.diabres.2021.108732
Flokas, M. E., Alevizakos, M., Shehadeh, F., Andreatos, N., Mylonakis, E. (2017). Extended-spectrum β-lactamase-producing enterobacteriaceae colonisation in long-term care facilities: a systematic review and meta-analysis. Int. J. Antimicrob. Agents. 50 (5), 649–656. doi: 10.1016/j.ijantimicag.2017.08.003
Fuzi, M., Rodriguez Baño, J., Toth, A. (2020). Global evolution of pathogenic bacteria with extensive use of fluoroquinolone agents. Front. Microbiol. 11. doi: 10.3389/fmicb.2020.00271
Gavazzi, G., Krause, K. H. (2002). Ageing and infection. Lancet Infect. Dis. 2 (11), 659–666. doi: 10.1016/s1473-3099(02)00437-1
Giufrè, M., Ricchizzi, E., Accogli, M., Barbanti, F., Monaco, M., Pimentel de Araujo, F., et al. (2017). Colonization by multidrug-resistant organisms in long-term care facilities in Italy: a point-prevalence study. Clin. Microbiol. Infect. 23 (12), 961–967. doi: 10.1016/j.cmi.2017.04.006
Grundmann, H., Glasner, C., Albiger, B., Aanensen, D. M., Tomlinson, C. T., Andrasević, A. T., et al. (2017). Occurrence of carbapenemase-producing klebsiella pneumoniae and escherichia coli in the European survey of carbapenemase-producing enterobacteriaceae (EuSCAPE): a prospective, multinational study. Lancet Infect. Dis. 17 (2), 153–163. doi: 10.1016/S1473-3099(16)30257-2
Heppner, H. J., Cornel, S., Peter, W., Philipp, B., Katrin, S. (2013). Infections in the elderly. Crit. Care Clinics. 29 (3), 757–774. doi: 10.1016/j.ccc.2013.03.016
Horcajada, J. P., Montero, M., Oliver, A., Sorlí, L., Luque, S., Gómez-Zorrilla, S., et al. (2019). Epidemiology and treatment of multidrug-resistant and extensively drug-resistant pseudomonas aeruginosa infections. Clin. Microbiol. Rev. 32 (4), e00031–e00019. doi: 10.1128/CMR.00031-19
Hrabák, J., Chudáčkova, E., Papagiannitsis, C. C. (2014). Detection of carbapenemases in enterobacteriaceae: a challenge for diagnostic microbiological laboratories. Clin. Microbiol. Infect. 20 (9), 839–853. doi: 10.1111/1469-0691.12678
Infectious Diseases Society of America (IDSA), Spellberg, B., Blaser, M., Guidos, R. J., Boucher, H. W., Bradley, J. S., et al. (2011). Combating antimicrobial resistance: policy recommendations to save lives. Clin. Infect. Dis. 52 (Suppl 5), S397–S428. doi: 10.1093/cid/cir153
Jonsson, K., Claesson, B. E. B., Hedelin, H. (2011). Urine cultures from indwelling bladder catheters in nursing home patients: a point prevalence study in a Swedish county. Scand. J. Urol Nephrol. 45 (4), 265–269. doi: 10.3109/00365599.2011.562236
Juthani-Mehta, M., Quagliarello, V. J. (2010). Infectious diseases in the nursing home setting: challenges and opportunities for clinical investigation. Clin. Infect. Dis. 51 (8), 931–936. doi: 10.1086/656411
Kohler, P., Seiffert, S. N., Kessler, S., Rettenmund, G., Lemmenmeier, E., Qalla Widmer, L., et al. (2022). Molecular epidemiology and risk factors for extended-spectrum β-Lactamase-Producing enterobacterales in long-term care residents. J. Am. Med. Dir Assoc. 23 (3), 475–481.e5. doi: 10.1016/j.jamda.2021.06.030
Latour, K., Catry, B., Broex, E., Vankerckhoven, V., Muller, A., Stroobants, R., et al. (2012). Indications for antimicrobial prescribing in European nursing homes: results from a point prevalence survey: ANTIMICROBIAL PRESCRIPTIONS IN EUROPEAN NURSING HOMES. Pharmacoepidemiol. Drug Saf. 21 (9), 937–944. doi: 10.1002/pds.3196
Leitner, E., Schreiner, E., Neuhold, M., Bozic, M., Pux, C., Pichler, G., et al. (2020). Low prevalence of clostridium difficile colonization in patients in long-term care facilities in graz, Austria: a point-prevalence study. Am. J. Infect. Control 48 (10), 1144–1147. doi: 10.1016/j.ajic.2019.12.011
Leitner, E., Zechner, E., Ullrich, E., Zarfel, G., Luxner, J., Pux, C., et al. (2018). Low prevalence of colonization with multidrug-resistant gram-negative bacteria in long-term care facilities in graz, Austria. Am. J. Infect. Control 46 (1), 76–80. doi: 10.1016/j.ajic.2017.07.004
Loeb, M. (2000). Antibiotic use in long-term-care facilities: many unanswered questions. Infect. Control Hosp Epidemiol. 21 (10), 680–683. doi: 10.1086/501713
Mallia, G., Van Toen, J., Rousseau, J., Jacob, L., Boerlin, P., Greer, A., et al. (2018). Examining the epidemiology and microbiology of clostridium difficile carriage in elderly patients and residents of a healthcare facility in southern Ontario, Canada. J. Hosp Infect. 99 (4), 461–468. doi: 10.1016/j.jhin.2018.01.020
McClean, P., Hughes, C., Tunney, M., Goossens, H., Jans, B. (2011). European Surveillance of antimicrobial consumption (ESAC) nursing home project group. Antimicrobial. prescribing Eur. Nurs. homes. J. Antimicrob. Chemother. 66 (7), 1609–1616. doi: 10.1093/jac/dkr183
McClean, P., Tunney, M., Gilpin, D., Parsons, C., Hughes, C. (2012). Antimicrobial prescribing in residential homes. J. Antimicrob. Chemother. 67 (7), 1781–1790. doi: 10.1093/jac/dks085
McKinnell, J. A., Miller, L. G., Singh, R. D., Gussin, G., Kleinman, K., Mendez, J., et al. (2020). High prevalence of multidrug-resistant organism colonization in 28 nursing homes: an “Iceberg effect.” J. Am. Med. Dir Assoc. 21 (12), 1937–1943.e2. doi: 10.1016/j.jamda.2020.04.007
McKinnell, J. A., Singh, R. D., Miller, L. G., Kleinman, K., Gussin, G., He, J., et al. (2019). The SHIELD orange county project: multidrug-resistant organism prevalence in 21 nursing homes and long-term acute care facilities in southern California. Clin. Infect. Dis. 69 (9), 1566–1573. doi: 10.1093/cid/ciz119
Mody, L., Bradley, S. F., Huang, S. S. (2013). Keeping the “home” in nursing home: implications for infection prevention. JAMA Intern. Med. 173 (10), 853–854. doi: 10.1001/jamainternmed.2013.330
Nakai, M., Oka, K., Watanabe, G., Kamei, K., Tsukada, N., Mori, R., et al. (2022). Epidemiology and molecular characterization of fecal carriage of third-generation cephalosporin-resistant enterobacterales among elderly residents in Japan. J. Infect. Chemother. 28 (4), 569–575. doi: 10.1016/j.jiac.2021.12.033
Nguyen, H. Q., Tunney, M. M., Hughes, C. M. (2019). Interventions to improve antimicrobial stewardship for older people in care homes: a systematic review. Drugs Aging. 36 (4), 355–369. doi: 10.1007/s40266-019-00637-0
Nicolle, L. E., Bentley, D. W., Garibaldi, R., Neuhaus, E. G., Smith, P. W. (2000). SHEA Long-Term–care committee. Antimicrobial. Use Long-Term–Care Facilities. Infect. Control Hosp Epidemiol. 21 (8), 537–545. doi: 10.1086/501798
Nucleo, E., Caltagirone, M., Marchetti, V. M., D'Angelo, R., Fogato, E., Confalonieri, M., et al. (2018). Colonization of long-term care facility residents in three Italian provinces by multidrug-resistant bacteria. Antimicrob. Resist. Infect. Control 7, 33. doi: 10.1186/s13756-018-0326-0
OECD (2011) Health at a glance 2011: OECD indicators. organisation for economic Co-operation and development. Available at: https://www.oecd-ilibrary.org/social-issues-migration-health/health-at-a-glance-2011_health_glance-2011-en (Accessed March 8, 2023).
Oliva, A., Giacobbe, D. R., Di Luca, M., Miller, N. S. (2018). New insights into infections due to multidrug resistant gram negative bacteria: the interplay between Lab and clinic. BioMed. Res. Int. 2018, 8905874. doi: 10.1155/2018/8905874
Perez, F., Hujer, A. M., Hujer, K. M., Decker, B. K., Rather, P. N., Bonomo, R. A. (2007). Global challenge of multidrug-resistant acinetobacter baumannii. Antimicrob. Agents Chemother. 51 (10), 3471–3484. doi: 10.1128/AAC.01464-06
Piccirilli, A., Cherubini, S., Azzini, A. M., Tacconelli, E., Lo Cascio, G., Maccacaro, L., et al. (2021). Whole-genome sequencing (WGS) of carbapenem-resistant k. pneumoniae isolated in long-term care facilities in the northern Italian region. Microorganisms 9 (9), 1985. doi: 10.3390/microorganisms9091985
Poirel, L., Walsh, T. R., Cuvillier, V., Nordmann, P. (2011). Multiplex PCR for detection of acquired carbapenemase genes. Diagn. Microbiol. Infect. Dis. 70 (1), 119–123. doi: 10.1016/j.diagmicrobio.2010.12.002
Ribbe, M. W., Ljunggren, G., Steel, K., Topinková, E., Hawes, C., Ikegami, N., et al. (1997). Nursing homes in 10 nations: a comparison between countries and settings. Age Ageing. 26 (suppl 2), 3–12. doi: 10.1093/ageing/26.suppl_2.3
Ricchizzi, E., Latour, K., Kärki, T., Buttazzi, R., Jans, B., Moro, M. L., et al. (2018). Antimicrobial use in European long-term care facilities: results from the third point prevalence survey of healthcare-associated infections and antimicrobial use, 2016 to 2017. Euro Surveill. 23 (46), pii=1800394. doi: 10.2807/1560-7917.ES.2018.23.46.1800394
Rodriguez, C., Korsak, N., Taminiau, B., Avesani, V., Van Broeck, J., Delmée, M., et al. (2014). Clostridium difficile infection in elderly nursing home residents. Anaerobe 30, 184–187. doi: 10.1016/j.anaerobe.2014.08.007
Rodríguez-Villodres, Á, Martín-Gandul, C., Peñalva, G., Guisado-Gil, A. B., Crespo-Rivas, J. C., Pachón-Ibáñez, M. E., et al. (2021). Prevalence and risk factors for multidrug-resistant organisms colonization in long-term care facilities around the world: a review. Antibiotics 10 (6), 680. doi: 10.3390/antibiotics10060680
Rotjanapan, P., Dosa, D., Thomas, K. S. (2011). Potentially inappropriate treatment of urinary tract infections in two Rhode island nursing homes. Arch. Intern. Med. 171 (5), 438–443. doi: 10.1001/archinternmed.2011.13
Ruiz-Garbajosa, P., Hernández-García, M., Beatobe, L., Tato, M., Méndez, M. I., Grandal, M., et al. (2016). A single-day point-prevalence study of faecal carriers in long-term care hospitals in Madrid (Spain) depicts a complex clonal and polyclonal dissemination of carbapenemase-producing enterobacteriaceae. J. Antimicrob. Chemother. 71 (2), 348–352. doi: 10.1093/jac/dkv355
Smith, P. W., Bennett, G., Bradley, S., Drinka, P., Lautenbach, E., Marx, J., et al. (2008). SHEA/APIC guideline: infection prevention and control in the long-term care facility, July 2008. Infect. Control Hosp Epidemiol. 29 (9), 785–814. doi: 10.1086/592416
Strausbaugh, L. J., Crossley, K. B., Nurse, B. A., Thrupp, L. D. (1996). Antimicrobial resistance in long-term-care facilities. Infect. Control Hosp Epidemiol. 17 (2), 129–140. doi: 10.1086/647257
Stuart, R. L., Wilson, J., Bellaard-Smith, E., Brown, R., Wright, L., Vandergraaf, S., et al. (2012). Antibiotic use and misuse in residential aged care facilities: antibiotic use in residential care. Intern. Med. J. 42 (10), 1145–1149. doi: 10.1111/j.1445-5994.2012.02796.x
Suetens, C. (2012). Healthcare-associated infections in European long-term care facilities: how big is the challenge? Euro Surveill. 17 (35), pii=20259. doi: 10.2807/ese.17.35.20259-en
Tacconelli, E., Mazzaferri, F., de Smet, A. M., Bragantini, D., Eggimann, P., Huttner, B. D., et al. (2019). ESCMID-EUCIC clinical guidelines on decolonization of multidrug-resistant gram-negative bacteria carriers. Clin. Microbiol. Infect. 25 (7), 807–817. doi: 10.1016/j.cmi.2019.01.005
Terveer, E. M., Crobach, M. J. T., Sanders, I. M. J. G., Vos, M. C., Verduin, C. M., Kuijper, E. J. (2017). Detection of clostridium difficile in feces of asymptomatic patients admitted to the hospital. J. Clin. Microbiol. 55 (2), 403–411. doi: 10.1128/JCM.01858-16
Toth, D. J. A., Khader, K., Slayton, R. B., Kallen, A. J., Gundlapalli, A. V., O'Hagan, J. J., et al. (2017). The potential for interventions in a long-term acute care hospital to reduce transmission of carbapenem-resistant enterobacteriaceae in affiliated healthcare facilities. Clin. Infect. Dis. 65 (4), 581–587. doi: 10.1093/cid/cix370
Urbánek, K., Kolár, M., Lovecková, Y., Strojil, J., Santavá, L. (2007). Influence of third-generation cephalosporin utilization on the occurrence of ESBL-positive klebsiella pneumoniae strains. J. Clin. Pharm. Ther. 32 (4), 403–408. doi: 10.1111/j.1365-2710.2007.00836.x
van Buul, L. W., van der Steen, J. T., Veenhuizen, R. B., Achterberg, W. P., Schellevis, F. G., Essink, R. T., et al. (2012). Antibiotic use and resistance in long term care facilities. J. Am. Med. Dir Assoc. 13 (6), 568.e1–568.13. doi: 10.1016/j.jamda.2012.04.004
van den Dool, C., Haenen, A., Leenstra, T., Wallinga, J. (2016). The role of nursing homes in the spread of antimicrobial resistance over the healthcare network. Infect. Control Hosp Epidemiol. 37 (7), 761–767. doi: 10.1017/ice.2016.59
van Duin, D. (2012). Diagnostic challenges and opportunities in older adults with infectious diseases. Clin. Infect. Dis. 54 (7), 973–978. doi: 10.1093/cid/cir927
van Duin, D., Paterson, D. L. (2016). Multidrug-resistant bacteria in the community: trends and lessons learned. Infect. Dis. Clin. North Am. 30 (2), 377–390. doi: 10.1016/j.idc.2016.02.004
Wang, L., Lansing, B., Symons, K., Flannery, E. L., Fisch, J., Cherian, K., et al. (2012). Infection rate and colonization with antibiotic-resistant organisms in skilled nursing facility residents with indwelling devices. Eur. J. Clin. Microbiol. Infect. Dis. 31 (8), 1797–1804. doi: 10.1007/s10096-011-1504-7
Keywords: LTCF, colonization, ESBL, carbapenem-resistant, carbapenemase, C. difficile, risk factors, epidemiology
Citation: Azzini AM, Be G, Naso L, Lambertenghi L, Salerno ND, Coledan I, Bazaj A, Mirandola M, Miotti J, Mazzaferri F, Accordini S, Lo Cascio G and Tacconelli E (2023) Risk factors for colonization with multidrug-resistant Gram-negative bacteria and Clostridioides difficile in Long Term Care Facilities (LTCFs) residents: the evidence from 27 facilities in a high endemic setting. Front. Cell. Infect. Microbiol. 13:1155320. doi: 10.3389/fcimb.2023.1155320
Received: 31 January 2023; Accepted: 19 May 2023;
Published: 12 June 2023.
Edited by:
Israel Nissan, Ministry of Health, IsraelReviewed by:
Avi Peretz, The Baruch Padeh Medical Center, Poriya, IsraelCopyright © 2023 Azzini, Be, Naso, Lambertenghi, Salerno, Coledan, Bazaj, Mirandola, Miotti, Mazzaferri, Accordini, Lo Cascio and Tacconelli. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Anna Maria Azzini, YW5uYW1hcmlhLmF6emluaUB1bml2ci5pdA==
†These authors share last authorship
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.