
95% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cell. Infect. Microbiol. , 16 February 2023
Sec. Clinical Microbiology
Volume 13 - 2023 | https://doi.org/10.3389/fcimb.2023.1137067
This article is part of the Research Topic Alternative non-pharmacological treatments based on stem cell towards the infection of pathogens and its sequelas. View all 5 articles
 Bing-Yan Wang1*
Bing-Yan Wang1* Aize Cao2
Aize Cao2 Meng-Hsuan Ho3
Meng-Hsuan Ho3 Derek Wilus4
Derek Wilus4 Sally Sheng1Hsiu-Wan Meng1Elissa Guerra1Jianming Hong1
Sally Sheng1Hsiu-Wan Meng1Elissa Guerra1Jianming Hong1 Hua Xie3*
Hua Xie3*The present study aimed at identifying risk factors associated with periodontitis development and periodontal health disparities with emphasis on differential oral microbiota. The prevalence of periodontitis is recently rising dentate adults in the US, which presents a challenge to oral health and overall health. The risk of developing periodontitis is higher in African Americans (AAs), and Hispanic Americans (HAs) than in Caucasian Americans (CAs). To identify potentially microbiological determinations of periodontal health disparities, we examined the distribution of several potentially beneficial and pathogenic bacteria in the oral cavities of AA, CA, and HA study participants. Dental plaque samples from 340 individuals with intact periodontium were collected prior to any dental treatment, and levels of some key oral bacteria were quantitated using qPCR, and the medical and dental histories of participants were obtained retrospectively from axiUm. Data were analyzed statistically using SAS 9.4, IBM SPSS version 28, and R/RStudio version 4.1.2. Amongst racial/ethnic groups: 1) neighborhood medium incomes were significantly higher in the CA participants than the AA and the HA participants; 2) levels of bleeding on probing (BOP) were higher in the AAs than in the CAs and HAs; 3) Porphyromonas gingivalis levels were higher in the HAs compared to that in the CAs; 4) most P. gingivalis detected in the AAs were the fimA genotype II strain that was significantly associated with higher BOP indexes along with the fimA type IV strain. Our results suggest that socioeconomic disadvantages, higher level of P. gingivalis, and specific types of P. gingivalis fimbriae, particularly type II FimA, contribute to risks for development of periodontitis and periodontal health disparities.
Periodontitis is one of the most widespread infectious diseases among adults, with an estimated 46% of dentate adults aged 30 years and older in the US suffering from some forms of the disease (Eke et al., 2015). Based on the data from the National Health and Nutrition Examination Surveys I, II, and III, periodontitis disproportionately affects different racial and ethnic groups. African Americans (AAs) and Hispanic Americans (HAs) experience higher incidences of periodontitis than Caucasian Americans (CAs) even after adjustment for all co-factors (Borrell et al., 2002; Thornton-Evans et al., 2013; Eke et al., 2020). Longitudinal studies on the natural history of periodontitis suggest that modifiable and non-modifiable risk factors potentially influence the onset, clinical presentation, and progression of the disease (Loe et al., 1978; Okamoto et al., 1988; Michalowicz et al., 1991; Grossi et al., 1994; Kornman et al., 1997; Borrell et al., 2004; Borrell and Talih, 2012; Genco and Borgnakke, 2013; Thornton-Evans et al., 2013). Smoking, age, and gender, as well as genetic and socioeconomic factors are well-known risk factors for periodontitis (Stashenko et al., 2011; Borrell and Crawford, 2012; Ioannidou, 2017; Naorungroj et al., 2017; Sutton et al., 2017). Additionally, the oral microbiome is a necessary, although insufficient, etiologic factor of periodontitis (Socransky and Haffajee, 2000; Jenkinson and Lamont, 2005). Porphyromonas gingivalis, one of the putative periodontal pathogens, has been well studied. P. gingivalis in the oral cavity, even in low abundance, can disrupt host-microbial homeostasis and elevate the virulence potential of oral microbial communities (Hajishengallis et al., 2011; Hajishengallis et al., 2012).
We previously reported an antagonistic relationship between P. gingivalis and Streptococcus cristatus (Wang et al., 2009). We found that S. cristatus can repress FimA expression in several P. gingivalis strains, including strains of fimA types I, II, and III (Xie et al., 2000; Xie et al., 2007; Wang et al., 2009). S. cristatus surface protein, arginine deiminase (ArcA), was identified as the signaling molecule to which P. gingivalis responds by repressing the expression of the fimA gene and consequently reducing production of fimbrial adhesin, FimA (Xie et al., 2007; Wu and Xie, 2010). We also discovered the expression of the arcA gene to be significantly higher in S. cristatus than in Streptococcus gordonii, suggesting that these two streptococcal species play distinct roles in the highly orchestrated dental plaque (Lin et al., 2008). Recently, we reported that the ratio of S. cristatus to P. gingivalis was significantly higher in CAs than in HAs and AAs with periodontitis (Wang et al., 2021). Based on these observations, we speculate that the interaction of specific bacteria may play an important role in periodontal health disparities. In the present work, we focused on levels of keystone pathogens and accessory bacteria and investigated a potential link between microbial compositions, particularly the prevalence of P. gingivalis and S. cristatus, and risks of periodontitis in AAs, CAs, and HAs with intact periodontium. Our results suggest that differences in the compositions of oral microbial communities may influence susceptibility to periodontitis.
The research protocol was approved by the Committee for the Protection of Human Subjects of the University of Texas Health Science Center at Houston (IRB number: HSC-DB-17-0636). Candidates were screened during routine dental visits at the clinic of the School of Dentistry, University of Texas Health Science Center at Houston between 2017 and 2022. Individuals aged 21-75 years with self-reported ethnicity/race of AAs, CAs, or HAs were enrolled after the initial periodontal examination that included determination of plaque index (PI), bleeding on probing (BOP) level, probing depth, and clinical attachment level on all teeth (Newman et al., 2018). Radiographs were taken during this screening phase to assess bone loss. The clinical oral examinations were performed by trained dental examiners who are faculty members of the School of Dentistry, University of Texas Health Science Center at Houston. The examiners are calibrated annually in the diagnosis of periodontitis. Based on the 2017 World Workshop classification (I.L. et al., 2018; Trombelli et al., 2018), all study participants diagnosed as periodontal health on an intact periodontium or biofilm-induced gingivitis on an intact periodontium met the following criteria: >24 teeth; no alveolar bone loss or clinical attachment loss; pocket depth ≤3mm (excluding pseudo pocket); no antibiotic therapy in the previous six months; and not pregnant. Information on demographics and self-reported dental and medical histories of the participants were abstracted from the Electronic Health Record. The socioeconomic statuses of these participants were determined by obtaining median incomes based on residential zip codes (https://www.incomebyzipcode.com/).
Dental plaque samples were collected by board-certified periodontists using sterile paper points at baseline prior to any dental treatment and labeled in numbers according to sampling sequences. The paper points were placed in the mesiobuccal sulci of the first molar in each quadrant for 1 minute and then immersed immediately in an Eppendorf tube containing 0.5 ml of Tris-EDTA (TE) buffer (pH 7.5) (Wang et al., 2009). Oral bacteria were harvested by centrifugation, and the bacterial pellet was resuspended in 100 µl TE buffer. Bacterial chromosomal DNA was released by two cycles of freezing at -80°C overnight and boiling for 10 minutes.
Oral bacteria including P. gingivalis and S. cristatus, were enumerated by qPCR, using the SYBR Green PCR mix (Bio-Red Laboratories Inc., Redmond, WA, USA) with species-specific primers listed in Table 1. P. gingivalis strains with different fimA genotypes were determined by PCR with strain-specific primers (Zheng et al., 2011). The level of total bacteria was determined using primers corresponding to the conserved sequences of cyanobacterial small subunit rRNA genes (Turner et al., 1999) (Table 1). Bacterial standard curves used to calculate the number of bacterial cells were prepared by quantifying known amounts of genomic DNA from each bacterial species using qPCR (Wang et al., 2009). Briefly, bacteria were grown in standard media, and optical density of bacteria was determined and adjusted to OD600=1.0 (containing approximately 109 bacteria in one mL). After serials dilution, qPCR was conducted and corresponded to an OD. Bacterial ratios were obtained using numerical levels of two bacteria from the same sample. Bacterial quantitation by qPCR was performed by a designated technician without any knowledge of subject information. Clinical data abstraction and analysis were performed by different designated faculty members.
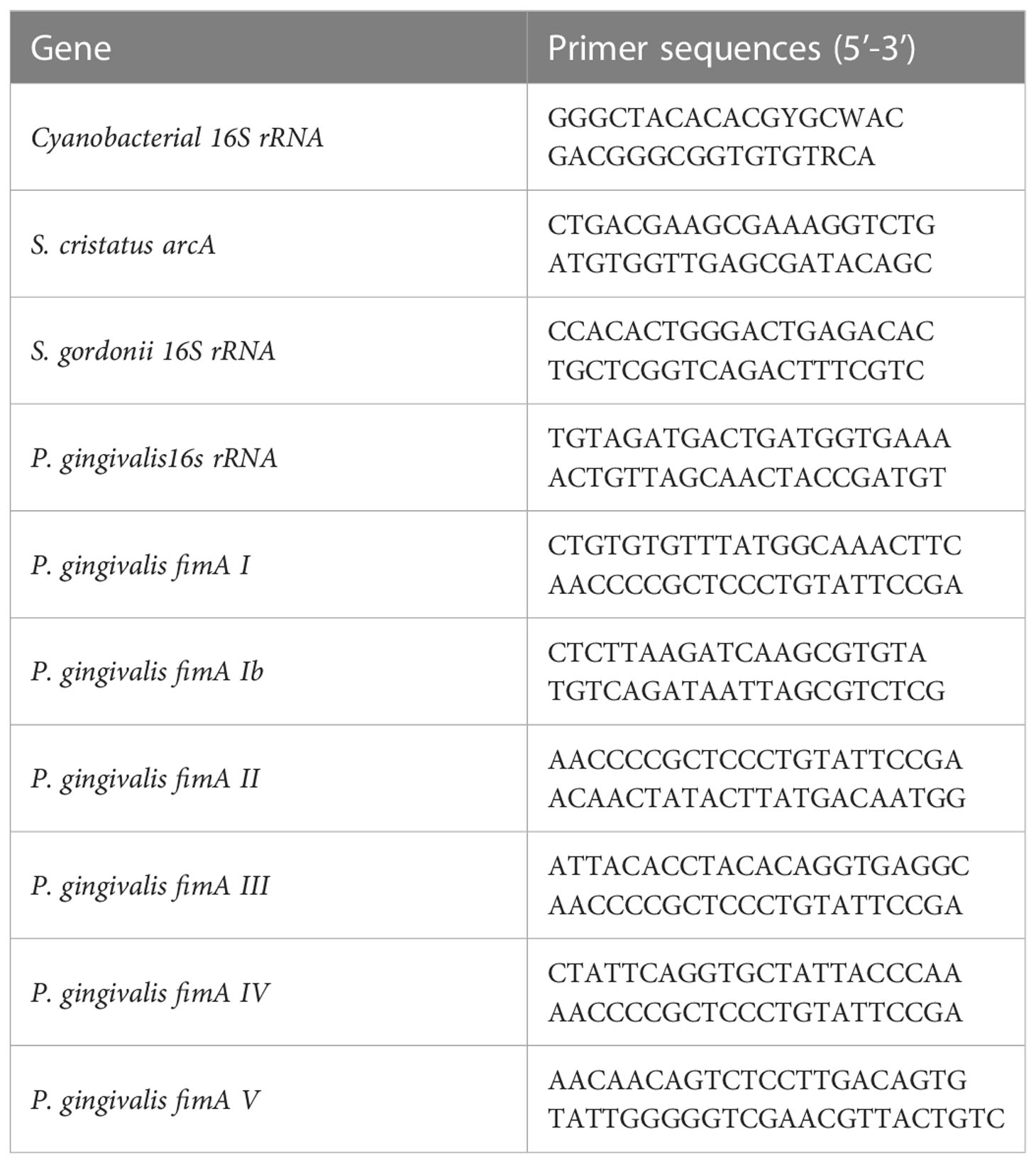
Table 1 Primers used in this study.
Statistical analysis was performed for each group. Continuous variables were assessed for normality and log10-transformed as needed. Two-sided statistical tests were performed using a 5% significance level. Comparison of demographics, dental and medical histories, and oral microbial profiles among AAs, CAs, and HAs of different ages was performed using one-way analysis of means (ANOVA) for continuous variables and the chi-square test or Fisher’s exact test for categorical variables. Ordinal logistic regression was used to measure the association between race/ethnicity and levels of P. gingivalis with adjustment for age. The SAS software (version 9.4; SAS Institute, Cary, NC), IBM SPSS (version 28) and R/RStudio version 4.1.2 were used to conduct all statistical analyses.
Three hundred and forty individuals with intact periodontium were enrolled, including 104 AAs, 115 CAs, and 121 HAs. No significant difference was found among these racial and ethnic groups with regards to age, gender, and total number of teeth. To investigate whether social inequalities exist among these groups, neighborhood median incomes based on the participates’ zip codes were obtained. As presented in Table 2, the neighborhood median income of the CA group was significantly higher ($72,000) than those of the AA and HA groups ($59,000 and $54,000, respectively) (P<0.001).
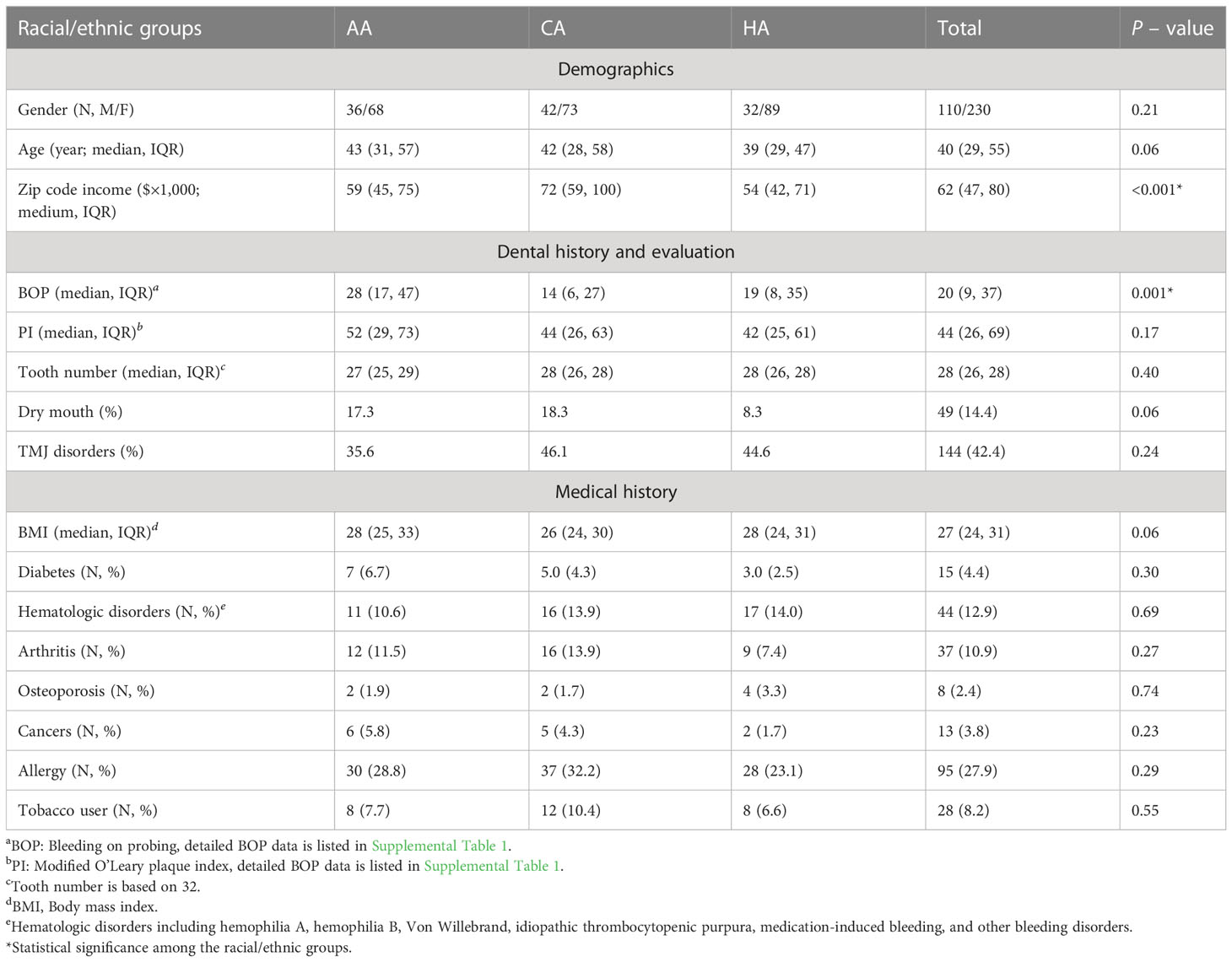
Table 2 Characteristics of the study cohort.
Significant difference BOP levels were found among the racial/ethnic groups of the study participants. The highest degree of BOP was observed in the AA group with an interquartile range (IQR) of 28, followed by that in the HA group (IQR of 19) and in the CA group (IQR of 14) (p < 0.001) (Table 2). The severities of BOP levels in these groups were further investigated. We found 39.1% of the CAs to have BOP level lower than 10% compared to 33.1% of HAs and 14.4% of the AAs (P-value <0.001) (Table 3). While, BOP levels greater than 30% was found in 48.1% of the AAs, 30.6% of the HAs, and only 20.9 of the CAs, indicating that levels of periodontal inflammation were more severe in the AA and HA participants. However, no significant differences were present in PI and incidences of some well-known risks of periodontitis including diabetes and tobacco use among the AAs, CAs, and HAs of this periodontal healthy cohort.
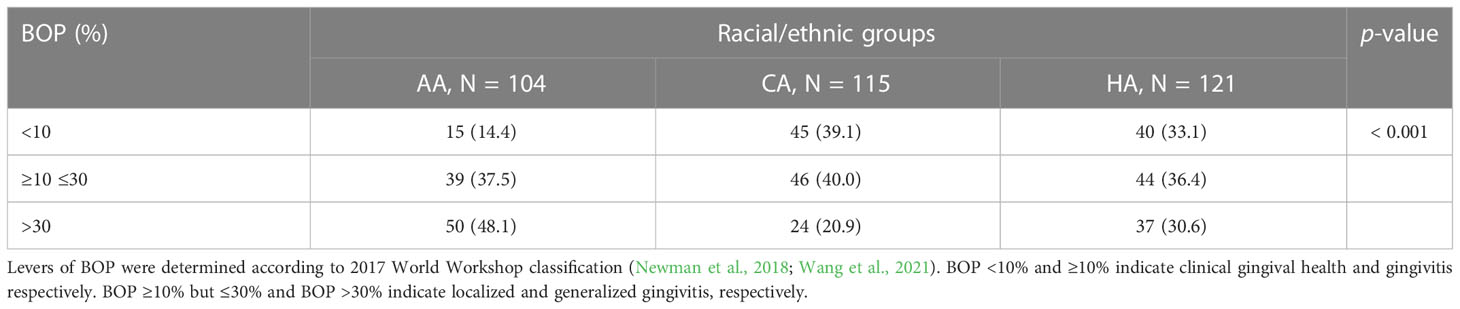
Table 3 Levels of BOP in different racial/ethnic groups.
Levels of P. gingivalis and S. cristatus in the dental plaque samples were determined using qPCR with specific primers. P. gingivalis was detected in 23.5% of all participants (80/340). Detection rates of P. gingivalis were in 21.2% of the AAs, 18.2% of the CAs, and 30.6% of the HAs (Table 4), respectively; however, statistical significance was not reached. In addition, higher prevalence of P. gingivalis was found among younger participants (aged 21-35 years) of the AA (7.7%) and the HA (9.9%) groups than that in the CA group (4.3%), suggesting that AAs and HAs may be at risk for developing periodontitis at a younger age. Moreover, 68.2% of P. gingivalis-positive AA subjects (15/22) had greater than 10,000 P. gingivalis cells in their dental plaque samples, while 48.7% of P. gingivalis-positive HA subjects (18/37) had greater than 10,000 P. gingivalis cells in their plaque samples. In contrast, only 33% of P. gingivalis-positive CAs (7/21) had greater than 10,000 P. gingivalis cells in their plaque samples. The higher prevalence of P. gingivalis among younger participants (<35 years old) and higher levels of P. gingivalis in dental plaque samples from the AA and HA participants suggest a likelihood periodontal health disparity (Table 4). We further analyzed P. gingivalis levels across the racial/ethnic groups using an ordinal regression, with P. gingivalis level as a categorical outcome variable and age as a predictor. Compared to the CA participants, the HA participants had a significantly higher level of P. gingivalis, after adjusting for age (P-value = 0.019) with an adjusted odds ratio (AOR) of 2.413, indicating that HAs have a higher chance to carry a relatively more P. gingivalis. The AAs also exhibited higher levels of P. gingivalis compared to the CAs after adjusting for age [AOR = 1.812), though the difference was not statistically significant.
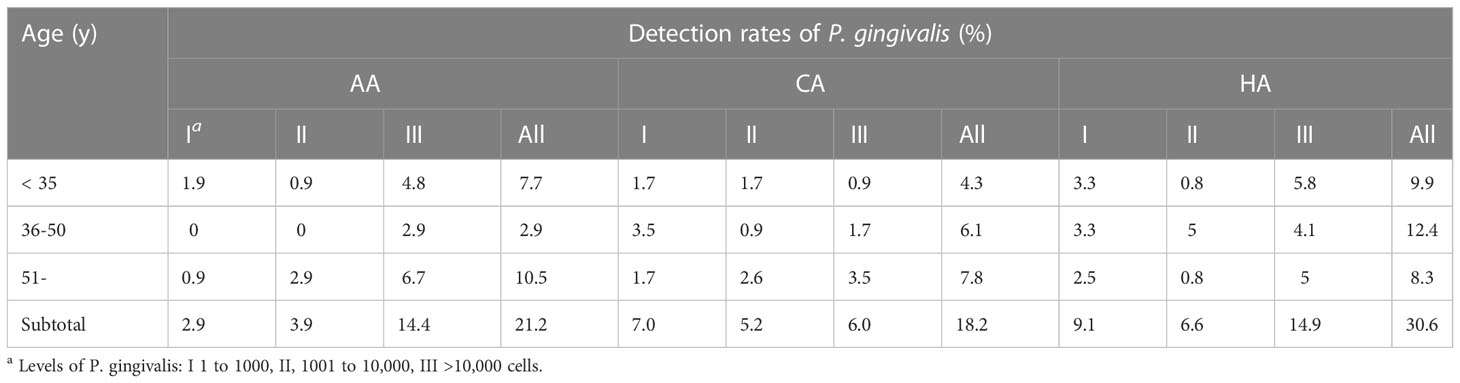
Table 4 Prevalence of P. gingivalis in participants of different ages and racial/ethnic groups.
As P. gingivalis is classified into six fimA genotypes (types I and Ib to V) based on their nucleotide sequences of the fimA gene, the fimA genotype in each dental plaque sample was examined. The Detection rates of genotypes I, Ib, II, III, IV, and V were 5.6%, 3.8%, 5.0%, 4.4%, 2.6% and 2.1%, respectively. As shown in Table 5, no significant difference in the distribution of types I, Ib, III, IV, and V among the groups was detected. However, a significantly higher detection rate (50%) of type II in the AA group than in the CA (9.5%) and HA groups (10.8%) (P=0.009) was observed.
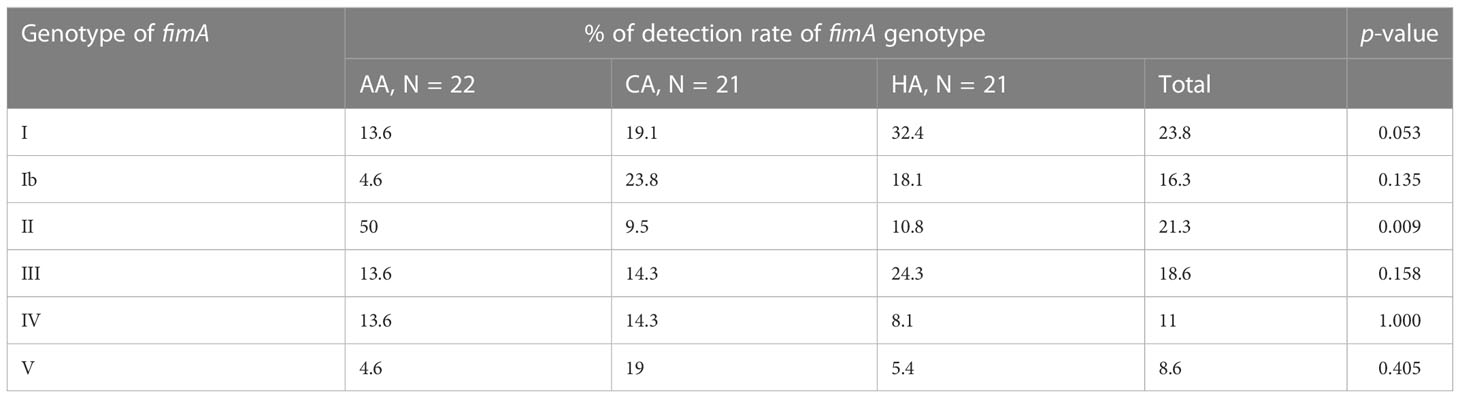
Table 5 Distribution of P. gingivalis fimA genotypes among different racial/ethnic groups.
To test whether the presence of P. gingivalis impacts the abundance of microbial communities, we quantitated bacterial levels in the dental plaque samples using qPCR with specific primers of cyanobacterial 16S rRNA. We found that 61.9 % of P. gingivalis-negative participants had fewer than 108 total bacterial cells, whereas only 41.2% of P. gingivalis-positive participants had fewer than 108 bacterial cells (Table 6). In other words, significantly more P. gingivalis-positive subjects had greater than 108 total bacterial cells in their dental plaque samples (58.8%) than P. gingivalis-negative participants (P = 0.001). Association of FimA types with BOP and total bacterial levels was examined using ANOVA, which demonstrated that participants carrying fimA genotypes II or IV strain had higher BOP levels, followed by those with genotype I strain. Conversely, individuals carrying the fimA genotypes types Ib, III, and V strains exhibited significantly lower BOP levels (P=0.028) (Table 7). However, no significant association between BOP levels and total bacterial levels was observed. These results suggest an association between FimA types II and IV with periodontal inflammation and health disparity.

Table 6 Impact of P. gingivalis on bacterial biofilm formation.
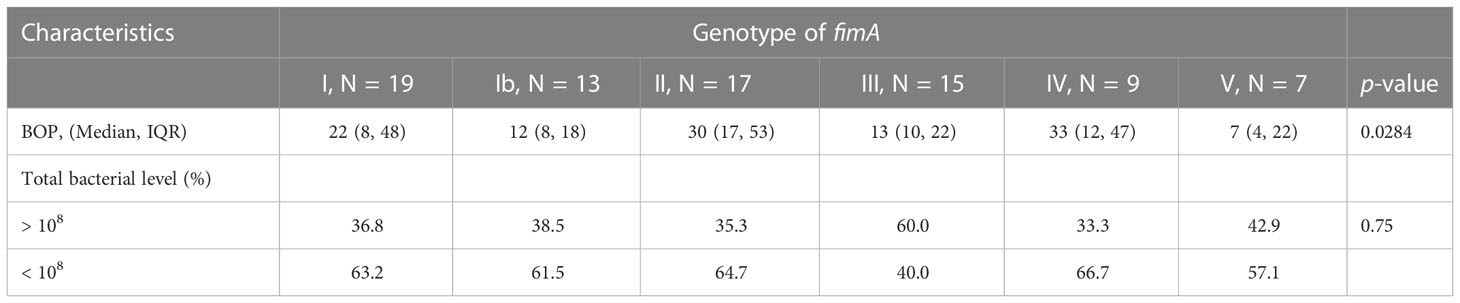
Table 7 Correlation between the fimA genotypes and BOP levels or total bacteria numbers.
Based on our previous observation that S. cristatus can inhibit the formation of P. gingivalis biofilm (Xie et al., 2000), we anticipated that a higher ratio of S. cristatus and P. gingivalis links to lower the risk for periodontitis development. The ratio of S. cristatus to P. gingivalis among the racial/ethnic groups was sequentially examined and compared. As shown in Table 8, only 40.9% of P. gingivalis-positive participants in the AA group had a ratio of higher than 100. On the other hand, 66.7% and 45.9% of P. gingivalis-positive participants in the CA and HA groups, respectively, had a ratio of higher than 100. Only 33.3% of P. gingivalis-positive participants in the CA group had a ratio of lower than 100, compared to 59.1% in the AA and 54.1% in HA groups. Although the percentage differences were not significantly different among the groups (P=0.17), it was clear that more participants in the AA group had the lower S. cristatus:P. gingivalis ratio and fared the worst in periodontal health. We are currently investigating a larger cohort of study participants in order to obtain statistically significant results.

Table 8 Correlation between P. gingivalis and S. cristatus in P. gingivalis-positive participants.
To assess the potential risk factors for periodontitis development, we performed a comprehensive study to analyze the demographics, oral microbiological profiles, and clinical features of study subjects from different racial/ethnic backgrounds, all with an intact periodontium. Several factors that may contribute to periodontal health disparities were identified. Current models for the pathogenesis of periodontitis recognize P. gingivalis as a keystone pathogen that elevates the virulence of the entire microbial community (Hajishengallis et al., 2011; Darveau et al., 2012; Hajishengallis et al., 2012; Hajishengallis and Lamont, 2014). One key finding in this study is the differential detection rates of P. gingivalis among the AA, CA, and HA groups. P. gingivalis was detected in 23.5% of all participants; this percentage is similar to a previously reported rate of 25% (Griffen et al., 1998). However, the detection rate of P. gingivalis to be the highest in the HA group, when participants in specific groups were examined. Moreover, the detection rate of P. gingivalis in younger participants (aged 21–35 years) was higher in the AA and HA groups than in the CA group. More participants in the AA and HA groups exhibited higher levels of P. gingivalis in their dental plaques compared to the CA group. Our results suggest that the relatively high levels of P. gingivalis detected at younger ages may contribute to a higher risk for periodontitis in AA and HA populations. Our observations are in accordance with a previous analysis of 16S rRNA genes using deep sequencing that showed a higher abundance of Bacteroidetes and higher prevalence of P. gingivalis in AA than in CA subjects (Yang et al., 2019).
In the light of detection of P. gingivalis in dental plaques from both periodontitis patients and periodontally healthy subjects, it was suggested that different subsets of P. gingivalis strains exist in diseased and healthy periodontal sites (Griffen et al., 1998). An increasing body of evidence reveals that P. gingivalis strains with types II and IV FimA are often associated with periodontitis (Amano et al., 2000; van der Ploeg et al., 2004; Miura et al., 2005; Wang et al., 2020), while strains with type I fimA are associated with healthy periodontal tissues (Amano et al., 2000). In this study, the distribution of P. gingivalis fimA genotypes in the different racial/ethnic groups was compared. We found that the majority of P. gingivalis-positive individuals in the AA group carry the strain with type II fimA, which was significantly higher than that in the CA and HA groups. In addition, the type II and IV strains appeared to be associated with higher levels of BOP. These findings could explain a higher prevalence of periodontitis in the AA population (Amano et al., 1999; van der Ploeg et al., 2004; Miura et al., 2005; Wang et al., 2020). It is possible that P. gingivalis strains with fimA types II and IV in periodontally healthy subjects more likely break up a balanced host immune and induce uncontrolled inflammation in the periodontium (Yang et al., 2004).
We previously identified a negative correlation between P. gingivalis and S. cristatus in dental plaque samples from periodontitis patients (Wang et al., 2009). In the present study, higher ratios of S. cristatus to P. gingivalis in P. gingivalis-positive subjects in the CA group than those in the AA and HA groups with intact periodontium were also observed. It is reasonable to speculate that higher ratios of S. cristatus to P. gingivalis can keep P. gingivalis in check and inhibit the ability of the latter to elevate the virulence of the oral microbiota. In other words, the lower ratios found in the AA and the HA groups may render these individuals more susceptible to periodontitis.
It is well known that diabetes is a major risk factor for periodontitis (Preshaw et al., 2012). According to the CDC (https://www.cdc.gov), the incidence of new diabetes cases is higher among non-Hispanic AAs and people of Hispanic origin than among non-Hispanic Asians and non-Hispanic CAs. We did not observe an uneven distribution of diabetes cases among the different racial/ethnic groups in our study cohort of 340 participants. Smoking is another significant risk factor for periodontal disease development and progression (Zhang et al., 2019). According to the American Lung Association (https://www.lung.org/quit-smoking/smoking-facts/impact-of-tobacco-use/tobacco-use-racial-and-ethnic), adult smoking rates are 16.8% in AAs, 16.6% in CAs, and 10.1% in HAs, which are higher than what we observed in our cohort (9.2% in the AAs, 10.8% in the CAs, and 6.7% in the HAs). Although the smoking rate in the HA group appeared to be lower than that in the AA group and the CA group, the differences in percentages were not statistically significant. One plausible reason is that our sample size was not large enough to detect significant differences in diabetes incidence and smoking rate. In addition, participants in this study were recruited at dental clinic in an academic setting; hence, the cohort may not be representative of the general population. Future studies on larger and more representative patient cohorts are warranted. Moreover, our observation of zip code incomes agrees with a previously reported likelihood of an association between neighborhood socioeconomic circumstances and periodontitis (Borrell et al., 2006). However, further studies are needed to examine how neighborhood socioeconomic conditions impact the development of periodontitis and periodontal health disparities.
In this study, we collected dental plaque samples only once from the participants diagnosed as periodontal health or biofilm-induced gingivitis on an intact periodontium (without periodontitis) during their initial periodontal examination. The participants were not followed after the sample collection. Therefore, this study only provides preliminary information about the possible factors associated with periodontal health and further studies are needed in the future to discern their precise role in periodontitis development. Additionally, the present study was limited on P. gingivalis and several key oral bacteria. Whole bacterial profiles of the samples are under investigated using metagenome shotgun sequencing in our lab, which should provide clearer pictures on core microbiota associated with periodontal health disparities.
In conclusion, this work highlights the importance of differential oral microbiota in periodontal health disparities. Several risk factors may be linked to periodontal health disparities, including the presence of P. gingivalis at higher levels and at younger ages, the prevalence of specific subsets of P. gingivalis strains, and lower ratios of S. cristatus/P. gingivalis.
The original contributions presented in the study are included in the article/Supplementary Material. Further inquiries can be directed to the corresponding authors.
The studies involving human participants were reviewed and approved by the Committee for the Protection of Human Subjects of the University of Texas Health Science Center at Houston. The patients/participants provided their written informed consent to participate in this study.
HX and B-YW conceived the study and supervised the project. AC and DW performed and verified the statistical analyses. B-YW, SS, and H-WM enrolled study participants. EG, JH, and B-YW collected medical and dental history data. M-HH and JH helped sample process. All authors contributed to the article and approved the submitted version.
The study was supported in part by grant MD007586 from the National Institute on Minority Health and Health Disparities, United States of America.
The authors are grateful to all study participants for their contribution to this research. The authors thank Krishna Kookal for abstracting clinical parameters from the Electronic Health Record at the School of Dentistry, University of Texas Health Science Center at Houston. The authors also thank the Biostatistics Core at Meharry Medical College for help with data analysis and the Meharry Office of Scientific Editing and Publications for editorial assistance.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
The Supplementary Material for this article can be found online at: https://www.frontiersin.org/articles/10.3389/fcimb.2023.1137067/full#supplementary-material
Supplementary Table 1 | Individual clinical data of the cohort.
Amano, A., Kuboniwa, M., Nakagawa, I., Akiyama, S., Morisaki, I., Hamada, S. (2000). Prevalence of specific genotypes of porphyromonas gingivalis fimA and periodontal health status. J. Dental Res. 79, 1664–1668. doi: 10.1177/00220345000790090501
Amano, A., Nakagawa, I., Kataoka, K., Morisaki, I., Hamada, S. (1999). Distribution of porphyromonas gingivalis strains with fimA genotypes in periodontitis patients. J. Clin. Microbiol. 37, 1426–1430. doi: 10.1128/JCM.37.5.1426-1430.1999
Borrell, L. N., Burt, B. A., Gillespie, B. W., Lynch, J., Neighbors, H. (2002). Periodontitis in the United States: Beyond black and white. J. Public Health Dent. 62, 92–101. doi: 10.1111/j.1752-7325.2002.tb03428.x
Borrell, L. N., Burt, B. A., Neighbors, H. W., Taylor, G. W. (2004). Social factors and periodontitis in an older population. Am. J. Public Health 94, 748–754. doi: 10.2105/AJPH.94.5.748
Borrell, L. N., Burt, B. A., Warren, R. C., Neighbors, H. W. (2006). The role of individual and neighborhood social factors on periodontitis: The third national health and nutrition examination survey. J. periodontol. 77, 444–453. doi: 10.1902/jop.2006.050158
Borrell, L. N., Crawford, N. D. (2012). Socioeconomic position indicators and periodontitis: Examining the evidence. Periodontology 2000 58, 69–83. doi: 10.1111/j.1600-0757.2011.00416.x
Borrell, L. N., Talih, M. (2012). Examining periodontal disease disparities among U.S. adults 20 years of age and older: NHANES III (1988-1994) and NHANES 1999-2004. Public Health Rep. 127, 497–506. doi: 10.1177/003335491212700505
Darveau, R. P., Hajishengallis, G., Curtis, M. A. (2012). Porphyromonas gingivalis as a potential community activist for disease. J. Dental Res. 91, 816–820. doi: 10.1177/0022034512453589
Eke, P. I., Borgnakke, W. S., Genco, R. J. (2020). Recent epidemiologic trends in periodontitis in the USA. Periodontology 2000 82, 257–267. doi: 10.1111/prd.12323
Eke, P. I., Dye, B. A., Wei, L., Slade, G. D., Thornton-Evans, G. O., Borgnakke, W. S., et al. (2015). Update on prevalence of periodontitis in adults in the United States: NHANES 2009 to 2012. J. periodontol. 86, 611–622. doi: 10.1902/jop.2015.140520
Genco, R. J., Borgnakke, W. S. (2013). Risk factors for periodontal disease. Periodontology 2000 62, 59–94. doi: 10.1111/j.1600-0757.2012.00457.x
Griffen, A. L., Becker, M. R., Lyons, S. R., Moeschberger, M. L., Leys, E. J. (1998). Prevalence of porphyromonas gingivalis and periodontal health status. J. Clin. Microbiol. 36, 3239–3242. doi: 10.1128/JCM.36.11.3239-3242.1998
Grossi, S. G., Zambon, J. J., Ho, A. W., Koch, G., Dunford, R. G., Machtei, E. E., et al. (1994). Assessment of risk for periodontal disease. i. risk indicators for attachment loss. J. periodontol. 65, 260–267. doi: 10.1902/jop.1994.65.3.260
Hajishengallis, G., Darveau, R. P., Curtis, M. A. (2012). The keystone-pathogen hypothesis. Nat. Rev. Microbiol. 10, 717–725. doi: 10.1038/nrmicro2873
Hajishengallis, G., Lamont, R. J. (2014). Breaking bad: Manipulation of the host response by porphyromonas gingivalis. Eur. J. Immunol. 44, 328–338. doi: 10.1002/eji.201344202
Hajishengallis, G., Liang, S., Payne, M. A., Hashim, A., Jotwani, R., Eskan, M. A., et al. (2011). Low-abundance biofilm species orchestrates inflammatory periodontal disease through the commensal microbiota and complement. Cell Host Microbe 10, 497–506. doi: 10.1016/j.chom.2011.10.006
I.L., C., Chapple, B. L., Mealey, T. E., Van Dyke, P. M., Bartold, H., Dommisch, P., et al. (2018). Periodontal health and gingival diseases and conditions on an intact and a reduced periodontium: Consensus report of workgroup 1 of the 2017 world workshop on the classification of periodontal and peri-implant diseases and conditions. J. Clin. periodontol. 45 Suppl 20, S68–S77.
Ioannidou, E. (2017). The sex and gender intersection in chronic periodontitis. Front. Public Health 5, 189. doi: 10.3389/fpubh.2017.00189
Jenkinson, H. F., Lamont, R. J. (2005). Oral microbial communities in sickness and in health. Trends Microbiol. 13, 589–595. doi: 10.1016/j.tim.2005.09.006
Kornman, K. S., Crane, A., Wang, H. Y., di Giovine, F. S., Newman, M. G., Pirk, F. W., et al. (1997). The interleukin-1 genotype as a severity factor in adult periodontal disease. J. Clin. periodontol. 24, 72–77. doi: 10.1111/j.1600-051X.1997.tb01187.x
Lin, X., Lamont, R. J., Wu, J., Xie, H. (2008). Role of differential expression of streptococcal arginine deiminase in inhibition of fimA expression in porphyromonas gingivalis. J. bacteriol. 190, 4367–4371. doi: 10.1128/JB.01898-07
Loe, H., Anerud, A., Boysen, H., Smith, M. (1978). The natural history of periodontal disease in man. the rate of periodontal destruction before 40 years of age. J. periodontol. 49, 607–620. doi: 10.1902/jop.1978.49.12.607
Michalowicz, B. S., Aeppli, D., Virag, J. G., Klump, D. G., Hinrichs, J. E., Segal, N. L., et al. (1991). Periodontal findings in adult twins. J. periodontol. 62, 293–299. doi: 10.1902/jop.1991.62.5.293
Miura, M., Hamachi, T., Fujise, O., Maeda, K. (2005). The prevalence and pathogenic differences of porphyromonas gingivalis fimA genotypes in patients with aggressive periodontitis. J. periodontal Res. 40, 147–152. doi: 10.1111/j.1600-0765.2005.00779.x
Naorungroj, S., Slade, G. D., Divaris, K., Heiss, G., Offenbacher, S., Beck, J. D. (2017). Racial differences in periodontal disease and 10-year self-reported tooth loss among late middle-aged and older adults: the dental ARIC study. J. Public Health dentistry 77, 372–382. doi: 10.1111/jphd.12226
Newman, M., Takei, H., Klokkevold, H., Carranza, F. (2018). Newman And carranza's clinical periodontology.
Okamoto, H., Yoneyama, T., Lindhe, J., Haffajee, A., Socransky, S. (1988). Methods of evaluating periodontal disease data in epidemiological research. J. Clin. periodontol. 15, 430–439. doi: 10.1111/j.1600-051X.1988.tb01597.x
Preshaw, P. M., Alba, A. L., Herrera, D., Jepsen, S., Konstantinidis, A., Makrilakis, K., et al. (2012). Periodontitis and diabetes: A two-way relationship. Diabetologia 55, 21–31. doi: 10.1007/s00125-011-2342-y
Socransky, S. S., Haffajee, A. D. (2000). Periodontal microbial ecology. Periodontology 38 (2005), 135–187.
Stashenko, P., Van Dyke, T., Tully, P., Kent, R., Sonis, S., Tanner, A. C. (2011). Inflammation and genetic risk indicators for early periodontitis in adults. J. periodontol. 82, 588–596. doi: 10.1902/jop.2010.100443
Sutton, J. D., Salas Martinez, M. L., Gerkovich, M. M. (2017). Environmental tobacco smoke and periodontitis in united states non-smokers, 2009 to 2012. J. periodontol. 88, 565–574. doi: 10.1902/jop.2017.160725
Thornton-Evans, G., Eke, P., Wei, L., Palmer, A., Moeti, R., Hutchins, S., et al. (2013). And prevention, periodontitis among adults aged >/=30 years - united states, 2009-2010. Morbidity mortal. weekly Rep. Surveill. summaries 62 Suppl 3, 129–135.
Trombelli, L., Farina, R., Silva, C. O., Tatakis, D. N. (2018). Plaque-induced gingivitis: Case definition and diagnostic considerations. J. Clin. periodontol. 45 Suppl 20, S44–S67.
Turner, S., Pryer, K. M., Miao, V. P., Palmer, J. D. (1999). Investigating deep phylogenetic relationships among cyanobacteria and plastids by small subunit rRNA sequence analysis. J. Eukaryot. Microbiol. 46, 327–338. doi: 10.1111/j.1550-7408.1999.tb04612.x
van der Ploeg, J. R., Giertsen, E., Ludin, B., Morgeli, C., Zinkernagel, A. S., Gmur, R. (2004). Quantitative detection of porphyromonas gingivalis fimA genotypes in dental plaque. FEMS Microbiol. Lett. 232, 31–37. doi: 10.1016/S0378-1097(04)00064-3
Wang, B. Y., Lu, T., Cai, Q., Ho, M. H., Sheng, S., Meng, H. W., et al. (2021). Potential microbiological risk factors associated with periodontitis and periodontal health disparities. Front. Cell. infect. Microbiol. 11, 789919. doi: 10.3389/fcimb.2021.789919
Wang, B. Y., Wu, J., Lamont, R. J., Lin, X., Xie, H. (2009). Negative correlation of distributions of streptococcus cristatus and porphyromonas gingivalis in subgingival plaque. J. Clin. Microbiol. 47, 3902–3906. doi: 10.1128/JCM.00072-09
Wang, H., Zhang, W., Wang, W., Zhang, L. (2020). The prevalence of fimA genotypes of porphyromonas gingivalis in patients with chronic periodontitis: A meta-analysis. PloS One 15, e0240251. doi: 10.1371/journal.pone.0240251
Wu, J., Xie, H. (2010). Role of arginine deiminase of streptococcus cristatus in porphyromonas gingivalis colonization. Antimicrob. Agents chemother. 54, 4694–4698. doi: 10.1128/AAC.00284-10
Xie, H., Cook, G. S., Costerton, J. W., Bruce, G., Rose, T. M., Lamont, R. J. (2000). Intergeneric communication in dental plaque biofilms. J. bacteriol. 182, 7067–7069. doi: 10.1128/JB.182.24.7067-7069.2000
Xie, H., Lin, X., Wang, B. Y., Wu, J., Lamont, R. J. (2007). Identification of a signalling molecule involved in bacterial intergeneric communication. Microbiology 153, 3228–3234. doi: 10.1099/mic.0.2007/009050-0
Yang, H. W., Huang, Y. F., Chou, M. Y. (2004). Occurrence of porphyromonas gingivalis and tannerella forsythensis in periodontally diseased and healthy subjects. J. periodontol. 75, 1077–1083. doi: 10.1902/jop.2004.75.8.1077
Yang, Y., Zheng, W., Cai, Q., Shrubsole, M. J., Pei, Z., Brucker, R., et al. (2019). Racial differences in the oral microbiome: Data from low-income populations of African ancestry and European ancestry. mSystems 4. doi: 10.1128/mSystems.00639-19
Zhang, Y., He, J., He, B., Huang, R., Li, M. (2019). Effect of tobacco on periodontal disease and oral cancer. Tob. Induc. Dis. 17, 40. doi: 10.18332/tid/106187
Keywords: Porphyromonas gingivalis, periodontitis, health disparities, race, risk factor
Citation: Wang B-Y, Cao A, Ho M-H, Wilus D, Sheng S, Meng H-W, Guerra E, Hong J and Xie H (2023) Identification of microbiological factors associated with periodontal health disparities. Front. Cell. Infect. Microbiol. 13:1137067. doi: 10.3389/fcimb.2023.1137067
Received: 03 January 2023; Accepted: 07 February 2023;
Published: 16 February 2023.
Edited by:
Rodolfo García-Contreras, Faculty of Medicine, National Autonomous University of Mexico, MexicoReviewed by:
Sasanka Chukkapalli, Texas A&M University College Station, United StatesCopyright © 2023 Wang, Cao, Ho, Wilus, Sheng, Meng, Guerra, Hong and Xie. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Bing-Yan Wang, YmluZy15YW4ud2FuZ0B1dGgudG1jLmVkdQ==; Hua Xie, aHhpZUBtbWMuZWR1
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.