 Min Jin1,2†
Min Jin1,2† Zhixiang Gao
Zhixiang Gao Zhanli Wang
Zhanli Wang- 1School of Public Health, Baotou Medical College, Baotou, China
- 2Collaborative Innovation Center of Zoonotic Diseases and Translational Medicine, Baotou Medical College, Baotou, China
- 3School of Public Health, Inner Mongolia Medical University, Hohhot, China
- 4Inner Mongolia Key Laboratory of Disease-Related Biomarkers, The Second Affiliated Hospital, Baotou Medical College, Baotou, China
Brucellosis is a common zoonotic disease that is widely spread worldwide and poses a major threat to human health. Clinically, it often presents with non-specific symptoms such as fever, excessive sweating, malaise, myalgia, arthralgia, loss of appetite, weight loss, and enlarged liver, spleen and lymph nodes. The disease has a long and recurrent course, often accumulating in multiple systems and organs. Of these, osteoarticular involvement is the most common complication, with a prevalence of approximately 2-77%, usually manifesting as spondylitis, sacroiliac arthritis and peripheral arthritis. Hepatosplenomegaly is seen in about 50% of patients with brucellosis, and gastrointestinal disturbances such as abdominal pain, nausea, and vomiting are common. Although respiratory involvement is less common, pneumonia, pleurisy, pleural effusion, and pulmonary nodules have been reported. Besides, approximately 2-20% of cases involve infections of the male genitourinary system, mainly manifesting as unilateral epididymal-orchitis and orchitis. The most serious complication facing brucellosis is cardiovascular involvement, and although the overall mortality rate of brucellosis is about 1% and the incidence of brucellosis endocarditis is less than 2%, more than 80% of deaths are associated with endocarditis. Furthermore, brucellosis is complicated by hematologic disease, with anemia occurring in approximately 20-53% of children during the acute phase. In addition, the neurological incidence of brucellosis is about 0.5-25%, mainly manifested as meningitis. In this study, we review the multisystem complications of brucellosis with the aim of improving early diagnosis, timely treatment and prevention of long-term complications.
1 Introduction
Brucellosis is a common zoonotic disease caused by the Gram-negative, parthenogenic, intracellular parasitic Brucella, with approximately 500,000 new cases each year. The disease was discovered in 1860 by a British physician JA Marston on the Mediterranean island of Maltese, classified as an independent infectious disease, and named “Mediterranean flaccid fever” and “Maltese fever” In 1887, British army doctor David Bruce first isolated “Micrococcus Maltese” from the spleen of a soldier who died on Malta island, identifying the disease’s causative agent. Subsequently, the disease brucellosis was named in honor of Bruce (Shakir, 2021). In 1985, the World Health Organization (WHO) Expert Committee on Brucellosis classified the genus Brucella into six biological species and 19 biological subtypes (classical biotyping): B. melitensis, B. abortus, B. suis, B. ovis, B. neotomae, and B. canis (Jiao et al., 2021). The most common pathogenic species for human brucellosis is B. melitensis, while B. abortus is the weakest type (Deng et al., 2019). Brucella is an expanding genus. With advances in microbiology, genomics, molecular biology, and other technologies, several natural hosts have been identified, such as dolphins, whales, camels, bison, foxes, baboons, bats, and frogs. Interestingly, the emergence of new species has weakened the value of classical biotypes. Brucella can enter the body through direct contact, conjunctival inoculation, gastrointestinal tract, respiratory tract, and biological transmission (Whatmore and Foster, 2021).
Brucella is a group of micro-globular or short rod-shaped bacteria (0.5–0.7/0.6–1.5 μm), nonmotile, and slow-growing (Deng et al., 2019). Without classical virulence factors, such as flagella, spores, plasmid, and exotoxin.,Lipopolysaccharide (LPS), outer membrane protein (OMP), Type IV secretion system (T4SS), and BvrR/BvrS system contribute to virulence of Brucella. The pathogenicity depends on its ability to multiply and survive within macrophages (Głowacka et al., 2018). The bacteria has strong resistance in the natural environment and is sensitive to light, heat, acid, and common disinfectants. It can survive for about 120 days in the secretions of sick animals, excretion and organs of dead animals, and for 60 days in dairy products (Unuvar et al., 2019). Brucella can enter the body through direct contact, conjunctival inoculation, gastrointestinal tract, respiratory tract, and biological transmission. While, nosocomial contagion is an important mode of infection. In particular, laboratory workers are likely to acquire the bacteria through aerosols or direct contact (Li et al., 2020).The disease is common in the Middle East, Asia, Africa, South and Central America, the Mediterranean, and the Caribbean. More than 170 countries and territories worldwide have reported cases of brucellosis, with outbreaks in Syria, Mexico, Peru, Argentina and Africa were severely affected (Pappas et al., 2006; Giambartolomei and Delpino, 2019). Clinically, brucellosis is manifested with non-specific symptoms, such as fever, excessive sweating, malaise, loss of appetite, testicular enlargement, joint pain, skin rash, and enlarged liver, spleen, and lymph nodes. Although complicated symptoms, fever and arthralgia are the main manifestations (Dean et al., 2012).
The diagnosis of brucellosis depends mainly on the epidemiological history of the patient, clinical manifestations, serological tests and bacterial cultures. The rose Bengal test (RBT) is commonly used for primary screening because of its high sensitivity, low cost and simplicity. The standard agglutination test (SAT) titer ≥1:160 and the 2-mercaptoethanol test (2-ME) titer ≥1:80 are considered diagnostic when coupled with a compatible clinical presentation. Of course, the results of both SAT and 2-ME experiments are related to the characteristics of the patient population and the quality of the reagents used. A SAT ≥1:320 is still recommended as a cut-off value for serological diagnosis of human brucellosis in endemic areas. In areas with low disease prevalence, the titre range of 1:40 to 1:80 in 2-ME experiment can be considered for the diagnosis of brucellosis (Yagupsky et al., 2019).
Brucellosis is a significant public health issue in developing countries, posing a major threat to human health the entire social and economic development. Because its clinical symptoms are not specific, it is easy to be misdiagnosed and that leads to chronic phase. What is more, If treatment is not taken in the acute phase, various complications will occur, resulting in disability, skeletal deformity, and even death. Besides, brucellosis may accumulate complications of the locomotor-osteoarticular system, digestive system, respiratory system, genitourinary system, cardiovascular system, nervous system, and blood, posing a major threat to human health the entire social and economic development. This article provides a systematic review of brucellosis-related complications.
2 Motion-osteoarticular system
Involvement of bone and joint is the most common complication of brucellosis, with a prevalence of approximately 2-77%. Brucella osteoarthropathy usually presents as spondylitis, sacroiliac arthritis, peripheral arthritis and osteomyelitis, while bursitis and tenosynovitis are rare. 2-60% prevalence of Brucella spondylitis, 2-45% prevalence of sacroiliac arthritis, and 14-26% prevalence of peripheral arthritis were reported (Unuvar et al., 2019).
Brucella spondylitis is the most common and severe manifestation of the osteoarthritis system, prevalent in elderly patients, often presenting as chronic back pain with fever, systemic symptoms, and dysfunction and teratogenicity in advanced stages of the disease. Spondylitis is dominated by involvement of the lumbar spine, followed by the thoracic and cervical spine (60% in the lumbar spine, 19% in the thoracic spine, and 12% in the cervical spine). The lumbar spine, an important weight-bearing structure of the human spine, is highly mobile and contains many cancellous bones and a rich venous plexus where bacterial emboli are more likely to lodge. The lumbar spine mainly presents with focal lesions, with the L4 and L5 vertebrae predominantly involved, and discontinuous multi-site vertebral segmental injuries are less common (Unuvar et al., 2019). Spondylodiscitis is common at the L3-L4, L4-L5 and L5-S1 levels and can also accumulate in multiple regions of the cervical, thoracic and lumbar spine (Ma et al., 2021). Complex brucellosis spondylitis is severe and the infection can spread from the vertebrae to adjacent tissues such as the epidural, prevertebral and paravertebral tissues, major lumbar muscles and nerve roots. These manifestations can lead to spinal stenosis and trigger spinal cord and nerve compression with muscle spasm, motor weakness, sensory abnormalities and, in severe cases, neurological complications, such as paraplegia (Ulu-Kilic et al., 2014). High-resolution magnetic resonance imaging (MRI) is more useful in diagnosing brucellosis spondylitis (Charalambides et al., 2010).
Sacroiliac arthritis is more prevalent in patients infected with sheep seed bacteria, and its presentation can be unilateral or bilateral, predominantly in young people with significant pain. The incidence was higher in the 15-35 years age group, accounting for 55.1% (Hizel et al., 2007). It is usually accompanied by fever, low back pain and hip pain. Examination revealed positive straight-leg-rise maneuvers test and FABER test, and may be lead to easily misdiagnosed easily. Bone scans, MRIs, and arthrocentesis can avoid misdiagnosis (Dayan et al., 2009). Several studies have confirmed that elevated C-reactive protein is positively associated with the presence of sacroiliitis, C-reactive protein is expected to be a new diagnostic marker (Hizel et al., 2007).
Brucellosis complicated with peripheral arthritis is more common in children and adolescents, often accumulated knee joint, hip joint, ankle joint, etc. The typical symptoms of knee arthritis are swelling and pain in one joint (Zamani et al., 2011). The initial symptoms of hip arthritis are not obvious, but as the disease progresses, the pain worsens, accompanied by limited movement and deformity of the lower limbs. Physical examination showed deep tenderness and percussive pain at the lesion site, accompanied by a positive Tomas sign and positive “4” test; diagnosis and treatment are challenging. Delayed treatment can lead to severe complications, such as femoral head dislocation and ischemic necrosis (Jahmani et al., 2021). Shoulder arthritis is common in the elderly, with symptoms lasting long and often requiring an extended period to recover from joint damage. On the other hand, wrist, and ankle arthritis is relatively mild, and the prognosis is satisfactory (Bosilkovski et al., 2016).
Osteomyelitis is usually hematogenous. When Brucella invades the body, it can enter the bone marrow through blood-borne transmission and invade the bone marrow and bone cortex in a big way. Patients may present with recurrent high fever (wave fever), malaise, muscle aches, and joint pain. In adults, osteomyelitis accumulates in the spine and is characterized by spinal fever and pain, while in adolescents, osteomyelitis of the knee (Mete et al., 2012).
3 Digestive system
Gastrointestinal symptoms are common in patients with brucellosis and can manifest as decreased appetite, nausea, vomiting, abdominal pain, diarrhea and constipation, and hepatosplenomegaly in about 50% of patients with brucellosis. If gastrointestinal disturbances are present, gastrointestinal complications should be considered (Dean et al., 2012).
The liver is the most extensive reticuloendothelial phagocytic system in the body and is capable of a rapid and controlled response to invasion by pathogenic microorganisms. Brucella, however, can use the immune tolerance of the liver to evade the immune response and persist in the host. Brucella can stimulate hepatic shape cell activation and secretion of collagen, forming scar tissue and leading to chronic fibrosis or cirrhosis. Liver function is usually normal in Brucella-infected individuals, with the most common abnormalities manifesting as increases in transaminases and alkaline phosphatase that are not specific. However, all cases of elevated liver enzymes cannot be classified as liver involvement, and acute hepatitis due to brucellosis is not too common (Giambartolomei and Delpino, 2019).
Reductions in hemoglobin and platelets often accompany the digestive complications caused by brucellosis. Patients mostly consume raw milk, and on examination they may present with fever, excessive sweating, nausea, vomiting, abdominal pain, and other symptoms such as right quadrant tenderness, hepatosplenomegaly, and yellowing of the sclera. Serological tests and imaging can confirm the diagnosis, and abdominal computed tomography (CT) is more sensitive than abdominal ultrasound (Denk and Ozden, 2015). In a study of 251 patients with brucellosis, Pourbagher et al. identified 21 (8.4%) patients with splenomegaly, 15 (6%) patients with hepatomegaly, 4 (1.6%) patients with splenic abscess, 2 (0.8%) patients with splenic cyst, 2 (0.8%) patients with acute appendicitis, 1 patient (0.4%) with acute acalculous cholecystitis (Pourbagher et al., 2006).
In areas where brucellosis is endemic, patients with cirrhosis may be complicated by bacterial peritonitis. However, Brucella infection can also directly trigger ascites, which is extremely rare. Infection is usually detected by lymphocytic exudate, which may be related to the immune response of the abdominal mononuclear phagocytic system (Kantarçeken et al., 2005). In brucellosis combined with liver abscess, patients may present with intermittent fever, nausea, vomiting, right upper abdominal pain, and right upper abdominal peritoneal irritation on examination (Le Moigne et al., 2016). Patients with concurrent splenic abscess often have fever, arthralgia, and persistent dull pain in the left upper abdomen. The development of splenic abscesses may be associated with Brucella endocarditis. In hepatosplenic abscesses, routine antimicrobial therapy and puncture drainage are adequate measures (Deveer et al., 2013).
Brucellosis with acute cholecystitis is usually non-chronic and the pathogenesis is unknown. Usually, patients present on examination with fever, malaise, right upper abdominal pain, sometimes constipation and marked abdominal pressure with rebound pain, and Murphy’s sign is usually positive (Hariz et al., 2019). Brucella may also enter the pancreas through the biliary system and bloodstream, leading to acute pancreatitis, usually with fever, abdominal pain, nausea, vomiting, extensive mucosal yellowing of the skin and pancreatic edema, and elevated hepatobiliary enzymes may be associated with acute pancreatitis (Berber et al., 2014).
4 Respiratory system
Respiratory infections of brucellosis are rare and most are reported as clinical cases; pneumonia, pleurisy, pulmonary nodules, pulmonary granuloma, pleural effusion, lung abscess, thoracic abscess, pneumothorax, lymph node enlargement and mediastinal disease have been reported (Pappas et al., 2003; Olukman, 2008).
In a retrospective study, Georgios Pappas et al. found respiratory involvement in only 37 of 450 patients with brucellosis. Patients presented mainly with fever and cough, with individual symptoms such as dyspnea, manifesting as lobar pneumonia, bronchopneumonia, pleural effusion and hilar lymph node enlargement (Pappas et al., 2003). Pulmonary brucellosis may be associated with inhalation of contaminated aerosols and transmission of bacteraemia. However, it is rarely severe and effective with conventional therapy for simple brucellosis (Olukman, 2008). Erdem et al. retrospectively studied respiratory infections in patients with brucellosis in Turkey over a ten-year period from 2002 to 2012. Out of 133 patients with pulmonary brucellosis, 123 (92.5%) presented with acute infection and most presented with pneumonia (Erdem et al., 2014). Most of the patients with pneumonia had a history of consuming raw, unpasteurized milk or dairy products. The clinical presentation was mainly fever and cough, with an audible wet rales in the lungs, which could be further confirmed by imaging. Serologic testing or blood cultures confirm Brucella infection, and laboratory tests may be accompanied by elevated C-reactive protein, erythrocyte sedimentation rate, calcitoninogen, and other inflammatory markers (Xie et al., 2019). In addition, massive infiltration of inflammatory cells in the lungs may lead to massive pulmonary changes and pleural effusions (Singh et al., 2005).
In pulmonary nodules complicated by brucellosis, patients may present with bilateral pulmonary nodules on chest radiographs and CT, in addition to chest pain (Sevilla López et al., 2011). Brucellosis can also be complicated by pleural effusion, and in addition to the typical symptoms of pleurisy, such as chest pain, patients may present with cough and dyspnea. Pleural effusions are mainly lymphatic exudate, high in protein, low in pH and sugar, and may be positive for Brucella culture. Treatment may include antimicrobial and thoracentesis tube drainage and, if necessary, pulmonary cortical debridement (Erdem et al., 2014). Brucellosis is easily overlooked when it accumulates in the lungs, and clinical workers should pay attention to the patient’s epidemiologic history, serologic testing, and imaging for comprehensive evaluation, as well as for differentiation from tuberculosis and other respiratory diseases, with bronchoscopy feasible when necessary (Pericherla et al., 2021).
5 Genitourinary system
Approximately 2-20% of brucellosis cases involve the genitourinary system and often present clinically with fever, swelling of the epididymis, and scrotal pain. The most common complications of genitourinary brucellosis are unilateral epididymal-orchitis and orchitis, followed by prostatitis, cystitis, vaginitis and tubo-ovarian abscesses, with less frequent renal involvement (Batirel et al., 2020).
Brucellosis with testicular infection is predominant in the acute phase. In a retrospective study, Zhou Yan et al. found complications of genitourinary injury in 22 of 801 patients admitted with brucellosis over a 10-year period. Male patients were mostly complicated by orchitis, epididymal-orchitis, prostatitis and urethral stricture, mainly manifested by fever, testicular swelling, pain and difficulty in urination. Only one woman was complicated by vaginitis and cervicitis, manifested by increased leucorrhea, menstrual irregularities and lower abdominal distension (Zhou et al., 2020). Epididymitis often coexists with orchitis, called epididymal-orchitis, and is clinically characterized by persistent fever, acute scrotal pain, swelling and congestion, and may be accompanied by rare testicular abscesses, atrophy and oligospermia (Gozdas and Bal, 2020).Safwat et al.found a significantly impaired reproductive system and a higher prevalence of erectile dysfunction (ED) in patients with chronic brucellosis, accounting for 70% of cases, and associated with testicular atrophy and serum decreased serum testosterone levels (Safwat et al., 2018).
The accumulated kidneys of brucellosis can be divided into three types. First, acute interstitial nephritis or pyelonephritis occurring in the acute phase of brucellosis, mostly associated with hematuria, proteinuria or pusuria. Second chronic brucellosis with renal involvement, which can lead to chronic granulomatous interstitial nephritis with caseous necrosis and calcification, similar to renal tuberculosis or chronic nonspecific pyelonephritis. Third, brucellosis endocarditis with renal involvement is associated (Conkar et al., 2018). Patients with renal involvement have varying degrees of hematuria and proteinuria in addition to the typical symptoms of brucellosis, such as fever, hyperhidrosis, malaise, and loss of appetite (Ceylan et al., 2009). If the lesions accumulate in the glomerulus, patients tend to present with abnormal urinary sediment, proteinuria or azotemia. The pathogenesis of this disease is usually related to the deposition of circulating immune complexes (Kusztal et al., 2007). Acute renal failure due to brucellosis is rare and is mainly caused by acute interstitial nephritis caused by direct invasion of the kidney by Brucella infection. Patients may present with oliguria or anuria and significant elevation of urea nitrogen and creatinine (Ghanei et al., 2009).
6 Cardiovascular system
Patients with brucellosis are usually associated with varying degrees of ventricular diastolic dysfunction and myocardial injury. Recurrent chronic infection with Brucella can lead to vascular endothelial dysfunction and promote atherosclerosis, leading to various cardiovascular complications (Togan et al., 2015).
Infective endocarditis is the most common complication of brucellosis combined with the cardiovascular system, although its incidence is less than <2% of patients with brucellosis (Ece et al., 2020). Endocarditis often invades the aortic and mitral valves, and patients often present with fever, malaise, and chest pain, along with elevated C-reactive protein or erythrocyte sedimentation rate. Infective endocarditis can lead to venous thrombosis, organ embolism, and heart failure, which can be fatal. Although the overall mortality rate of brucellosis is approximately 1%, >80% of brucellosis deaths are associated with endocarditis (Tuncer et al., 2008; Açar et al., 2015). Studies have shown that embolic events are present in 22%-43% of patients with infective endocarditis. Acute myocardial infarction and ischemic stroke due to endocarditis caused by Brucella infection are usually associated with septic artery embolism. The most common site of infected coronary embolism is the left anterior descending branch; however, coronary angiography performed during active endocarditis may lead to systemic embolism (Açar et al., 2015; Randa et al., 2021). Brucella infection can also lead to aortic involvement, and extensive diagnostic testing for Brucella aortic involvement and aneurysm formation should be performed in patients over 50 years of age with positive Brucella blood cultures and presenting with fever, back pain, or chest pain (Cascio et al., 2012).
Brucella infection can also lead to arrhythmias or coronary ischemic changes. Lu et al. found abnormalities in 31/108 (28.7%) patients with brucellosis. The ECG showed sinus bradycardia, precontraction of the ventricles, conduction block, ST-T abnormalities, Q-wave abnormalities and poor R-wave progression (Lu et al., 2021).
7 Blood system
Hematologic abnormalities in brucellosis may be associated with altered iron metabolism due to infection, hypersplenism, phagocytosis, myelosuppression, diffuse anticoagulation, and autoimmune hemolysis (Okur et al., 2012).
Brucellosis is complicated by hematologic disease and most commonly occurs in pediatric patients in the acute phase; patients may have hepatosplenomegaly and lymph node enlargement. Anemia is the most common hematologic complication, occurring in approximately 20-53% of children; the incidence of leukopenia is approximately 8-38%; thrombocytopenia 2-16%; and the incidence of pancytopenia is usually less than 10%.Justman et al. found that in 511 brucellosis disease, 68 (13%) were anemic, 144 (28%) were leukopenic, 74 (14%) were thrombocytopenic, and 9 (2%) were allocytopenic (Justman et al., 2018).
Patients with brucellosis complicated with pancytopenia often present with fever, loss of appetite, joint pain and other symptoms, and bone marrow aspiration can show histiocytic hemophagocytosis and granuloma formation (Sari et al., 2008). Brucella infection can also be complicated by secondary thrombocytopenic purpura, which is mainly manifested as fever and ecchymosis in the extremities, and may be accompanied by severe thrombocytopenia in laboratory tests (Bhasin et al., 2021). Brucellosis can also cause hemophagocytic lymphohistiocytosis (HLH), in which patients may present with fever, hepatosplenomegaly, cytopenia, hypofibrinogenemia, hypertriglyceridemia, and hyposideremia. Histiocytic proliferation and phagocytosis were observed in bone marrow aspirates (Mittal et al., 2021). Meanwhile, Bakri et al. reported the first case of bone marrow fibrosis caused by brucellosis leading to pancytopenia (Bakri et al., 2010). Brucellosis may also be associated with hematological malignancies. In addition, Brucella infection can also lead to myelodysplastic syndrome (MDS) and gammopathy (Wang et al., 2020).
8 Nervous system
The incidence of brucellosis in the nervous system is about 0.5-25%, and its pathogenesis may be related to the direct invasion of intracellular microorganisms or the immune mechanism of neuropathological changes caused by infection (Kanjo et al., 2021).
Neurobrucellosis (NB) presents in three forms: meningitis, chronic peripheral disease and diffuse central nervous system disease (Gul et al., 2009). The diagnosis depends on the patient’s clinical presentation, cerebrospinal fluid testing, imaging, serological testing, and bacterial culture. Cerebrospinal fluid testing revealed lymphocytosis, an increased protein level, and a decreased glucose concentration. In patients with abnormal signs and suspected brucellosis, cranial MRI is preferred (Díaz-Vintimilla et al., 2021). Meningitis is the most common manifestation of neurobrucellosis. In addition, meningoencephalitis, myelitis, radiculitis, cranial nerve involvement, cerebrovascular disease, brain abscess, intracranial hypertension, hydrocephalus, epidural abscess, demyelinating disease, Guillain-Barre syndrome (GBS), cerebral venous thrombosis, paraplegia, and aphasia have been reported (Maji et al., 2020).
Patients with neurobrucellosis may present with fever, headache, accompanied by meningeal irritation, hyperalgesia and confusion [73]. Infection of the central nervous system in brucellosis can also lead to the syndrome of inappropriate secretion of antidiuretic hormone (SIADH), which is also prevalent in brucellosis. Bala et al. detected SIADH in 35 of 160 (21.9%) children and adolescents with brucellosis. The pathogenesis of SIADH remains unclear and may be related to hypoxia and hypovolemia (Bala et al., 2016).
9 Other
The prevalence of brucellosis complicated with skin lesions is about 5-17%. It is broadly divided into four categories: disseminated papules, nodular rashes (most common), erythema nodosum lesions, generalized maculopapules, and generalized purpura. The pathogenesis may be related to hypersensitivity, immune complex deposition, vaccination or blood transmission of Brucella (Al Jasser and Al Ajroush, 2012; Uçmak et al., 2014).
Rolando et al. found that of 1551 patients with brucellosis admitted over a 26-year period, 52 had ocular brucellosis (3.4%). Among them, 43 cases (82.7%) had uveitis. Ocular involvement is common in the chronic phase of brucellosis, especially in young women aged 16-35 years, who often present with blurred vision (Rolando et al., 2008). Brucella infection can also cause cervical brucellosis lymphadenopathy, and patients usually complain of neck swelling. Submandibular mass and local lymph node necrosis were seen on neck CT, which required needle biopsy to confirm infection to rule out malignancy (Yilmaz et al., 2009). In infectious thyroiditis caused by brucellosis, patients often have anterior neck pain and swelling, accompanied by sore throat, mild dysphagia and hoarseness, and goiter can be seen on physical examination. If left untreated, a thyroid abscess may develop. Thyroid ultrasound and thyroid function measurement can complement the diagnosis (Cvetkova et al., 2019).
Breast involvement after Brucella infection is less common. Nonetheless, it can be complicated by mastitis and breast abscesses, and patients may present with fever, breast pain, swelling, and patchy erythema around the areola. Breast ultrasound, pus culture, and needle biopsy can help diagnose infection. Although breast infection is rare in lactating women, pregnancy and a history of breast augmentation may be predisposing factors (Jensenius et al., 2008).
10 Conclusion
Brucellosis is a systemic disease that may accumulate in multiple tissues and organs of the body, consisting of the musculoskeletal system, reproductive system, central nervous system, liver, heart, and lungs (see Table 1 for details of involvement/complication rates). The existence of these complications brings great challenges to diagnosis and treatment. A diagnosis should be made with a comprehensive judgment on multiple examinations and test results, so as to improve the diagnostic accuracy and avoid misdiagnosis or underdiagnosis. On the other hand, a reasonable therapy plan should be formulated according to the state of illness and the involved tissues and organs. It is recommended to take two or more antibiotics combined treatment, reducing delayed treatment and misdiagnosis, preventing the occurrence of chronicity, improving the treatment effect of brucellosis, and avoiding recurrence and complications.
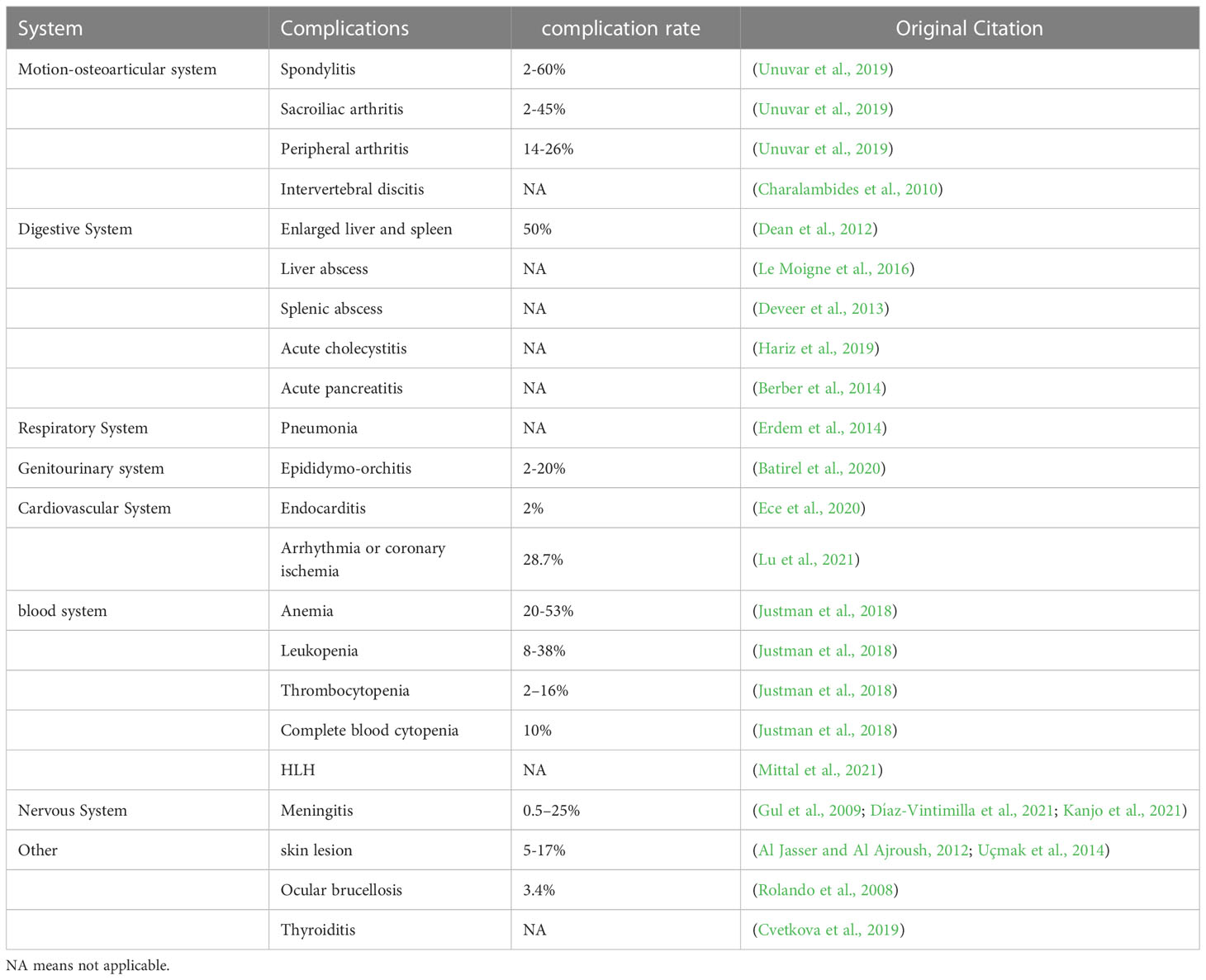
Table 1 Multisystem complications of brucellosis and their involvement/complication rates.
Author contributions
ZG, ZW, and MJ contributed to the conception and design of this study. ZF, RG, and XL performed the literature collection. MJ and ZF wrote the first draft of the manuscript. All the authors contributed to manuscript revision, read, and approved the version as submitted.
Funding
This study was supported by the Inner Mongolia Autonomous Region Science and Technology Innovation guide Project (CXYD2021BT01), the Inner Mongolia Natural Science Foundation Project (2021MS08048).
Conflict of interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Publisher’s note
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
References
Açar, G., Ozkok, A., Dönmez, C., Avcı, A., Alizade, E., Yanartaş, M., et al. (2015). Myocardial infarction due to septic coronary artery embolism in the course of brucella endocarditis. Herz. 40 (2), 335–337. doi: 10.1007/s00059-013-4011-z
Al Jasser, M., Al Ajroush, W. (2012). Brucellosis presenting as septal panniculitis with vasculitis. Int. J. Dermatol. 51 (12), 1526–1529. doi: 10.1111/j.1365-4632.2010.04783.x
Bakri, F. G., Al-Bsoul, N. M., Magableh, A. Y., Shehabi, A., Tarawneh, M., Al-Hadidy, AM., et al. (2010). Brucellosis presenting as myelofibrosis: first case report. Int. J. Infect. Dis. 14 (2), e158–e160. doi: 10.1016/j.ijid.2009.03.018
Bala, K. A., Doğan, M., Kaba, S., Akbayram, S., Aslan, O., Kocaman, S., et al. (2016). The syndrome of inappropriate secretion of anti-diuretic Hormone(SIADH) and brucellosis. Med. Sci. Monit. 22, 3129–3134. doi: 10.12659/MSM.899977
Batirel, A., Regmi, S. K., Singh, P., Mert, A., Konety, B. R., Kumar, R. (2020). Urological infections in the developing world: an increasing problem in developed countries. World J. Urol 38 (11), 2681–2691. doi: 10.1007/s00345-020-03120-3
Berber, I., Erkurt, M. A., Yetkin, F., Unlu, S., Yilmaz, S., Bazna, S. (2014). A rare disease in the differential diagnosis of acute pancreatitis: acute brucellosis. Intern. Med. 53 (20), 2401–2404. doi: 10.2169/internalmedicine.53.2510
Bhasin, A., Singal, R. K., Chaudhary, D., Sharma, SK., Arora, S., Setia, R., et al. (2021). Thrombotic thrombocytopenic purpura in a patient with brucella infection. J. Assoc. Physicians India 69 (10), 11–12.
Bosilkovski, M., Zezoski, M., Siskova, D., Miskova, S., Kotevska, V., Labacevski, N. (2016). Clinical characteristics of human brucellosis in patients with various monoarticular involvements. Clin. Rheumatol 35 (10), 2579–2584. doi: 10.1007/s10067-016-3207-z
Cascio, A., De, Caridi, G., Lentini, S., Benedetto, F., Stilo, F., Passari, G., et al. (2012). Involvement of the aorta in brucellosis: the forgotten,life-threatening complication. a systematic review. Vector Borne Zoonotic Dis. 12 (10), 827–840. doi: 10.1089/vbz.2012.0965
Ceylan, K., Karahocagil, M. K., Soyoral, Y., Sayarlioğlu, H., Karsen, H., Dogan, E., et al. (2009). Renal involvement in brucella infection. Urology 73 (6), 1179–1183. doi: 10.1016/j.urology
Charalambides, C., Papademetriou, K., Sgouros, S., Sakas, D. (2010). Brucellosis of the spine affecting multiple non-contiguous levels. Br. J. Neurosurg. 24 (5), 589–591. doi: 10.3109/02688697
Conkar, S., Kosker, M., Cevik, S., Ay, M. (2018). Association of brucellosis with renal tubular and glomerular damage in children in Turkey. Saudi J. Kidney Dis. Transpl 29 (2), 284–289. doi: 10.4103/1319-2442.229288
Cvetkova, M., Bitoska, I., Poposki, K., Jakimovski, D., Bosilkovski, M. (2019). Acute thyroiditis associated with brucellosis: A case report. Pril (Makedon Akad Nauk Umet Odd Med. Nauki) 40 (2), 113–117. doi: 10.2478/prilozi-2019-0022
Dayan, L., Deyev, S., Palma, L., Rozen, N. (2009). Long-standing, neglected sacroiliitis with remarked sacro-iliac degenerative changes as a result of brucella spp.infection. Spine J. 9 (3), e1–e4. doi: 10.1016/j.spinee.2008.03.011
Dean, A. S., Crump, L., Greter, H., Hattendorf, J., Schelling, E., Zinsstag, J. (2012). Clinical manifestations of human brucellosis: a systematic review and meta-analysis. PLoS Negl. Trop. Dis. 6 (12), e1929. doi: 10.1371/journal.pntd.0001929
Deng, Y., Liu, X., Duan, K., Peng, Q. (2019). Research progress on brucellosis. Curr. Med. Chem. 26 (30), 5598–5608. doi: 10.2174/0929867325666180510125009
Denk, A., Ozden, M. (2015). A case of brucellosis presenting with acute hepatitis and bicytopenia. Infez Med. 23 (2), 178–181.
Deveer, M., Sozen, H., Çullu, N., Sivrioglu, A. K. (2013). Splenic abscess due to acute brucellosis. BMJ Case Rep. 2013, bcr2012008485. doi: 10.1136/bcr-2012-008485
Díaz-Vintimilla, J. J., Rosales Hernández, L. A., Zapata-Arenas, R., Sánchez-Montes, S., Becker, I. (2021). Subacute transverse myelitis as a clinical presentation of neurobrucellosis. J. Infect. Dev. Ctries 15 (9), 1359–1363. doi: 10.3855/jidc.14753
Ece, İ., Epçaçan, S., Bayhan, Gİ., Türe, M. (2020). Diastolic dysfunction in patients with brucellosis despite the absence of infective endocarditis. Cardiol. Young 30 (12), 1840–1843. doi: 10.1017/S1047951120002930
Erdem, H., Inan, A., Elaldi, N., Tekin, R., Gulsun, S., Ataman-Hatipoglu, C., et al. (2014). Brucellosis study group. respiratory system involvement in brucellosis: the results of the kardelen study. Chest 145 (1), 87–94. doi: 10.1378/chest.13-0240
Ghanei, E., Miladipour, A., Nasrollahi, A., Homayuni, M. (2009). Brucellosis with kidney failure. Iran J. Kidney Dis. 3 (2), 109–111.
Giambartolomei, G. H., Delpino, M. V. (2019). Immunopathogenesis of hepatic brucellosis. Front. Cell Infect. Microbiol. 9. doi: 10.3389/fcimb.2019.00423
Głowacka, P., Żakowska, D., Naylor, K., Niemcewicz, M., Bielawska-Drózd, A. (2018). Brucella -virulence factors, pathogenesis and treatment. Pol. J. Microbiol. 67 (2), 151–161. doi: 10.21307/pjm-2018-029
Gozdas, H. T., Bal, T. (2020). Brucellar epididymo-orchitis: a retrospective study of 25 cases. Aging Male 23 (1), 29–32. doi: 10.1080/13685538.2019.1573892
Gul, H. C., Erdem, H., Bek, S. (2009). Overview of neurobrucellosis: a pooled analysis of 187 cases. Int. J. Infect. Dis. 13 (6), e339–e343. doi: 10.1016/j.ijid.2009.02.015
Hariz, A., Beji, I., Hamdi, M. S., Cherif, E. (2019). Brucellosis, an uncommon cause of acute acalculous cholecystitis: two new cases and concise review. BMJ Case Rep. 12 (9), e229616. doi: 10.1136/bcr-2019-229616
Hizel, K., Guzel, O., Dizbay, M., Karakus, R., Senol, E., Arman, D., et al. (2007). Age and duration of disease as factors affecting clinical findings and sacroiliitis in brucellosis. Infection 35 (6), 434–437. doi: 10.1007/s15010-007-6361-z
Jahmani, R., Obeidat, O., Yusef, D. (2021). Brucella septic hip arthritis: A case report. Am. J. Case Rep. 22, e928592. doi: 10.12659/AJCR.928592
Jensenius, M., von der Lippe, B., Hermansen, N. O., Jahr, G., Caugant, DA., Høiby, EA., et al. (2008). Brucellar mastitis: presentation of a case and review of the literature. Int. J. Infect. Dis. 12 (1), 98–100. doi: 10.1016/j.ijid
Jiao, H., Zhou, Z., Li, B., Xiao, Y., Li, M., Zeng, H., et al. (2021). The mechanism of facultative intracellular parasitism of brucella. Int. J. Mol. Sci. 22 (7), 3673. doi: 10.3390/ijms22073673
Justman, N., Fruchtman, Y., Greenberg, D., Ben-Shimol, S. (2018). Hematologic manifestations of brucellosis in children. Pediatr. Infect. Dis. J. 37 (6), 586–591. doi: 10.1097/INF.0000000000001900
Kanjo, M. A., Ahmed, H. M., Alnahari, E. A. (2021). Unusual presentation of neurobrucellosis in jeddah, kingdom of Saudi Arabia. Neurosci. (Riyadh) 26 (4), 385–388. doi: 10.17712/nsj.2021.4.20210030
Kantarçeken, B., Harputluoğlu, M. M., Bayindir, Y., Bayraktar, M. R., Aladağ, M., Hilmioğlu, F. (2005). Spontaneous bacterial peritonitis due to brucella melitensis in a cirrhotic patient. Turk J. Gastroenterol. 16 (1), 38–40.
Kusztal, M., Dorobisz, A., Kuzniar, J., Garcarek, J., Koscielska-Kasprzak, K., Kaminska, D., et al. (2007). Dissecting aneurysm of the thoracic aorta in a patient with nephrotic syndrome and brucellosis. Int. Urol Nephrol. 39 (2), 641–645. doi: 10.1007/s11255-006-9090-9
Le Moigne, F., Vitry, T., Gérôme, P., Vinurel, N., Ducerf, C., Rode, A., et al. (2016). Necrotizing pseudotumoral hepatic brucelloma: Imaging-pathologic correlation. Diagn. Interv Imaging 97 (2), 243–246. doi: 10.1016/j.diii.2014.08.007
Li, N., Yu, F., Peng, F., Zhang, X., Jia, B. (2020). Probable sexual transmission of brucellosis. IDCases. 21, e00871. doi: 10.1016/j.idcr.2020.e00871
Lu, L. H., Song, Y. Q., Wu, Q. M., Wang, Z., Chen, YF., Dong, Q., et al. (2021). Analysis of electrocardiogram among 108 patients with brucella. Int. J. Gen. Med. 14, 5251–5254. doi: 10.2147/IJGM.S322019
Ma, L., Ma, J., Chen, X., Dong, L. (2021). A 10-year retrospective comparative analysis of the clinical features of brucellosis in children and adults. J. Infect. Dev. Ctries 15 (8), 1147–1154. doi: 10.3855/jidc.13962
Maji, S., Manjunath, N., Bahubali, V. H., Shome, R., Palaniappan, M., Lahiri, S., et al. (2020). Chandrashekar n. neurobrucellosis: A neglected entity? an update from tertiary care neurocentre of south East Asia. J. Neurol. Sci. 411, 116683. doi: 10.1016/j.jns.2020.116683
Mete, B., Kurt, C., Yilmaz, M. H., Ertan, G., Ozaras, R., Mert, A., et al. (2012). Vertebral osteomyelitis: eight years' experience of 100 cases. Rheumatol Int. 32 (11), 3591–3597. doi: 10.1007/s00296-011-2233-z
Mittal, J., Kumar, P., Goyal, J. P., Purohit, A. (2021). Haemophagocytic lymphohistiocytosis secondary to brucellosis in a young child. BMJ Case Rep. 14 (3), e240759. doi: 10.1136/bcr-2020-240759
Okur, M., Erbey, F., Bektaş, MS., Kaya, A., Doğan, M., Acar, M. N., et al. (2012). Retrospective clinical and laboratory evaluation of children with brucellosis. Pediatr. Int. 54 (2), 215–218. doi: 10.1111/j.1442-200X.2011.03558.x
Olukman, O. (2008). Pulmonary involvement in childhood brucellosis: a case report. Vector Borne Zoonotic Dis. 8 (2), 245–248. doi: 10.1089/vbz.2007.0185
Pappas, G., Bosilkovski, M., Akritidis, N., Mastora, M., Krteva, L. (2003). Tsianos E.Brucellosis and the respiratory system. Clin. Infect. Dis. 37 (7), e95–e99. doi: 10.1086/378125
Pappas, G., Papadimitriou, P., Akritidis, N., Christou, L. (2006). Tsianos EV. the new global map of human brucellosis. Lancet Infect. Dis. 6 (2), 91–99. doi: 10.1016/S1473-3099(06)70382-6
Pericherla, S., Gupta, N., Saravu, K. (2021). Clinical profile and treatment outcomes of patients with brucellosis: a hospital-based cohort study from southern India. Infez Med. 29 (1), 65–69.
Pourbagher, M. A., Pourbagher, A., Savas, L., Turunc, T., Demiroglu, Y. Z., Erol, I., et al. (2006). Clinical pattern and abdominal sonographic findings in 251 cases ofbrucellosis in southern Turkey. AJR Am. J. Roentgenol 187 (2), W191–W194. doi: 10.2214/AJR.05.0241
Randa, T., Christelle, E., Rachoin, R., Bassam, H., Nabil, T., Madonna, M., et al. (2021). Brucella involving the heart: a hidden disease. Int. J. Cardiovasc. Imaging 37 (10), 2901–2904. doi: 10.1007/s10554-021-02261-9
Rolando, I., Olarte, L., Vilchez, G., Lluncor, M., Otero, L., Paris, M, et al. (2008). Ocular manifestations associated with brucellosis: a 26-year experience in Peru. Clin. Infect. Dis. 46 (9), 1338–1345. doi: 10.1086/529442
Safwat, A. S., Hasanain, A. F., Mahran, A., Bakkar, S., Abdel-Aal, S., Nafee, A. (2018). Erectile dysfunction among patients with chronic brucellosis. Int. J. Impot Res. 30 (5), 230–236. doi: 10.1038/s41443-018-0068-9
Sari, I., Altuntas, F., Hacioglu, S., Kocyigit, I., Sevinc, A., Sacar, S., et al. (2008). A multicenter retrospective study defining the clinical and hematological manifestations of brucellosis and pancytopenia in a large series: Hematological malignancies, the unusual cause of pancytopenia in patients with brucellosis. Am. J. Hematol. 83 (4), 334–339. doi: 10.1002/ajh.21098
Sevilla López, S., Quero Valenzuela, F., Piedra Fernández, I. (2011). Bilateral pulmonary nodules due to brucellosis. Arch. Bronconeumol 47 (6), 320–321. doi: 10.1016/j.arbres.2011.02.003
Singh, M., Salaria, M., Kumar, L. (2005). Pneumonic presentation of brucellosis. Indian J. Pediatr. 72 (1), 65–66. doi: 10.1007/BF02760583
Togan, T., Ciftci, O., Gunday, M., Narci, H., Arslan, H. (2015). Does brucellosis cause arterial stiffness and ventricular remodelling through inflammation? Acta Cardiol. 70 (2), 185–195. doi: 10.1080/ac.70.2.3073510
Tuncer, M., Ekim, H., Güneş, Y., Güntekin, Ü. (2008). Atrial septal defect presenting with brucella endocarditis. Circ. J. 72 (12), 2096–2097. doi: 10.1253/circj.cj-07-0980
Uçmak, F., Uçmak, D., Beştaş, R., Azizoğlu Anli, R., Adanir, H. (2014). Acute brucellosis associated with leukocytoclastic vasculitis and splenic infarct. Infez Med. 22 (4), 326–330.
Ulu-Kilic, A., Karakas, A., Erdem, H., Turker, T., Inal, A. S., Ak, O., et al. (2014). Update on treatment options for spinal brucellosis. Clin. Microbiol. Infect. 20 (2), O75–O82. doi: 10.1111/1469-0691.12351
Unuvar, G. K., Kilic, A. U., Doganay, M. (2019). Current therapeutic strategy in osteoarticular brucellosis. North Clin. Istanb 6 (4), 415–420. doi: 10.14744/nci.2019.05658
Wang, W., Lu, X., Li, C., Ri, M. J., Cui, W. (2020). A man with recurrent fever, arthritis, and rashes-brucellosis? a case report. BMC Infect. Dis. 20 (1), 18. doi: 10.1186/s12879-019-4746-0
Whatmore, A. M., Foster, J. T. (2021). Emerging diversity and ongoing expansion of the genus brucella. Infect. Genet. Evol. 92, 104865. doi: 10.1016/j.meegid.2021.104865
Xie, S., Zhou, Y., Zheng, R., Zuo, W., Zhang, Y., Wang, Y., et al. (2019). Childhood pneumonia due to brucellosis: A case report. Med. (Baltimore) 98 (27), e16247. doi: 10.1097/MD.0000000000016247
Yagupsky, P., Morata, P., Colmenero, J. D. (2019). Laboratory diagnosis of human brucellosis. Clin. Microbiol. Rev. 33 (1), e00073–e00019. doi: 10.1128/CMR.00073-19
Yilmaz, M., Bayazit, N., Gürbüzler, L., Ercan, N., Ceylan, A., Bayazit, Y. (2009). Isolated cervical lympadenopathy: unusual presentation of localised brucellosis. Int. J. Clin. Pract. 63 (4), 674–675. doi: 10.1111/j.1742-1241.2005.00812.x
Zamani, A., Kooraki, S., Mohazab, R. A., Zamani, N., Matloob, R., Hayatbakhsh, M. R., et al. (2011). Epidemiological and clinical features of brucella arthritis in 24 children. Ann. Saudi Med. 31 (3), 270–273. doi: 10.4103/0256-4947.81543
Keywords: brucellosis, complications, osteoarthritis, endocarditis, meningitis
Citation: Jin M, Fan Z, Gao R, Li X, Gao Z and Wang Z (2023) Research progress on complications of Brucellosis. Front. Cell. Infect. Microbiol. 13:1136674. doi: 10.3389/fcimb.2023.1136674
Received: 03 January 2023; Accepted: 20 March 2023;
Published: 31 March 2023.
Edited by:
Zeliang Chen, School of Public Health, Sun Yat-sen University, ChinaReviewed by:
İlhami Çelik, University of Health Sciences, TürkiyeNazan Tuna, Namik Kemal University, Türkiye
Copyright © 2023 Jin, Fan, Gao, Li, Gao and Wang. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Zhixiang Gao, Z3p4aWFuZzcxNjc3MDVAMTYzLmNvbQ==; Zhanli Wang, d2FuZy56aGFubGlAaG90bWFpbC5jb20=
†These authors have contributed equally to this work and share first authorship