 Hua-Liang Huang†
Hua-Liang Huang† Hong-Bo Guo
Hong-Bo Guo
94% of researchers rate our articles as excellent or good
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.
Find out more
ORIGINAL RESEARCH article
Front. Cell. Infect. Microbiol., 06 January 2023
Sec. Clinical Microbiology
Volume 12 - 2022 | https://doi.org/10.3389/fcimb.2022.987260
Objective: To explore the carrying status and homology of carbapenem resistant Acinetobacter baumannii (CRAB) in our hospital.
Methods: From January 2015 to December 2017, 52 strains of acinetobacter baumannii isolated from the bacteria room of the clinical laboratory of Baogang hospital in Inner Mongolia were selected as the research object. K-B disk diffusion method and Vitek-2 were used to determine the drug sensitivity of Acinetobacter baumannii. The drug resistance gene was detected by polymerase chain reaction (PCR) and its homology was analyzed by pulsed field gel electrophoresis (PFGE).
Results: Except for Cefoperazone/sulbactam, other antibiotics were resistant to ab. The detection rate of drug resistance gene class C β-lactamases (ADC) was 100%, and the higher detection rates of other drug resistance genes were class D β-lactamases (OXA)-51 (36 strains, 90.0%),disinfectant gene qacE△1-sull (32 strains, 80.0%), and klebsiella pneumoniae carbapenemase (KPC) gene was not detected. 2-8 drug resistance genes were detected in each CRAB strain, and the strains with 6 drug resistance genes were the most (15 strains, 37.5%); Among the detected drug-resistant gene combinations, ADC+OXA-23 + OXA-51 gene was detected at the same time (29 strains, 72.5%), followed by ADC+ intl1 + qacE △ 1-sull gene (26 strains, 65.0%), ADC + qacE △ 1-sull + ant (3 ‘‘) -i gene (19 strains, 47.5%), and 11 strains (27.5%). There were 19 different types in PFGE homology test, each type was 1-9 strains, including 9 strains of A5 type and 8 strains of A18 type, mainly from intensive care unit.
Conclusion: CRAB in the hospital is highly resistant to common clinical antibiotics. OXA-23 and OXA-51 genes are most likely to be the main factors causing drug resistance of Acinetobacter baumannii in the hospital. Homology analysis showed that there was CRAB nosocomial infection transmission in different wards of the hospital.
Acinetobacter baumannii (AB) is a conditional pathogen (Yuxing and Hong, 2007), accounting for more than 80% of clinically isolated Acinetobacter. It widely exists in hospital environment and nature (Zhizhi et al., 2017). Due to the abuse of antibiotics, the continuous variation of bacteria and the timeliness of the research and development of new antibiotics, the number of effective drugs that can be used for multidrug-resistant AB continues to decrease (Chen et al., 2015). From 1993 to 2004, AB resistance in the United States increased 10 times (Lockhart et al., 2007). In China, AB resistance also increased from 31% ~ 39% in 2005 to 62.4% ~ 66.7% in 2014 (Hu et al., 2016). AB infection has become an increasingly prominent public health problem (Chen et al., 2015) and the main threat of global nosocomial infection (Anunnatsiri and Tonsawan, 2011). Imipenem (IPM), belonging to carbapenems, is a kind of broad-spectrum and efficient antibiotics β− Lactam antibiotics have strong antibacterial activity against AB, but with the wide clinical application, the drug resistance rate is increasing year by year (Yanan et al., 2021).Carbapenem resistant Acinetobacter baumannii (CRAB) refers to ab that is resistant to carbapenem antibiotics such as imipenem or meropenem (Chen et al., 2015). At present, it is considered that carbapenemase production is the main reason for ab’s resistance to carbapenem antibiotics (Yanan et al., 2021).
The drug resistance mechanism of AB is very complex and can be mediated by a variety of drug resistance mechanisms. If the expression of outer membrane protein changes, it can cause the barrier of antibiotic permeability; Changes of topoisomerase and DNA gyrase; Overexpression of efflux pump of various drugs (Abdi et al., 2020). This paper will analyze the drug resistance characteristics and main epidemic types of Acinetobacter baumannii in our hospital, so as to provide basis for clinical better selection of antibiotics and control of nosocomial infection. This paper studies the homology and drug resistance mechanism of drug-resistant CRAB, which is reported as follows.
40 CRAB strains isolated from the bacteria room of the clinical laboratory of Inner Mongolia Baogang hospital from January 2015 to December 2017 were selected as the research objects. Remove duplicate strains isolated from the same patient. The isolated strains were identified and tested by automatic microbial identification and drug sensitivity instrument. Some drug sensitivity tests and reviews were conducted by disk diffusion method (K-B method). The drug sensitivity results were judged according to the American Society for clinical laboratory standardization (CLSI) version 2021. The quality control strains were Escherichia coli ATCC25922, Pseudomonas aeruginosa atcc27853, enzyme producing Escherichia coli atcc35218 and Klebsiella pneumoniae atcc70060.
PCR FQZD (BIOER), nucleic acid electrophoresis apparatus (DYY-6C, Beijing 61), automatic gel imaging analysis system (ZF-258, Shanghai Jia Peng), fluorescence quantitative polymerase chain reaction (PCR) instrument (FQD-48A, BIOER company), electronic constant temperature stainless steel water bath pot (HHS-2S, Shanghai Yichang instrument).
RNA extraction reagent and DNA loading buffer were purchased from cwbio company. Dnamarker DL2000, reverse transcription PCR kit and Supermix were purchased from tran company. Agarose and dyes were purchased from xhly company.
The susceptibility of the strains to 15 kinds of antibiotics was detected by disk diffusion method (K-B method). Antibacterial drugs include: Cefoperazone/sulbactam, cefotaxime, ceftriaxone, levoflOXAcin, tobramycin, ceftazidime, imipenem, meropenem, piperacillin, piperacillin/tazobactam, gentamicin, amikacin, cefepime, minocycline, compound minocycline, etc. The pieces of paper were purchased from oxid. Columbia blood tablet was purchased from French merier company, and MH tablet was purchased from Zhengzhou Beiruite company. The judgment of drug sensitivity results shall be carried out according to the 2021 standard of American Society for clinical laboratory standardization (CLSI) (Humphries et al., 2021).
PFGE homology detection: after CRAB was isolated and cultured, the bacteria suspension with OD value of 3.6 ~ 4.0 was adjusted by turbidimeter. Add 1%seakem gold SDS to prepare gel. Digest with protease K, wash with pure water for 2 times, and then wash with TE for 4 times, about 15min each time. ApaI endonuclease was used for enzyme digestion and incubated in 37°C water bath for 4H. PFGE was performed in a pulsed field gel electrophoresis apparatus. The electrophoretic parameters were 5 ~ 20s, 14°C, 120° pulse angle electrophoresis for 19h. After electrophoresis, nucleic acid staining was performed, which was put into a gel apparatus for observation and photo preservation.
Eight strains of multidrug-resistant bacteria were selected as the drug-resistant group, and the gene expression levels of the strains in the drug-resistant group and the sensitive group were detected.
Extract the strain RNA according to the operation steps of the bacterial RNA extraction kit of Omega company, use the nucleic acid protein analyzer to detect the concentration of RNA and carry out electrophoresis. The genes were amplified by realtime PCR. The reaction system is 20ul, including 0.4ul of upstream and downstream primers and 5 UL of cDNA template, 2 × PerfectStartTM Green qPCR Super Mix10uL. Make up the volume to 20ul with DD H2O. The amplification conditions were three-step, the first step was 95 °C, 30s; 1 cycle; The second step is 95 °C, 5S; 60 °C, 30s, 40 cycles. See Table 1.
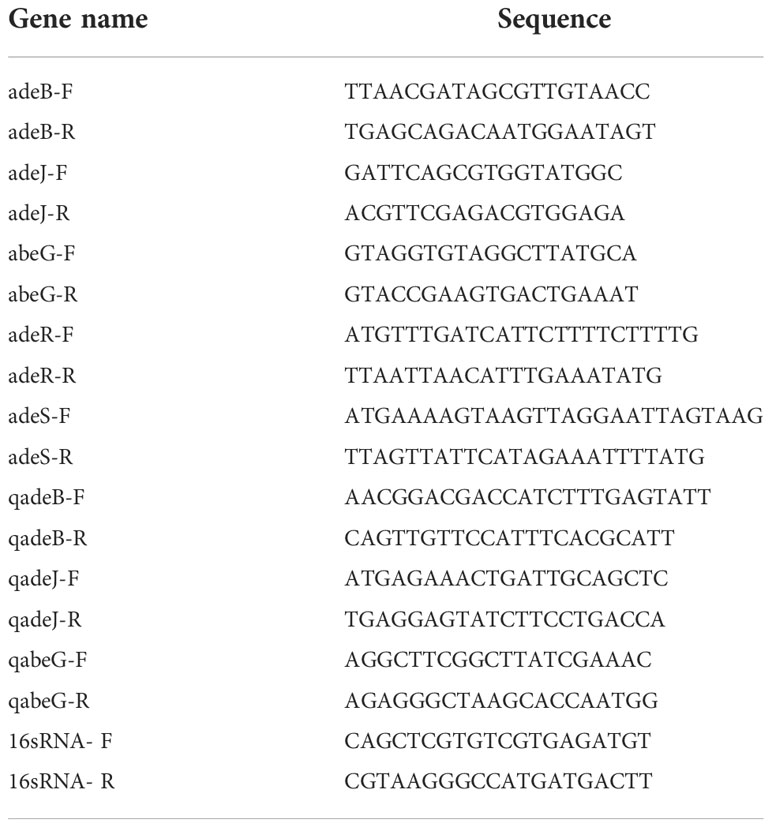
Table 1 Gene primer sequence and product size of realtime PCR.
Import the images saved by the gel imager into the bionumerily software for processing and analysis, and calculate the similarity coefficient between the strains with the Dice coefficient (Humphries et al., 2021). SD=2nxy/(nx+ny). Where nx represents the total number of bands of strain x, ny represents the total number of bands of strain y, nxy is the number of bands common to strain xy, and SD reflects the similarity of strains. The range is 0-1. 0 means completely different and 1 means exactly the same. The similarity coefficient of 80% is the typing boundary value, the similarity ≥ 80% is the same subtype, and the similarity < 80% is different genotypes.
A total of 40 CRAB strains were collected from 40 patients. The sources of specimens were vascular catheter tip (9 strains), drainage fluid (5 strains), blood (5 strains), bronchial lavage fluid (5 strains), urine (4 strains), secretion (4 strains), sputum (4 strains), cerebrospinal fluid (2 strains), ascites (1 strain), bile (1 strain), and 28 strains of CRAB were from intensive care unit (ICU). See Table 2.
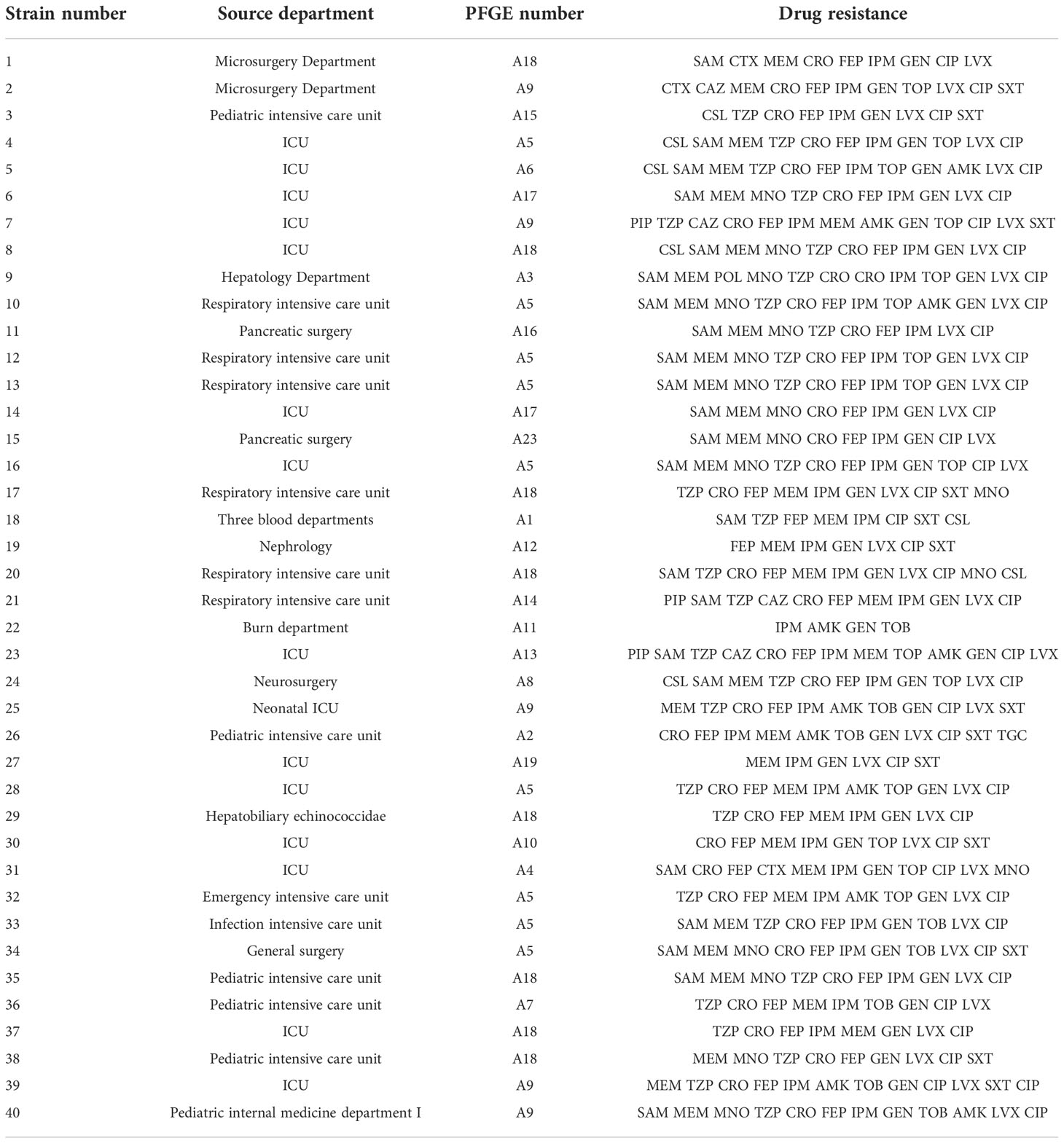
Table 2 Drug resistance spectrum of 40 crabs.
Among them, 40 AB strains were resistant to cefotaxime, ceftriaxone, levoflOXAcin, tobramycin, ceftazidime, imipenem, meropenem, piperacillin, piperacillin/tazobactam, gentamicin, amikacin, cefepime and minocycline, and the resistance rate was 100%. 10 AB strains were sensitive to Cefoperazone/sulbactam, and the resistance rate was 25.0%. 36 AB strains were sensitive to cotrimOXAzole, and the resistance rate was 90.4%. See Table 3.
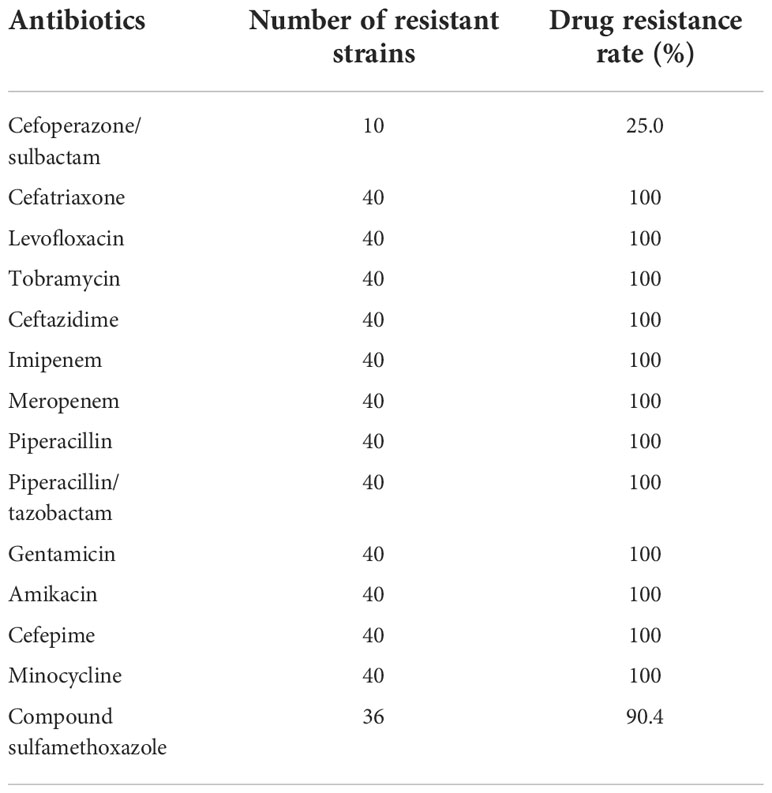
Table 3 Resistance of strains of CRAB resistant bacteria to common antibiotics.
ADC gene was detected in all 40 CRABs. The detection rates of other drug resistance genes were OXA-51 (90.0%), qacE△1-sull (80.0%), OXA-23 (77.5%), intl1 (72.5%), and KPC gene was not detected. 2-8 drug resistance genes were detected in each CRAB strain, and the strains with 6 drug resistance genes were the most (37.5%); Among the drug-resistant gene combinations detected, ADC + OXA-23 + OXA-51 gene was the most detected at the same time (29 strains, 72.5%), followed by ADC + intl1 + qacE△1-sul1 gene (26 strains, 65.0%), ADC + qacE△1-sull + ant (3″) -1 gene (19 strains, 47.5%), ADC + OXA-23 + OXA-51 + intl1 + qacE△1-sull gene (18 strains, 45.0%), and 11 strains (27.5%). ADC+ant (3″) -i + ACC(3) -i gene was detected. See Figure 1 and Table 4.

Figure 1 PCR amplification map of some drug resistance genes. M:Marker;1、2、3、7 and 11 are the amplification results of ADC, OXA-23, oxa-51, qacE△1-sull and TEM genes respectively.
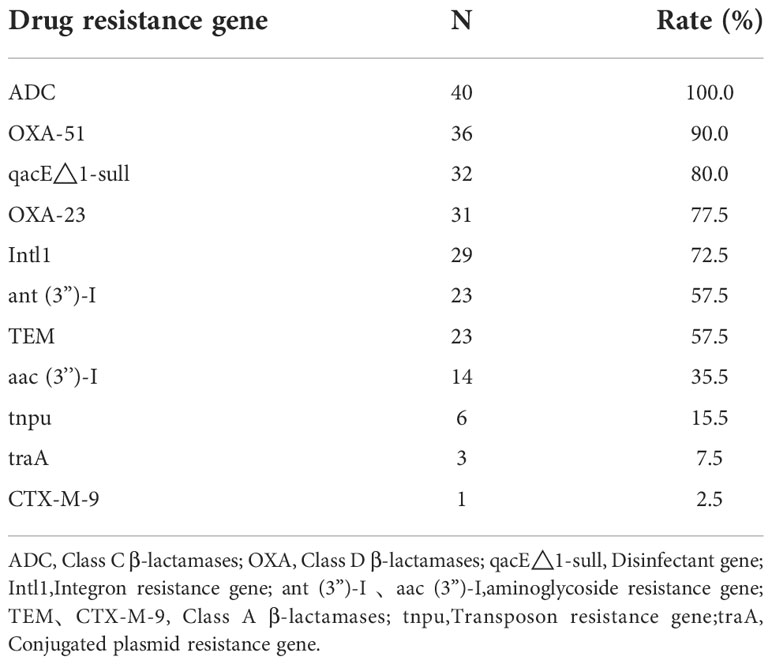
Table 4 Detection of main drug resistance genes of 40 crab strains.
40 CRAB PFGE clustering map showed that the number of electrophoretic bands ranged from 22 to 29, as shown in Figure 2. Divided into A1-A19, 19 different types of belt. The resistance spectrum for each type is detailed in Table 4. Each band type contained 1-9 strains, of which strains 4, 10, 12, 13, 16, 28, 32, 33, 34 were A5 type, strains 1,8,17,20,29,35,37,38 were A18 type, strains 2,7,25,39,40 were A9 type, strains 15,23 were A13 type, strains 6,14 were A17 type, and the remaining 14 band types contained only 1 strain. See Figure 3 and Table 2.
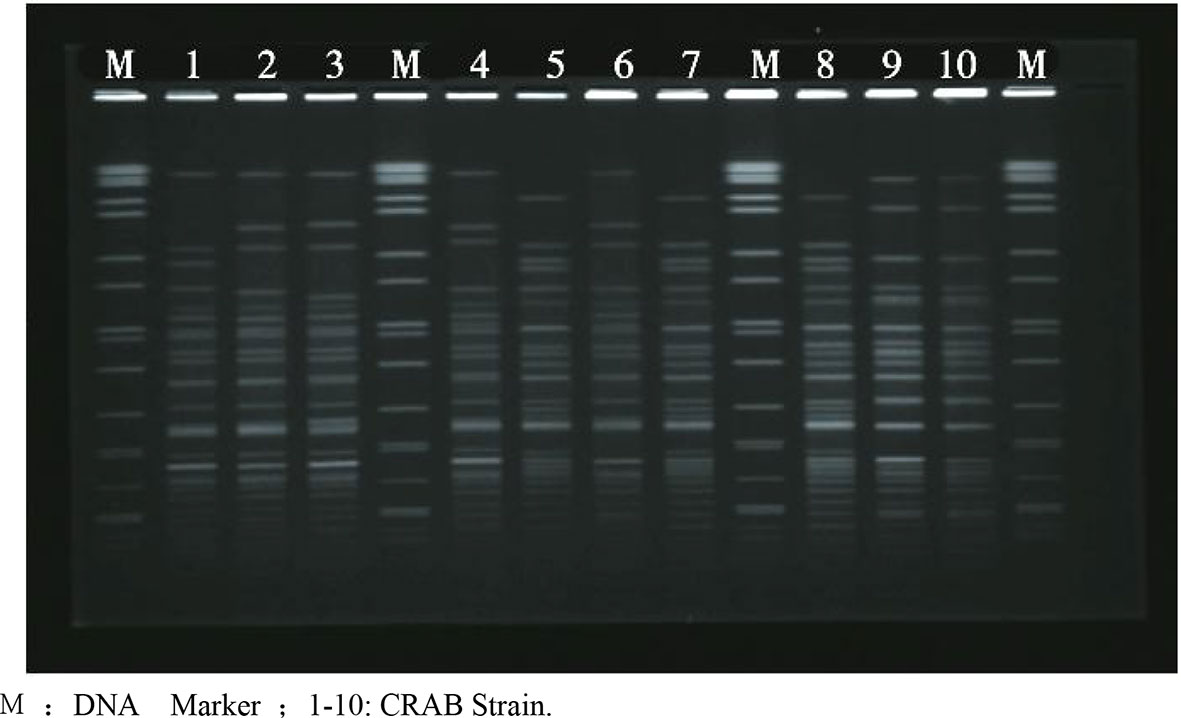
Figure 2 PFGE electrophoresis patterns of some crab strains. M: DNA Marker ;1-10: CRAB Strain.
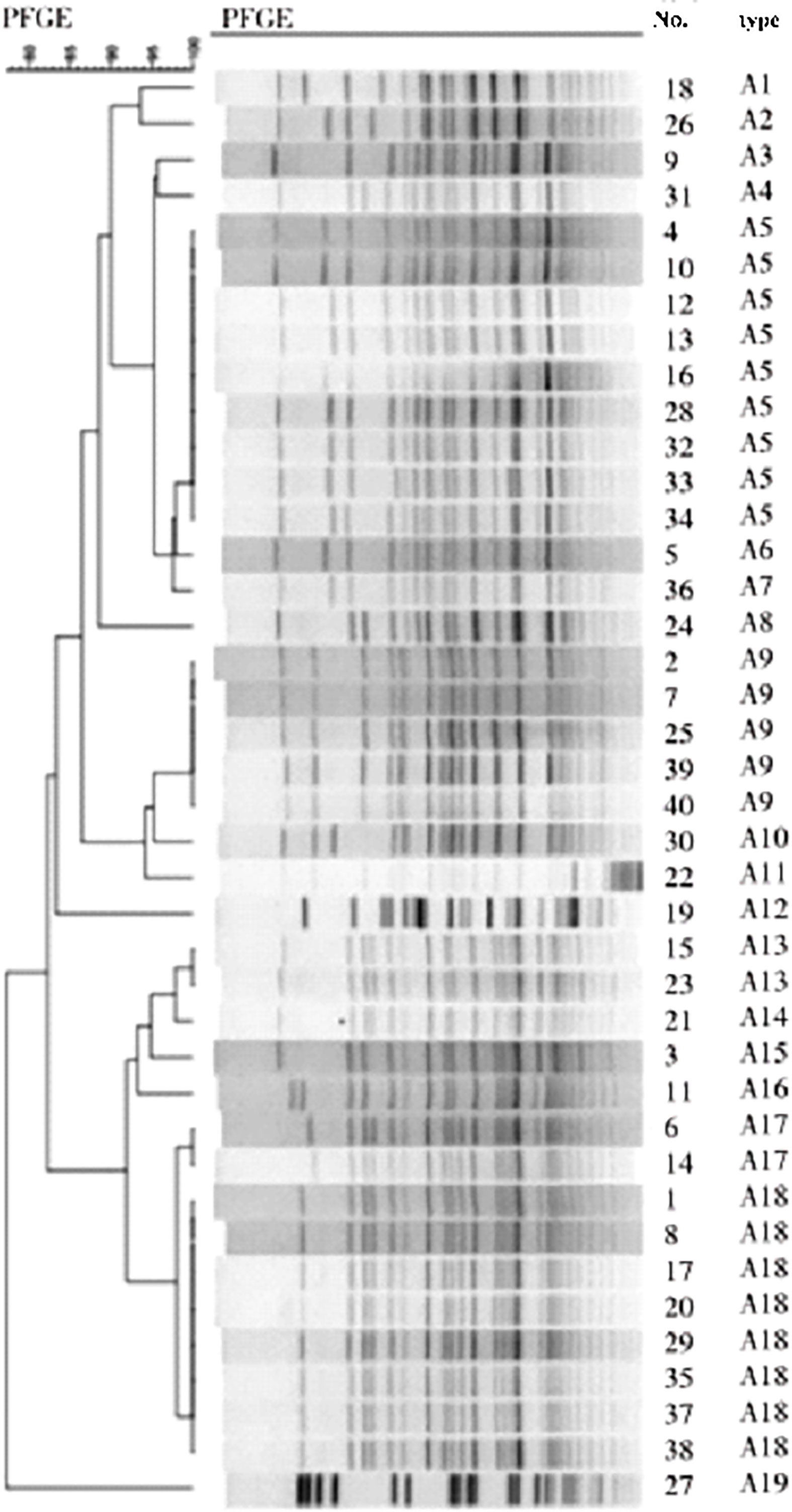
Figure 3 PFGE clustering tree of 40 crabs.
Acinetobacter baumannii is an aerobic gram-negative conditional pathogen, which widely exists in the hospital environment. Due to its strong viability and resistance, the infection of Acinetobacter baumannii has become a difficult problem to be solved in hospitals all over the world. Due to the irrational use of antibiotics and the lack or inadequate implementation of nosocomial infection management and control measures, the drug resistance of bacteria is on the rise. Multidrug resistant AB has become the main pathogen of nosocomial infection (Anunnatsiri and Tonsawan, 2011) and spread all over the world. Among them, 40 CRAB strains were resistant to cefotaxime, ceftriaxone, levoflOXAcin, tobramycin, ceftazidime, imipenem, meropenem, piperacillin, piperacillin/tazobactam, gentamicin, amikacin, cefepime and minocycline mic50. MIC90 also far exceeded the break point of drug resistance, and the drug resistance phenomenon was very serious. The drug resistance mechanism of multidrug resistant AB is very complex, including the production of various drugs β-Lactamase, decrease of outer membrane permeability, change of drug target, overexpression of efflux pump and production of biofilm (Ming, 2015).
Produced by bacteria β- Lactamases are mainly divided into four categories, and category a mainly refers to broad spectrum β- Lactamases, including TEM, SHV, KPC, etc; Class B metal β- Lactamases, including imp, vim and sim; Class C is amp C enzyme; Class D is OXAcillinase, also known as OXAcarbapenemase, of which OXA-23 is the most common OXAcillinase in China. Various β-The combined action of lactamases can mediate the resistance of Acinetobacter baumannii to penicillin, carbapenems, monocyclic amides and cephalosporins (Wanzhen et al., 2012). In this study, the resistance rate of 40 CRABs to carbapenems and cephalosporins was 100%, indicating that β- Lactamase is one of the causes of drug resistance.
The detection rates of OXA-51 and OXA-23 were 90.0% and 77.5% respectively. The detection rate of OXA-23 gene was basically similar to that reported in the domestic literature (Qinglan et al., 2019), and no new subtype was detected. The appearance of CRAB is closely related to the accumulation of drug-resistant genes by integron. Integron is an original that captures drug-resistant genes and can be transmitted. It exists on chromosomes, plasmids or transposons. Class I ~ III integron is mainly related to ab resistance, of which class I integron is the most common. The detection rate of class I integron (intl1 gene) in our hospital is 72.5%, which is basically similar to that reported in domestic literature. The detection rates of aminoglycoside resistant genes ant (3 ‘‘) -i and AAC (3) -i were 57.5% and 35%, respectively,. 0%. It is reported in the literature that 16S rRNA methylase can cause bacterial resistance to aminoglycoside antibiotics (Daiguihua, Yanbinbin, Wangbin, Fengweisi, Malinlin, Limingcheng, 2019). Such genes can be transmitted between strains through a variety of ways, such as transposons, integrons and plasmids, which may lead to epidemics in hospitals (Yi, 2020), and the epidemics of aminoglycoside resistance genes in different hospitals or in the same hospital at different times (He et al., 2017). The results of this study showed that there were only 11 strains containing aminoglycoside resistant gene ant (3’’) -i + aac(3) -i CRAB, which was not the main resistant gene prevalent in the hospital.
The detection rate of disinfectant resistance gene qacE△1-sull was 80.0%. At present, the most studied disinfectant resistance gene is quaternary ammonium disinfectant resistance gene, namely qac gene. The qac gene family includes qac A, qac B, qac C, qac d, qacE, qac F, etc. (Harding et al., 2018). It is a common phenomenon that clinical AB strains carry qacE△1 gene (Hamidian and Nigro, 2019), which shows resistance through the expression of multiple compound efflux pump genes of pathogenic bacteria. Literature (Lishuwang, Jiangmeijie, Zhanggang, 2013) reported that the detection rate of qacE△1-sull was more than 90%. The detection rate of qacE△1-sull in our hospital was 80%, slightly lower than that reported in the literature, but we should also pay attention to it. The detection rate of integron resistance gene intl1 was 72.5% Integron can make qacE△1-sull gene spread between AB and ab. it is speculated that the high detection rate of qacE△1-sull gene in this hospital may be related to the high detection rate of integron resistant gene. The detection rate of transposon resistance gene in our hospital was 15.0%, which was relatively low. TEM type β- Lactamases belong to broad spectrum β- The encoding gene of lactamase, which is located on the TNL sequence of the transposon of the drug-resistant plasmid, can be transferred to other bacteria through the conjugation of the encoding plasmid, and can hydrolyze the third generation cephalosporins. This is also the main reason for the increasing resistance of AB clinical isolates to cephalosporins in recent years. The detection rate of ADC was as high as 100%, indicating that ADC was an inherent drug resistance gene of ab. Research (Liu et al., 2018) shows that ADC will change its ability to hydrolyze drugs when its coding gene is mutated. The detection rate of conjugated plasmid resistance gene TRAA was 7.5%. No new drug resistance genotype was found in this test.
In this study, the number of CRAB strains is relatively small, and CRAB resistant to imipenem and meropenem has not been studied. Some cases of increased sensitivity of AB to imipenem may be omitted due to the deletion of OXA-23 gene (Scaife et al., 1995). More samples of different types will be collected in the future to analyze the relationship between drug resistance and drug resistance genes and the homology. KPC gene is not detected in this study, so KPC chromogenic plate method can be considered for verification.
This study showed that the main drug resistance genes of CRAB were ADC, OXA-51 and OXA-23. TEM, ADC, OXA-51 and OXA-23 genotypes are higher in CRAB, which is the main cause of β-lactam resistance. Homology study showed that there was a small range of drug resistance gene clone transmission in Acinetobacter baumannii in our hospital. Hospital infection control monitoring should be actively carried out to prevent CRAB clone transmission. We should reasonably use antibacterial drugs, strengthen the improvement of existing antibacterial drugs and the research and development of new antibacterial drugs.
The original contributions presented in the study are included in the article/supplementary material. Further inquiries can be directed to the corresponding author.
This study was conducted in accordance with the Declaration of Helsinki and approved by the ethics committee of Inner Mongolia Baogang hospital.
H-BG conceived of the study, and H-LH participated in its design and coordination, and Y-YL helped to draft the manuscript. All authors read and approved the final manuscript.
2017 Autonomous Region Health and Family Planning Scientific Research Plan Project 201702127 Carbapenem-resistant A. baumannii drug resistance mechanism study.
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article, or claim that may be made by its manufacturer, is not guaranteed or endorsed by the publisher.
Abdi, S. N., Ghotaslou, R., Ganbarov, K., Mobed, A., Tanomand, A., Yousefi, M., et al. (2020). Acinetobacter baumannii efflux pumps and antibiotic resistance. Infect. Drug Resist. 13, 423–434. doi: 10.2147/IDR.S228089
Anunnatsiri, S., Tonsawan, P. (2011). Risk factors and clinical outcomes of multidrug-resistant acinetobacter baumannii bacteremia at a university hospital in Thailand. Southeast. Asian J. Trop. Med. Public Health 42 (3), 693–703. doi: 10.1016/j.ijid.2010.02.2042
Chen, C. H., Lin, L. C., Chang, Y. J., Chen, Y. M., Chang, C. Y., Huang, C. C. (2015). Infection control programs and antibiotic control programs to limit transmission of multi-drug resistant acinetobacter baumannii infections: Evolution of old problems and new challenges for institutes. Int. J. Environ. Res. Public Health 12 (8), 8871–8882. doi: 10.3390/ijerph120808871
Daiguihua, Yanbinbin, Wangbin, Fengweisi, Malinlin, Limingcheng (2019). Characteristics and homology analysis of metalloenzyme and integrase genes carried by multidrug resistant acinetobacter baumannii. J. Beihua. Univ. (NATURAL. Sci. EDITION). 20 (03), 333–336. doi: CNKI:SUN:ZLYY.0.2019-03-010
Hamidian, M., Nigro, S. J. (2019). Emergence, molecular mechanisms and global spread of carbapenem-resistant acinetobacter baumannii. Microb. Genom. 5 (10), e000306. doi: 10.1099/mgen.0.000306
Harding, C. M., Hennon, S. W., Feldman, M. F. (2018). Uncovering the mechanisms of acinetobacter baumannii virulence. Nat. Rev. Microbiol. 16 (2), 91–102. doi: 10.1038/nrmicro.2017.148
He, P., Li, S. W., Wan, X. Y. (2017). The mechanism of drug resistance in acinetobacter baumannii and updates of development in novel antibiotics. Zhonghua. Nei. Ke. Za. Zhi. 56 (10), 777–780. doi: 10.3760/cma.j.issn.0578-1426.2017.10.017
Hu, F. P., Guo, Y., Zhu, D. M., Wang, F., Jiang, X. F., Xu, Y. C., et al. (2016). Resistance trends among clinical isolates in China reported from CHINET surveillance of bacterial resistance, 2005-2014. Clin. Microbiol. Infect. 22 Suppl 1, S9–14. doi: 10.1016/j.cmi.2016.01.001
Humphries, R., Bobenchik, A. M., Hindler, J. A., Schuetz, A. N. (2021). Overview of changes to the clinical and laboratory standards institute Performance standards for antimicrobial susceptibility testing, M100, 31st edition. J. Clin. Microbiol. 59 (12), e0021321. doi: 10.1128/JCM.00213-21
Lishuwang, Jiangmeijie, Zhanggang (2013). Detection of plasmid mediated quinolone resistance gene and qacE△1 gene of multidrug resistant acinetobacter baumannii isolated at different times in the hospital. Chin. J. Exp. Clin. Infect. Dis. 7 (05), 717–720.
Liu, Q., Hassan, K. A., Ashwood, H. E., Gamage, H. K. A. H., Li, L., Mabbutt, B. C., et al. (2018). Regulation of the aceI multidrug efflux pump gene in acinetobacter baumannii. J. Antimicrob. Chemother. 73 (6), 1492–1500. doi: 10.1093/jac/dky034
Lockhart, S. R., Abramson, M. A., Beekmann, S. E., Gallagher, G., Riedel, S., Diekema, D. J., et al. (2007). Antimicrobial resistance among gram-negative bacilli causing infections in intensive care unit patients in the united states between 1993 and 2004. J. Clin. Microbiol. 45 (10), 3352–3359. doi: 10.1128/JCM.01284-07
Ming, Y. (2015). Lun research progress on drug resistance mechanism of acinetobacter baumannii. Chin. J. Exp. Diagn. 19 (12), 2156–2158. doi: CNKI:SUN:ZSZD.0.2015-12-064
Qinglan, L., Bixiao, W., Huang, L., zhangyaoping (2019). Carbapenem resistant acinetobacter baumannii in Western guangxi β- genotyping of lactamase. Lab. Med. Clin. 16 (12), 1665–1668. doi: CNKI:SUN:JYYL.0.2019-12-011
Scaife, W., Young, H. K., Paton, R. H., Amyes, S. G. (1995). Transferable imipenem-resistance in acinetobacter species from a clinical source. J. Antimicrob. Chemother. 36 (3), 585–586. doi: 10.1093/jac/36.3.585
Wanzhen, L., Lu, Y., Guilan, W., Weihua, P., Xuefei, H., Yang, Y. (2012). Studies on six genes and isabal insertion sequences of carbapenem resistant acinetobacter baumannii. Lab. Med. 27 (09), 749–753. doi: 10.3969/j.issn.1673-8640.2012.09.014
Yanan, M., Sumei, W., Jiandong, Z. (2021). Research progress on drug resistance mechanism of carbapenem resistant acinetobacter baumannii. Med. Theory Pract. 34 (15), 2578–2580. doi: 10.19381/j.issn.1001-7585.2021.15.009
Yi, X (2020). Detection and homology analysis of multidrug resistant genes in acinetobacter baumannii. Kunming. Med. Univ. doi: 10.27202/d.cnki.gkmyc.2020.000200
Yuxing, N, Hong, S. (2007). Clinical microbiology and testing (Beijing: People's Health Publishing House), 159–162.
Keywords: carbapenem resistant Acinetobacter baumannii, drug resistance gene, pulsed field gel electrophoresis, homology, infection microbiology
Citation: Huang H-L, Li Y-Y and Guo H-B (2023) Detection and homology analysis of carbapenem resistant Acinetobacter baumannii resistance gene. Front. Cell. Infect. Microbiol. 12:987260. doi: 10.3389/fcimb.2022.987260
Received: 06 July 2022; Accepted: 08 September 2022;
Published: 06 January 2023.
Edited by:
Yang Zhang, University of Pennsylvania, United StatesReviewed by:
Yu Zhou, Institut Pasteur of Shanghai (CAS), ChinaCopyright © 2023 Huang, Li and Guo. This is an open-access article distributed under the terms of the Creative Commons Attribution License (CC BY). The use, distribution or reproduction in other forums is permitted, provided the original author(s) and the copyright owner(s) are credited and that the original publication in this journal is cited, in accordance with accepted academic practice. No use, distribution or reproduction is permitted which does not comply with these terms.
*Correspondence: Hong-Bo Guo, aG9uZzIyYm9AMTYzLmNvbQ==
†These authors have contributed equally to this work
Disclaimer: All claims expressed in this article are solely those of the authors and do not necessarily represent those of their affiliated organizations, or those of the publisher, the editors and the reviewers. Any product that may be evaluated in this article or claim that may be made by its manufacturer is not guaranteed or endorsed by the publisher.
Research integrity at Frontiers
Learn more about the work of our research integrity team to safeguard the quality of each article we publish.