 Nansi López-Valverde1
Nansi López-Valverde1 Antonio López-Valverde
Antonio López-Valverde- 1Department of Medicine and Medical Specialties, Faculty of Health Sciences, Universidad Alcalá de Henares, Madrid, Spain
- 2Department of Surgery, Instituto de Investigación Biomédica de Salamanca (IBSAL), University of Salamanca, Salamanca, Spain
Peri-implant diseases are pathological conditions that affect the survival of dental implants. Etiological studies are limited, accepting a prevalence of 20% at the implant level and 24% at the patient level. The benefits of adjuvant metronidazole are controversial. A systematic review and meta-analysis of RCTs according to PRISMA and PICOS was performed with an electronic search over the last 10 years in MEDLINE (PubMed), WOS, Embase, and Cochrane Library. The risk of bias was measured using the Cochrane Risk of Bias tool and the methodological quality using the Jadad scale. Meta-analysis was performed with RevMan version 5.4.1, based on mean difference and standard deviation, with 95% confidence intervals; the random-effects model was selected, and the threshold for statistical significance was defined as p < 0.05. A total of 38 studies were collected and five were selected. Finally, one of the studies was eliminated because of unanalyzable results. All studies reached a high methodological quality. A total of 289 patients were studied with follow-up periods from 2 weeks to 1 year. Statistical significance was only found, with respect to the use of adjunctive metronidazole, in the pooled analysis of the studies (p = 0.02) and in the analysis of the radiographic values reported on peri-implant marginal bone levels, in the studies with a 3-month follow-up (p = 0.03). Discrepancies in the use of systemic metronidazole require long-term randomized clinical trials (RCTs) to determine the role of antibiotics in the treatment of peri-implantitis.
1 Introduction
Mucositis and peri-implantitis are considered peri-implant diseases associated with biofilms and affect osseointegrated implants (Berglundh et al., 2018). For clinicians to establish a clear differentiation with the peri-implant health status and apply a correct treatment, these pathologies require a clear definition, and it is generally accepted that mucositis is a reversible inflammation of the peri-implant soft tissues, and peri-implantitis, induced by plaque, is considered one of the most frequent late biological complications in dental implantology, affecting hard and soft tissues, generating a loss of peri-implant bone support, and reducing osseointegration (Schwarz et al., 2006; Smeets et al., 2014). It is usually associated with bleeding in the peri-implant sulcus, spontaneous or provoked, increased suppuration, and increased probing depth of the peri-implant pocket (Schwarz et al., 2018).
Dental implantology has made it necessary to investigate the oral microbiota in certain pathogenic situations, with the aim of demonstrating that the formation of biofilms is a determining factor in the loss of peri-implant bone support. However, despite the similarity with periodontal diseases, etiological studies of peri-implant diseases are limited, and common causative organisms have been identified for both pathologies, mainly gram-negative anaerobic bacteria, such as Porphyromonas gingivalis, Prevotella intermedia, Tannerella forsythia, Eikenella corrodens, Filifactor alocis, Aggregatibacter actinomycetemcomitans, and Staphylococcus aureus; however, there is controversy about the homogeneity of biofilm composition in both pathologies (Persson and Renvert, 2014; Sahrmann et al., 2020; Jiang et al., 2021; Mulla et al., 2021).
Precisely, the different diagnostic definitions condition the ranges of their prevalence, lower in peri-implantitis than in mucositis, with an approximate range, for the latter, between 28% and 77% of the subjects and between 12% and 43% of the implant sites (Zitzmann and Berglundh, 2008; Koldsland et al., 2010). A recent study on 474 implants in 275 patients showed peri-implantitis with a prevalence of 20% at the implant level and 24% at the patient level (Zitzmann and Berglundh, 2008).
Surgical and non-surgical treatments of peri-implantitis, based on the scientific evidence of periodontal treatments, are aimed at controlling infection and reducing the bacterial load, and it is known that surgical treatments alone have proven to be ineffective (Renvert et al., 2008; Rodrigo et al., 2018). The benefits of local or systemic antibacterials, used as adjuvants, have also been demonstrated (Liñares et al., 2019), and it is a frequent practice to prescribe systemic antibiotics for the treatment of peri-implant diseases and other dental pathologies, since, in addition to exerting an antimicrobial effect, they facilitate healing (Javed et al., 2013).
In peri-implant lesions, it has been observed that non-surgical treatments combined with systemic metronidazole reduce the probing depth (Liñares et al., 2019), although some research has indicated that the efficacy of adjuvant antibiotics in the non-surgical treatment of peri-implantitis may be conditioned by the severity of the disease (van Winkelhoff, 2012; Park et al., 2021).
Therefore, this systematic review and meta-analysis aimed to address the following specific question: In patients with peri-implantitis, is adjuvant local or systemic treatment with metronidazole effective on signs of inflammation and bone destruction?
2 Materials and methods
The review protocol was developed and structured according to the Preferred Reporting Items for Systematic Review and Meta-Analyses (PRISMA) statement (Page et al., 2021) (Table 1). The review was registered in INPLASY under registration number INPLASY202310015.
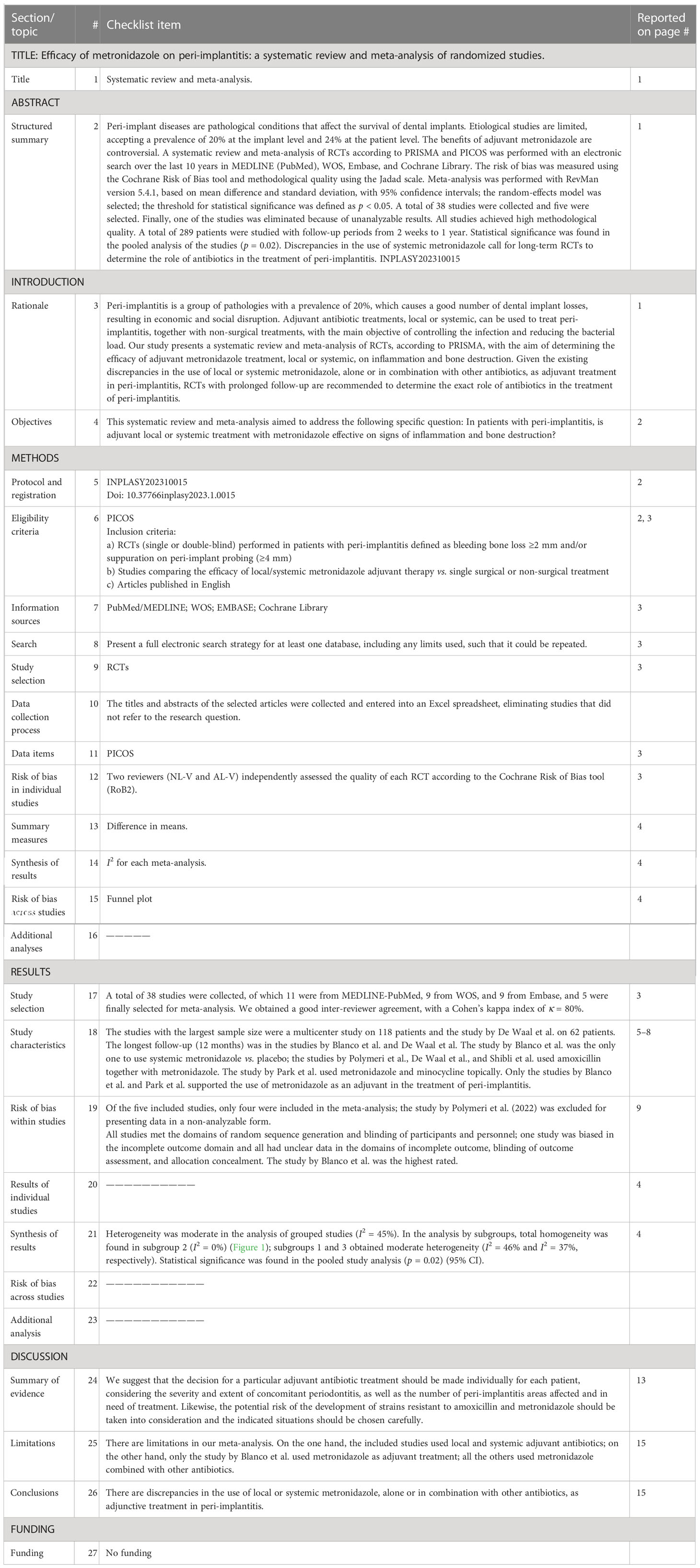
Table 1 PRISMA checklist.
2.1 PICOS and focused question
The focused question used for the literature search was structured according to the Participants, Interventions, Control, Outcomes, Study design (PICOS) format: In patients with peri-implantitis, is adjuvant local or systemic treatment with metronidazole effective on changing signs of inflammation and bone destruction?
(P) Population: patients receiving adjuvant treatment with local or systemic metronidazole.
(I) Intervention: surgical or non-surgical treatment of peri-implantitis.
(C) Comparison: patients not receiving adjuvant treatment with metronidazole.
(O) Outcomes: primary outcomes: bleeding on probing, bleeding rate, suppuration, and probing depth. Secondary outcomes: clinical attachment level, bone level (radiographic test), and implant failure.
(S) Study design: randomized controlled trials.
2.2 Information source and search strategy
Four electronic databases were searched for relevant articles published in the last 10 years up to December 2022: MEDLINE (through PubMed), WOS, Embase, and Cochrane Library. The search filter “Randomized Controlled Trial” was applied. The electronic search was complemented with a manual search in the following journals: Clinical Implant Dentistry and Related Research, Clinical Oral Implants Research, International Journal of Oral and Maxillofacial Implants, Journal of Clinical Periodontology, and Journal of Periodontology.
The following Medical Subject Headings (MeSH) terms were used: “Dental implants,” “Dental plaque,” “Peri-Implantitis/prevention and control,” “Anti-Bacterial Agents/therapeutic use,” “Metronidazole/therapeutic use,” and “Humans.” Boolean AND/OR operators were used to refine the search. In addition, relevant studies from the grey literature and reference lists of the included studies (cross-references) were also examined. The search strategy and PICOS format are shown in Table 2.
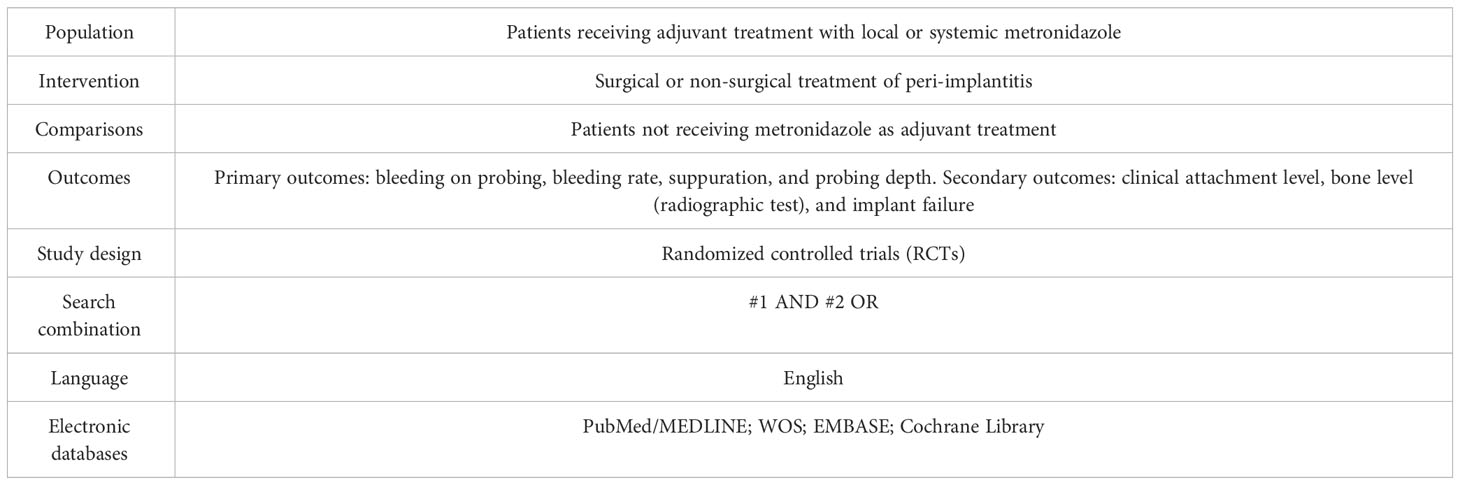
Table 2 The search strategy and PICOS format.
2.3 Inclusion and exclusion criteria
The inclusion criteria were as follows:
a) RCTs (single or double-blind) performed in patients with peri-implantitis defined as bleeding, bone loss ≥2 mm, and/or suppuration on peri-implant probing (≥ 4 mm)
b) Studies comparing the efficacy of local/systemic metronidazole adjuvant therapy vs. single surgical or non-surgical treatment
c) Articles published in English
The exclusion criteria were as follows:
a) Less than five patients per treatment group
b) Lack of clinical or radiographic data on bone destruction
c) Case series or clinical cases
d) Undefined cases and non-relevant studies
2.4 Data extraction and analysis and study selection
The titles and abstracts of the selected articles were collected and entered into an Excel spreadsheet, eliminating studies that did not refer to the research question. Two reviewers (NL-V and AL-V) independently selected titles and abstracts. Cohen’s kappa index (κ) (Cohen, 1968) was calculated to determine the degree of agreement between reviewers, and discrepancies between the two reviewers, regarding the inclusion of eligible studies, were reviewed and discussed by a third reviewer (JAB-R).
Subsequently, the selected articles were obtained for review, data extraction, and inclusion. Bibliographic references of the included studies were also reviewed as possible sources of additional studies.
2.5 Risk of bias of the included studies
Two reviewers (NL-V and AL-V) independently assessed the quality of each RCT according to the Cochrane Risk of Bias tool (RoB2) (Minozzi et al., 2022). Five domains of bias (randomization process, deviations from intended interventions, missing outcome data, outcome measurement, and selection of reported outcomes) were assessed. The Cochrane Handbook for Systematic Reviews of Interventions was used. The rating “high” indicated a high risk of bias, “low” indicated a low risk of bias, and “borderline” indicated the presence of bias due to uncertainty or lack of information about possible bias. Studies were classified as low, high risk of bias, or borderline. Any discrepancies in the assessment of RoB2 were discussed between the two reviewers with the aim of reaching a consensus.
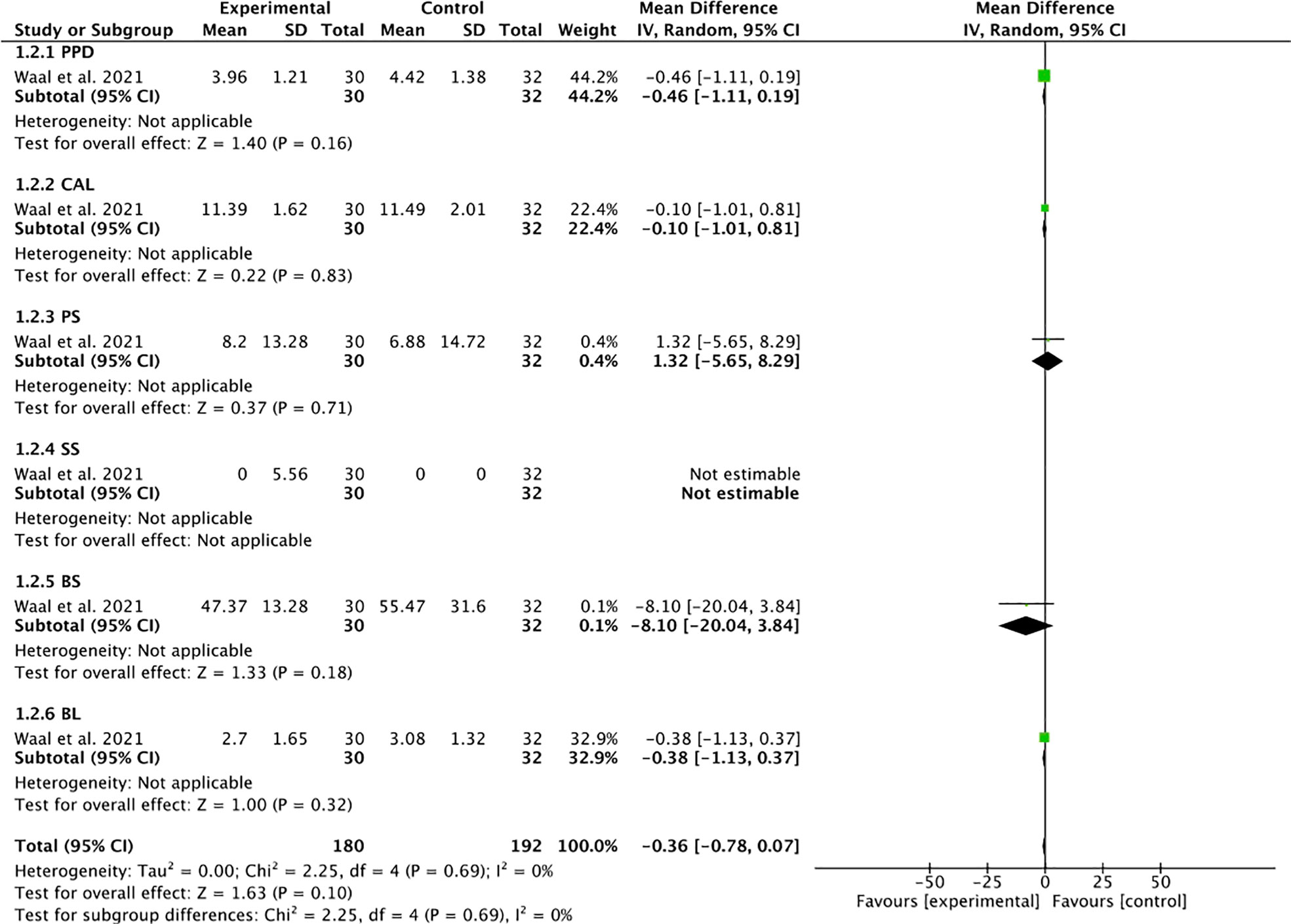
Figure 1 Forest plot for subgroup 2 (PPD, CAL, PS, SS, BS, BL).
2.6 Quality of the reports of the included studies
The Jadad scale (Oxford quality scoring system) (Jadad et al., 1996) defines the methodological quality of the studies based on the description of randomization, blinding, and dropouts, and was used to assess the methodological quality of the included studies. The scale ranges from 0 to 5: a score ≤2 means low quality of the reports and a score ≥3 means high quality.
2.7 Data analysis
Meta-analysis was performed using Review Manager (RevMan Software version 5.4.1; The Cochrane Collaboration, Copenhagen, Denmark; 2020). A meta-analysis was performed based on the mean difference (MD) and standard deviation (SD) to estimate effect size, with 95% confidence intervals (CI) for adverse event outcomes. The random-effects model was selected considering the uncertainty in I2 when few studies are used in the meta-analysis due to the expected methodological heterogeneity in the included studies. The heterogeneity was interpreted as follows: low I2 = 25%, moderate I2 = 50%, and high I2 = 75%. The threshold for statistical significance was defined as p < 0.05.
3 Results
3.1 Characteristics of the studies
A total of 38 studies were collected, of which 11 were from MEDLINE-PubMed, 9 from WOS, 9 from Embase, and 9 from the Cochrane Library; finally, five (Shibli et al., 2019; De Waal et al., 2021; Park et al., 2021; Blanco et al., 2022; Polymeri et al., 2022) were finally selected for meta-analysis. A good inter-reviewer agreement was obtained with a Cohen’s kappa index of κ = 80% (Figure 2).
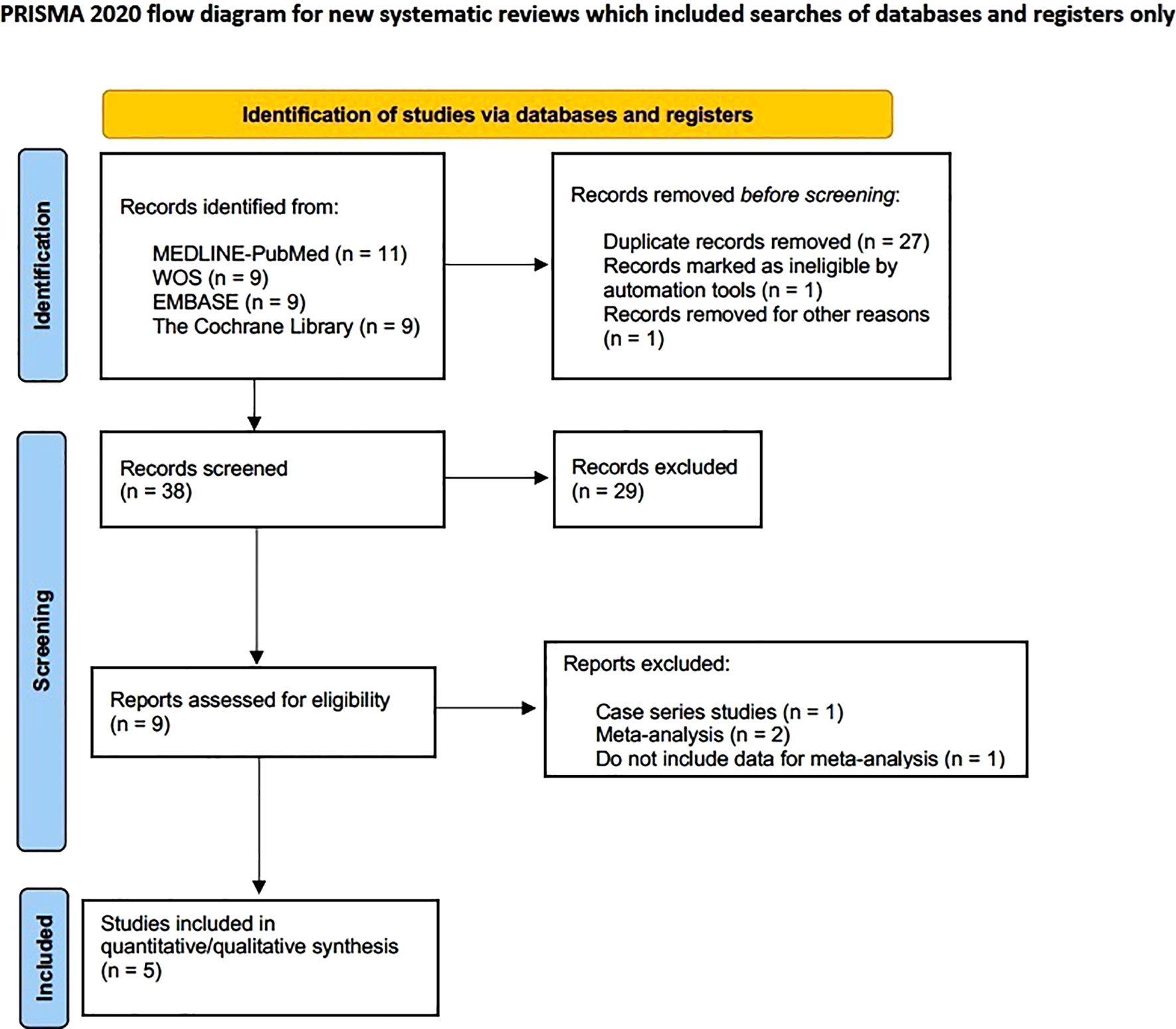
Figure 2 Flow diagram.
The studies with the largest sample size were a multicenter study on 118 patients (Park et al., 2021) and the study by De Waal et al. (2021) on 62 patients. The longest follow-up (12 months) was in the studies by Blanco et al. and De Waal et al (De Waal et al., 2021; Blanco et al., 2022). The study by Blanco et al. (2022) was the only one to use systemic metronidazole vs. placebo; the studies by Polymeri et al., De Waal et al., and Shibli et al (Shibli et al., 2019; De Waal et al., 2021; Polymeri et al., 2022). used amoxicillin together with metronidazole. The study by Park et al. (2021) used metronidazole and minocycline topically. Only the studies by Blanco et al. and Park et al (Park et al., 2021; Blanco et al., 2022). supported the use of metronidazole as an adjuvant in the treatment of peri-implantitis (Table 3).
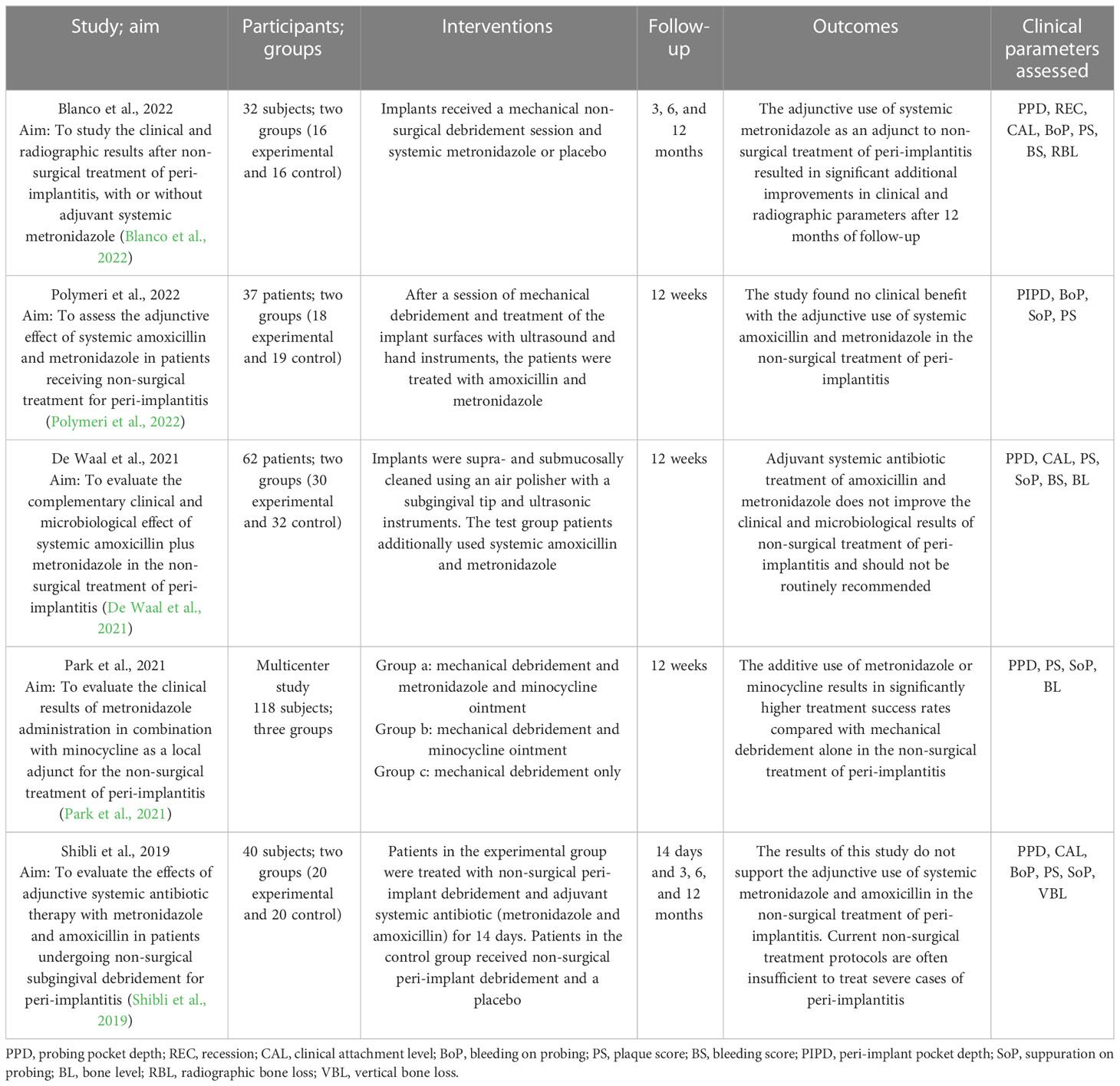
Table 3 General characteristics of the selected studies.
Table 4 describes the specific characteristics of the studies. Three indicated the pathogen studied (De Waal et al., 2021; Park et al., 2021; Blanco et al., 2022), two the type of implant (De Waal et al., 2021; Polymeri et al., 2022), and two more (Park et al., 2021; Blanco et al., 2022) used C-reactive protein (CRP) to detect and quantify bacterial DNA. To assess peri-implant marginal radiographic bone levels, all the included studies used intraoral radiographs. The Shapiro–Wilk test was the most commonly used in statistical analyses (Park et al., 2021; Blanco et al., 2022; Polymeri et al., 2022). A history of associated periodontitis was only considered in three of the studies (De Waal et al., 2021; Blanco et al., 2022; Polymeri et al., 2022).
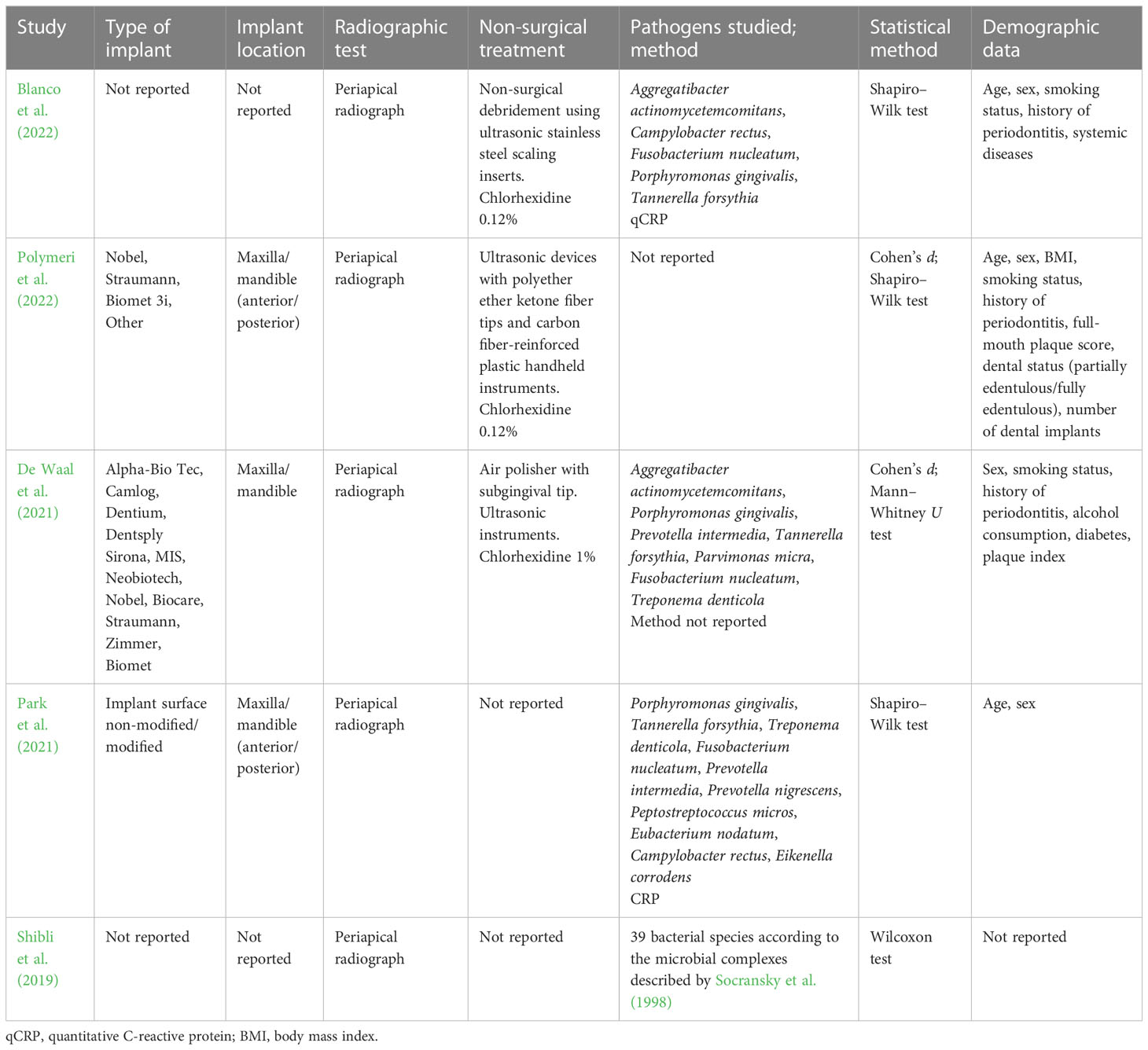
Table 4 Specific characteristics of the studies included.
3.2 Methodological quality
All the studies included in the meta-analysis achieved a score on the Jadad scale compatible with high methodological quality (≥3 points), with the study by Blanco et al. (2022) achieving the highest score (Table 5).
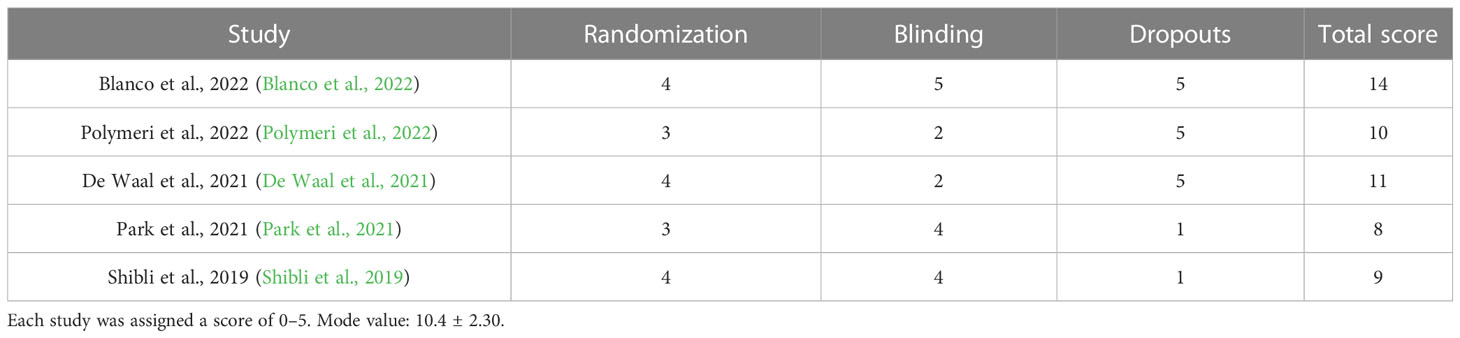
Table 5 Jadad quality score of randomized clinical trials (RCTs) included in the meta-analysis.
3.3 Risk of bias assessment
Of the five included studies (Shibli et al., 2019; De Waal et al., 2021; Park et al., 2021; Blanco et al., 2022; Polymeri et al., 2022), only four were included in the meta-analysis (Shibli et al., 2019; De Waal et al., 2021; Park et al., 2021; Blanco et al., 2022); the study by Polymeri et al. (2022) was excluded for presenting data in a non-analyzable form.
All studies met the domains of random sequence generation and blinding of participants and personnel; one study was biased in the incomplete outcome domain (Shibli et al., 2019), and all had unclear data in the domains of the incomplete outcome, blinding of outcome assessment, and allocation concealment. The study by Blanco et al. (2022) was the highest rated (Figure 3).
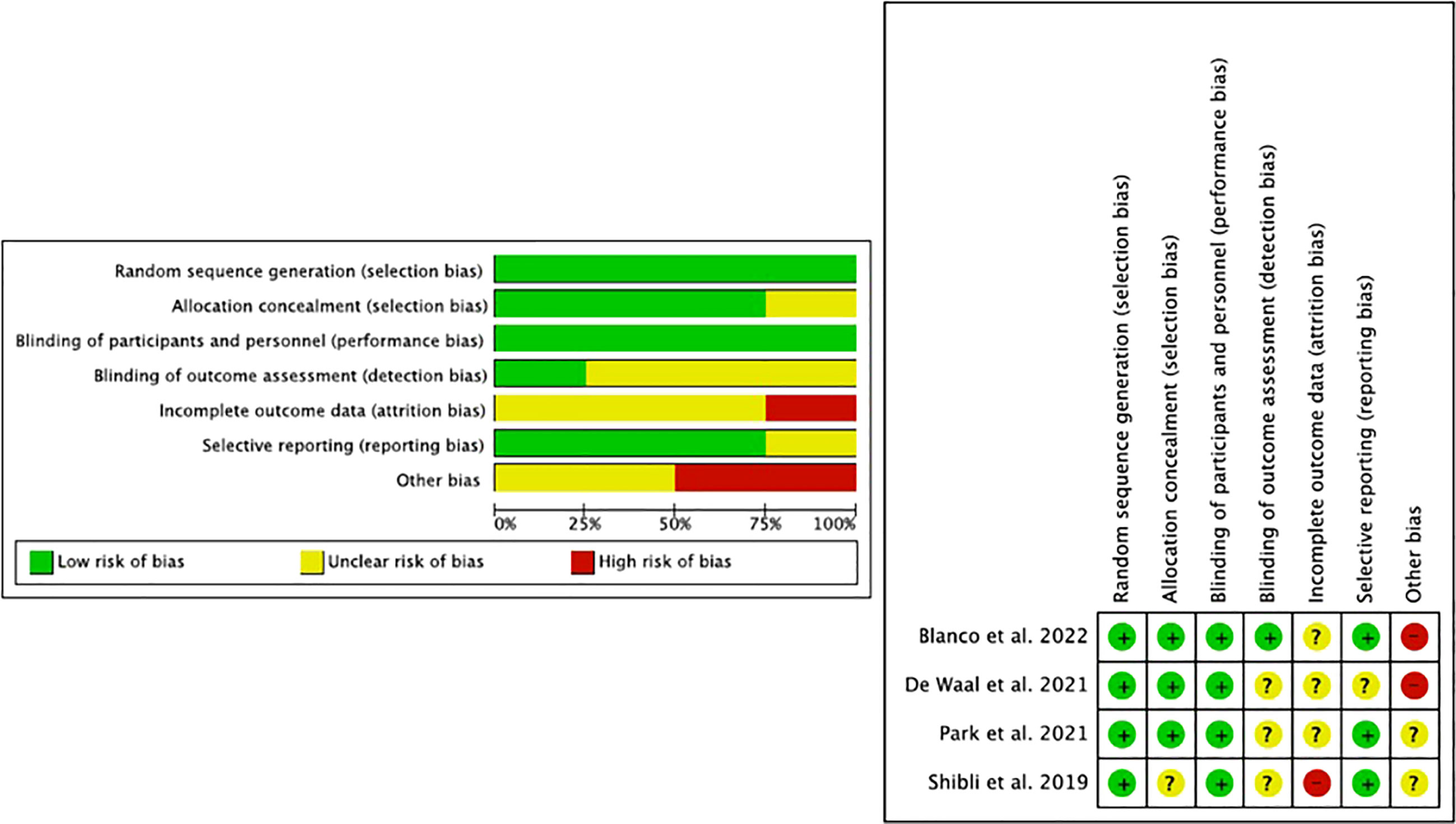
Figure 3 Risk of bias assessment.
3.4 Qualitative synthesis
The selected studies included a total of 289 patients, and follow-up periods ranged from 2 weeks to 1 year. The studies with the most complete follow-up were those by Blanco et al. (2022) and Shibli et al. (2019) at 3, 6, and 12 months. The plaque score (PS) parameter was considered in all the included studies, followed by the probing pocket depth (PPD) (Shibli et al., 2019; De Waal et al., 2021; Park et al., 2021; Blanco et al., 2022) and suppuration on probing (SoP) (Shibli et al., 2019; De Waal et al., 2021; Park et al., 2021; Polymeri et al., 2022) parameters. The bleeding score (BS) parameter was measured in only one study (De Waal et al., 2021) (Table 3). All studies included in the meta-analysis (Shibli et al., 2019; De Waal et al., 2021; Park et al., 2021; Blanco et al., 2022) used radiographic parameters to assess peri-implant marginal bone levels (Table 4). The bone level (BL) parameter was measured in two studies (De Waal et al., 2021; Park et al., 2021), radiographic bone loss (RBL) in one (Blanco et al., 2022), and vertical bone loss (VBL) in another (Shibli et al., 2019).
3.5 Quantitative synthesis and meta-analysis results
Only four of the included studies were used for meta-analysis (Shibli et al., 2019; De Waal et al., 2021; Park et al., 2021; Blanco et al., 2022). The highest weight was given to the multicenter study by Park et al. (2021) due to the high number of patients included in the study. Meta-analysis of adverse outcomes could not be performed due to a lack of data.
Heterogeneity was moderate in the analysis of grouped studies (I2 = 45%) (Figure 4). In the analysis by subgroups, total homogeneity was found in subgroup 2 (I2 = 0%) (Figure 1); subgroups 1 and 3 obtained moderate heterogeneity (I2 = 46% and I2 = 37%, respectively) (Figures 5, 6). Statistical significance was found only in the pooled analysis of the studies (p = 0.02) (95% CI) (Figure 4). Subgroup 2, which analyzed studies investigating PPD, clinical attachment level (CAL), PS, suppuration score (SS), BS, and BL (Figure 1), was the furthest from statistical significance (p = 0.69).
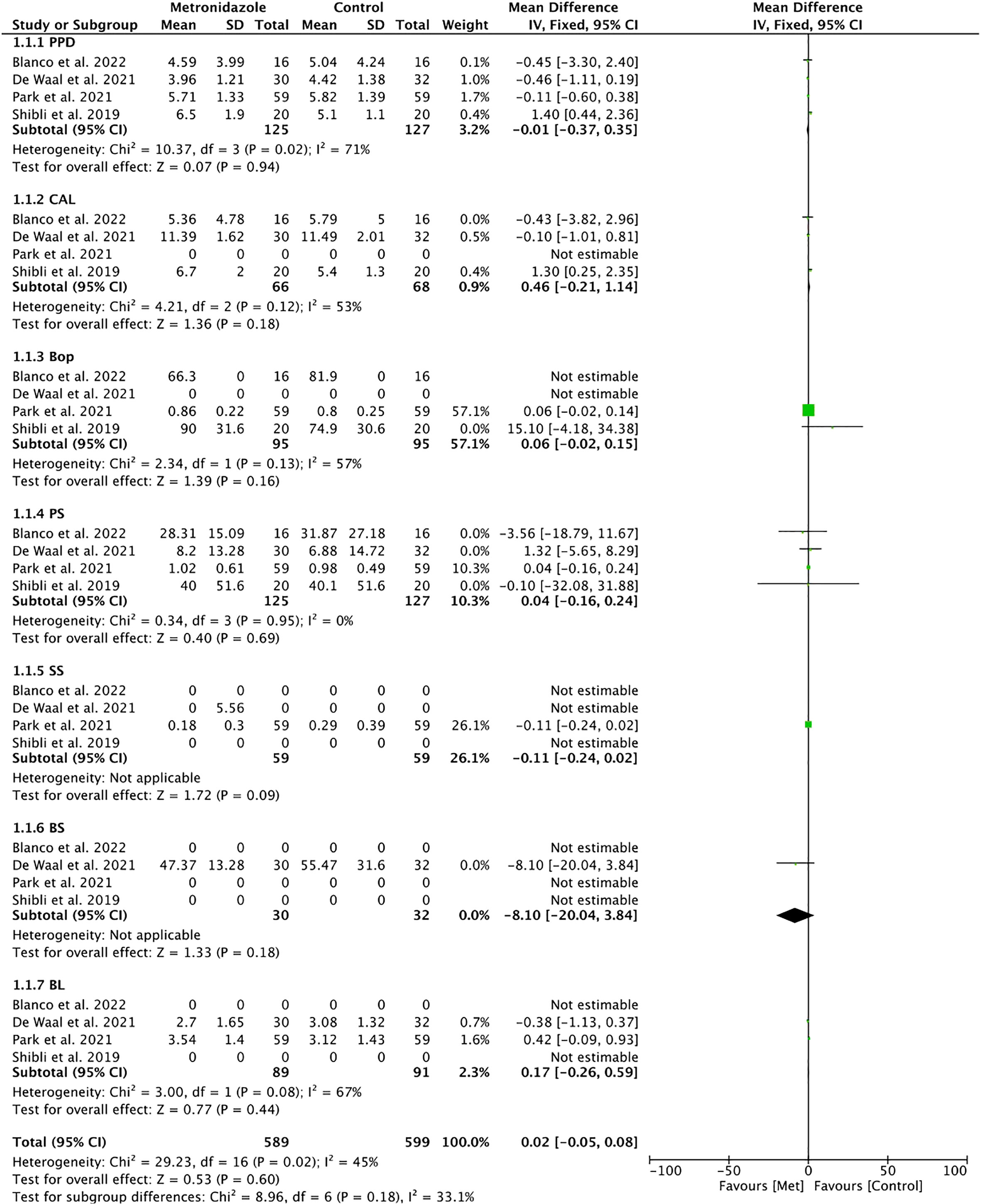
Figure 4 Forest plot for the grouped studies.
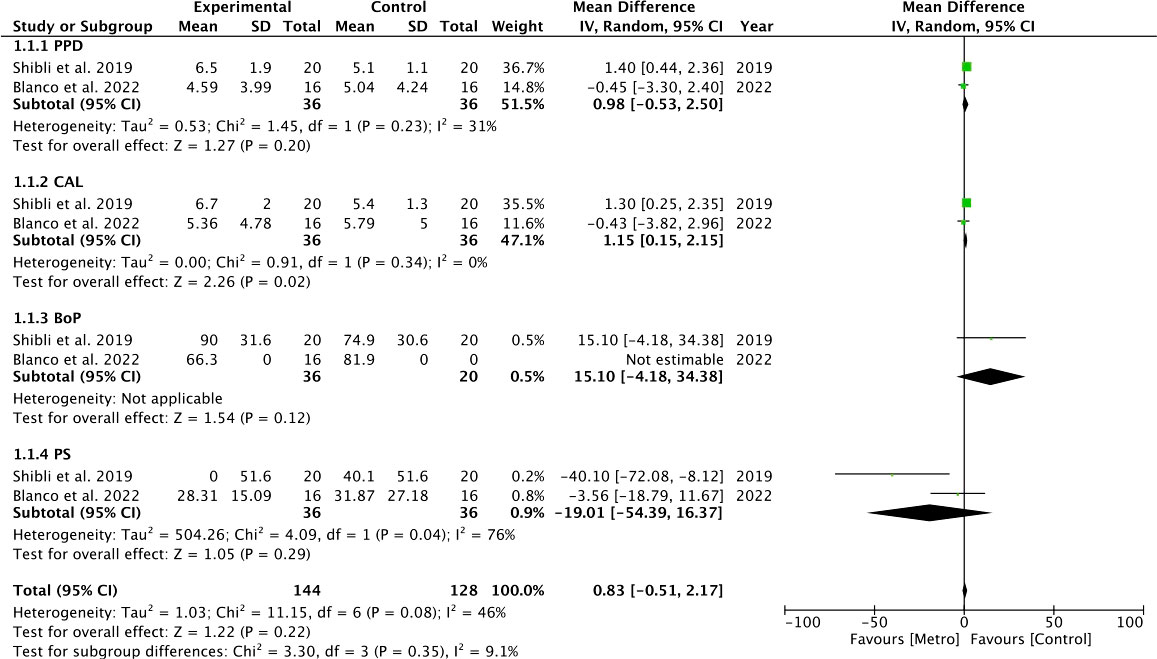
Figure 5 Forest plot for subgroup 1 (PPD, CAL, BoP, PS).
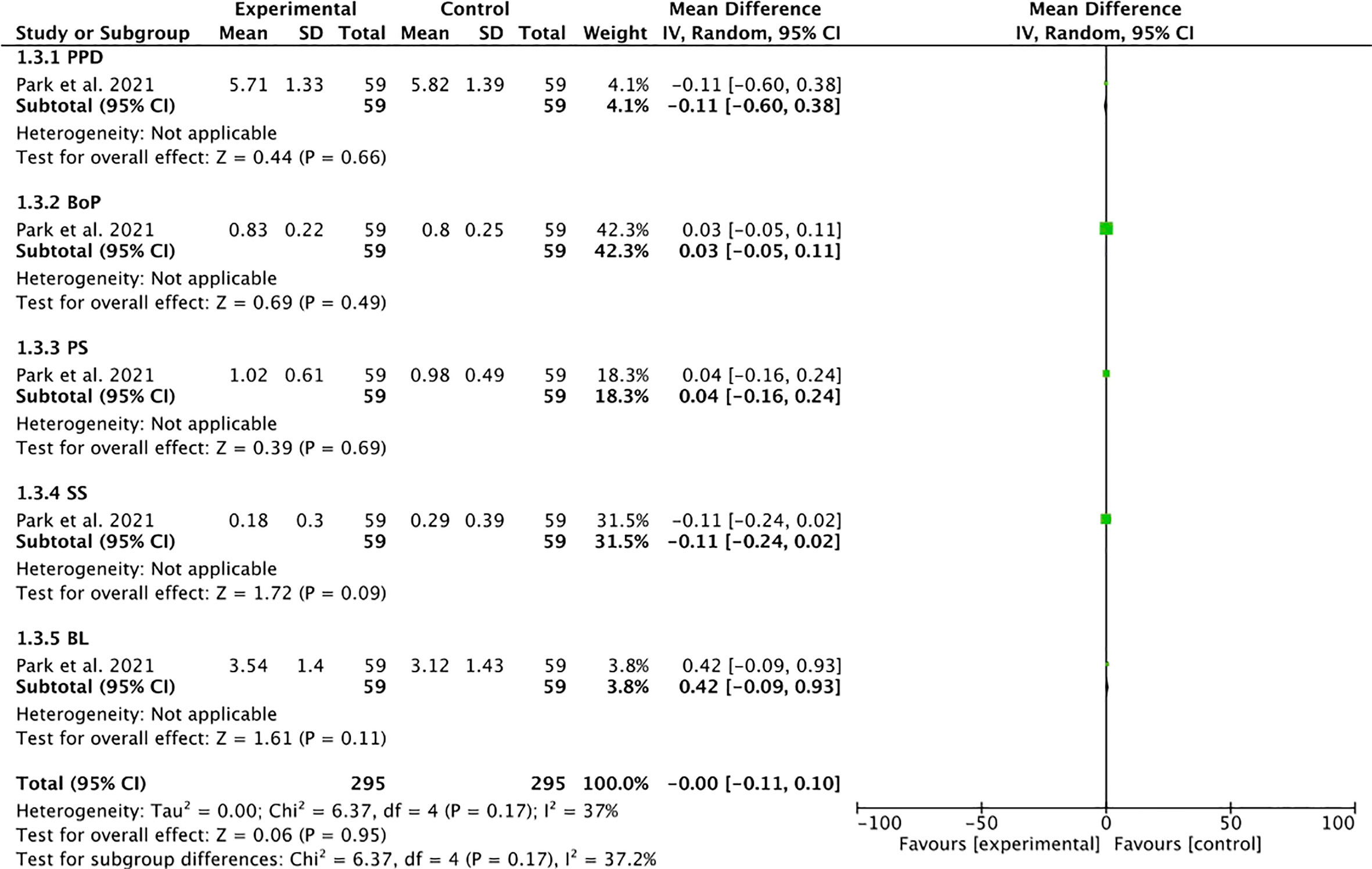
Figure 6 Forest plot for subgroup 3 (PPD, BoP, PS, SS, BL).
Three subgroups were performed for the radiographic values reported on peri-implant marginal bone levels: the first from the pooled studies included in the meta-analysis (Shibli et al., 2019; De Waal et al., 2021; Park et al., 2021; Blanco et al., 2022), the second from studies with a 3-month follow-up (De Waal et al., 2021; Park et al., 2021; Blanco et al., 2022), and the third from studies with a 12-month follow-up (Shibli et al., 2019; Blanco et al., 2022) (Figure 7). Heterogeneity was moderate for the three subgroups (I2 < 75%). Statistical significance (p = 0.03) was found only in the 3-month follow-up subgroup. The bone level loss was also analyzed separately in studies using systemic antibiotics (Shibli et al., 2019; De Waal et al., 2021; Blanco et al., 2022), finding overall homogeneity (I2 = 0%), so a fixed-effects model was performed; however, no statistical significance was found between groups (p = 0.60) (Figure 8). The study by Park et al. (2021), in which topical antibiotics were used, could not be analyzed because it only provided data at the bone level at the baseline of treatment.
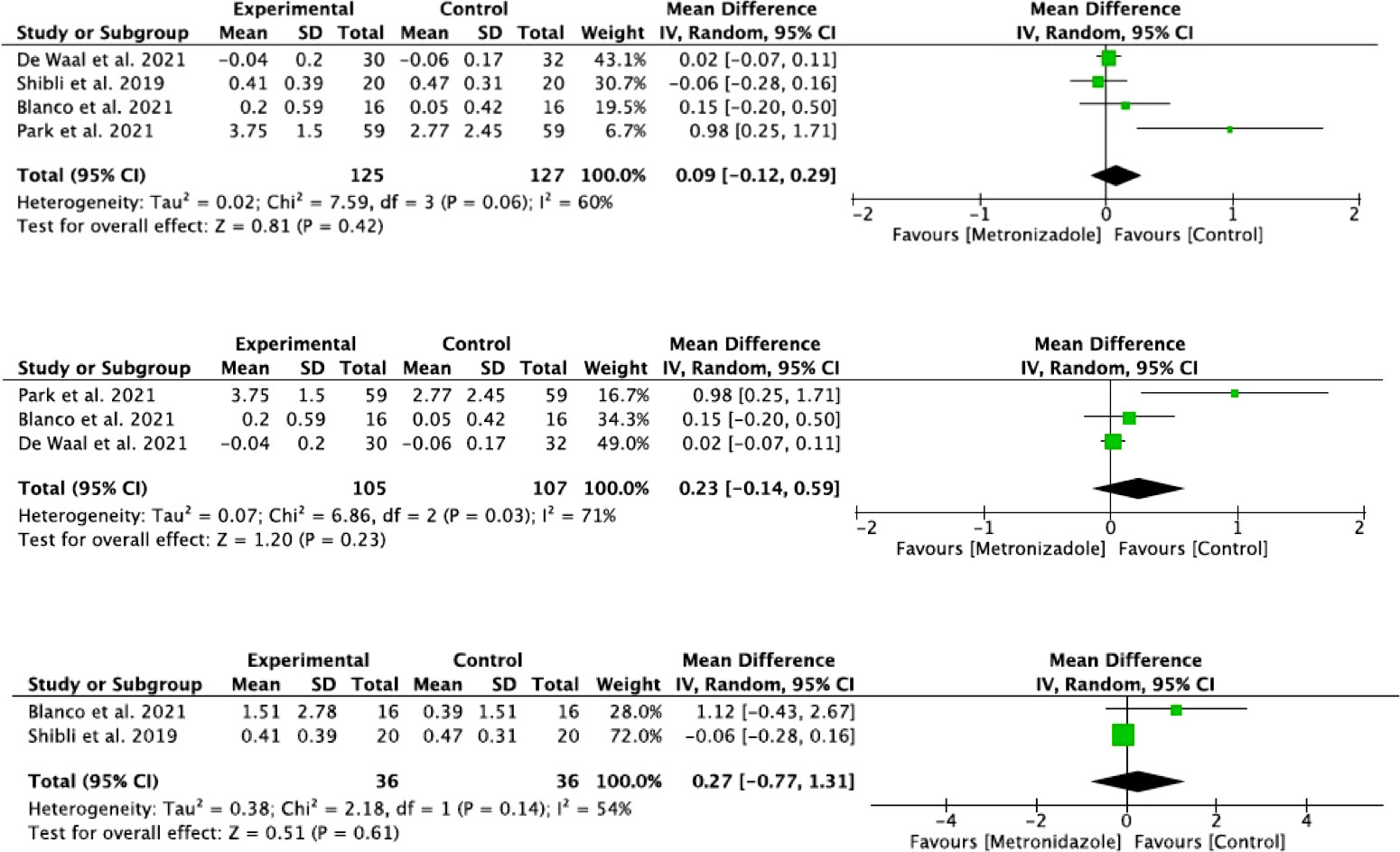
Figure 7 Forest plot for radiographic evaluation of all studies: radiographic evaluation of studies with a 3-month follow-up and radiographic evaluation of studies with a 12-month follow-up.

Figure 8 Forest plot for BL of studies in which systemic antibiotics were used.
3.6 Publication bias
Although we are aware that publication bias is not advisable when the meta-analysis is composed of fewer than 10 studies (Higgins and Thompson, 2002) (as is our case), we preferred to include it in the overall analysis.
The funnel plot analysis suggested moderate publication bias. In general, the estimated effect is associated with the horizontal axis and the sample size with the vertical axis. The studies that measured BoP (Shibli et al., 2019; Blanco et al., 2022; Polymeri et al., 2022) showed the greatest asymmetry (Figure 9).
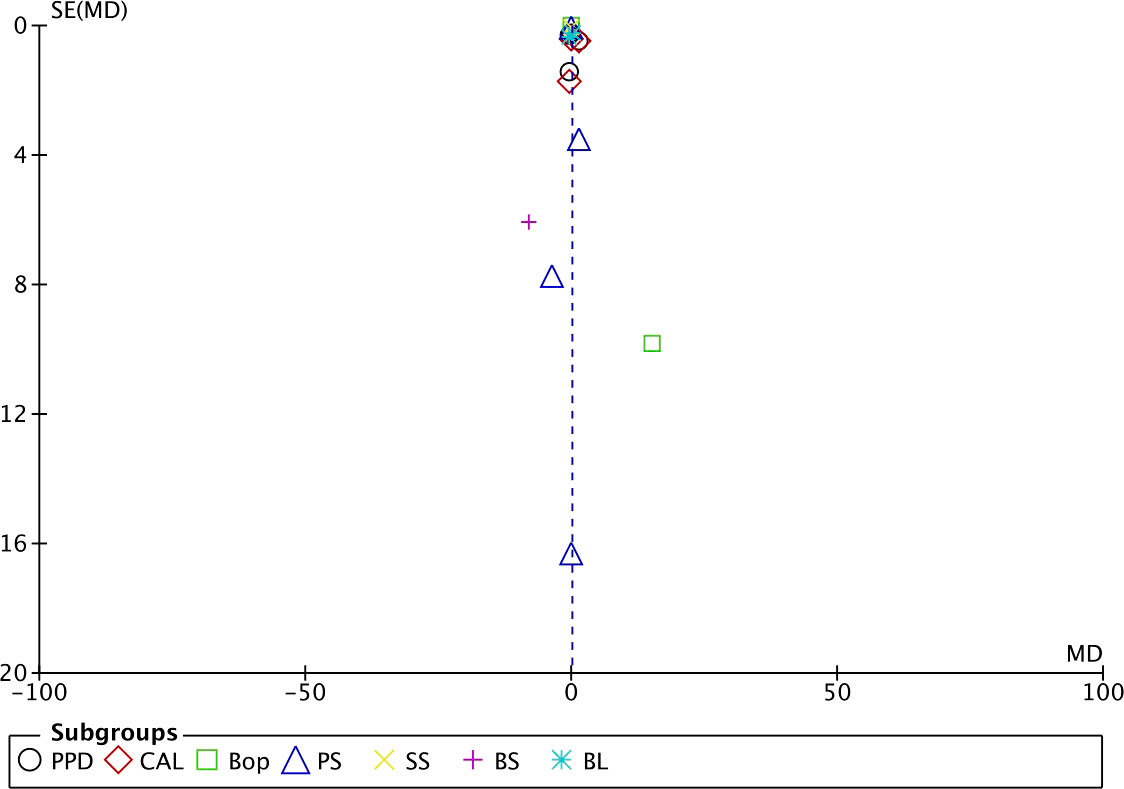
Figure 9 Funnel plot.
4 Discussion
Systematic reviews on the efficacy of adjuvant antibiotics in the treatment of peri-implantitis are scarce, and we did not find any meta-analysis that analyzed the efficacy of this antimicrobial (i.e., metronidazole), so this systematic review aimed to evaluate the efficacy of metronidazole as an adjuvant in the treatment of peri-implantitis. In total, five RCTs were included in the analysis, of which four were analyzed and one was eliminated for providing non-analyzable data.
The absence of BoP is evidence of the absence of inflammation, which should be the first target in the treatment of peri-implantitis, and according to recent recommendations, the results of peri-implantitis treatment should be evaluated after 6 months of healing, based on outcomes including multiple parameters: bone fill, peri-implant soft tissue recession, BoP, SoP, and PPD (Sanz and Chapple, 2012). However, in our meta-analysis, only the studies by Blanco et al. and Shibli et al (Shibli et al., 2019; Blanco et al., 2022). performed a 3-, 6-, and 12-month follow-up; the studies by De Waal et al. and Park et al (De Waal et al., 2021; Park et al., 2021). performed a single 12-week follow-up.
Mombelli and Decaillet (Mombelli and Décaillet, 2011) highlighted the growth of gram-negative anaerobic species in peri-implant pockets, compatible with peri-implantitis, and that peri-implant disease can be considered a mixed anaerobic infection, warning of the benefits of combined mechanical and chemical treatments. All the studies included in our meta-analysis combined mechanical debridement and adjuvant antibiotic treatment; however, in this aspect, several studies have demonstrated the benefits of the use of systemic antibiotics as an adjunct to non-surgical treatment of peri-implantitis (Liñares et al., 2019; Nart et al., 2020), although a Cochrane systematic review (Esposito et al., 2012) warned that there is no reliable evidence to suggest which interventions might be the most effective in the treatment of this pathology. A recent systematic review and meta-analysis by Ramanauskaite et al. (2021) found that adjunctive reconstructive measures in conjunction with surgical treatment of peri-implantitis were beneficial in terms of radiographic reduction of the bony defect and reduced soft tissue recession, despite not improving mucosal inflammation; likewise, systemic antibiotics did not provide any benefit to the outcomes of non-reconstructive surgical treatment of peri-implantitis.
According to the results obtained in our study, the pooled RCT analysis demonstrated the effect of metronidazole as an adjuvant treatment after 12 weeks (p = 0.02). A statistically significant result (p = 0.03) was also obtained in the analysis of studies with shorter follow-up (3 months).
Blanco et al. (2022) obtained at 12 months a significant reduction in PPD (2.53 vs. 1.02 mm) and CAL (2.14 vs. 0.53 mm) in the test group compared with the control group. Similarly, Shibili et al (Shibli et al., 2019). with metronidazole plus adjuvant amoxicillin found at 12 months a probing reduction of 3.1 mm in the antibiotic group vs. 1.8 mm in the control group, despite including in their study compromised cases, with PD >5 mm, peri-implant bone loss >4 mm, and BoP and/or SoP. Studies, such as Cionca et al. using systemic metronidazole and amoxicillin, significantly improved clinical outcomes at 6 months after non-surgical full-mouth periodontal debridement, thus significantly reducing the need for additional treatment (Cionca et al., 2009). In contrast, the studies by Polymeri et al., de Waal et al., and Park et al (De Waal et al., 2021; Park et al., 2021; Polymeri et al., 2022). found no clinical benefits with adjunctive antibiotic treatment; the results coincided with Stein et al. (2017) who found that, in a study of 45 patients with chronic periodontitis, carriers of 164 implants with peri-implantitis, treatment with adjunctive metronidazole/amoxicillin had no significant benefits in the changes in mean PPD, CAL, and BoP values at 12 months of treatment. Blanco et al. (2022), with the use of metronidazole as adjuvant treatment, found a significantly higher radiographic bone gain at 12 months in the test group compared with the control group (2.15 mm test vs. 0.95 mm control). In contrast, Shibli et al., with metronidazole and amoxicillin and the same follow-up time, found no significant differences between the groups (Shibli et al., 2019). In this regard, some authors have even suggested that the prescription of amoxicillin plus metronidazole as an adjunct to non-surgical treatment should be limited to patients with specific microbiological profiles, especially those positive for A. actinomycetemcomitans, as this germ is known to resist mechanical treatment particularly well (Mombelli et al., 2000; Dannewitz et al., 2007); however, Mombelli et al. (2013), in a longitudinal study of 82 patients with 41 positive cases for A. actinomycetemcomitans and 41 negative cases, also found no specific benefit from the use of metronidazole in combination with amoxicillin.
Certain similarities in terms of biomarkers of bone destruction and causative microbial agents, in peri-implant and periodontal pathologies and the frequent coincidence of both in the same patient, have led some researchers to investigate both pathologies together or to design studies on peri-implantitis based on those performed on periodontitis (Mombelli and Décaillet, 2011), although Liu et al. and Zhang et al (Liu et al., 2020; Zhang et al., 2022). observed that peri-implantitis and periodontitis have significantly different microRNA and long-chain RNA expression profiles, indicating that osteoclast differentiation pathways are more active in peri-implantitis than in periodontitis.
On the other hand, it is known that an individual’s immune response to bacterial aggression is influenced by genetic and epigenetic factors, as well as environmental factors. It has been shown that inflammatory diseases, such as peri-implantitis and periodontitis, can be enhanced by epigenetic modifications in certain subjects (Larsson et al., 2022). A recent systematic review concluded with the need for future research to explore the functional role of specific microRNAs and their possible role as therapeutic targets (Asa'ad et al., 2020). A correlation between IL-1-specific gene polymorphisms and peri-implant bone loss has also been described in smoking subjects, although smoking is not considered a conclusive risk factor (Feloutzis et al., 2003; Dreyer et al., 2018; Schwarz et al., 2018).
The present meta-analysis has some limits that must be emphasized. On the one hand, the included studies used local and systemic adjuvant antibiotics; on the other hand, only the study by Blanco et al. (2022) used metronidazole as an adjuvant treatment; all the others (Shibli et al., 2019; De Waal et al., 2021; Park et al., 2021) used metronidazole combined with other antibiotics. Another aspect to consider would be the different implant surfaces used in the studies. It has been reported that the mean peri-implant bone loss around moderately and minimally roughened surfaces is less than around roughened surfaces; however, certain studies have reported that the clinical impact of surface roughness alone on bone loss and the risk of peri-implantitis appears to be rather limited and of minimal clinical importance (Renvert et al., 2011; De Bruyn et al., 2017). Only three of the studies included in our meta-analysis took into account implant type or surface modification (De Waal et al., 2021; Park et al., 2021; Polymeri et al., 2022), yet all considered age, sex of patients, and location of inserted implants, although Dreyer et al (Feloutzis et al., 2003), in a systematic review, reported with a medium–high level of evidence that the age and sex of the patients were not related to peri-implantitis.
On the other hand, Song et al. (2020) proposed that implants placed in anterior regions, both maxillary and mandibular, would have a higher prevalence of peri-implantitis compared with posterior regions, and in our meta-analysis, only two of the included studies (De Waal et al., 2021; Park et al., 2021) reported on the site of implant placement; they also combined implants in the anterior and posterior sites. However, some studies have drawn attention to the “clustering effect,” considering that implants placed in the same mouth should not be considered as independent (Pikner and Gröndahl, 2009).
The outcome reports of the included studies were conducted at different time periods, and although Sanz et al (Sanz and Chapple, 2012). recommend evaluating the results of peri-implantitis treatment 6 months after healing, we have not found unanimity in this recommendation; a systematic review by Heitz-Mayfield and Mombelli chose a 12-month re-evaluation period to evaluate the satisfactory outcome of treatment (Heitz-Mayfield and Mombelli, 2014).
Finally, although all studies used radiographic evaluation by intraoral radiography to assess the peri-implant bone loss, there are other useful radiographic techniques, such as multislice computed tomography and cone-beam volumetric imaging, which offer certain advantages to implant dentistry, such as the representation of intraosseous lesions in three planes, on a real scale and without overlapping or distortion. In addition, computer-assisted image analysis, such as subtraction radiography, allows the detection of small changes in bone density (Heitz-Mayfield, 2008; Naveau et al., 2019; Trivedi et al., 2022). The different cutoff levels reported for the different clinical parameters and the different methods of statistical analysis in the included studies should also be taken into account; only three of them (Park et al., 2021; Blanco et al., 2022; Polymeri et al., 2022) resorted to the Shapiro–Wilk test to contrast the normality of the data.
All this could bias the results, and therefore, the results obtained in our meta-analysis should be taken with caution.
Therefore, we consider that the decision on a specific adjuvant antibiotic treatment should be made individually for each patient, taking into account the severity and extent of peri-implantitis and possible concomitant periodontitis, as well as the number of affected areas requiring treatment. Likewise, the potential risk of the development of strains resistant to metronidazole or to the chosen antimicrobial combination should be taken into account, and the protocol to be followed in each indicated situation should be carefully decided (Ardila et al., 2010; Veloo et al., 2012). On the other hand, the approach to incipient peri-implantitis is of vital importance, since bone defects in advanced stages require complete debridement and repositioning of the marginal mucosa to allow the patient effective oral hygiene, generally compromising the esthetic outcome of prosthetic restorations (Figuero et al., 2014).
5 Conclusions
Adjuvant local or systemic administration of metronidazole in the treatment of peri-implantitis remains of questionable efficacy and with serious discrepancies among investigators.
Due to the heterogeneity of the types of treatment, the reported administration protocols, and, ultimately, the heterogeneity of the studies, we have not been able to draw definitive conclusions about its effect in the adjuvant treatment of peri-implantitis.
In certain pathologic situations of peri-implantitis, metronidazole, alone or in combination with other antibiotics, could be beneficial as an adjuvant to surgical treatment, always weighing the benefits against the disadvantages.
Long-term RCTs with standardized methodologies would be desirable and justifiable to determine the exact role of metronidazole as an adjuvant treatment for peri-implantitis.
Author contributions
Conceptualization: NL-V and AL-V. Methodology: NL-V. Validation: JB-R. Formal analysis: NL-V. Resources: AL-V. Data curation: NL-V. Writing—original draft preparation: NL-V. Writing—review and editing: NL-V and AL-V. All authors contributed to the article and approved the submitted version.
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Ardila, C. M., Granada, M. I., Guzmán, I. C. (2010). Antibiotic resistance of subgingival species in chronic periodontitis patients. J. Periodontal Res. 45, 557–563. doi: 10.1111/j.1600-0765.2010.01274.x
Asa'ad, F., Garaicoa-Pazmiño, C., Dahlin, C., Larsson, L. (2020). Expression of MicroRNAs in periodontal and peri-implant diseases: a systematic review and meta-analysis. Int. J. Mol. Sci. 21, 4147. doi: 10.3390/ijms21114147
Berglundh, T., Armitage, G., Araujo, M. G., Avila-Ortiz, G., Blanco, J., Camargo, P. M., et al. (2018). Peri-implant diseases and conditions: consensus report of workgroup 4 of the 2017 world workshop on the classification of periodontal and peri-implant diseases and conditions. J. Clin. Periodontol. 45, SS286–SS291. doi: 10.1111/jcpe.12957
Blanco, C., Pico, A., Dopico, J., Gándara, P., Blanco, J., Liñares, A. (2022). Adjunctive benefits of systemic metronidazole on non-surgical treatment of peri-implantitis. a randomized placebo-controlled clinical trial. J. Clin. Periodontol. 49, 15–27. doi: 10.1111/jcpe.13564
Cionca, N., Giannopoulou, C., Ugolotti, G., Mombelli, A. (2009). Amoxicillin and metronidazole as an adjunct to full-mouth scaling and root planing of chronic periodontitis. J. Periodontol. 80, 364–371. doi: 10.1902/jop.2009.080540
Cohen, J. (1968). Weighted kappa: nominal scale agreement with provision for scaled disagreement or partial credit. Psychol. Bull. 70, 213–220. doi: 10.1037/h0026256
Dannewitz, B., Pohl, S., Eickholz, P., Kim, T. S. (2007). Clinical and microbiological effects of a combined mechanic-antibiotic therapy in subjects with actinobacillus actinomycetemcomitans-associated periodontitis. Am. J. Dent. 20, 153–156.
De Bruyn, H., Christiaens, V., Doornewaard, R., Jacobsson, M., Cosyn, J., Jacquet, W., et al. (2017). Implant surface roughness and patient factors on long-term peri-implant bone loss. Periodontol 73, 218–227. doi: 10.1111/prd.12177
De Waal, Y. C. M., Vangsted, T. E., Van Winkelhoff, A. J. (2021). Systemic antibiotic therapy as an adjunct to non-surgical peri-implantitis treatment: a single-blind RCT. J. Clin. Periodontol. 48, 996–1006. doi: 10.1111/jcpe.13464
Dreyer, H., Grischke, J., Tiede, C., Eberhard, J., Schweitzer, A., Toikkanen, S. E., et al. (2018). Epidemiology and risk factors of peri-implantitis: a systematic review. J. Periodontal Res. 53, 657–681. doi: 10.1111/jre.12562
Esposito, M., Grusovin, M. G., Worthington, H. V. (2012). Treatment of peri-implantitis: what interventions are effective? A Cochrane systematic review. Eur. J. Oral. Implantol. 5, 21–41.
Feloutzis, A., Lang, N. P., Tonetti, M. S., Bürgin, W., Brägger, U., Buser, D., et al. (2003). IL-1 gene polymorphism and smoking as risk factors for peri-implant bone loss in a well-maintained population. Clin. Oral. Implants Res. 14, 10–17. doi: 10.1034/j.1600-0501.2003.140102.x
Figuero, E., Graziani, F., Sanz, I., Herrera, D., Sanz, M. (2014). Management of peri-implant mucositis and peri-implantitis. Periodontol 66, 255–273. doi: 10.1111/prd.12049
Heitz-Mayfield, L. J. (2008). Peri-implant diseases: diagnosis and risk indicators. J. Clin. Periodontol. 35, 292–304. doi: 10.1111/j.1600-051X.2008.01275.x
Heitz-Mayfield, L. J., Mombelli, A. (2014). The therapy of peri-implantitis: a systematic review. Int. J. Oral. Maxillofac. Implants. 29, 325–345. doi: 10.11607/jomi.2014suppl.g5.3
Higgins, J. P., Thompson, S. G. (2002). Quantifying heterogeneity in a meta-analysis. Stat. Med. 21, 1539–1558. doi: 10.1002/sim.1186
Jadad, A. R., Moore, R. A., Carroll, D., Jenkinson, C., Reynolds, D. J., Gavaghan, D. J., et al. (1996). Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin. Trials. 17, 1–12. doi: 10.1016/0197-2456(95)00134-4
Javed, F., Alghamdi, A. S., Ahmed, A., Mikami, T., Ahmed, H. B., Tenenbaum, H. C. (2013). Clinical efficacy of antibiotics in the treatment of peri-implantitis. Int. Dent. J. 63, 169–176. doi: 10.1111/idj.12034
Jiang, Q., Yu, Y., Xu, R., Zhang, Z., Liang, C., Sun, H., et al. (2021). The temporal shift of peri-implant microbiota during the biofilm formation and maturation in a canine model. Microb. Pathog. 158, 105100. doi: 10.1016/j.micpath.2021.105100
Koldsland, O. C., Scheie, A. A., Aass, A. M. (2010). Prevalence of peri-implantitis related to severity of the disease with different degrees of bone loss. J. Periodontol. 81, 231–238. doi: 10.1902/jop.2009.090269
Larsson, L., Kavanagh, N. M., Nguyen, T. V. N., Castilho, R. M., Berglundh, T., Giannobile, W. V. (2022). Influence of epigenetics on periodontitis and peri-implantitis pathogenesis. Periodontol 90, 125–137. doi: 10.1111/prd.12453
Liñares, A., Pico, A., Blanco, C., Blanco, J. (2019). Adjunctive systemic metronidazole to nonsurgical therapy of peri-implantitis with intrabony defects: a retrospective case series study. Int. J. Oral. Maxillofac. Implants. 34, 1237–1245. doi: 10.11607/jomi.7343
Liu, Y., Liu, Q., Li, Z., Acharya, A., Chen, D., Chen, Z., et al. (2020). Long non-coding RNA and mRNA expression profiles in peri-implantitis vs periodontitis. J. Periodontal Res. 55, 342–353. doi: 10.1111/jre.12718
Minozzi, S., Dwan, K., Borrelli, F., Filippin, G. (2022). Reliability of the revised cochrane risk-of-bias tool for randomised trials (RoB2) improved with the use of implementation instruction. J. Clin. Epidemiol. 141, 99–105. doi: 10.1016/j.jclinepi.2021.09.021
Mombelli, A., Cionca, N., Almaghlouth, A., Décaillet, F., Courvoisier, D. S., Giannopoulou, C. (2013). Are there specific benefits of amoxicillin plus metronidazole in aggregatibacter actinomycetemcomitans-associated periodontitis? double-masked, of efficacy and safety. J. Periodontol 84, 715–724. doi: 10.1902/jop.2012.120281
Mombelli, A., Décaillet, F. (2011). The characteristics of biofilms in peri-implant disease. J. Clin. Periodontol. 38, 203–213. doi: 10.1111/j.1600-051X.2010.01666.x
Mombelli, A., Schmid, B., Rutar, A., Lang, N. P. (2000). Persistence patterns of porphyromonas gingivalis, prevotella intermedia/nigrescens, and actinobacillus actinomyetemcomitans after mechanical therapy of periodontal disease. J. Periodontol. 71, 14–21. doi: 10.1902/jop.2000.71.1.14
Mulla, M., Mulla, M., Hegde, S., Koshy, A. V. (2021). In vitro assessment of the effect of probiotic lactobacillus reuteri on peri-implantitis microflora. BMC Oral. Health 21, 408. doi: 10.1186/s12903-021-01762-2
Nart, J., Pons, R., Valles, C., Esmatges, A., Sanz-Martín, I., Monje, A. (2020). Non-surgical therapeutic outcomes of peri-implantitis: 12-month results. Clin. Oral. Investig. 24, 675–682. doi: 10.1007/s00784-019-02943-8
Naveau, A., Shinmyouzu, K., Moore, C., Avivi-Arber, L., Jokerst, J., Koka, S. (2019). Etiology and measurement of peri-implant crestal bone loss (CBL). J. Clin. Med. 8, 166. doi: 10.3390/jcm8020166
Page, M. J., McKenzie, J. E., Bossuyt, P. M., Boutron, I., Hoffmann, T. C., Mulrow, C. D., et al. (2021). The PRISMA (2020). statement: an updated guideline for reporting systematic reviews. BMJ 29 (372), n71. doi: 10.1016/j.ijsu.2021.105906
Park, S. H., Song, Y. W., Cha, J. K., Lee, J. S., Kim, Y. T., Shin, H. S., et al. (2021). Adjunctive use of metronidazole-minocycline ointment in the nonsurgical treatment of peri-implantitis: a multicenter randomized controlled trial. Clin. Implant Dent. Relat. Res. 23, 543–554. doi: 10.1111/cid.13006
Persson, G. R., Renvert, S. (2014). Cluster of bacteria associated with peri-implantitis. Clin. Implant Dent. Relat. Res. 16, 783–793. doi: 10.1111/cid.12052
Pikner, S. S., Gröndahl, K. (2009). Radiographic analyses of "advanced" marginal bone loss around brånemark dental implants. Clin. Implant Dent. Relat. Res. 11, 120–133. doi: 10.1111/j.1708-8208.2008.00098.x
Polymeri, A., van der Horst, J., Anssari Moin, D., Wismeijer, D., Loos, B. G., Laine, M. L. (2022). Non-surgical peri-implantitis treatment with or without systemic antibiotics: a randomized controlled clinical trial. Clin. Oral. Implants Res. 33, 548–557. doi: 10.1111/clr.13914
Ramanauskaite, A., Fretwurst, T., Schwarz, F. (2021). Efficacy of alternative or adjunctive measures to conventional non-surgical and surgical treatment of peri-implant mucositis and peri-implantitis: a systematic review and meta-analysis. Int. J. Implant Dent. 7, 112. doi: 10.1186/s40729-021-00388-x
Renvert, S., Polyzois, I., Claffey, N. (2011). How do implant surface characteristics influence peri-implant disease? J. Clin. Periodontol. 38, 214–222. doi: 10.1111/j.1600-051X.2010.01661.x
Renvert, S., Roos-Jansåker, A. M., Claffey, N. (2008). Non-surgical treatment of peri-implant mucositis and peri-implantitis: a literature review. J. Clin. Periodontol. 35, 305–315. doi: 10.1111/j.1600-051X.2008.01276.x
Rodrigo, D., Sanz-Sánchez, I., Figuero, E., Llodrá, J. C., Bravo, M., Caffesse, R. G., et al. (2018). Prevalence and risk indicators of peri-implant diseases in Spain. J. Clin. Periodontol. 45, 1510–1520. doi: 10.1111/jcpe.13017
Sahrmann, P., Gilli, F., Wiedemeier, D. B., Attin, T., Schmidlin, P. R., Karygianni, L. (2020). The microbiome of peri-implantitis: a systematic review and meta-analysis. Microorganisms 8, 661. doi: 10.3390/microorganisms8050661
Sanz, M., Chapple, I. L. (2012). Clinical research on peri-implant diseases: consensus report of working group 4. working group 4 of the VIII European workshop on periodontology. J. Clin. Periodontol. 39, 202–206. doi: 10.1111/j.1600-051X.2011.01837.x
Schwarz, F., Bieling, K., Nuesry, E., Sculean, A., Becker, J. (2006). Clinical and histological healing pattern of peri-implantitis lesions following non-surgical treatment with an Er:YAG laser. Lasers Surg. Med. 38, 663–671. doi: 10.1002/lsm.20347
Schwarz, F., Derks, J., Monje, A., Wang, H. L. (2018). Peri-implantitis. J. Clin. Periodontol. 45, S246–S266. doi: 10.1002/JPER.16-0350
Shibli, J. A., Ferrari, D. S., Sirom, R. S., Figueiredo, L. C., Faveri, M., Feres, M. (2019). Microbiological and clinical effects of adjunctive systemic metronidazole and amoxicillin in the non-surgical treatment of peri-implantitis: 1 year follow-up. Braz. Oral. Res. 33, e080. doi: 10.1590/1807-3107bor-2019.vol33.0080
Smeets, R., Henningsen, A., Jung, O., Heiland, M., Hammächer, C., Stein, J. M. (2014). Definition, etiology, prevention and treatment of peri-implantitis–a review. Head Face Med. 10, 34. doi: 10.1186/1746-160X-10-34
Socransky, S. S., Haffajee, A. D., Cugini, M. A., Smith, C., Kent, R. L., Jr. (1998). Microbial complexes in subgingival plaque. J. Clin. Periodontol. 25, 134–144. doi: 10.1111/j.1600-051X.1998.tb02419.x
Song, X., Li, L., Gou, H., Xu, Y. (2020). Impact of implant location on the prevalence of peri-implantitis: a systematic review and meta- analysis. J. Dent. 103, 103490. doi: 10.1016/j.jdent.2020.103490
Stein, J. M., Hammächer, C., Said-Yekta Michael, S. (2017). Combination of ultrasonic decontamination, soft tissue curettage and submucosal air polishing with povidone-iodine application for non-surgical therapy of peri-implantitis: 12 months clinical outcomes. J. Periodontol. 15, 1–13. doi: 10.1902/jop.2017.170362
Trivedi, A., Trivedi, S., Narang, H., Sarkar, P., Sehdev, B., Pendyala, G., et al. (2022). Evaluation of pre- and post-loading peri-implant crestal bone levels using cone-beam computed tomography: an In vivo study. J. Contemp Dent. Pract. 23, 79–82. doi: 10.5005/jp-journals-10024-3245
van Winkelhoff, A. J. (2012). Antibiotics in the treatment of peri-implantitis. Eur. J. Oral. Implantol. 5, S43–S50.
Veloo, A. C., Seme, K., Raangs, E., Rurenga, P., Singadji, Z., Wekema-Mulder, G., et al. (2012). Antibiotic susceptibility profiles of oral pathogens. Int. J. Antimicrob. Agents. 40, 450–454. doi: 10.1016/j.ijantimicag.2012.07.004
Zhang, H., Yuan, Y., Xue, H., Yu, R., Huang, H. (2022). MicroRNA sequence and function analysis in peri-implantitis and periodontitis: an animal study. J. Periodontal Res. 57, 1043–1055. doi: 10.1111/jre.13045
Keywords: dental implants, peri-implantitis, antibacterial agents/therapeutic use, metronidazole, RCTs, meta-analysis
Citation: López-Valverde N, López-Valverde A and Blanco-Rueda JA (2023) Efficacy of adjuvant metronidazole therapy on peri-implantitis: a systematic review and meta-analysis of randomized clinical studies. Front. Cell. Infect. Microbiol. 13:1149055. doi: 10.3389/fcimb.2023.1149055
Received: 20 January 2023; Accepted: 02 May 2023;
Published: 23 May 2023.
Edited by:
Krisztina M. Papp-Wallace, JMI Laboratories, United StatesReviewed by:
Costanza Soldini, International University of Catalonia, SpainProfessor Douglas Deporter, University of Toronto, Canada
Copyright © 2023 López-Valverde, López-Valverde and Blanco-Rueda. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Antonio López-Valverde, YWxvcGV6dmFsdmVyZGVAdXNhbC5lcw==